Back to Journals » Drug Design, Development and Therapy » Volume 20
Remimazolam Reduces the Cough Reflexes in Elderly Patients Undergoing Fiberoptic Bronchoscopy Under Remifentanil/Cipepofol-Based Anaesthesia: A Randomized Clinical Trial
Authors Wang X, Qin Y, Wei Y ![]() , Xu B, Lan H, Huang X, Chen Q, Cao H, Wu X, Chen H, Liu S, Guan X
, Xu B, Lan H, Huang X, Chen Q, Cao H, Wu X, Chen H, Liu S, Guan X ![]()
Received 10 November 2025
Accepted for publication 27 January 2026
Published 7 February 2026 Volume 2026:20 580302
DOI https://doi.org/10.2147/DDDT.S580302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas Panos
Xianting Wang,1,* Yanlin Qin,1,* Yingbing Wei,1,* Bing Xu,2 Hongmeng Lan,1 Xiaofang Huang,3 Qiuling Chen,1 Huiyu Cao,1 Xiaoshan Wu,1 Huihe Chen,4 Susu Liu,1 Xuehai Guan1
1Department of Anaesthesiology, the First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, People’s Republic of China; 2Department of Rehabilitation, the People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, Guangxi, People’s Republic of China; 3Department of Anaesthesiology, the First People’s Hospital of Qinzhou, Qinzhou, Guangxi, People’s Republic of China; 4Department of Emergency, Wuming Hospital of Guangxi Medical University, Naning, Guangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuehai Guan, Department of Anaesthesiology, the First Affiliated Hospital of Guangxi Medical University, 6 Shuangyong Road, Nanning, Guangxi, 530021, People’s Republic of China, Tel\Fax +86-771-5356250, Email [email protected] Susu Liu, Department of Anaesthesiology, the First Affiliated Hospital of Guangxi Medical University, 6 Shuangyong Road, Nanning, Guangxi, 530021, People’s Republic of China, Tel\Fax +86-771-5356250, Email [email protected]
Background: Fiberoptic bronchoscopy (FOB) is one of the most common critical procedures for diagnosis and treatment of respiratory diseases. We aimed to determine whether remimazolam reduces the cough reflexes in patients undergoing FOB under remifentanil/cipepofol-based anaesthesia.
Methods: This was a single-center, single-blinded, randomized study. We included 90 adult patients underwent FOB with ASA I–III, aged 60– 90 years. Patients were randomly assigned to cipepofol (CIP) group or remimazolam-cipepofol (RMZ-CIP) group. In the CIP group, anaesthesia was induced sequentially with remifentanil and cipepofol. In the RMZ-CIP group, anaesthesia was induced sequentially with remifentanil, remimazolam, and cipepofol. A laryngeal mask airway (LMA) was inserted in both groups when the BIS ≤ 60. Anaesthesia was maintained with remifentanil and cipepofol with a BIS value between 40 and 60. The primary outcome was the incidence and severity of cough reflexes during the first FOB. The secondary outcomes included vital signs, characteristics of FOB and anaesthesia, administration of vasoactive drugs, and adverse events.
Results: The incidence of cough reflexes during FOB was lower in the RMZ-CIP group than that in the CIP group (38% vs 62%, p=0.029). The total consumption of cipepofol and remifentanil was higher in CIP group than in the RMZ-CIP group (40.89 [31.41– 61.90] mg vs 27.019 [21.41– 41.91] mg, p< 0.001; 0.38 [0.42– 0.50] mg vs 0.22 [0.20– 0.26] mg, p< 0.001). Cipepofol consumption during anaesthesia induction was higher in the CIP group than in the RMZ-CIP group (p< 0.001). No difference was found in terms of vital signs, the characteristics of FOB, anaesthesia, and adverse events.
Conclusion: The combination of remimazolam reduced the incidence of cough reflexes and dosage of cipepofol and remifentanil in elderly patients undergoing FOB under remifentanil/cipepofol-based anaesthesia.
Clinical Trial Registration: Chinese Clinical Trial Registry (ChiCTR2300079139).
Keywords: remimazolam, cipepofol, cough reflex, fiberoptic bronchoscopy
Introduction
Population aging is increasing globally, and this demographic change has impacted health, socioeconomic, and healthcare system challenges.1 With advancing age, the pulmonary system of geriatric individuals exhibits increased vulnerability to pathogenic microorganisms.2 Fiberoptic bronchoscopy (FOB) is an important procedure in the diagnosis and treatment of respiratory diseases. Several guidelines recommend FOB under optimal sedation, which improves the comfort of surgeons and patients and minimizes adverse events, such as cough reflexes, bronchospasm, and perioperative stress.3,4 Complex FOB procedures, such as endobronchial inspection, transbronchial lung biopsy, and ultrasound-guided needle aspiration, require patients to exert restraint and cooperation, which can be achieved with general anaesthesia.
Various sedatives such as benzodiazepines, propofol, ketamine, and dexmedetomidine are often used in FOB. However, shortcomings include undetermined onset time and offset time, injection pain, respiratory depression, or circulatory adverse events make anaesthesiologists unwilling to use them in critically ill patients.5 Cipepofol is a newly designed intravenous general anaesthetic. Cipepofol generates potent sedation by attaching to gamma-aminobutyric acid-A-binding receptors (GABAARs). It is non-inferior to propofol in terms of anaesthesia success, short onset time, and offset time, with no injection pain, lower risk of hypotension, and respiratory depression.6–9 Cipepofol reduced the incidence of agitation in intensive care unit patients and was safely and effectively used for long-term sedation in patients on mechanical ventilation safely and effectively.10–12 Our previous report showed that a combination of cipepofol and remifentanil can be successfully used for FOB.8
Remimazolam, a novel ultra-short-acting benzodiazepine, exerts sedative effects by binding to GABAARs in the central nervous system.13 Remimazolam has been used for gastrointestinal endoscopy, bronchoscopy, general anaesthesia, and anaesthesia in critically ill patients with hepatic and renal dysfunction safely and effectively.5,14–16 No trial has investigated the potential effect of the combination of cipepofol and remimazolam in preventing cough reflexes in elderly patients undergoing FOB. We hypothesized that the combination of cipepofol and remimazolam would significantly reduce the incidence of cough reflexes compared with cipepofol alone in elderly patients undergoing FOB, resulting in less potential tracheal injury and improved comfort of surgeons and patients.
Methods
Study Design and Patients
This was a single-center, prospective, randomized controlled trial. The study protocol was approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangxi Medical University (No.2023-E739-01; Chairperson: Songqing He; approval date: December 22, 2023). This trial was registered at https://www.chictr.org.cn (26 December 2023, ChiCTR2300079139). The guiding principles of the Declaration of Helsinki and the 2010 CONSORT statement were followed when conducted and reported. Written informed consent was obtained from all the patients before enrollment in the trial.
Ninety patients scheduled to undergo FOB under general anaesthesia were included. The inclusion criteria were as follows: aged 60–90 years, ASA I–III. Patients with severe hypertension (systolic blood pressure ≥180 mmHg or diastolic blood pressure ≥110 mmHg), severe arrhythmias, severe cardiac insufficiency of New York Heart Association (NYHA) class III or higher, severe hepatic or renal dysfunction, history of psychotropic drug use, and difficult airways were excluded. Women in labor or breastfeeding and those whose preoperative state of consciousness was difficult to determine independently or accurately were excluded too.
Randomization and Masking
Random numbers were generated using the EpiCalc 2000 software. All patients were randomly assigned to receive anaesthesia with either cipepofol (CIP group) or cipepofol combined with remimazolam (RMZ-CIP group) during FOB in a 1:1 ratio. Sealed envelopes were used to hide the group allocation. A few minutes before anaesthesia induction, an assistant who was not involved in anaesthesia opened the envelopes to prepare the medications. The patients, surgeons, cough reflex assessors, attending anaesthesiologist in charge of the post anaesthesia care unit (PACU), and data collectors were unaware of group allocation. The attending anaesthesiologist who performed the anaesthesia was not blinded to the group allocation for patient safety. The data analysts were unaware of the group allocation only after the data were analyzed.
