")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
RELAX and FIRMNESS: The Combination of Muscle Relaxation with Botulinum Toxin and Collagen Biostimulation with Calcium Hydroxyapatite for the Treatment of the Cervical Region
Authors Faria GE , Palo JS , Torres AR, Machado AC , Boggio RF
Received 24 August 2023
Accepted for publication 30 September 2023
Published 6 October 2023 Volume 2023:16 Pages 2781—2791
DOI https://doi.org/10.2147/CCID.S430762
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Gladstone EL Faria, Juliana S Palo, Andre R Torres, Ana CHR Machado, Ricardo F Boggio
Cosmiatry Department, Instituto Boggio, São Paulo, SP, Brazil
Correspondence: Gladstone EL Faria, Cosmiatry Department, Instituto Boggio, Rua Cincinato Braga nr 37. 8 floor, São Paulo, SP, 01333-011, Brazil, Email [email protected]
Introduction: There are several therapeutic modalities for neck rejuvenation, especially calcium hydroxylapatite. Botulinum toxin, by relaxing the mm. platysma, also provides improvement in facial contour. Combination treatments for this region are usually recommended as they offer better results.
Objective: This study evaluated the efficacy and safety of the joint dilution of both products (Relax and Firmness – RF), applied in the same device, based on the treatment in the topography of the platysma muscle, ie, starting from the lower third of the face and extending to the neck.
Methods: Prospective, blinded, controlled study with 10 participants randomly assigned to RF and 5 in the control group (treated with CaHA only). Results were recorded through the Vectra platform and subjectively evaluated through the GAIS scale by participants and blinded evaluators. Objective analysis was performed using corneometry. Times evaluated: pre-treatment, 30 and 90 days. Considered statistically significant when p< 0.1.
Results: 100% of the RF group reported “excellent improvement” at D30 and 30% at D90. In the control group, 100% reported “very improved” at D30 and 20% rated “excellent improvement” at D90. A higher and earlier satisfaction rate was observed in the RF group. No difference in corneometry was found between the groups at D30. At D90, the control group had a mean increase of 0.24 versus 5.17 in the RF group (p-value=0.089*). When we analyzed the percentage variation from baseline, the control group was stable, while the RF showed a mean increase of 8.89% (p-value=0.062*).
Discussion: We demonstrated the safety and effectiveness of the association of both products, diluted and applied together through microcannulas. Minimization of punctures, patient comfort, and technique based on the anatomy of the platysma muscle underlie the technique. High rates of early satisfaction due to botulinum toxin (Relaxation) and late satisfaction due to CaHA (Firmness).
Keywords: calcium hydroxylapatite, botulinum toxin, rejuvenation, neck, platysma muscle
Introduction
Skin aging of the cervical region is a common complaint of patients, evolving with skin laxity and atrophy, loss of mandibular contour, hyperactivity of the platysma muscle, and formation of platysmal bands.1–3
The skin of the region, characteristically quite thin, is subject to the effects of gravity, as well as to the intense activity of the platysma muscle, whose contraction favors the depression not only of the lower third but of the entire face.
Given the multiple factors related to aging of the region, combined therapies provide better results. The subdermal application of calcium hydroxylapatite (CaHA) induces an increase in the synthesis of collagen and elastin, increases the production of components of the extracellular matrix such as proteoglycans, improves dermal elasticity, allows skin retraction in the submental region, and increases the thickness of the local skin, desirable for this anatomical topography.4–6 Several techniques are described for the use of botulinum toxin in the treatment of the muscles of the cervical region, especially in the platysma muscle, either to improve mandibular contour or to relax the platysmal bands. The application is usually done with needles, requiring multiple punctures and is usually performed at a different time from the application of calcium hydroxylapatite.7–12
Addressing different targets of neck aging by combining techniques simultaneously, such as collagen biostimulation with calcium hydroxylapatite and botulinum toxin for muscle relaxation, would provide advantages to the applicator and the patient. To the applicator, ease of technique and agility. To the patient, comfort by avoiding multiple punctures and multiple visits to the doctor’s office, as well as an improvement in the perception of the therapeutic result.
The improvement in the perception of results is related to the combination of early and late effects provided by the technique. The earliest effect is related to muscle relaxation with botulinum toxin, being noticed about 5 to 7 days after the application. The latter effect is related to collagen biostimulation, thus increasing the satisfaction rates with the treatment.
Objective
We evaluate the efficacy and safety of the joint application of calcium hydroxylapatite associated with botulinum toxin, in the same device, using microcannulas, for the treatment of tissue aging in the neck region.
