Back to Journals » Patient Preference and Adherence » Volume 17
Relationship Between Symptom Burden and Self-Management Among Patients with Chronic Heart Failure: A Cross-Sectional Study
Authors Li J, Feng L, Shui X, Deng C, Hu A
Received 15 May 2023
Accepted for publication 1 August 2023
Published 7 August 2023 Volume 2023:17 Pages 1909—1921
DOI https://doi.org/10.2147/PPA.S419796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Qizhi (Cathy) Yao
JinLian Li,1,* LiQing Feng,1,* Xing Shui,1 Chengsong Deng,2 Ailing Hu3
1Department of Cardiac Care Unit, the Third Affiliated Hospital, SunYat-Sen University, Guangzhou, People’s Republic of China; 2Department of Neurology Medicine, Lingnan Hospital, the Third Affiliated Hospital, SunYat-Sen University, Guangzhou, People’s Republic of China; 3Department of Nursing, the Third Affiliated Hospital, SunYat-Sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ailing Hu, Department of Nursing, the Third Affiliated Hospital, SunYat-Sen University, Guangzhou, People’s Republic of China, Tel/Fax +86-13527658998, Email [email protected]
Background: Chronic heart failure (CHF) is a cardiovascular disease that seriously jeopardizes global human health. Studies indicate that good self-management can be effective in controlling disease symptoms. However, there is still insufficient evidence on the association between self-management and symptom burden among CHF patients. This study aimed to observe and assess the correlation of the self-management with the symptom burden and each dimension status in patients with CHF.
Methods: This was a cross-sectional study. Data were collected in-hospital using convenience sampling, and 128 patients with CHF were included. A general data questionnaire was used to collect demographic and disease-related data. The Memorial Symptom Assessment Scale-Heart Failure was used to measure patients’ symptom burdens. The Heart Failure Self-Management Scale was used to measure the self-management level of patients. The correlation between self-management and symptom burden was analyzed using the Spearman correlation.
Results: The total scores for symptom burden and self-management were 1.26 ± 0.49 and 49.97 ± 7.14, respectively. The total score of self-management was negatively correlated with that of symptom burden. The univariate linear regression analysis indicated that age, place of residence, smoking, residence status, New York Heart Association grade of cardiac function, and attitude toward the disease were risk factors for symptom burden. The multiple linear regression analysis indicated that the regression model with symptom burden as a dependent variable included three variables: drug management, symptom management, and attitude toward the disease.
Conclusion: Hospitalized patients with CHF had heavy overall symptom burdens, and their self-management levels were moderate to low. There was a negative correlation between the total self-management score and each dimension of symptom burden.
Keywords: chronic heart failure, symptom burden, self-management
Background
Heart failure (HF) is a complex syndrome characterized by insufficient cardiac pumping function to meet the metabolic demands of the body, resulting in organ hypoperfusion or pulmonary congestion, affecting the health and quality of life (QOL) of millions of people worldwide.1,2 The diagnosis of HF requires a comprehensive assessment of symptoms, signs, cardiac structural and functional abnormalities, and biomarker levels.3 HF can be divided into two types: acute and chronic. Chronic heart failure (CHF) is a persistent state of HF that may be stable, deteriorating, or decompensated.4 The European Society of Cardiology (ESC) released the latest guidelines on the diagnosis and treatment of acute and chronic HF in 2021,5 providing clinicians with evidence-based recommendations. HF has a significant impact on the QOL of patients, including physical, psychological, and social aspects.6 Many patients with HF value improving QOL as important as prolonging life, if not more.7 The QOL of CHF patients is influenced by many factors, among which the most important is symptom burden.8 Symptom burden refers to the degree of discomfort associated with the disease that patients experience over a certain period of time, including pain, dyspnea, edema, fatigue, etc.9 CHF patients have a high symptom burden, which seriously affects their daily activities and psychological state.10 Therefore, effectively assessing and managing the symptom burden of CHF patients is the key to improving their QOL.
Self-management refers to patients’ ability to reduce the impact of disease on their body through their own effective regulation behaviors in the process of coping with the disease by improving self-efficacy, monitoring disease symptoms, mastering disease self-management knowledge, and coping with the occurrence of disease-related symptoms.11,12 Health professionals have widely recognized the importance of self-management among patients with chronic diseases. In recent years, the self-management of patients with CHF has attracted increasing attention. Effective self-management can improve QOL and reduce the rate of rehospitalization among patients with CHF.13,14 This is supported by CHF clinics and rehabilitation programs in standard care.15,16 However, the self-management level of patients with CHF remains substandard.
The negative effects on the health status and QOL of patients with CHF can be directly attributed to their symptom burdens.17,18 According to the theory of symptom self-management, clinical practice can be influenced by optimizing symptom self-management.19 Previous studies on the correlation between self-management and symptom burden have focused largely on patients with chronic obstructive pulmonary disease and hemodialysis.20,21 These studies revealed a negative correlation between self-management and symptom burden; that is, most patients with CHF have heavy symptom burdens and poor self-management.22,23 Good self-management can effectively control disease symptoms. However, there are few reports on the relationship between self-management and symptom burden among patients with CHF.
Therefore, this study aimed to 1) investigate the current status of the symptom burden of hospitalized patients with CHF in China using a questionnaire survey, 2) analyze the influencing factors, and 3) explore the correlation between self-management and symptom burden. The results of this study may provide a scientific basis for clinical nursing practice and interventional research.
