Back to Journals » Psychology Research and Behavior Management » Volume 16
Relationship Between Severity of Gastrointestinal Symptoms and Anxiety Symptoms in Patients with Chronic Gastrointestinal Disease: The Mediating Role of Illness Perception
Authors Wang Z, Lu Y, Li L, Wu X, Liu J, Tang J, Wang W ![]() , Lu L
, Lu L
Received 5 July 2023
Accepted for publication 26 November 2023
Published 5 December 2023 Volume 2023:16 Pages 4921—4933
DOI https://doi.org/10.2147/PRBM.S429132
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Zixuan Wang,1 Yuanchen Lu,1 Li Li,2 Xiaoting Wu,2 Junliang Liu,2 Jie Tang,3 Wei Wang,3 Lili Lu2
1First Medical College, Xuzhou Medical University, Xuzhou, People’s Republic of China; 2Department of Gastroenterology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, People’s Republic of China; 3School of Public Health, Xuzhou Medical University, Xuzhou, People’s Republic of China
Correspondence: Wei Wang, School of Public Health, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China, Tel +86-15152118260, Email [email protected] Lili Lu, Department of Gastroenterology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, 221004, People’s Republic of China, Tel +86-15905204534, Email [email protected]
Purpose: Anxiety, as an important public health issue, may frequently trouble the chronic GI patients with severe symptoms. In this study, we aimed to investigate the relationship between the severity of GI symptoms and anxiety symptoms and further examine whether this relationship was mediated through illness perception.
Patients and Methods: A total of 295 patients with chronic GI disease from the affiliated hospital of Xuzhou Medical University were enrolled in this cross-sectional study. They were interviewed with self-reported questionnaires containing demographic variables, clinical variables, and several self-rating scales. Multivariable linear regression models were established to explore the relationship between the severity of GI symptoms and anxiety symptoms. Finally, we performed the mediation analysis to test the mediating effect of illness perception.
Results: After adjustments for key demographic and clinical covariates, the severity of GI symptoms was positively associated with anxiety symptoms (β=0.214, 95% CI: 0.009– 0.028, P < 0.001). Additionally, the results of the mediation analysis suggested that illness perception partially mediated the association between the severity of GI symptoms and anxiety symptoms with a mediating ratio of 25.3%.
Conclusion: Our findings indicated that chronic GI patients with more severe GI symptoms were more likely to have anxiety symptoms and this effect is partially mediated by illness perception. Therefore, illness perception is recommended to be integrated into the routine assessment of chronic GI patients, and perception-based interventions may be beneficial in relieving anxiety symptoms among patients with severe chronic GI diseases.
Keywords: illness perception, anxiety symptoms, severity of GI symptoms, chronic GI diseases, mediating effect
Introduction
Gastrointestinal (GI) diseases cover multiple groups of clinical conditions that endanger public health worldwide, constituting a persistent challenge for the patient’s quality of life and healthcare use.1,2 A large proportion of gastrointestinal diseases are characterized by a chronic relapsing process, such as inflammatory bowel disease (IBD), chronic gastritis, peptic ulcers, enteritis polyposa, and Helicobacter pylori infection. There is increasing evidence indicating that anxiety symptoms, as a common psychological disorder, have a relatively high prevalence among chronic GI patients,3–5 for instance, the prevalence of anxiety symptoms in IBD patients, peptic ulcer patients, and chronic gastritis patients is 32.1%,6 32.8%,7 and 36.4%,8 respectively. Because patients with GI diseases often need continuous daily medication, repeated medical treatment, and even hospitalization,9 which negatively impacts their life quality and adds to their disease burden, they may be at a higher risk for anxiety.10,11 The psychological problems of chronic GI patients have always been a thorny issue. It is well known that symptoms of anxiety can lead to poorer health-related quality of life in the general population12 and a previous study suggested that the poor mental health of inpatients is related to the length of hospitalization and risk of readmission.13 Therefore, understanding the spectrum of determinants of anxiety symptoms and further investigating the potential interaction between these recognized determinants are necessary for promoting the mental health of these chronic GI patients.
There are multiple factors contributing to anxiety symptoms of chronic GI patients and the effect of GI symptoms severity on patients’ psychological state has received increasing attention. Patients with chronic GI disease often suffer from various somatic symptoms in daily life, such as abdominal pain, diarrhea, acid reflux, nausea, and constipation. Accumulating evidence has shown that patients who suffer from more severe disease-related somatic pain tend to have a higher rate of psychological comorbidity, particularly anxiety and depressive symptoms.14 A longitudinal cohort study found that in comparison with those inactive GI diseases, patients with active disease symptoms were more susceptible to anxiety.15 The interaction between GI symptoms and psychological disorders is often attributed to a complex and bi-directional communication between the GI tract and the brain (brain-gut axis), which affect the function of both organs.16–18 The human intestinal microorganism has been reported to communicate with the brain in a bidirectional pathway.19 It is believed that GI disease patients are often accompanied by gut microbiota disturbance,20 thus, people with more severe GI symptoms are more susceptible to anxiety symptoms mediated by the brain-gut axis. Remarkably, despite plenty of evidence emphasized that increased disease activity was associated with worsening anxiety symptoms, some works have exhibited different results. A study during lockdown from COVID-19 reported that even patients with remission of inflammatory bowel disease could also experience severe anxiety symptoms, especially female patients with Crohn’s disease.21 Consequently, to explore the exact effect of GI symptoms severity on patients’ psychological state, it is necessary to conduct more in-depth research in the future.
In the long-term struggle with health threats, patients formulated relatively mature cognitive representations and beliefs of their illness. These cognitive and emotional representations were collectively referred to as illness perceptions. According to Leventhal’s common-sense model, illness perception guided subsequent medical-seeking behaviors and affected health outcomes.22 It was also worth noting that consistent evidence has shown that patients with negative illness perception were more susceptible to psychological disorders such as anxiety in some chronic GI diseases.23,24 Additionally, a previous study found that those patients who perceived more severe GI symptoms also tended to report more negative illness perceptions.25 Therefore, in theory, the relationship between the severity of GI symptoms and anxiety symptoms may be mediated by illness perception. However, as far as we know, evidence elucidating the mediating effects of illness perception in this relationship has not been reported previously.
Although the severity of GI symptoms may be an associated risk factor for anxiety symptoms, before achieving a satisfactory curative effect, it is still difficult to relieve patients’ anxiety symptoms. However, patients’ cognitive representations and briefs about their illnesses are not fixed or changeless. A growing body of evidence suggested that illness perceptions can be positively restructured by cognitive behavioral interventions, thus helping patients improve their psychological well-being.26–28 Moreover, a review on the role of cognitive-behavioral psychotherapy also explored a probable beneficial effect of psychotherapy in recovering IBD patients’ therapeutic adherence. Patients with higher recovering adherence often have better control of the disease and lower disease-dependent activities, which indirectly reduces the incidence of psychological comorbidities.29 An in-depth understanding of the role of illness perception as a mediator in the relationship between the severity of GI symptoms and anxiety symptoms will provide a theoretical basis for perception-based interventions targeted at reducing anxiety symptoms in patients with chronic GI disease. The purpose of this study, therefore, was to explore whether there was a positive association between the severity of GI symptoms and anxiety symptoms, and specifically examine whether this association was mediated through illness perception.