Materials and Methods
The project was submitted to the Research Ethics Committee (FAM – Centro Universitário das Américas) under CAAE number: 61457522.1.0000.9487 with a favorable opinion for the conduction of the study under resolution number 5.642.484. All ethical principles were followed during the research, as well as the principles in the Helsinki Declaration. Inclusion criteria were women with flaccidity grades 1 and 2 proposed by Narins, et al,13 regardless of age. Participants with formal contraindications or allergies to the injectable components were excluded from the study.
This is a prospective and controlled study, in which 15 volunteers were distributed between intervention and control groups. Of these, 10 were randomly assigned to the intervention group and received treatment for their neck regions as described in the Relax and Firmness technique (botulinum toxin associated with calcium hydroxylapatite). Another five volunteers, in the control group, received treatment for the cervical region exclusively with the calcium hydroxylapatite biostimulator, according to the same application technique. Written informed consent was provided by all the participants prior to any intervention with permission to publish their images.
All treatments were performed on the same day, by the same professional, at Instituto Boggio, São Paulo, Brazil. The control group received treatment with a syringe containing 1.5 mL calcium hydroxylapatite (Radiesse, Merz North America, Inc., Raleigh, North Carolina, USA) diluted in a 1:4 ratio in a solution of 4.5 mL saline solution and 1.5 mL lidocaine 2% with epinephrine, totaling a volume of 7.5 mL,14,15 applied with a 22g – 5cm microcannula, as shown in Figure 1. A total volume of 7.5 mL was applied with the use of vectored figures as already published by this group of researchers.16 A small adaptation in the distribution of the vectorized figures was made in order to reserve 1.5 mL of the solution for application on the jaw line from the Jowl (0.75 mL per side). The reason for this adaptation is the possibility of starting treatment of the neck exactly by the mandibular contour, a region known to respond well to both biostimulation and botulinum toxin treatment.
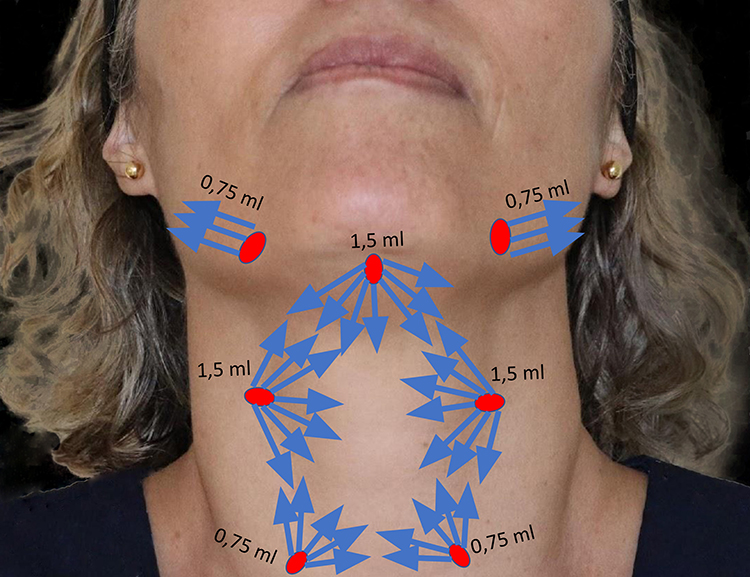 |
Figure 1 Application demarcation with solution quantities. |
The intervention group, which received the Relax and firmness protocol, was demarcated exactly like the control group, but botulinum toxin (IncobotulinumtoxinA – Xeomin; Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany) was added to the CaHA dilution. The final dose of botulinum toxin, corresponding to 35 international units, was calculated based on the technique proposed by Trindade et al associated with the treatment of proximal platysmal bands.9,10 The dilution of the botulinum toxin was made with 2 mL of saline solution. Figure 2 shows the dilution of the Relax and firmness group with botulinum toxin and CaHA.
