Back to Journals » Psychology Research and Behavior Management » Volume 15
Reliability and Validity of the Arabic Version of Attitudes Towards Intellectual Disability Questionnaire-Short Form (A-ATTID-S)
Authors Jelleli H ![]() , Guelmami N, Ben Mohamed K, Hindawi O
, Guelmami N, Ben Mohamed K, Hindawi O ![]() , Bouassida A
, Bouassida A
Received 8 February 2022
Accepted for publication 5 May 2022
Published 20 May 2022 Volume 2022:15 Pages 1283—1293
DOI https://doi.org/10.2147/PRBM.S358181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Hilmi Jelleli,1 Noomen Guelmami,1,2 Khouloud Ben Mohamed,3,4 Omar Hindawi,5 Anissa Bouassida1
1Higher Institute of Sport and Physical Education of Kef, University of Jendouba, Jendouba, Tunisia; 2Postgraduate School of Public Health, Department of Health Sciences (DISSAL), University of Genoa, Genoa, Italy; 3National Institute of Health and Medical Research, Marseille, France; 4Carthage University, Tunis, Tunisia; 5College of Physical Education and Sport Science, Hashemite University, Zarqa, Jordan
Correspondence: Hilmi Jelleli, Higher Institute of Sport and Physical Education of Kef, University of Jendouba, Jendouba, Tunisia, Tel +201695937471, Email [email protected]
Purpose: Positive attitudes toward intellectual disability contribute to the effective inclusion of people with intellectual disability (PWID) in society, thereby enhancing their quality of life. The literature on tools for measuring attitudes towards PWID in Arabic is limited. The aim of this study was to adapt and validate the Attitudes towards Intellectual Disability Questionnaire-Short Form (ATTID-S) using an Arab population to assess its factor structure and reliability.
Materials and Methods: A total of 812 Arabic native speakers who lived in Tunisia were recruited. The exploratory sample consisted of 223 subjects divided into male (n = 121, 54.26%) and female (n = 102, 45.74%) with an age range of between 18 and 64 (mean = 32.7 ± 9.2 years). The confirmatory sample comprised 589 participants, male (n = 357, 60.61%) and female (n = 232, 39.38%), with a mean age of 31.61 (SD = 12.43). A cross-cultural translation of ATTID-S was carried. The Arab attitudes towards intellectual disability scale (A-ATTID-S) was tested using exploratory factor analysis, followed by confirmatory factor analysis.
Results: Exploratory factor analysis revealed a five-factor solution explaining up to 68.74 of the total variation, with items having lambda factor loadings ranging from 0.53 to 0.9. Subsequently, confirmatory factor analysis, which used a wide range of goodness-of-fit indices that met the recommended standards, confirmed the measure’s robustness. The internal consistency reliability of each of the subscales was investigated using reliability analysis. Cronbach’s alpha scores for the subscales and total score were satisfactory. Moreover, differences in the A-ATTID-S scores between male and female with age as covariate were demonstrated.
Conclusion: The A-ATTID-S is a good psychometric scale that can be used to assess the attitude of a general population towards intellectual disability in the Arabic-speaking world.
Keywords: intellectual disability, affective, knowledge, interaction, social integration
Corrigendum for this paper has been published.
Introduction
There are several neurodevelopmental diseases that are linked with cognitive impairment because of abnormalities in dendrites and dendritic spines. This is known as intellectual disability. Recently, intellectual disability has been defined as a condition characterized by significant limitations in both intellectual functioning and adaptive behavior that originates before the age of 22.2 According to DSM-5 impairment of general mental capacity affects adaptive functioning in three domains: intellectual, social, and practical.3
In an environmental approach, intellectual disability would be correlated with the degree of support needed by a person to ensure their social adaptation.4–6 Social adaptation is the complicated challenge faced by some PWID,7 so an inclusive environment would be essential. Most societies boast of being inclusive and they encourage citizens to collaborate in the social integration of PWID.8–10 However, despite actions that support the social inclusion of PWID at the individual, organizational, and governmental levels,11 these people commonly suffer from marginalization,12 harassment,13 and social exclusion.14 Because PWID may face such challenges they are often denied their rights to education, employment, and family life.15
Attitudes towards PWID are recognized as the major obstacle to their social integration in Arab world.16–18 In this regard, authors highlighted existing inequalities in Arab countries between PWID and other people. It is therefore essential to learn more about these attitudes to promote the desired social change.19 An attitude is a partially permanent set of feelings20,21 that refers to what the person feels in relation to an attitudinal subject.20,22 It focuses on beliefs,20,22–25 expectations, and opinions held by a person in relation to an attitudinal subject1,23,26 and behavioral predispositions27–29 that reside with the intention of behaving in a certain way when faced with an attitudinal object.30 Attitude studies have several perspectives, ranging from the genesis and process of attitude change to the effects of attitudes on individual behavior and interactions with others.31 In all perspectives, the assessment of attitude remains essential. Several instruments to assess attitudes towards people with disabilities have been developed. However, those regarding attitudes towards PWID are minimal.32
The most commonly used among the assessment scales of attitudes towards the PWID are the Mental Retardation Attitude Inventory,33,34 which is a scale of 29 items divided into four factors (integration-segregation, social distance, private rights and subtle derogatory beliefs), the Community Living Attitude Scale,35 which is a scale of 40 items divided into four factors (empowerment, similarity, exclusion and shelter), and the Attitude Towards Intellectual Disability questionnaire,26 which is a scale of 64 items divided into five factors (discomfort, sensibility or tenderness, knowledge of causes, knowledge of capacity and rights, and interaction). Among these three tools, only the attitude towards intellectual disability (ATTID) questionnaire respects the tripartite attitude formation. Moreover, the ATTID questionnaire is the only questionnaire based on a multidimensional model of attitudes (cognitive, affective and behavioral), which is recognized as a standard of good practice.1 Due to time constraints (22 minutes to administer) and resources, a short version of ATTID was designed and validated.1 Although there are many studies on attitudes towards PWID,17,34,36,37 Arabic psychometric tools remain insufficient.
Including a student with a PWID in school or social group activities is less common than including a student with a physical handicap, according to previous research.38 However, it is critical to assess professional’s attitudes toward people with intellectual disabilities in the educational setting. Previous studies have shown that the attitudes of teachers have an effect on students’ interactions.39
However, to our knowledge, there is only one validated scale in Arabic for assessing attitudes toward intellectually disabled people (the Arabic version of the Behavioral Intention to Interact with Peers with Intellectual Disability Scale).40 However, the two-factor scale, which measures behavioral intentions in and out of school, was designed to assess only student attitudes.
