Back to Journals » Risk Management and Healthcare Policy » Volume 19
Relationship Between Reflective Practice and Caring Behaviors Among Psychiatric Nurses: A Latent Profile Analysis
Authors Ren Y, Li J ![]() , Lin X, Luo S
, Lin X, Luo S
Received 15 October 2025
Accepted for publication 1 February 2026
Published 11 February 2026 Volume 2026:19 574450
DOI https://doi.org/10.2147/RMHP.S574450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Yanjuan Ren, Jie Li, Xiaomin Lin, Shanxia Luo
Mental Health Center, West China Hospital / West China School of Nursing, Sichuan University, Chengdu, 610041, People’s Republic of China
Correspondence: Shanxia Luo, Mental Health Center, West China Hospital/West China School of Nursing, Sichuan University, Chengdu, 610041, People’s Republic of China, Email [email protected]
Introduction: Reflective practice has emerged as a critical competency for psychiatric nurses, enabling them to critically evaluate and adapt their care approaches. Growing evidence suggests that reflective practice may serve as a key driver of high-quality caring behaviors, which are essential for establishing therapeutic relationships and improving outcomes in mental health settings. This study aimed to classify latent profiles of reflective practice among psychiatric nurses and examine their effects on caring behaviors.
Methods: This cross-sectional study was conducted to recruit psychiatric nurses from ten mental health treatment centers across ten hospitals in Sichuan Province, China, between January and March 2024. Psychiatric nurses completed an online investigation encompassing the Reflective Practice Questionnaire and the Caring Behaviors Inventory (CBI). Latent profile analysis (LPA) and hierarchical regression analysis were employed to achieve the study objectives.
Results: A total of 346 psychiatry nurses were included in this study. The reflective practice of psychiatric nurses was classified into three subgroups in this study: “passive reflective participants” (n=48, 13.9%), “moderately balanced reflective practitioners” (n=175, 50.6%), and “high-achieving reflective leaders” (n=123, 35.5%). The hierarchical regression analysis revealed a significant positive association between distinct profiles of reflective practice and psychiatric nurses’ caring behaviors (ΔR2 = 0.420, p < 0.001).
Conclusion: The identification of three distinct reflective practice profiles (“passive reflective participants”, “moderately balanced reflective practitioners”, and “high-achieving reflective leaders”) provides a nuanced understanding of the reflective practice among psychiatry nurses. Targeted development programs, such as peer mentoring for the “passive” group and the “moderate” group, could be designed based on individual profile membership to optimize caring behaviors in psychiatric nursing.
Keywords: psychiatric nurses, reflective practice, caring behaviors, latent profile analysis
Introduction
The global healthcare model is undergoing a paradigm shift from a primarily symptom-focused technological orientation toward patient-centered care, a transition that highlights the growing demand for humanistic caring approaches—particularly in mental health.1 According to statistics, people with mental disorders experience stigma and emotional neglect in 62% of cases, much higher than people with physical illnesses.2 As well as being one of the crucial concepts in the field of nursing, caring behaviors consolidate the triple attributes of scientific rigor, artistic creativity, and humanistic values.3 The essence of psychiatric nursing is therapeutic interpersonal interaction, which is centered on facilitating patients to reestablish social functioning through caring behaviors, including emotional support, empathetic communication, and dignity preservation.4 More crucially, as the primary caregivers for patients with mental illnesses, the caring behaviors of psychiatric nurses typically have a direct impact on the quality of care for patients during the rehabilitation process.5 Specifically, earlier evidence demonstrated that poor caring behaviors were significantly associated with negative patient outcomes, including infections, falls, and readmissions.6,7 However, there is a tendency for the present nursing education system to be “technologically oriented”, resulting in a structural deficit of caring behaviors among nurses in the clinical setting. Prior studies have indicated that the caring behaviors of psychiatric nurses are not favorable.8,9 This highlights the urgent clinical value of reviewing psychiatric nurses’ caring behaviors and their facilitators, as well as developing targeted strategies.
Reflective practice is a process whereby actions and decisions are reviewed with a view to improving practice, and consists of two modes: “reflection in action” (immediate adjustment of strategies) and “reflection after action” (in-depth analysis after the event).10 In the field of nursing, it is considered to be the integration of evidence-based best practices with personalized care plans drawing on experience and knowledge, thus supporting caregivers to react effectively to unexpected problems.11 Moreover, reflective practice is currently regarded as one of the competencies that nursing practitioners should be equipped with.12 Empirical research has demonstrated that reflective practice contributes to the achievement of excellent therapeutic interactions by enhancing nurses’ communication skills and critical thinking skills.13,14 However, despite the growing interest in reflective practice among nurse groups, few studies have focused on the condition of reflective practice among psychiatric nurses, highlighting a significant research gap. In addition, the majority of studies evaluated nurses’ reflective practice based only on scale scores, which led to inaccurate estimates by ignoring, to a large extent, their population heterogeneity, as the level of reflective practice may be affected by a variety of demographic factors such as educational level, age, and length of service.15 Therefore, an attempt was made to initiate a person-centered latent profiling (LPA) approach to accurately categorize psychiatric nurses’ reflective practice. Furthermore, existing empirical evidence has established that reflective practice contributes to improved critical thinking competencies, enhanced caring capacity, and reduced incidence of moral distress among nursing professionals.11,16 Nevertheless, the specific association between nurses’ reflective practice patterns and their demonstrated caring behaviors remains theoretically unexplored, representing a critical knowledge gap in nursing science. This under-explored relationship warrants particular attention given its potential to inform both clinical training paradigms and patient-centered care models.
Social Cognitive Theory (SCT), recognized for its robust utility in explicating the relationships among personal, behavioral, and environmental factors within occupational settings, has emerged as a pivotal theoretical framework in the nursing management field.17,18 The SCT postulates that when individuals enhance their cognitive capacities and actively engage in reflective practices, their self-efficacy and confidence are significantly elevated, thereby promoting improved practical behaviors.19,20 Consequently, grounded in SCT, we hypothesize that psychiatric nurses’ reflective practice is significantly associated with their caring behaviors. Thus, this study aimed to classify latent profiles of reflective practice among psychiatric nurses and examine their effects on caring behaviors. Based on the theoretical, knowledge-based and practical gaps discussed in the aforementioned literature, the latent profiles of reflective practice among psychiatric nurses and its relationship with caring behaviors merit further exploration. Therefore, drawing on these premises, we derived three testable hypotheses in this study:
Hypothesis 1: The reflective practice among psychiatric nurses could be classified into different latent profiles based on dimensional scores. Hypothesis 2: The latent profiles of psychiatric nurses’ reflective practice vary according to demographic characteristics. Hypothesis 3: The identified profiles of reflective practice serve as predictive indicators for the caring behaviors among psychiatric nurses.
