")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 17
Relevance of Procalcitonin Levels as a Marker of Severity and Predictor of Mortality, Initiation and Duration of Antibiotics in Patients Admitted with Acute Pancreatitis: A Retrospective Cohort Study
Authors Mann BK , Bhandohal JS, Kalha I, Fox K, Jean B
Received 19 December 2023
Accepted for publication 7 February 2024
Published 9 February 2024 Volume 2024:17 Pages 31—39
DOI https://doi.org/10.2147/CEG.S453345
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Santosh Shenoy
Baldeep Kaur Mann,1 Janpreet Singh Bhandohal,1 Ishaan Kalha,2 Kasey Fox,1 Brian Jean3
1Division of Hospital Medicine, Department of Medicine, Kern Medical Center, Bakersfield, CA, USA; 2Division of Gastroenterology, Department of Medicine, Kern Medical Center, Bakersfield, CA, USA; 3Biostatistician, Professor Emeritus, Kern Medical Center, Bakersfield, CA, USA
Correspondence: Baldeep Kaur Mann, Division of Hospital Medicine, Department of Medicine, Kern Medical Center, 1700 Mount Vernon Ave, Bakersfield, CA, 93306, USA, Email [email protected]
Introduction: Procalcitonin levels have been studied to predict the benefit of adding antibiotics in a patient with acute pancreatitis. Through this study, we are searching for any possible correlation between serum procalcitonin levels and the severity of acute pancreatitis (included acute on chronic cases) to determine whether procalcitonin levels can predict a benefit from antibiotic therapy in acute pancreatitis.
Methods: This is a retrospective cohort study involving patients with acute pancreatitis and acute on chronic pancreatitis. We included all hospitalized patients admitted to Kern Medical from January 2020 to October 2022 with a diagnosis of acute pancreatitis in a consecutive manner. The primary outcome studied was mortality related to the pancreatitis episode. Logistic regression was used to control numerous confounders.
Results: Based on univariate analysis of procalcitonin, we found starting antibiotics on the day of admission statistically significant. We also found the median differences in mortality to be mildly significant (difference = 0.79, p = 0.0640) based on procalcitonin values. In a multivariate analysis of ln(procalcitonin), we found lipase (p = 0.0249), duration of antibiotics (p = 0.0009), multi-organ failure (p = 0.0045) to be statistically significant, and lactate being mildly significant in the multivariate model (p = 0.0643).
Conclusion: The procalcitonin level can predict the initiation of antibiotics, duration of antibiotics, multi-organ failure, and mortality in patients with acute pancreatitis.
Keywords: procalcitonin, pancreatitis, acute pancreatitis
Introduction
Background
The course of illness for acute pancreatitis can range from self-limiting to extremely protracted, ending in sepsis, multiple-organ dysfunction syndrome, and death.1 Laboratory studies, including lipase levels, assist in confirming the diagnosis of pancreatitis. A serum lipase level three times the normal’s upper limit is 100% indicative of acute pancreatitis.2 Because of large variations in the hospital course of acute pancreatitis, several scoring systems have been developed to aid physicians in the clinical assessment of acute pancreatitis. The Ranson criteria is one of the oldest and most well-known.3 Another score used for the severity of acute pancreatitis is The Acute Physiology and Chronic Health Evaluation (APACHE II), which includes complex calculations correlating with mortality and severity of the disease.4 The Bedside Index for Severity of Acute Pancreatitis (BISAP) score was developed specifically to be calculated at the bedside and to predict the severity of the disease.5 One meta-analysis found that the BISAP score was more sensitive and specific than the Ranson or APACHE-II.6 Finally, the computed tomography (CT) scoring index or Balthazar score uses contrast CT scans to measure the amount of pancreatic inflammation and necrosis.2 Several inflammatory markers have been implicated in the pathophysiology of acute pancreatitis. One study found that patients with acute pancreatitis who had elevated procalcitonin levels early in the course of the disease were more likely to develop necrotic infectious pancreatitis.7 Another study found that procalcitonin levels were significantly elevated in patients with pancreatic infections and were associated with multi-organ dysfunction.8
Objectives
Through this study, we are searching for any possible correlation between serum procalcitonin levels and the severity of acute pancreatitis (included acute on chronic cases) to determine whether procalcitonin levels can predict a benefit from antibiotic therapy in acute pancreatitis. We also evaluated for a correlation between procalcitonin levels and measured inflammatory markers, BISAP score, and Modified CT severity index.
