Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Relationship Between Monocyte-to-High-Density Lipoprotein Cholesterol Ratio and Visceral Obesity in Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Authors Hu Y ![]() , Zheng J, Xing Y, Song Y, Wu X
, Zheng J, Xing Y, Song Y, Wu X ![]()
Received 1 October 2025
Accepted for publication 28 November 2025
Published 22 December 2025 Volume 2025:18 Pages 4755—4765
DOI https://doi.org/10.2147/DMSO.S518916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Ye Hu,1 Jia Zheng,2 Yubo Xing,1 Yingxiang Song,1 Xiaohong Wu1
1Geriatric Medicine Center, Department of Endocrinology, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, 310014, People’s Republic of China; 2Center for General Practice Medicine, Department of Nutrition, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, 310014, People’s Republic of China
Correspondence: Xiaohong Wu, Geriatric Medicine Center, Department of Endocrinology, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, 310014, People’s Republic of China, Tel/Fax +86-579-85893937, Email [email protected]
Purpose: The study aimed to explore the relationship between the monocyte-to-high-density lipoprotein cholesterol ratio (MHR) and visceral fat area (VFA) in patients with type 2 diabetes mellitus (T2DM).
Patients and Methods: A total of 2156 patients with T2DM who received medical treatment at Zhejiang Provincial People’s Hospital participated in this study. Patients were categorized into two groups based on VFA: the increased VFA group (VFA ≥ 100 cm2, n = 1091) and the normal VFA group (VFA < 100 cm2, n = 1065). Biochemical indicators were measured via blood tests, whereas VFA was measured using bioelectrical impedance analysis. Spearman correlation and linear regression analysis were conducted to examine the association between MHR and VFA. Receiver operating characteristic (ROC) curves for predicting the VFA were constructed, and areas under the ROC curves were estimated.
Results: MHR level was significantly higher in the increased VFA group (p < 0.001) than in the normal VFA group. Spearman correlation analysis showed a positive association between VFA and MHR (r = 0.366, p < 0.001). Multivariate linear regression analysis revealed that elevated MHR is an independent factor for increased VFA (β = 20.64, 95% CI 13.46– 27.82, p < 0.001). After stratification by hemoglobin A1c levels and diabetes duration, MHR remained independently associated with VFA. ROC analysis indicated that MHR has a predictive effect on VFA, with an area under the curve of 0.708 (specificity = 58%, sensitivity = 73%).
Conclusion: MHR levels are associated with visceral fat area in patients with T2DM, which has a modest predictive value, and it may be useful in detecting visceral obesity.
Keywords: visceral fat area, monocyte-to-high-density lipoprotein cholesterol ratio, type 2 diabetes mellitus, abdominal fat distribution
Introduction
In recent years, the prevalence of type 2 diabetes mellitus (T2DM) has gradually increased, with obesity becoming a significant risk factor. Obesity, particularly visceral obesity, is closely associated with many diseases that pose serious health threats to humans.1,2 Visceral fat accumulation is a key risk factor contributing to insulin resistance and impaired glucose metabolism, which is often accompanied by increased cytokines and other inflammatory markers.3,4
Monocytes are key cells that secrete pro-inflammatory and pro-oxidative factors, and their increase is linked to subclinical inflammation.5 High-density lipoproteins (HDLs) play an anti-inflammatory role by inhibiting monocyte activity and preventing their differentiation into macrophages.6 Several studies have shown that monocytes and monocyte-derived markers are associated with inflammatory conditions.7–9 HDL-based markers have also been linked to various inflammatory conditions, including hypertension, hepatic steatosis, thyroiditis, and metabolic syndrome.10,11
In recent years, the peripheral blood monocyte-to-high-density lipoprotein cholesterol ratio (MHR), a novel inflammatory marker, has garnered significant interest owing to its association with various metabolic diseases, including atherosclerosis.12 Research has demonstrated that both obesity and T2DM are linked to a high inflammatory burden.13–15 Particularly, visceral obesity leads to adipose tissue dysfunction and compromised adipocytokine secretion, which triggers oxidative stress and inflammatory response, ultimately inducing insulin resistance and T2DM.16–18 Additionally, obesity, particularly visceral obesity, places the body in a state of chronic inflammation, which aggravates insulin resistance in patients with T2DM, increases the risk of vascular complications, and elevates the mortality of patients.19 Therefore, we hypothesize that MHR acts as a predictor of visceral obesity.
Previous studies have established that the MHR is significantly elevated in patients with metabolic syndrome and is closely associated with conditions like obesity and polycystic ovarian syndrome.20,21 However, the relationship between MHR and visceral obesity in patients with T2DM, as well as its predictive role, have not been explored. This distinction is critical because T2DM confers a disproportionately higher risk of cardiovascular disease, and visceral fat accumulation is a key driver of this risk, independent of general obesity.22 The prevalence of T2DM and visceral obesity is constantly increasing worldwide, in China alone, the prevalence of diabetes has surpassed 11%.23 Therefore, identifying a simple, cost-effective biomarker like MHR that can reflect visceral fat area (VFA) in T2DM patients holds significant practical value. It could aid in early risk stratification, allowing for more targeted interventions in resource-limited settings. This study analyzed the correlation between MHR levels and VFA in patients with T2DM and evaluated the predictive value of MHR on visceral obesity.
Methods
Study Design and Participants
This cross-sectional study analyzed the relationship between MHR levels and visceral obesity. Our research team had previously explored the association between thyroid autoimmunity and visceral fat distribution in T2DM patients within a similar but very small sample size population.24 The present study extends this line of inquiry by focusing on a novel inflammatory marker, MHR, which has not been previously examined in relation to visceral obesity in T2DM patients in our cohort.
In this study, a total of 2156 patients with T2DM who received medical treatment at Zhejiang Provincial People’s Hospital between July 2020 and July 2023 were included. All participants provided complete questionnaire data, underwent physical examinations, and completed laboratory assessments.
The inclusion criteria were as follows: (1) age ≥ 18 years; (2) diagnosis of T2DM based on the 2020 American Diabetes Association (ADA) Standards of Medical Care in Diabetes.
The exclusion criteria were as follows: (1) acute diabetic complications, such as ketoacidosis, hyperosmolar hyperglycemia state, and acute infections; (2) history of hematological disorders; (3) history of malignant tumors; (4) having hyperthyroidism or hypothyroidism; (5) currently taking lipid-lowering therapy, GLP-1RA, SGLT2i, thiazolidinediones, systemic steroids, and thyroid medications; (6) severe dysfunction of the heart, liver, or kidneys; (7) pregnancy or lactation. The screening process is shown in Figure 1.