Materials and Methods
Research Design and Participants
This cross-sectional study was conducted at XXX Hospital in Guangzhou, China. Patients with CHF in the cardiovascular department and cardiac care unit (CCU) between December 2021 and June 2022 were recruited using a convenience sampling method.
Inclusion criteria were (1) having met the Chinese diagnostic criteria for heart failure issued by the Chinese Medical Association in 2018, which included (i) increased natriuretic peptide, (ii) at least one of the following conditions being observed: left ventricular hypertrophy and/or left atrial enlargement and abnormal diastolic function, and (iii) clinical diagnosis of CHF, (2) having been assigned New York Heart Association (NYHA) class II or above, (3) have a disease duration ≥ 3 months, (4) absence of cognitive dysfunction and ability to complete the questionnaire independently or with the help of investigators or family members, (5) being ≥ 18 years of age, and (6) providing informed consent to participate in the study. Participants with malignant tumors, severe organ (liver, kidney, brain, and lung) failure, previous or current mental illness, or currently pregnant were excluded.
This study was approved by the Ethics Committee of The Third Affiliated Hospital, Sun Yat-sen University ([2022]02–020-01). The research conforms to the provisions of the Declaration of Helsinki as revised in Edinburgh in 2000. Informed consent was obtained from all participants.
Data Collection
The data were collected using a questionnaire. Questionnaires with ≥ 20% missing data were excluded. A self-designed general information questionnaire (including sociodemographic and disease-related data) was used to obtain basic information about the patient. Symptom status of patients was measured using the Chinese version of the Memorial Symptom Assessment Scale-Heart Failure (MSAS-HF),24 and the Heart Failure Self-Management Scale compiled by Shi et al.25
The general information questionnaire was designed by the researchers and included sociodemographic and disease-related data. Sociodemographic data included sex, age, education level, smoking, drinking, occupation, body mass index (BMI), marital status, ethnic group, family per capita monthly income, living status, living alone or with others, medical expense payment method, and patients’ attitude toward the disease. Disease-related data included NYHA classification of cardiac function, type of medication, left ventricular ejection fraction (LVEF), course of the disease, comorbidities, number of hospitalizations within six months, B-type natriuretic peptide (BNP) precursor, serum potassium, serum sodium, C-reactive protein, and serum prealbumin.
The Chinese version of MSAS-HF comprises 32 items: 21 physical symptoms, five heart failure symptoms, and six psychological symptoms, to assess the patient’s experience of symptoms in the past seven days, including the prevalence, frequency, severity, and distress of symptoms. They are asked to report the frequency rated on a scale from 1 to 4 (rarely to almost constantly) if the symptom is present, severity rated on a scale from 1 to 4 (mild to very severe), and distress rated on a scale from 0 to 4 (not at all to very severe). Lower numbers indicate less distress, frequency, and severity. Symptom burden scores are determined by the mean of the distress, frequency, and severity of each symptom. The total symptom burden score is the overall mean for all symptoms. Cronbach’s α coefficients for the subscales of heart failure symptoms, psychological symptoms, and physical symptoms, and the total scale were 0.807, 0.898, 0.925, and 0.946, respectively. A confirmatory factor analysis of the three symptom dimensions revealed the following fit indices: goodness of fit index (GFI) = 0.82, comparative fit index (CFI) = 0.87, and normed fit index (NFI) = 0.79. This indicated that the model-fitting effect of the scale was good.19 Cronbach’s α coefficient of the scale was 0.766 for 128 patients with CHF.
The Heart Failure Self-Management Scale was rated on a four-point Likert scale (1 = never; 4 = always). The scale includes 20 items in four dimensions: diet, symptom, social-psychological adjustment, and drug management. The minimum and maximum scores of the scale are 20 and 80, respectively, with higher scores indicating better self-management. The standardized score rate was used to divide the self-management level (score rate = actual score/highest score × 100%), and patients’ self-management level was divided into high, medium, and low, with score rates of ≥ 80%, 60%-79%, and < 60%, respectively. The mean content validity ratio (CVR) of the scale was 0.98, Cronbach’s α coefficient of the internal consistency reliability was 0.78, and the one-week test-retest reliability was 0.83.20 Cronbach’s α coefficient of the scale was 0.773 for 128 patients with CHF.
Statistical Analyses
Bedside real-time ultrasound examination was performed on the patients using the GE Vivid T8 color Doppler ultrasound diagnostic device according to the requirements of the “Technical Specifications for Clinical Application of Critical Ultrasound”.26 All image acquisition was performed by ultrasound physicians with more than 5 years of work experience. The patients were in the left lateral position, and the left ventricular ejection fraction (LVEF), early diastolic peak velocity of mitral valve (E), late diastolic peak velocity of mitral valve (A), early diastolic peak velocity of mitral annulus (e′) and other indicators were measured. The left ventricular ejection fraction (LVEF) was calculated using the biplane Simpson method, and the E/A ratio and E/e´ ratio were used as indicators to evaluate the left ventricular diastolic function. E/A<0.8 or E/e’>14 indicated left ventricular diastolic dysfunction.27
SPSS 25.0 was used for the statistical analyses, and a two-sided test was used for statistical inference. Statistical significance was set at p < 0.05. The mean ± standard deviation, median, and interquartile range were used to describe age, BMI, BNP precursor, serum potassium, serum sodium, serum prealbumin value, left ventricular ejection fraction (LVEF), course of disease, number of symptoms, symptom burden score, and self-management score. Frequencies and percentages were used to describe sex, smoking, drinking, family per capita income, highest education, living situation, marital status, occupation, medical treatment charge of payment, place of residence, cardiac function, type of medicine, combined diseases, patient attitude toward the disease, C-reactive protein normal or not, and the number of hospitalizations within six months. Univariate analyses, including a t-test, analysis of variance, and rank-sum test, were used to explore the differences in symptom burden among patients with different demographic and disease-related characteristics. The least significant difference (LSD) method was used for pairwise comparisons of three or more groups. The Kolmogorov–Smirnov test was used to check the normal distribution of continuous data. A Spearman rank correlation was used to analyze the correlation between self-management and symptom burden in patients. A multiple linear regression analysis was used to analyze the potential influencing factors of symptom burden in patients, with the general data and scores of self-management dimensions as independent variables and the total score of patients’ symptom burdens and scores of each dimension as dependent variables.