Interventions
All patients fasted for 8 hours preoperatively. Peripheral veins were established 15 min before surgery, and infusion of Ringer’s lactate was initiated to maintain potency (4 mL/kg/h). Standard monitoring included non-invasive blood pressure (NIBP), electrocardiogram, peripheral capillary oxygen saturation (SpO2), end-expiratory carbon dioxide (ETCO2), and Bispectral Index (BIS; Covidien, MA, United States). Before anaesthesia induction, all patients received oxygen (100%, 6 L/min) using a face mask for 3 min. The doses and infusion rates of cipepofol and remimazolam were based on the drug inserts and pre-experiments. In the CIP group, anaesthesia was induced using remifentanil (Hengrui, Lianyungang, China) and cipepofol (Haisco, Shenyang, China). Remifentanil was administered by using a target-controlled infusion pump (Veryark, Nanning, China). The initial plasma concentration of remifentanil was set at 3 ng/mL. After the plasma concentration of remifentanil equilibrated with the concentration in the effector compartment, cipepofol was administrated in an initial dose of 0.4 mg/kg, added 0.1 mg/kg each time with 1 min interval until BIS ≤ 60. When the BIS ≤ 60, a laryngeal mask airway (LMA) was inserted, and the allocation was verified by chest auscultation. In the RMZ-CIP group, anaesthesia was induced with remifentanil, remimazolam (Hengrui, Lianyungang, China), and cipepofol. Remifentanil was administered in the same manner as that in the CIP group. After the plasma concentration of remifentanil equilibrated with the concentration in the effector compartment, remimazolam (0.2 mg/kg) was administrated intravenously. Then cipepofol was administrated in an initial dose of 0.2 mg/kg, added 0.1 mg/kg each time with 1 min interval until BIS ≤ 60. The LMA was inserted and the allocation was verified as in the CIP group. In both groups, anaesthesia was maintained with remifentanil (plasma concentration: 2.5–4.5 ng/mL) and cipepofol (0.4–1.5 mg/kg/h), maintaining BIS value within 40 and 60. Two experienced endoscopists performed the FOB through the LMA. Lidocaine (2%) was sprayed with a syringe on the vocal cords (2 mL), trachea (5 mL), main carina (2 mL), right main bronchi (2 mL), and left bronchi (2 mL). To ensure precise delivery of topical lidocaine to the target mucosal area, a modified spraying technique was employed. After drawing up lidocaine into the syringe, an additional 4 mL of air was aspirated to create an air column behind the liquid. This air column was then used to flush the entire volume of lidocaine through the delivery catheter, ensuring complete expulsion of the medication and accurate topical application under direct visual guidance. All drugs were discontinued at the end of FOB, and the patients were sent to the PACU.
Outcome Measures
The primary outcome was the incidence and severity of cough reflexes during the first FOB insertion. Cough severity was scored on a 4-point scale during the first FOB insertion as follows: grade 1 (0 cough); grade 2 (1 or 2 consecutive coughs); grade 3 (3 or 4 consecutive coughs) and grade 4 (≥ 5 consecutive coughs).
The secondary outcomes included the incidence and severity of limb and vocal cord movements (graded on a 4-point scale during the first FOB insertion as previously8), vital signs, anaesthetic and surgical characteristics, and adverse events. NIBP, heart rate, SpO2, respiratory rate, and BIS values were recorded 5 min before anaesthesia induction, at the loss of consciousness (LOC, assessed by MOAA/S), at BIS ≤ 60, at the beginning of FOB, at the end of FOB, and at the time of awakening. Consumption of sedative, analgesic, and vasoactive drugs was determined. The duration of LOC, BIS ≤ 60, FOB, and anaesthesia were recorded. Adverse events (injection pain, hypotension, hypertension, tachycardia [>100 beats/min], bradycardia [<50 beats/min], bronchospasm, nausea and vomiting, dysphoria, delirium, and respiratory depression) occurring during FOB were also recorded. Hypotension was defined as a decrease in mean blood pressure (MBP) of ≥20% from baseline and was treated with ephedrine intravenously. Hypertension was defined as an increase in MBP≥20% from baseline and was treated with urapidil intravenously. Respiratory depression was defined as meeting one of the following criteria: respiratory rate < 8 breaths/min, apnea, or SpO2 ≤ 90% for > 15s.
Sample Size
Our preliminary experiments showed that the cough reflexes rates in the CIP and RMZ-CIP groups were 60 and 28%, respectively. Based on these preliminary results, 38 patients were included in each group using the PASS (version 11.0; NCSS statistical software, Utah, USA, α=0.05 (bilaterally), β=0.80). Considering a potential loss (15%) during follow-up, the sample size was increased to 45 patients in each group.
Statistical Analysis
Statistical analysis was performed using the GraphPad Prism software (version 9.5; Dotmatics, Boston, USA). Normally distributed and variance-equal variables (checked by Shapiro–Wilk test) are presented as means (standard deviation [SD]) and were analyzed by unpaired-t test or repeated-measures two-way analysis of variance (ANOVA) with Geisser-Greenhouse correction, followed by Bonferroni multiple comparison test. Non-normally distributed or variance-unequal variables were presented as medians (interquartile range [IQR]) and were analyzed using the Mann–Whitney U-test. Categorical variables were expressed as numbers (proportions) and analyzed using Fisher’s exact test. A p-value of less significance was set at p < 0.05.
Results
Patients
One hundred and one patients were assessed for eligibility (Figure 1; from December 26, 2023, to July 2, 2024). Of these, five patients did not meet the inclusion criteria and six patients declined to participate. Ninety patients were randomized into either the CIP or RMZ-CIP group (n=45). Three patients were excluded from the final analysis due to protocol violation (n = 1) or missing data (n = 2) in each group (Figure 1).
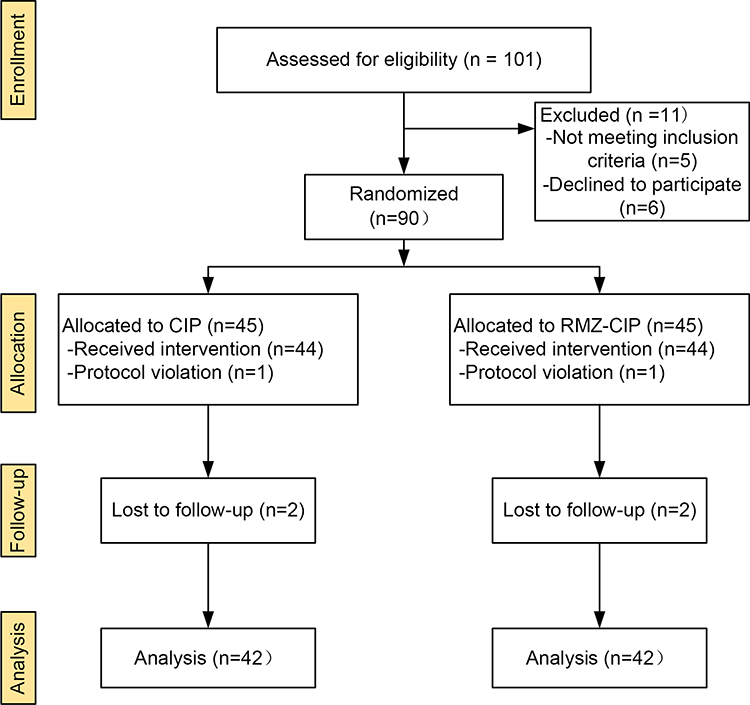 |
Figure 1 CONSORT flow. CONSORT indicates consolidated standards for reporting of trials. |
Tables 1 and 2 summarize the demographic data. The demographics were similar between the groups in terms of age, height, weight, body mass index (BMI), sex, ASA physical status, history, indications for FOB, and diagnostic procedures.