Methods
Study Population and Data Collection
This cross-sectional study was designed according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. The study was carried out from June 2022 to October 2022 at the affiliated hospital of Xuzhou Medical University, during this period, the investigators distributed questionnaires to patients who had definite diagnoses of chronic GI diseases (eg inflammatory bowel disease, chronic gastritis, peptic ulcers, enteritis polyposa, and Helicobacter pylori infection) by professional physician according to the guidelines. The exclusion criteria were as follows: (1) unable to fill out a questionnaire (inability to read or write, severe cognitive impairment); (2) with questionable diagnoses; (3) in critical condition, such as with decompensated and severe comorbidities; (4) with already known psychiatric diagnoses; (5) refusing to cooperate. Whole process of the study was voluntary and anonymous for the participants. Total of 313 questionnaires were sent out. According to the above inclusion and exclusion criteria, 295 eligible patients were ultimately recruited. This study was conducted in accordance with the principles of the Declaration of Helsinki. The Research Ethics Committee at the affiliated hospital of Xuzhou Medical university approved this study protocol and the potential study population was informed about the research in advance and provided with written informed consent before they filled out the questionnaire.
Structure of the Questionnaire
The self-administered questionnaire was divided into two parts. In the first part of the questionnaire, demographic and clinical characteristics were recorded, containing age, gender, educational level, permanent residence, job category, monthly income, marital status, sleep duration, and whether suffer from hypertension. Whereas the second part was composed of three scales, including the Brief Illness Perception Questionnaire (BIPQ), Generalized Anxiety Disorder Scale (GAD-7), and Gastrointestinal Symptom Rating Scale (GSRS).
Measures
Illness Perceptions
Patients’ perceptions regarding their disease were assessed with the Chinese version of the Brief Illness Perception Questionnaire (BIPQ).30 The BIPQ is a validated 9-item self-management questionnaire widely applied to the research of patients’ cognitive and emotional representations of disease.31 The BIPQ has sound psychometric properties and has already been used for diseases of the digestive system.31 All the questions reflected patients’ subjective thoughts toward their disease. Item 1 to item 8 were rated on a 0 to 10 point Likert scale. Notably, items 3, 4, and 7 were scored in reverse. All the first eight item scores were summed to obtain a total BIPQ score, with higher scores representing a more negative perception of the illness.30 Item 9 of BIPQ was an open-end question that asked the patients to list what they thought to be the most important factors contributing to the onset of their disease, whereas item 9 was not considered in this study. Item 1 to 8 was classified into three dimensions including cognitive dimension, emotional dimension, and comprehensibility of illness. The construct validity and internal consistency of the 8-item BIPQ have been well confirmed in GI disease population.32,33 Cronbach’s α of BIPQ in the current study was 0.773.
Anxiety Symptoms
The emergence of anxiety symptoms was recognized with the Generalized Anxiety Disorder Scale (GAD-7). The GAD-7 is a reliable 7-item self-administered instrument that widely serves as a tool for screening generalized anxiety symptoms in primary care settings,34 and this scale has already been used in patients with digestive disorders by numerous studies.8,35 Each item was rated on a Likert scale (from 0-not at all to 3-nearly every day), with higher scores indicating greater anxiety severity. Score levels of 0–4, 5–9, 10–14, and 15–21 indicated no, mild, moderate, and severe anxiety, respectively.36 As per common practice, the emergence of anxiety symptoms was defined as a total GAD-7 score ≥5. The reliability and validity of the GAD-7 have been well demonstrated.37 Cronbach’s α of GAD-7 in the current study was found to be 0.887.
The Severity of GI Symptoms
The 15-item Gastrointestinal Symptom Rating Scale (GSRS) was used to measure the severity of GI symptoms. This interview-based rating scale has been used for assessment of GI symptoms in various chronic digestive diseases, such as irritable bowel syndrome, peptic ulcer disease, dyspepsia, and gastrointestinal reflux disease.38–40 It consisted of 15 questions designed to evaluate the severity of common gastrointestinal symptoms. We recorded the answer using a four-point Likert scale from 0 to 3, where 0 represented no symptoms and 3 represented very severe symptoms that patients’ social functioning was severely compromised. Total GSRS scores ranged from 0 to 45 with higher scores representing worse gastrointestinal symptoms.38 The scale had good reliability and validity.39 The Cronbach’s α was 0.741 in this study.
Statistical Analyses
Demographic and clinical characteristics of the participants were reported using N (%) for categorical variables and mean ± standard deviation (SD) for continuous variables. To examine the relationship between the severity of GI symptoms and anxiety symptoms, the study participants were classified into the anxiety symptoms group and no anxiety symptoms group according to their GAD-7 scores, and the total GSRS was transformed into a quartile variable (total GSRS score: 0–4, 5–7, 8–10 and 11–37). Then, we conducted three multivariable linear regression models: model 1, no covariates were adjusted; model 2, age and gender were adjusted; model 3, all the covariates presented in Table 1 were adjusted. Pearson correlation analysis was used to examine the association of severity of GI symptoms, illness perception, and anxiety symptoms. Finally, the mediation analysis was performed with PROCESS v3.3 in SPSS to test the mediating effect of illness perception on the relationship between the severity of GI symptoms and anxiety symptoms. Bias-corrected bootstrapping with 5000 iterations was implemented to yield a percentile-based confidence interval, which does not rely on the assumption of the normal sampling distribution.41 The indirect impact was controlled according to the value of the 95% confidence interval and when the confidence interval did not contain 0, the intermediary effect held. All statistical analyses were performed in SPSS, version 26.0, and P < 0.05 was considered statistically significant.