Results
A total of 136 questionnaires were distributed, and 135 questionnaires were collected, with a recovery rate of 99.26%. Among the 135 questionnaires, seven were invalid (five missing survey items and two missing test results), and 128 were valid, with a validity rate of 94.81%.
Characteristics
Among the patients, 40.6% were women, and 59.4% were men. The average age was 68.19 ± 15.51 years (range: 30–92 years), and the majority of the patients were over 60 years old (69.5%). All patients were Han Chinese, and 76.6% were married. Of the patients, 66.4% had never consumed alcohol, and 58.6% had never smoked. Occupation was mainly retired (61.5%), and the per capita monthly household income was mostly more than 8000 yuan/month (42.2%). A total of 47.7% of the patients paid for treatment using medical insurance. Most patients had a primary school education or below and a junior high school education, accounting for 39% and 30.5%, respectively. Most of the patients (75.0%) lived in provincial capital cities. Few patients (8.6%) lived alone. Most patients (55.5%) had an optimistic attitude toward the disease. The detailed results are listed in Table S1.
Of the 128 patients, 54 (42.2%) had an LVEF ≤40%, 19 (14.8%) had an LVEF between 40 and 50, as well as 55 (43%) had an LVEF ≥50. In addition, 95 of the 128 patients had reduced LV diastolic function. The heart function grade of NYHA was mainly III (45.3%). A total of 53.1% of the patients had a disease duration of >5 years. Most patients (53.9%) had two or more diseases. A total of 46.1% of patients had EF values above 50%. The number of hospitalizations within six months was mainly once (58.6%). Most patients (56.2%) had abnormal C-reactive levels. Of the patients, 85.9% had normal serum potassium levels, and 69.5% had normal serum sodium levels. Most of the patients (68%) had abnormal serum prealbumin levels. The detailed results are presented in Table S2.
Symptom Burden of Patients
The incidence of the 32 symptoms ranged from 12.5% to 89.84%, and 16 of them were more than 50%. The top five incidences were shortness of breath (89.84%), difficulty sleeping (82.81%), lack of energy (75.78%), difficulty breathing when lying flat (75.78%), and dry mouth (71.88%) (Figure 1A). The total number of symptoms ranged from 3 to 30, with an average of 15.14 ± 4.85 and a median of 14.5. The number of physical symptoms was at least 2, at most 20, with a median of 9. The number of psychological symptoms was at least 0, at most 6, with a median of 4. The number of heart failure symptoms was at least 0, at most 5, with a median of 3.
 |
Figure 1 (A) Frequency of patient symptom burden. (B) Proportion of patients with a symptom burden of ≥3 points (ranging from moderately severe to very severe) for symptom severity. (C) Proportion of patients with symptom burden with a symptom distress score of ≥3 (ranging from quite a bit to very much). |
The total symptom burden score was 1.26 ± 0.49. The score for psychological symptoms was 1.37 ± 0.71, for heart failure symptoms was 1.35 ± 0.79, and for physical symptoms was 1.07 ± 0.42 (Table 1). Among those symptoms, the most severe (ranging from moderately severe to very severe) were shortness of breath (57.81%), difficulty sleeping (57.03%), difficulty breathing when lying flat (50.78%), waking up breathless (41.41%), lack of energy (39.84%) and lack of appetite (35.94%). The top six most distressing (ranging from quite a bit to very much) symptoms were the same as the six listed above (Figures 1B and C).