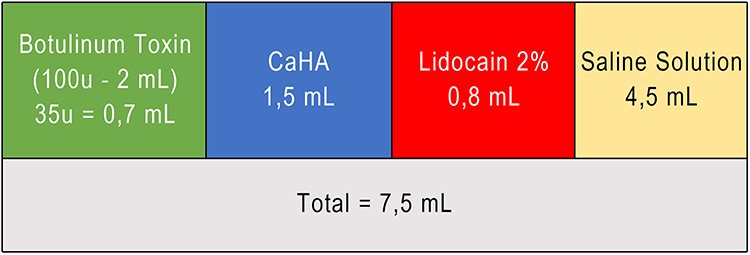 |
Figure 2 Product dilution in the Relax and Firmness technique. |
Three-dimensional photographic documentation was performed using Vectra® (Canfield Scientific, Parsippany, NJ, USA) before the procedure, 15 and 90 days after the procedure with the participants at rest and during maximum contraction of the platysma muscle. The subjective evaluation was performed using the Global Aesthetic Improvement Scale - GAIS (Table 1), applied to the participants and the researchers.14
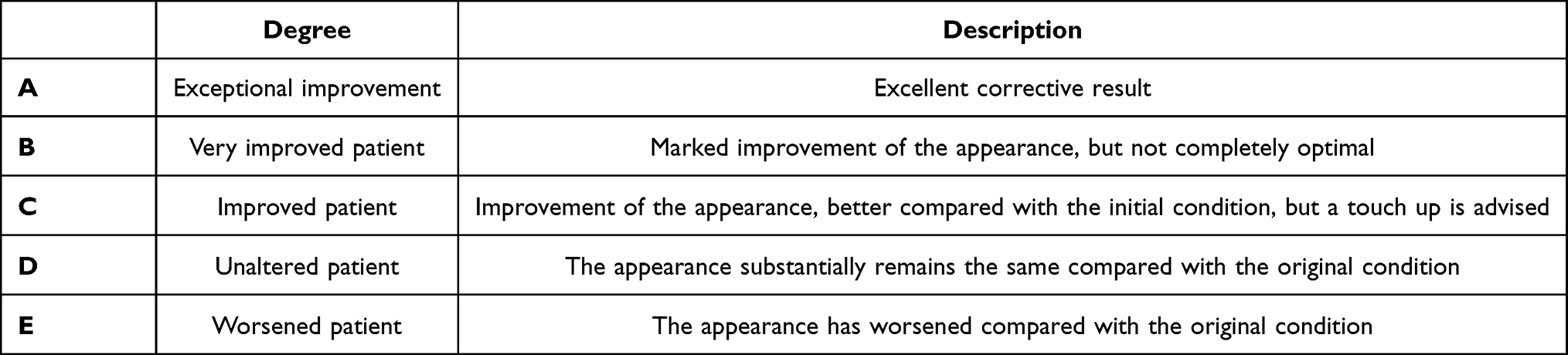 |
Table 1 GAIS – Global Aesthetic Improvement Scale |
In all evaluations, the participants were asked about adverse events, as well as the following questions: was there an improvement in your mandibular contour? (yes/no); are you satisfied enough to repeat the procedure? (yes/no).
As an objective method to evaluate the results, the hydration of the stratum corneum was assessed using the Corneometer MPA 580 (Courage+Khazaka electronic GmbH, Germany). These measurements were made under strict control of room temperature and humidity, so as not to interfere with the measurements.
The statistical analysis was carried out through non-parametric statistical methods, once the distribution was considered non-normal. For comparison between groups, the Mann–Whitney test was applied. The change in hydration gain for each month as a function of baseline was also calculated. For intra-group gain comparison, Friedman test was applied. Due to the sample size, it was considered statistically significant when p<0.1 (10%). SPSS V26 (2019), Minitab 21.2 (2022), and Excel Office 2010 software were used for statistical analysis.
Results
All participants in the study were females, aged between 32 and 58 years, with a mean of 46 years in the intervention group and 42 years in the control group. The average body mass index was 24 kg/m2 in the intervention group and 22 kg/m2 in the control group (Table 2). All participants had complaints related to neck laxity between 1 and 2, associated with loss of mandibular contour.