Methods
Study Design
This is a retrospective cohort study involving patients with acute pancreatitis and acute on chronic pancreatitis.
Setting
Kern Medical is a safety net hospital serving the community of Kern County in Central California. The hospital is a referral center for multiple peripheral health care centers. Physicians at Kern Medical are involved in the management of acute pancreatitis on a daily basis. A significant proportion of patients presenting to Kern Medical with acute pancreatitis are clinically ill and often have evidence of pancreatic necrosis. Our study included all of the inpatients who were admitted from January 2020 to October 2022 with the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes indicative of acute pancreatitis in a consecutive manner. The Kern Medical Center Institutional Review Board approved the study (Approval # 22138). Patient informed consent was waived because anticipated number of patients was 200 and the study needed records from the past (since January 2020), but patient data including HIPAA-specified individual identifiers were kept confidential in compliance with the Declaration of Helsinki. The manuscript was written based on the STROBE (Strengthening the Reporting of observational studies in Epidemiology) checklist.
Participants
Data was collected from Electronic Medical Records with the following eligibility criteria:
Inclusion Criteria
- Any patient greater than 16 years of age admitted to the hospital for acute pancreatitis or acute on chronic pancreatitis.
Exclusion Criteria
- Patients less than 16 years of age
- Incarcerated patients
- Procalcitonin not available within 48–72 hours of admission
- Chronically elevated lipase levels in patients with chronic pancreatitis or patients with elevated lipase levels who were hospitalized for other reasons, such as cholecystitis, bowel perforation, pancreatic cancer, trauma to the pancreas, intra-abdominal abscesses, septic shock, CKD, chronic alcoholism, peptic ulcer disease, s/p ERCP/choledocholithiasis, cirrhosis in the absence of symptoms of pancreatitis
Variables
The primary outcome of the study was mortality related to the pancreatitis episode. The other secondary outcomes were multi-organ failure, length of stay, and number of subsequent admissions. The exposures were considered if a patient was admitted to the Intensive Care Unit (ICU), initiating antibiotics on the day of admission, and the duration of antibiotics. The predictor variables were procalcitonin, amylase, lipase, biliary etiology, the neutrophil ratio on the day of admission, ESR, CRP, lactate, LDH, D-Dimer, triglyceride levels, alcohol use, acute on chronic cases, BISAP score, and modified CT severity index. The potential confounders were other active infections, age, and gender. According to the revised Atlanta Classification, diagnostic criteria for acute pancreatitis included a serum lipase value three times the upper limit of normal with clinical symptoms of epigastric pain with/without associated symptoms of nausea/vomiting.9
Participants were enrolled based on the algorithm in Figure 1. The characteristics of categorical and continuous variables are shown in Table 1 and Table 2, respectively. Our patients had >60% missing values for LDH, amylase, D-Dimer, ESR, and CRP. Therefore, these variables were excluded from the statistical analysis. None of the categorical variables had missing data. Only ten patients had antibiotics initiated on subsequent days, but we only studied patients with the initiation of antibiotics on the day of admission.
