Back to Journals » Clinical Ophthalmology » Volume 20
Relationship Between Lifestyle During School Years, Ocular Biomechanics and Refractive Status in Adult Myopes
Authors Baptista PML ![]() , Marques JH
, Marques JH ![]() , Santos GF
, Santos GF ![]() , Alves MJ, Freitas T
, Alves MJ, Freitas T ![]() , Abreu AC
, Abreu AC ![]() , Monteiro S
, Monteiro S ![]() , Pinto MDC
, Pinto MDC ![]() , Ambrósio Jr R
, Ambrósio Jr R ![]() , Menéres P
, Menéres P ![]() , Beirão JM
, Beirão JM ![]()
Received 29 September 2025
Accepted for publication 5 February 2026
Published 26 March 2026 Volume 2026:20 571074
DOI https://doi.org/10.2147/OPTH.S571074
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Pedro Manuel Luís Baptista,1,2 João Heitor Marques,1,2 Gabriel Freitas Santos,1 Maria João Alves,2 Teresa Freitas,2 Ana Carolina Abreu,1,2 Sílvia Monteiro,1,2 Maria Do Céu Pinto,1 Renato Ambrósio Jr,3,4 Pedro Menéres,1,2 João Melo Beirão1,2
1Ophthalmology Department, Centro Hospitalar E Universitário de Santo António, Oporto, Portugal; 2Instituto de ciências Biomédicas Abel Salazar, Oporto, Portugal; 3RioVision Hospital, Rio de Janeiro, Brasil; 4Instituto de Olhos Renato Ambrósio Jr, Rio de Janeiro, Brasil
Correspondence: Pedro Manuel Luís Baptista, Email [email protected]
Purpose: To investigate the relationship between ocular biomechanical properties in adult myopes and lifestyle habits during school years, aiming to identify behavioral patterns that may influence ocular tissue behavior and refractive development.
Methods: This cross-sectional study included adult myopes. Biomechanical parameters were obtained using the Corvis ST®. Variables analyzed included the first- and second-generation parameters. Demographic and lifestyle data were collected through a validated retrospective questionnaire (google form) including outdoor activity levels, sleep posture, digital device usage, educational attainment, family history of myopia, allergic conditions and eye rubbing. Statistical comparisons were made between subgroups based on these factors.
Results: The study included 390 myopic eyes, with a mean spherical equivalent (SE) of − 5,09± 3,8D from 195 individuals with a mean age of 32,72± 5,4 years-old. Lower ocular rigidity and a higher myopic spherical equivalent was found in eyes from individuals with personal history of allergies (p=0,00; p=0,03), family history of myopia (p=0,00; p=0,00), predominance of indoor extracurricular activities during school years (p=0,07; p=0,03) and exposure to touchscreen devices under 15 years-old (p=0,00; p=0,05). Eyes submitted to rubbing habits (p=0,05) or from individuals with higher academic degree (p=0,01) showed higher spherical equivalent. Eyes from individuals with predominantly ventral sleeping habits showed lower CBI (p=0,06) and TBI (p=0,01). A multivariable regression found a later age of digital device initiation (β = 0.0446, p = 0.014) to be predictor of higher Stress Strain Index and family history of myopia exhibited negative association (β = – 0.044, p = 0.014).
Conclusion: This study highlights the potential pivotal role of ocular tissue and its biomechanical behavior in translating demographic factors and lifestyle habits during the period of ocular growth into the refractive status later in adulthood. These findings pave the way for the use of ocular biomechanical analysis as one of the predictors of myopia in the future.
Keywords: biomechanics, cornea, CorVis, lifestyle, myopia, myopic progression
Introduction
Myopia is an ophthalmic condition with a markedly increasing prevalence over recent decades.1 Initially emerging in East Asian countries, it is now widespread across most industrialized nations. In addition to the growing burden on eye care services aimed at optimizing individual refractive status — and thereby improving both personal and professional functioning—the rising incidence of high myopia is associated with an increased risk of vision-threatening complications, including retinal detachment, myopic choroidal neovascularization, and glaucoma, often at a young age.2
The primary long-term goal is to prevent myopia progression effectively, thereby mitigating this global public health concern. Achieving this requires a comprehensive understanding of key risk factors. In recent years, behavioral aspects have received increasing attention, with the most robust evidence supporting associations with reduced time spent outdoors and higher educational attainment.3 However, with current societal and technological changes, early exposure to digital devices may also play a significant role.4
Given that axial myopia is the most common form, pathological ocular elongation must involve tissue remodeling that may be influenced by modifiable behavioral factors. Emerging evidence suggests a potential role for dopamine-mediated signaling in the sclera as a central mechanism driving axial elongation.5 Although recent evidence suggests a causal relationship between ocular biomechanical behavior and myopia,6 a three-dimensional relationship incorporating lifestyle factors has not yet been investigated.
Recent technological advances allow in vivo assessment of ocular biomechanical properties using a non-contact tonometer integrated with a Scheimpflug camera (CORVIS ST®), which captures dynamic tissue response to an air puff stimulus.7
As we hypothesize that specific childhood lifestyle factors are associated with measurable differences in adult ocular biomechanics and refractive status, the present study aims to describe refractive status and ocular biomechanics in a sample of Caucasian adult myopes and relate it to their lifestyle habits from childhood and adolescence.
Materials and Methods
Design
This is an observational cross-sectional study. The study adhered to the tenets of the Declaration of Helsinki.
Setting and Ethics Committee
Centro Hospitalar e Universitário de Santo António, Oporto, Portugal. The study was accepted by the Centro Hospitalar e Universitário de Santo António Ethical Commission (nr 158-DEFI/160-CE). Written informed consent was obtained from all participants.
Population and Exclusion Criteria
The study population consisted of adults consecutively selected from the refractive surgery screening appointments at our center within a 2-year period (between 2022 and 2024). Exclusion criteria were: familial or personal ocular pathologic history besides myopia and allergies; amblyopia history; ocular surgeries or trauma history; ocular inflammation at the time of examinations; corneal leucomas or other corneal or conjunctival pathologies; inability to perform the exams; inability to answer the questionnaire.
Objective Refraction Data
The KR-800 Auto Kerato-Refractometer® (TOPCON, Japan) was used to measure objective refractive status - (Sphere (S), Cylinder (C) and Spherical Equivalent (SE).
Ocular Biomechanical Data
Biomechanical assessment was made by means of Scheimpflug camera, with Corvis ST® (OCULUS), through the dynamic corneal response (DCR) parameters. The Corvis ST® is a noncontact tonometer system with a collimated air pulse offering a consistent pressure profile that acquires 4300 frames/s using an ultra-high-speed Scheimpflug camera with ultraviolet-free 455 nm blue light, covering 8.5 mm horizontally of a single slit to allow evaluation of corneal deformation.7 Only exams with “OK” quality score were included. Both first generation parameters - from the direct analysis of the corneal excursion image in three different timepoints, including Whole Eye Movement (WEM) – and second-generation parameters – algorithms including Stiffness Parameter in A1 (SP-A1) and Stress Strain Index (SS-I) - were analyzed. Table 1 summarizes all Scheimpflug-based parameters used in the study and their explanation, including which tissue each of them is most associated with and the theoretically expected behavior in the presence of higher values. Table 2 describes the biomechanical characterization of the sample.