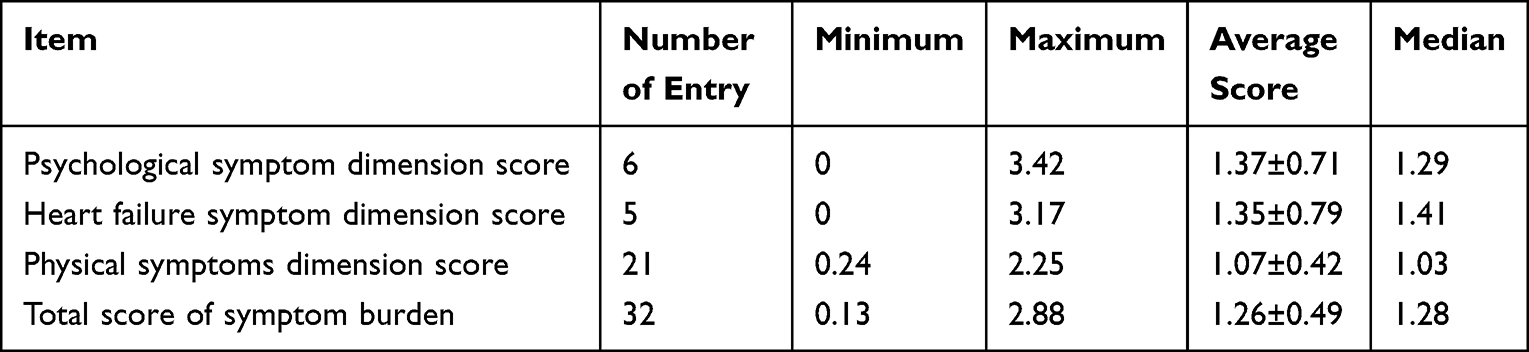 |
Table 1 Total Score of Symptom Burden and Scores of Each Dimension of the Study Subjects (n=128) |
Self-Management Level of Patients
The total self-management was 49.97 ± 7.14, the score rate was (50.17 ± 12.48)%, and the median value was 61.25%. The score rate of the drug management dimension was the highest (69.06 ± 14.85)%, and the symptom management dimension was the lowest (50.17 ± 12.48%; Table 2). Among the self-management level of patients, the high level accounted for 5.5%, the moderate level accounted for 53.1%, and the low level accounted for 41.4%. The scores of drug management, diet management, and social-psychological adjustment management were mainly at a moderate level, while most patients (75%) were at a low level in the symptom management dimension (Table 3).
 |
Table 2 The Total Score of Self-Management, and the Score and Score Rate of Each Dimension of the Subjects (n=128) |
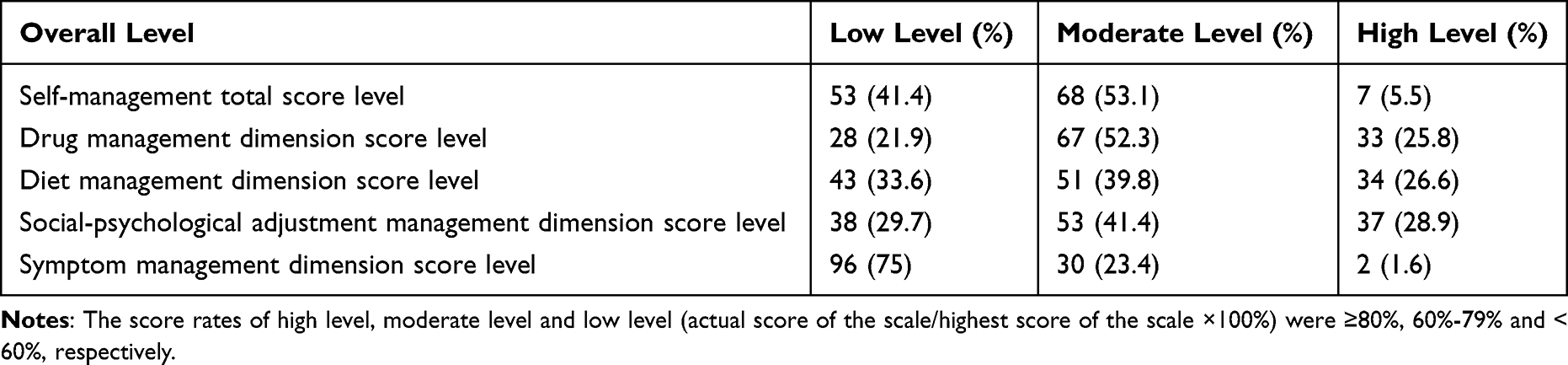 |
Table 3 The Level of Self-Management Behavior of the Subjects (n=128) |
Influencing Factors of Symptom Burden
Univariate analysis revealed that age, place of residence, smoking, living situation, heart function grade of NYHA, and patients’ attitude toward the disease were significantly associated with symptom burden (Table 4). In addition, the total self-management score was negatively correlated with the total symptom burden score (r = −0.381, p < 0.01; Table 5, Figure 2).
 |
Table 4 Univariate Analysis of Total Score of Symptom Burden, Symptom Burden Dimension Score, Physical Symptom Burden Dimension Score, Psychological Symptom Burden Dimension Score in Patients with Chronic Heart Failure (n=128) |
 |
Table 5 Correlation Analysis Between Self-Management and Symptom Burden (n=128) |
 |
Figure 2 Association of total self-management score with total symptom burden score. |
Furthermore, a multiple linear regression model was constructed with symptom burden and each dimension score as the dependent variables, and the significant influencing factors obtained from univariate analysis, including age, place of residence, smoking, living situation, heart function grade of NYHA, patients’ attitude toward the disease, drug management, symptom management, and social-psychological adjustment management as the independent variables. A multivariate analysis of the symptom burden total scores revealed that both symptom management and drug management negatively affected the total scores (p = 0.005, p = 0.014, respectively). The symptom burden of patients with negative and extremely pessimistic attitudes toward the disease was significantly higher than that of optimistic patients (p = 0.002, p < 0.001, respectively). Multivariate analysis of the physical symptom burden dimension score demonstrated that symptom management and social-psychological adjustment negatively affected the physical symptom burden dimension (p < 0.001). Multivariate analysis of psychological symptom burden dimension scores indicated that social-psychological adjustment management negatively affected the physical symptom burden dimension (p < 0.001). Symptom burden was significantly higher among patients who had a very negative attitude toward the disease than those who had a positive attitude (p < 0.001; Table 6).