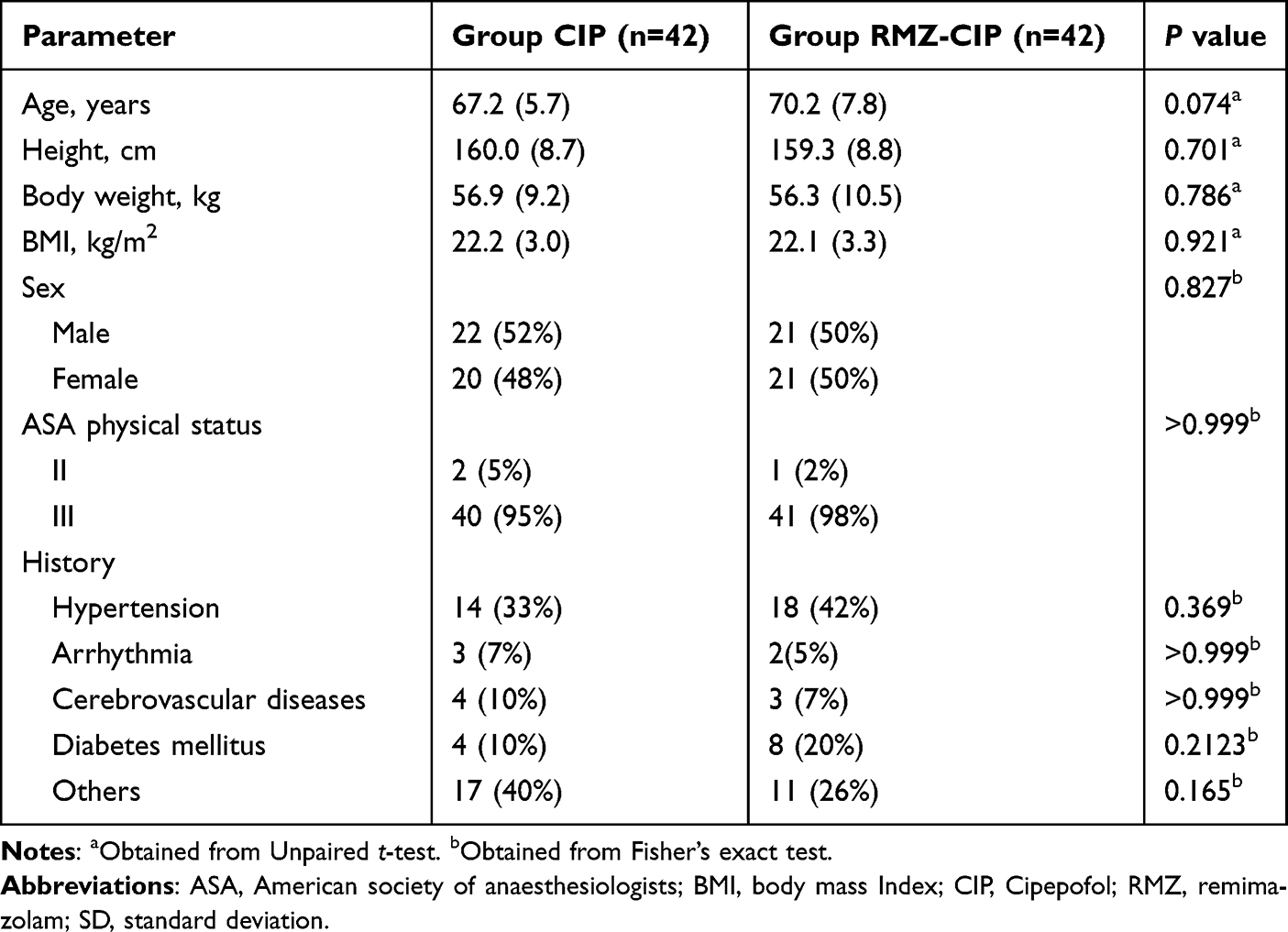 |
Table 1 Patient Characteristic. Values are Means (SD) or Number (Proportion) |
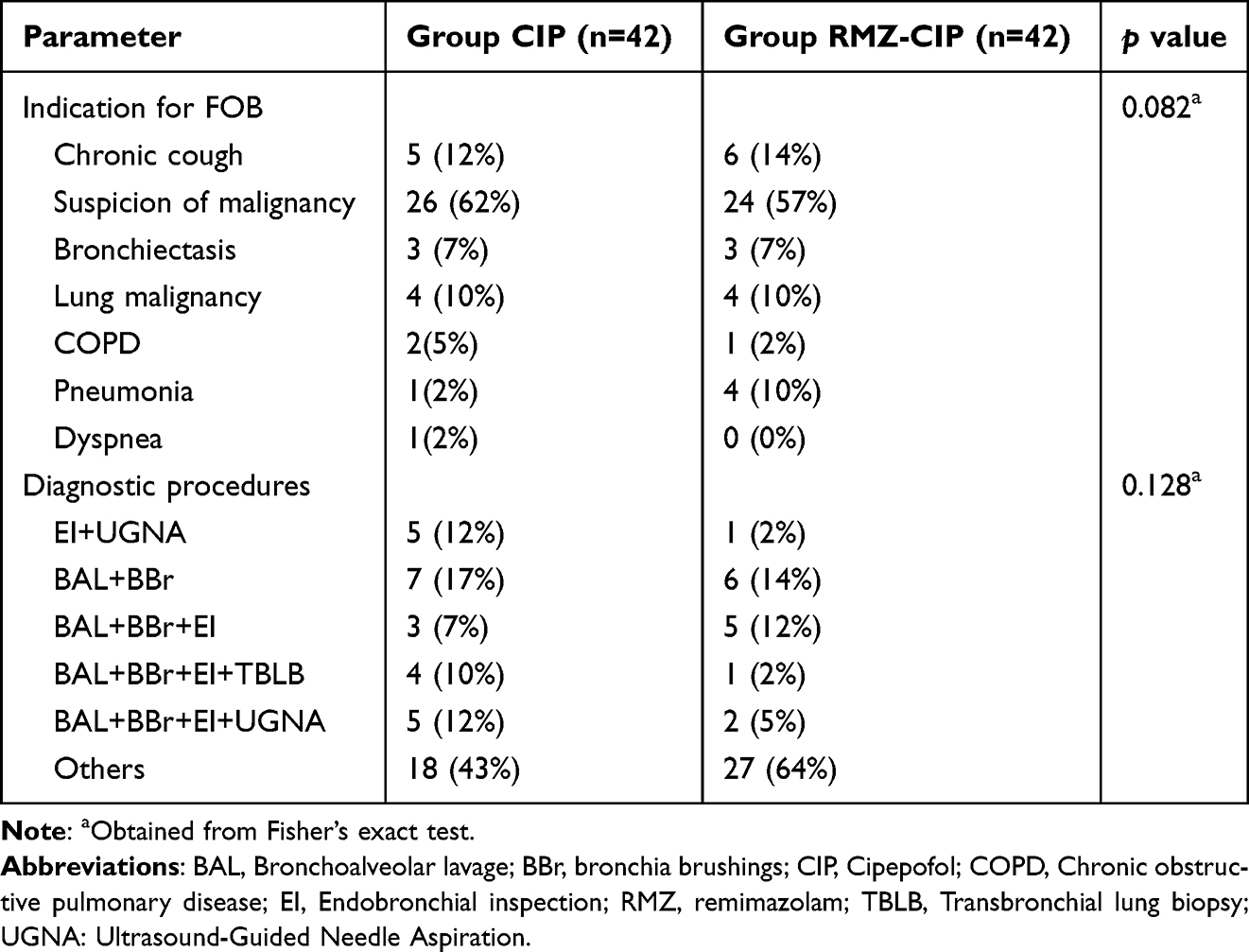 |
Table 2 Indication and Distribution of Fiberoptic Bronchoscopy. Values are Number (Proportion) |
Incidence of Cough Reflexes
The primary outcomes are shown in Table 3. The incidence of cough reflexes was higher in the CIP group than that in the RMZ-CIP group (26 [62%] vs 16 [38%], p=0.029). Eight (19%), nine (21%), and nine (21%) patients in the CIP group were classified as grade 2, grade 3, and grade 4, respectively. Six (14%), six (14%), and four (10%) patients in the RMZ-CIP group were classified as grades 2, 3, and 4, respectively. There was no difference in the severity of the cough reflexes between the groups (p=0.146).