The objective of this study was to adapt and validate an Arabic version of ATTID-S and to examine the impact of demographic characteristics on the attitudes toward PWID in Tunisia.
Materials and Methods
Ethical Declaration
This research has been approved by the local ethics committee of the Higher Institute of Physical Education and Sports of Kef, code 041/2021. Prior to the start of our research, participants provided written informed consent. In accordance with ethical principles, confidentiality and anonymity were ensured by assigning an identification code to each questionnaire. The data was stored in a secure database to which only the research group had access. This study was realized according to the principles enshrined in the Declaration of Helsinki (3rd edition 2013) and in accordance with the Medical Research Involving Human Subjects Act (WMO).
Participants
Randomly selected a total of 812 participants were voluntarily education professionals participated in the present study. All the subjects are teachers and civil servants, have a higher level of education (at least bachelor degree) and exercise their professions in several university establishments in Tunisia.
Subjects, who are Arabic native speakers, worked in schools and universities, and lived in Tunisia and were assigned to two samples. The exploratory sample consisted of 223 subjects divided into male (n = 121, 54.26%) and female (n = 102, 45.74%) with an age range of between 18 and 64 (mean = 32.7 ±9.2 years).
The confirmatory sample comprised 589 participants, male (n = 357, 60.61%) and female (n = 232, 39.38%), with a mean age of 31.61 (SD = 12.43). All of the respondents volunteered to participate in the study.
Instrument
The ATTID-S1 is a 36-item questionnaire that measures the attitudes of the general population towards people with intellectual disabilities. Participants are asked to answer the questions using a 5-point Likert scale, ranging from “strongly agree” (1) to “strongly disagree” (5). The items measure the cognitive (15 items), affective (14 items) and behavioral (7 items) dimensions. The assessment of the affective and behavioral dimensions is preceded by two vignettes, one featuring a person with PWID with a higher level of functioning (Dominique) and the other, a PWID with a lower functional level (Raphaël). The first names of the two PWID in the thumbnail have been modified to suit the Arab context (eg, Anis instead of Dominique and Kaïs instead of Raphaël). ATTID-S has demonstrated robust validity and reliability.1 The conceptual validity of ATTID-S was examined by a principal component analysis which revealed five factors: discomfort and sensitivity or tenderness; these two factors make up the affective dimension; knowledge of ability and rights; and knowledge causes (both in the cognitive dimension) and interaction (behavioral dimension). The five-factor solution accounted for 47.6% of the explained variance. The Cronbach’s alpha coefficient ranges from 0.67 to 0.89, which is considered acceptable for good internal consistency.41
Adaptation
A cross-cultural translation of ATTID-S was carried out in cooperation with two Tunisian psychologists who used English fluently in their scientific activities and who were blind to the studies purpose. The first translated the English version into Arabic, and the second translated this Arabic version back into English. The re-translated version was compared to the original version of ATTID-S by a committee of English-speaking Tunisian clinical psychologists (authors are not included in this committee). Following the discussion, and to keep the functional conformity of the Arabic version, changes and corrections concerning some words and expressions were proposed by the committee of appointed psychologists. These corrections and changes have been made (eg ambiguities on the term Electronic store in the Arabic context have been raised), and the final version of the A-ATTID-S has been approved.