Materials and Methods
Study Design, Setting, and Participants
This study employed a cross-sectional design and recruited psychiatric nurses using a convenience sampling method. Participants were recruited from mental health treatment centers across ten hospitals in Sichuan Province, China, between January and March 2024. The specific details and results of the participant enrollment process are illustrated in Figure 1. The inclusion criteria for this study were: (1) registered nurses holding a valid national professional license, (2) having at least one year of clinical experience, and (3) providing informed consent to participate voluntarily. Nurses who were on leave (including medical, maternity, or personal leave) during the study period were excluded from participation.
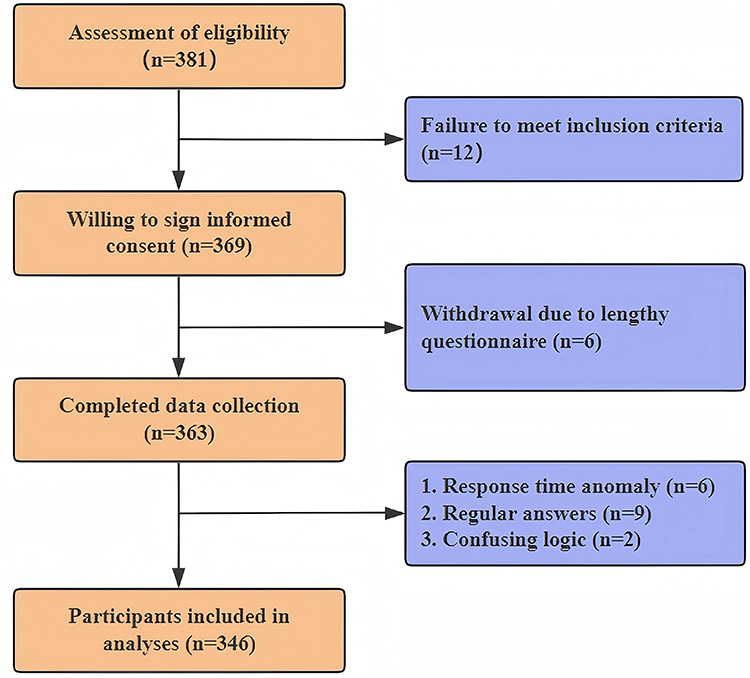 |
Figure 1 Flowchart of participant selection and inclusion. |
In cross-sectional study designs, a widely accepted guideline for sample size calculation recommends at least 10 events per predictor parameter to maintain model stability and ensure reliable estimation of regression coefficients.21 For this study, accounting for a potential 20% attrition rate with 12 candidate predictor variables, the minimum required sample size was determined to be 144 participants.
Measurements
Demographic Information Questionnaire
The structured questionnaire comprises eleven demographic variables: gender, age, marital status, hospital tiers, educational background, personnel attribution, monthly personal income, professional title, number of children, work experience (years), and rotational night shift.
Reflective Practice Questionnaire
This questionnaire, compiled by Priddis and Rogers22 and cross-culturally adapted into Chinese by Xue,23 was utilized to assess nurses’ reflective practice in this investigation. This 33-item instrument employs a 6-point Likert response format (1 = strongly disagree to 6 = strongly agree), organized across five distinct dimensions: “reflective practice skills and desire for improvement”, “self‐confidence”, “average job satisfaction”, “reflective practice acumen”, and “pressures from reflective practice”. The scale demonstrated excellent reliability in the Chinese adaptation (Cronbach’s α = 0.95).23 In the current sample, the scale maintained satisfactory internal consistency (Cronbach’s α = 0.970).
Caring Behaviors Inventory (CBI)
The CBI, originally developed by Wolf24 and subsequently revised by Da,25 was employed to evaluate nurses’ caring behaviors in this study. This 24-item instrument comprises three dimensions: “respectfulness and connectedness”, “knowledge and skill”, and “assurance”. Participants responded to items using a 6-point Likert scale anchored at 1 (never) and 6 (always), with higher composite scores indicating more frequent demonstrations of caring behaviors in clinical practice. A prior study on the validity and reliability of the CBI showed a Cronbach’s α of 0.977.25 In addition, this study revealed that the scale remained at a prominent level of reliability with a total Cronbach’s α of 0.971.
Data Collection
The data collection was conducted by six uniformly trained research assistants (designated nursing managers from participating clinical units) using the “Questionnaire Star” platform. To minimize potential social desirability bias, participants were assured of the anonymity and confidentiality of their responses by the research assistants, emphasizing that their answers would not affect their employment or evaluation. Potential participants accessed the survey through unique QR codes distributed via institutional WeChat groups, with mandatory electronic informed consent obtained through a digital interface that detailed study objectives, confidentiality measures, and participation requirements before questionnaire commencement. To ensure data quality, the platform incorporated multiple validation safeguards: (1) IP address restriction, avoiding duplicate submissions; (2) response time parameters (10–15 minutes); (3) mandatory item completion. A two-stage screening process was employed, combining automated exclusion of aberrant responses (regular response patterns, excessive length of time to fill in, or too short, or logical inconsistencies) with subsequent independent manual review by two researchers to confirm data validity before analytical processing.
Statistical Analysis
The latent profile analysis of reflective practice was conducted using Mplus 8.3, based on the scores of each dimension of the Reflective Practice Questionnaire, and the optimal number of profile classifications was selected by gradually increasing the profiles according to the fit indices test. Model fit was assessed using the Akaike information criterion (AIC), Bayesian information criterion (BIC), and sample-adjusted BIC (aBIC), with lower values indicating superior fit.26 Classification accuracy was evaluated via entropy, where values approaching 1 reflect higher precision. Additionally, the Lo-Mendell-Rubin likelihood ratio test (LMRT) and bootstrapped likelihood ratio test (BLRT) were employed to compare nested models (k vs k-1 classes), with p < 0.05 signifying that the k-class model provided a statistically better fit.27
Data were analyzed using SPSS 27.0 software. Continuous material was expressed as mean and standard deviation, while categorical variables were described using frequencies and percentages. The independent samples t-test and one-way analysis of variance (ANOVA) were implemented to detect differences between groups. Hierarchical linear regression was utilized to determine the effect of reflective practice on caring behaviors. P < 0.05 was considered statistically significant (two-sided).
