Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Relationship Between Type 1 Diabetes Mellitus and Dental Caries Status with Related Oral Health Indicators in Children
Authors Wang M ![]() , Xia T, Wang Y
, Xia T, Wang Y
Received 12 March 2025
Accepted for publication 15 July 2025
Published 11 August 2025 Volume 2025:18 Pages 2807—2814
DOI https://doi.org/10.2147/DMSO.S527842
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Mengxing Wang, Tian Xia, Ying Wang
Department of Stomatology, Capital Center For Children’s Health, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Mengxing Wang, Department of Stomatology, Capital Center For Children’s Health, Capital Medical University, No. 2 Yabao Road, Chaoyang District, Beijing, 100020, People’s Republic of China, Email [email protected]
Objective: This study aims to explore the relationship between type 1 diabetes mellitus (T1DM) and dental caries status along with related oral health indicators.
Methods: A case-control study was conducted with a retrospective analysis of 40 diagnosed T1DM patients (patient group) and 40 age- and gender-matched healthy children (control group) treated at our hospital from 2020 to 2023. All participants underwent oral health assessments and relevant clinical examinations. By comparing the levels of related indicators between diabetic patients and healthy children, this study provides a scientific basis for prevention and treatment.
Results: There was no significant difference in general baseline characteristics between the two groups (P> 0.05). The levels of fasting blood glucose (FBG), 2-hour postprandial blood glucose (2h PBG), and glycated hemoglobin (HbA1c) were significantly higher in the patient group (P< 0.05). The incidence of dental caries was significantly higher in the patient group (P< 0.05). Additionally, the patient group had higher gingival bleeding index, plaque index, and probing depth (P< 0.05). The salivary pH value in the patient group was also significantly higher (P< 0.05). However, there was no significant difference in salivary immunoglobulin A (sIgA) and salivary immunoglobulin G (sIgG) between the groups (P> 0.05). This study is limited by its small sample size (n=40 per group) and single-center retrospective design.
Conclusion: Type 1 diabetes mellitus may alter saliva composition, while hyperglycemia can cause gingival inflammation and affect periodontal health. These changes may interfere with tooth mineralization, increasing caries risk in children.
Keywords: dental caries status, gingival index, pediatric, salivary immunoglobulin A, sIgA, salivary immunoglobulin G, sIgG, type 1 diabetes mellitus
Introduction
Type 1 diabetes mellitus (T1DM) is an autoimmune disease characterized by the destruction of pancreatic β-cells and absolute insulin deficiency. It predominantly occurs in children and adolescents, with an increasing incidence in recent years.1–3 Since insulin plays a crucial role in maintaining normal metabolism, T1DM patients experience persistent hyperglycemia, which not only disrupts energy metabolism but also adversely affects multiple organ systems. In recent years, researchers worldwide have increasingly focused on the relationship between diabetes and oral health, particularly the impact of diabetes on the oral environment in children.4–6 Dental caries, one of the most common oral diseases in children, has a complex pathogenesis influenced by local oral hygiene, dietary habits, and plaque accumulation, as well as systemic diseases.7,8 Numerous studies have demonstrated that hyperglycemia can alter the composition and function of saliva, leading to imbalances in pH, changes in mineral content, and abnormalities in immunoglobulin levels. These changes may weaken saliva’s self-cleaning and antimicrobial properties, creating favorable conditions for the colonization of cariogenic bacteria. Additionally, T1DM patients often exhibit immune dysfunction, which may exacerbate local inflammatory responses in the oral cavity, leading to increased gingival bleeding and plaque accumulation. However, despite existing research, the precise mechanisms linking T1DM to dental caries development remain incompletely understood, particularly regarding synergistic effects on salivary biomarkers and periodontal health in pediatric populations.
This study retrospectively analyzed the oral health status of children diagnosed with T1DM and healthy controls at our hospital from 2020 to 2023. The objective was to explore the comprehensive impact of T1DM on the oral environment and dental development in children. Beyond being a metabolic disorder, T1DM has profound effects on oral health. Understanding the relationship between diabetes and dental caries is crucial for recognizing the systemic effects of the disease and promoting multidisciplinary prevention and treatment strategies. Therefore, this study holds significant clinical and public health value.