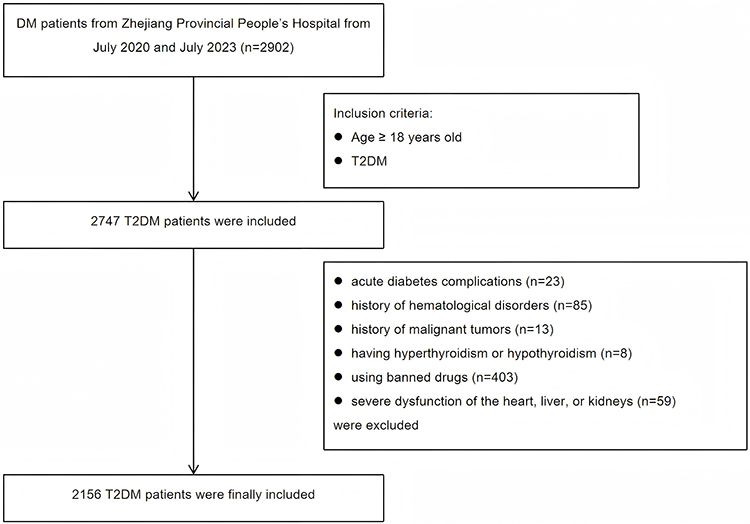 |
Figure 1 Flow chart of study. |
Data Collection
Demographic and clinical data were collected using a standardized questionnaire, including age, sex, T2DM duration, medical history, medication use, and lifestyle factors such as smoking and alcohol consumption. Anthropometric measurements (height, weight, waist circumference, hip circumference) and blood pressure were recorded. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2).
Laboratory indicators were based on early-morning venous blood after an 8 hours fast, and the detection items included: white blood cell count (WBC), monocyte count (MONO), hemoglobin (Hb), platelet count (PLT), fasting blood glucose (FBG), fasting insulin (FINS), glycated hemoglobin (HbA1c), lipid profile (total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C)), liver and renal function markers (albumin (ALB), aspartate aminotransferase (AST), alanine transaminase (ALT), alkaline phosphatase (ALP), blood urea nitrogen (BUN), serum creatinine (Scr)), uric acid (UA), and thyroid function indicators (free thyroxine (FT4), free triiodothyronine (FT3), and thyroid stimulating hormone (TSH)). Insulin resistance was estimated using the homeostasis model assessment (HOMA-IR) formula: FINS (mU/L) × FBG (mmol/L) / 22.5. There was missing data on ALP for 56 participants and missing data on AST for 54 participants. We used the random forest method for imputation. The important research indicators were complete.
VFA and subcutaneous fat area (SFA) were measured using bioelectrical impedance analysis (BIA) with the DUALSCAN HDS-2000. The measurement was conducted in the morning after an overnight fast, with participants in a supine position, having emptied their bladder, and was performed by the same nurse using the same equipment. Based on the VFA, participants were divided into two groups: the increased VFA group (VFA ≥ 100 cm2, n = 1091) and the normal VFA group (VFA < 100 cm2, n = 1065).
Statistical Analysis
Data distribution was assessed using the Kolmogorov–Smirnov test. Normally distributed continuous variables were expressed as mean ± standard deviation, while non-normally distributed variables were reported as median (interquartile range). Group comparisons were performed using Student’s t-test or Mann–Whitney U-test, as appropriate. Categorical variables were compared using chi-square tests. The relationship between MHR and VFA was analyzed using Spearman correlation analysis. Univariate and multivariate linear regression models were constructed to identify factors associated with VFA. Meanwhile, two linear regression models were performed to adjust for confounding factors. Model 1 adjusted for age and sex. Model 2 further adjusted for drinking habits, and levels of waist circumference, SFA, ALT, Scr, TG, FT3. Subgroup analyses were conducted based on the duration of diabetes (< 10 vs ≥10 years) and HbA1c levels (< 7% vs ≥ 7%) to assess the consistency of the MHR-VFA association. Receiver operating characteristic (ROC) curves for predicting the VFA were constructed, and areas under the ROC curves were estimated.
Statistical analyses were conducted using SPSS software (version 26.0; IBM Corp., Armonk, NY, USA) and R software (version 4.1.0; R Foundation for Statistical Computing, Auckland, New Zealand). R packages, including ggplot2, mice, survival, missForest, VIM, Hmisc, rms, regplot, tableone, and glmnet, were used for data analysis and visualization. Statistical significance was set at P<0.05 for all tests.
Results
Participant Clinical Characteristics
An overview of the study characteristics of the two groups was presented in Table 1. In contrast to the T2DM without visceral obesity group, smoking and drinking habit incidences were significantly higher in the T2DM with visceral obesity group (39.32% vs 26.29% [p < 0.001] and 44.55% vs 30.80% [p < 0.001], respectively). The indices of blood pressure, BMI, waist circumference, SFA, HOMA-IR, FBG, HbA1c, ALT, AST, ALP, ALB, Scr, UA, TG, FT3, TSH and MHR were significantly higher in the T2DM with visceral obesity group than those in the T2DM without visceral obesity group (p < 0.05); conversely, HDL-C, age and duration were significantly lower (p < 0.05). No significant differences were observed in the levels of BUN, TC, LDL-C, FT4 and PLT between the two groups.