 |
Table 1 Proportions of Categorical Variables (There Were No Missing Elements) |
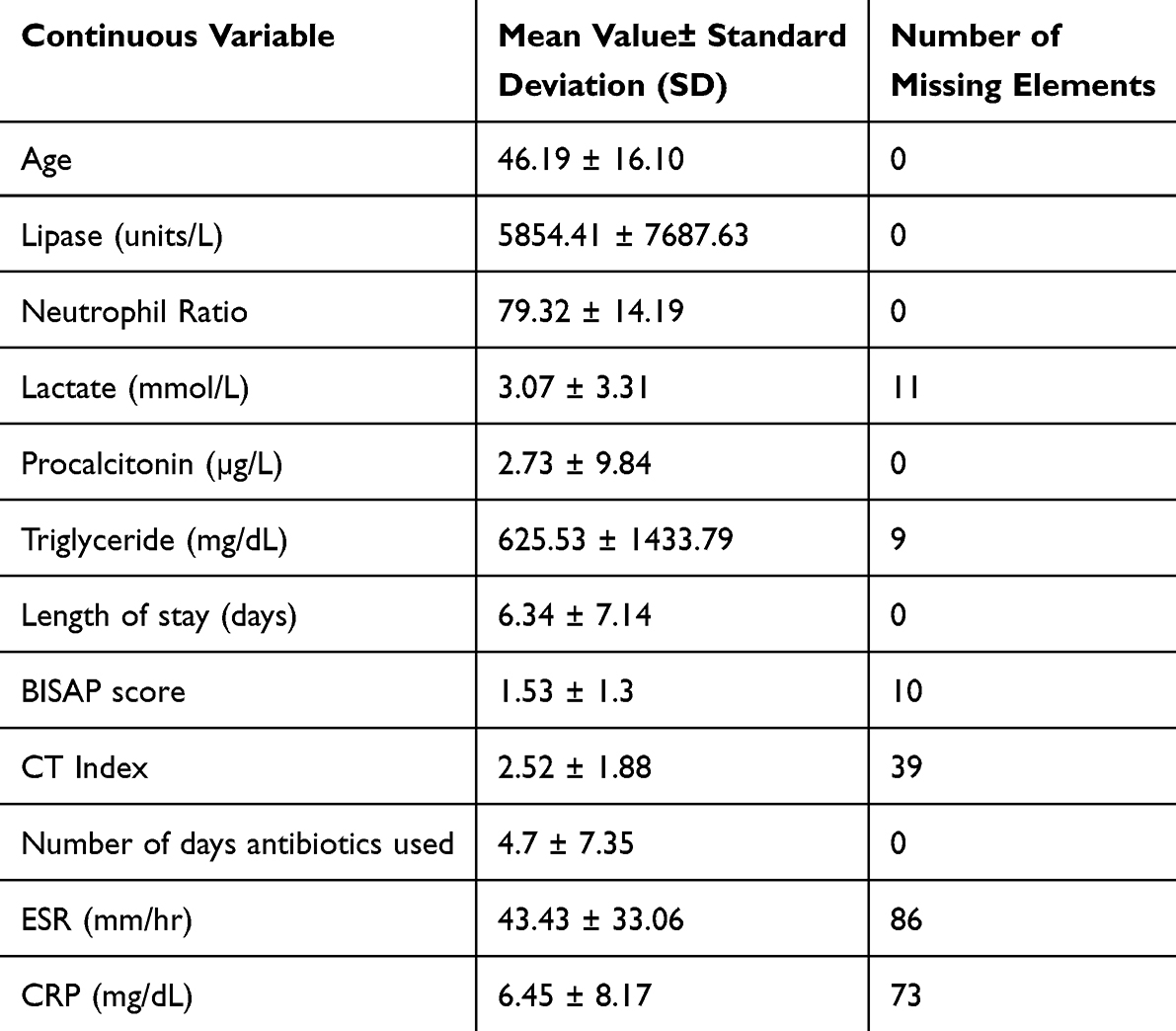 |
Table 2 Mean and Standard Deviation Value for the Continuous Variables Along with Missing Elements |
 |
Figure 1 The algorithm shows the strategy involved in the enrollment of the patients and the inclusion and exclusion criteria followed to obtain the patients of interest. |
Data Sources
BISAP score was calculated based on BUN, impaired mental status on admission, SIRS criteria ≥2, age >60 years, and presence of pleural effusion on chest X-ray. The modified CT severity Index was calculated based on CT findings wherever available (localized fluid collections, ascites, percentage of pancreatic necrosis, etc.).
Bias
The study can have selection bias as we enrolled only patients with a procalcitonin level available. No follow-up was needed; thus, our study did not have information bias due to the loss of follow-up. The confusion bias due to confounding was minimized using the multivariate technique, ie, logistic regression.
Study Size
The sample size was calculated based on Sample Size Calculator (clincalc.com), and it was found that 132 individuals were needed for an anticipated incidence of mortality of 8% for our study group with a known incidence of mortality of 16.310 in severe acute pancreatitis. [statistical power 80%, Type I error rate 0.05, Type II error rate 0.2.]