Subjects and Methods
Study Subjects
This retrospective case-control study was conducted based on a series of cases from our hospital. Children diagnosed with type 1 diabetes mellitus (T1DM) at our hospital between 2020 and 2023 were selected as study subjects. Eligible patients were registered, and after excluding those who did not meet the complete inclusion criteria, a total of 40 patients were enrolled in the T1DM group. Additionally, 40 age- and gender-matched healthy children who underwent routine health examinations at our hospital during the same period were selected as the healthy control group. This study was approved by the Children’s Hospital affiliated to Capital Institute of Pediatric (Approval No.: 2021-JU0193) and conducted in accordance with the 1964 Declaration of Helsinki and its amendments. The IRB waived informed consent requirements because: (1) this retrospective study used anonymized medical records; (2) the research posed minimal risk to participants; and (3) obtaining consent was impracticable due to the study’s retrospective nature. All patient data were de-identified and stored securely, with access restricted to the research team to ensure confidentiality.
Inclusion Criteria
Inclusion Criteria
1) Diagnosed with T1DM according to the diagnostic criteria established by the World Health Organization (WHO) and relevant guidelines6,9,10 with confirmation from the hospital’s endocrinology department; 2) Aged between 6 and 14 years, within the mixed dentition or early permanent dentition stage; 3) Had not received any special oral health interventions that could affect dental health during the study period, such as orthodontic treatment or fluoride application; 4) No history of other systemic diseases or immune system disorders.
Exclusion Criteria
1) Presence of other systemic diseases (eg, genetic metabolic disorders, autoimmune diseases); 2) Regular use of medications affecting oral ecology (eg, antibiotics within 2 months, immunosuppressants); 3) Previous orthodontic treatment or other dental interventions that might influence the occurrence of dental caries; 4) Incomplete oral health data or inability to cooperate with the examination.
Inclusion Criteria for Healthy Children
Inclusion Criteria
1) No antibiotic treatment in the past two months; 2) No other systemic diseases; 3) Normal intelligence; 4) Age and gender matched with the children in the patient group.
Exclusion Criteria
1) Use of antibiotics within the past two months or presence of other systemic diseases; 2) Previous orthodontic treatment or other dental interventions that could affect the occurrence of dental caries; 3) Incomplete oral health data or inability to cooperate with the examination; 4) Regular sugar-rich diet (>3 times/day sweets) or severe oral hygiene neglect (brushing <1 time/day).
Methods
The incidence of dental caries was calculated based on the World Health Organization (WHO) 1997 diagnostic criteria.11–13 Blood glucose levels, including glycated hemoglobin (HbA1c), fasting blood glucose (FBG), and 2-hour postprandial blood glucose (2h PBG), were measured for both groups. According to the WHO 1997 diagnostic standards, plaque index, gingival bleeding index, and periodontal probing depth were recorded and analyzed.
Saliva samples were collected between 9:00–11:00 AM following a 1-hour fasting period. Stimulated saliva (4–5 mL) was obtained using a standardized paraffin gum-chewing protocol (2 g paraffin gum, 60 cycles/min, 5-minute duration). Fresh samples were immediately processed: salivary pH was measured using a pH meter, and a 1 mL aliquot was stored in liquid paraffin at 0°C for transport within 30 minutes. The remaining sample was centrifuged at 3000 r/min for 10 minutes, and the supernatant was stored at –80°C. Quantification of sIgA and sIgG was performed using ELISA on 1 mL of the supernatant, with readings obtained via a microplate reader. To account for potential confounding variables, demographic and behavioral data such as oral hygiene frequency and dietary sugar intake were extracted from medical records for both groups.
Data Analysis
GraphPad Prism 8 was used for image processing. Data were organized and analyzed using SPSS 26.0. Measurement data were expressed as mean ± standard deviation (±s), and comparisons between groups were conducted using t-tests. Categorical data were expressed as [n (%)], and intergroup comparisons were performed using the χ²-test. Post-hoc power analysis conducted using G*Power 3.1 (α=0.05, effect size=0.6), achieving 83% power for primary outcomes (dental caries incidence). A significance level of P < 0.05 was considered statistically significant.
Results
General Data
The patient group (n = 40; 22M/18F, age 9.11 ± 2.24 years) and control group (n = 40; 21M/19F, age 9.57 ± 2.11 years) showed no significant differences in baseline characteristics (P > 0.05). Critically, key confounding factors (oral hygiene practices and dietary habits) were also comparable between groups (P > 0.05), as documented in medical records. See Table 1.
