Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Relationship Between Self-Care Behavior and Cognitive Function in Hospitalized Adult Patients with Type 2 Diabetes: A Cross-Sectional Study
Authors Yang J ![]() , Zhang Z, Zhang L, Su Y, Sun Y, Wang Q
, Zhang Z, Zhang L, Su Y, Sun Y, Wang Q
Received 2 November 2019
Accepted for publication 17 January 2020
Published 29 January 2020 Volume 2020:13 Pages 207—214
DOI https://doi.org/10.2147/DMSO.S236966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Jin Yang,1,* Zhenzhen Zhang,2,* Lijie Zhang,3 Ye Su,3 Yumei Sun,3 Qun Wang1
1Department of Endocrinology and Metabolism, Peking University Third Hospital, Beijing 100191, People’s Republic of China; 2Department of Cardiology, The First Affiliated Hospital of Chongqing Medical University, Chongqing 400016, People’s Republic of China; 3Peking University School of Nursing, Beijing 100191, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yumei Sun
Peking University School of Nursing, Beijing 100191, People’s Republic of China
Tel +86-10-13641042422
Fax +86-10-82266722
Email [email protected]
Qun Wang
Department of Endocrinology and Metabolism, Peking University Third Hospital, 49 North Garden Road, Haidian District, Beijing 100191, People’s Republic of China
Tel +86-10-15611908590
Fax +86-10-82265025
Email [email protected]
Purpose: To investigate the relationship between diabetes self-care behavior and cognitive function of hospitalized young and middle-aged Chinese patients with type 2 diabetes mellitus (T2DM).
Patients and Methods: In this cross-sectional study, young and middle-aged T2DM patients (age range, 35– 65 years) were recruited at 4 tertiary hospitals between July 2016 and January 2017. Data pertaining to self-care behavior and cognitive function were collected using two questionnaires (the Summary of Diabetes Self-care Activities [SDSCA] and the Montreal Cognitive Assessment [MoCA], respectively). Multivariate linear regression analysis was performed to assess the correlation between cognitive function and self-care activities.
Results: A total of 140 patients with diabetes were enrolled (mean age, 53.79± 7.96 years). The mean duration of T2DM was 10.83± 6.76 years. Regarding SDSCA performance, the mean scores for foot care and blood glucose monitoring were 2.20± 2.57 and 1.98± 2.45, respectively, which were the worst; scores for exercise (4.01± 2.58) and diet (3.16± 1.89) were better, while scores for medication administration (5.26± 2.79) were the best. The prevalence of cognitive impairment was 37.9% (53 patients). After variables adjustment, delayed recall showed a significant correlation with blood sugar monitoring behavior (B =0.224, P=0.019); visual space and executive function (B=0.255, P=0.009) and abstraction (B=− 0.337, P=0.001) showed a correlation with foot care behavior.
Conclusion: Cognitive ability affects the self-care behavior of patients with T2DM. Assessment of cognitive function may help inform patient education interventions to improve the self-care behavior of these patients.
Keywords: young and middle-aged, cognitive impairment, self-care behaviors, type 2 diabetes mellitus
Introduction
Type 2 diabetes mellitus (T2DM) is a major health issue and a primary cause of mortality across the world.1,2 The condition is also referred to as adult-onset diabetes as it typically occurs in the middle- and late adulthood.3,4 More than 4 million people are affected by T2DM annually worldwide, which imposes a considerable economic burden on the patients and the society.4 In addition, T2DM decreases the life expectancy of people who have the disease by about 15 years.5 In 2010, the reported prevalence of diabetes among Chinese adults was approximately 11.6%.6
Self-care behavior in the context of diabetes refers to actions taken by patients to deal with their disease based on their knowledge and skills; these include physical activity, healthy diet plan, self-monitoring of glucose level, and adherence to medication.7 Self-care behavior of patients with diabetes has a positive impact on achievement of glycemic control and can reduce the risk of cardiovascular complications by 80%.8,9 Diabetes may accelerate cognitive aging and is a risk factor for cognitive dysfunction.9 In addition, cognitive dysfunction can affect the self-care behavior of patients with diabetes. As self-care behavior is important for diabetes management, characterization of its relationship with cognitive dysfunction is a key imperative.
Diabetes is associated with cognitive change because it may influence some of the cognitive changes. At the same time, diabetes self-management tasks require multiple cognitive skills. Several studies have focused on the relationship between cognitive dysfunction and self-management of diabetes in older people. For instance, cognitive dysfunction showed an association with worse self-care behavior or caused unreasonable diabetes self-care behavior, such as they do not know what to do in the event of low blood sugar or how to manage medication in the event of sickness.10–12 Cognitive dysfunction has an adverse effect on self-care behavior, while poor glycemic control has also been shown to be a risk factor for cognitive dysfunction.13,14
Middle-aged patients with T2DM were found to exhibit a certain degree of cognitive dysfunction.15,16 However, the impact of cognitive dysfunction on the self-care behavior of young and middle-aged adult patients is not well characterized. The objective of this study was to examine the relationship between cognitive dysfunction and self-care behavior in a sample of Chinese adult patients with diabetes aged 35–65 years. This age-group represents the predominant segment of the Chinese workforce. We hypothesized that among patients with T2DM, those with more severe cognitive dysfunction would exhibit worse behavior pertaining to their diabetes self-care management.