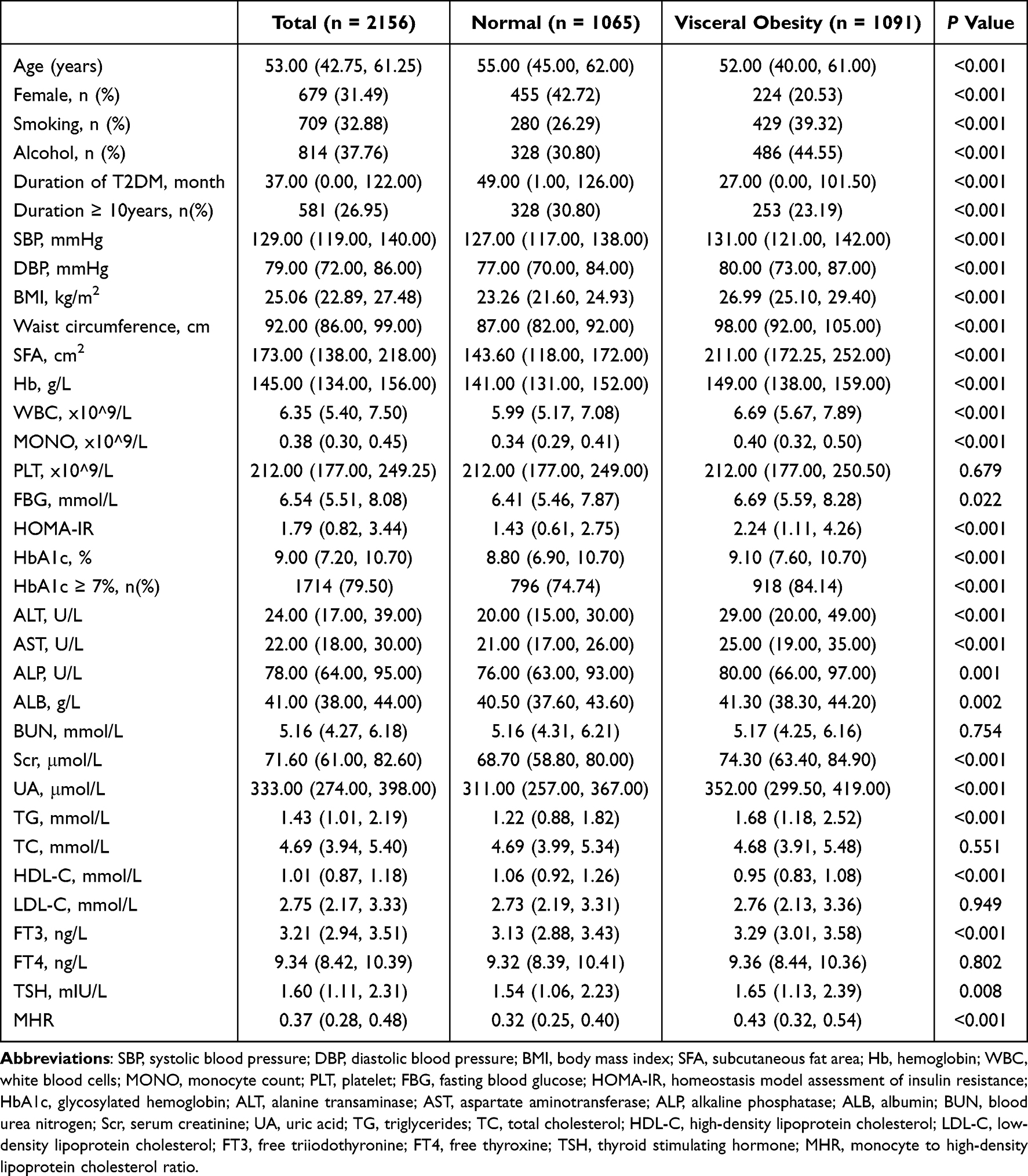 |
Table 1 Clinical Characteristics of T2DM Patients with and without Visceral Obesity |
Correlations Between MHR and VFA
To further assess the relationship between MHR and visceral obesity, we analyzed the correlation between VFA and MHR. The Spearman correlation analysis indicated that an increased MHR was significantly positively correlated with VFA (r = 0.366, p < 0.001) (Figure 2).
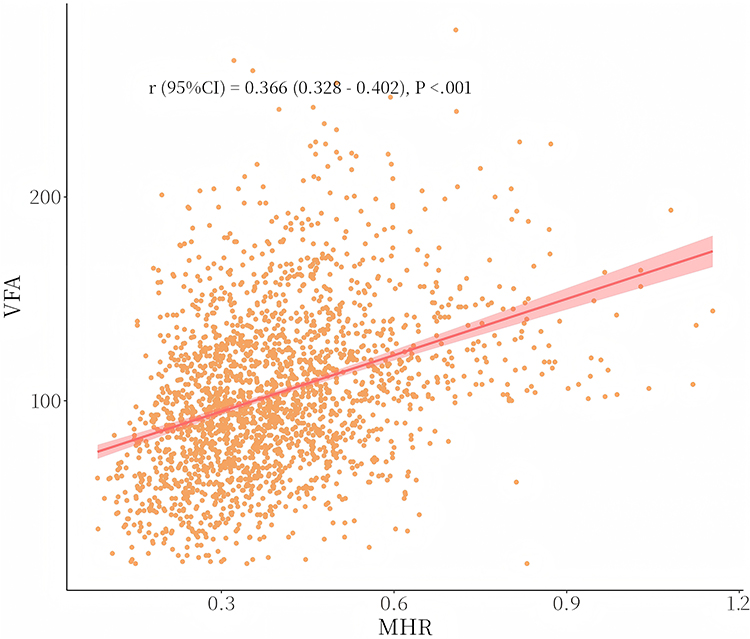 |
Figure 2 The correlations between MHR and VFA: an increased MHR was significantly positively correlated with VFA (r = 0.366, p < 0.001). |
Association Between the MHR and VFA in Patients with T2DM
We conducted a univariate linear regression analysis to assess the variables influencing visceral obesity in patients with T2DM. Using VFA as the dependent variable, the independent variables were sequentially screened (Table 2). Variables with p < 0.05, including age, sex, smoking and drinking habits, duration of T2DM, and levels of HbA1c, MHR, SBP, DBP, BMI, waist circumference, SFA, FBG, ALT, AST, ALB, Scr, UA, TG, FT3, and TSH, were included in the multivariate linear regression analysis. The multiple linear regression model revealed that elevated MHR was an independent factor for increased VFA (β = 20.64, 95% confidence interval [CI] 13.46–27.82, p < 0.001) (Table 3).