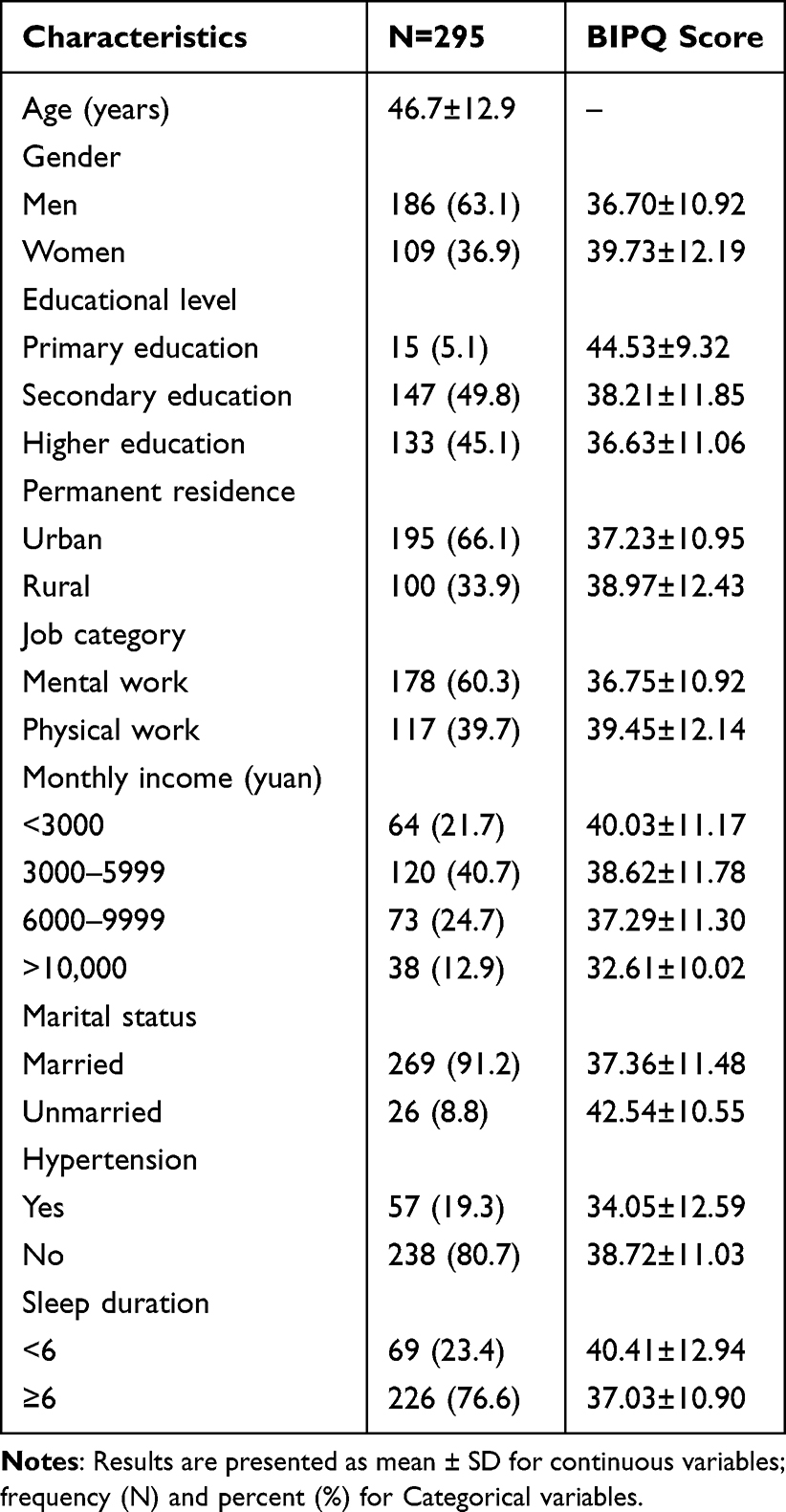 |
Table 1 Demographic and Clinical Characteristics of the Study Population |
Results
Patient Characteristics
In this study, a total of 313 questionnaires were sent out, and 295 valid questionnaires were returned ultimately, with an effective response rate of 94.2%. For the total sample, 109 female and 186 male patients were involved, and they were definitely diagnosed with chronic GI diseases, such as inflammatory bowel disease, IBD, chronic gastritis, peptic ulcers, enteritis polyposa, and Helicobacter pylori infection. The mean age was 46.7 (SD:12.9), ranging from 18 to 70. The demographic and clinical characteristics and the mean BIPQ score of the study population by covariates are summarized in Table 1.
Relationship Between Severity of Gastrointestinal Symptoms and Anxiety
According to the GAD-7 scores, 218 participants were assigned to the no-anxiety symptoms group (GAD-7 score <5), and the remaining 77 participants were assigned to the anxiety symptoms group (GAD-7 score ≥5). The results of the multivariable linear regression analysis were presented in Table 2. We found a significant positive association between the severity of GI symptoms (measured by GSRS scores) and the risk of anxiety symptoms in all three models: model 1 (β=0.247, 95% CI: 0.012–0.031, P < 0.001); model 2 (β=0.246, 95% CI: 0.012–0.031, P < 0.001); model 3 (β=0.214, 95% CI: 0.009–0.028, P < 0.001). As the GSRS score increased, the risk of having anxiety symptoms kept growing significantly. For multivariable regression, the independent variable GSRS score was divided into four groups according to the quartile methods. The trend remained significant among different GSRS score quartile groups (P for trend < 0.05 in each model). After adjustment for all the demographic and clinical covariates presented in Table 1, compared with patients with a 0–4 total GSRS score, patients reporting a GSRS score of 11 or higher had a 3.3-fold risk for anxiety symptoms.
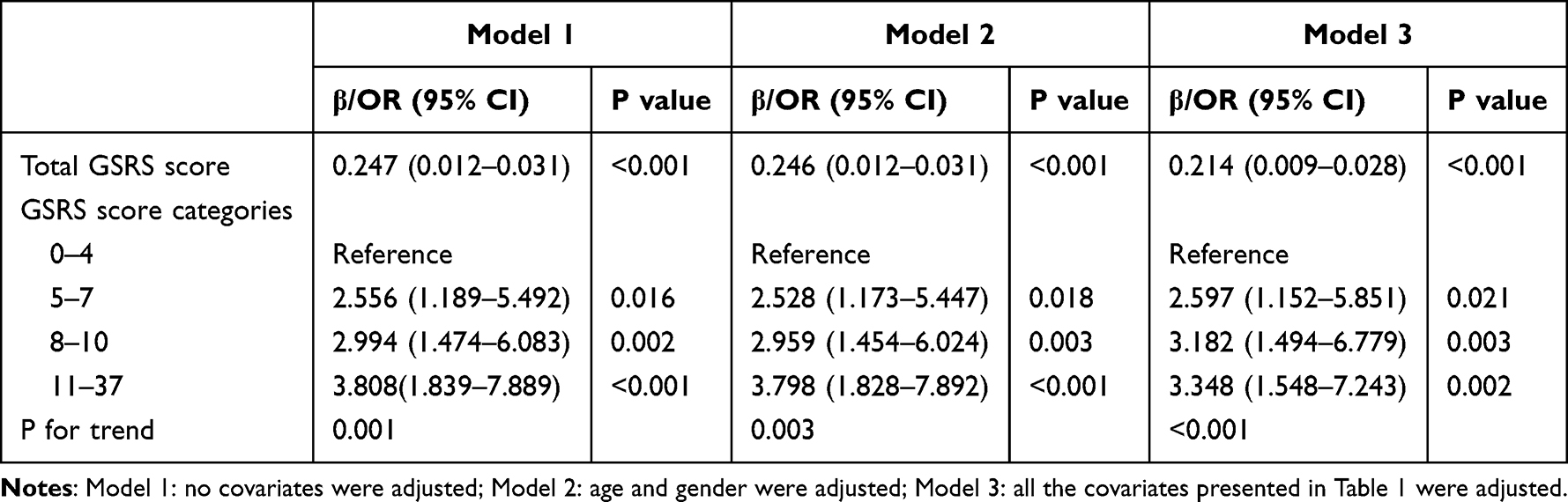 |
Table 2 Relationship Between Severity of GI Symptoms (Measured by GSRS Score) and Anxiety Symptoms |
Correlation Analysis
Significant correlations of the severity of GI symptoms, illness perception, and anxiety symptoms were found in the Pearson correlation analysis (Table 3). The severity of GI symptoms (r=0.308, P<0.01) and illness perception (r=0.317, P<0.01) were both positively associated with anxiety symptoms. Additionally, the severity of GI symptoms was also positively associated with illness perception (r=0.321, P<0.01).