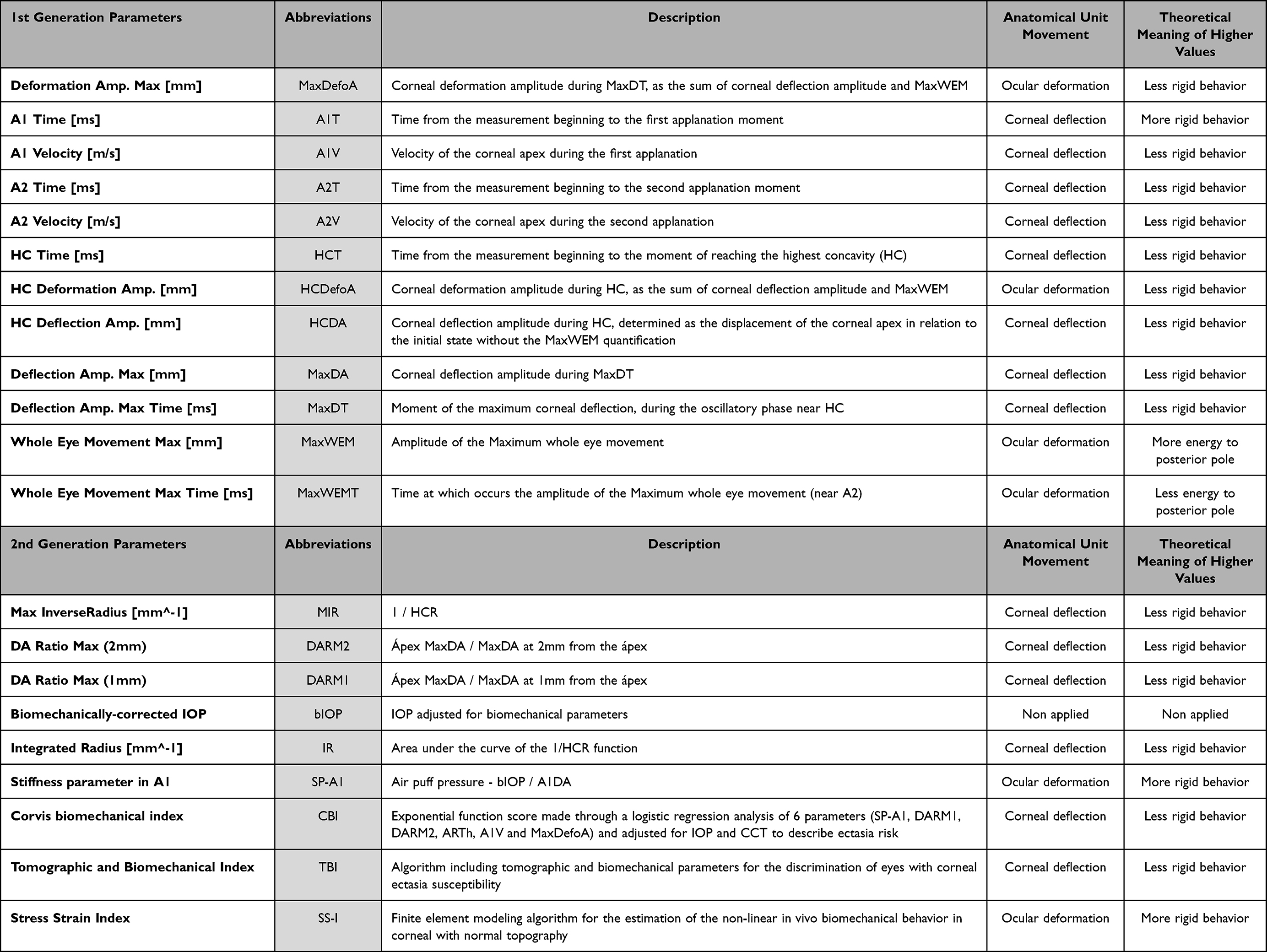 |
Table 1 Scheimpflug Camera-Derived Corneal Biomechanical Parameters with Explanation and Abbreviations |
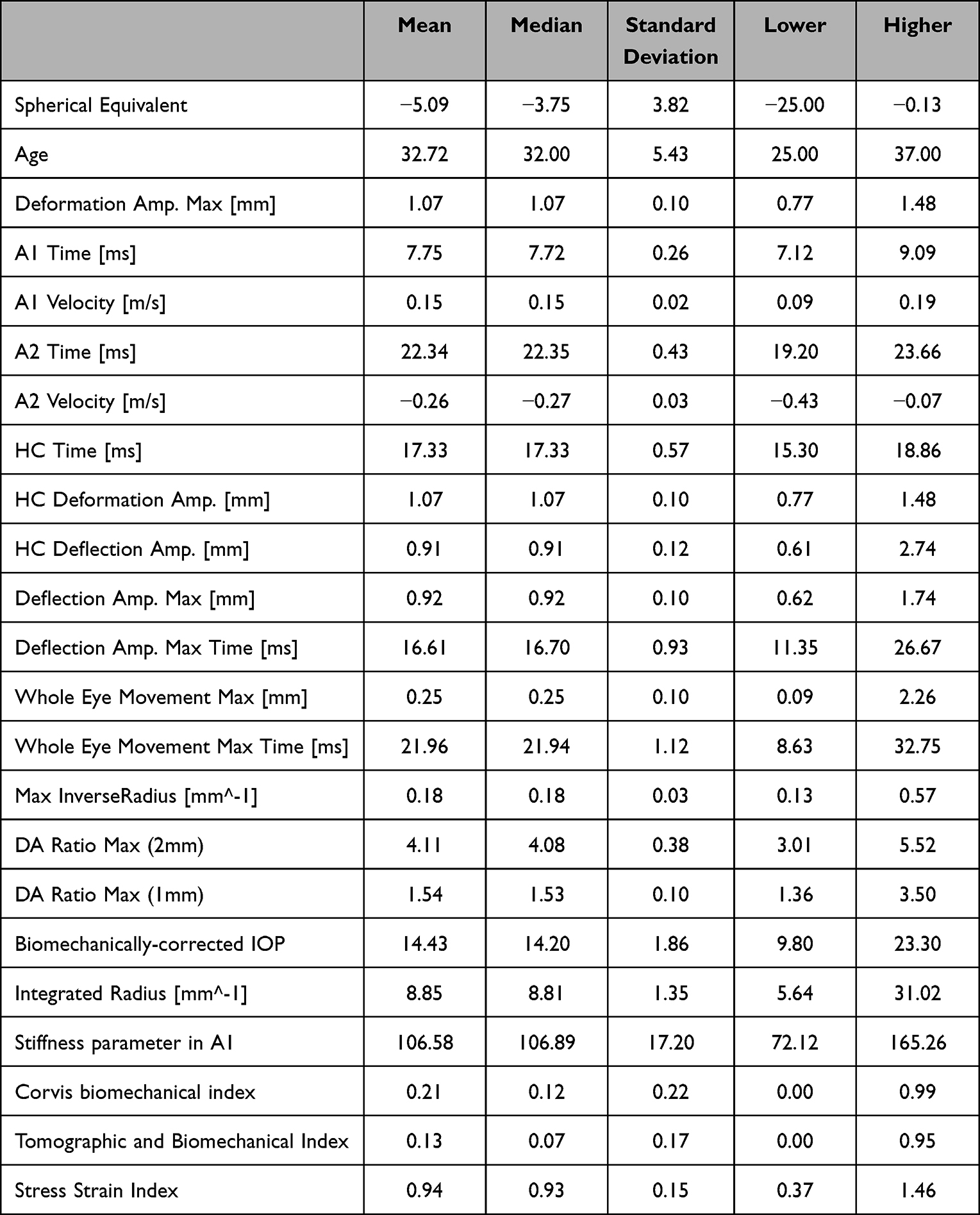 |
Table 2 Descriptive Statistics of the Full Sample |
Lifestyle Data
General health data and lifestyle data related to adolescence were assessed through a questionnaire validated by the Centro Hospitalar e Universitário de Santo António Ethical Commission (nr 158-DEFI/160-CE). Anonymized data were collected via Google Form® (Figure S1).