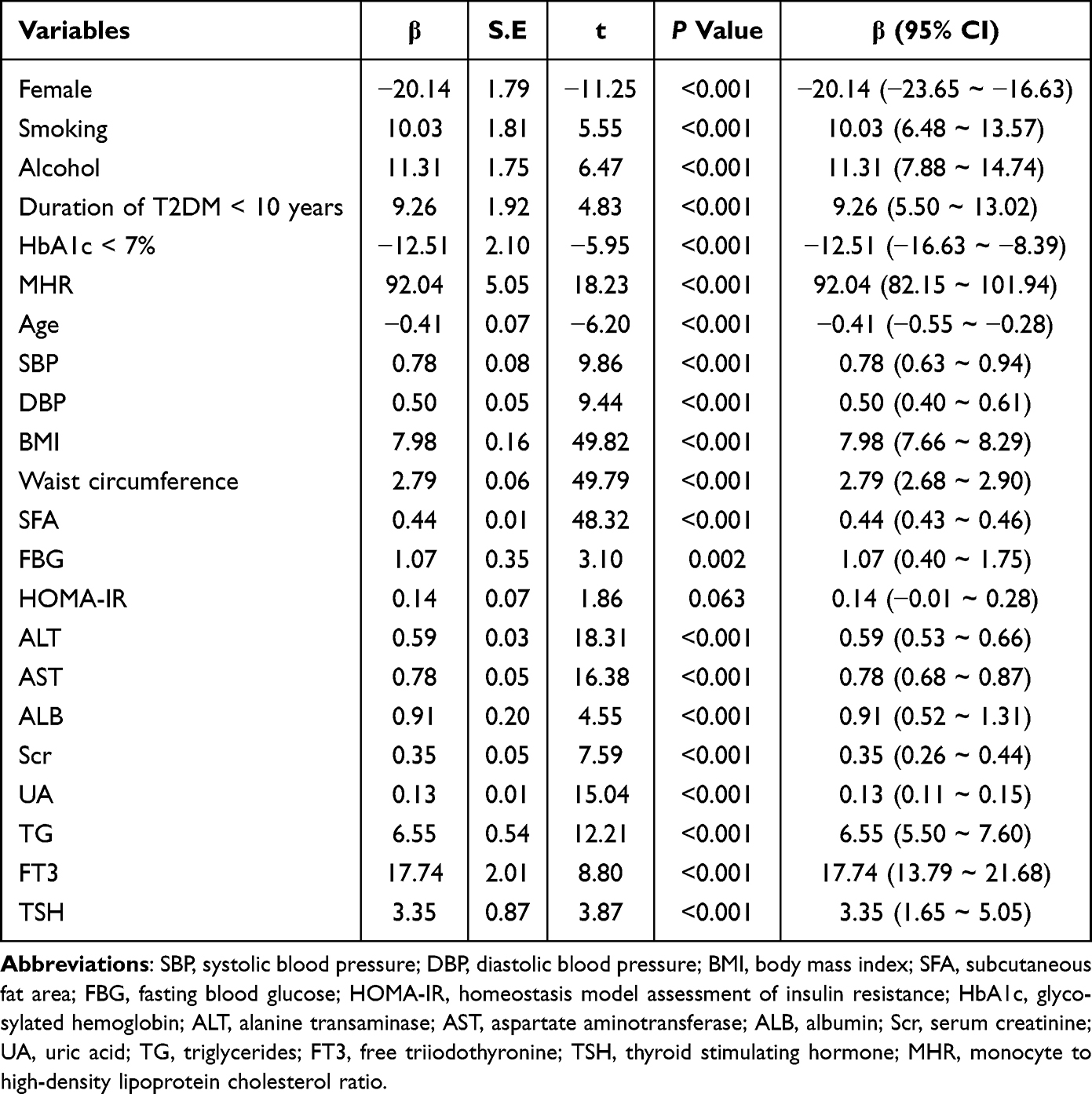 |
Table 2 Univariate Linear Regression Analysis for Factors Associated with VFA in T2DM Patients |
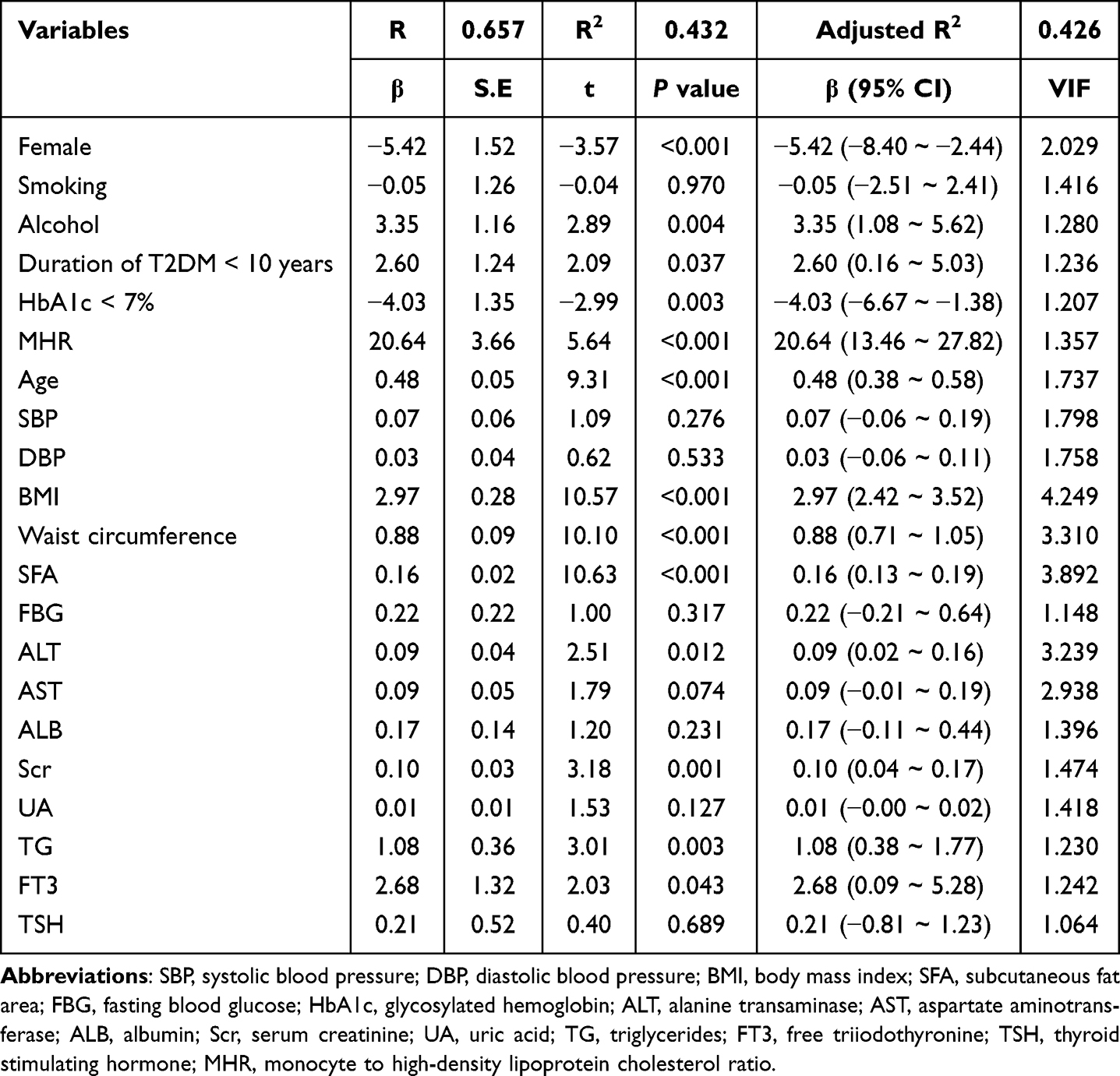 |
Table 3 Multivariate Linear Regression Analysis for Independent Factors Associated with VFA in T2DM Patients |
Subgroup Analysis
Univariate linear regression analysis showed that MHR was associated with VFA (β = 92.04, 95% CI 82.15–101.94, p < 0.001). After adjusting for age and sex, MHR was still associated with the VFA (β = 80.09, 95% CI 69.76–90.42, p < 0.001). We further adjusted for the drinking habits, and levels of waist circumference, SFA, ALT, Scr, TG and FT3, MHR remained independently associated with the VFA (β = 22.10, 95% CI 14.97–29.23, p < 0.001). Moreover, we performed a subgroup linear regression according to HbA1c levels (< 7% vs ≥ 7%) and T2DM duration (< 10 vs ≥ 10 years). After adjusting for age and sex, MHR remained associated with the VFA in all subgroups. After further adjusting for the other variables, MHR was still independently associated with VFA (p < 0.05) (Table 4).