Methods
Study Design and Patients
This was a cross-sectional study. The study protocol was approved by the Peking University Institutional Review Board and the ethics committee at each of the participant hospitals. The purpose of the study was explained to the participants, and written informed consent was obtained prior to their enrolment.
From July 2016 to January 2017, consecutive patients with T2DM who qualified the eligibility criteria were enrolled at the Peking University Third Hospital, the Peking University People’s Hospital, Peking University First Hospital, and the Beijing Haidian Hospital. The inclusion criteria were: 1) patients aged 35–65 years who were diagnosed based on the 1999 WHO diagnostic criteria for diabetes;16 2) duration of diabetes: more than 1 year; 3) education level: primary school and above. The exclusion criteria were 1) patients with malignant tumor or severe heart, lung, or kidney disease; 2) history of cerebrovascular disease; 3) history of any other disease that can lead to central nervous system damage, such as trauma, tumor, or infection; 4) patients with major depression, schizophrenia, or dementia; 5) patients with impaired ability for hearing, reading, or writing and those with difficulty in language expression; 6) patients with impaired ability to take care of themselves.
Measures
Demographic and Clinical Characteristics
Data pertaining to following variables were collected: 1) demographic variables, including sex, age, level of education, body mass index (BMI), long-term residence, marital status, occupation, and average monthly income per person of their family; 2) clinical variables disease, including the duration of diabetes, current treatment, glycosylated hemoglobin level, history of symptomatic/severe hypoglycemia, concomitant diseases, and complications of diabetes.
The Summary of Diabetes Self-Care Activities (SDSCA)
The SDSCA scale is a self-report quantitative measure of diabetes self-care. The scale was originally developed by Toobert et al in 1994 and its validity and reliability is well documented17–19 Wan et al translated it into Chinese in 2008.19 The scale consists of 11 items that cover the self-care behavior in the context of diabetes including assessment of diet (general and specific), blood sugar monitoring, exercise, foot care, and cigarette smoking. Each item has a minimum score of 0 and a maximum score of 7, based on which the scores for each dimension were the summary of scores for every item, the mean score for each dimension was calculated using the formula: actual scores for each dimension/numbers of items. The total score range for SDSCA is 0–77. The higher the score is, the better the self-care is.
The scale has a good structural validity. The overall Cronbach’s α of SDSCA is 0.62 (test–retest reliability: 0.8; Kaiser-Meyer-Olkin (KMO) value: 0.64).
Montreal Cognitive Assessment (MoCA)
MoCA is a widely used scale to screen for mild cognitive impairment. Several versions of the scale are currently available.20,21 We used the Chinese version, which includes seven dimensions, namely visual space and execution ability, naming, attention, language, abstraction, memory and delayed recall, and orientation.19 The total score range is 0–30 points; a score of ≥26 points was defined as normal cognition while a score of <26 points was considered indicative of cognitive dysfunction (mild cognitive impairment). The higher the score, the better is the cognitive function.
Dimensional analysis of the scale has been performed, and each cognitive domain is delineated as a functional abnormality in the domain.11,12 If the subject has received education for ≤12 years, the total score is increased by 1 to correct the impact of the education level. The Cronbach’s α scale of MoCA was 0.818. MoCA has been shown to exhibit 90% sensitivity and 87% specificity for screening for mild cognitive impairment.21
Procedure
A trained diabetes nurse educator collected the essential clinical information of patients and completed the cognitive function scales. After obtaining written informed consent, the participants were invited to a comfortable and quiet reception room for data collection. First, the patient filled up a demographic questionnaire, and then the diabetes nurse educator conducted the SDSCA survey and MoCA assessment. Other disease-related information was collected from the inpatient medical records.
Statistical Analysis
The data were entered and analyzed using SPSS20.0 statistical software (SPSS Inc., Chicago, IL, USA). Normally distributed continuous variables are expressed as mean ± standard deviation (SD), and categorical variables are expressed as frequency and percentage. The association between groups were analyzed by one-way analysis of variance (ANOVA) or Pearson Chi-squared test. Multivariate linear regression analysis was performed to assess the correlation between cognitive function and self-management behavior of patients. Variables that showed a significant association with cognitive function on univariate analysis were treated as covariates in the multivariate regression analysis. Using the forward stepwise regression, 0.05 was set as the inclusion criteria to analyze the correlation between the dimensions of self-care behavior and the cognitive function. P values <0.05 were considered indicative of statistical significance.