Quantitative Variables
Many of the continuous variables, including procalcitonin, lipase, neutrophil ratio, and triglyceride levels, were found to be heavily skewed. Therefore, these were categorized based on their values. The procalcitonin levels were categorized in four sets of 0.10–0.49 ng/mL: Minor or no significant inflammatory response; 0.50–1.99 ng/mL: Moderate risk for progression to severe systemic infection; Procalcitonin level 2.00–9.99 ng/mL: Severe systemic inflammatory response; Procalcitonin level > or = 10.00 ng/mL: high likelihood of severe sepsis or septic shock. Lipase values were categorized into low lipase elevation group (200–400 U/L), moderate elevation group (400–600 U/L), and high elevation group (≥600 U/L). Neutrophil ratio values were coded as <50% low, 50–75% normal, and more than 75% high. Triglycerides were grouped as normal <150 mg/dL, mild hypertriglyceridemia: 150–199 mg/dL, moderate hypertriglyceridemia: 200–499 mg/dL and severe hypertriglyceridemia: ≥500 mg/dL.
Statistical methods
The collected data was compiled in a Microsoft Excel sheet. The variables were identified as continuous or categorical. The continuous variables were studied using descriptive statistics and were expressed as mean ± standard deviation and quartiles. The p-value of ≤0.05 was considered significant for the study. Mild statistical significance was noted for p-values greater than 0.05 but less than 0.10. The missing data underwent deletion via dropping variables if the data was missing more than 60% of the observations and those variables were insignificant. Logistic regression was used to control numerous confounders by which the adjusted odds ratio was produced. The adjusted odds ratio was controlled and adjusted for multiple confounders or covariates.11,12
Results
The univariate analysis for procalcitonin is shown in Table 3. The natural log transformation of variable procalcitonin [ln(procalcitonin)] was taken to address severe violations of model assumptions needed for linear regression and ANOVA, not necessarily for all univariate analyses completed. Since even with the log transformation, the data were still skewed with clear violations of the normality assumptions, the analysis was turned to a permutation approach for ANOVA to address group means, and a post hoc multiple comparison Kruskal–Wallis test with Bonferroni p-value adjustments was performed for medians.
 |
Table 3 Univariate Analysis for Procalcitonin. P-values for Categorical Variables with More Than Two Levels Reflect P-values Based on Ln(Procalcitonin) for Both Permutation Based ANOVA (Means) and Kruskal-Wallis (Medians) |
Based on univariate analysis of Procalcitonin, we found the starting of antibiotics on the day of admission to be statically significant for the difference in means (difference = 4.06, p = 0.0051) and medians (difference = 0.66, p = 0.0000). We also found the median differences in mortality to be mildly significant (difference = 0.79, p = 0.0640). We also found the medians of procalcitonin to be statistically significant based on mortality (difference = 1.38, p = 0.0640).
A permutation ANOVA based on ln(procalcitonin), comparing levels of hypertriglyceridemia, neutrophil level, and lipase level, also showed statistical significance. Hypertriglyceridemia indicated a statistically significant difference between means (p = 0.0012). Two-way comparisons of the means indicate a statistically significant difference between the levels Moderate and Normal (p = 0.0065) triglyceride levels, indicating Moderate > Normal. No other two-way comparison was found to be statistically significant. A Kruskal-Wallis test indicated statistically significant differences between the medians of triglyceride levels, indicating that Normal is lower than Mild (p = 0.04) and Moderate (p = 0.0080) (Figure 2). Neutrophil levels indicate a statistically significant difference between the means of ln(procalcitonin) (p = 0.0086). A permutation post hoc multiple comparisons indicate a statistical significance between the differences of Normal-Low (difference = −2.25, p = 0.0099), High–Low (difference = −1.95, p = 0.0125) neutrophil levels.