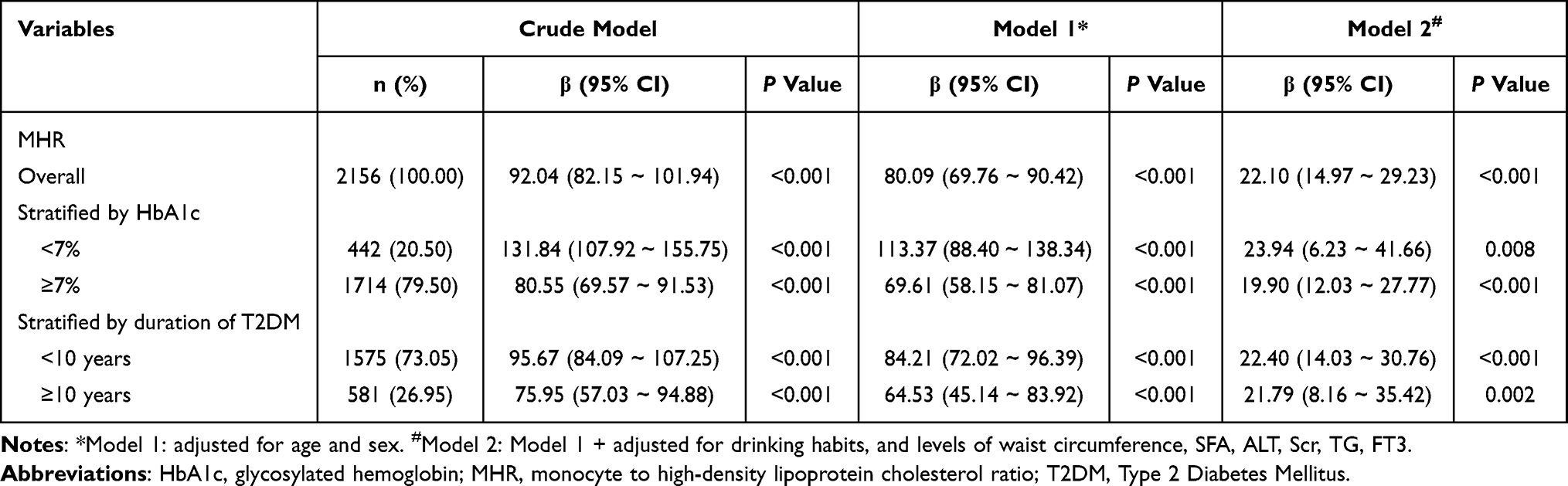 |
Table 4 Linear Regression Analysis Assessing the Association of the MHR with VFA |
Comparison of MHR, HDL-C, and MONO for Predicting the VFA in Patients with T2DM
The ROC curves and AUCs for MHR, HDL-C, and MONO were shown in Figure 3 and Table 5. The AUC of MHR, HDL-C, and MONO was respectively 0.708 (95% CI: 0.687–0.730), 0.653 (95% CI: 0.630–0.676), and 0.658 (95% CI: 0.635–0.681). In addition, the difference in AUC between MHR and HDL-C was 0.0552 (Z = 5.380, p < 0.001), between MHR and MONO was 0.0504 (Z = 6.645, p < 0.001), between MONO and HDL-C was 0.00472 (Z = 0.289, p = 0.772). The predictive effect of MHR on VFA was superior to that of HDL-C or MONO alone, and the difference was significant.
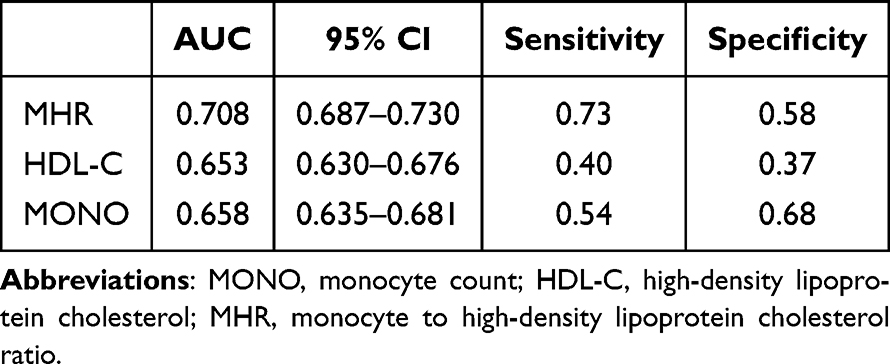 |
Table 5 The AUC of MHR, HDL-C, and MONO for Predicting the VFA in Patients with T2DM |
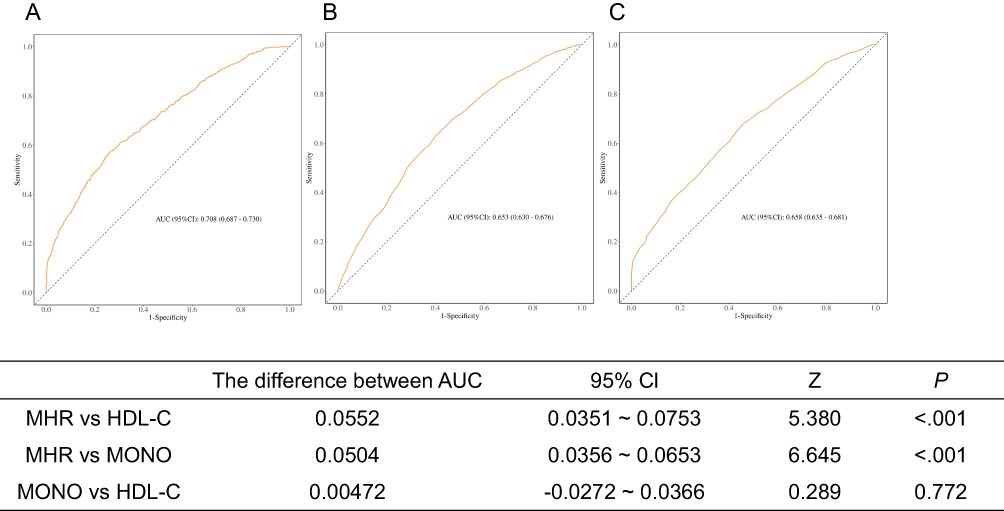 |
Figure 3 (A) ROC curve of MHR for predicting the VFA; (B) ROC curve of HDL-C for predicting the VFA; (C) ROC curve of MONO for predicting the VFA. |
Discussion
Obesity and T2DM are main public health concerns worldwide. Obesity is closely related to a variety of chronic diseases, including T2DM, hypertension, hyperlipidemia, and cardiovascular disease (CVD).25 The prevalence of obesity among adults has nearly tripled in the past decade, and abdominal obesity has risen by nearly half.26 Previous studies have shown an increase in cardiovascular health markers and a decrease in abnormal glucose metabolism. Conversely, an elevation in cardiovascular risk factors such as obesity is associated with an increase in T2DM.27 Notably, visceral obesity is considered a major risk factor for various metabolic diseases, especially T2DM and CVD, and may play a role through a series of adipose-specific cytokines (such as leptin), inflammatory cytokines, and immune cytokines.28,29 Circulating monocytes can independently predict CVD risk. HDLs play an anti-inflammatory role by inhibiting the activity of mononuclear cells and their differentiation into macrophages.6,27 Therefore, MHR, as the ratio of two conventional test indicators, is regarded as a contemporary marker of de novo inflammation. In this study, we selected patients with T2DM as study participants and analyzed for the first time the correlation between the novel inflammatory index MHR and VFA and its predictive role in this population. This study is the first to evaluate the direct relationship between visceral obesity and MHR in a Chinese population with T2DM.