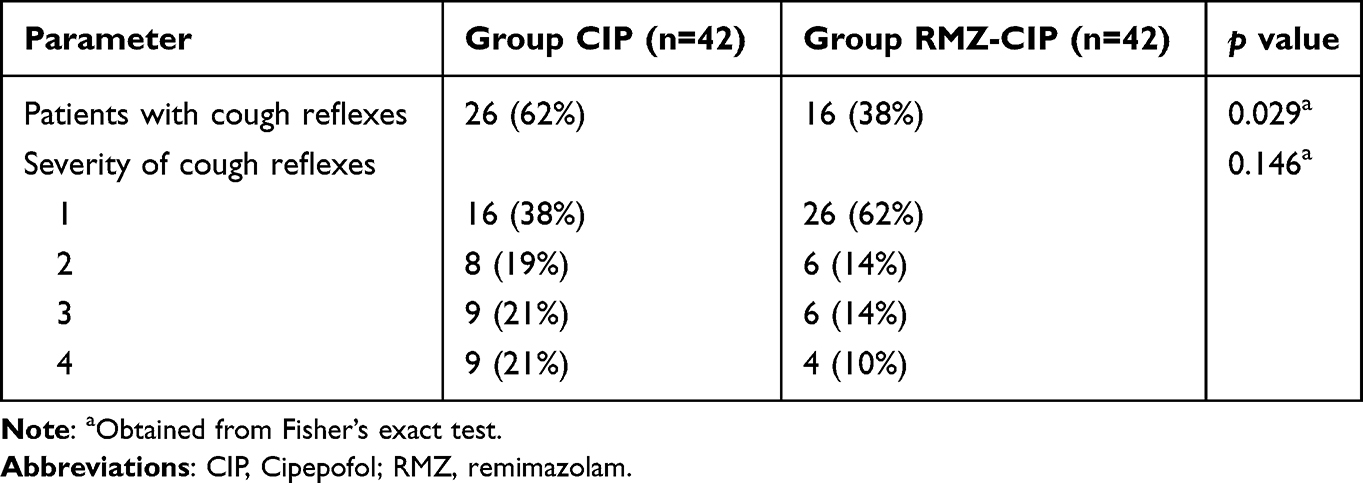 |
Table 3 Incidence and Severity of Cough Reflexes During Fiberoptic Bronchoscopy. Values are Number (Proportion) |
Incidence and Severity of Vocal Cord Reflexes
Table 4 shows the incidence and severity of the vocal cord reflexes. There was no difference in the incidence and severity of vocal cord reflexes between groups (p>0.05).
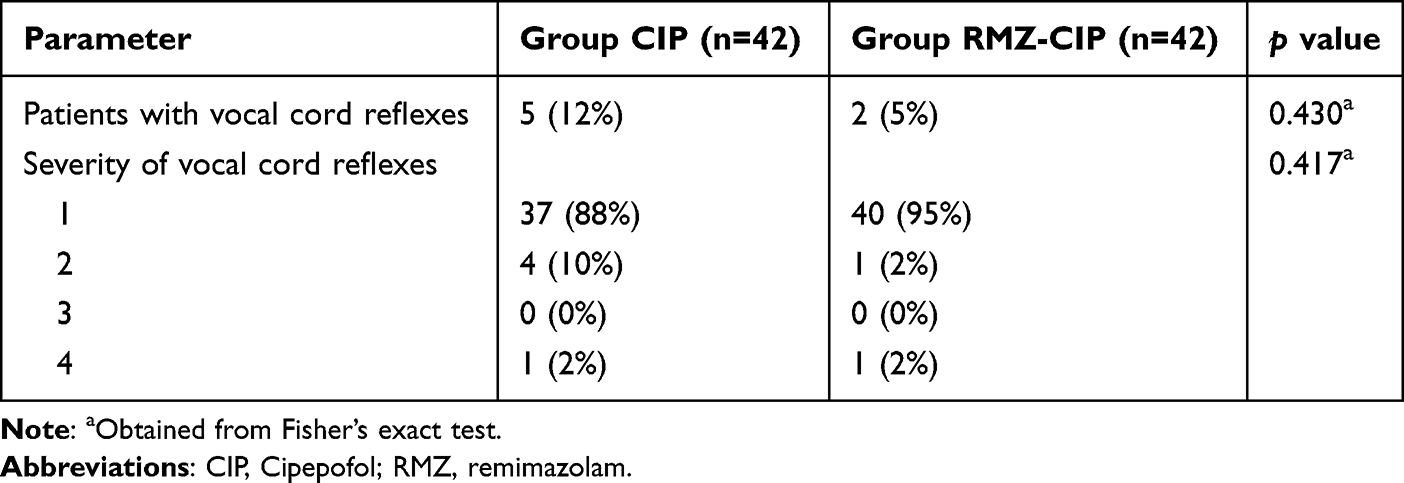 |
Table 4 Incidence and Severity of Vocal Cord Reflexes During Fiberoptic Bronchoscopy. Values are Number (Proportion) |
Incidence and Severity of Limbs Movement
Table 5 shows the incidence and severity of limb movements during FOB. The incidence of limb movement was higher in the CIP group than that in the RMZ-CIP group (18 [43%] vs 5 [12%], p=0.002). In terms of the severity of limb movement, 16 (38%), 2 (5%), and 0 (0%) patients in the CIP group were classified as grade 2, grade 3, and grade 4, respectively, and 5 (12%), 0 (0%), and 0 (0%) patients in the RMZ-CIP group were classified as grade 2, grade 3, and grade 4, respectively. There was a significant difference in the severity of limb movement between the groups (p=0.002).
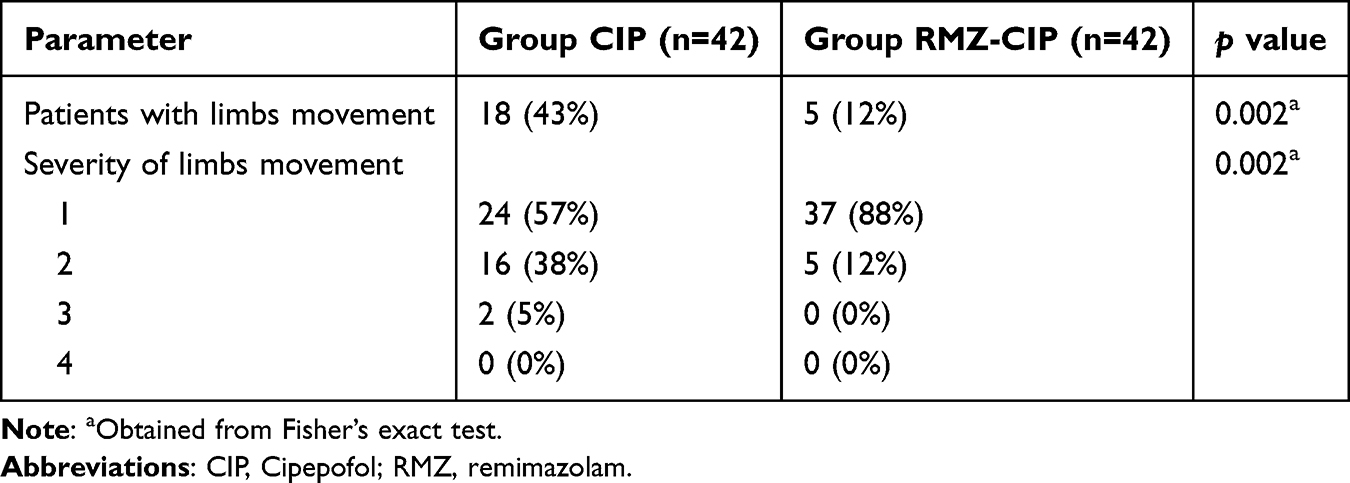 |
Table 5 Incidence and Severity of Limbs Movement During Fiberoptic Bronchoscopy. Values are Number (Proportion) |
Characteristic of Anaesthesia and Surgery
Table 6 summarizes the characteristics of anaesthesia and surgery. There was no difference between the groups in terms of the length from induction to LOC, length from induction to BIS ≤ 60, length from drug withdrawal to eye opening, length of anaesthesia, length of FOB, and crystalloid infusion volume (p>0.05).