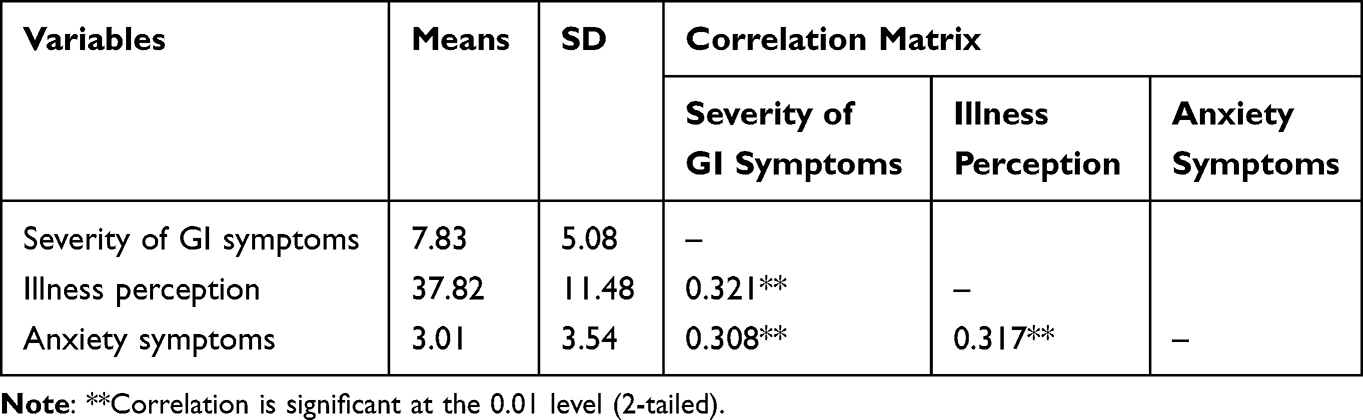 |
Table 3 Means, Standard Deviations and Pearson Correlation Coefficients of the Three Variables |
Correlation Analysis
Significant correlations of the severity of GI symptoms, illness perception, and anxiety symptoms were found in the Pearson correlation analysis (Table 3). The severity of GI symptoms (r = 0.308, P < 0.01) and illness perception (r = 0.317, P < 0.01) were both positively associated with anxiety symptoms. Additionally, the severity of GI symptoms was also positively associated with illness perception (r = 0.321, P<0.01).
Mediation Analysis
The results of the mediating effect of illness perception on the relationship between the severity of GI symptoms and anxiety symptoms are shown in Table 4. The total effect (path c) of the severity of GI symptoms on anxiety symptoms severity was 0.308 (P < 0.001, 95% CI = 0.138–0.291). The path a (standardized coefficient = 0.321, P < 0.001, 95% CI = 0.480–0.972), and path b (standardized coefficient = 0.243, P < 0.001, 95% CI = 0.040–0.110) were also significant, indicating that illness perception was positively associated with severity of GI symptoms and anxiety symptoms. When the effect of the severity of GI symptoms on anxiety symptoms was mediated by illness perception, the direct effect (path c’) of it was only 0.230 and was still significant (P < 0.001). Illness perception mediated the relationship between the severity of GI symptoms and anxiety symptoms (indirect effect value = 0.078, 95% CI = 0.029–0.087). The results suggested that illness perception acted as a partial mediator between the severity of GI symptoms and anxiety symptoms with the proportion of mediating effect of 25.3%. The model for the mediating effect of illness perception was illustrated in Figure 1.
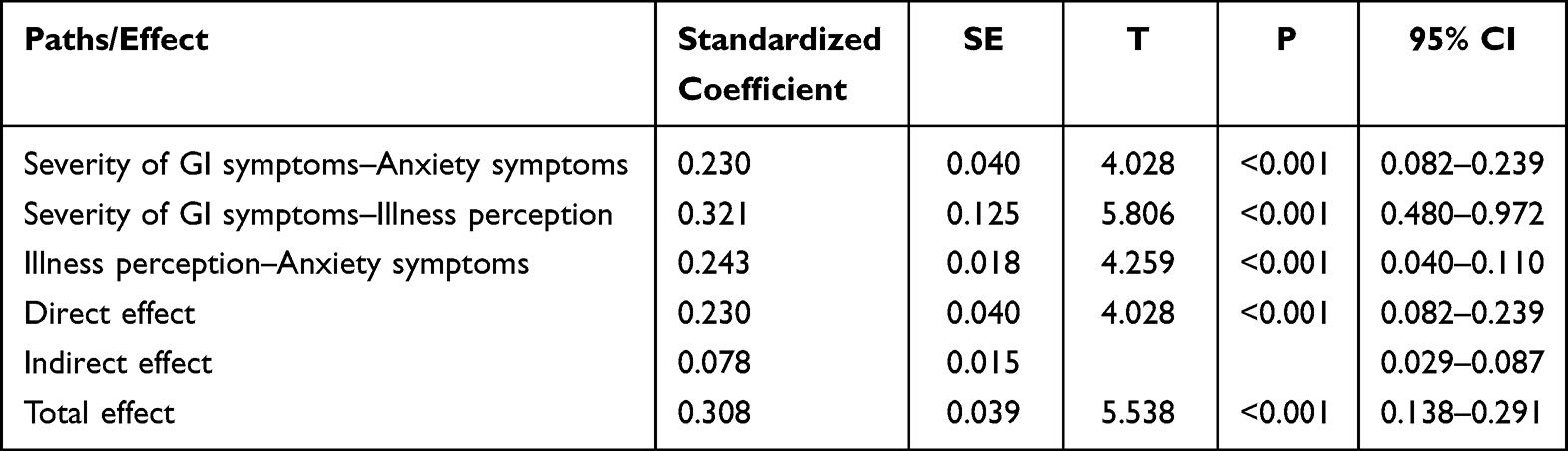 |
Table 4 Results of Mediation Analysis for the Mediating Effect of Illness Perception |
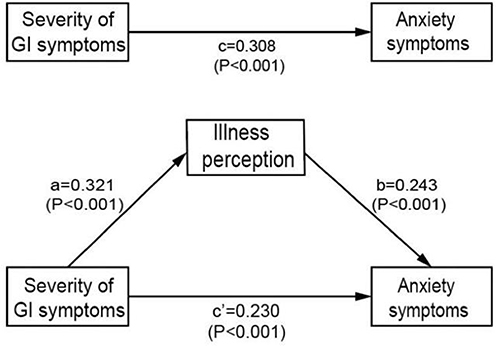 |
Figure 1 A model for the mediating effect of Illness perception. Notes: c path represents total effect; a*b path represents indirect effect; c’ path represents direct effect. All path standardized coefficients and P values are displayed in the model. |
Discussion
Previous studies have not yet explored the relationship between the severity of GI symptoms, illness perception, and anxiety symptoms among chronic GI patients using the mediation model. In this cross-sectional study, we have clarified: (1) The severity of GI symptoms was positively associated with anxiety symptoms; (2) Illness perception partially mediated the association between the severity of GI symptoms and anxiety symptoms with the mediating ratio of 25.3%.