Inter-Individual Analysis
Individual ocular biomechanical behavior was compared according to the following factors: family history of myopia; personal history of allergic conditions; educational attainment; predominant types of extracurricular activities during childhood and adolescence; age of initial exposure to touchscreen digital devices; and predominant sleep position.
Inter-Eye Analysis
Ocular biomechanics parameters were compared to address differences in the groups of eyes with predominantly ipsilateral sleeping position and those submitted to rubbing habits.
Statistical Analysis
Descriptive statistics of the dataset were calculated for ocular biomechanics and lifestyle parameters. Normality of the data was tested with the Shapiro–Wilk and Kolmogorov–Smirnov tests. When parametric analysis could be applied, the Student’s t-test was used to compare the variables. When nonparametric tests were needed, the Wilcoxon rank-sum test was applied.
A multivariable linear regression model was built to identify independent predictors of the SS-I. The dependent variable was SS-I, while independent variables were the 8 lifestyle and demographic variables listed in Tables 3–6, with confounding factors being age and IOP. Inter-eye correlation was accounted for using Generalized Estimating Equations (GEE). Model assumptions, including linearity and homoscedasticity, were verified through residual analysis. Statistical significance was defined as p < 0.05.
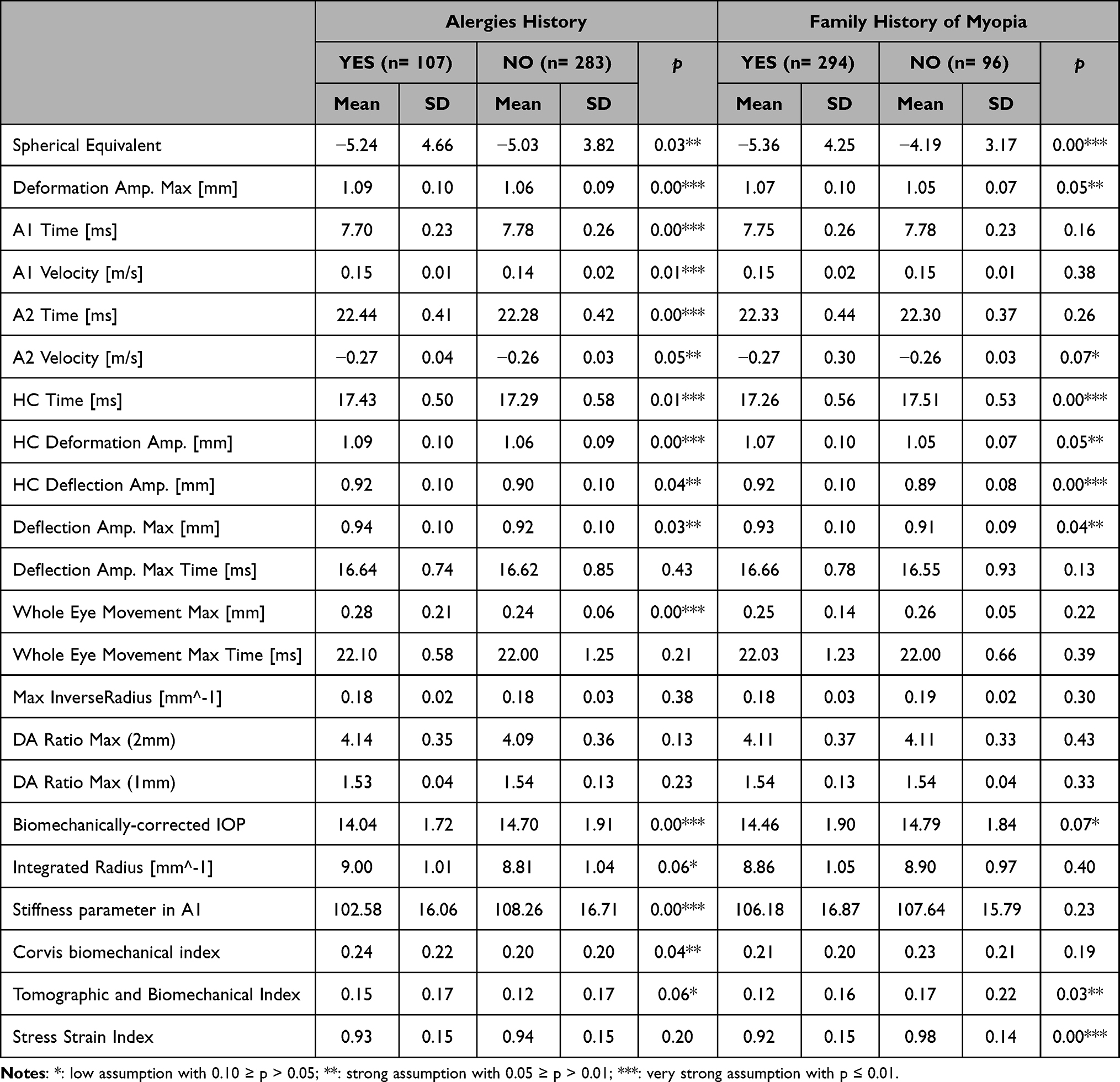 |