Ethical Considerations
This study received ethical approval from the ethics committee of hospital (No. 20231846). All participants provided electronic informed consent after reviewing the study details. To ensure confidentiality, data were anonymized, encrypted, and accessible only to the research team. Nurse leaders involved in data collection were instructed not to influence responses, and participants were assured that their answers would not impact their employment or evaluations. These measures were implemented to maintain ethical integrity, protect privacy, and minimize bias.
Results
Demographic Characteristics of Participants
A total of 346 psychiatry nurses from secondary (61.3%) and tertiary (38.7%) hospitals were included in this study (Table 1). The sample was predominantly female (83.8%, n=290) compared to male (16.2%, n=56), with the majority aged 31–45 years (56.9%). In addition, most participants were married (72.0%) and held at least an undergraduate degree (76.9%). The workforce composition revealed three key characteristics: First, contractual employment predominated (83.8%), with junior professional titles being the most common (57.8%). Second, the majority fell within the mid-range income bracket of 5000–10000 Yuan monthly (64.2%). Regarding family structure, participants with one child represented the largest subgroup (42.2%), followed by those without children (35.5%). Work experience distribution showed two nearly equivalent cohorts: those with 1–10 years (48.6%) and 11–20 years (44.8%) of service. Notably, rotational night shift work was reported by most respondents (67.3%).
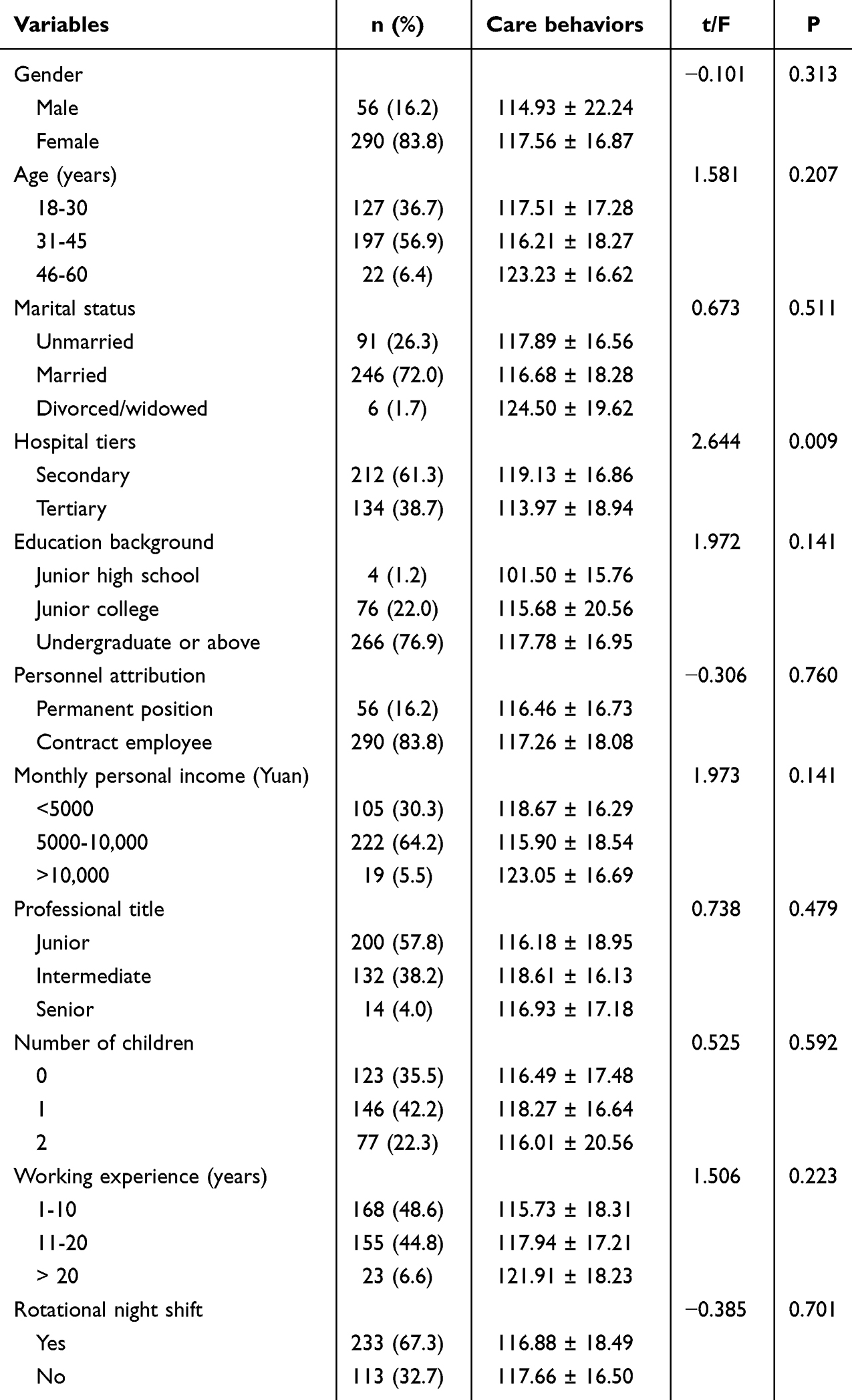 |
Table 1 Characteristics of Participants and Univariate Analysis of Caring Behaviors |
Latent Profile of Reflective Practice Among Psychiatry Nurses
Based on the dimensional scores of reflective practice among psychiatric nurses, we constructed five latent profile models (Table 2). Comparative analysis of model fit indices revealed that Model 3 demonstrated relatively lower AIC, BIC, and aBIC values, with an entropy of 0.914. Both LMRT and BLRT tests reached statistical significance, indicating that Model 3 showed significantly better fit than Models 1 and 2. However, although Models 4 and 5 exhibited lower AIC, BIC, and aBIC values compared to Model 3, along with higher entropy, their smallest profile proportions were below 5%, which might compromise statistical stability, potentially leading to over-fitting and reduced classification accuracy. Consequently, we selected the three-profile model as the optimal classification for psychiatric nurses’ reflective practice.