 |
Table 6 Multivariate Analysis of Total Score of Symptom Burden, Symptom Burden Dimension Score, Physical Symptom Burden Dimension Score, Psychological Symptom Burden Dimension Score in Patients with Chronic Heart Failure (n=128) |
Discussion
HF is a global public health challenge, a common clinical syndrome caused by abnormal cardiac structure or function.15 The management of HF patients is very complex, and even in clinically stable conditions, they often suffer from symptoms such as dyspnea, depression, fatigue and cognitive impairment, which affect their quality of life.28 These symptom burden also limit the social participation and interpersonal interaction of HF patients, making it difficult for them to maintain normal social roles and relationships.29 Self-management is an effective strategy to improve the prognosis of chronic diseases, and an important component of the treatment of chronic disease patients.30 A growing body of evidence suggests that good self-management can effectively control disease symptoms.20,21 However, there is currently a lack of evidence on the relationship between self-management and symptom burden among patients with CHF. This study examined the associations between each dimension of self-management and the various symptom burden domains in hospitalized patients with CHF, and this may be helpful for clinical practice. There are two major findings of this study: 1) Both symptom management and drug management negatively affected the total and dimension scores of the symptom burden; 2) The regression model showed that symptom management, drug management, and patients’ attitudes toward the disease explained 31.1% of the variance in symptom burden among hospitalized patients with CHF.
Among the 128 hospitalized patients with CHF, 40.6% were women and 59.4% were men, which was in line with the epidemiological distribution of CHF. The lower proportion of female patients may be attributed to the cardiovascular protective effect of estrogen.31 Conversely, women had a relatively healthy lifestyle and focused more on the prevention of heart failure.32 The incidence and prevalence of CHF rose with age, and it could rise by 80 times from 10 years old to 60 years old.33 Although 50% of HF patients were aged over 75 years, most clinical trials included younger patients with a mean age of 61 years.34 This concurred with our study, which had a mean age of above 60 years (69.5%) for the patients, which might be due to the progressive decline of cardiovascular compensatory capacity, the impairment of cardiac pumping function, the enhancement of myocardial and arterial stiffness, and the elevation of cardiac load in elderly patients.35,36 The majority of patients had a disease duration of more than five years (53.1%), and only 28.9% of patients had a disease duration of less than one year, which reflected that CHF is a chronic progressive disease with a long course. Moreover, we found that 68% of hospitalized patients had serum albumin levels below the normal range. Since serum albumin is an indicator of nutritional status,37 this suggests that these patients are at risk of malnutrition. We speculate that this may be related to gastrointestinal congestion caused by CHF, which affects the patients’ appetite and intestinal absorption function. However, this hypothesis still needs further experimental verification.
This study revealed that patients with CHF had heavy overall symptom burdens, and the dimension of heart failure symptom burden had the highest score. The total symptom burden score was 1.26 ± 0.49, and the mean number of total symptoms was 15.14±4.85, which was higher than those reported by previous studies on CHF by Haedtke et al (13.6±6.8) and Lin et al (9.1±5.9).8,38 The subjects included in this study were all hospitalized, the majority were in NYHA class III (45.3%) or IV (33.6%), a total of 53.1% of the patients had a disease duration of >5 years, and most of them had acute exacerbation of CHF, which may explain the heavy overall symptom burdens. Bennett et al also reported that patients with heart failure have difficulties recognizing the symptoms of heart failure, which leads to a delay in seeking medical treatment and mistaken diagnoses of other diseases, causing aggravation of heart failure.39 The top five symptoms with the highest severity scores and distress scores were shortness of breath, difficulty sleeping, difficulty breathing when lying flat, waking up breathless, and lack of energy. This result is slightly different from those reported in previous studies,40 which might be associated with decreased cardiac output, systemic and pulmonary circulation congestion, and decreased cardiopulmonary endurance in patients with CHF. This result suggests that we should strengthen the management of these symptoms in hospitalized patients with CHF.
The total self-management score was 49.97 ± 7.14, which was in line with Chew et al.41 The overall self-management level of most patients remained medium or low. Among the self-management dimensions, drug management, diet management, and social-psychological adjustment management were at a moderate level, and symptom management was at a low level. Drug therapy is a common treatment for CHF.42,43 Standardized drug therapy can improve patients’ heart function and heart failure symptoms and reduce the number of hospitalizations, thereby improving patient QOL and reducing symptom burden.44 The present study had a drug management dimension score of 13.81 ± 2.97 (score rate median: 70.00%), which was a moderate level. Clinically, it is necessary to optimize drug treatment plans, reduce drug types, and strengthen drug education and guidance for patients and their families. Among the self-management dimensions, the symptom management dimension had the lowest score, at a low level. This may be due to the lack of attention of patients in recording urine volume, weighing, water restriction, and edema monitoring. In addition, the patients were less alert and more sensitive to symptoms of heart failure. Kobayashi et al revealed that only 57.4% of patients knew how to self-assess heart failure symptoms.45 In our study, only 3.1% of the patients monitored their weight daily, and 43.7% knew how to self-assess heart failure symptoms. These findings have significant implications for the tertiary prevention of CHF patients, which refers to the prevention of complications and deterioration of the disease after diagnosis and treatment. Tertiary prevention aims to improve the quality of life, functional status, and survival of patients with chronic diseases, such as CHF and glaucoma.46,47 Therefore, it is necessary to implement various forms of health education to strengthen the knowledge of symptom management in patients with CHF.