Table 3 Comparison of Refractive Status and Ocular Biomechanical Parameters Between Eyes from Individuals with or without History of Allergies and Family History of Myopia |
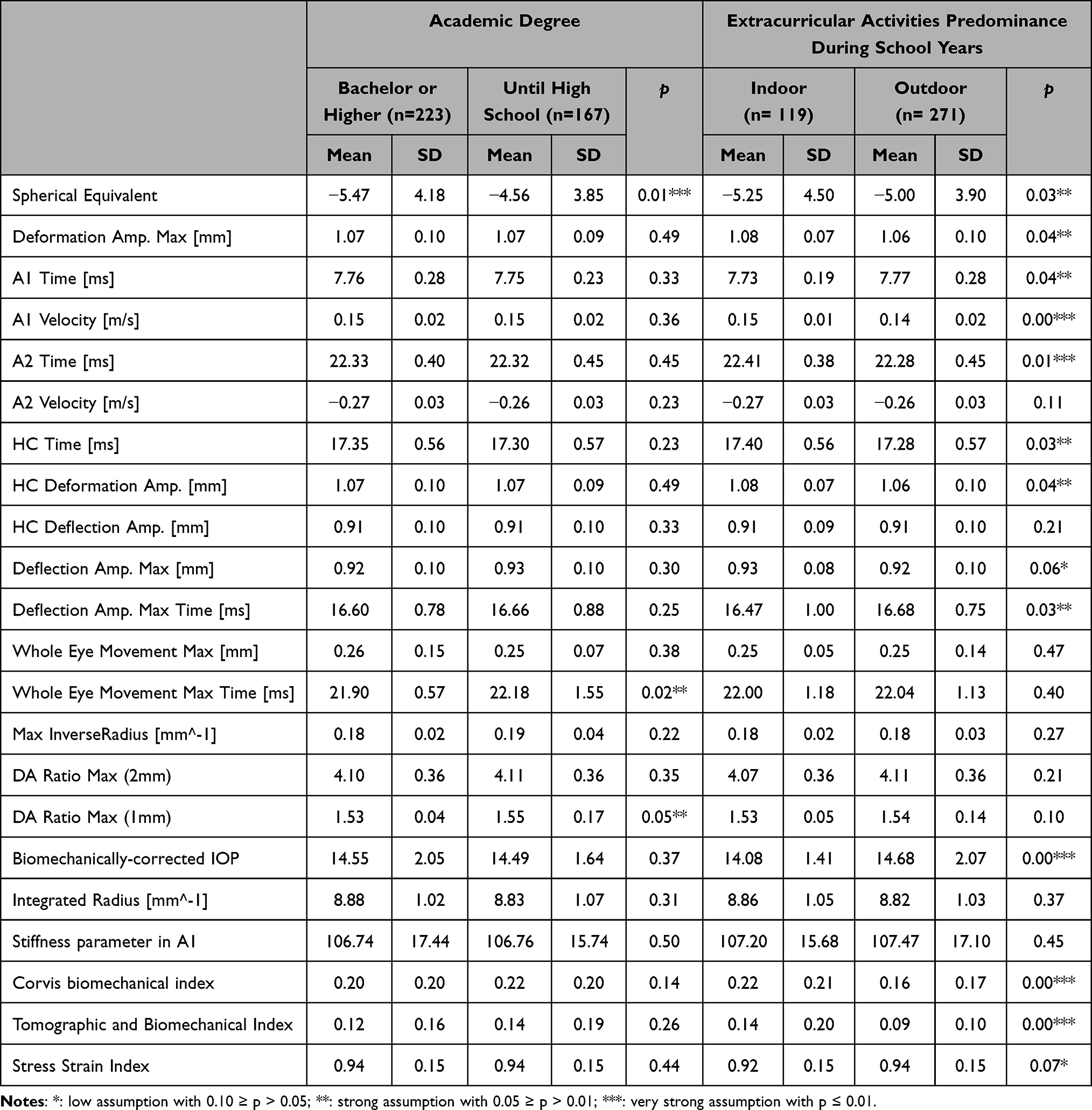 |
Table 4 Comparison of Refractive Status and Ocular Biomechanical Parameters Between Eyes from Individuals with Different Academic Degrees and Different Types of Extracurricular Activities During School years |
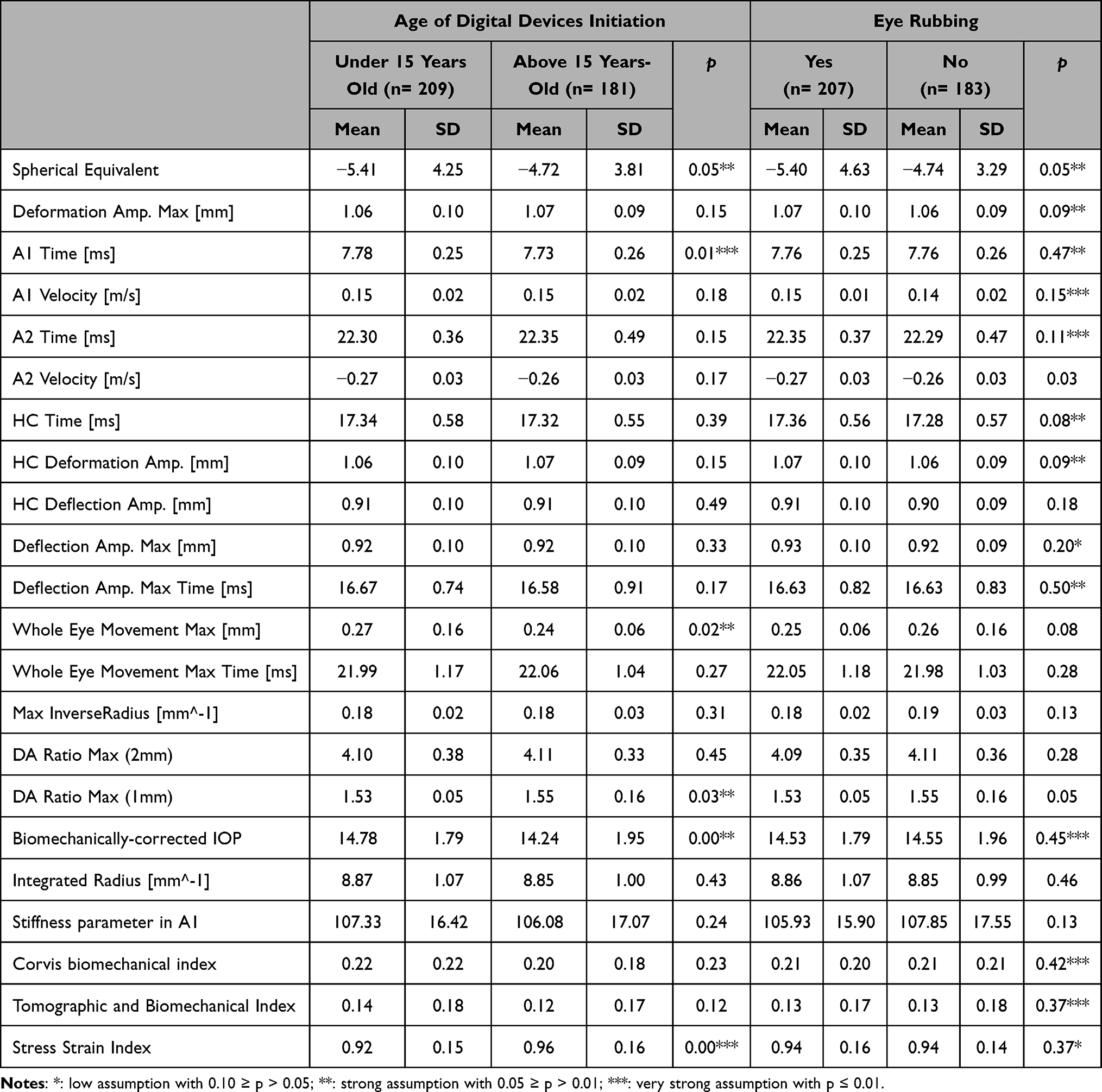 |
Table 5 Comparison of Refractive Status and Ocular Biomechanical Parameters Between Eyes from Individuals with Different Ages of Digital Devices Initiation and with or without Eye-Rubbing Habits |
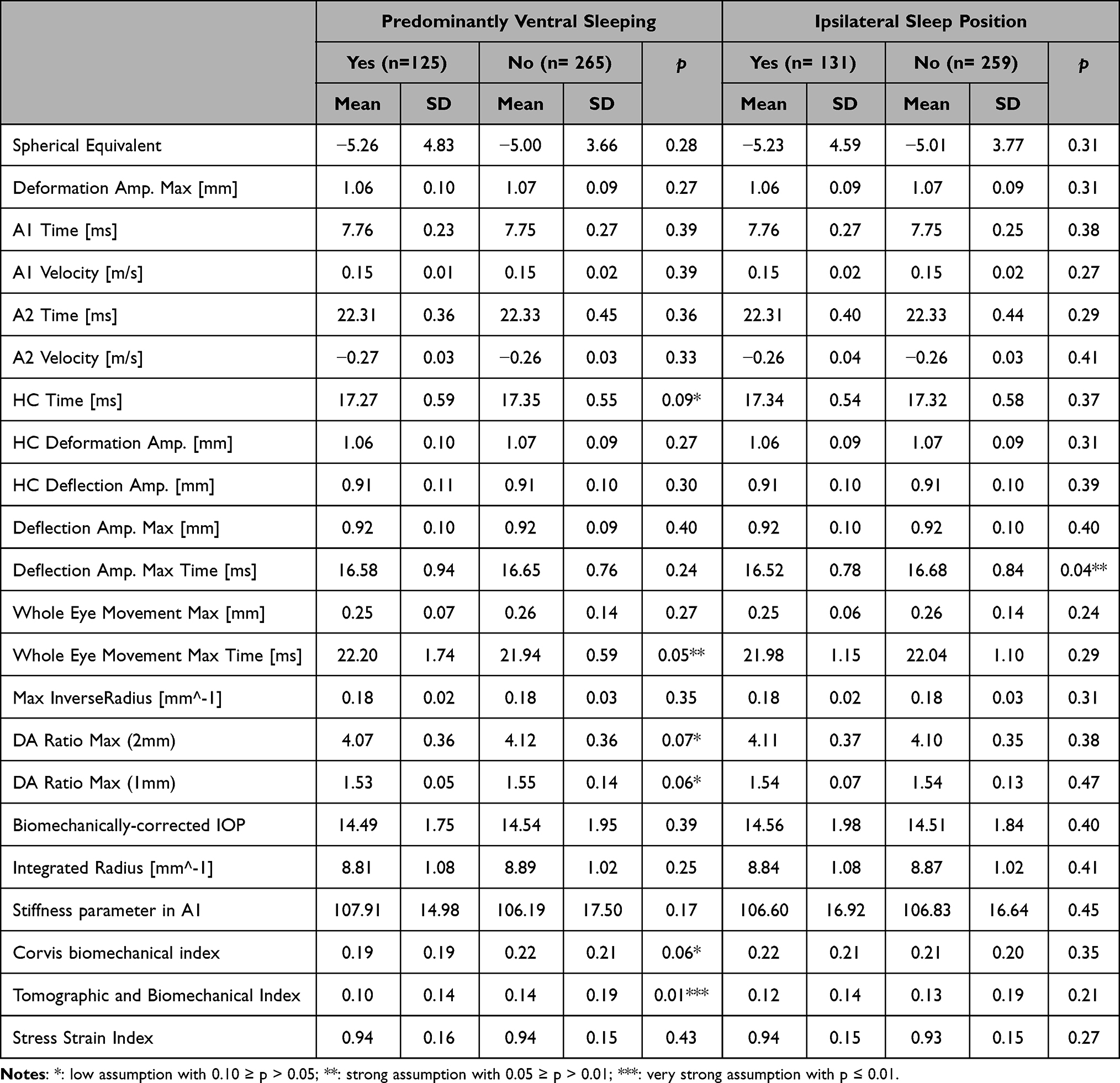 |
Table 6 Comparison of Refractive Status and Ocular Biomechanical Parameters Between Eyes from Individuals with or without Predominantly Ventral Sleeping Position and Eyes with or without Ipsilateral Sleeping Position |
All analyses were performed using the SPSS v30.0 software. All values are shown as mean ± standard deviation unless otherwise specified. All p-values (p) were 2-sided. For the null hypothesis: a low assumption was considered when 0.05 < p ≤ 0.10; a strong assumption was considered when 0.01 < p ≤ 0.05; a very strong assumption was considered when p ≤ 0.01.
Results