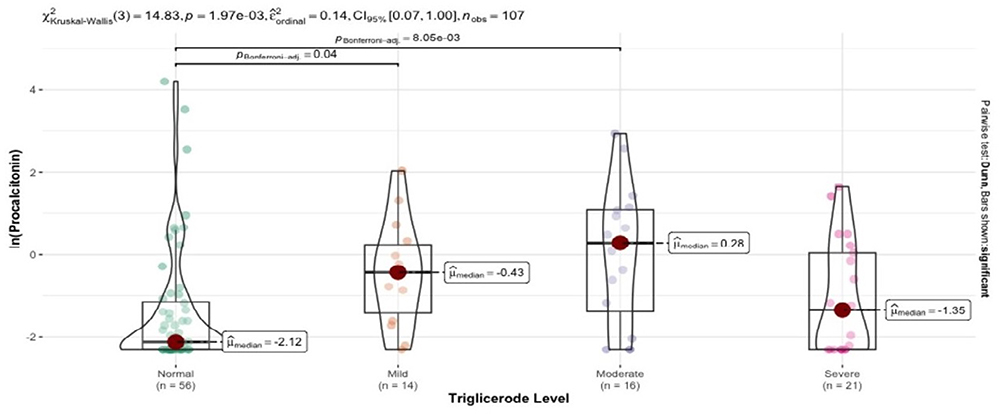 |
Figure 2 Kruskal–Wallis test indicates higher median procalcitonin values in mild (p=0.04) and moderate hypertriglyceridemia (p=0.0080). |
In a multivariate analysis of ln(procalcitonin), we found lipase (p = 0.0249), duration of antibiotics (p = 0.0009), multi-organ failure (p = 0.0045) to all be statistically significant, and lactate being mildly significant in the multivariate model (p = 0.0643). For every unit increase in lipase, we expect an increase in the natural log of procalcitonin of 0.040802. We found no relationship between procalcitonin values and BISAP score. The comparison of the lowest levels of procalcitonin to the highest levels recorded suggests an increase (based on the model) of one day in the duration of antibiotics. A 5 unit increase in lactate is expected to increase ln(Procalcitonin) by (0.0861*5 = 0.4305) or roughly 1.5380 on the original Procalcitonin scale. A linear model of log_procalcitonin predicting the initiation of antibiotics showed statistical significance p < 0.05 and suggested a mean difference of approximately 3.66 ng/mL between the procalcitonin of patients who were started antibiotics on the day of admission and those who were not.
Multivariate analysis was also performed for other outcomes using seven models (such as antibiotic used on the day of admission, duration of antibiotics, mortality related to pancreatitis and length of stay in the hospital, number of subsequent admissions, ICU admission, and multi-organ failure) to decrease the effect of confounding variables. Nonparametric bootstrap linear regression was applied for multivariate analysis of outcome length of stay instead of multiple linear regression technique.13 Modeling suggested the following:
- A patient with an underlying active infection was 15.95 times more likely to have antibiotics started on the day of admission, and we expect to see an increased duration of antibiotics by 5.7 days.
- For every unit increase in lactate, there is an increase in the odds of antibiotic on the day of admission of 1.22, and we expect to see an increase in the odds of multi-organ failure of 1.30 over the previous lactate value.
- For every unit increase in BISAP, there is an increase in the odds of mortality by 2.76, duration of antibiotics by 1.7 days, length of stay by 2.37 days, ICU admission by 8.46, and multi-organ failure by 5.52 over the previous BISAP value.
- For every unit increase in the modified CT Severity Index, we expect to see an increase in the duration of antibiotics by 0.8140 days.
- Patients with severe hypertriglyceridemia are expected to have 2.97 days longer stay and are 73.67 times more likely to be admitted to ICU than those with normal levels. Moderate hypertriglyceridemia is 26 times more likely to be admitted to the ICU than normal levels.
- Patients with alcoholism have an increase in odds of readmission of 3.45 compared to patients without a history of alcoholism. Chronicity increases the odds of readmission by 3.88.
- The odds of a patient with alcoholic/diabetic ketoacidosis being admitted to the ICU is 8.64 times, and multi-organ failure is 8.64 times higher than a patient without ketoacidosis.