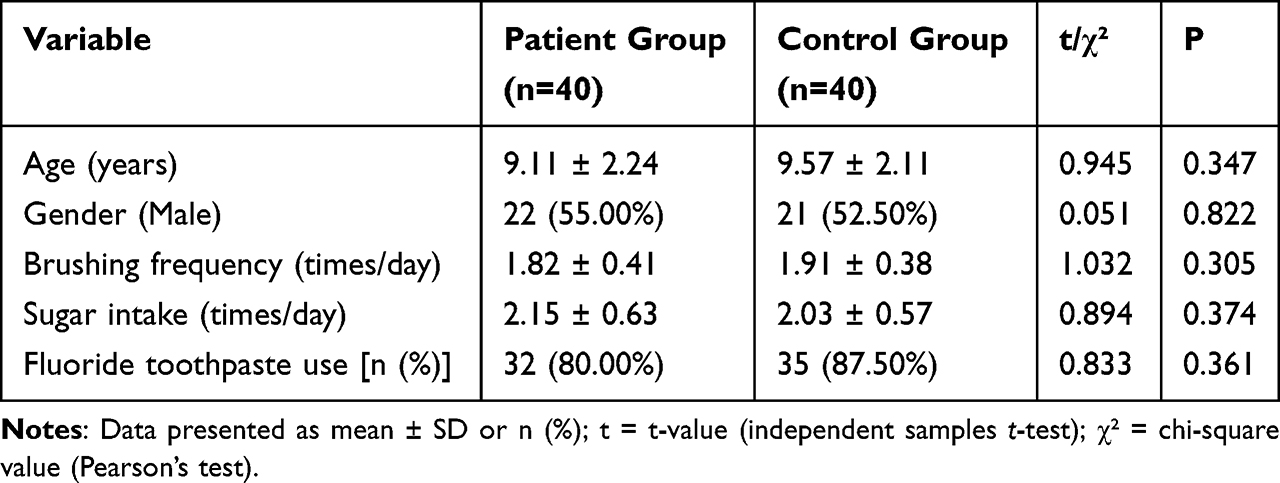 |
Table 1 Comparison of General Characteristics Between the Two Groups |
Incidence of Dental Caries
The incidence of dental caries was significantly higher in the patient group compared to the control group. Specifically, 17 cases (42.50%) in the patient group had dental caries, whereas only 6 cases (15.00%) were observed in the control group. This difference was statistically significant (χ² = 7.384, P = 0.007). The number of dental caries cases in the patient group was approximately 2.8 times that of the control group, suggesting a significant association between type 1 diabetes mellitus (T1DM) and an increased risk of dental caries in children (Table 2).
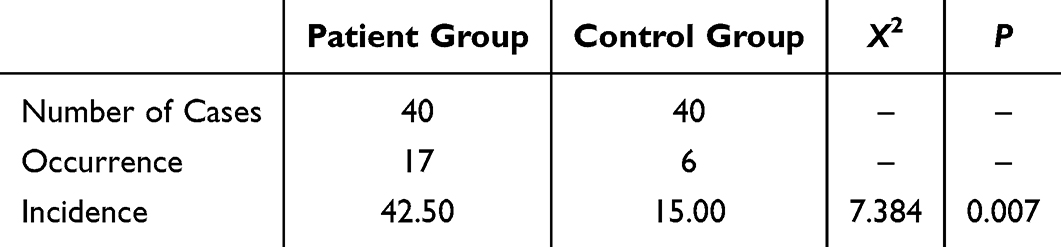 |
Table 2 Comparison of Dental Caries Incidence Between the Two Groups |
Blood Glucose Levels
Blood glucose control was significantly poorer in the patient group compared to the control group. The fasting blood glucose (FBG) level in the patient group was 8.34±1.52 mmol/L, significantly higher than 4.72±0.63 mmol/L in the control group (t = 14.82, P < 0.001). The 2-hour postprandial blood glucose (2 h PBG) was 12.67±2.15 mmol/L in the patient group, compared to 6.01±0.89 mmol/L in the control group (t = 18.23, P < 0.001). Glycated hemoglobin (HbA1c) was 8.9±1.2% in the patient group and 5.1±0.6% in the control group (t = 17.94, P < 0.001), indicating that children with diabetes remained in a prolonged hyperglycemic state (Figure 1).