As a predictor of QOL and hospitalization, symptom burden is a significant outcome of interest for evaluating the effectiveness of self-care interventions in CHF patients.48 In this study, a correlation analysis of self-management and symptom burden revealed a negative correlation between the total score of self-management and each dimension of symptom burden. The lower the level of self-management, the higher the burden of psychological symptoms, heart failure symptoms, and physical symptoms, which ultimately affects the total symptom burden of patients. This finding is inconsistent with the evidence that patient self-management is linked to reduced mortality risk and fewer hospital admissions in CHF patients.49 Similarly, Bringsvor et al recently reported a negative correlation between self-management and symptom burden in patients with chronic obstructive pulmonary disease.20 Weiss et al and Saleh et al also reported significant improvements in symptom burden following implementation of a self-management intervention.50,51 Moreover, the multivariate analysis showed that better drug and symptom management indicated a lower symptom burden score. This result suggests that we should strengthen drug management and symptom management in order to reduce the symptom burden of hospitalized patients with CHF. In addition, patients with an optimistic attitude toward diseases had a lower overall symptom burden score than patients with a negative attitude toward the disease. We know that personal coping styles play an important role in maintaining a person’s physical and mental health.52 Patients with a negative attitude toward the disease are prone to anxiety, irritability, sadness, and other pessimistic emotions.53 They are also more sensitive to the stimulation of negative events and are more likely to produce physical symptoms in the body.54 Patients with an optimistic attitude toward the disease generally adopt a positive coping style when they encounter stressful events.55 Besides, after hospitalization, social support from family and close ones is crucial for CHF patients to obtain psychological comfort and face their condition positively.56 Taken together, increasing the symptom management and drug management ability in self-management can reduce the level of symptom burden of hospitalized patients with CHF. Therefore, it is necessary to implement various forms of health education to strengthen the knowledge of symptom management and drug management in patients with CHF.
Limitations
This study has some limitations. First, convenience sampling was conducted in only one hospital, and the sample size was relatively small, which limited the promotion of the research results. Second, this was a cross-sectional study, which only investigated the symptom burden of patients one week before hospitalization. However, the symptom burden and self-management of patients with CHF changed over time, and there were differences between the different periods. Therefore, future studies should expand the sample size and investigate the correlation between self-management and symptom burden in patients with CHF in different regions and levels of hospitals. Furthermore, a longitudinal study should be conducted to explore the level of self-management and symptom burden in patients and to analyze the changes in self-management and symptom burden in different periods. Third, this study lacked direct measurements of cardiac output, intestinal congestion or absorption, which were mentioned as possible factors affecting the nutritional status of patients with CHF. These measurements could provide more evidence to support or refute our hypothesis. Therefore, future studies should also include these measurements to verify the relationship between CHF, gastrointestinal congestion, intestinal absorption and nutritional status.
Conclusions
In conclusion, hospitalized patients with CHF had heavy overall symptom burdens, and their self-management level was moderate to low. In addition, there was a negative correlation between the total self-management score and each dimension of symptom burden. Better drug and symptom management were associated with lower symptom burden scores. Therefore, clinical staff should provide individualized and comprehensive interventions and education for CHF patients according to their different symptoms and self-management levels, in order to improve their quality of life and prognosis.
Highlights
1. Patients with CHF had heavy overall symptom burdens, and the dimension of heart failure symptom burden had the highest score.
2. Patients’ self-management levels were moderate to low.
3. Better drug and symptom management indicated a lower symptom burden score.
Acknowledgment
JinLian Li and LiQing Feng are co-first authors for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gupta AK, Tomasoni D, Sidhu K, Metra M, Ezekowitz JA. Evidence-based management of acute heart failure. Canadian J Cardiol. 2021;37(4):621–631. doi:10.1016/j.cjca.2021.01.002
2. Lin X, Fang L. Pharmaceutical treatment for heart failure. Coronary Artery Dis. 2020;269–295. doi:10.1007/978-981-15-2517-9_7
3. Núñez J, de la Espriella R, Rossignol P, et al. Congestion in heart failure: a circulating biomarker‐based perspective. A review from the Biomarkers Working Group of the Heart Failure Association, European Society of Cardiology. Eur J Heart Fail. 2022;24(10):1751–1766. doi:10.1002/ejhf.2664