Studies have revealed that MHR can safely and effectively predict disease progression and prognosis, and previous studies have confirmed that MHR is associated with CVD, ischemic stroke, and kidney disease.30–32 For example, a study by Karatas et al demonstrated that, compared with patients with T2DM exhibiting normoalbuminuria and healthy controls, MHR was significantly higher in individuals with diabetic nephropathy, and independently associated with urinary ALB to creatinine ratio.33 Vahit et al found that the MHR of patients with metabolic syndrome was significantly higher than that of healthy individuals, and it is well-established that obesity, especially central (visceral) obesity, is a key contributor to metabolic syndrome.21 Additionally, a study of patients with polycystic ovary syndrome (PCOS) revealed that the MHR levels in the PCOS group were significantly higher than those in the control group. Furthermore, patients with both obesity and PCOS exhibited significantly higher MHR levels than lean patients with PCOS.34 Therefore, we hypothesized that MHR, as a novel inflammatory indicator, may be associated with visceral obesity. This study found that MHR in patients with T2DM and visceral obesity was significantly higher than in those without visceral obesity, and that MHR was positively correlated and independent associated with VFA. The main risk factors for the occurrence of diabetic complications are poor blood sugar control and a long disease course.35–37 After we stratified participants based on HbA1c level and disease course, MHR remained independently associated with VFA. Our discovery was in the same direction as previous researches.
However, the mechanisms underlying the interaction between MHR and visceral obesity remain unclear. Previous studies have found that monocytes and macrophages play an important role in the synthesis and release of pro-inflammatory and pro-oxidative cytokines.38 In the context of obesity, hypertrophic adipocytes and hypoxia within expanding visceral adipose tissue (VAT) secrete chemokines which recruit circulating classical monocytes into VAT. Upon infiltration, these monocytes differentiate into macrophages and can polarize towards a pro-inflammatory M1 phenotype, amplifying local inflammation through cytokine signaling (eg, TNF-α, IL-6) and contributing to systemic insulin resistance.39,40 Moreover, the migration of peripheral blood mononuclear cells contributes not only to the accumulation of macrophages in adipose tissue but also to their proliferation in adipose tissue.41–43 HDL-C has been shown to protect endothelial cells from the harmful effects of LDL-C and prevent the oxidation of LDL-C, acting as an anti-inflammatory and antioxidant agent.44–46 However, a low HDL-C level, as often seen in visceral obesity, may thus fail to adequately counterbalance these pro-inflammatory processes. Therefore, studies suggest that MHR, as the ratio of MONO and HDL-C, can more objectively reflect the level of inflammatory response, and the body’s chronic inflammatory response is closely related to obesity and insulin resistance.
Our findings align with this pathophysiological model. The positive correlation and the independent association of MHR with VFA we observed suggest that this circulating inflammatory indicator is robustly linked to visceral fat accumulation. MHR integrates both pro-inflammatory (monocyte) and anti-inflammatory (HDL-C) signals from the systemic circulation, the strength of this association likely reflects the interplay between systemic inflammation and adipose-tissue-specific inflammatory pathways. In our ROC analysis, MHR had superior predictive value for VFA compared to MONO or HDL-C alone (AUC: 0.708 vs 0.658 and 0.653, respectively), implying that the ratio captures synergistic pathophysiological information. Furthermore, we also compared the contributions of HDL-C and MONO. If HDL-C were the predominant driver, we might expect a stronger inverse correlation and a larger AUC difference compared to MONO, which was not the case (MONO vs HDL-C AUC difference: 0.00472, p=0.772). Therefore, it is more appropriate to use MHR which is a circulating proxy to explore the correlation with VFA.
Our study has several limitations. First, magnetic resonance imaging (MRI) and computerized tomography (CT) are internationally recognized as more precise methods, but previous researches have demonstrated that BIA correlated highly with CT measurements, and even believed that BIA could be an alternative to CT to evaluate VFA in patients with T2DM.47,48 Second, the participants included in this study were recruited from Zhejiang Province in China, which may limit the generalizability of our findings owing to potential differences in race, lifestyle, and regional characteristics. Third, given the cross-sectional design of this study, causality between MHR and visceral obesity could not be established. Further longitudinal studies are warranted to clarify these relationships and explore their underlying mechanisms.
Conclusion
Elevated MHR was positively associated with VFA in T2DM patients, which has a modest predictive value. This index is simple, cost-effective, and extensively used in clinical settings, making it a practical indicator for screening and predicting visceral obesity. Therefore, routine screening of this index in patients with T2DM may help detect and intervene in visceral obesity at an early stage, thereby reducing the risk of associated cardiovascular events.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Clearance
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Zhejiang Provincial People’s Hospital (Ethics Approval Number: QT2024208). As this study was retrospective in nature, the ethical review granted an exemption from informed consent based on the initial patient consent form. Therefore, the study was conducted without obtaining informed consent from the survey participants.