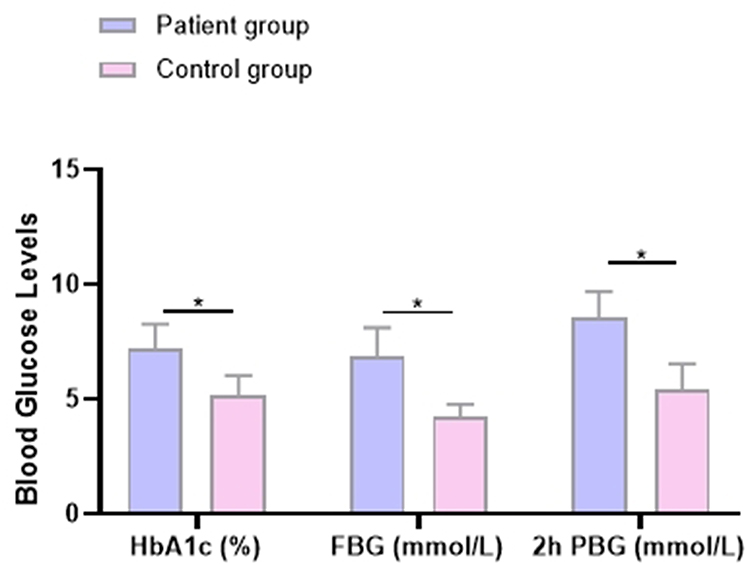 |
Figure 1 Comparison of Blood Glucose Indicators Between the Two Groups. Note: *Indicates a significant difference between the two groups (P < 0.05). |
Periodontal Clinical Indicators
Periodontal health was significantly worse in the patient group. The gingival bleeding index was 2.45±0.67 in the patient group, compared to 1.02±0.34 in the control group (t = 12.56, P < 0.001). The plaque index was 2.88±0.73 in the patient group, significantly higher than 1.21±0.41 in the control group (t = 13.25, P < 0.001). Periodontal probing depth was also greater in the patient group (3.12±0.55 mm) than in the control group (2.03±0.32 mm) (t = 11.89, P < 0.001). These findings indicate that children with diabetes are more prone to gingival inflammation and plaque accumulation (Figure 2).
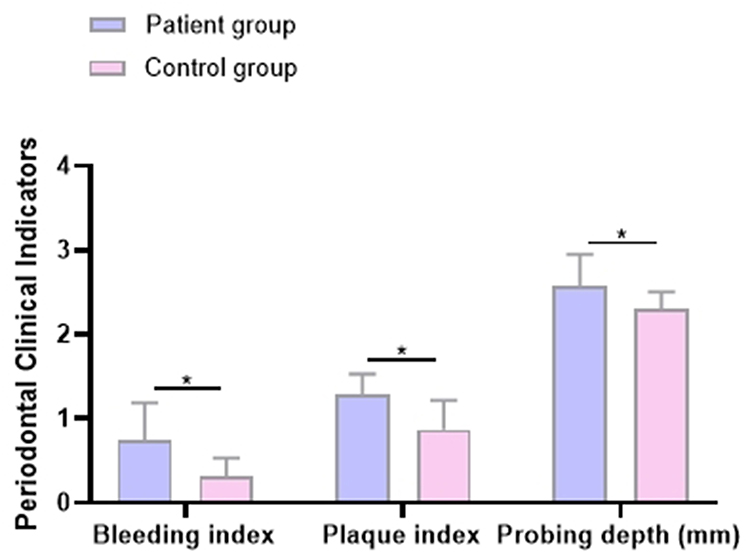 |
Figure 2 Comparison of Periodontal Clinical Indicators Between the Two Groups. Note: *Indicates a significant difference between the two groups (P < 0.05). |
Salivary pH
The salivary pH was significantly elevated in the patient group. The average salivary pH in the patient group was 7.42±0.21, which was higher than 6.89±0.18 in the control group (t = 12.03, P < 0.001). Increased salivary alkalinity may weaken its buffering capacity against acidic environments, thereby promoting dental caries development (Figure 3).