Results
Clinical Characteristics of Patients
A total of 140 young and middle-aged patients with T2DM were enrolled. The mean age of patients was 53.8±7.9 years. The mean duration of diabetes was 10.83±6.8 years. The complications in this study cohort included hypertension, hyperlipidemia, coronary heart disease, retinopathy/cataract, peripheral neuropathy, and diabetic foot. Only 11 participants (7.9%) were found using only lifestyle interventions for the treatment of diabetes. Mild cognitive impairment was found in 53 (37.8%) patients (Table 1).
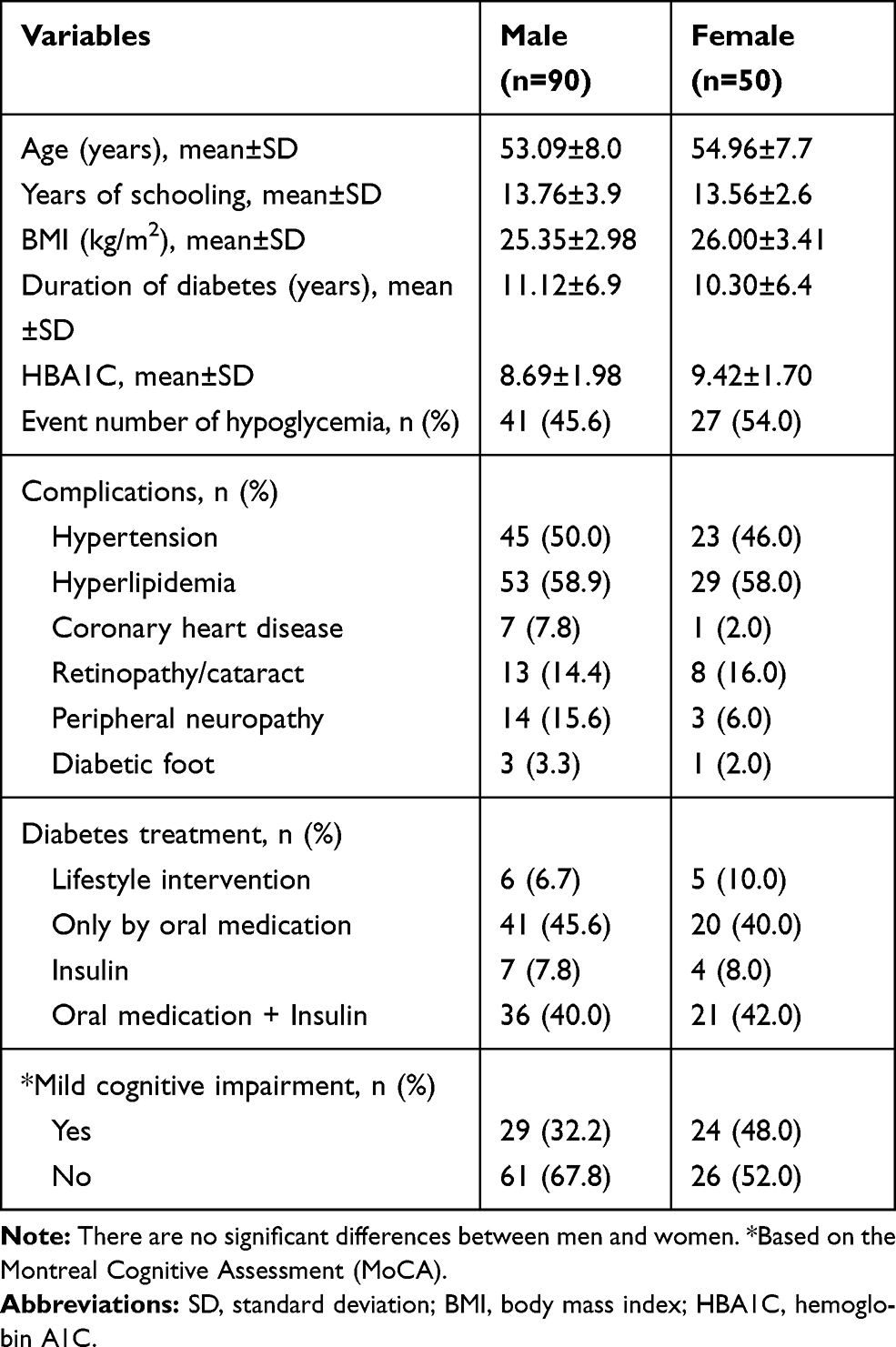 |
Table 1 Basic Characteristics of the Study Population (n=140) |
SDSCA
The self-report SDSCA survey showed that 5.7% (8/140) patients had good self-care behavior, 46.7% (65/140) patients had medium self-care behavior, and 47.9% (67/140) patients had poor self-care behavior.
Among all the self-care behavioral dimensions, the mean scores for foot care and blood glucose monitoring were 2.20±2.57 and 1.98±2.45, respectively, which were the worst; scores for lifestyle management including exercise (4.01±2.58) and diet (3.16±1.89) were better, while scores for medication administration (5.26±2.79) were the best (Table 2).