Acknowledgments
The authors gratefully acknowledge the participation and cooperation of all patients in this study, as well as the Department of Endocrinology of the Zhejiang Provincial People’s Hospital. Moreover, the authors appreciate the support provided by the Key Laboratory of Endocrine Gland Diseases in Zhejiang Province.
Author Contributions
Conceptualization: Ye Hu, Xiaohong Wu. Data curation: Ye Hu, Yubo Xing, Yingxiang Song. Formal analysis: Ye Hu, Jia Zheng. Funding acquisition: Ye Hu, Xiaohong Wu. Investigation: Ye Hu, Yubo Xing. Methodology: Ye Hu, Jia Zheng. Project administration: Ye Hu, Xiaohong Wu. Resources: Xiaohong Wu. Writing-original draft: Ye Hu. Writing-review & editing: Ye Hu, Jia Zheng, Xiaohong Wu. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Zhejiang Province Science and Technology Plan Project (2021R52022); Zhejiang Province Health Innovative Talents Project (2021-CXRC07-01); General Scientific Research Project of Zhejiang Provincial Education Department (No. Y202352799); Medical Science and Technology Project of Zhejiang Province (2024KY726); Zhejiang Province Science and Technology Project (2024C03085).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Malone JI, Hansen BC. Does obesity cause type 2 diabetes mellitus (T2DM)? Or is it the opposite. Pediatr Diabetes. 2019;20(1):5–9. doi:10.1111/pedi.12787
2. GBD Adult BMI Collaborators. Global, regional, and national prevalence of adult overweight and obesity, 1990-2021, with forecasts to 2050: a forecasting study for the Global Burden of Disease Study 2021. Lancet. 2025;405(10481):813–838. doi:10.1016/S0140-6736(25)00355-1
3. Miyazaki Y, DeFronzo RA. Visceral fat dominant distribution in male type 2 diabetic patients is closely related to hepatic insulin resistance, irrespective of body type. Cardiovasc Diabetol. 2009;8(1):44. doi:10.1186/1475-2840-8-44
4. Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiol Rev. 2013;93(1):359–404. doi:10.1152/physrev.00033.2011
5. Guilliams M, Mildner A, Yona S. Developmental and Functional Heterogeneity of Monocytes. Immunity. 2018;49(4):595–613. doi:10.1016/j.immuni.2018.10.005
6. Yvan-Charvet L, Bonacina F, Guinamard RR, Norata GD. Immunometabolic function of cholesterol in cardiovascular disease and beyond. Cardiovasc Res. 2019;115(9):1393–1407. doi:10.1093/cvr/cvz127
7. Kocak MZ, Aktas G, Duman TT, et al. Monocyte lymphocyte ratio As a predictor of Diabetic Kidney Injury in type 2 Diabetes mellitus; The MADKID Study. J Diabetes Metab Disord. 2020;19(2):997–1002. doi:10.1007/s40200-020-00595-0
8. Tang X, Tan Y, Yang Y, et al. Association of the Monocyte-to-High-Density Lipoprotein Cholesterol Ratio With Diabetic Retinopathy. Front Cardiovasc Med. 2021;8:707008. doi:10.3389/fcvm.2021.707008
9. Duan Y, Luo J, Pan X, et al. Association between inflammatory markers and non-alcoholic fatty liver disease in obese children. Front Public Health. 2022;10:991393. doi:10.3389/fpubh.2022.991393
10. Kocak MZ, Aktas G, Erkus E, Sincer I, Atak B, Duman T. Serum uric acid to HDL-cholesterol ratio is a strong predictor of metabolic syndrome in type 2 diabetes mellitus. Rev Assoc Med Bras. 2019;65(1):9–15. doi:10.1590/1806-9282.65.1.9
11. Groenen AG, Halmos B, Tall AR, Westerterp M. Cholesterol efflux pathways, inflammation, and atherosclerosis. Crit Rev Biochem Mol Biol. 2021;56(4):426–439. doi:10.1080/10409238.2021.1925217
12. Li Y, Guo X, Ge J, et al. Sex differences in associations of metabolic inflammation and insulin resistance with incident type 2 diabetes mellitus: a retrospective cohort of adults with annual health examinations. Lipids Health Dis. 2025;24(1):50. doi:10.1186/s12944-025-02473-1
13. Lontchi-Yimagou E, Sobngwi E, Matsha TE, Kengne AP. Diabetes mellitus and inflammation. Curr Diab Rep. 2013;13(3):435–444. doi:10.1007/s11892-013-0375-y
14. Grandl G, Wolfrum C. Hemostasis, endothelial stress, inflammation, and the metabolic syndrome. Semin Immunopathol. 2018;40(2):215–224. doi:10.1007/s00281-017-0666-5
15. Ying W, Fu W, Lee YS, Olefsky JM. The role of macrophages in obesity-associated islet inflammation and β-cell abnormalities. Nat Rev Endocrinol. 2020;16(2):81–90. doi:10.1038/s41574-019-0286-3
16. González N, Moreno-Villegas Z, González-Bris A, Egido J, Lorenzo Ó. Regulation of visceral and epicardial adipose tissue for preventing cardiovascular injuries associated to obesity and diabetes. Cardiovasc Diabetol. 2017;16(1):44. doi:10.1186/s12933-017-0528-4
17. Al-Sulaiti H, Diboun I, Agha MV, et al. Metabolic signature of obesity-associated insulin resistance and type 2 diabetes. J Transl Med. 2019;17(1):348. doi:10.1186/s12967-019-2096-8
18. Stefan N. Metabolically Healthy and Unhealthy Normal Weight and Obesity. Endocrinol Metab. 2020;35(3):487–493. doi:10.3803/EnM.2020.301
19. Halim M, Halim A. The effects of inflammation, aging and oxidative stress on the pathogenesis of diabetes mellitus (type 2 diabetes). Diabetes Metab Syndr. 2019;13(2):1165–1172. doi:10.1016/j.dsx.2019.01.040
20. Herkiloglu D, Gokce S. Correlation of monocyte/HDL ratio (MHR) with inflammatory parameters in obese patients diagnosed with polycystic ovary syndrome. Ginekol Pol. 2021;92(8):537–543. doi:10.5603/GP.a2020.0191
21. Vahit D, Akboga MK, Samet Y, Hüseyin E. Assessment of monocyte to high density lipoprotein cholesterol ratio and lymphocyte-to-monocyte ratio in patients with metabolic syndrome. Biomarker Med. 2017;11(7):535–540. doi:10.2217/bmm-2016-0380