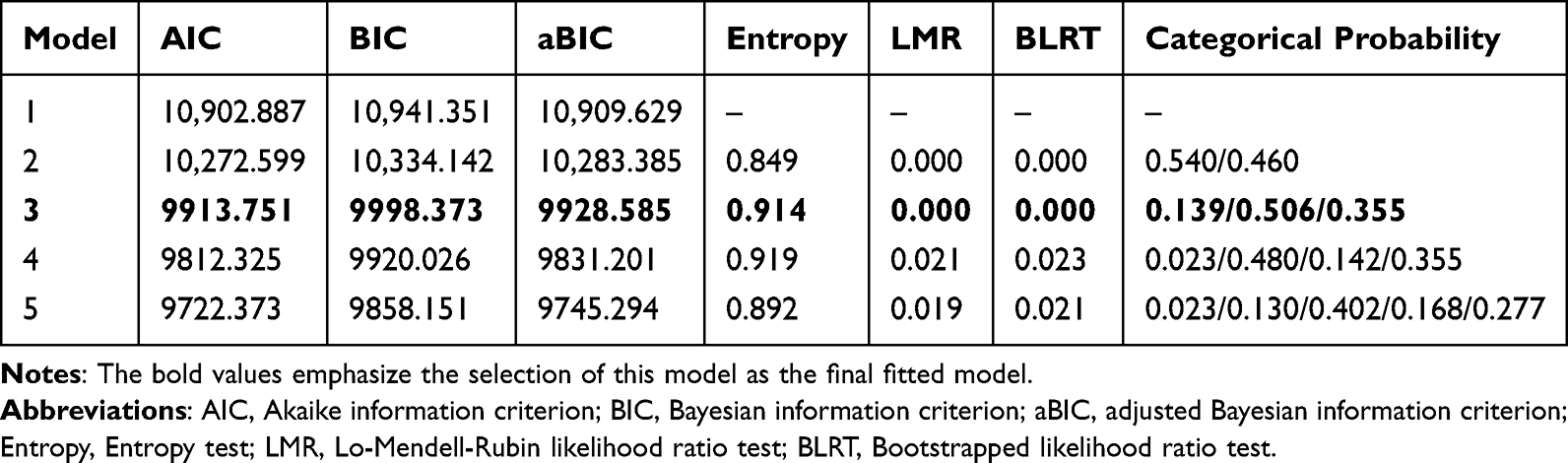 |
Table 2 Latent Profile Analysis of Reflective Practice Among Nurses with Fit Indices |
The five-dimensional scores corresponding to the three latent profiles of reflective practice among psychiatric nurses are detailed in Figure 2. According to the scoring criteria, each dimension of the reflective practice questionnaire has an ideal value, with scores closer to this ideal indicating better performance in that dimension. However, Profile 1 showed significantly lower mean scores across all dimensions compared to the ideal values and was markedly inferior to Profile 2 and Profile 3. Therefore, this group was defined as “Passive reflective participants”. In Profile 2, the scores for all dimensions were relatively close to the ideal level, leading to its designation as “Moderately balanced reflective practitioners”. Finally, Profile 3 demonstrated scores highly consistent with the ideal level and was thus labeled “High-achieving reflective leaders”. The proportions of Profiles 1, Profile 2, and Profile 3 in the total sample were 13.9% (n = 48), 50.6% (n = 175), and 35.5% (n = 123), respectively.
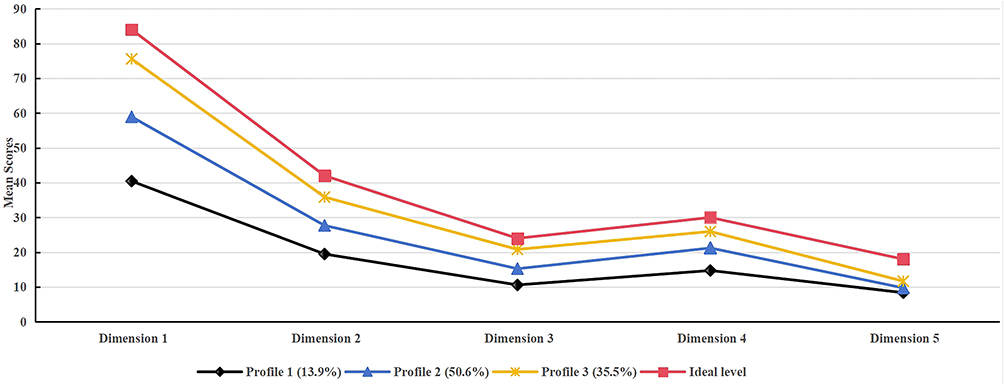 |
Figure 2 Latent profile analysis result of reflective practice. |
Demographic Variations in Latent Profiles of Reflective Practice
Demographic characteristics across the identified latent profiles of reflective practice among psychiatric nurses were compared using univariate analyses, as detailed in Table 3. Significant differences were observed in marital status, hospital tiers, educational background, and work experience (all P < 0.05). Specifically, Profile 3 comprised predominantly nurses from secondary hospitals, with higher proportions of married individuals and those with undergraduate or above and longer working experience. This profile also contained significantly more experienced nurses compared to Profile 1 and Profile 2. Moreover, no significant differences were found in gender, personnel attribution, monthly income, professional title, number of children, and rotational night shift status (all P > 0.05).