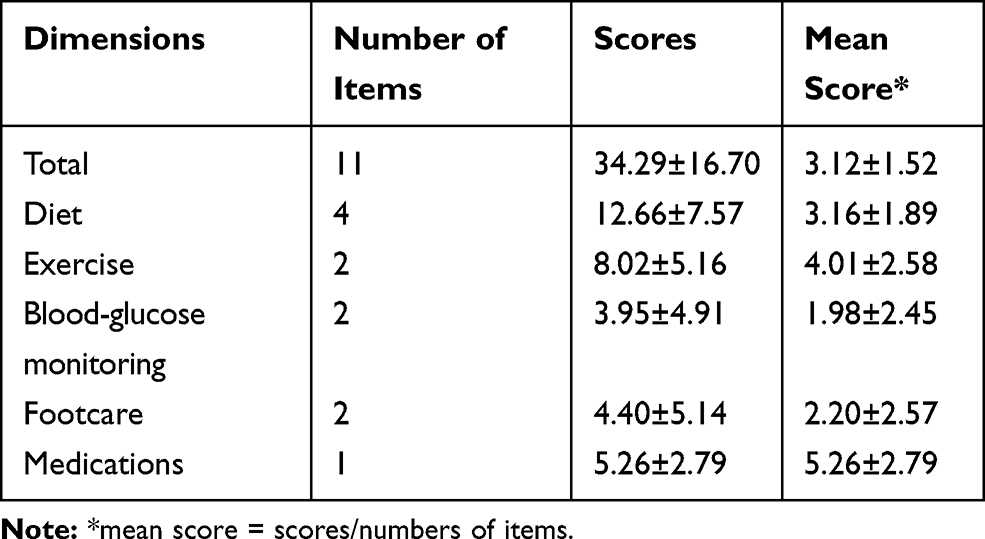 |
Table 2 Summary of Diabetes Self-Care Activities (SDSCA) of the Study Population (n=140) |
MoCA Assessment Results and Univariate Analysis of Mild Cognitive Impairment
In this study, 37.9% (53/140) patients had mild cognitive impairment. With respect to various dimensions of cognitive function (from high to low), 85.0% (119/140) patients had delayed recall function, 3.6% (103/140) had impaired language function, 50.7% (71/140) had impaired visuospatial ability and executive function, 18.6% (26/140) had impaired attention function, 11.4% (16/140) had impaired abstract function, and 11.4% (16/140) had impaired orientation function. On univariate analysis, age (t/χ2=−4.53, P=0.001), years of schooling (t/χ2=2.40, P=0.018), and duration of diabetes (t/χ2=−3.08, P=0.002) were associated with mild cognitive impairment (Table 3).
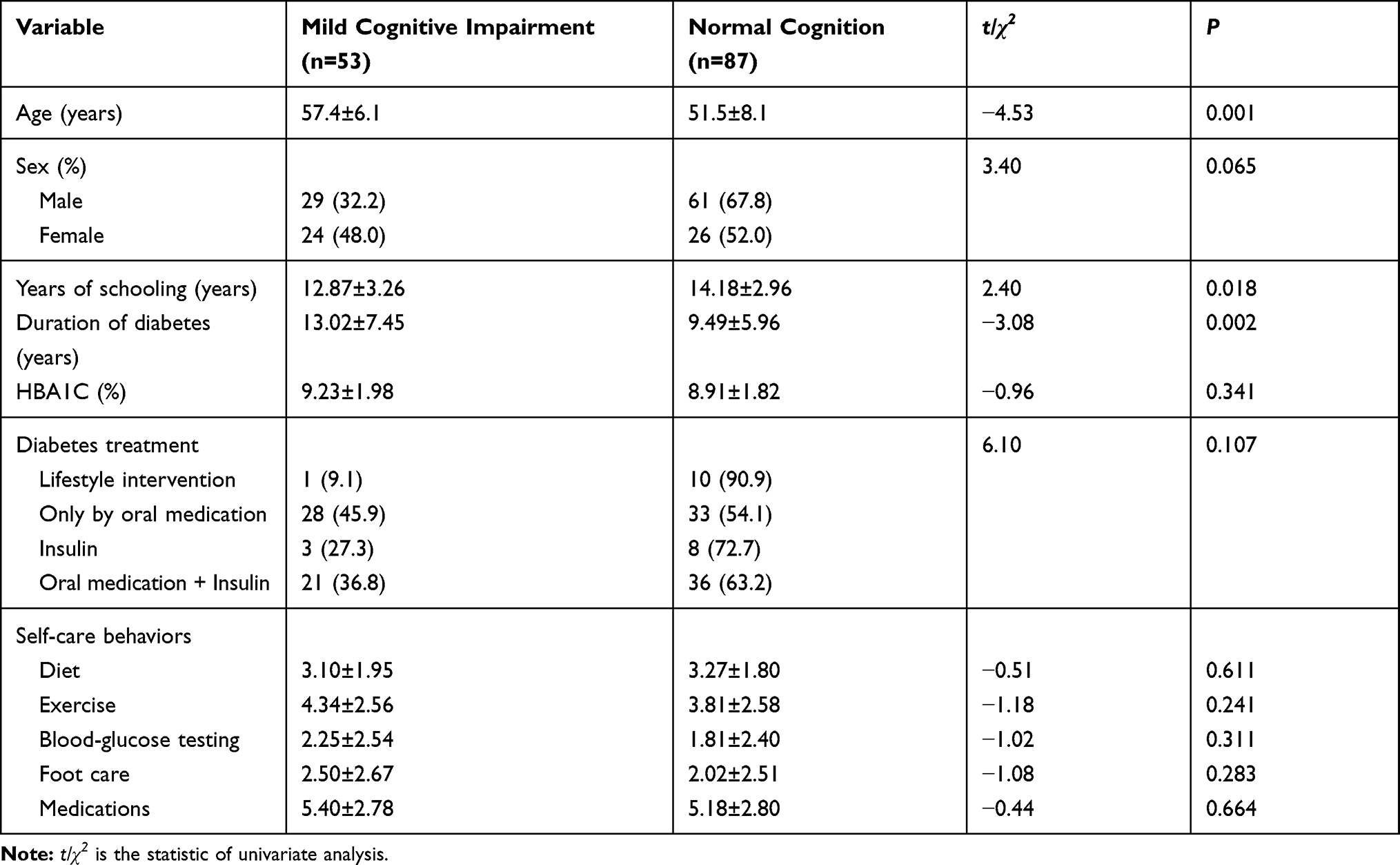 |
Table 3 Results of Univariate Analysis of Mild Cognitive Impairment (Categorical Variables) (n=140) |
The Association of Each Dimension of Self-Care Behavior with Cognitive Function
Based on the results of univariate analysis, age, sex (0=male, 1=female), years of schooling, duration of diabetes, hemoglobin A1C (HBA1C), and treatment (0=oral medication, 1=oral medication + insulin) were included as covariates in the multiple stepwise regression. The results showed no significant correlation of cognitive function with lifestyle (diet, exercise) management, or medication management. However, delayed recall was associated with blood glucose monitoring (B=0.224, P=0.019), while visual space and executive function (B=0.255, P=0.009) and abstract (B=−0.337, P=0.001) were related to foot care (Table 4).
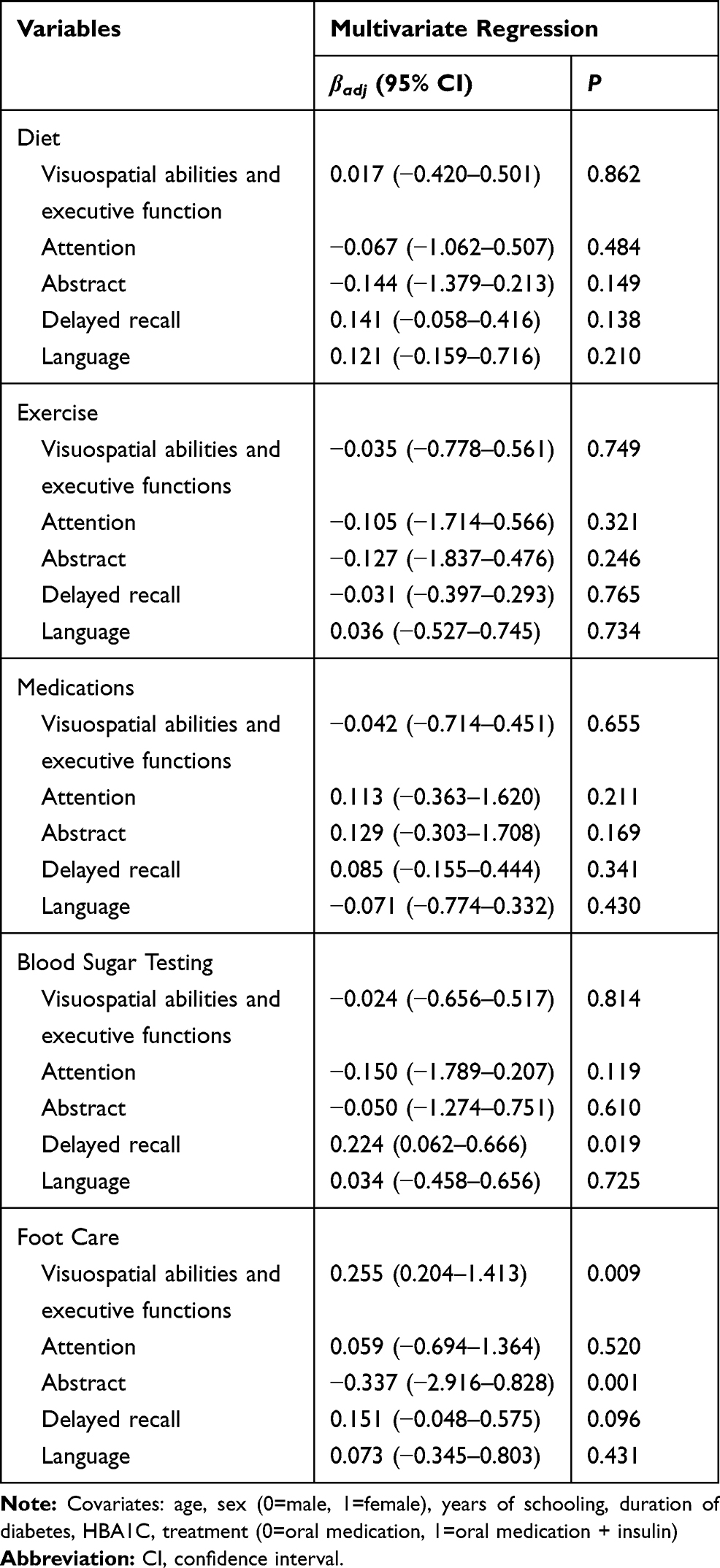 |
Table 4 Results of Multivariate Regression Analysis Showing the Association of Each Dimension of Self-Care Behaviors with Cognitive Function (n=140) |
Discussion
Diabetes is a chronic metabolic disease characterized by chronic hyperglycemia. The self-management level of patients with diabetes directly affects the quality of integrated diabetes management.5 Among the dimensions of self-care behaviors assessed in this study, the drug management score was the highest; this may be attributable to the good therapeutic effect of hypoglycemic drugs, which helps improve the patient’s medication compliance.22–25 Poor diet and