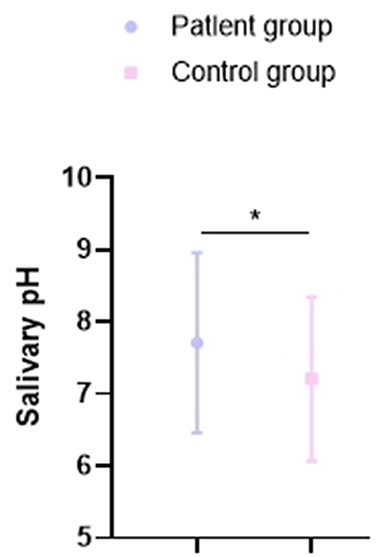 |
Figure 3 Comparison of Salivary pH Between the Two Groups. Note: *Indicates a significant difference between the two groups (P < 0.05). |
Immunoglobulin Levels
There was no significant difference between the two groups in sIgA and sIgG levels (P > 0.05), suggesting that the local oral immune function of children with diabetes was not significantly altered by the disease (Figure 4).
 |
Figure 4 Comparison of Immunoglobulin Levels Between the Two Groups. |
Discussion
In recent years, increasing attention has been directed toward the oral health of pediatric patients with type 1 diabetes mellitus (T1DM), particularly regarding their susceptibility to dental caries. This study contributes to the current literature by systematically analyzing multiple oral health indicators—including salivary pH, gingival bleeding index, and plaque index—in conjunction with glycemic control parameters such as HbA1c, fasting blood glucose (FBG), and 2-hour postprandial blood glucose (2h PBG) in children with T1DM.
Our findings demonstrate that the incidence of dental caries in children with T1DM was significantly higher than in healthy controls, which is consistent with previous studies suggesting a positive correlation between poor glycemic control and increased caries risk.14,15 Notably, glycemic indices (HbA1c, FBG, and 2h PBG) were significantly elevated in the T1DM group, indicating persistent hyperglycemia. Chronic hyperglycemia may adversely affect tooth mineralization and salivary gland function, contributing to a higher caries risk. Specifically, disturbances in calcium and phosphate metabolism during tooth development can result in hypomineralized enamel with diminished acid resistance, thereby increasing susceptibility to demineralization by cariogenic bacteria.16,17
Although many studies support this association, some reports, such as those by Al-Badr et al and Pachoński et al have found no significant difference in caries prevalence between diabetic and non-diabetic children.18–20 These discrepancies may stem from population heterogeneity or the influence of confounding factors such as oral hygiene behaviors, dietary habits, and medication use. Nevertheless, our study carefully accounted for these factors, finding no significant intergroup differences in oral hygiene frequency or sugar intake, thereby strengthening the association between hyperglycemia and caries in our cohort.
From a mechanistic perspective, hyperglycemia may increase caries risk via several pathways. First, it impairs salivary gland function, leading to hyposalivation and reduced buffering capacity, which alters the acid-base equilibrium in the oral cavity and creates an environment favorable to bacterial acid production.21–25 Second, hyperglycemia disrupts enamel mineralization during critical periods of tooth development, resulting in structurally compromised enamel that is more susceptible to caries. Third, diabetic children may consume carbohydrate-rich foods or sugary beverages—sometimes as part of hypoglycemia management—which increases substrate availability for cariogenic microbes. Furthermore, diabetic conditions may impair periodontal tissue repair and immune function, facilitating gingival inflammation and enhancing bacterial pathogenicity.
Importantly, this study also revealed that gingival bleeding and plaque indices were significantly elevated in the T1DM group compared to controls, suggesting a higher prevalence of gingival inflammation. This may be attributed to diabetes-induced microvascular changes that reduce gingival tissue resilience and repair capacity. In addition, shifts in the oral microbiota—such as increased colonization by Streptococcus mutans and Lactobacillus—under hyperglycemic conditions could further exacerbate gingival inflammation and dental plaque accumulation.26,27
Another key finding of this study is the significantly higher stimulated salivary pH observed in diabetic children. While an acidic oral environment is typically associated with dental caries, elevated salivary pH—possibly due to dietary modifications, metabolic changes, or reduced salivary flow—may paradoxically increase the risk of gingival inflammation by promoting calculus formation and altering the composition of the oral microbiome.28,29 Although traditionally considered protective, a higher pH in the context of altered salivary composition may reflect impaired buffering rather than homeostatic balance. Therefore, monitoring salivary pH in diabetic patients could serve as a useful adjunct in oral health risk assessment.