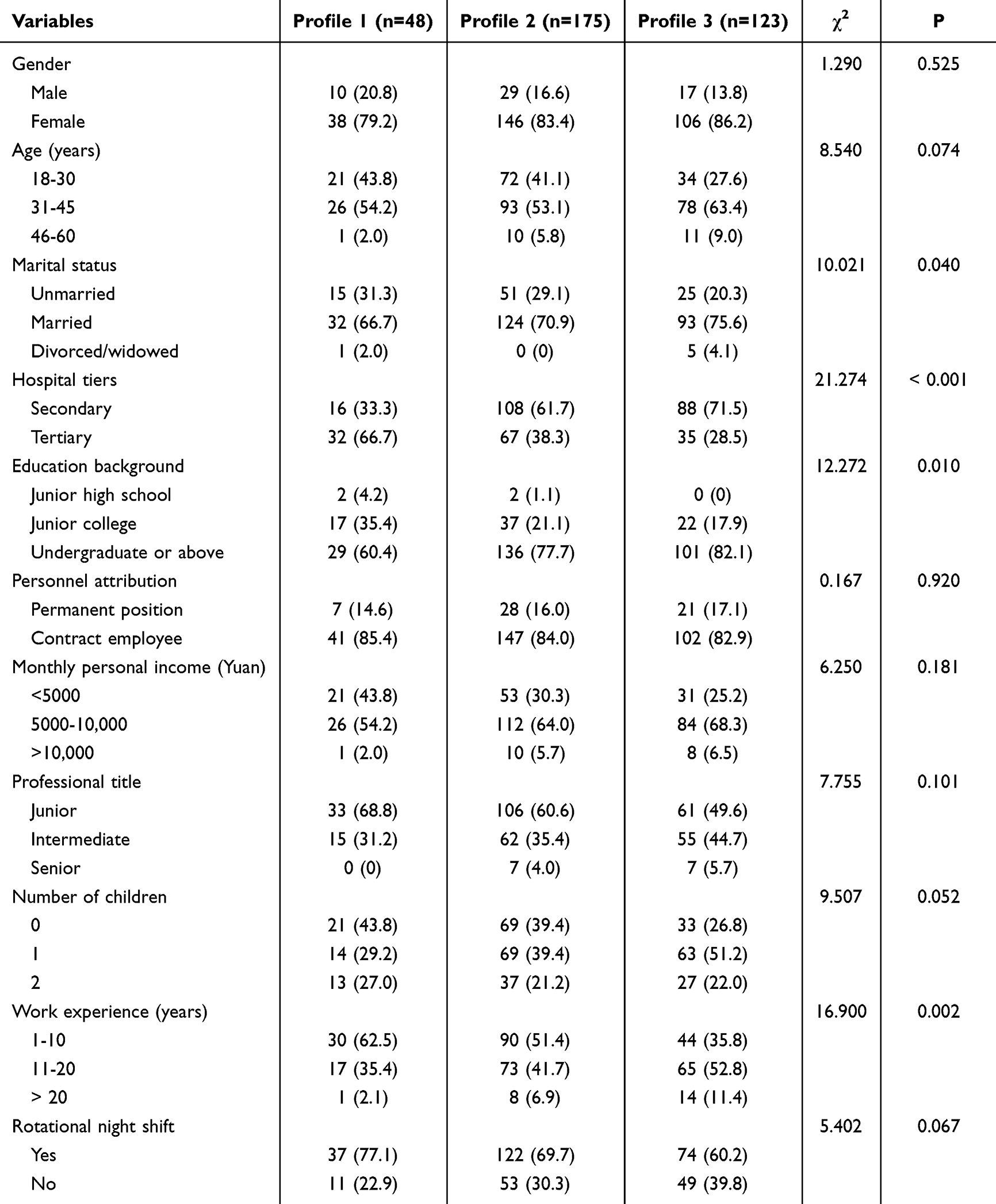 |
Table 3 Demographic Variations in Latent Profiles of Reflective Practice |
Comparison of caring Behaviors Among Psychiatry Nurses Across the Three Profiles
As shown in Table 4, significant differences in caring behaviors were observed across the three latent profiles (all P < 0.001). Profile 3 consistently demonstrated the highest scores across all dimensions, including respectfulness and connectedness, knowledge and skill, and assurance, resulting in the highest overall care behavior score. Profile 2 exhibited intermediate performance, while Profile 1 scored significantly lower in all dimensions (all LSD tests: P3 > P2 > P1).
 |
Table 4 Profiles Differences in Caring Behaviors |
Univariate Analysis and Hierarchical Linear Regression Analysis of Caring Behaviors Among Psychiatry Nurses
The univariate analysis (Table 1) revealed significant variations in hospital tiers in caring behaviors across different demographic characteristics. Specifically, nurses working in secondary hospitals demonstrated significantly higher caring behavior scores compared to those in tertiary hospitals (P < 0.05). Therefore, the hospital tiers were subsequently included in the hierarchical regression analysis as a covariate to examine the independent effect of profile membership reflective practice on caring behaviors. Moreover, no statistically significant differences were observed based on gender, age, marital status, educational background, personnel attribution, monthly income, professional title, number of children, work experience, and rotational night shift status (all P > 0.05).
A hierarchical linear regression analysis was performed to examine the effect of reflective practice profiles on psychiatric nurses’ caring behaviors. Hospital tiers and latent profiles of reflective practice were entered as dummy-coded independent variables using the first term as a reference, and caring behaviors as the dependent variable. The results indicated that tertiary hospitals showed a significant negative association with caring behaviors in Model 1 (β = −0.141, p = 0.009). Moreover, the inclusion of latent profiles of reflective practice in Model 2 substantially enhanced the model’s explanatory power, accounting for an additional 42.0% of the variance in caring behaviors (ΔR2 = 0.420). Specifically, compared to Profile 1, Profile 2 (β = 0.430, p < 0.001) and Profile 3 (β = 0.914, p < 0.001) demonstrated significantly higher caring behavior, with Profile 3 exhibiting the most pronounced effect size (Table 5).