Relationship Between Severity of Gastrointestinal Symptoms and Anxiety Symptoms
In this study, those who perceived more severe GI symptoms also tended to have a higher incidence of anxiety symptoms after adjusting for demographic and clinical variables. This association was as per our expectations because many previous studies have demonstrated that the severity of GI symptoms had a positive association with a high incidence of psychological comorbidity.4,14 In an observational study, 4217 outpatients with functional gastrointestinal disorders completed the evaluation for their anxiety symptoms and GI symptoms, and the results showed that with an increase in the frequency and severity of GI symptoms, the prevalence of anxiety symptoms increased in a stepwise manner.42 Similarly, a case-control study reporting the prevalence of anxiety symptoms in chronic GI disease patients relative to healthy controls also suggested that chronic GI symptoms affected psychological behavior.5 A previous study evaluated the role of psychopathological functioning and its relationship with GI symptoms severity in 69 patients with inflammatory bowel disease or irritable bowel syndrome, finding that a higher level of anxiety was significantly associated with greater disease severity.43 Furthermore, besides the severity of GI symptoms, previous studies demonstrated that the number of GI symptoms was also significantly associated with anxiety symptoms. A study conducted in 15 primary care clinics found a significantly increased risk for psychological disorders such as generalized anxiety disorder and panic disorder as the number of GI symptoms increased, specifically, in comparison with patients with no GI symptoms, the risk for anxiety in patients with one, two, and three GI symptoms increased 3.7-fold, 6.5-fold, and 7.2-fold, respectively.44 All of these studies above consistently demonstrated a significant association between GI symptoms and anxiety symptoms, supporting our findings. However, contrary to our results, a previous study performed among 32 outpatients with clinically diagnosed irritable bowel syndrome did not find a specific correlation between the load of disease severity and anxiety symptoms.45 The heterogeneity of studies, including study population, controlling variables, study sample size, and the choice of scales for evaluating the severity of GI symptoms and anxiety symptoms, might lead to different conclusions on the relationship between the severity of GI symptoms and anxiety symptoms.
Recently, the mechanisms by which GI symptoms severity correlates with anxiety symptoms have been extensively studied, among which the major mechanism behind this bidirectional relationship was gut-brain axis mechanism. The functional activity of the host digestive system and central nervous system is integrated by a neurohumoral communication system, which is called the gut-brain axis.46 Serious GI symptoms are often accompanied by disturbance of the intestinal microbiome and several studies have found that a dysbiosis of the gut microbiota can exert an influence on the central nervous system (CNS) through the gut-brain axis.47 In other words, the onset of anxiety symptoms in patients with severe GI symptoms may be attributed to the activation of the gut-brain axis.48 A large amount of evidence suggested that the communication between human intestinal microorganisms and the brain is a complex and bidirectional interaction, indicating that the severity of GI symptoms and anxiety symptoms are interactional and can drive each other.49 There are multiple possible mechanisms of gut–brain interaction have been revealed, including the release of inflammatory signals,50 activation of the hypothalamic-pituitary-adrenal (HPA) axis,51 excessive activation of glial cells,52 and decrease of a variety of neurotransmitters (eg GABA, 5-HT)53,54 and neurotrophic factors (eg BDNF).54 In summary, bidirectional communication between the GI tract and the brain via the brain-gut axis was one of an explanation of the association between the severity of GI symptoms and anxiety symptoms.
Mediating Role of Illness Perception in the Relationship Between Severity of Gastrointestinal Symptoms and Anxiety Symptoms
In recent years, the deepening understanding of chronic GI diseases has made it possible for the early detection, diagnosis, and treatment of the diseases, together with the application of newly developed medicine, making the life span of patients with chronic GI diseases improved.55,56 In a continuous struggle with chronic symptoms, patients have a general understanding and give meaning to their illness experience, formulating a relatively mature illness perception. However, to date, there is remarkably little research focusing on the illness perceptions of patients with chronic GI disease, and the association of severity of disease symptoms, patients’ illness perceptions, and their psychological state has not received enough attention from physicians in primary health care. To the best of our knowledge, this is the first report of the mediating role of illness perception in the relationship between the severity of gastrointestinal symptoms and anxiety symptoms among patients with chronic GI disease. The results of the mediating model showed that illness perception plays a partial mediating role between the severity of GI symptoms and anxiety symptoms.
As a result of mediating analysis, the mediating variable, illness perception, had a significant positive correlation with the severity of GI symptoms, indicating that those who perceived more severe GI symptoms also tended to report more negative illness perception. This result was consistent with the finding of a previous cohort study that suggested that illness perception was significantly and strongly associated with increased disability severity in patients with chronic inflammatory bowel disease.25 Chronic GI patients often suffered from multiple serious somatic symptoms in daily life, such as abdominal pain, diarrhea, acid reflux, nausea, and constipation, in which case their quality of life and social functioning can be compromised to a greater or lesser extent.57,58 Notably, the effects of the disease and its treatment can be insidious and intrusive. The uncertainty of GI symptoms and the unpredictability of relapse times can be tricky for patients with chronic GI disease, requiring them to adjust and cope with the transformation of health status. Therefore, the association between the severity of GI symptoms and illness perception can be explained by the effect of compromised life quality and social functioning on the formation of negative illness perception.
Additionally, we also found a positive association between illness perception and anxiety symptoms. Leventhal’s common-sense model constructs a theoretical framework for the association between illness perception and health outcomes that illness perception leads to significant individual differences in their understanding and coping strategies towards health threat, thus guiding subsequent medical-seek behaviors, including treatment willingness and medication adherence.22,59,60 It was worth noting that accumulating evidence has shown that illness perception was strongly related to psychological outcomes. Overall, previous studies in some other chronic diseases, such as multiple sclerosis,61 coronary artery disease,62 and cancers63,64 consistently indicated that an individual’s illness-related cognitive representations and beliefs are strongly associated with anxiety symptoms, specifically, the more negative illness perception was, the higher likelihood of anxiety symptoms. Using the Common-Sense Model (CSM), a cross-sectional study carried out among 261 patients with inflammatory bowel disease provided a reasonable explanation for the association between illness perception and psychological disorders. It examined the psychological mediators of psychological distress, finding that positive illness perception reduces the risk of psychological distress through increased self-efficacy and positive coping strategies.65
As a major finding of this study, illness perception serves as a partial mediator in the relationship between the severity of gastrointestinal symptoms and anxiety symptoms, indicating that patients’ beliefs and expectations regarding their illness indirectly influence the effect of GI symptoms severity on anxiety symptoms. The mediating role of illness perception suggests that illness perception, as a potentially modifiable factor, may be promising and effective in improving anxiety symptoms among these chronic GI patients with severe GI symptoms. Based on the common-sense model, perception-based interventions such as cognitive behavior therapy (CBT) have been thought to be a useful therapeutic interventions for reducing psychological distress by reversing negative illness perceptions.66 A randomized controlled trial among patients with irritable bowel syndrome (IBS) found that after a short period of cognitive behavioral therapy interventions mediated by changes in illness-related cognitions, improvements in GI symptoms were observed.67 In another psychosocial aftercare program, 57 patients received interventions for illness perceptions and were followed up for one year.68 Results showed that positive changes in illness perceptions were related to an improvement in patient’s psychological well-being, providing forceful evidence for the clinical prospect of perception-based interventions in improving the mental health of chronic GI patients. Of note, the Brief Illness Perception Questionnaire (BIPQ) has perfect psychometric properties and predictive validity and has been widely applied to the research of illness perceptions in hundreds of illness types and in 26 languages from 36 countries.31 The use of BIPQ as a brief and efficient screening instrument for those with relatively negative illness perceptions may contribute to identifying the targeted patients who are probable to benefit from perception-based interventions by challenging their negative perceptions of the illness. Timely and accurate assessment of illness perception is crucial to promote psychological health and well-being in patients with chronic GI diseases. Considering the reliability and validity of BIPQ in the initial screening of illness perception, therefore, we recommend the routine clinical use of this scale for evaluating illness perceptions in chronic GI patients.