4. Wang X, Zhang C, Cardiovascular Group GB, et al.; Chinese Medical Association. Chinese expert consensus on the diagnosis and treatment of chronic heart failure in elderly patients (2021). Aging Med. 2022;5(2):78–93. doi:10.1002/agm2.12215
5. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
6. Alharbi M, Alharbi F, AlTuwayjiri A, et al. Assessment of health-related quality of life in patients with heart failure: a cross-sectional study in Saudi Arabia. Health Qual Life Outcomes. 2022;20(1):1–7. doi:10.1186/s12955-022-02040-7
7. Lewis EF, Johnson PA, Johnson W, Collins C, Griffin L, Stevenson LW. Preferences for quality of life or survival expressed by patients with heart failure. J Heart Lung Transplant. 2001;20(9):1016–1024. doi:10.1016/s1053-2498(01)00298-4
8. Haedtke CA, Moser DK, Pressler SJ, Chung ML, Wingate S, Goodlin SJ. Influence of depression and gender on symptom burden among patients with advanced heart failure: insight from the pain assessment, incidence and nature in heart failure study. Heart Lung. 2019;48(3):201–207. doi:10.1016/j.hrtlng.2019.02.002
9. Gill A, Chakraborty A, Selby D. What is symptom burden: a qualitative exploration of patient definitions. J Palliat Care. 2012;28(2):83–89. doi:10.1177/104990910001700408
10. Jaarsma T, Hill L, Bayes‐Genis A, et al. Self-care of heart failure patients: practical management recommendations from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2021;23(1):157–174. doi:10.1002/ejhf.2008
11. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7. doi:10.1207/S15324796ABM2601_01
12. Schumacher C, Hussey L, Hall V. Heart failure self-management and normalizing symptoms: an exploration of decision making in the community. Heart Lung. 2018;47(4):297–303. doi:10.1016/j.hrtlng.2018.03.013
13. Otsu H, Moriyama M. Effectiveness of an educational self-management program for outpatients with chronic heart failure. Jpn J Nurs Sci. 2011;8(2):140–152. doi:10.1111/j.1742-7924.2010.00166.x
14. Zhao Q, Chen C, Zhang J, Ye Y, Fan X. Effects of self-management interventions on heart failure: systematic review and meta-analysis of randomized controlled trials. Int J Nurs Stud. 2020;110:103689. doi:10.1016/j.ijnurstu.2020.103689
15. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18(8):891–975. doi:10.1002/ejhf.592
16. Atherton JJ, Sindone A, De Pasquale CG, et al. National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand: guidelines for the Prevention, Detection, and Management of Heart Failure in Australia 2018. Heart Lung Circ. 2018;27(10):1123–1208. doi:10.1016/j.hlc.2018.06.1042
17. Alpert CM, Smith MA, Hummel SL, Hummel EK. Symptom burden in heart failure: assessment, impact on outcomes, and management. Heart Fail Rev. 2017;22(1):25–39. doi:10.1007/s10741-016-9581-4
18. Baik D, Reading M, Jia H, Grossman LV, Masterson Creber R. Measuring health status and symptom burden using a web-based mHealth application in patients with heart failure. Eur J Cardiovasc Nurs. 2019;18(4):325–331. doi:10.1177/1474515119825704
19. Hoffman AJ. Enhancing self-efficacy for optimized patient outcomes through the theory of symptom self-management. Cancer Nurs. 2013;36(1):E16–26. doi:10.1097/NCC.0b013e31824a730a
20. Bringsvor HB, Skaug K, Langeland E, et al. Symptom burden and self-management in persons with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2018;13:365–373. doi:10.2147/COPD.S151428
21. Yufang Z, Raoping W, Xiaoying Z, Xiaoqing Y. Correlations and status of self-management level and quality of life in patients undergoing maintenance hemodialysis. Modern Clin Nursing. 2015;14(08):1–4.
22. Li DF, Yin DR, Huang WL, et al. Investigation of self-management behaviors and its influencing factors in elderly patients with Chronic Heart Failure. Chine Nursing Manage. 2020;20(03):360–366.
23. Hu Y, Jiang J, Xu L, et al. Symptom clusters and quality of life among patients with chronic heart failure: a cross-sectional study. Jpn J Nurs Sci. 2021;18(1):e12366.
24. Guo JY, Lv R, Zhang J, Wu XY, Ji SM, L Z. Reliability and validity of the Chinese version of Memorial Symptom Assessment Scale-Heart Failure. Chine J Nursing. 2014;49(12):1448–1452.
25. Xiaoqing S, Weixin C, Beiwen W, Xiaofang Y, Minxia L, Jie G. Preliminary construction of self-management scale of heart failure patients. Chine Nursing Res. 2012;26(35):3347–3350.
26. Yin WH, Wang XT, et al. Technical specification for clinical application of critical ultrasonography. Chin J Intern Med. 2018;57(6):397–417.
27. Nagueh Sherif F, Smiseth Otto A, Appleton Christopher P, et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: an Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2014;17(12):1321–1360. doi:10.1093/ehjci/jew082
28. Pressler SJ, Gradus-Pizlo I, Chubinski SD, et al. Family caregivers of patients with heart failure: a longitudinal study. J Cardiovasc Nurs. 2013;28(5):417–428. doi:10.1097/JCN.0b013e3182563877
29. Olano-Lizarraga M, Wallström S, Martín-Martín J, Wolf A. Interventions on the social dimension of people with chronic heart failure: a systematic review of randomized controlled trials. Eur J Cardiovasc Nurs. 2023;22(2):113–125. doi:10.1093/eurjcn/zvac051
30. Lin CC, Hwang SJ. Patient-Centered Self-Management in Patients with Chronic Kidney Disease: challenges and Implications. Int J Environ Res Public Health. 2020;17(24). doi:10.3390/ijerph17249443