Procedure
Respondents were not given any further instructions on how to answer the questions other than those already included in the questionnaire. The A-ATTID-S was distributed in five schools and three universities over a period of one week. The average response time to the questionnaire was 12 minutes.
Statistical Tools
As a preliminary analysis, visual inspection was used to check for missing values and analyze the data. The Kurtosis and Skewness were used to examine the normality of the data distribution. Unweighted least squares with a direct Oblimin rotation were used for the exploratory analysis. The Kaiser–Meyer–Olkin (KMO) statistic was used to assess whether the data was suitable for factor analysis. The KMO value must be greater than 0.50 in order to accept the factorial solution.42 The chi-square value of the Bartlett sphericity test was also calculated,43 which should not be significant. The factors were retained when the eigenvalues were greater than 1, and the scree plot was examined. In addition, if an item’s factor loading was less than 0.5, it was deleted.42,44 Confirmatory factor analyses were used to evaluate the instrument’s factor structure. The instrument’s reliability was assessed using the Cronbach’s coefficient. Differences between genders with age as Covariate were realized by analysis of Covariance ANCOVA.
Descriptive statistical analyses, exploratory factor structure and internal consistency indices were performed with SPSS for Windows, version 26 (IBM Corp), whereas confirmatory factor analysis was established with Amos software for Windows, version 23 (IBM Corp).
Results
Descriptive Statistics and Exploratory Factor Analysis
The normality of the distributions was supported by the skewness and kurtosis coefficients shown in Table 1 with the descriptive statistics, and the lambda factor loadings.
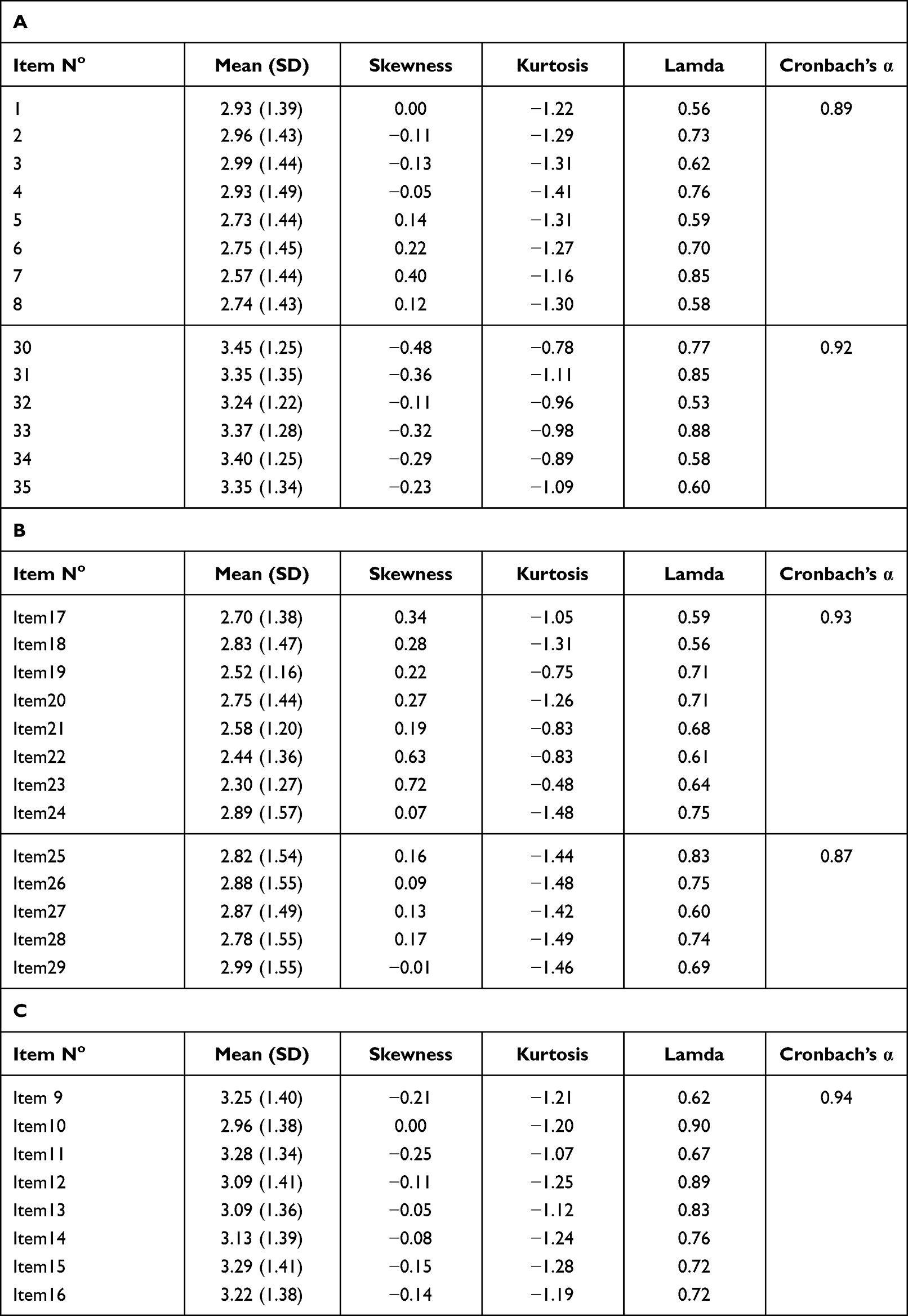 |
Table 1 Exploratory Factor Analysis of the a-ATTID-S (N=223) |
Based on the results of KMO and Bartlett test of sphericity, The A-ATTID-S was found to be appropriate for factorial solution (KMO=0.946; Chi2 = 6288.25; df = 595; P<0.001). Exploratory factor analysis revealed a five-factor solution that explained up to 68.74% of the total variance, with items having lambda factor loadings ranging from 0.53 to 0.90. The five factors explained 43.44%, 9.75%, 5.65%, 5.34%, and 4.55% of the total variance, respectively. Furthermore, the scree plot supports the five-factor solution; a clear change in the slope can be seen in Figure 1. The emerging factors were Discomfort (Items: 09, 10, 11, 12, 13, 14, 15, 16), Knowledge of capacity and rights (items: 01, 02, 03, 04, 05, 06, 07, 08), Interaction (30, 31, 32, 33, 34, 35), Sensitivity or tenderness (Items: 17, 18, 19, 20, 21) and Knowledge of causes (Items: 22, 23, 24, 25, 26, 27, 28, 29).
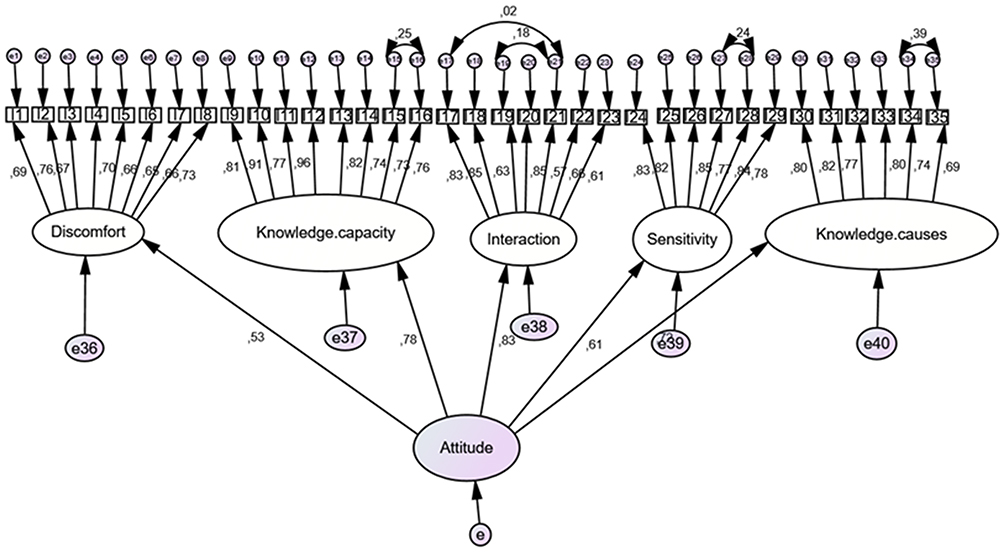 |
Figure 1 Scree plot for the principal component analysis of A-ATTID-S. |
Reliability
The internal consistency reliability of each of the subscales was investigated using reliability analysis. Cronbach’s alpha scores for discomfort (0.94), the knowledge of capacity and rights (0.89), interaction (0.92), sensitivity or tenderness (0.93) and knowledge of causes (0.87) subscales were satisfactory (see Table 1).
Confirmatory Factor Analysis
Figure 2 gives an overview of the confirmatory factor analysis model for the A-ATTID-S; we notice that all items contributed effectively to the pre-established theoretical constructs, as suggested by43,44 and that factorial weight greater than 0.71 can be considered excellent. The results of the confirmatory factor analysis supported the A-ATTID-S five-component structure.