The better understanding of illness perception and its effect in the relationship between severity of GI symptoms and anxiety symptoms will provide a brand-new direction for clinical intervention to relieve patients’ anxiety symptoms. Early and targeted interventions designed to reverse negative illness perception may be an effective way to improve patients’ anxiety symptoms. For medical staff, paying more attention to patients’ illness perception and bring the routine assessment of the patient’s illness perception into the clinical practice may be necessary. Patient education is a crucial part in the intervention for negative illness perception. Most of negative illness perception is originated from poor understanding of their disease and treatment, therefore, medical staff can educate patients on the basic characteristics, course, treatment, nursing, and prognosis about their illness, and teach them appropriate coping strategies to help them eliminate fear and confusion about illness. In this way, patients will have a clearer understanding of their illness, and will be more likely to develop a positive perception of their illness. In a word, at the clinical level, illness perception is expected to become a key point of psychological intervention on patients with chronic GI disease in the future.
Strengths and Limitations
The current study focused on the relationship between the severity of GI symptoms and anxiety symptoms, and examined whether this relationship was mediated through illness perception, which has not been widely explored among chronic GI patients in the past. The findings of this study contribute to a deeper understanding of the relationship between the severity of GI symptoms, illness perception, and anxiety symptoms in patients suffering from chronic GI disease. Additionally, we found that the effect of the severity of GI symptoms on anxiety symptoms was indirectly mediated via illness perception, which laid a theoretical basis for perception-based interventions to improve mental health. Overall, our study provided useful guidance for clinical practice to focus on the mediating effect of illness perception on the relationship between the severity of GI symptoms and anxiety symptoms, suggesting that interventions targeting changing negative illness perceptions have a potential benefit in relieving anxiety symptoms of patients with severe chronic GI diseases.
This study has some limitations to be considered in the interpretation of our results. First, the cross-sectional design is limited to determining the relationships between variables, as a result, the causality cannot be determined. To further investigate how patients’ illness perception impacts on the relationship between the severity of GI symptoms and anxiety symptoms over time, longitudinal follow-up studies are essential in the future. Moreover, our study was a small sample size and single-center study, only containing 295 participants; thus, a more extensive and multi-center sample is necessary to further test the representativeness of our findings.
Additionally, due to the lack of specific medication information about the patients, it is difficult to determine whether these drugs have any side effects causing anxiety. Therefore, there may be some confounding effects in the analysis process. Furthermore, the use of a single cohort for analysis is another limitation of this study. Chronic gastrointestinal diseases are known to have distinct microbial compositions and functionalities, influenced by factors, such as genetic background, environmental factors, dietary habits, treatment regimens, and individual characteristics. The role of microbial communities in the gut-brain axis may vary across different diseases. Therefore, for certain specific diseases, the findings of this study may not fully align with the real-life scenario. Moreover, due to the small sample size, it is not sufficient to do subgroup analysis by disease type. This should be further explored in the future research. Another potential limitation of our study that cannot be ignored is the use of the self-administered instrument for measuring the severity of patients’ GI symptoms. Although this scale has been demonstrated to have great reliability and validity for evaluating the severity of common gastrointestinal symptoms, patients may offer a biased assessment of their disease severity for various social and psychological factors, which could have led to potential reporting bias and ultimately interfere with the interpretation of our results. The authenticity and accuracy of self-report measures are still to be considered in comparison with the physician-based diagnosis. Therefore, future studies must combine self-reported and physician-based GI symptoms severity to make a comprehensive assessment of the severity of GI symptoms. Moreover, although previous studies have confirmed the reliability and validity of GSRS for the assessment of GI symptoms in various chronic digestive diseases, such as irritable bowel syndrome, peptic ulcer disease, dyspepsia, and gastrointestinal reflux disease, whether this questionnaire has the same weight in different chronic digestive diseases should also be taken into account in the future studies.
Conclusion
This study provides an in-depth understanding of the relationship among severity of GI symptoms, illness perception, and anxiety symptoms among patients with chronic GI disease, finding that the severity of GI symptoms was positively associated with anxiety symptoms and illness perception serves as a partial mediator in this association. Study results suggest that routine assessment of illness perceptions is necessary, especially for those who suffer from more severe GI symptoms, and interventions targeted at changing negative illness perceptions appear to have a potential benefit in relieving anxiety symptoms of patients with severe chronic GI diseases.
Ethics Approval and Consent to Participants
This study was conducted in accordance with the principles of the Declaration of Helsinki. The Research Ethics Committee at the affiliated hospital of Xuzhou Medical university approved this study protocol, and informed consent was signed by each participant before they fill out the questionnaire.
Acknowledgments
We would like to express our sincere appreciation to all participants in this study. We would also like to thank the affiliated hospital of Xuzhou Medical University for the successful conduct of the study.
Funding
This work was supported by the National Natural Science Foundation of China (grant number: 82003484) and Science and technology project of Affiliated Hospital of Xuzhou Medical University (grant number: 2021ZA16).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ranasinghe N, Devanarayana NM, Rajindrajith S, et al. Functional gastrointestinal diseases and psychological maladjustment, personality traits and quality of life. BMC Gastroenterol. 2018;18(1):33. doi:10.1186/s12876-018-0760-8
2. Sperber AD, Bangdiwala SI, Drossman DA, et al. Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome foundation global study. Gastroenterology. 2021;160(1):99–114.e3. doi:10.1053/j.gastro.2020.04.014
3. Neuendorf R, Harding A, Stello N, Hanes D, Wahbeh H. Depression and anxiety in patients with inflammatory bowel disease: a systematic review. J Psychosom Res. 2016;87:70–80. doi:10.1016/j.jpsychores.2016.06.001
4. Fond G, Loundou A, Hamdani N, et al. Anxiety and depression comorbidities in irritable bowel syndrome (IBS): a systematic review and meta-analysis. Eur Arch Psychiatry Clin Neurosci. 2014;264(8):651–660. doi:10.1007/s00406-014-0502-z
5. Shah E, Rezaie A, Riddle M, Pimentel M. Psychological disorders in gastrointestinal disease: epiphenomenon, cause or consequence? Ann Gastroenterol. 2014;27(3):224–230.