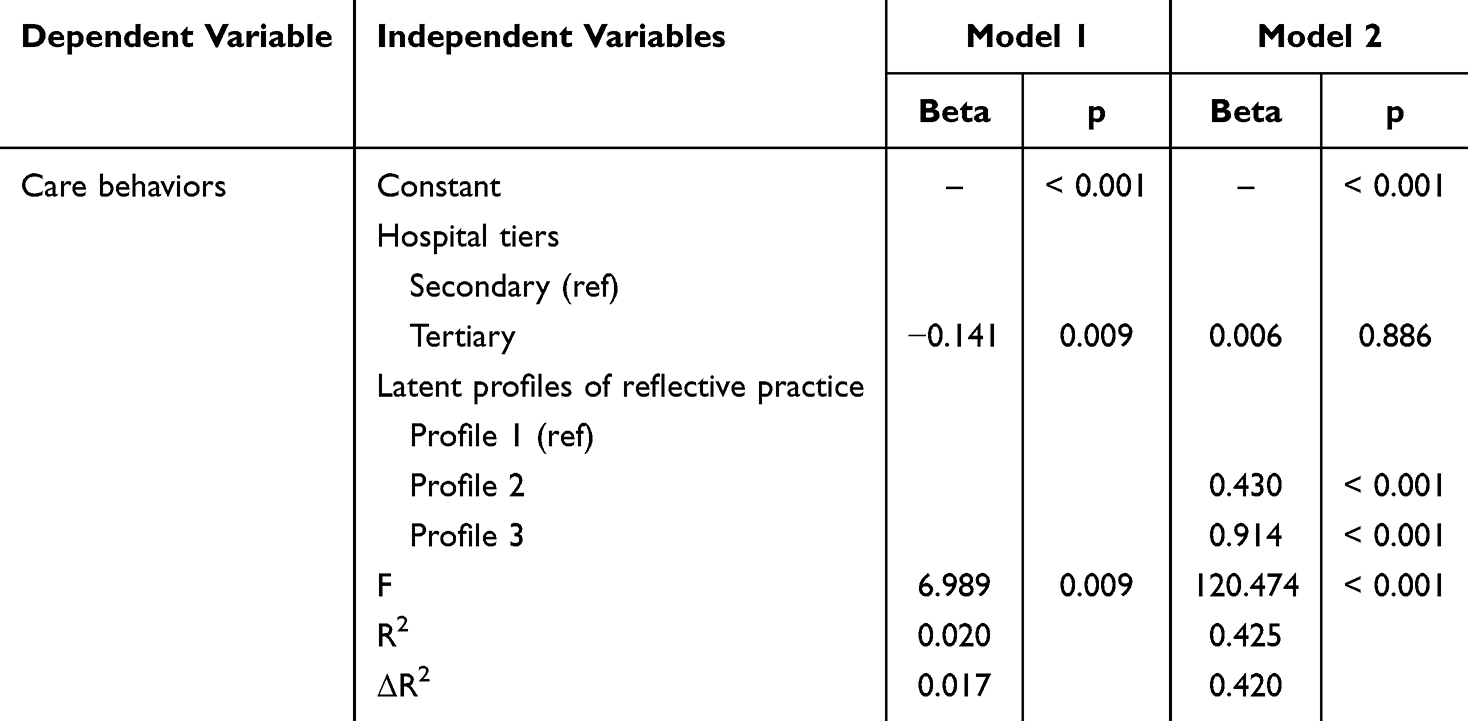 |
Table 5 The Relationship Between Different Latent Profiles of Reflective Practice and Caring Behaviors in Hierarchical Linear Regression |
Discussion
This study identified different latent profiles of reflective practice among psychiatry nurses and examined their relationship with caring behaviors. To our knowledge, this study represents the first empirical investigation examining the association between latent profiles of reflective practice and caring behaviors among psychiatric nurses. The current findings provide valuable insights for hospital executives to systematically identify distinct patterns of reflective practice in psychiatry nurses. More importantly, these evidence-based profiles may inform the development of targeted organizational interventions aimed at enhancing psychiatry nurses’ caring behaviors outcomes in clinical settings.
Our findings revealed that reflective practice of psychiatry nurses can be categorized into three latent profiles: “Passive reflective participants” (13.9%), “Moderately balanced reflective practitioners” (50.6%), and “High-achieving reflective leaders” (35.5%). The results indicated that psychiatric nurses demonstrated promising reflective practice, as “moderately balanced practitioners” and “high-achieving reflective leaders” comprising 86.1% of the sample. This robust distribution suggests an established culture of reflection within psychiatric nursing, likely stemming from the specialty’s unique demands for adaptive clinical decision-making and emotional regulation in complex mental health scenarios. The high prevalence of excellent reflective practitioners may reflect effective institutional support systems, including regular clinical supervision and mandatory case discussions that are more intensive than in general nursing settings.28 These results indicate that psychiatric nursing has potentially developed a self-reinforcing ecosystem for cultivating reflective practice, though the “passive reflective participants” highlight that some targeted interventions should be established to achieve universal reflective competence.
In our study, the latent profiles of reflective practice among psychiatric nurses demonstrated statistically significant differences in some demographic characteristics, including marital status, hospital tiers, educational background, and work experience. Specifically, psychiatric nurses who are married, work in secondary hospitals, have a bachelor’s degree or above, and possess relatively long work experience are more likely to be identified as “high-achieving reflective leaders”. Earlier research has revealed that married individuals tend to exhibit enhanced emotional maturity and superior conflict-resolution competencies, which are transferable to clinical practice settings.29 The marital relationship provides psychiatric nurses with robust social support, which effectively buffers occupational stress and preserves cognitive resources for reflective practice, thereby facilitating sustained engagement in both reflective activities and quality improvement initiatives.23 Moreover, psychiatric nurses in secondary hospitals manifest superior reflective practice primarily due to more favorable workload conditions and lower levels of burnout. Compared to tertiary hospitals, secondary facilities manage a lower proportion of acute cases, resulting in significantly reduced quantitative and emotional demands on nurses. This, in turn, may lead to lower levels of emotional exhaustion among nursing staff. This workload advantage preserves both temporal availability and cognitive-psychological capacity for systematic reflective practice.30 Furthermore, tertiary hospitals often adopt a “technological-medical” orientation, emphasizing acute crisis management through rapid diagnosis and pharmacological intervention. This focus may sideline the relationship-based, time-intensive nature of reflective practice. In contrast, secondary hospitals typically prioritize stable patient management and rehabilitation within a more holistic care paradigm, which naturally supports reflective dialogue and ongoing professional development. In addition, the superior reflective practice performance among psychiatric nurses holding bachelor’s degrees or higher likely stems from the formative influence of advanced education. University-level training provides systematic instruction in critical thinking methodologies and evidence-based practice principles.31 This educational foundation enables more effective translation of theoretical knowledge into clinical practice, as manifested in heightened abilities to analyze complex cases and implement reflective solutions.32 Finally, the enhancement of reflective practice capacity with increasing clinical experience among psychiatric nurses primarily stems from the synergistic interaction between accumulated case exposure and professional cognitive development. As work experience grows, nurses establish comprehensive clinical pattern recognition databases through repeated management of diverse psychiatric presentations, providing a robust comparative foundation for in-depth reflection.6
Our findings revealed that reflective practice was positively associated with psychiatric nurses’ caring behaviors. This positive correlation could be explained through interconnected cognitive and behavioral mechanisms. Reflective practice embodies multiple attributes, including pro-activity, critical thinking, and openness.10 Through this process, psychiatric nurses engage in continuous self-evaluation and adjustment, enabling them to develop more effective patient-centered strategies and improve clinical decision-making accuracy.13 Furthermore, reflective practice also enhances individuals’ capacity for compassionate care by strengthening their emotional regulation abilities. Previous studies have confirmed that reflective practitioners exhibit stronger neural connectivity related to empathy.32 These effects are particularly prominent in psychiatric settings due to the specialty’s unique demands for therapeutic alliance building and high-stakes emotional labor. Consequently, psychiatric nurses should pay more attention to reflective practice in clinical settings by engaging in structured activities such as maintaining reflective writing and participating in case-based discussions. These methods facilitate the systematic consolidation of clinical experience, cultivate critical thinking competencies, and promote the continuous development of evidence-based, patient-centered care strategies, ultimately enhancing patient outcomes.