22. Makhmudova U, Wild B, Williamson A, et al. Visceral Adipose Tissue, Aortic Distensibility and Atherosclerotic Cardiovascular Risk Across Body Mass Index Categories. Eur J Prev Cardiol. 2025. doi:10.1093/eurjpc/zwaf447
23. Jia W, Chan JC, Wong TY, Fisher EB. Diabetes in China: epidemiology, pathophysiology and multi-omics. Nat Metab. 2025;7(1):16–34. doi:10.1038/s42255-024-01190-w
24. Hu Y, Zheng J, Ye X, Song Y, Wu X. Association Between Elevated Thyroid Peroxidase Antibody and Abdominal Fat Distribution in Patients with Type 2 Diabetes Mellitus. Diabetes Metab Syndr Obes. 2022;15:863–871. doi:10.2147/DMSO.S345507
25. De Lorenzo A, Gratteri S, Gualtieri P, Cammarano A, Bertucci P, Di Renzo L. Why primary obesity is a disease. J Transl Med. 2019;17(1):169. doi:10.1186/s12967-019-1919-y
26. NCD Risk Factor Collaboration (NCD-RisC) Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390(10113):2627–2642. doi:10.1016/S0140-6736(17)32129-3
27. Ren Y, Wang W, Zou H, et al. Association between ideal cardiovascular health and abnormal glucose metabolism in the elderly: evidence based on real-world data. BMC Geriatr. 2024;24(1):414. doi:10.1186/s12877-023-04632-4
28. Gastaldelli A, Cusi K, Pettiti M, et al. Relationship between hepatic/visceral fat and hepatic insulin resistance in nondiabetic and type 2 diabetic subjects. Gastroenterology. 2007;133(2):496–506. doi:10.1053/j.gastro.2007.04.068
29. Shulman GI. Ectopic fat in insulin resistance, dyslipidemia, and cardiometabolic disease. N Engl J Med. 2014;371(12):1131–1141. doi:10.1056/NEJMra1011035
30. Kanbay M, Solak Y, Unal HU, et al. Monocyte count/HDL cholesterol ratio and cardiovascular events in patients with chronic kidney disease. Int Urol Nephrol. 2014;46(8):1619–1625. doi:10.1007/s11255-014-0730-1
31. Shi WR, Wang HY, Chen S, Guo XF, Li Z, Sun YX. The impact of monocyte to high-density lipoprotein ratio on reduced renal function: insights from a large population. Biomarker Med. 2019;13(9):773–783. doi:10.2217/bmm-2018-0406
32. Wang HY, Shi WR, Yi X, Zhou YP, Wang ZQ, Sun YX. Assessing the performance of monocyte to high-density lipoprotein ratio for predicting ischemic stroke: insights from a population-based Chinese cohort. Lipids Health Dis. 2019;18(1):127. doi:10.1186/s12944-019-1076-6
33. Karatas A, Turkmen E, Erdem E, Dugeroglu H, Kaya Y. Monocyte to high-density lipoprotein cholesterol ratio in patients with diabetes mellitus and diabetic nephropathy. Biomarker Med. 2018;12(9):953–959. doi:10.2217/bmm-2018-0048
34. Usta A, Avci E, Bulbul CB, Kadi H, Adali E. The monocyte counts to HDL cholesterol ratio in obese and lean patients with polycystic ovary syndrome. Reprod Biol Endocrinol. 2018;16(1):34. doi:10.1186/s12958-018-0351-0
35. Giorda CB, Avogaro A, Maggini M, et al. Incidence and risk factors for stroke in type 2 diabetic patients: the DAI study. Stroke. 2007;38(4):1154–1160. doi:10.1161/01.STR.0000260100.71665.2f
36. Ma R. Epidemiology of diabetes and diabetic complications in China. Diabetologia. 2018;61(6):1249–1260. doi:10.1007/s00125-018-4557-7
37. Schiborn C, Schulze MB. Precision prognostics for the development of complications in diabetes. Diabetologia. 2022;65(11):1867–1882. doi:10.1007/s00125-022-05731-4
38. Ancuta P, Wang J, Gabuzda D. CD16+ monocytes produce IL-6, CCL2, and matrix metalloproteinase-9 upon interaction with CX3CL1-expressing endothelial cells. J Leukoc Biol. 2006;80(5):1156–1164. doi:10.1189/jlb.0206125
39. Weisberg SP, McCann D, Desai M, Rosenbaum M, Leibel RL, Ferrante Jr AW. Obesity is associated with macrophage accumulation in adipose tissue. J Clin Invest. 2003;112(12):1796–1808. doi:10.1172/JCI200319246
40. Li H, Meng Y, He S, et al. Macrophages, Chronic Inflammation, and Insulin Resistance. Cells. 2022;11(19):3001. doi:10.3390/cells11193001
41. Oh DY, Morinaga H, Talukdar S, Bae EJ, Olefsky JM. Increased macrophage migration into adipose tissue in obese mice. Diabetes. 2012;61(2):346–354. doi:10.2337/db11-0860
42. Amano SU, Cohen JL, Vangala P, et al. Local proliferation of macrophages contributes to obesity-associated adipose tissue inflammation. Cell Metab. 2014;19(1):162–171. doi:10.1016/j.cmet.2013.11.017
43. Nagareddy PR, Kraakman M, Masters SL, et al. Adipose tissue macrophages promote myelopoiesis and monocytosis in obesity. Cell Metab. 2014;19(5):821–835. doi:10.1016/j.cmet.2014.03.029
44. Navab M, Reddy ST, Van Lenten BJ, Fogelman AM. HDL and cardiovascular disease: atherogenic and atheroprotective mechanisms. Nat Rev Cardiol. 2011;8(4):222–232. doi:10.1038/nrcardio.2010.222
45. Ikenaga M, Higaki Y, Saku K, Uehara Y. High-Density Lipoprotein Mimetics: a Therapeutic Tool for Atherosclerotic Diseases. J Atheroscler Thromb. 2016;23(4):385–394. doi:10.5551/jat.33720
46. De Matteis C, Petruzzelli S, Graziano G, et al. Improving cardiovascular risk stratification: the role of abdominal obesity in predicting MACEs. Cardiovasc Diabetol. 2025;24(1):328. doi:10.1186/s12933-025-02885-4
47. Park KS, Lee DH, Lee J, et al. Comparison between two methods of bioelectrical impedance analyses for accuracy in measuring abdominal visceral fat area. J Diabetes Complications. 2016;30(2):343–349. doi:10.1016/j.jdiacomp.2015.10.014
48. Omura-Ohata Y, Son C, Makino H, et al. Efficacy of visceral fat estimation by dual bioelectrical impedance analysis in detecting cardiovascular risk factors in patients with type 2 diabetes. Cardiovasc Diabetol. 2019;18(1):137. doi:10.1186/s12933-019-0941-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.