Discussion
Acute pancreatitis is a common diagnosis for patients admitted to the hospital. Elevated inflammatory markers and diagnostic tools have evolved over time to predict its severity and clinical outcomes. PCT is a 116‐amino acid polypeptide primarily used for diagnosing bacterial infections, but it is now used in patients with metastatic diseases and neuroendocrine tumors.14
The literature supports the use of procalcitonin to promote the judicial use of antibiotics in cases of pancreatitis.15,16 It is also used to address the serious concerns regarding infection with Carbapenem-resistant organisms (CRO) that has become an evolving cause of mortality in acute pancreatitis. Procalcitonin and lactic acid represent two independent risk factors for mortality in acute pancreatitis with CRO infection.17 The importance of procalcitonin also lies in need for ERCP if pancreatitis has concomitant cholangitis, in which case the initiation of antibiotics can be crucial.18 A cut-off value of >0.5 ng/mL for plasma PCT was 100% sensitive and 80% specific for predicting antibiotic requirements.19 A ROC analysis suggested a cut-off threshold of 0.36 ng/mL for procalcitonin when the antibiotics were started (sensitivity 66%, specificity 79%).
The main objective of our study was to identify the potential correlation between procalcitonin levels and the severity of acute pancreatitis and determine if serum levels of procalcitonin help identify patients that would benefit from antibiotic therapy in acute pancreatitis. We also analyzed various other variables that could affect clinical outcomes in acute pancreatitis.
Based on univariate analysis of Procalcitonin, we found the starting of antibiotics on the day of admission to be statically significant for the difference in mean (difference = 4.06, p = 0.0051) and median (difference = 0.66, p = 0.0000) procalcitonin values. We also found the median differences in mortality to be mildly significant (difference = 0.79, p = 0.0640). We also found the medians of procalcitonin to be statistically significant based on mortality (difference = 1.38, p = 0.0640). A permutation ANOVA based on ln(procalcitonin), comparing levels of hypertriglyceridemia, neutrophil level, and lipase level, also showed statistical significance.
In a multivariate analysis of ln(procalcitonin), we found lipase (p = 0.0249), duration of antibiotics (p = 0.0009), multi-organ failure (p = 0.0045) to all be statistically significant, and lactate being mildly significant in the multivariate model (p = 0.0643). A linear model of log_procalcitonin showed a mean difference of approximately 3.66 ng/mL between the procalcitonin of patients who started antibiotics on the day of admission and those who were not.
Multivariate analysis was also performed for various clinical outcomes in acute pancreatitis. The seven models suggested few significant conclusions about the predictor variables in acute pancreatitis. The most interesting finding in these results was that with every unit increase in BISAP, there is an increase in the odds of mortality, duration of antibiotics, length of stay, and the likelihood of ICU admission with multi-organ failure. For every unit increase in the modified CT Severity Index, there were increased odds of increasing antibiotic duration. Patients with severe hypertriglyceridemia are more likely to have a more extended stay with a higher likelihood of admission to the ICU.
The internal validity of our study was maximized by controlling the confounding variables. Other indicators of internal validity include the BISAP, which is a significant and well-known predictor of mortality, duration of antibiotics, ICU admission, length of stay, and multi-organ failure.6 To improve the external validity/generalizability, we included clear eligibility criteria and collected multiple variables. We were able to collect an appropriate sample size. Intraobserver and interobserver variability were decreased by reviewing all the data twice by the same observer and cross-checking all the data by two observers. This resulted in increased reliability of the study. The limitations of our study include possible selection bias since this was a retrospective cohort.
Conclusions
The procalcitonin level can predict the initiation of antibiotics, duration of antibiotics, multi-organ failure, and mortality in patients with acute pancreatitis. A ROC analysis suggested a cut-off threshold of 0.36 ng/mL for procalcitonin when the antibiotics were started (sensitivity 66%, specificity 79%). Procalcitonin should always be included in the workup of acute pancreatitis. Procalcitonin levels may also help to predict triglyceride levels which may otherwise be unavailable on the day of admission.
Funding
There was no direct funding for this study. However, the article processing charges will be covered by Kern Medical.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Majidi S, Golembioski A, Wilson SL, Thompson EC. Acute pancreatitis: etiology, pathology, diagnosis, and treatment. South Med J. 2017;110(11):727–732. doi:10.14423/SMJ.0000000000000727
2. Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology. 1990;174(2):331–336. doi:10.1148/radiology.174.2.2296641
3. Ranson JH. Etiological and prognostic factors in human acute pancreatitis: a review. Am J Gastroenterol. 1982;77(9):633–638.