exercise management indicate room for further improvement in the lifestyle management of young and middle-aged T2DM patients.26,27 Poor foot care was consistent with the results of most previous studies in China.24 In addition, the scores for blood glucose monitoring were the lowest (3.95±4.91); in previous studies conducted in other countries, the average blood glucose monitoring score was about 6.0.28,29 Many patients in this study performed blood glucose testing only when they were seeking medical treatment or feeling unwell, which indicates poor compliance of patients with blood glucose monitoring.30 In addition to the health management education provided by physicians or educators, the relationship between patient cognitive function and self-care behavior should be explored, especially with regard to lifestyle, foot care, and blood glucose testing.10 The prevalence of cognitive impairment in our study was 37.9%, which showed that even in young and middle-aged T2DM patient, middle cognitive impairment was still an important issue; age, years of schooling, and duration of diabetes showed a significant correlation with mild cognitive impairment in young and middle-aged T2DM patients. We found that only 15.0% of hospitalized patients with T2DM showed good self-care behavior. The best performance among the various self-care behavioral domains was with respect to medication management, followed by diet and exercise management and blood glucose monitoring, while the worst performance was with respect to foot management. These findings are consistent with those of previous studies conducted among older people with T2DM in China.22,23,31–33 In summary, this study found poor self-management behavior of young and middle-aged patients with T2DM, which calls for concerted interventions involving diabetes educators.
The MoCA is a highly sensitive screening tool for mild cognitive impairment in older adults, and is also used in young to middle-aged adults.34–36 The cognitive function dimensions of diabetes self-management behaviors were mainly delayed recall, visuospatial abilities and executive function, and abstract. Among those dimensions, delayed recall was significantly related to blood glucose monitoring (P=0.019), while visuospatial abilities and executive functions (P=0.009) and abstract ability (P=0.001) were significantly associated with foot care. Delayed