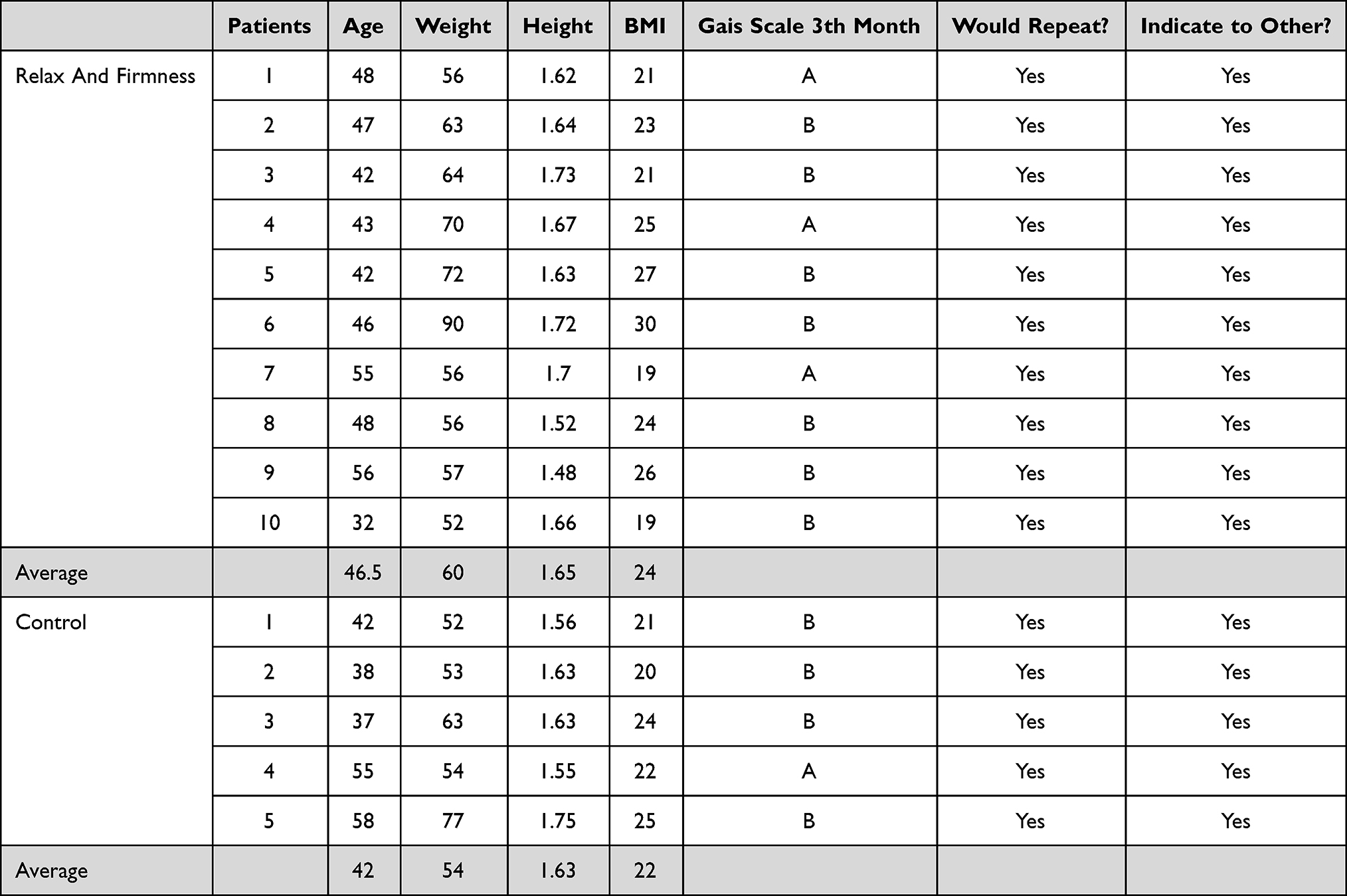 |
Table 2 Participant Demographics with Results |
The number of units of Incobotulinotoxin added to the dilution of calcium hydroxylapatite was 35 units (0.7 mL of the 100u dilution for 2mL). This number was found based on the average number of units performing hypothetical markings of the patients as if traditional needle treatment was performed, based on the techniques of Trindade et al10 for mandibular contouring, associated with Levi et al9 for proximal platysmal bands. Thus, the final solution applied was as follows: 0.7 mL of botulinum toxin + 1.5 mL of CaHA + 0.8 mL of lidocaine 2% + SF0.9% totaling 7.5 mL of final volume (1:4 dilution of CaHA).
The subjective evaluation, based on the GAIS scale, measured by the patients in the relax and firmness group, at 15 days of treatment showed the result of “excellent improvement” in 100% of cases, while for the control group the result was “very improved” in all participants. After 90 days of treatment, 30% (3/10) of the participants in the relax and firmness group reported “excellent improvement”, while 70% (7/10) reported “very improved.” For the control group at 90 days of treatment 20% (1/5) reported “excellent improvement”, while 80% reported “very improved.”