4. Larvin M, McMahon MJ. APACHE-II score for assessment and monitoring of acute pancreatitis. Lancet. 1989;2:201–205. doi:10.1016/S0140-6736(89)90381-4
5. Singh VK, Wu BU, Bollen TL, et al. A prospective evaluation of the bedside index for severity in acute pancreatitis score in assessing mortality and intermediate markers of severity in acute pancreatitis. Am J Gastroenterol. 2009;104:966–971. doi:10.1038/ajg.2009.28
6. Gao W, Yang HX, Ma CE. The value of BISAP score for predicting mortality and severity in acute pancreatitis: a systematic review and meta-analysis. PLoS One. 2015;10:e0130412.
7. Riché FC, Cholley BP, Laisné MJ, et al. Inflammatory cytokines, C reactive protein, and procalcitonin as early predictors of necrosis infection in acute necrotizing pancreatitis. Surgery. 2003;133(3):257–262. doi:10.1067/msy.2003.70
8. Rau BM, Kemppainen EA, Gumbs AA, et al. Early assessment of pancreatic infections and overall prognosis in severe acute pancreatitis by procalcitonin (PCT): a prospective international multicenter study. Ann Surg. 2007;245(5):745–754. doi:10.1097/01.sla.0000252443.22360.46
9. Banks PA, Bollen TL, Dervenis C, et al.; Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis–2012: revision of the Atlanta classification and definitions by international consensus. Gut. 62;2013:102–111. doi:10.1136/gutjnl-2012-302779
10. Fu CY, Yeh CN, Hsu JT, Jan YY, Hwang TL. Timing of mortality in severe acute pancreatitis: experience from 643 patients. World J Gastroenterol. 2007;13(13):1966–1969. PMID: 17461498; PMCID: PMC4146974. doi:10.3748/wjg.v13.i13.1966
11. Makowski D, Lüdecke D, Patil I, Thériault R, Ben-Shachar M, Wiernik B. Automated results reporting as a practical tool to improve reproducibility and methodological best practices adoption. CRAN; 2023. Available from: https://easystats.github.io/report/.
12. R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2023. Available from: https://www.R-project.org/.
13. Canty A, Ripley BD. 2022. boot: bootstrap R (S-Plus) Functions_. R package version 1.3-28.1. In: Davison AC, Hinkley DV, editors. Bootstrap Methods and Their Applications. Cambridge: Cambridge University Press. Available from: http://statwww.epfl.ch/davison/BMA/.
14. Wang WZ, Xu LJ, Hu DM, Tang W. Case of an abnormal procalcitonin-producing metastatic pancreatic neuroendocrine tumor. Clin Case Rep. 2020;8(11:2269–2272. doi:10.1002/ccr3.3187
15. Soulountsi V, Schizodimos T. Use of antibiotics in acute pancreatitis: ten major concerns. Scand J Gastroenterol. 2020;55(10):1211–1218. doi:10.1080/00365521.2020.1804995
16. Siriwardena AK, Jegatheeswaran S, Mason JM. PROCAP investigators. A procalcitonin-based algorithm to guide antibiotic use in patients with acute pancreatitis (PROCAP): a single-centre, patient-blinded, randomised controlled trial. Lancet Gastroenterol Hepatol. 2022;7(10):913–921. doi:10.1016/S2468-1253(22)00212-6
17. Wu D, Huang Y, Xiao J, Qin G, Liu H, Peng J. Risk factors for mortality among critical acute pancreatitis patients with carbapenem-resistant organism infections and drug resistance of causative pathogens. Infect Dis Ther. 2022;11(3):1089–1101. doi:10.1007/s40121-022-00624-w
18. Alberti P, Pando E, Mata R, et al. The role of procalcitonin as a prognostic factor for acute cholangitis and infections in acute pancreatitis: a prospective cohort study from a European single center. HPB. 2022;24(6):875–884. doi:10.1016/j.hpb.2021.10.016
19. Dias BH, Rozario AP, Olakkengil SA, V. A. Procalcitonin strip test as an independent predictor in acute pancreatitis. Indian J Surg. 2015;77(Suppl 3):1012–1017. doi:10.1007/s12262-014-1112-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.