recall refers to impaired ability to recall past events. This study found that the better the patient’s delayed recall, the better was the blood glucose monitoring; this finding was consistent with those reported by Compeán-Ortiz et al, who assessed 105 patients with middle-aged T2DM using the Wechsler Memory Scale and SDSCA scale.37 However, Primožič et al found that delayed recall was not associated with self-management behavior.29 Furthermore, Li et al used the SDSCA scale and the auditory word learning test (AVLT) to measure the self-management behavior and memory function of 51 middle-aged T2DM patients; the results showed that the worse the delayed recall, the better was the self-management behavior.23 This discrepancy may be attributable to differences with respect to the characteristics of the study cohorts and the screening tools. Visuospatial abilities and executive functions (alternating lines, cubes, clocks) refer to the general control mechanisms for the coordination and execution of complex cognitive tasks; these ensure that the cognitive systems implement specific goals in a flexible and optimized manner.38 A meta-analysis conducted by Tomlin et al found that implementation dysfunction may cause a decline in the self-management ability of patients with diabetes.11 In this study, we found that the better the visuospatial abilities and executive functions of the young and older patients, the better was their foot care. Primožič et al assessed 98 older people with T2DM; they found a significant association of visuospatial abilities and executive functions with self-management behavior (the better the visuospatial abilities and executive functions, the better were the patient’s self-management behaviors). In our study, the better the abstract ability, the worse was the foot care; to the best of our knowledge, no other study has found this association. The clinical relevance of this finding is that patients who have excellent abstract ability should be better educated about the need for feet examination. The evidence obtained from this study highlights the need for assessment of the cognitive function of patients with T2DM, for example, through face-to-face teaching of physicians and educators during hospitalization, and using informational means outside the hospital (APP management platform, etc.) in order to optimize patient management.