The same subjective evaluation using the GAIS scale was applied to those involved in the study. For the authors, at 15 days of treatment, evaluation of the participants at rest and during maximal contraction of the platysma muscle resulted in 100% of the cases with “excellent improvement” for the Relax and Firmness group, while for the control group two participants scored A, one B, and two C. At 90 days into the procedure, 3 of the five participants were rated “excellent improvement”, while 2 of the five control participants were rated “very improved.” For the Relax and Firmness group, 100% of the cases were evaluated as “excellent improvement” at 90 days of treatment. Results can be observed in Figures 3–5.
 |
Figure 3 Relax and Firmness technique before and 90 days after in maximum platysma muscle contraction. Clinical case 1: (A) before in profile position, (B) after in profile position, (C) before ¾, (D) after ¾); Clinical case 2: (E) before in profile; (F) after in profile, (G) before ¾, (H) after ¾). |
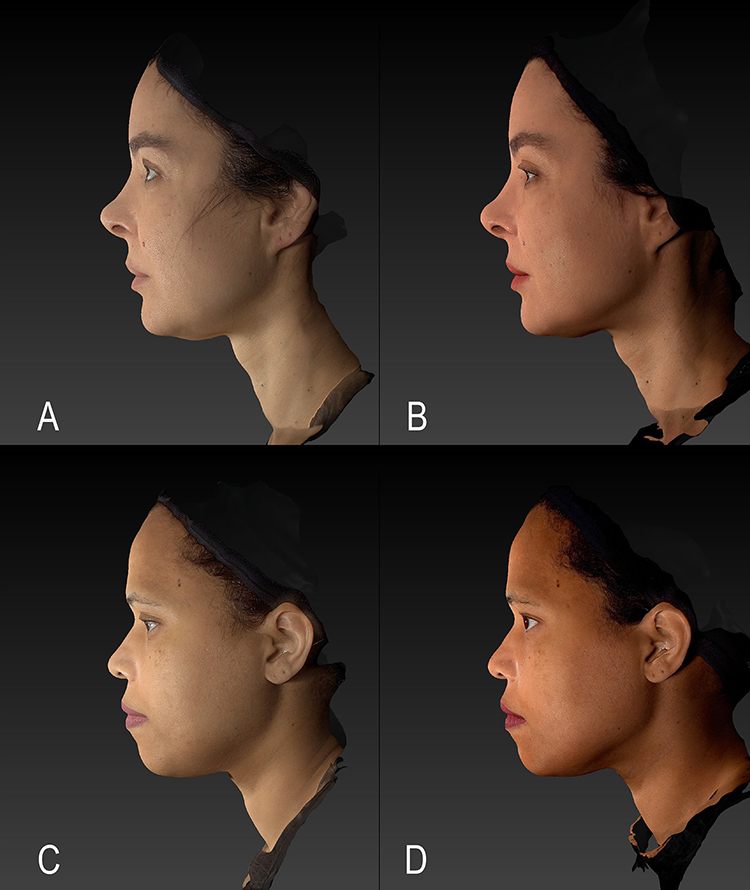 |
Figure 4 Relax and Firmness technique before and 90 days after at rest in the platysma muscle. Clinical case 3: (A) before at rest, (B) after at rest; Clinical case 4: (C) before at rest, (D) after at rest. |
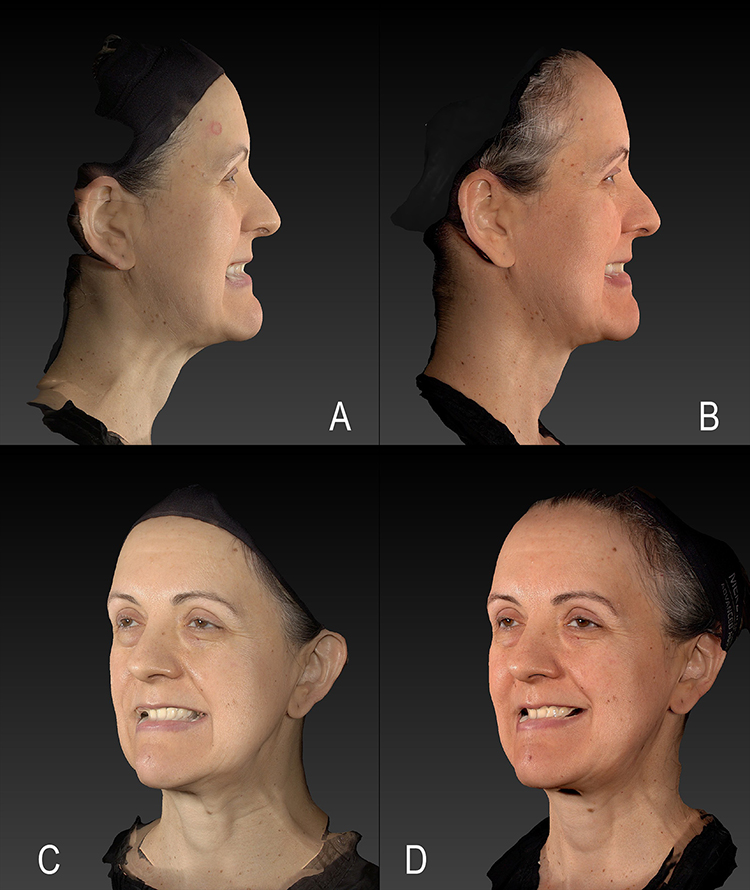 |
Figure 5 Control group in maximal platysma contraction. Clinical case 5: (A) before in profile position, (B) after in profile position; (C) before ¾, (D) after ¾. |
There were no reports of adverse effects such as nodules or major muscle paralysis in the neck region. Small punctual ecchymoses were reported by the participants but without major repercussions and self-resolving. In both groups, 100% of the patients reported improvement in their mandibular contour and 100%, also from both groups, were satisfied to the point of repeating the procedure and/or referring to it. It was indirectly observed that the satisfaction index, both by participants and observers, tended to be earlier in the Relax and Firmness group compared to the control group, probably due to the effect of botulinum toxin on the platysma muscle, promoting an early improvement in mandibular contour.