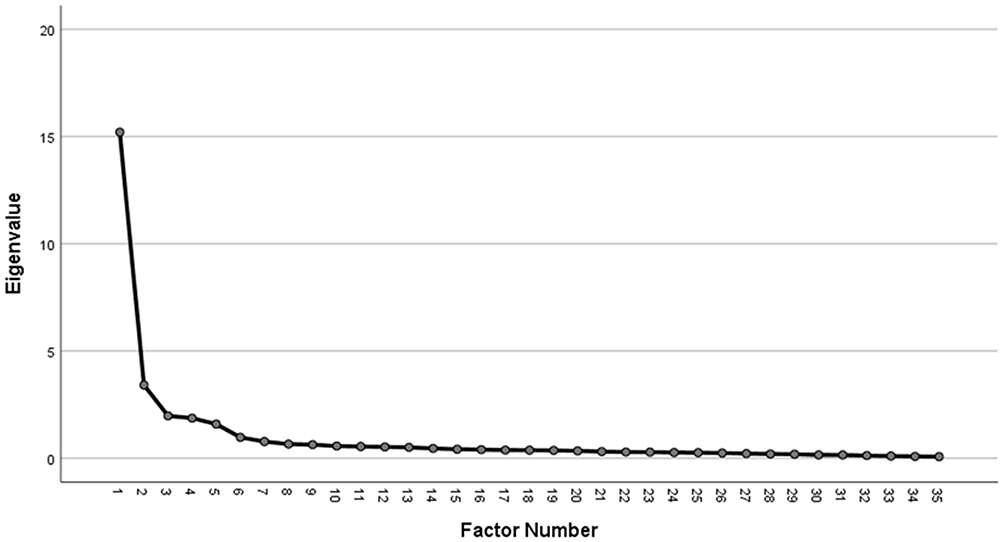 |
Figure 2 The final confirmatory factor analysis (CFA) of the A-ATTID-S. |
After adjustment of some errors in the established first order model (errors: e15-e16 for knowledge capacity, e16-e21, e17-e21 for the interaction factor, e27-e28 for the sensitivity and e34-35 for the knowledge causes), fit indexes were acceptable. As a matter of fact, the chi-square value (Chi2) was 5408.803 (p<0.01), DDL = 1431, the considerable ratio X2/DDL was 2.27 lower than the cut-off value 3.00 is acceptable. In addition, the incremental indices GFI, and AGFI proved values higher near the norm with a value of 0.88 and 0.90, respectively.45 Moreover, passementerie, the comparative fit index (CFI) and the Tucker Lewis index TLI values, which are 0.95 for both adjustment indices demonstrated an adequate cut-off values with 0.95 for each index. Finally, the root mean square error of approximation (RMSEA) displays an acceptable value of 0.046 < 0.1 and shows that the measurement errors are tolerable,46 the model gives an adequate adjustments index and conformed to theoretical thresholds.
Differences in Age and Gender
For testing differences among participants by gender and age, we conducted a multivariate analysis of covariance of the scale factors. Subsequently, we realized group differences with a covariance univariate analysis Ancona. The first step in this analysis gives descriptive statistics by gender with age as covariate. Descriptive statistics are illustrated in Table 2, whereas comparison results are shown in Table 3.
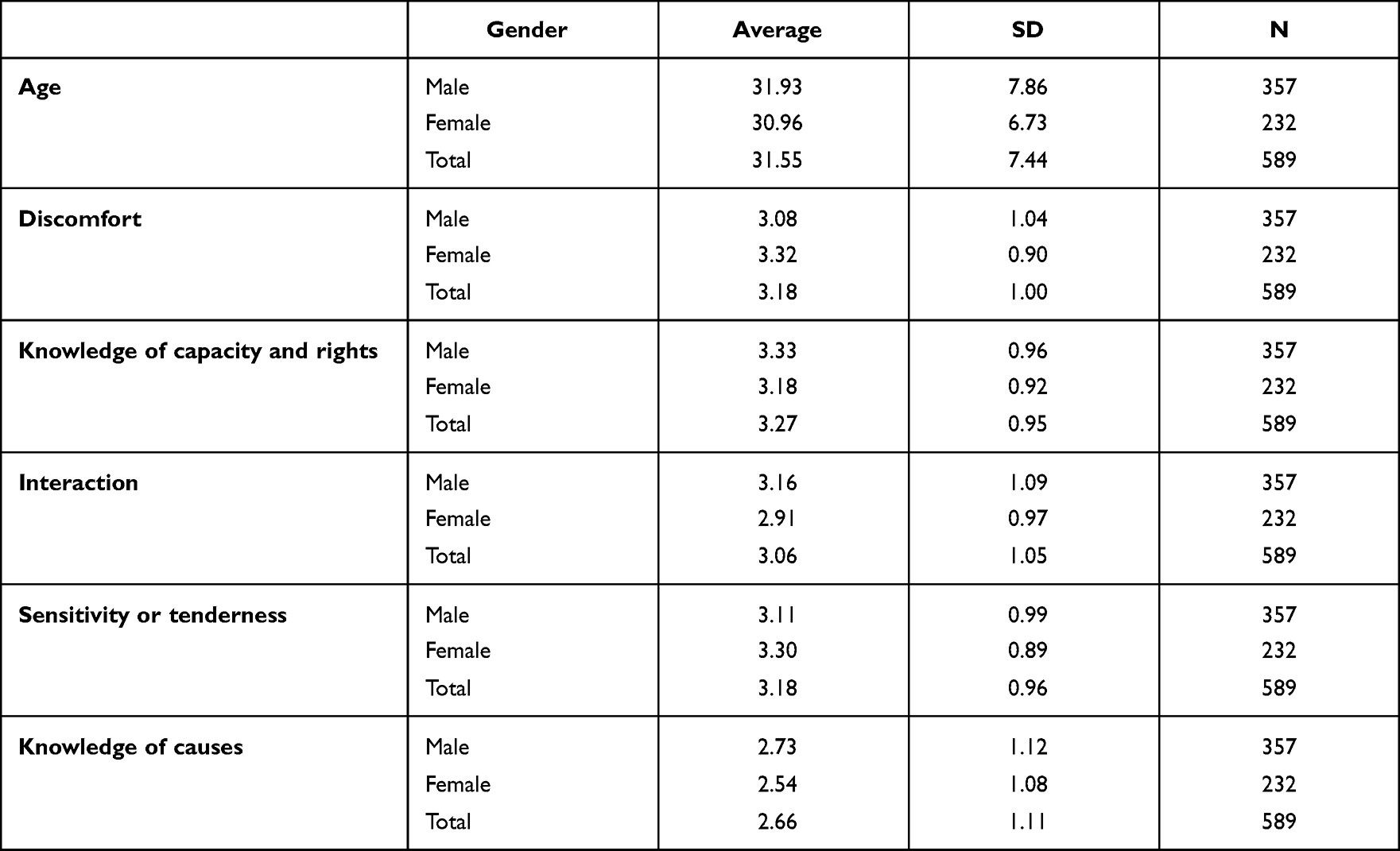 |
Table 2 Descriptive Statistics of a-ATTID-S Factors by Age and Gender |
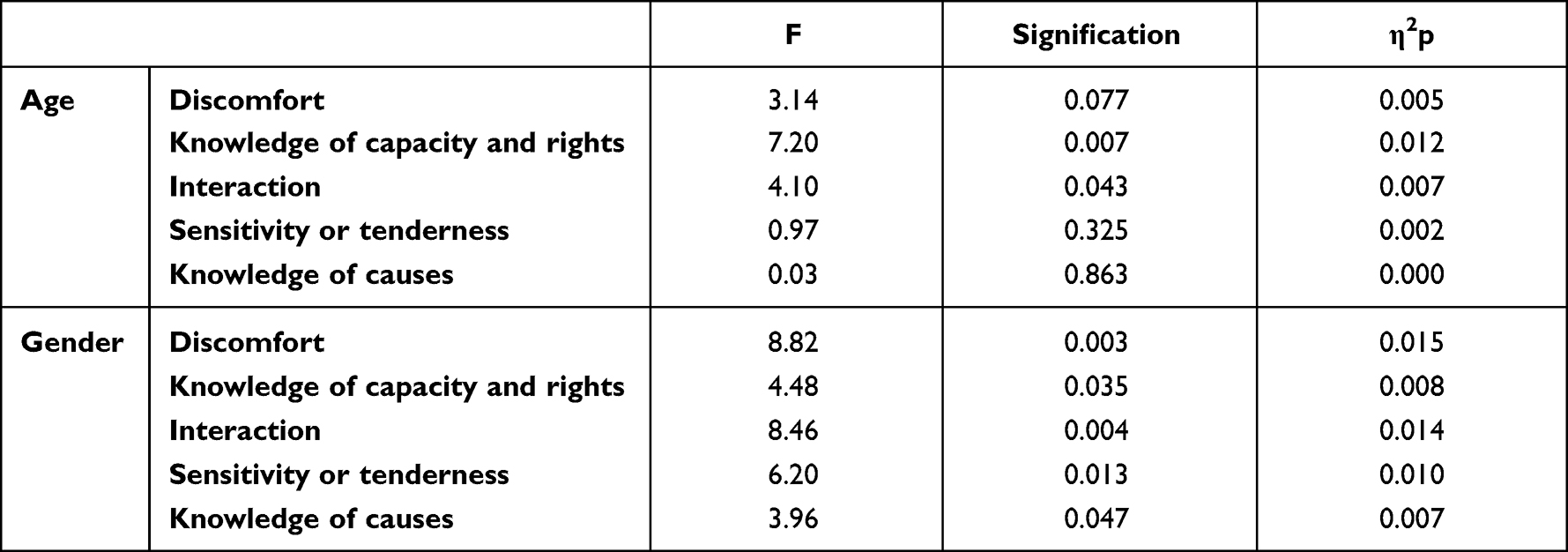 |
Table 3 Differences in Age and Gender |
Results of multivariate test showed a Wilks’ Lambda =0.98, multivariate F (5582) =2.22, p=0.51 and η2p = 0.02 for interaction age × gender. Since the multivariate test was non-significant, a univariate analysis of covariance was performed to examine differences between sex and age on the five subscales.
The findings also revealed a partial significant age effect for the “Knowledge of capacity and rights” (F (5;586) = 7.20, p = 0.007) and “Interaction” (F (5;586) = 4.1, p = 0.043) subscales (see Table 3). However, differences in gender showed significant differences for all subscales. In fact, differences are significant at p<0.01 F (5;586) =8.82 (η2p =0.015) and F (5;586) =8.46 (η2p = 0.014) for Discomfort and Interaction, respectively. Likewise, differences for Knowledge of capacity and rights (F (5;586) =4.48; η2p = 0.08), rights Sensitivity/tenderness (F (5;586) =6.20; η2p = 0.010) and Knowledge of causes (F (5;586) =3.96; η2p = 0.07) showed a significant value at p<0.05.
Discussion
The aim of this study was to adapt and validate the ATTID-S questionnaire1 using an Arab population in order to assess its factor structure and reliability.
The factor structure of A-ATTID-S appeared to be identical to that of ATTID-S. It respects the tripartite structure of attitude (affect, cognition, and behavior). Indeed, Cronbach’s alphas for the internal consistency of the five subscales were satisfactory. The exploratory factor analysis generated a five-factor structure, namely: (1) discomfort and (2) tenderness or tenderness (which constitute the affective dimension), (3) knowledge of capacity and rights, and (4) knowledge of the causes (which constitute the cognitive dimension) and (5) the interaction (behavioral dimension). The five factors of the A-ATTID-S preserved 36 items of the original questionnaire.1 Confirmatory factor analysis revealed consistency between the observed model and the theoretical model.