To the best of our knowledge, the correlation between cognitive function and self-care ability has not been previously assessed in Chinese hospitalized young and middle-aged T2DM patients. However, it is important to acknowledge that some limitations of this study should be considered while interpreting the results. First, the study population comprised of inpatients at four tertiary hospitals in Beijing; secondly, the sample size was relatively small, which limits the generalizability of our findings. Research in the community-based young and middle-aged T2DM population and the use of a larger sample size is required to determine more definitive evidence of the impact of cognitive function on diabetes self-care behavior. Furthermore, the Cronbach’s α value of the Chinese version of SDSCA (the most widely used in China) is low, which may have affected the accuracy of cognitive function assessment to some extent.
Conclusion
In summary, the self-care behavior of young and middle-aged Chinese patients with T2DM was found to be suboptimal. Some dimensions of the cognitive function including delayed recall, visuospatial abilities and executive functions, and abstract ability showed a significant direct association with self-care behavior. These findings suggest the need to educate young and middle-aged T2DM patients and to monitor their cognitive rehabilitation and self-care behavior to help improve the quality and level of diabetes management.
Ethics Approval and Informed Consent
This clinical trial was approved by the Ethics Committee of Peking University, and has been performed according to the ethical standards laid down in the 1964 Declaration of Helsinki. Informed consent was written by all individual participants included in the study.
Data Sharing Statement
The data used to support the findings of this study are included in the article.
Acknowledgment
This study was funded by grants from the National Key Research and Development Program of China (grant number 2018YFC1313900).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. IDF Diabetes Atlas Group. Update of mortality attributable to diabetes for the IDF diabetes atlas: estimates for the year 2013. Diabetes Res Clin Pract. 2015;109:461–465. doi:10.1016/j.diabres.2015.05.037
2. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. doi:10.1016/j.diabres.2009.10.007
3. Kao KT, Sabin MA. Type 2 diabetes mellitus in children and adolescents. Aust Fam Physician. 2016;45:401–406.
4. van Dieren S, Beulens JW, van der Schouw YT, Grobbee DE, Neal B. The global burden of diabetes and its complications: an emerging pandemic. Eur J Cardiovasc Prev Rehabil. 2010;17:s3–s8. doi:10.1097/01.hjr.0000368191.86614.5a
5. Schoenberg NE, Traywick LS, Jacobs-Lawson J, Kart CS. Diabetes self-care among a multiethnic sample of older adults. J Cross Cult Gerontol. 2008;23:361–376. doi:10.1007/s10823-008-9060-z
6. Xu Y, Wang L, He J, et al. Prevalence and control of diabetes in Chinese adults. JAMA. 2013;310:948–959. doi:10.1001/jama.2013.168118
7. Jordan DN, Jordan JL. Self-care behaviors of Filipino-American adults with type 2 diabetes mellitus. J Diabetes Complications. 2010;24:250–258. doi:10.1016/j.jdiacomp.2009.03.006
8. Povey RC, Clark-Carter D. Diabetes and healthy eating: a systematic review of the literature. Diabetes Educ. 2007;33:931–961. doi:10.1177/0145721707308408
9. Asche C, LaFleur J, Conner C. A review of diabetes treatment adherence and the association with clinical and economic outcomes. Clin Ther. 2011;33:74–109. doi:10.1016/j.clinthera.2011.01.019
10. Feil DG, Zhu CW, Sultzer DL. The relationship between cognitive impairment and diabetes self-management in a population-based community sample of older adults with type 2 diabetes. J Behav Med. 2012;35:190–199. doi:10.1007/s10865-011-9344-6
11. Tomlin A, Sinclair A. The influence of cognition on self-management of type 2 diabetes in older people. Psychol Res Behav Manag. 2016;9:7–20. doi:10.2147/PRBM.S36238
12. Wu X, Chen X, Wu J, Liu L, Pan B. Relationship between cognitive function, self-management behavior and self-efficacy in elderly patients with type 2 diabetes. Jiangsu J Prev Med. 2017;28:147–149.
13. Katon W, Pedersen HS, Ribe AR, et al. Effect of depression and diabetes mellitus on the risk for dementia: a national population-based cohort study. JAMA Psychiatry. 2015;72:612–619. doi:10.1001/jamapsychiatry.2015.0082
14. Wang Y, Song M, Yu L, et al. Mild cognitive impairment: vascular risk factors in community elderly in four cities of Hebei Province, China. PLoS One. 2015;10:e0124566. doi:10.1371/journal.pone.0124566
15. Duan S, Liu D, Li T, Guang J, Wei P, Wang J. The effect and characteristics of type 2 diabetes on cognitive function in middle-aged patients. J Third Mil Med Univ. 2016;38:314–319.