From an objective point of view, the participants were submitted to an evaluation of the deep hydration of the skin through the corneometry exam. In the control group, the baseline values were 60.1 and showed a slight decrease to 59.3 at D30 and an increase to 60.4 at D90. For the Relax and Firmness group, the average baseline value was 58.1, reaching a value of 61.3 after 1 month and, after 3 months, a value of 64.3 (Figure 6).
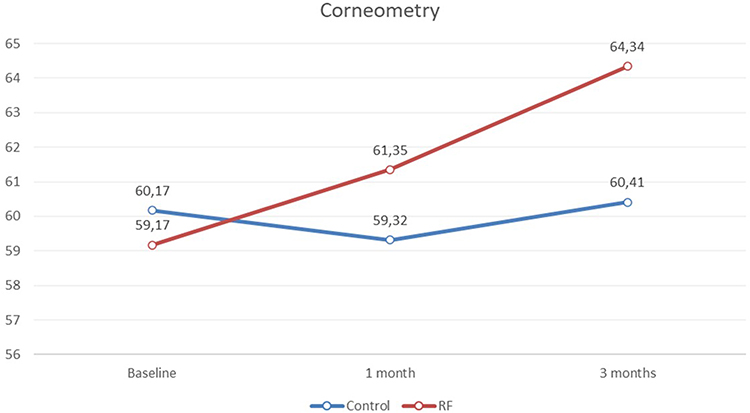 |
Figure 6 Hydration evaluation by corneometry between control group and Relax and Firmness (RF) baseline, 1 month post intervention and 3 months post-intervention. |
For the first month, there was no statistically significant difference between the groups. On the other hand, after 3 months it was observed that the Control Group had a mean increase of 0.24 against 5.17 in the RF (p-value = 0.089*). When the percentage variation from baseline was analyzed, the Control mean represented a reduction of −0.18% (considered a stabilization) against a mean increase of 8.89% in the RF (p-value = 0.062*) - (Figure 7).
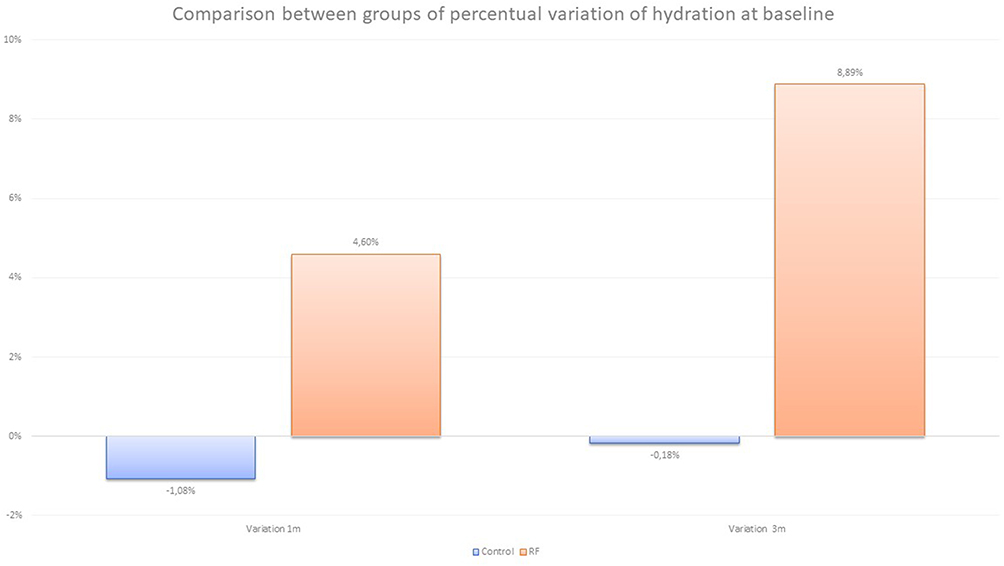 |
Figure 7 Hydration percentage variation from the baseline measured by corneometry. |
Discussion
Aging of the cervical region is a common complaint among patients. Its multifactorial origin requires combined therapy for satisfactory results. Collagen biostimulators are usually the main tool for the treatment of this region,17 but they have no repercussion on the improvement of facial contour with regard to muscular action, imposed mainly by the platysma muscle.10 For this purpose, botulinum toxin stands out, and there are several techniques for this, all of them with the use of needles, multiple punctures, and so far no description of combined therapy in the same session and with the same device.