Interestingly, no significant differences were observed in salivary sIgA or sIgG levels between the T1DM and control groups. This may be attributed to the limited sample size or inter-individual variability in mucosal immune response. While sIgA plays a central role in oral immunity and microbial homeostasis, the immunological alterations in pediatric diabetes are complex and may not be adequately captured by isolated measurements. Future studies with larger, well-characterized cohorts are warranted to explore the dynamic role of immunoglobulins and other immune mediators in modulating caries risk in diabetic populations.30
In summary, the present study reinforces the hypothesis that chronic hyperglycemia in children with T1DM contributes to both increased dental caries and periodontal disease risk through multifactorial mechanisms, including impaired enamel mineralization, altered salivary function, disrupted oral microbiota, and compromised immune defense. These findings underscore the necessity of integrated glycemic and oral health management strategies for children with diabetes. Early preventive interventions, regular dental assessments, and tailored oral hygiene education for diabetic children and their caregivers are essential to mitigate long-term oral health complications. Furthermore, this study provides a foundation for future multicenter, prospective studies aiming to develop precise, evidence-based preventive and therapeutic protocols.
Conclusion and Future Perspectives
This study demonstrates that children with type 1 diabetes mellitus (T1DM) exhibit significantly higher dental caries incidence (42.5% vs 15.0%, P<0.05), driven by chronic hyperglycemia-induced alterations in the oral environment—including pathological elevation of salivary pH (7.42 vs 6.89), periodontal inflammation, and impaired enamel mineralization. To translate these findings into clinical practice, we recommend: (1) mandatory oral assessments every 3 months for T1DM children, including salivary pH testing; (2) quarterly application of 1.23% acidulated phosphate fluoride (APF) gel for children with pH >7.2; and (3) establishment of joint diabetes-dental clinics coordinating HbA1c monitoring with periodontal evaluations. Future research should investigate molecular pathways linking hyperglycemia to enamel hypomineralization and conduct multicenter studies validating the proposed glycemic risk threshold (HbA1c >8.5%) for caries stratification.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li W, Huang E, Gao S. Type 1 diabetes mellitus and cognitive impairments: a systematic review. J Alzheimers Dis. 2017;57(1):29–36. doi:10.3233/JAD-161250
2. Pang H, Luo S, Xiao Y, et al. Emerging roles of exosomes in T1DM. Front Immunol. 2020;11:593348. doi:10.3389/fimmu.2020.593348
3. Lu X, Zhao C. Exercise and type 1 diabetes. Adv Exp Med Biol. 2020;1228:107–121.
4. Zhang J, Xiao Y, Hu J, Liu S, Zhou Z, Xie L. Lipid metabolism in type 1 diabetes mellitus: pathogenetic and therapeutic implications. Front Immunol. 2022;13:999108. doi:10.3389/fimmu.2022.999108
5. Reddy M, Gopalkrishna P. Type 1 diabetes and periodontal disease: a literature review. Can J Dent Hyg. 2022;56(1):22–30.
6. Kakleas K, Soldatou A, Karachaliou F, et al. Associated autoimmune diseases in children and adolescents with type 1 diabetes mellitus (T1DM). Autoimmun Rev. 2015;14(9):781–797. doi:10.1016/j.autrev.2015.05.002
7. Mathur VP, Dhillon JK. Dental caries: a disease which needs attention. Indian J Pediatr. 2018;85(3):202–206. doi:10.1007/s12098-017-2381-6
8. Balaji SM. Dental caries: research perspective. Indian J Dent Res. 2018;29(1):3. doi:10.4103/ijdr.IJDR_61_18
9. Muhammed Elamin S, Muhamad Arshad NF, Md Redzuan A, et al. Information needs on type 1 diabetes mellitus (T1DM) and its management in children and adolescents: a qualitative study. BMJ Open. 2024;14(4):e079606. doi:10.1136/bmjopen-2023-079606
10. Karavanaki K, Korona A, Karanasios S, et al. Predictors of the clinical severity of T1DM presentation at diagnosis in children and adolescents with type 1 diabetes mellitus (T1DM). Hormones. 2024;23(3):395–405. doi:10.1007/s42000-023-00518-7