The ATTID-S questionnaire has been cited in recent studies.47–50 To our knowledge, until the writing of this article, there has been no study on the adaptation or validation of this version of ATTID-S. However, several recently published studies have used the original version of ATTID.1,21,26,51–54 Other authors have also selected long-form ATTID items to measure attitudes.32,55 The original ATTID questionnaire was adapted for a sample of Italian teachers.56 The Italian version respects the tripartite attitude and consists of five factors divided into 70 items. Fit indices were acceptable for RMSEA and SRMR but poor for the CFI and TLI. Construct validity was also investigated by calculating the cross-correlation coefficients for the five dimensions of ATTID, which produced results very similar to those reported by the original version.
In addition, other scales that measure attitudes towards intellectual disability have been developed and validated. The Mental Retardation Attitude Inventory (MRAI)33 is a four-factor scale (integration-segregation, social distance, private rights, and subtle derogatory beliefs) divided into 29 items. Although this scale has acceptable reliability,57,58 the validity of its factor structure has been questioned in other cultural contexts.59–61 The second scale which is The Community Living Attitude Scale (CLAS) contains 40 items that make up the four subscales, namely: empowerment, similarity, exclusion, and accommodation.35 Studies with different samples from different countries have reported stable reliability.33,58,60,62–66 However, these two scales present factors identical to those of ATTID even though they have different names, such as “the private rights of people with mental retardation” in MRAI, named “similitude” in CLAS, and the subscale “knowledge of capacities and rights” in ATTID. Nevertheless, the crucial “discomfort” factor when interacting with PWID in ATTID is not taken into consideration when developing MRAI and CLAS. Previous research has shown that repeated contact and a good quality of relationship with PWID were significantly correlated with less discomfort in the presence of PWID.56,63,66–69
The present study also aimed to assess the differences in attitudes based on socio-demographic characteristics such as age and gender. Agreeing with our results, in a non-Arabic context, previous research showed that gender is a serious influential factor of attitudes towards PWID.70 The authors suggest that women have more positive attitudes towards PWID than men. Gender differences exist among siblings as well. For instance, it was found that women felt that they had grown more in terms of increased empathy compared to men towards siblings with disabilities.71,72 Regarding age, our results about “Knowledge of capacity and rights” and “Interaction” partially corroborates the studies of26,66,73 to confirm the existence of effect of age on the attitudes towards PWID. However, no significant differences are shown for “Discomfort”, “Sensitivity or tenderness”, and “Knowledge of causes”. These results are in agreement with other studies that have not found an age effect on attitudes towards PWID.74,75
Limitations
This research has some limitations. Participants’ responses, based on self-report, may arguably increase the risk of socially desirable responses67,76 and thus fail to report their exact attitudes towards PWID. In addition, this study investigated the impact of gender and age on attitudes towards PWID people. Other characteristics, such as education level and personality type, may have an impact on attitudes regarding PWID, and we did not consider them in our study. Indeed, previous studies have shown personality traits as serious moderators of attitude.29,77–80 Additionally, earlier study has established that high level of education is a significant predictor of positive attitudes toward PWID26,76,81–85. Further research may include personality traits and level of education to assess the attitudes of an Arab population towards PWID.