The present study included 390 eyes from 195 myopic individuals with a mean age of 32,72±5,43 years-old and a mean SE of −5,09±3,82 Diopters. Regarding the biomechanical analysis, the full sample showed a mean MaxDefoA of 1,07±0,1mm, a mean MaxWEM of 0.254±0,1mm, a mean MaxWEMT of 21,96±1,12 ms, a mean IR of 8,85± 1,35mm^−1, a mean SP-A1 of 106,58±17,20 and mean SS-I of 0.94±0,15. Full descriptive statistics are in Table 2. Tables 3–6 describe the differences between the subgroups.
Eyes from individuals with history of allergies showed higher values of absolute Spherical Equivalent (p≤0,05), MaxDefoA (p≤0,01), A1V (p≤0,01), A2T (p≤0,01), A2V (p≤0,05), HCT (p≤0,01), HCDefoA (p≤0,01), HCDA (p≤0,05), MaxDA (p≤0,05), MaxWEM (p≤0,01), IR (p≤0,01), CBI (p≤0,05) and TBI (p≤0,10) and lower values of A1T (p≤0,01), bIOP (p≤0,01) and SP-A1 (p≤0,01) (Table 3). Eyes from individuals with history of myopia in at least one parent showed higher values of Spherical Equivalent (p≤0,01), MaxDefoA (p≤0,05), A2V (p≤0,1), HCDefoA (p≤0,05), HCDA (p≤0,01) and MaxDA (p≤0,05) and lower values of HCT (p≤0,01), bIOP (p≤0,1), TBI (p≤0,05) and SS-I (p≤0,01) (Table 3).
Eyes from individuals with at least a bachelor’s degree showed higher values of Spherical Equivalent (p≤0,01) and lower values of MaxWEMT (p≤0,05) and DARM1 (p≤0,05) (Table 4). Eyes from individuals engaged primarily in indoor extracurricular activities presented higher values in Spherical Equivalent (p≤0,05), MaxDefoA (p≤0,05), A1V (p≤0,01), A2T (p≤0,01), HCT (p≤0,05), HCDefoA (p≤0,05), MaxDA (p≤0,05), CBI (p≤0,01) and TBI (p≤0,01) and lower values in A1T (p≤0,05), MaxDT (p≤0,005), bIOP (p≤0,01) and SS-I (p≤0,1) and (Table 4).