Limitations
Our findings should be interpreted considering several limitations. Firstly, the cross-sectional design inherently constrains the ability to establish causal relationships between reflective practice and caring behaviors. Secondly, the reliance on convenience sampling may compromise the external validity of the findings, as participants were recruited exclusively from specific hospitals in Sichuan Province, China, potentially limiting their representativeness of psychiatric nurses in other regions or healthcare settings. Finally, the utilization of self-report measures for assessing variables could introduce recall bias due to subjective reporting. Future research should consider employing a longitudinal study design or experimental interventions to investigate the sustained effects of reflective practice on the caring behaviors of psychiatric nurses over time. Additionally, qualitative approaches could be leveraged to explore the experiences and perceptions of psychiatric nurses regarding reflective practice and its influence on their caring behaviors.
Implications for Practice
The findings underscore the pivotal role of reflective practice in enhancing psychiatric nurses’ caring behaviors, which are fundamental to fostering therapeutic relationships and improving mental health outcomes. The identification of three distinct reflective practice profiles highlights the need for tailored professional development programs that address varying levels of reflective competency. For nursing practice, these results emphasize the importance of integrating structured reflective exercises, such as guided debriefings, peer discussions, or reflective writing, into routine clinical training. Healthcare institutions should prioritize fostering a culture of continuous reflection by providing dedicated time and resources for nurses to engage in reflective activities. Additionally, mentor-ship programs pairing “high-achieving reflective leaders” with less experienced nurses could facilitate skill transfer and strengthen team-wide reflective capacities.
From a policy perspective, incorporating reflective practice assessments into nurse competency evaluations may help identify gaps and guide targeted interventions. Future research should explore longitudinal effects of reflective practice enhancement programs on both nurse well-being and patient outcomes, particularly in high-stress psychiatric settings where emotional and cognitive resilience are critical. By systematically cultivating reflective practice, healthcare systems can optimize caring behaviors, ultimately advancing recovery-oriented care in mental health nursing.
Conclusions
In conclusion, the reflective practice of psychiatric nurses could be classified into three latent profiles: “passive reflective participants”, “moderately balanced reflective practitioners”, and “high-achieving reflective leaders”. In addition, the different categories of reflective practice exerted a significant positive relationship on the psychiatric nurses’ caring behaviors. To maximize these benefits, targeted interventions should be prioritized for nurses who are most at risk of low reflective practice, specifically junior nurses, those working in tertiary hospital settings, unmarried nurses, and those without a bachelor’s degree or higher. For these groups, nursing leadership should implement structured mentor-ship programs specifically pairing them with “high-achieving reflective leaders,” integrate brief, structured reflective exercises into shift routines, and provide training to enhance self-awareness. Furthermore, healthcare institutions should cultivate a supportive environment that encourages continuous reflection through peer discussions, debriefing sessions, and recognition of reflective excellence.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Ethics Committee of West China Hospital, Sichuan University (No. 20231846). This study complies with the Declaration of Helsinki. In this study, we adhered to ethical standards. Electronic written informed consent was obtained from participants before the start. They fully understood the study details through an electronic form and provided their consent electronically. During the process, strict confidentiality was maintained. Data collected were encrypted and access was restricted to the research team to ensure privacy protection.
Acknowledgment
Thanks to everyone for their help in study design, questionnaire distribution, recycling, input, and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for conducting this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Maity K, Lal P, Jyoti S, et al. Humanistic and holistic strategies for combating mental health sequelae in the elderly during the post-COVID Era. Ann Neurosci. 2024;31(4):292–12. doi:10.1177/09727531231208292
2. Knaak S, Mantler E, Szeto A. Mental illness-related stigma in healthcare: barriers to access and care and evidence-based solutions. Healthcare Manage Forum. 2017;30(2):111–116. doi:10.1177/0840470416679413
3. Labrague LJ, Obeidat AA. Pedagogical approaches to foster caring behaviors among nursing students: a scoping review. Nurs Educ Today. 2025;146(106547):106547. doi:10.1016/j.nedt.2024.106547
4. Salberg J, Hursti T, Ekselius L, Öster C. Evaluation of steps towards recovery – attitudes towards and experiences of a recovery-oriented nursing programme as an approach to evidence-based nursing practice in psychiatric in-patient care. Nordic J Psychiatry. 2025;79(4):280–287. doi:10.1080/08039488.2025.2492157
5. Tordoir A, van Laarhoven V, van Duijnhoven N, et al. The psychiatric mental health nurse practitioner in the general practice: a realist evaluation multiple case study. BMC Primary Care. 2025;26(1):136. doi:10.1186/s12875-025-02844-8