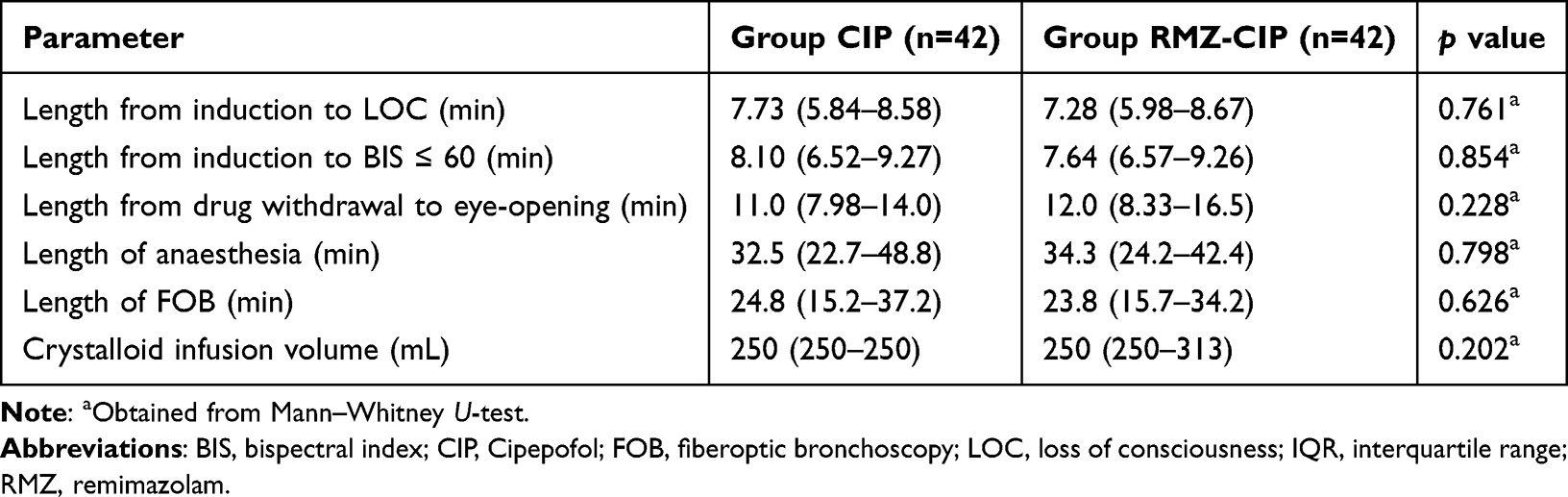 |
Table 6 Characteristic of Anaesthesia and Surgery. Values are Medians (IQR) |
Consumption of Anaesthetic and Vasoactive Drugs
Table 7 summarizes the consumption of anaesthetic and vasoactive drugs. The total consumption of cipepofol was higher in the CIP group than that in the RMZ-CIP group (40.89 [31.41–61.90] mg vs 27.01 [21.41–41.91] mg, p<0.001). The total consumption of remifentanil was higher in the CIP group than that in the RMZ-CIP group (0.38 [0.42–0.50] mg vs 0.22 [0.20–0.26] mg, p<0.001). There was no significant difference in the consumption of ephedrine, atropine, urapidil, or esmolol (p>0.05).
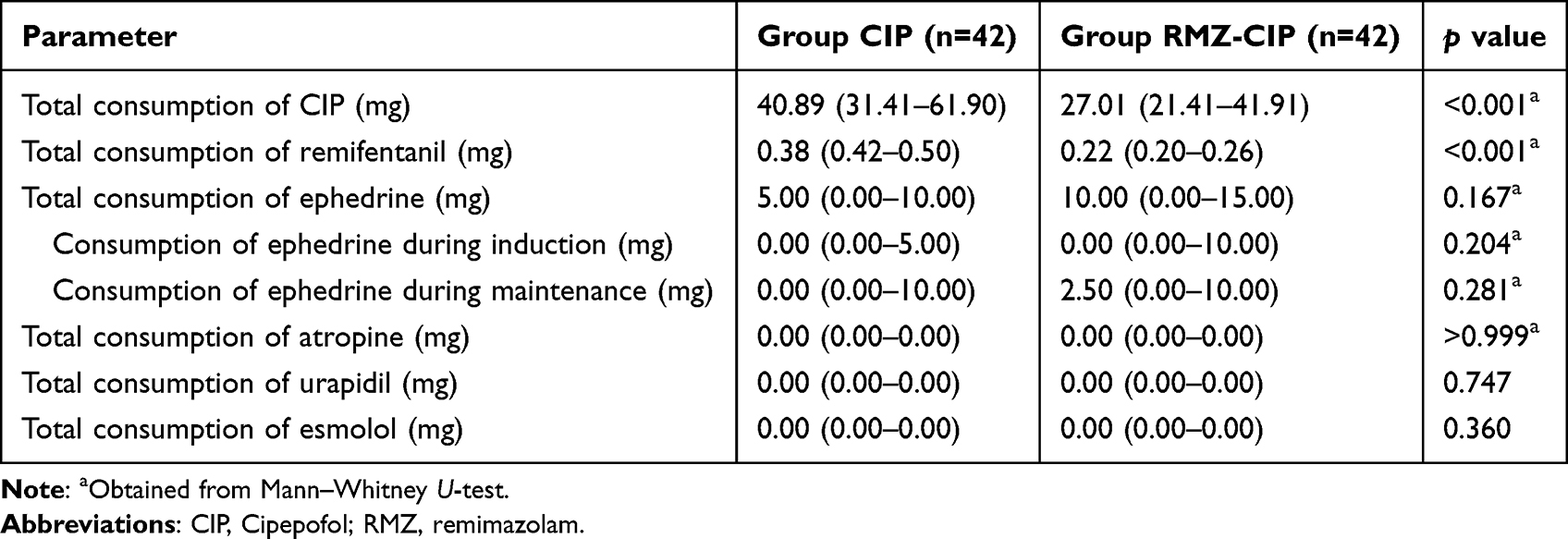 |
Table 7 Consumption of Anaesthetic and Vasoactive Drugs. Values are Medians (IQR) |
Adverse Events
Table 8 summarizes the adverse events. The main adverse events were hypotension, hypertension, tachycardia, and respiratory depression. None of the patients developed injection pain, bradycardia, or delirium. Few patients develop bronchospasm, nausea, and vomiting. However, there were no significant differences between the groups as mentioned above adverse events (p>0.05).