16. Chinese Diabetes Society. Guidelines for the prevention and treatment of type 2 diabetes in China (2013). Chin J Diabetes Mellitus. 2014;22:2–424. doi:10.3969/j.issn.1006-6187.2014.08.027
17. Toobert DJ, Glasgow RE. Assessing diabetes self-management: the summary of diabetes self-care activities questionnaire. Handbook Psychol Diabetes. 1994;351:75.
18. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23:943–950. doi:10.2337/diacare.23.7.943
19. Wan Q, Shang S, Lai X, Pan J. Reliability and validity of self-management behavior scale in patients with type 2 diabetes mellitus. Chin J Pract Nurs. 2008;24:26–27.
20. Lebedeva E, Huang M, Koski L. Comparison of alternate and original items on the montreal cognitive assessment. Can Geriatr J. 2016;19:15–18. doi:10.5770/cgj.19.216
21. Guo Q, Hong Z. Neuropsychological Assessment.
22. Ji J, Liu L, Lou Q, Yuan X, Yao P, Zhang D. Self-management behavior and blood glucose control in patients with type 2 diabetes mellitus. Chin J Nurs. 2014;49:4.
23. Li W, Sun Y, Feng Y, Wang Q. Self-management behavior and its relationship with memory function in patients with type 2 diabetes mellitus. Chin J Mod Nurs. 2015;3:254–258.
24. Chen M, Dou J, Zhuang X, et al. Investigation and study on the reasons for the change of national basic hypoglycemic drug therapy for patients with type 2 diabetes in Beijing community. Chin J Diabetes. 2016;24:778–781.
25. Yu P, Xiao X, Wang L, Wang L. The correlation between self-management behavior and blood glucose control in community type 2 diabetes patients. J Central South Univ. 2013;38:425–431.
26. Quan J. Status Quo of Self-Management Behavior and Its Influencing Factors in Middle-Aged and Elderly Patients with Type 2 Diabetes Mellitus. Yanji: Yanbian University; 2013.
27. Wang F, Yuan L, Li R, Xiong Z. Analysis of self-management behavior and influencing factors in hospitalized type 2 diabetes patients. J Nurs. 2015;30:29–31.
28. Thabit H, Kennelly SM, Bhagarva A, et al. Utilization of frontal assessment battery and executive interview 25 in assessing for dysexecutive syndrome and its association with diabetes self-care in elderly patients with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2009;86:208–212. doi:10.1016/j.diabres.2009.09.004
29. Primožič S, Tavčar R, Avbelj M, Dernovšek MZ, Oblak MR. Specific cognitive abilities are associated with diabetes self-management behavior among patients with type 2 diabetes. Diabetes Res Clin Pract. 2012;95:48–54. doi:10.1016/j.diabres.2011.09.004
30. Zhao W, Zhang J, Shuai Y, et al. Relationship between microvascular complication screening rate and knowledge level of diabetes mellitus in Beijing community. Chin J Diabetes Mellitus. 2015;8:47–481. doi:10.3760/cma.j.issn.1674-5809.2015.08005
31. Zhong X, Wang Z, Zhang L, Ji G, Wang X. The condition and influencing factors of self-management behavior of type 2 diabetes patients in urban communities. Chin J Health Educ. 2010;9:651–654.
32. Yue P, Chen X, Wang Y, Su X, Wu Y. Investigation and analysis of self-management behaviors and influencing factors of community type 2 diabetes patients. J Nurs Manag. 2013;7:478–480.
33. Sun S, Zhao W, Dong Y, Li Z. Analysis of the condition and influencing factors of self-management in diabetic patients. Chin J Nurs. 2011;46:5.
34. Siciliano M, Chiorri C, Passaniti C, Sant’Elia V, Trojano L, Santangelo G. Comparison of alternate and original forms of the Montreal Cognitive Assessment (MoCA): an Italian normative study. Neurol Sci. 2019;40:691–702. doi:10.1007/s10072-019-3700-7
35. Kumar N, Singh VB, Meena BL, et al. Mild cognitive impairment in young type 1 diabetes mellitus patients and correlation with diabetes control, lipid profile, and high-sensitivity C-reactive protein. Indian J Endocrinol Metab. 2018;22:780–784. doi:10.4103/ijem.IJEM_58_18
36. Ciudin A, Ortiz AM, Fidilio E, et al. Retinal microperimetry: a useful tool for detecting insulin resistance-related cognitive impairment in morbid obesity. J Clin Med. 2019;8(12):E2181. doi:10.3390/jcm8122181
37. Compeán-Ortiz LG, Gallegos EC, Gonzalez-Gonzalez JG, Gomez-Meza MV, Therrien B, Salazar BC. Cognitive performance associated with self-care activities in Mexican adults with type 2 diabetes. Diabetes Educ. 2010;36:268–275. doi:10.1177/0145721710361783
38. Baddeley A. Working memory: theories, models, and controversies. Annu Rev Psychol. 2012;63:1–29. doi:10.1146/annurev-psych-120710-100422
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.