Eyes from individuals who began using digital devices under 15 years-old exhibit lower values in SS-I (p≤0,01) and higher values in SE (p≤0,05), A1T (p≤0,01), MaxWEM (p≤0,05), DARM1 (p≤0,05) and bIOP (p≤0,01) (Table 5). Eyes from individuals reporting frequent eye rubbing present elevated values in Spherical Equivalent (p≤0,05), MaxDefoA (p≤0,1), A2V (p≤0,05), HCT (p≤0,1) and HCDefoA (p≤0,1) and lower values in MaxWEM (p≤0,1) and DARM1 (p≤0,05) (Table 5).
Eyes from individuals with predominantly ventral sleep position showed increased values of MaxWEMT (p≤0,05) and lower values of HCT (p≤0,1), DARM2 (p≤0,1), DARM1 (p≤0,1), CBI (p≤0,1) and TBI (p≤0,01) (Table 6). Eyes with predominantly ipsilateral sleeping position showed lower values of MaxDT (p≤0,05) (Table 6).
The final multivariable model found later age of digital device initiation (β = 0.0446, p = 0.014) as an independent predictor of a higher SS-I in adulthood and family history of myopia exhibited significant negative association (β = –0.044, p = 0.014) (Figure 1). The model explained approximately 16% of the variance in SS-I (adjusted R2 = 0.159).
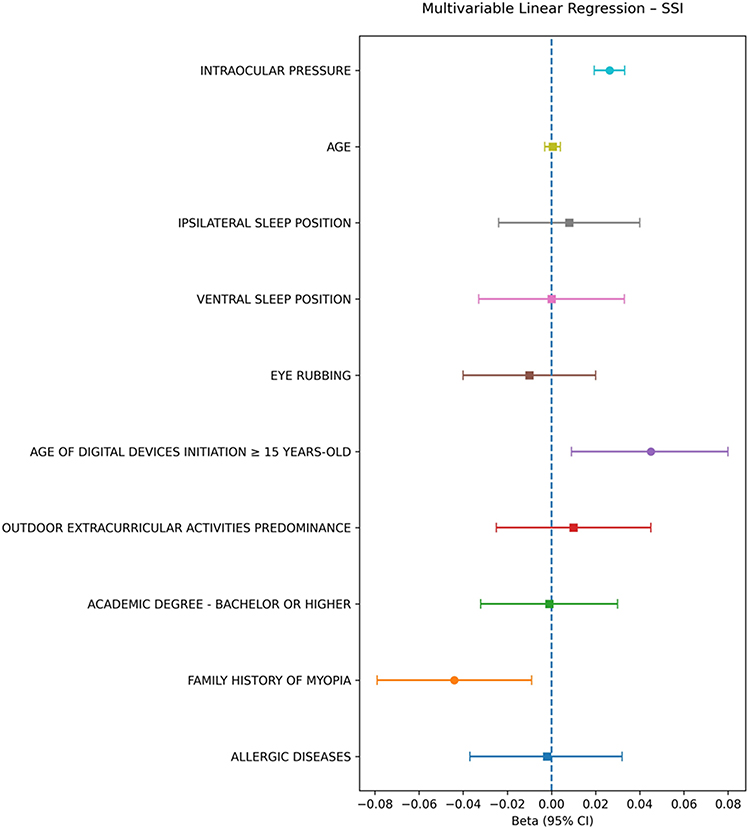 |
Figure 1 Multivariable linear regression model to identify independent predictors of the SS-I (Stress-Strain Index). |
Discussion
The present study aimed to analyze a large sample of myopic eyes from young adults, describing their ocular biomechanical behavior. To investigate the relationship between ocular biomechanics in myopic eyes and demographic and behavioral factors associated with myopia, a subgroup analysis was conducted. The sample was stratified into individuals exhibiting factors theoretically linked to higher degrees of myopia and those without such factors. Additionally, we examined other variables that, to our knowledge, have not been previously analyzed in this context but may be conceptually associated with myopia.
The mean age was 32,7, with a median of 32 years, representing an homogeneous sample and eliminating age as a confounding factor.8 Furthermore, none of the comparative analyses revealed significant age differences within each subgroup.
First, a significantly more myopic refractive status was observed in eyes of individuals with a family history of myopia in at least one parent, higher academic degree, a reported preference for indoor extracurricular activities during adolescence, earlier initiation of digital device use and in eyes exposed to eye rubbing. These findings are highly relevant, as they provide practical support for associations previously reported in the literature.9–19 Given these associations, the authors stratified the eyes according to demographic and lifestyle factors during late childhood and adolescence—a critical period for ocular elongation—aiming to identify differences in ocular biomechanical behavior among the groups. The objective was to investigate a potential tissue-based foundation for a causal relationship between the aforementioned factors and the refractive status of the eye in adulthood.
The study of ocular biomechanics using an air-puff tonometer coupled with a Scheimpflug camera enables not only the visualization of corneal deflection after an air puff but also the quantification of the complete axial deformation of the globe. This makes it an examination that describes the tissue behavior of the corneoscleral unit, which is theoretically the substrate for the emmetropization process.20 Although there is extensive literature regarding corneal biomechanics, particularly concerning ectatic diseases,21,22 the biomechanics of the corneoscleral unit remains largely unexplored.23 Nevertheless, there are already algorithms—considered second-generation parameters in the Corvis ST® —aimed at describing this ocular biomechanical behavior: the Stress-Strain Index (SSI) attempts, through a finite element modeling algorithm, to present a nonlinear measure of overall biomechanical behavior across various levels of the tissue’s stress-strain curve;24 the Stiffness Parameter at the first applanation of the cornea (SP-A1), which has proven to be the best parameter to infer global globe rigidity adjusted for a given intraocular pressure.25 On the other hand, Whole Eye Movement (WEM) parameters refer to the accessory anteroposterior displacement of the lateral corneal tissue, resulting from the residual energy not absorbed by corneal deflection and instead transmitted to and absorbed by the posterior segment of the eye, with inferred associations to the pathogenesis of axial myopia.26
Although biomechanical assessment using the Corvis ST® generates a wide range of additional parameters, the present discussion focuses on parameters most related to the biomechanical behavior of the corneoscleral unit and its hypothetic pivotal role between demographic and lifestyle factors during the years when school myopia develops and the refractive state in adulthood.
Two demographic factors were studied: a personal history of allergic diseases and a family history of myopia in first-degree relatives. The first of these factors showed the most significant differences, with allergic disease associated with greater corneal deflection (higher A1V, A2T, A2V, HCT, MaxDA, IR, CBI and TBI and lower A1T) as well as greater deformation of the corneoscleral unit (higher MaxDefoA, HCDefoA, MaxWEM, and lower SP-A1). These results support the positioning of allergies as an important risk factor for corneal ectatic disease27 and also add valuable information on a possible association with a cascade of events that predispose to a more compliant scleral tissue (higher MaxWEM and lower SP-A1) and, consequently, greater axial elongation and myopization, as we found significantly higher SE in this group of eyes.
Family history of myopia was associated with higher SE, as expected,28 and with a more compliant behavior of the corneoscleral unit, with higher total deformation measurements (higher MaxDefoA, HCDefoA), and notably a lower SS-I. Regarding the cornea, results were ambiguous, with findings both suggestive of greater deflection (higher HCDA and MaxDA) and of more rigid behavior (lower HCT and TBI). The authors hypothesize that myopia may lie at the opposite end of the spectrum from corneal ectatic disease during adolescence. In the former, the scleral tissue is more prone to remodeling and enhance axial elongation, whereas in the latter, the corneal tissue has a higher risk of ectatic disease due to external (eg, eye rubbing) and internal (eg, intraocular pressure) triggers. These data support evidence of biomechanical differences across different types of myopia29 and introduce the concept of a posterior-segment keratoconus-like condition, opening new perspectives for management approaches.