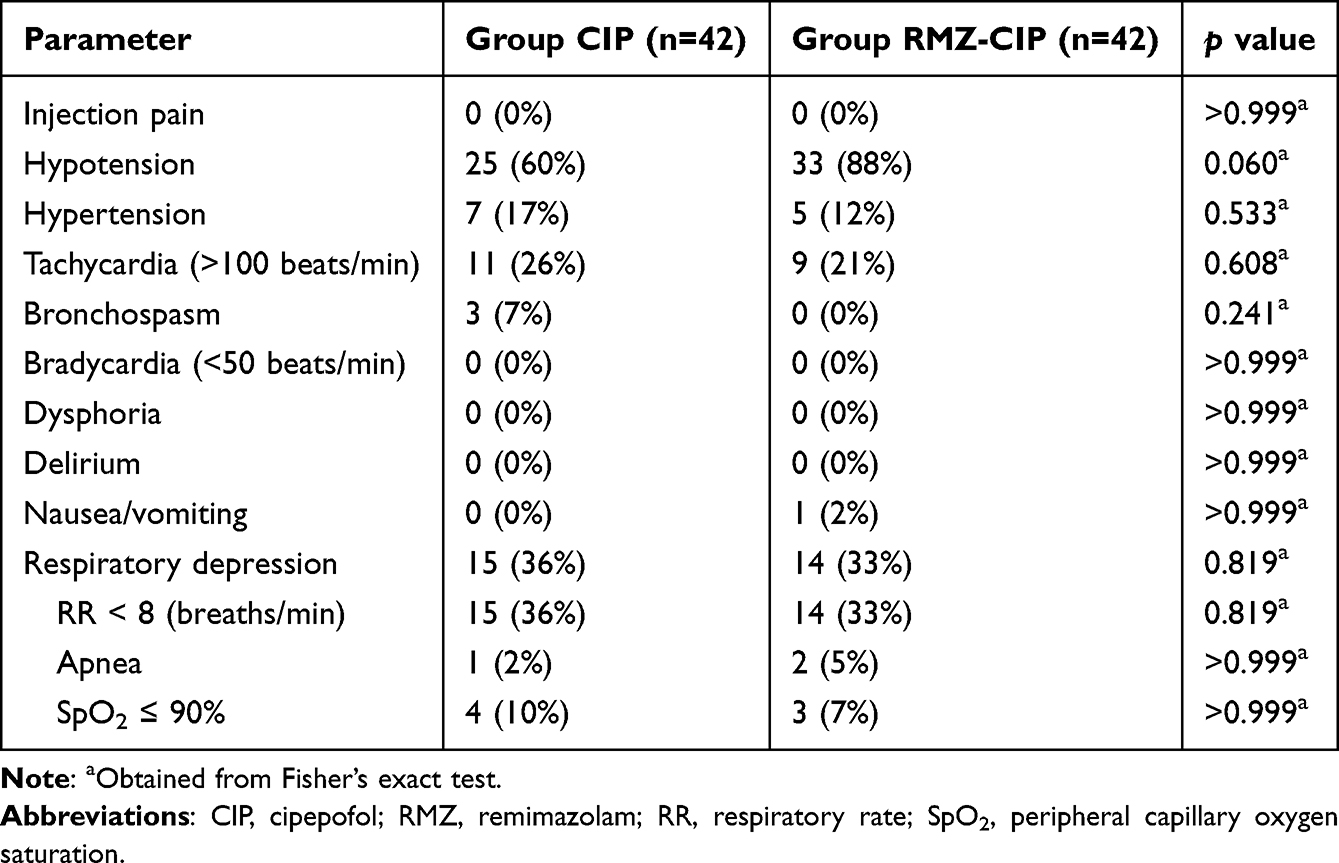 |
Table 8 Incidence of Adverse Event Between Groups. Values are Number (Proportion) |
Vital Signs
Figure 2 shows the vital signs. No significant differences were found between the groups in systolic blood pressure (SBP), diastolic blood pressure (DBP), HR, SpO2, respiratory rate, and BIS at different time points.
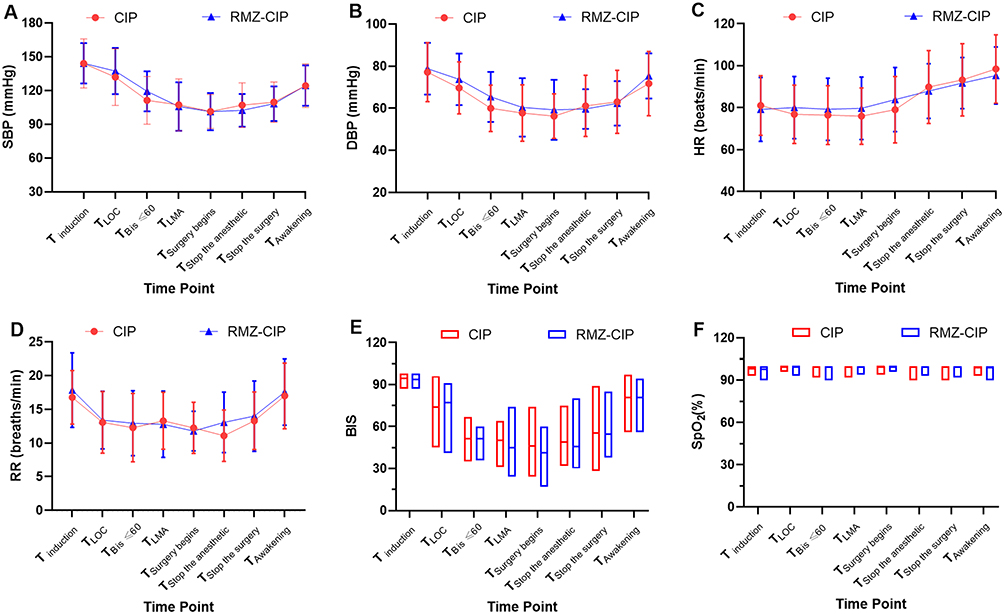 |
Figure 2 Changes in vital signs. Values are mean (SD) (A–D) or medians (IQR) (E and F). Data were analyzed by repeated-measures two-way analysis of variance with the Geisser-Greenhouse correction, followed by Bonferroni’s multiple comparison test. Abbreviations: CIP, cipepofol; Remi, remimazolam; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; SpO2, peripheral capillary oxygen saturation; RR, respiratory rate; LOC, loss of consciousness; BIS, Bispectral Index. |
Discussion
To our knowledge, this is the first study to evaluate the possibility of combining remimazolam with cipepofol to prevent cough reflexes in elderly patients undergoing FOB. The main finding of this study was that the combination of remimazolam reduced the incidence of cough reflexes and decreased the dosages of cipepofol and remifentanil in elderly patients undergoing FOB under remifentanil/cipepofol-based anaesthesia.
Many guidelines and consensuses recommend performing FOB under sedation with propofol, dexmedetomidine, ketamine, or midazolam.3,4 However, drawbacks, such as painful injections, respiratory and circulatory depression, bradycardia, and psychoneurological symptoms, hinder their use in critically ill patients.17–21 Cipepofol, a 2,6-disubstituted phenol derivative, induces anxiolytic, sedative, and hypnotic effects by acting on GABAARs.22 The efficacy and safety of cipepofol during the induction of general anaesthesia were not inferior to propofol.17 No patients in either group developed injection pain in our study, which is consistent with previous reports.17,23 At the same time, the incidence of hypotension was lower than propofol.17 The aforementioned advantages of cipepofol make it widely used in China.8,24–26
Cough reflexes are one of the main complications of FOB, which reduces the comfort of surgeons and patients and may lead to the development of arrhythmias, bronchospasm, tracheal mucosal edema, tracheal mucosal damage, and hypoxemia.27–29 The raphe nucleus of the medulla oblongata is involved in a variety of respiratory processes including breathing, cough, and other respiratory reflex.30 Previous studies have shown that GABAARs in the medulla oblongata inhibit the cough reflexes.31 Remimazolam is a new type of ultra-short-acting benzodiazepine that exerts sedative and anaesthetic effects by binding to GABAARs in the central nervous system. Remimazolam has been successfully used for anaesthesia induction and maintenance,32 with less incidence of post-induction hypotension than propofol.33 Both cipepofol and remimazolam have the ability to lower oxidative stress in the brain, which may be the mechanism underlying the reduction in cough reflexes and limb movement.34,35 Our results showed that the incidence of the cough reflexes and limb movement was higher in the CIP group than in the RMZ-CIP group. The difference between the two groups may be due to the different subunits acting at.32
We found that a higher incidence of cough reflexes was accompanied by a higher incidence of limb movement and severity of limb movement during FOB. This is because airway stimulation may trigger self-protective actions in the patients. Limb movement may affect the surgeon’s operation and increase the risk of airway injury. Conversely, the combination of remimazolam and cipepofol decreased the incidence of cough reflexes, accompanied by a lower incidence and severity of limb movement than cipepofol alone, decreasing the potential risk of airway injury. From the point of this view, we recommended the combination of remimazolam with cipepofol in FOB.