Conclusion
The aim of this study was to adapt, validate, and assess the factor structure, internal reliability, validity, sensitivity, and convergent validity of the Arab attitude towards intellectual disability. Based on the good loadings of the EFA factor, CFA fit indices, correlation matrix, sensitivity analysis and excellent internal consistency, A-ATTID-S showed robust psychometric properties. The instrument can be used to quantitatively assess the attitude of professionals in an educational context towards intellectual disability in the Arabic-speaking world.
Given the aforementioned limitations, more research on the subject is urgently needed, including generalization of the tool to the whole population, investigations into the relationship between attitudes towards intellectual disability and other psychological and contextual.
Abbreviations
PWID, people with intellectual disability; ATTID-S, Attitudes towards Intellectual Disability Questionnaire-Short Form; ATTID, attitude towards intellectual disability questionnaire; CLAS, Community Living Attitude Scale; MRAI, Mental Retardation Attitude Inventory; RMSEA, root mean square error of approximation; CFI, the comparative fit index; TLI, and the Tucker Lewis index; CFA, confirmatory factor analysis.
Practical Contributions
We therefore recommend the assessment of attitudes in the selection process of personnel working in the education field specifically for people with intellectual disabilities in the Arab world.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Morin D, Valois P, Crocker AG, Robitaille C. Development and psychometric properties of the Attitudes Toward Intellectual Disability Questionnaire–Short Form. J Intellect Disabil Res. 2019;63(6):539–547. doi:10.1111/jir.12591
2. Schalock RL, Luckasson R, Tassé MJ. An Overview of Intellectual Disability: definition, Diagnosis, Classification, and Systems of Supports. Am J Intellect Dev Disabil. 2021;126(6):439–442. doi:10.1352/1944-7558-126.6.439
3. Quach TT, Stratton HJ, Khanna R, et al. Intellectual disability: dendritic anomalies and emerging genetic perspectives. Acta Neuropathol. 2021;141(2):139–158. doi:10.1007/s00401-020-02244-5
4. Buckles J, Luckasson R, Keefe E. A systematic review of the prevalence of psychiatric disorders in adults with intellectual disability, 2003–2010. J Ment Health Res Intellect Disabil. 2013;6(3):181–207. doi:10.1080/19315864.2011.651682
5. Nader-Grosbois N, Seynhaeve I. Étude des profils multidimensionnels d’enfants à déficience intellectuelle et à trouble autistique. Partie II Chapitre. 2008;1:1.
6. Tourrette C. Evaluer les enfants avec des déficiences ou troubles du développement [To assess children with disabilities or developmental disorders]. Paris Dunod. 2006;1:95.
7. Jones AP, Frederickson N. Multi-informant predictors of social inclusion for students with autism spectrum disorders attending mainstream school. J Autism Dev Disord. 2010;40(9):1094–1103. doi:10.1007/s10803-010-0957-3
8. Bredewold F, Haarsma A, Tonkens E, Jager M. Convivial encounters: conditions for the urban social inclusion of people with intellectual and psychiatric disabilities. Urban Stud. 2020;57(10):2047–2063. doi:10.1177/0042098019869838
9. Barlott T, Aplin T, Catchpole E, et al. Connectedness and ICT: opening the door to possibilities for people with intellectual disabilities. J Intellect Disabil. 2020;24(4):503–521. doi:10.1177/1744629519831566
10. Terras MM, Jarrett D, McGregor SA. The Importance of Accessible Information in Promoting the Inclusion of People with an Intellectual Disability. Disabilities. 2021;1(3):132–150. doi:10.3390/disabilities1030011
11. Van Rooy G, Amadhila EM, Mufune P, Swartz L, Mannan H, MacLachlan M. Perceived barriers to accessing health services among people with disabilities in rural northern Namibia. Disabil Soc. 2012;27(6):761–775. doi:10.1080/09687599.2012.686877
12. Chalachanová A, Lid IM, Gjermestad A. Citizenship of persons with intellectual disabilities within the frame of inclusive research: a scoping review of studies to inform future research. Alter. 2021;15(2):139–152. doi:10.1016/j.alter.2020.09.001
13. Walker J, Scior K. Tackling stigma associated with intellectual disability among the general public: a study of two indirect contact interventions. Res Dev Disabil. 2013;34(7):2200–2210. doi:10.1016/j.ridd.2013.03.024
14. Carnemolla P, Robinson S, Lay K. Towards inclusive cities and social sustainability: a scoping review of initiatives to support the inclusion of people with intellectual disability in civic and social activities. City Cult Soc. 2021;2:100398. doi:10.1016/j.ccs.2021.100398
15. Palad YY, Barquia RB, Domingo HC, Flores CK, Padilla LI, Ramel JMD. Scoping review of instruments measuring attitudes toward disability. Disabil Health J. 2016;9(3):354–374. doi:10.1016/j.dhjo.2016.01.008
16. Slater P, McConkey R, Smith A, Dubois L, Shellard A. Public attitudes to the rights and community inclusion of people with intellectual disabilities: a transnational study. Res Dev Disabil. 2020;105:103754. doi:10.1016/j.ridd.2020.103754
17. Alnahdi GH, Schwab S, Elahdi A, Alnahdi AH. The positive impact of joint activities on students attitudes toward peers with disabilities. Front Psychol. 2021;3466.
18. Alkhateeb JM, Hadidi MS, Alkhateeb AJ. Inclusion of children with developmental disabilities in Arab countries: a review of the research literature from 1990 to 2014. Res Dev Disabil. 2016;49:60–75. doi:10.1016/j.ridd.2015.11.005
19. Schwartz C, Armony-Sivan R. Students’ attitudes to the inclusion of people with disabilities in the community. Disabil Soc. 2001;16(3):403–413. doi:10.1080/09687590120045978
20. Albarracín D, Johnson BT, Zanna MP, Kumkale GT. Attitudes: introduction and scope. Handb Attitudes. 2005;2005:3–19.
21. Morin D, Rivard M, Boursier CP, Crocker AG, Caron J. Norms of the A ttitudes T oward I ntellectual D isability Q uestionnaire. J Intellect Disabil Res. 2015;59(5):462–467. doi:10.1111/jir.12146
22. Maio GR, Haddock G, Spears R, Manstead ASR. Attitudes and intergroup relations. The Sage handbook of prejudice, stereotyping, and discrimination; 2010.