31. Iorga A, Cunningham CM, Moazeni S, Ruffenach G, Umar S, Eghbali M. The protective role of estrogen and estrogen receptors in cardiovascular disease and the controversial use of estrogen therapy. Biol Sex Differ. 2017;8(1):33. doi:10.1186/s13293-017-0152-8
32. Meyer S, Brouwers FP, Voors AA, et al. Sex differences in new-onset heart failure. Clin Res Cardiol. 2015;104(4):342–350. doi:10.1007/s00392-014-0788-x
33. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93–e621. doi:10.1161/CIR.0000000000001123
34. Azad N, Lemay G. Management of chronic heart failure in the older population. J Geriatr Cardiol. 2014;11(4):329–337. doi:10.11909/j.issn.1671-5411.2014.04.008
35. Semba RD, Sun K, Schwartz AV, et al. Serum carboxymethyl-lysine, an advanced glycation end product, is associated with arterial stiffness in older adults. J Hypertens. 2015;33(4):797–803. doi:10.1097/HJH.0000000000000460
36. Grau M, Barr RG, Lima JA, et al. Percent emphysema and right ventricular structure and function: the Multi-Ethnic Study of Atherosclerosis-Lung and Multi-Ethnic Study of Atherosclerosis-Right Ventricle Studies. Chest. 2013;144(1):136–144. doi:10.1378/chest.12-1779
37. Phelan PJ, O’Kelly P, Walshe JJ, Conlon PJ. The importance of serum albumin and phosphorous as predictors of mortality in ESRD patients. Ren Fail. 2008;30(4):423–429. doi:10.1080/08860220801964236
38. Lin CY, Miller JL, Lennie TA, et al. Perceived Control Predicts Symptom Status in Patients With Heart Failure. J Cardiovasc Nurs. 2020;35(6):530–537. doi:10.1097/JCN.0000000000000684
39. Bennett SJ, Cordes DK, Westmoreland G, Castro R, Donnelly E. Self-care strategies for symptom management in patients with chronic heart failure. Nurs Res. 2000;49(3):139–145. doi:10.1097/00006199-200005000-00004
40. Tantoy IY, Dhruva A, Cataldo J, et al. Differences in symptom occurrence, severity, and distress ratings between patients with gastrointestinal cancers who received chemotherapy alone or chemotherapy with targeted therapy. J Gastrointest Oncol. 2017;8(1):109–126. doi:10.21037/jgo.2017.01.09
41. Chew HSJ, Sim KLD, Choi KC, Chair SY. Effectiveness of a nurse-led temporal self-regulation theory-based program on heart failure self-care: a randomized controlled trial. Int J Nurs Stud. 2021;115:103872. doi:10.1016/j.ijnurstu.2021.103872
42. McKenzie DB, Cowley AJ. Drug therapy in chronic heart failure. Postgrad Med J. 2003;79(937):634–642. doi:10.1136/pmj.79.937.634
43. Greene SJ, Butler J, Albert NM, et al. Medical Therapy for Heart Failure With Reduced Ejection Fraction: the CHAMP-HF Registry. J Am Coll Cardiol. 2018;72(4):351–366. doi:10.1016/j.jacc.2018.04.070
44. Berliner D, Bauersachs J. Current Drug Therapy in Chronic Heart Failure: the New Guidelines of the European Society of Cardiology (ESC). Korean Circ J. 2017;47(5):543–554. doi:10.1016/j.jacc.2018.04.070
45. Kobayashi M, Wilcke C, Girerd N. Assessment of Patient Knowledge, Awareness, and Adherence in Heart Failure in a Real-Life Setting: insights from Data Acquired in Pharmacies. J Clin Med. 2022;11(3):863. doi:10.3390/jcm11030863
46. Munteanu GZ, Munteanu ZVI, Roiu G, et al. Aspects of Tertiary Prevention in Patients with Primary Open Angle Glaucoma. J Pers Med. 2021;11(9). doi:10.3390/jpm11090830
47. Unverzagt S, Klement A, Meyer G, Prondzinsky R. Interventions to enhance adherence to guideline recommendations in secondary and tertiary prevention of heart failure: a systematic review. J Clin Trials. 2014;4(192):2167–0870.1000192.
48. Heo S, Doering LV, Widener J, Moser DK. Predictors and effect of physical symptom status on health-related quality of life in patients with heart failure. Am J Crit Care. 2008;17(2):124–132. doi:10.1164/rccm.200612-1901OC
49. Toukhsati SR, Driscoll A, Hare DL. Patient self-management in chronic heart failure–establishing concordance between guidelines and practice. Cardiac Failure Rev. 2015;1(2):128. doi:10.15420/cfr.2015.1.2.128
50. Weiss DJ, Robertson S, Goebel JR. Pilot Implementation of a Low-Literacy Zone Tool for Heart Failure Self-management. J Hosp Palliat Nurs. 2019;21(6):475–481. doi:10.1097/NJH.0000000000000597
51. Saleh ZT, Elshatarat RA, Elhefnawy KA, et al. Effect of a Home-Based Mobile Health App Intervention on Physical Activity Levels in Patients With Heart Failure: a Randomized Controlled Trial. J Cardiovasc Nurs. 2023;38(2):128–139. doi:10.1097/JCN.0000000000000911
52. Yu H, Li M, Li Z, et al. Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry. 2020;20(1):426. doi:10.1186/s12888-020-02826-3
53. Spence MJ, Moss-Morris R. The cognitive behavioural model of irritable bowel syndrome: a prospective investigation of patients with gastroenteritis. Gut. 2007;56(8):1066–1071. doi:10.1136/gut.2006.108811
54. Overgaauw PA, Vinke CM, van Hagen MA, Lipman LJ. A one health perspective on the human–companion animal relationship with emphasis on zoonotic aspects. Int J Environ Res Public Health. 2020;17(11):3789. doi:10.3390/ijerph17113789
55. Dongmei L. Influence of the youth’s psychological capital on social anxiety during the covid-19 pandemic outbreak: the mediating role of coping style. Iran J Public Health. 2020;49(11):2060. doi:10.18502/ijph.v49i11.4721
56. Mekeres GM, Buhaș CL, Csep AN, et al. The Importance of Psychometric and Physical Scales for the Evaluation of the Consequences of Scars-A Literature Review. Clin Pract. 2023;13(2):372–383. doi:10.3390/clinpract13020034
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.