The consumption of cipepofol and remifentanil was higher in the CIP group than that in the RMZ-CIP group. These results imply that remimazolam significantly reduced the dosage of cipepofol and remifentanil under the same BIS values. These data suggest that remimazolam has a synergistic effect with cipepofol and remifentanil.
Adverse events, such as hypertension, tachycardia, respiratory depression, nausea, and vomiting, did not differ between the groups. No patients developed dysphoria, delirium or bradycardia in both groups. Although there was no difference in the incidence of hypotension, it was higher in the RMZ-CIP group than in the CIP group (88% vs 60%, p=0.06). The higher incidence of hypotension in the RMZ-CIP group may be due to several factors. First, the blood pressure is neuromodulated by GABAergic neurons. In spontaneously hypertensive rats, the activation of GABAARs in the posterior lobe of the hypothalamus has been shown to mitigates elevated blood pressure.36 Remimazolam may exert antihypertensive effects by serving as a GABAR agonist and enhancing the inhibitory effect of GABAARs in the central nervous system. Second, it has been shown that midazolam causes hypotension due to its vasodilatory effect by hyperpolarization of vascular wall smooth muscle cells.37 Both remimazolam and midazolam are benzodiazepines and we speculate that they have similar vasodilatory effects. Remimazolam-induced anaphylaxis (RIA) is a rare but serious complication of the IgE- and non-IgE-mediated pathways. Most RIA manifest with hypotension.38,39 Hypoxemia threatens patient safety during FOB therapy The incidence of hypoxemia was 10% and 7% in the CIP and RMZ-CIP groups, respectively, which was lower than that under anaesthesia with propofol.40 Our results indicated that the respiratory inhibition effect of remimazolam and cipepofol was slightly greater than propofol during FOB.41
Our study has some limitations. First, the external validity was weakened by single-center and single-blind designs. Our findings might not apply to individuals undergoing other treatments, because the study only included participants undergoing FOB. Additional research is required to validate our results for different demographic groups. Second, we did not evaluate stress-related indicators such as inflammatory factors and blood glucose levels. Both cipepofol and remimazolam reduced oxidative stress levels. However, this study did not examine the strength of stress resistance in the two groups. More studies are required to detect the link between cough reflexes and stress levels. Third, because only a single dose of remimazolam was used in our trial, the ideal dose of remimazolam to inhibit cough reflexes while maintaining spontaneous breathing requires further study. Fourth, because the BIS is commonly used to monitor the depth of propofol-based anaesthesia, there was a certain lag between the BIS and remimazolam concentrations, and the simulated predictions presented a certain error in the BIS.42 Whether BIS is suitable for remimazolam- or remifentanil/cipepofol-based anaesthesia requires further study. Fifth, although the cohort spanned a wide age range, the induction and titration of cipepofol were performed using a standardized, response-guided protocol. Dosing was initiated based on adjusted body weight and, more critically, was continuously titrated against BIS values and clinical responses. This protocol was designed to individualize sedation depth and mitigate the risk of overdose across all ages, including the very elderly. Age-stratified sensitivity check did not indicate a lower induction dose in the older group within this cohort under our titration protocol. Nevertheless, prospective studies focusing on the very elderly are needed to define optimal dosing strategies for this population.
Conclusions
The combination of remimazolam reduced the incidence of cough reflexes and dosage of cipepofol and remifentanil in elderly patients undergoing FOB under remifentanil/cipepofol-based anaesthesia. There were no differences in the characteristics of anaesthesia, surgery, or adverse effects between the groups.
Clinical Trial Registration
The study was registered in the Chinese Clinical Trial Registry (ChiCTR2300079139, Principal investigator: Xuehai Guan, Date of 18 registration: 2023-12-26).
Abbreviations
CIP, cipepofol; Remi, remimazolam; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; SpO2, peripheral capillary oxygen saturation; RR, respiratory rate; LOC, loss of consciousness; BIS, Bispectral Index.
Data Sharing Statement
The data generated in this study are available from the corresponding author (Xuehai Guan) upon request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Natural Science Foundation of Guangxi Zhuang Autonomous Region (2024GXNSFAA010222), the Clinical Research “Climbing” Program of the First Affiliated Hospital of Guangxi Medical University (YYZS2022005), the Guangxi Zhuang Autonomous Region Health Commission’s Self-Fund Research Project on Western Medicine (Z-A20230492), and the Guangxi Zhuang Autonomous Region Traditional Chinese Medicine Appropriate Technology Development and Promotion Project (GZSY22-59).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Leoste J, Stromberg-Jarvis K, Robal T, Marmor K, Kangur K, Rebane AM. Testing scenarios for using telepresence robots in healthcare settings. Comput Struct Biotechnol J. 2024;24:105–12. doi:10.1016/j.csbj.2024.01.004
2. Cho SJ, Stout-Delgado HW. Aging and lung disease. Annu Rev Physiol. 2020;82(1):433–459. doi:10.1146/annurev-physiol-021119-034610
3. Du Rand IA, Blaikley J, Booton R, et al. British thoracic society guideline for diagnostic flexible bronchoscopy in adults: accredited by NICE. Thorax. 2013;68 Suppl 1(Suppl 1):i1–i44. doi:10.1136/thoraxjnl-2013-203618
4. Wahidi MM, Jain P, Jantz M, et al. American college of chest physicians consensus statement on the use of topical anesthesia, analgesia, and sedation during flexible bronchoscopy in adult patients. Chest. 2011;140(5):1342–1350. doi:10.1378/chest.10-3361
5. Zhao MJ, Hu HF, Li XL, Li XM, Wang DC, Kuang MJ. The safety and efficacy between remimazolam and propofol in intravenous anesthesia of endoscopy operation: a systematic review and meta-analysis. Int J Surg. 2023;109(11):3566–3577. doi:10.1097/JS9.0000000000000638
6. Akhtar SMM, Fareed A, Ali M, et al. Efficacy and safety of ciprofol compared with propofol during general anesthesia induction: a systematic review and meta-analysis of randomized controlled trials (RCT). J Clin Anesth. 2024;94:111425. doi:10.1016/j.jclinane.2024.111425
7. Wang J, Wang R, Ma X, et al. Comparative efficacy of ciprofol and propofol in reducing respiratory depression during ERCP anesthesia: a randomized controlled trial. BMC Anesthesiol. 2024;24(1):404. doi:10.1186/s12871-024-02791-4
8. Lan HM, Liu SS, Liao YQ, et al. EC50 and EC95 of remifentanil for inhibiting bronchoscopy responses in elderly patients during fiberoptic bronchoscopy under ciprofol sedation: an up-and-down sequential allocation trial. Drug Des Devel Ther. 2024;18:6487–6497. doi:10.2147/DDDT.S490907
9. Liu Z, Jin Y, Wang L, Huang Z. The effect of ciprofol on postoperative delirium in elderly patients undergoing thoracoscopic surgery for lung cancer: a prospective, randomized, controlled trial. Drug Des Devel Ther. 2024;18:325–339. doi:10.2147/DDDT.S441950