23. Ajzen I, Cote NG. Attitudes and the prediction of behavior. Attitudes Attitude Change. 2008;1:13.
24. Ajzen I, Fishbein M. The influence of attitudes on behavior. Journal of Health Psychology. 2005;10(1):
25. Wyer JRS, Albarracín D. Belief Formation, Organization, and Change: cognitive and Motivational Influences. 2005.
26. Morin D, Rivard M, Crocker AG, Boursier CP, Caron J. Public attitudes towards intellectual disability: a multidimensional perspective. J Intellect Disabil Res. 2013;57(3):279–292. doi:10.1111/jir.12008
27. Findler L, Vilchinsky N, Werner S. The multidimensional attitudes scale toward persons with disabilities (MAS) construction and validation. Rehabil Couns Bull. 2007;50(3):166–176. doi:10.1177/00343552070500030401
28. Petty RE, Cacioppo JT. Attitudes and Persuasion: classic and Contemporary Approaches. Routledge; 2018.
29. Wolska A, Malina A. Personality and attitudes towards people with mental disorders: preliminary studies results. Int J Soc Psychiatry. 2020;66(3):270–278. doi:10.1177/0020764020906433
30. Stephen R, David D, Philippe GM. L’essentiel des concepts et des pratiques. Paris Pearson Educ Fr 6e Édition P. 2008;523:25–46.
31. Seccombe JA. Attitudes towards disability in an undergraduate nursing curriculum: the effects of a curriculum change. Nurse Educ Today. 2007;27(5):445–451. doi:10.1016/j.nedt.2006.08.003
32. Boo LSH, Nie Y. Attitude towards persons with intellectual disability scale: further development. Curr Psychol. 2018;37(4):760–768. doi:10.1007/s12144-017-9560-5
33. Antonak RF, Harth R. Psychometric Analysis and Revision of the Mental Retardation Attitude Inventory (“ Accepted by Louis Rowitz”). Ment Retard. 1994;32(4):272.
34. Wang Z, Xu X, Han Q, Chen Y, Jiang J, Ni GX. Factors associated with public attitudes towards persons with disabilities: a systematic review. BMC Public Health. 2021;21(1):1058. doi:10.1186/s12889-021-11139-3
35. Henry D, Keys C, Jopp D, Balcazar F. The community living attitudes scale, mental retardation form: development and psychometric properties. Ment Retard. 1996;34(3):149.
36. Desroches ML, Howie VA, Wilson NJ, Lewis P. Nurses’ attitudes and emotions toward caring for adults with intellectual disability: an international replication study. J Nurs Scholarsh. 2022;54(1):117–124. doi:10.1111/jnu.12713
37. Morin D, Valois P, Crocker AG, Robitaille C, Lopes T. Attitudes of health care professionals toward people with intellectual disability: a comparison with the general population. J Intellect Disabil Res. 2018;62(9):746–758. doi:10.1111/jir.12510
38. Gasser L, Chilver-Stainer J, Buholzer A, Perrig-Chiello P. Soziales und moralisches Denken von Kindern über den Ein-und Ausschluss behinderter Kinder. Z Für Pädagog Psychol. 2012;1:547.
39. Luttropp A, Granlund M. Interaction–it depends–a comparative study of interaction in preschools between children with intellectual disability and children with typical development. Scand J Disabil Res. 2010;12(3):151–164. doi:10.1080/15017410903175677
40. Alnahdi GH, Schwab S. Psychometric properties of the Arabic version of the behavioral intention to interact with peers with intellectual disability scale. Front Psychol. 2020;11:1212. doi:10.3389/fpsyg.2020.01212
41. Kline P. Handbook of Psychological Testing. Routledge; 2013.
42. Hair J, Anderson RE, Tatham RL, Black WC. Multivariate data with readings. US Am Prentice Hall Inc. 1995;1:87.
43. Westfall PH, Henning KS. Understanding Advanced Statistical Methods. Boca Raton, FL, USA: CRC Press; 2013.
44. Ware JJE, Gandek B. Methods for testing data quality, scaling assumptions, and reliability: the IQOLA Project approach. J Clin Epidemiol. 1998;51(11):945–952. doi:10.1016/S0895-4356(98)00085-7
45. Iacobucci D. Structural equations modeling: fit indices, sample size, and advanced topics. J Consum Psychol. 2010;20(1):90–98. doi:10.1016/j.jcps.2009.09.003
46. Roussel P. Méthodes de développement d’échelles pour questionnaires d’enquête. Manag Ressour Hum Méthodes Rech En Sci Hum Soc. 2005;2:245–276.
47. Albaum C, Mills A, Morin D, Weiss JA. Attitudes Toward People With Intellectual Disability Associated With Integrated Sport Participation. Adapt Phys Act Q. 2021;1(aop):1–23.
48. Cutrona SF. In-Service Teacher Education and Secondary School Teacher Attitudes Toward Inclusion. Grand Canyon University; 2021. PhD Thesis.
49. Form NK. Kısa Form Geliştirme: yöntemler, Öneriler ve İncelemeler. J Meas Eval Educ Psychol. 2020;11(3):302–310.
50. Pivarč J. Attitudes of Czech primary school pupils towards people with intellectual disabilities: the role of experience and participant demographics. Educ Stud. 2020;1:1–20. doi:10.1080/03055698.2020.1746637
51. Lee JS. The Effect of Interpersonal Contact on Attitudes Change Toward People with Intellectual or Developmental Disabilities. UCLA; 2016. PhD Thesis.