Educational level and time spent outdoors during childhood and adolescence are the most consistently associated lifestyle factors with myopic progression,9,30 although no evidence exists regarding their role in tissue behavior modulation. In the present study, individuals with at least a bachelor’s degree had higher SE and lower MaxWEMT and DARM1, reflecting proportionally greater deformation of the corneoscleral unit compared to central corneal deflection, with more energy translating to the posterior pole, as Whole Eye Movement is longer and occurs earlier in these eyes. The authors infer that this greater energy transmission to the posterior pole may trigger dopaminergic pathway cascades31,32 with axial elongation. The group of individuals reporting a preference for extracurricular activities in outdoor environments during their school years showed lower values of SE and a clearly more rigid biomechanical profile—both corneal (higher A1T and lower A1V, A2T, HCT, MaxDA, CBI and TBI) and corneoscleral (lower MaxDefoA, HCDefoA), particularly with a higher SS-I. First, these results support the extensive evidence of UV radiation’s role in corneal stiffness33 and suggest that a natural cross-linking process may also modulate scleral tissue compliance and, consequently, emmetropization regulation, pointing toward potential therapeutic avenues.34 Additionally, it supports the theory that ultraviolet light acts as a catalyst for dopamine release, which subsequently reduces scleral compliance, thereby preventing excessive ocular growth.32
Digital devices, although less consistently associated, have in recent years gained prominence as a contributing factor in myopia progression during childhood and adolescence,12,15,35 and the COVID-19 pandemic further substantiated this link.36 This study divided individuals into those who began using touchscreen digital devices before the age of 15 and those who did not. It’s important to note that, given the current habits, a more meaningful division would have been made between those who started before the age of 2 and the remainder. However, since this sample refers to individuals who were 15 years-old in the early 1990s - when such devices did not exist - this division was not feasible. Besides highlighting the drastic changes in habits since then, these results underscore the relevance of this factor and its potential for future studies. In the present study, individuals who started using such devices before the age of 15 years-old were more myopic and showed lower SS-I. They also displayed signs of biomechanical behavior in the corneoscleral unit suggesting greater energy transmission to the posterior pole, as indicated by a lower DARM1 and a higher MaxWEM, which reflects lateral movement beyond corneal deflection. This may be the first description of an alteration in the individual tissue behavior fingerprint conditioned by early digital device use, reinforcing this factor’s relevance and opening the door to further investigation.
Although the pillow effect has been suggested as a trigger for keratoconus,37 the evidence is controversial. On the other hand, it has never been proposed as a factor related to myopia. The present study separated individuals who reported ventral sleeping habits during adolescence. These individuals exhibited descriptors of stiffer corneas (lower HCT, DARM2, DARM1, CBI and TBI), and also a higher MaxWEMT, indicating increased accessory movement of corneoscleral tissue. Together, these data suggest once again that corneal ectasia and myopia may represent opposite ends of the biomechanical spectrum and/or that these corneas may have a reduced capacity for energy absorption, with greater transmission to the posterior pole and proportionally more scleral tissue remodeling. The study also conducted an inter-eye analysis, showing that eyes submitted to ipsilateral sleeping position had lower MaxDT values, indicating greater corneal stiffness. While this parameter lacks consistent supporting evidence, it reinforces the hypothesis that the pillow effect could be included as a factor associated in the emmetropization process in future studies.
Although eye rubbing is the most important trigger in the progression of corneal ectatic disease,37,38 evidence linking it to myopia is scarce.39 It is important to highlight that, in the present study, this group of eyes was more myopic. However, although some differences in the biomechanical behavior of these eyes were observed, the results lacked consistency.
Upon analysis of the adjusted multivariable model, a family history of myopia and early-age exposure to digital devices were identified as predictors of reduced ocular rigidity in adulthood, supporting the concept of an individual biomechanical “fingerprint” shaped by genetic load and lifestyle factors. The fact that this study was conducted in individuals whose childhood occurred in the 1990s—prior to the widespread use of touchscreen smartphones or tablets—enhances its clinical relevance, as the relative contribution of lifestyle-related factors is likely to be even greater in contemporary cohorts.
The main limitations of the present study are its retrospective observational design and the reliance on subjectively reported data through questionnaires about past events. However, it yielded several clinically relevant findings that the authors want to highlight. Firstly, significantly higher absolute SE values were found in individuals with lifestyle factors theoretically associated with greater myopization. Secondly, in a large and relatively age-homogeneous sample, the parameters that best describe total ocular biomechanical behavior - SP-A1 and SS-I - showed differences compatible with more compliant corneoscleral units in eyes belonging to individuals with a history of allergies, a family history of myopia in first-degree relatives and early digital device use, and less compliant units in those belonging to individuals who engaged more time in outdoor extracurricular activities during school years.
Conclusion
History of allergies, family history of myopia, early digital device use, and greater time spent in indoor extracurricular activities were all associated with more compliant corneal–scleral units and higher refractive error. In the multivariable analysis, family history of myopia and early initiation of digital device use emerged as independent predictors of a less stiff ocular biomechanical profile in adulthood. Taken together, these findings highlight the potential central role of ocular tissue biomechanics in translating demographic factors and childhood lifestyle habits during the period of ocular growth into refractive status later in adult life.
Acknowledgments
We would like to thank the technicians who performed the examinations.
Disclosure
Prof. Dr. Renato Ambrósio Jr is a consultant for Oculus. The authors report no other conflicts of interest in this work.
References
1. Liang J, Pu Y, Chen J, et al. Global prevalence, trend and projection of myopia in children and adolescents from 1990 to 2050: a comprehensive systematic review and meta-analysis. Br J Ophthalmol. 2025;109(3):362. doi:10.1136/bjo-2024-325427
2. Du Y, Meng J, He W, Qi J, Lu Y, Zhu X. Complications of high myopia: an update from clinical manifestations to underlying mechanisms. Adv Ophthalmol Pract Res. 2024;4(3):156–13. doi:10.1016/j.aopr.2024.06.003
3. Martínez-Albert N, Bueno-Gimeno I, Gené-Sampedro A. Risk factors for myopia: a review. J Clin Med. 2023;12(18):6062.
4. Ha A, Lee YJ, Lee M, Shim SR, Kim YK. Digital screen time and myopia: a systematic review and dose-response meta-analysis. JAMA Network Open. 2025;8(2):e2460026. doi:10.1001/jamanetworkopen.2024.60026
5. Kim DH, Hwang J-M, Yang HK. Topical dopamine application on form-deprivation myopia in rabbits. Life. 2025;15(3):461.
6. Li X, Luo S, Lin K, et al. Causal links between corneal biomechanics and myopia: evidence from bidirectional mendelian randomization in the UK biobank. Bioengineering. 2025;12(4). In eng. doi:10.3390/bioengineering12040412.