11. Kutsch VK. Dental caries: an updated medical model of risk assessment. J Prosthet Dent. 2014;111(4):280–285. doi:10.1016/j.prosdent.2013.07.014
12. Bowen WH. Dental caries - not just holes in teeth! A perspective. Mol Oral Microbiol. 2016;31(3):228–233. doi:10.1111/omi.12132
13. Rai A, Sundas S, Dhakal N, et al. Assessment of dental caries based on ICDAS and WHO criteria: a comparative study. Int J Paediatr Dent. 2024;34(1):77–84. doi:10.1111/ipd.13099
14. Tatsiopoulou P, Porfyri G-N, Bonti E, et al. Priorities in the interdisciplinary approach of Specific Learning Disorders (SLD) in children with Type I Diabetes Mellitus (T1DM). From theory to practice. Brain Sci. 2020;11(1):4. doi:10.3390/brainsci11010004
15. Wang CH, Yen H-R, Lu W-L, et al. Adjuvant probiotics of Lactobacillus salivarius subsp. salicinius AP-32, L. johnsonii MH-68, and Bifidobacterium animalis subsp. lactis CP-9 attenuate glycemic levels and inflammatory cytokines in patients with type 1 diabetes mellitus. Front Endocrinol. 2022;13:754401. doi:10.3389/fendo.2022.754401
16. Kostopoulou E, Papachatzi E, Skiadopoulos S, et al. Seasonal variation and epidemiological parameters in children from Greece with type 1 diabetes mellitus (T1DM). Pediatr Res. 2021;89(3):574–578. doi:10.1038/s41390-020-0899-1
17. Al-Badr AH, AlJameel AH, Halawany HS, et al. Dental caries prevalence among Type 1 diabetes mellitus (T1DM) 6- to 12-year-old children in Riyadh, Kingdom of Saudi Arabia compared to non-diabetic children. Saudi Dent J. 2021;33(5):276–282. doi:10.1016/j.sdentj.2020.03.005
18. Pachoński M, Jarosz-Chobot P, Koczor-Rozmus A, et al. Dental caries and periodontal status in children with type 1 diabetes mellitus. Pediatr Endocrinol Diabetes Metab. 2020;26(1):39–44. doi:10.5114/pedm.2020.93249
19. Triebl Z, Bencze B, Bányai D, et al. Poor glycemic control impairs oral health in children with type 1 diabetes mellitus - a systematic review and meta-analysis. BMC Oral Health. 2024;24(1):748. doi:10.1186/s12903-024-04516-y
20. Mishra MB, Mishra S. Sugar-sweetened beverages: general and oral health hazards in children and adolescents. Int J Clin Pediatr Dent. 2011;4(2):119–123. doi:10.5005/jp-journals-10005-1094
21. Tan L, Zhong -M-M, Zhao Y-Q, et al. Type 1 diabetes, glycemic traits, and risk of dental caries: a Mendelian randomization study. Front Genet. 2023;14:1230113. doi:10.3389/fgene.2023.1230113
22. Manjushree R, Manjushree R, Shetty AK, et al. Evaluation of salivary components and dental plaque in relation to dental caries status in type 1 diabetes mellitus. Int J Clin Pediatr Dent. 2022;15(Suppl 2):S121–s125. doi:10.5005/jp-journals-10005-2325
23. Bimstein E, Zangen D, Abedrahim W, et al. Type 1 diabetes mellitus (Juvenile Diabetes)—a review for the pediatric oral health provider. J Clin Pediatr Dent. 2019;43(6):417–423. doi:10.17796/1053-4625-43.6.10
24. Sampaio N, Mello S, Alves C. Dental caries-associated risk factors and type 1 diabetes mellitus. Pediatr Endocrinol Diabetes Metab. 2011;17(3):152–157.
25. Lifshitz F, Casavalle PL, Bordoni N, et al. Oral health in children with obesity or diabetes mellitus. Pediatr Endocrinol Rev. 2016;14(2):159–167. doi:10.17458/PER.2016.LCB.Oralhealth
26. Bordoni NE, Salgado PA, Squassi AF. Comparison between indexes for diagnosis and guidance for treatment of dental caries. Acta Odontol Latinoam. 2021;34(3):289–297. doi:10.54589/aol.34/3/289
27. Zero DT. Dental caries process. Dent Clin North Am. 1999;43(4):635–664. doi:10.1016/S0011-8532(22)00818-7
28. Arevalo O, Miranda P, Gereige RS. Dental caries: early intervention and the role of the pediatrician. Pediatr Rev. 2023;44(6):301–310. doi:10.1542/pir.2022-005626
29. Gao X, Jiang S, Koh D, et al. Salivary biomarkers for dental caries. Periodontol. 2016;70(1):128–141. doi:10.1111/prd.12100
30. Winter GB. Epidemiology of dental caries. Arch Oral Biol. 1990;35 Suppl:1s–7s. doi:10.1016/0003-9969(90)90124-S
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.