6. Barberio B, Zamani M, Black CJ, Savarino EV, Ford AC. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(5):359–370. doi:10.1016/S2468-1253(21)00014-5
7. Babić E, Bevanda M, Karin M, et al. Anxiety, depression and personality types in patients with inflammatory bowel disease: comparisons with peptic ulcer and the general population. Psychiatr Danub. 2021;33(1):48–56. doi:10.24869/psyd.2021.48
8. Wu H, Liang G, Kong M, et al. The status and risk factors for anxiety/depression in patients with atrophic chronic gastritis: a cross-sectional study. Ann Palliat Med. 2022;11(10):3147–3159. doi:10.21037/apm-22-730
9. Ananthakrishnan AN. Personalizing therapy for inflammatory bowel diseases. Expert Rev Gastroenterol Hepatol. 2013;7(6):549–558. doi:10.1586/17474124.2013.824693
10. Wen Z, Li X, Lu Q, et al. Health related quality of life in patients with chronic gastritis and peptic ulcer and factors with impact: a longitudinal study. BMC Gastroenterol. 2014;14(1):149. doi:10.1186/1471-230X-14-149
11. Ganz ML, Sugarman R, Wang R, Hansen BB, Håkan-Bloch J. The economic and health-related impact of crohn’s disease in the United States: evidence from a nationally representative survey. Inflamm Bowel Dis. 2016;22(5):1032–1041. doi:10.1097/MIB.0000000000000742
12. Moffitt TE, Harrington H, Caspi A, et al. Depression and generalized anxiety disorder: cumulative and sequential comorbidity in a birth cohort followed prospectively to age 32 years. Arch Gen Psychiatry. 2007;64(6):651–660. doi:10.1001/archpsyc.64.6.651
13. Beeler PE, Cheetham M, Held U, Battegay E. Depression is independently associated with increased length of stay and readmissions in multimorbid inpatients. Eur J Intern Med. 2020;73:59–66. doi:10.1016/j.ejim.2019.11.012
14. Perera MJ, Schneiderman N, Sotres-Alvarez D, Daviglus M, Mirabal SM, Llabre MM. Are anxious and depressive symptoms associated with gastrointestinal symptoms in the Hispanic community health study/study of Latinos (HCHS/SOL)? J Racial Ethn Health Disparities. 2021;8(3):712–722. doi:10.1007/s40615-020-00831-6
15. Marrie RA, Graff LA, Fisk JD, Patten SB, Bernstein CN. The relationship between symptoms of depression and anxiety and disease activity in IBD over time. Inflamm Bowel Dis. 2021;27(8):1285–1293. doi:10.1093/ibd/izaa349
16. Lach G, Schellekens H, Dinan TG, Cryan JF. Anxiety, depression, and the microbiome: a role for gut peptides. Neurother J Am Soc Exp Neurother. 2018;15(1):36–59. doi:10.1007/s13311-017-0585-0
17. Liu Y, Wang H, Gui S, et al. Proteomics analysis of the gut-brain axis in a gut microbiota-dysbiosis model of depression. Transl Psychiatry. 2021;11(1):568. doi:10.1038/s41398-021-01689-w
18. Gracie DJ, Hamlin PJ, Ford AC. The influence of the brain-gut axis in inflammatory bowel disease and possible implications for treatment. Lancet Gastroenterol Hepatol. 2019;4(8):632–642. doi:10.1016/S2468-1253(19)30089-5
19. Capuco A, Urits I, Hasoon J, et al. Current perspectives on gut microbiome dysbiosis and depression. Adv Ther. 2020;37(4):1328–1346. doi:10.1007/s12325-020-01272-7
20. Sun D, Ge X, Tang S, et al. Bacterial characteristics of intestinal tissues from patients with crohn’s disease. Front Cell Infect Microbiol. 2021;11:711680. doi:10.3389/fcimb.2021.711680
21. Spina A, Mazzarella C, Dallio M, et al. The lesson from the first Italian lockdown: Impacts on anxiety and depressive symptoms and sleep quality in patients with remission of inflammatory bowel disease. Rev Recent Clin Trials. 2022;17(2):109–119. doi:10.2174/1574887117666220328125720
22. Diefenbach MA, Leventhal H. The common-sense model of illness representation: theoretical and practical considerations. J Soc Distress Homeless. 1996;5(1):11–38. doi:10.1007/BF02090456
23. Eindor-Abarbanel A, Naftali T, Ruhimovich N, et al. Important relation between self-efficacy, sense of coherence, illness perceptions, depression and anxiety in patients with inflammatory bowel disease. Frontline Gastroenterol. 2021;12(7):601–607. doi:10.1136/flgastro-2020-101412
24. Knowles SR, Gass C, Macrae F. Illness perceptions in IBD influence psychological status, sexual health and satisfaction, body image and relational functioning: a preliminary exploration using structural equation modeling. J Crohns Colitis. 2013;7(9):e344–e350. doi:10.1016/j.crohns.2013.01.018
25. van der Have M, Fidder HH, Leenders M, et al. Self-reported disability in patients with inflammatory bowel disease largely determined by disease activity and illness perceptions. Inflamm Bowel Dis. 2015;21(2):369–377. doi:10.1097/MIB.0000000000000278
26. Dempster M, McCorry NK, Brennan E, Donnelly M, Murray LJ, Johnston BT. Do changes in illness perceptions predict changes in psychological distress among oesophageal cancer survivors? J Health Psychol. 2011;16(3):500–509. doi:10.1177/1359105310386633
27. Petrie KJ, Perry K, Broadbent E, Weinman J. A text message programme designed to modify patients’ illness and treatment beliefs improves self-reported adherence to asthma preventer medication. Br J Health Psychol. 2012;17(1):74–84. doi:10.1111/j.2044-8287.2011.02033.x
28. Sararoudi RB, Motmaen M, Maracy MR, Pishghadam E, Kheirabadi GR. Efficacy of illness perception focused intervention on quality of life, anxiety, and depression in patients with myocardial infarction. J Res Med Sci Off J Isfahan Univ Med Sci. 2016;21:125. doi:10.4103/1735-1995.196607
29. Gravina AG, Pellegrino R, Palladino G, et al. Targeting the gut-brain axis for therapeutic adherence in patients with inflammatory bowel disease: a review on the role of psychotherapy. Brain-Appar Commun J Bacomics. 2023;2(1):2181101. doi:10.1080/27706710.2023.2181101
30. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
31. Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the brief illness perception questionnaire. Psychol Health. 2015;30(11):1361–1385. doi:10.1080/08870446.2015.1070851
32. De Gucht V. Illness perceptions mediate the relationship between bowel symptom severity and health-related quality of life in IBS patients. Qual Life Res. 2015;24(8):1845–1856. doi:10.1007/s11136-015-0932-8
33. Knowles SR, Cook SI, Tribbick D. Relationship between health status, illness perceptions, coping strategies and psychological morbidity: a preliminary study with IBD stoma patients. J Crohns Colitis. 2013;7(10):e471–e478. doi:10.1016/j.crohns.2013.02.022
34. Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146(5):317–325. doi:10.7326/0003-4819-146-5-200703060-00004
35. Luo Y, Keefer L. Role of psychological questionnaires in clinical practice and research within functional gastrointestinal disorders. Neurogastroenterol Motil. 2021;33(12):e14297. doi:10.1111/nmo.14297
36. Swinson RP. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evid Based Med. 2006;11(6):184. doi:10.1136/ebm.11.6.184
37. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
38. Svedlund J, Sjödin I, Dotevall G. GSRS--a clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig Dis Sci. 1988;33(2):129–134. doi:10.1007/BF01535722
39. Kulich KR, Madisch A, Pacini F, et al. Reliability and validity of the Gastrointestinal Symptom Rating Scale (gsrs) and Quality Of Life In Reflux And Dyspepsia (QOLRAD) questionnaire in dyspepsia: a six-country study. Health Qual Life Outcomes. 2008;6:12. doi:10.1186/1477-7525-6-12
40. Kulich KR, Reguła J, Stasiewicz J, Jasinski B, Carlsson J, Wiklund I. Psychometric validation of the polish translation of the Gastrointestinal Symptom Rating Scale (gsrs) and Quality Of Life In Reflux And Dyspepsia (qolrad) questionnaire in patients with reflux disease. Pol Arch Med Wewn. 2005;113(3):241–249.
41. Mackinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivar Behav Res. 2004;39(1):99. doi:10.1207/s15327906mbr3901_4
42. Pinto-Sanchez MI, Ford AC, Avila CA, et al. Anxiety and depression increase in a stepwise manner in parallel with multiple fgids and symptom severity and frequency. Am J Gastroenterol. 2015;110(7):1038–1048. doi:10.1038/ajg.2015.128
43. Piacentino D, Cesarini M, Badiali D, Pallotta N, Biondi M, Corazziari ES. The central role of psychopathology and its association with disease severity in inflammatory bowel disease and irritable bowel syndrome. Riv Psichiatr. 2019;54(2):75–83. doi:10.1708/3142.31248
44. Mussell M, Kroenke K, Spitzer RL, Williams JBW, Herzog W, Löwe B. Gastrointestinal symptoms in primary care: prevalence and association with depression and anxiety. J Psychosom Res. 2008;64(6):605–612. doi:10.1016/j.jpsychores.2008.02.019
45. Mikocka-Walus A, Turnbull D, Moulding N, Wilson I, Andrews JM, Holtmann G. Psychological comorbidity and complexity of gastrointestinal symptoms in clinically diagnosed irritable bowel syndrome patients. J Gastroenterol Hepatol. 2008;23(7 Pt 1):1137–1143. doi:10.1111/j.1440-1746.2007.05245.x
46. Collins SM, Surette M, Bercik P. The interplay between the intestinal microbiota and the brain. Nat Rev Microbiol. 2012;10(11):735–742. doi:10.1038/nrmicro2876
47. Foster JA, McVey Neufeld KA. Gut-brain axis: how the microbiome influences anxiety and depression. Trends Neurosci. 2013;36(5):305–312. doi:10.1016/j.tins.2013.01.005
48. Lee Y, Kim YK. Understanding the connection between the gut-brain axis and stress/anxiety disorders. Curr Psychiatry Rep. 2021;23(5):22. doi:10.1007/s11920-021-01235-x
49. Fairbrass KM, Lovatt J, Barberio B, Yuan Y, Gracie DJ, Ford AC. Bidirectional brain-gut axis effects influence mood and prognosis in IBD: a systematic review and meta-analysis. Gut. 2022;71(9):1773–1780. doi:10.1136/gutjnl-2021-325985
50. Agirman G, Yu KB, Hsiao EY. Signaling inflammation across the gut-brain axis. Science. 2021;374(6571):1087–1092. doi:10.1126/science.abi6087
51. Cryan JF, O’Riordan KJ, Cowan CSM, et al. The microbiota-gut-brain axis. Physiol Rev. 2019;99(4):1877–2013. doi:10.1152/physrev.00018.2018
52. Guida F, Turco F, Iannotta M, et al. Antibiotic-induced microbiota perturbation causes gut endocannabinoidome changes, hippocampal neuroglial reorganization and depression in mice. Brain Behav Immun. 2018;67:230–245. doi:10.1016/j.bbi.2017.09.001
53. Liang L, Zhou H, Zhang S, Yuan J, Wu H. Effects of gut microbiota disturbance induced in early life on the expression of extrasynaptic GABA-A receptor α5 and δ subunits in the hippocampus of adult rats. Brain Res Bull. 2017;135:113–119. doi:10.1016/j.brainresbull.2017.09.014
54. Hoban AE, Moloney RD, Golubeva AV, et al. Behavioural and neurochemical consequences of chronic gut microbiota depletion during adulthood in the rat. Neuroscience. 2016;339:463–477. doi:10.1016/j.neuroscience.2016.10.003
55. Torres J, Bonovas S, Doherty G, et al. ECCO guidelines on therapeutics in crohn’s disease: medical treatment. J Crohns Colitis. 2020;14(1):4–22. doi:10.1093/ecco-jcc/jjz180
56. Magro F, Gionchetti P, Eliakim R, et al. Third European evidence-based consensus on diagnosis and management of ulcerative colitis. part 1: definitions, diagnosis, extra-intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo-anal pouch disorders. J Crohns Colitis. 2017;11(6):649–670. doi:10.1093/ecco-jcc/jjx008
57. Marinelli C, Savarino E, Inferrera M, et al. Factors influencing disability and quality of life during treatment: a cross-sectional study on IBD patients. Gastroenterol Res Pract. 2019;2019:5354320. doi:10.1155/2019/5354320
58. Mules TC, Swaminathan A, Hirschfeld E, et al. The impact of disease activity on psychological symptoms and quality of life in patients with inflammatory bowel disease-results from the stress, anxiety and depression with disease activity (sadd) study. Aliment Pharmacol Ther. 2022;55(2):201–211. doi:10.1111/apt.16616
59. Dhaliwal HS, Singh R, Abraham AM, et al. Perception of illness and its association with treatment willingness in patients with newly diagnosed nonalcoholic fatty liver disease. Dig Dis Sci. 2021;66(12):4197–4207. doi:10.1007/s10620-020-06794-2
60. Kucukarslan SN. A review of published studies of patients’ illness perceptions and medication adherence: lessons learned and future directions. Res Soc Adm Pharm. 2012;8(5):371–382. doi:10.1016/j.sapharm.2011.09.002
61. Janssens ACJW, van Doorn PA, de Boer JB, van der Meché FGA, Passchier J, Hintzen RQ. Perception of prognostic risk in patients with multiple sclerosis: the relationship with anxiety, depression, and disease-related distress. J Clin Epidemiol. 2004;57(2):180–186. doi:10.1016/S0895-4356(03)00260-9
62. Kunschitz E, Friedrich O, Schöppl C, Maitz J, Sipötz J. Illness perception patterns in patients with coronary artery disease. Psychol Health Med. 2017;22(8):940–946. doi:10.1080/13548506.2016.1271439
63. Zhang N, Fielding R, Soong I, et al. Illness perceptions as predictors of psychological distress among head and neck cancer survivors: a longitudinal study. Head Neck. 2018;40(11):2362–2371. doi:10.1002/hed.25343
64. McCorry NK, Dempster M, Quinn J, et al. Illness perception clusters at diagnosis predict psychological distress among women with breast cancer at 6 months post diagnosis. Psychooncology. 2013;22(3):692–698. doi:10.1002/pon.3054
65. Kantidakis JD, Moulding R, Knowles SR. Psychological mediators of psychological distress and quality of life in inflammatory bowel disease. J Psychosom Res. 2021;149:110596. doi:10.1016/j.jpsychores.2021.110596
66. Mikocka-Walus A, Andrews JM, Bampton P. Cognitive behavioral therapy for IBD. Inflamm Bowel Dis. 2016;22(2):E5–E6. doi:10.1097/MIB.0000000000000672
67. Chilcot J, Moss-Morris R. Changes in illness-related cognitions rather than distress mediate improvements in irritable bowel syndrome (IBS) symptoms and disability following a brief cognitive behavioural therapy intervention. Behav Res Ther. 2013;51(10):690–695. doi:10.1016/j.brat.2013.07.007
68. Fischer MJ, Wiesenhaan ME, Does-den Heijer A, Kleijn WC, Nortier JWR, Kaptein AA. From despair to hope: a longitudinal study of illness perceptions and coping in a psycho-educational group intervention for women with breast cancer. Br J Health Psychol. 2013;18(3):526–545. doi:10.1111/j.2044-8287.2012.02100.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.