Calcium hydroxylapatite has long-term effect due to biostimulation of collagen, elastin, and proteoglycans4–6. Besides, it can promote improvement in the cutaneous hydration and elasticity with a single application. However, more than one session is usually indicated to achieve better results. The improvement of the mandibular contour is achieved with the application of botulinum toxin in the region, due to the relaxation of the platysma muscle, being observed in a few days after the application.
Combination therapy involving botulinum toxin and calcium hydroxylapatite, diluted in the same syringe and applied with the use of cannulas, has the potential to minimize needle punctures and add the short-term benefits of botulinum toxin (relaxation) and the long-term benefits of CaHA (firmness).
The present study was able to demonstrate high indices of satisfaction for both patients and professionals in the long term (D90), but in the short term (D15) the indices of satisfaction of the relax and firmness group are higher than the control group, due to the earlier effects related to botulinum toxin.
The biostimulator, per se, has the ability to increase the production of collagen, elastin, and proteoglycans and consequently parameters of hydration and cutaneous turgor18, but this study documented that, by still unclear mechanisms, botulinum toxin potentiated the deep hydration of the skin, through corneometric data. There are several studies involving botulinum toxin beyond wrinkle control, but mainly for skin quality. The postulated mechanisms for this are reduction of pore size, control of sebum secretion and erythema, and improvement of skin texture.19–21 Previous discussions about combined therapies, focusing on neck rejuvenation with botulinum toxin, CaHA, and hyaluronic acid, have been presented in scientific events with promising results.22
Another innovation related to this clinical research refers to the marking for the treatment of the neck area. Previous publications treat the neck area always below the jawline but based on anatomical knowledge related to the jawline and anatomy of the platysma muscle (Figure 8), we chose to consider the contiguity of the lower third of the face, at the level of the jawline with the neck. This strategy is already considered for isolated treatments with botulinum toxin, but has not yet been considered in terms of biostimulation. It is understood, therefore, that joint evaluation between the two sub-units (lower third of the face and neck) should be encouraged when the Relax and Firmness technique is chosen.
 |
Figure 8 Anatomical dissection performed by the authors demonstrating the platysma muscle, which in this specimen reaches up to the middle third of the face. |
The small number of participants is a limitation of this study, but even so, positive results were demonstrated, with statistical significance after 3 months of application when compared to the control group. Furthermore, the safety and efficacy of the Relax and Firmness technique is demonstrated, not only for rejuvenation of the neck region but also for an improvement in the face–pace transition, with high rates of satisfaction. Further studies, involving more invasive techniques, should shed light on the capacity of botulinum toxin to optimize the action of collagen biostimulators.
Conclusion
The Relax and Firmness technique, comprising the association of botulinum toxin and CaHA, diluted together and applied to the same device (microcannula) for the rejuvenation of the cervical region, has proven to be effective and safe, with high rates of satisfaction in the short and long term and with potential improvement in objective parameters such as elasticity and hydration.
Funding
Merz Aesthetics LATAM, through its affiliate in Brazil, Merz Farmaceutica Comercial Ltda, funded translation to English, statistical analysis, and open access fee. Despite this support, this study was conducted with autonomy and independence by the medical authors, and Merz Farmacêutica Comercial, Ltda. had no participation or influence on design, conduct, collect, assess, or evaluate the presented data.