52. Murch AJ, Choudhury T, Wilson M, Collerton E, Patel M, Scior K. Explicit and implicit attitudes towards people with intellectual disabilities: the role of contact and participant demographics. J Appl Res Intellect Disabil. 2018;31(5):778–784. doi:10.1111/jar.12429
53. Phillips BA, Fortney S, Swafford L. College students’ social perceptions toward individuals with intellectual disability. J Disabil Policy Stud. 2019;30(1):3–10. doi:10.1177/1044207318788891
54. Sermier Dessemontet R, Morin D, Crocker AG. Exploring the relations between in-service training, prior contacts and teachers’ attitudes towards persons with intellectual disability. Int J Disabil Dev Educ. 2014;61(1):16–26. doi:10.1080/1034912X.2014.878535
55. Araten-Bergman T, Werner S. Social workers’ attributions towards individuals with dual diagnosis of intellectual disability and mental illness. J Intellect Disabil Res. 2017;61(2):155–167. doi:10.1111/jir.12300
56. Arcangeli L, Bacherini A, Gaggioli C, Sannipoli M, Balboni G. Attitudes of mainstream and special-education teachers toward intellectual disability in Italy: the relevance of being teachers. Int J Environ Res Public Health. 2020;17(19):7325. doi:10.3390/ijerph17197325
57. Bazzo G, Nota L, Soresi S, Ferrari L, Minnes P. Attitudes of social service providers towards the sexuality of individuals with intellectual disability. J Appl Res Intellect Disabil. 2007;20(2):110–115. doi:10.1111/j.1468-3148.2006.00308.x
58. Krajewski J, Flaherty T. Attitudes of high school students toward individuals with mental retardation. Ment Retard. 2000;38(2):154–162. doi:10.1352/0047-6765(2000)038<0154:AOHSST>2.0.CO;2
59. Al-Kandari HY, Salih FA. Adapting antonak and harth’s mental retardation attitude inventory for Kuwait’s culture. Dig Middle East Stud. 2008;17(1):1–31. doi:10.1111/j.1949-3606.2008.tb00144.x
60. Hampton NZ, Xiao F. Psychometric properties of the mental retardation attitude inventory-revised in Chinese college students. J Intellect Disabil Res. 2008;52(4):299–308. doi:10.1111/j.1365-2788.2007.01020.x
61. Sam KL, Li C, Lo SK. Validation of the mental retardation attitude inventory-revised (MRAI-R): a multidimensional rasch analysis. Int J Soc Sci Humanity. 2016;6(7):519–524. doi:10.7763/IJSSH.2016.V6.703
62. Al-Kandari HY. High school students’ contact with and attitudes towards persons with intellectual and developmental disabilities in Kuwait. Aust Soc Work. 2015;68(1):65–83. doi:10.1080/0312407X.2014.946429
63. Horner-Johnson W, Keys C, Henry D, et al. Attitudes of Japanese students toward people with intellectual disability. Journal of Intellectual Disability Research. 2002;46(5):365–378. doi:10.1046/j.1365-2788.2002.00406.x
64. McManus JL, Feyes KJ, Saucier DA. Contact and knowledge as predictors of attitudes toward individuals with intellectual disabilities. J Soc Pers Relatsh. 2011;28(5):579–590. doi:10.1177/0265407510385494
65. Rice CJ. Attitudes of undergraduate students toward people with intellectual disabilities: considerations for future policy makers. Coll Stud J. 2009;43(1):207–216.
66. Yazbeck M, McVilly K, Parmenter TR. Attitudes toward people with intellectual disabilities: an Australian perspective. J Disabil Policy Stud. 2004;15(2):97–111. doi:10.1177/10442073040150020401
67. Balogh R, Brownell M, Ouellette-Kuntz H, Colantonio A. Hospitalisation rates for ambulatory care sensitive conditions for persons with and without an intellectual disability-a population perspective. J Intellect Disabil Res. 2010;54(9):820–832. doi:10.1111/j.1365-2788.2010.01311.x
68. Kowalska J, Winnicka J. Attitudes of undergraduate students towards persons with disabilities; the role of the need for social approval. Pol Psychol Bull. 2013;44(1):40–49. doi:10.2478/ppb-2013-0005
69. Shakespeare T. Disability Rights and Wrongs Revisited. Routledge; 2013.
70. Marcone R, Caputo A, Esposito S, Senese VP. Prejudices towards people with intellectual disabilities: reliability and validity of the Italian Modern and Classical Prejudices Scale. Journal of Intellectual Disability Research. 2019;63(8):911–916. doi:10.1111/jir.12590
71. Prino LE, Scigala D, Fabris MA, Longobardi C. The moderating role of gender in siblings of adults with intellectual disabilities. Interpersona: An International Journal on Personal Relationships. 2019;13(1):1–13. doi:10.5964/ijpr.v13i1.323
72. Hodapp RM, Urbano RC, Burke MM. Adult female and male siblings of persons with disabilities: findings from a national survey. Intellect Dev Disabil. 2010;48(1):52–62. doi:10.1352/1934-9556-48.1.52
73. Scior K. Public awareness, attitudes and beliefs regarding intellectual disability: a systematic review. Res Dev Disabil. 2011;32(6):2164–2182. doi:10.1016/j.ridd.2011.07.005
74. Lau JT. Discriminatory attitudes to people with intellectual disability or mental health difficulty. Int Soc Work. 1999;42(4):431–444. doi:10.1177/002087289904200405
75. Pace JE, Shin M, Rasmussen SA. Understanding attitudes toward people with Down syndrome. Am J Med Genet A. 2010;152(9):2185–2192. doi:10.1002/ajmg.a.33595
76. Burge P, Ouellette-Kuntz H, Lysaght R. Public views on employment of people with intellectual disabilities. J Vocat Rehabil. 2007;26(1):29–37.
77. Bergman MM. A theoretical note on the differences between attitudes, opinions, and values. Swiss Polit Sci Rev. 1998;4(2):81–93. doi:10.1002/j.1662-6370.1998.tb00239.x
78. Di Maggio I, Ginevra MC, Santilli S, Nota L. Elementary school students’ attitudes towards peers with disabilities: the role of personal and contextual factors. J Intellect Dev Disabil. 2021;1–9.
79. Loehlin JC. Chapter Six. Resemblance in Personality and Attitudes Between Parents and their Children. In: Unequal Chances. Princeton University Press; 2009:192–207.
80. Lynn M. Effects of the Big Five personality traits on tipping attitudes, motives, and behaviors. Int J Hosp Manag. 2021;92:102722. doi:10.1016/j.ijhm.2020.102722
81. Akrami N, Ekehammar B, Claesson M, Sonnander K. Classical and modern prejudice: attitudes toward people with intellectual disabilities. Res Dev Disabil. 2006;27(6):605–617. doi:10.1016/j.ridd.2005.07.003
82. Antonak RF, Livneh H. Psychosocial adaptation to disability and its investigation among persons with multiple sclerosis. Soc Sci Med. 1995;40(8):1099–1108. doi:10.1016/0277-9536(94)00167-R
83. Esterle M, Sastre MTM, Mullet E. Judging the acceptability of sexual intercourse among people with learning disabilities: French laypeople’s viewpoint. Sex Disabil. 2008;26(4):219–227. doi:10.1007/s11195-008-9093-9
84. MacDonald JD, MacIntyre PD. A rose is a rose: effects of label change, education, and sex on attitudes toward mental disabilities. J Dev Disabil. 1999;6(2):15–31.
85. Ouimet J, De Man AF. Correlates of attitudes toward the application of eugenics to the treatment of people with intellectual disabilities. Soc Behav Personal Int J. 1998;26(1):69–74. doi:10.2224/sbp.1998.26.1.69
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.