6. Mukaihata T, Kato Y, Swa T, Fujimoto H. Work engagement of psychiatric nurses: a scoping review. BMJ Open. 2024;14(4):e081941. doi:10.1136/bmjopen-2023-081941
7. Turner K, Bjarnadottir R, Jo A, et al. Patient falls and injuries in U.S. psychiatric care: incidence and trends. Psychiatric Serv. 2020;71(9):899–905. doi:10.1176/appi.ps.202000004
8. Foster K, Roche M, Giandinoto J-A, Furness T. Workplace stressors, psychological well-being, resilience, and caring behaviours of mental health nurses: a descriptive correlational study. Int J Mental Health Nurs. 2020;29(1):56–68. doi:10.1111/inm.12610
9. Yu M, Wang H, Wu Y, et al. The influence of emotional intelligence on psychiatric nurses’ care behavior, and the chain mediating role of compassion fatigue and perception of management. J Psychosocl Nurs Mental Health Serv. 2025;63(2):35–43. doi:10.3928/02793695-20241101-02
10. Patel KM, Metersky K. Reflective practice in nursing: a concept analysis. Int J Nurs Knowledge. 2022;33(3):180–187. doi:10.1111/2047-3095.12350
11. Zia T, Sabeghi H, Mahmoudirad G. Problem-based learning versus reflective practice on nursing students’ moral sensitivity. BMC Nurs. 2023;22(1):215. doi:10.1186/s12912-023-01377-8
12. Kapachika M, Baluwa MA, Mbakaya BC, Mhango L, Bvumbwe T. Knowledge, practices and barriers of reflective practice among undergraduate nursing and midwifery students in malawi. Adv Med Educ Prac. 2025;16:825–836. doi:10.2147/AMEP.S507766
13. Tolosa‐Merlos D, Moreno‐Poyato AR, González‐Palau F, Pérez‐Toribio A, Casanova‐Garrigós G, Delgado‐Hito P, MiRTCIME.CAT Working Group. Exploring the therapeutic relationship through the reflective practice of nurses in acute mental health units: a qualitative study. J Clin Nurs. 2023;32(1–2):253–263. doi:10.1111/jocn.16223
14. Weis J, Zoffmann V, Greisen G, Egerod I. The effect of person-centred communication on parental stress in a NICU: a randomized clinical trial. Acta paediatrica. 2013;102(12):1130–1136. doi:10.1111/apa.12404
15. Bembridge E, Crowfoot G, Wilson R, Reis J. Digital reflective practice among new graduate nurses - A scoping review. Nurse Education Today. 2025;150(106688):106688. doi:10.1016/j.nedt.2025.106688
16. Ibrahim Khalil A, Abou Hashish E. Exploring how reflective practice training affects nurse interns’ critical thinking disposition and communication skills. Nurs Manage. 2022;29(5):20–26. doi:10.7748/nm.2022.e2045
17. Mahdizadeh S-M, Sany SBT, Sarpooshi DR, Jafari A, Mahdizadeh M. Predictors of preventive behavior of nosocomial infections in nursing staff: a structural equation model based on the social cognitive theory. BMC Health Serv Res. 2021;21(1):1187. doi:10.1186/s12913-021-07205-6
18. She R, Chen X, Li L, Li L, Huang Z, Lau JTF. Factors associated with behavioral intention of free and self-paid severe acute respiratory coronavirus virus 2 (SARS-CoV-2) vaccination based on the social cognitive theory among nurses and doctors in China. Infect Control Hosp Epidemiol. 2022;43(5):609–615. doi:10.1017/ice.2021.201
19. Xu Z, Zhao B, Zhang Z, et al. Prevalence and associated factors of secondary traumatic stress in emergency nurses: a systematic review and meta-analysis. Euro J Psychotraumatol. 2024;15(1). doi:10.1080/20008066.2024.2321761
20. Zhao J, Wang Y, Xiao B, et al. Behaviors and influencing factors of Chinese oncology nurses towards hospice care: a cross-sectional study based on social cognitive theory in 2022. BMC Palliative Care. 2024;23(1):53. doi:10.1186/s12904-024-01385-8
21. Noordzij M, Tripepi G, Dekker FW, Zoccali C, Tanck MW, Jager KJ. Sample size calculations: basic principles and common pitfalls. Nephrol Dialysis Transplant. 2010;25(5):1388–1393. doi:10.1093/ndt/gfp732
22. Priddis L, Rogers SL. Development of the reflective practice questionnaire: preliminary findings. Reflective Pract. 2018;19(1):89–104. doi:10.1080/14623943.2017.1379384
23. Xu L, Lin L, Guan A, et al. Factors associated with reflective practice among specialist nurses in China: a latent profile analysis. Nurs Open. 2024;11(12):e70114. doi:10.1002/nop2.70114
24. Wolf ZR, Colahan M, Costello A, Warwick F. Relationship between nurse caring and patient satisfaction. Medsurg Nurs. 1998;7(2):99.
25. Chen JY, Chen HF, Wang XH, Zong QZ, Yao ZZ. Moral sensitivity and caring behavior in nursing interns: the mediating role of empathy. Front Public Health. 2024;12:1360940. doi:10.3389/fpubh.2024.1360940
26. Vrieze SI. Model selection and psychological theory: a discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychological Methods. 2012;17(2):228–243. doi:10.1037/a0027127
27. Nylund-Gibson K, Garber AC, Carter DB, et al. Ten frequently asked questions about latent transition analysis. Psychological Methods. 2023;28(2):284–300. doi:10.1037/met0000486
28. Cadorette J, McCurry M, Danells Chin E. Reflective transition practice model: the new graduate registered nurse. Nurs Sci Quarterly. 2023;36(3):282–291. doi:10.1177/08943184231169763
29. Li YM, Luo YF. The influencing factors of clinical nurses’ problem solving dilemma: a qualitative study. Int J Qualitat Stud Health Well-Being. 2022;17(1):2122138. doi:10.1080/17482631.2022.2122138
30. Cho H, Steege LM, Pavek KU. Psychological detachment from work during nonwork time as a moderator and mediator of the relationship of workload with fatigue and sleep in hospital nurses. Sleep Health. 2024;10(5):558–566. doi:10.1016/j.sleh.2024.05.005
31. Li H, Xu R, Gao D, et al. Evidence-based practice attitudes, knowledge and skills of nursing students and nurses, a systematic review and meta-analysis. Nurs Educ Prac. 2024;78(104024). doi:10.1016/j.nepr.2024.104024
32. Mösler T, Poppek S, Leonhard C, Collet W. Reflective skills, empathy, wellbeing, and resilience in cognitive-behavior therapy trainees participating in mindfulness-based self-practice/self-reflection. Psychol Rep. 2023;126(6):2648–2668. doi:10.1177/00332941221094482
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.