Disclosure
Dr Gladstone Faria is a speaker for Merz Aesthetics, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Trévidic P, Criollo-Lamilla G. Platysma bands: is a change needed in the surgical paradigm? Plast Reconstr Surg. 2017;139(1):41–47. doi:10.1097/PRS.0000000000002894
2. Alcalá BE, Bravo BS. Novel classifications for muscular contraction of the lower face and neck. Dermatol Surg. 2019;45(8):1080–1084. doi:10.1097/DSS.0000000000001813
3. Boggio RF. Anatomia facial aplicada. DiLivros; 2022.
4. Graivier MH, Bass LS, Busso M, Jasin ME, Narins RS, Tzikas TL. Calcium hydroxylapatite (Radiesse) for correction of the mid-and lower face: consensus recommendations. Plast Reconstr Surg. 2007;120(6S):55S–66S. doi:10.1097/01.prs.0000285109.34527.b9
5. Cogorno Wasylkowski V. Body vectoring technique with Radiesse® for tightening of the abdomen, thighs, and brachial zone. Clin Cosmet Investig Dermatol. 2015;267–273. doi:10.2147/CCID.S75631
6. González N, Goldberg DJ. Evaluating the effects of injected calcium hydroxylapatite on changes in human skin elastin and proteoglycan formation. Dermatol Surg. 2019;45(4):547–551. doi:10.1097/DSS.0000000000001809
7. Brandt FS, Ballin AC, Green JB, et al. Orbicularis oris, mentalis, depressor anguli oris. In: Botulinum Toxin E-Book: Procedures in Cosmetic Dermatology Series. Elsevier Health Sciences; 2012:123.
8. Faria GE, Vilela CL, Bastos AQ, et al. Loss of definition of the submental contour: correct diagnosis and treatment algorithm. Surg Cosmet. 2022;14:e20220131.
9. Levy Phillip M. The ‘Nefertiti lift’: a new technique for specific re‐contouring of the jawline. J Cosmet Laser Ther. 2007;9(4):249–252. doi:10.1080/14764170701545657
10. de Almeida AR, Romiti A, Carruthers JD. The facial platysma and its underappreciated role in lower face dynamics and contour. Dermatol Surg. 2017;43(8):1042–1049. doi:10.1097/DSS.0000000000001135
11. Bravo BSF, De Bastos JT, Da Rocha CR, et al. Definition of the mandibular angle using botulinum toxin type A: a new technique for the improvement of mandibular contour and definition. J Clin Aesthet Dermatol. 2019;12(11):32.
12. Wu WT. Microbotox of the lower face and neck: evolution of a personal technique and its clinical effects. Plast Reconstr Surg. 2015;136(5):92S–100S. doi:10.1097/PRS.0000000000001827
13. Narins RS, Carruthers J, Flynn TC, et al. Validated assessment scales for the lower face. Dermatol Surg. 2012;38(2):333–342. doi:10.1111/j.1524-4725.2011.02247.x
14. Goldie K, Peeters W, Alghoul M, et al. Global consensus guidelines for the injection of diluted and hyperdiluted calcium hydroxylapatite for skin tightening. Dermatol Surg. 2018;44:S32–S41. doi:10.1097/DSS.0000000000001685
15. de Almeida AT, Figueredo V, da Cunha AL, et al. Consensus recommendations for the use of hyperdiluted calcium hydroxylapatite (Radiesse) as a face and body biostimulatory agent. PRS Global Open. 2019;7(3). doi:10.1097/GOX.0000000000002160
16. de Lima Faria GE, Dos Santos DB, Tartare A, Bento AM, Boggio RF. Standardization of the body vectoring technique with calcium hydroxyapatite. Surg Cosmet. 2020;12(2):172–178.
17. Guida S, Longhitano S, Spadafora M, et al. Hyperdiluted calcium hydroxylapatite for the treatment of skin laxity of the neck. Dermatol Ther. 2021;34(5):e15090. doi:10.1111/dth.15090
18. Yutskovskaya YA, Kogan EA. Improved neocollagenesis and skin mechanical properties after injection of diluted calcium hydroxylapatite in the neck and décolletage: a pilot study. J Drugs Dermatol. 2017;16(1):68–74.
19. Hanna E, Xing L, Taylor JH, Bertucci V. Role of botulinum toxin A in improving facial erythema and skin quality. Arch Dermatol Res. 2021;2021:1–10.
20. Beuttler MM, Harrington HD, Hooper DO. Beyond muscle: a narrative review of onabotulinum toxin A for skin quality. J Drugs Dermatol. 2021;20(9):958–962. doi:10.36849/JDD.6038
21. Fabi SG, Park JY, Goldie K, Wu W. Microtoxin for improving pore size, skin laxity, sebum control, and scars: a roundtable on integrating intradermal botulinum toxin type A microdoses into clinical practice. Aesth Surg J. 2023;43(9):1015.
22. Sanctis Pecora C. Calcium Hydroxyapatite combined with neurotoxin injection for the improvement of jawline contouring and neck. In:
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.