10. Sun X, Zhang M, Zhang H, Fei X, Bai G, Li C. Efficacy and safety of ciprofol for long-term sedation in patients receiving mechanical ventilation in ICUs: a prospective, single-center, double-blind, randomized controlled protocol. Front Pharmacol. 2023;14:1235709. doi:10.3389/fphar.2023.1235709
11. Liu Y, Peng Z, Liu S, et al. Efficacy and safety of ciprofol sedation in ICU patients undergoing mechanical ventilation: a multicenter, single-blind, randomized, noninferiority trial. Crit Care Med. 2023;51(10):1318–1327. doi:10.1097/CCM.0000000000005920
12. Liu GL, Wu GZ, Ge D, et al. Efficacy and safety of ciprofol for agitation and delirium in the ICU: a multicenter, single-blind, 3-arm parallel randomized controlled trial study protocol. Front Med Lausanne. 2022;9:1024762. doi:10.3389/fmed.2022.1024762
13. Valk BI, Struys M. Etomidate and its analogs: a review of pharmacokinetics and pharmacodynamics. Clin Pharmacokinet. 2021;60(10):1253–1269. doi:10.1007/s40262-021-01038-6
14. Xu H, Wang L, Zhu W, Ren C, Liu G, Liu Y. Comparison of the safety and efficacy of remimazolam besylate versus dexmedetomidine for patients undergoing fiberoptic bronchoscopy: a prospective, randomized controlled trial. Drug Des Devel Ther. 2024;18:2317–2327. doi:10.2147/DDDT.S460949
15. Hu B, Zhang M, Wu Z, et al. Comparison of remimazolam tosilate and etomidate on hemodynamics in cardiac surgery: a randomised controlled trial. Drug Des Devel Ther. 2023;17:381–388. doi:10.2147/DDDT.S401969
16. Kim SH, Cho JY, Kim M, et al. Safety and efficacy of remimazolam compared with midazolam during bronchoscopy: a single-center, randomized controlled study. Sci Rep. 2023;13(1):20498. doi:10.1038/s41598-023-47271-w
17. Liang P, Dai M, Wang X, et al. Efficacy and safety of ciprofol vs. propofol for the induction and maintenance of general anaesthesia: a multicentre, single-blind, randomised, parallel-group, Phase 3 clinical trial. Eur J Anaesthesiol. 2023;40(6):399–406. doi:10.1097/EJA.0000000000001799
18. Kotani Y, Pruna A, Turi S, et al. Propofol and survival: an updated meta-analysis of randomized clinical trials. Crit Care. 2023;27(1):139. doi:10.1186/s13054-023-04431-8
19. Verret M, Le JBP, Lalu MM, et al. Effectiveness of dexmedetomidine on patient-centred outcomes in surgical patients: a systematic review and Bayesian meta-analysis. Br J Anaesth. 2024;133(3):615–627. doi:10.1016/j.bja.2024.06.007
20. Quibell R, Fallon M, Mihalyo M, Twycross R, Wilcock A. Ketamine. J Pain Symptom Manag. 2015;50(2):268–278. doi:10.1016/j.jpainsymman.2015.06.002
21. Frasca L, Sarubbi A, Longo F, et al. Remifentanil-propofol-ketamine- based total intravenous anesthesia with spontaneous breathing for adult rigid bronchoscopy. J Clin Med. 2025;14(2):377. doi:10.3390/jcm14020377
22. Qin L, Ren L, Wan S, et al. Design, synthesis, and evaluation of novel 2,6-disubstituted phenol derivatives as general anesthetics. J Med Chem. 2017;60(9):3606–3617. doi:10.1021/acs.jmedchem.7b00254
23. Li J, Wang X, Liu J, et al. Comparison of ciprofol (HSK3486) versus propofol for the induction of deep sedation during gastroscopy and colonoscopy procedures: a multi-centre, non-inferiority, randomized, controlled phase 3 clinical trial. Basic Clin Pharmacol Toxicol. 2022;131(2):138–148. doi:10.1111/bcpt.13761
24. Qin K, Qin WY, Ming SP, Ma XF, Du XK. Effect of ciprofol on induction and maintenance of general anesthesia in patients undergoing kidney transplantation. Eur Rev Med Pharmacol Sci. 2022;26(14):5063–5071. doi:10.26355/eurrev_202207_29292
25. Lu YF, Wu JM, Lan HY, Xu QM, Shi SQ, Duan GC. Efficacy and safety of general anesthesia induction with ciprofol in hip fracture surgery of elderly patients: a randomized controlled trial. Drug Des Devel Ther. 2024;18:3951–3958. doi:10.2147/DDDT.S475176
26. Lan H, Shan W, Wu Y, et al. Efficacy and safety of ciprofol for sedation/anesthesia in patients undergoing hysteroscopy: a randomized, parallel-group, controlled trial. Drug Des Devel Ther. 2023;17:1707–1717. doi:10.2147/DDDT.S414243
27. Hirose T, Okuda K, Ishida H, et al. Patient satisfaction with sedation for flexible bronchoscopy. Respirology. 2008;13(5):722–727. doi:10.1111/j.1440-1843.2008.01311.x
28. Reisin L, Blaer Y, Jafari J, Manoach M. Cough-induced nonsustained ventricular tachycardia. Chest. 1994;105(5):1583–1584. doi:10.1378/chest.105.5.1583
29. Irani F, Sanchis J. Inspiration- and cough-induced atrioventricular block. Can Med Assoc J. 1971;105(7):735–736.
30. Budzińska K, Romaniuk JR. The role of raphe and tractus solitarius neuronal structures in the modulation of respiratory pattern in rabbits. Acta Neurobiol Exp. 1995;55(3):155–164. doi:10.55782/ane-1995-1072
31. Martvon L, Kotmanova Z, Dobrolubov B, et al. Modulation of cough reflex by gaba-ergic inhibition in medullary raphé of the cat. Physiol Res. 2020;69(Suppl 1):S151–s161. doi:10.33549/physiolres.934401
32. Lan H, Cao H, Liu S, et al. Efficacy of remimazolam tosilate versus propofol for total intravenous anaesthesia in urological surgery: a randomised clinical trial. Eur J Anaesthesiol. 2024;41(3):208–216. doi:10.1097/EJA.0000000000001938
33. Fechner J, El-Boghdadly K, Spahn DR, et al. Anaesthetic efficacy and postinduction hypotension with remimazolam compared with propofol: a multicentre randomised controlled trial. Anaesthesia. 2024;79(4):410–422. doi:10.1111/anae.16205
34. Duan M, Yu N, Liu J, et al. Remimazolam suppresses oxidative stress and apoptosis in cerebral ischemia/reperfusion injury by regulating AKT/GSK-3β/NRF2 pathway. Drug Des Devel Ther. 2025;19:111–128. doi:10.2147/DDDT.S478692
35. Ding J, Wang BY, Yang YF, et al. Ciprofol ameliorates myocardial ischemia/reperfusion injury by inhibiting ferroptosis through upregulating HIF-1α. Drug Des Devel Ther. 2024;18:6115–6132. doi:10.2147/DDDT.S480514
36. Wible JH, DiMicco JA, Luft FC. Hypothalamic GABA and sympathetic regulation in spontaneously hypertensive rats. Hypertension. 1989;14(6):623–628. doi:10.1161/01.HYP.14.6.623
37. Klockgether-Radke AP, Pawlowski P, Neumann P, Hellige G. Mechanisms involved in the relaxing effect of midazolam on coronary arteries. Eur J Anaesthesiol. 2005;22(2):135–139. doi:10.1017/S0265021505000256
38. Lee J, Kim SH. Remimazolam-induced anaphylaxis and cardiovascular collapse: a narrative systematic review of eleven cases. Medicina. 2024;60(6):971.
39. Nakai T, Kako E, Ota H, So M, Sobue K. Remimazolam anaphylaxis in a patient not allergic to brotizolam: a case report and literature review. BMC Anesthesiol. 2024;24(1):204. doi:10.1186/s12871-024-02591-w
40. Lo YL, Lin TY, Fang YF, et al. Feasibility of bispectral index-guided propofol infusion for flexible bronchoscopy sedation: a randomized controlled trial. PLoS One. 2011;6(11):e27769. doi:10.1371/journal.pone.0027769
41. Wang C, Gao Y, Li J, et al. Safety and effectiveness of the combination of remimazolam tosilate and propofol in gastroscopy: a multicenter, randomized controlled, single-blind clinical trial. Front Pharmacol. 2023;14:1124667. doi:10.3389/fphar.2023.1124667
42. Zhou Y, Hu P, Huang Y, et al. Population pharmacokinetic/pharmacodynamic model-guided dosing optimization of a novel sedative HR7056 in Chinese healthy subjects. Front Pharmacol. 2018;9:1316. doi:10.3389/fphar.2018.01316
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.