7. Baptista PM, Ambrosio R, Oliveira L, Meneres P, Beirao JM. Corneal biomechanical assessment with ultra-high-speed scheimpflug imaging during non-contact tonometry: a prospective review. Clin Ophthalmol. 2021;15:1409–1423. In eng. doi:10.2147/opth.S301179
8. Guo Y, Guo -L-L, Yang W, Tian L, Jie Y. Age-related analysis of corneal biomechanical parameters in healthy Chinese individuals. Sci Rep. 2024;14(1):21713. doi:10.1038/s41598-024-72054-2
9. McKnight CM, Sherwin JC, Yazar S, et al. Myopia in young adults is inversely related to an objective marker of ocular sun exposure: the Western Australian Raine cohort study. Am J Ophthalmol. 2014;158(5):1079–1085.In eng. doi:10.1016/j.ajo.2014.07.033
10. Pan C-W, Ramamurthy D, Saw S-M. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiol Opt. 2012;32(1):3–16. In eng. doi:10.1111/j.1475-1313.2011.00884.x
11. Sherwin JC, Reacher MH, Keogh RH, Khawaja AP, Mackey DA, Foster PJ. The association between time spent outdoors and myopia in children and adolescents: a systematic review and meta-analysis. Ophthalmology. 2012;119(10):2141–2151. In eng. doi:10.1016/j.ophtha.2012.04.020
12. Foreman J, Salim AT, Praveen A, et al. Association between digital smart device use and myopia: a systematic review and meta-analysis. Lancet Digit Health. 2021;3(12):e806–e818.In eng. doi:10.1016/s2589-7500(21)00135-7
13. Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K. Parental history of myopia, sports and outdoor activities, and future myopia. Invest Ophthalmol Vis Sci. 2007;48(8):3524–3532. In eng. doi:10.1167/iovs.06-1118
14. Guggenheim JA, Northstone K, McMahon G, et al. Time outdoors and physical activity as predictors of incident myopia in childhood: a prospective cohort study. Invest Ophthalmol Vis Sci. 2012;53(6):2856–2865.In eng. doi:10.1167/iovs.11-9091
15. Loughman J, Flitcroft DI. Are digital devices a new risk factor for myopia? Lancet Digit Health. 2021;3(12):e756–e757. In eng. doi:10.1016/s2589-7500(21)00231-4
16. Guo L, Yang J, Mai J, et al. Prevalence and associated factors of myopia among primary and middle school-aged students: a school-based study in Guangzhou. Eye. 2016;30(6):796–804. doi:10.1038/eye.2016.39
17. Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279–1285.In eng. doi:10.1016/j.ophtha.2007.12.019
18. Ip JM, Saw SM, Rose KA, et al. Role of near work in myopia: findings in a sample of Australian school children. Invest Ophthalmol Vis Sci. 2008;49(7):2903–2910.In eng. doi:10.1167/iovs.07-0804
19. Grzybowski A, Kanclerz P, Tsubota K, Lanca C, Saw S-M. A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmol. 2020;20(1):27. doi:10.1186/s12886-019-1220-0
20. Metlapally R, Wildsoet CF. Scleral mechanisms underlying ocular growth and myopia. Prog Mol Biol Transl Sci. 2015;134:241–248. In eng. doi:10.1016/bs.pmbts.2015.05.005
21. Ambrósio R Jr, Lopes BT, Faria-Correia F, et al. Integration of Scheimpflug-based corneal tomography and biomechanical assessments for enhancing ectasia detection. J Refract Surg. 2017;33(7):434–443.In eng. doi:10.3928/1081597x-20170426-02
22. Ambrósio R Jr, Machado AP, Leão E, et al. Optimized artificial intelligence for enhanced ectasia detection using scheimpflug-based corneal tomography and biomechanical data. Am J Ophthalmol. 2023;251:126–142. doi:10.1016/j.ajo.2022.12.016
23. Gallego P, Martínez-García C, Pérez-Merino P, Ibares-Frías L, Mayo-Iscar A, Merayo-Lloves J. Scleral changes induced by atropine in chicks as an experimental model of myopia. Ophthalmic Physiol Opt. 2012;32(6):478–484. In eng. doi:10.1111/j.1475-1313.2012.00940.x
24. Eliasy A, Chen KJ, Vinciguerra R, et al. Determination of corneal biomechanical behavior in-vivo for healthy eyes using CorVis ST tonometry: stress-strain index. Front Bioeng Biotechnol. 2019;7(105). In eng. doi:10.3389/fbioe.2019.00105.
25. Roberts CJ, Mahmoud AM, Bons JP, et al. Introduction of two novel stiffness parameters and interpretation of air puff-induced biomechanical deformation parameters with a dynamic scheimpflug analyzer. J Refract Surg. 2017;33(4):266–273.In eng. doi:10.3928/1081597x-20161221-03
26. Li DL, Qin Y, Zheng YJ, et al. Refractive associations with whole eye movement distance and time among chinese university students: a corvis ST study. Transl Vis Sci Technol. 2023;12(12):13.In eng. doi:10.1167/tvst.12.12.13
27. Halim WH, Jamaludin MI, Cheng TC. Corneal biomechanics in patients with allergic conjunctivitis. Ind J Ophthalmol. 2024;72(Suppl 5):S728–s733. In eng. doi:10.4103/ijo.Ijo_654_24
28. Morgan I, Rose K. How genetic is school myopia? Prog Retin Eye Res. 2005;24(1):1–38. In eng. doi:10.1016/j.preteyeres.2004.06.004
29. Sun Y, Guo Y, Pang R, Peng J, Cao K, Wang N. Corneal biomechanical properties and potential influencing factors in varying degrees of myopia. Sci Rep. 2024;14(1):20626. doi:10.1038/s41598-024-71676-w
30. Williams KM, Bertelsen G, Cumberland P, et al. Increasing prevalence of myopia in Europe and the impact of education. Ophthalmology. 2015;122(7):1489–1497.In eng. doi:10.1016/j.ophtha.2015.03.018
31. Shu Z, Chen K, Wang Q, et al. The role of retinal dopamine D1 receptors in ocular growth and myopia development in mice. J Neurosci. 2023;43(48):8231–8242.In eng. doi:10.1523/jneurosci.1196-23.2023
32. Zhou X, Pardue MT, Iuvone PM, Qu J. Dopamine signaling and myopia development: what are the key challenges. Prog Retin Eye Res. 2017;61:60–71. In eng. doi:10.1016/j.preteyeres.2017.06.003
33. Borchert GA, Kandel H, Watson SL. Epithelium-on versus epithelium-off corneal collagen crosslinking for keratoconus: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2024;262(6):1683–1692. In eng. doi:10.1007/s00417-023-06287-8
34. Wang M, Corpuz CCC, Zhang F. Shaping eyeballs by scleral collagen cross-linking: a hypothesis for myopia treatment. Front Med Lausanne. 2021;8:655822. In eng. doi:10.3389/fmed.2021.655822
35. Priftis N, Panagiotakos D. Screen time and its health consequences in children and adolescents. Children. 2023;10(10). In eng. doi:10.3390/children10101665
36. Mesce M, Ragona A, Cimino S, Cerniglia L. The impact of media on children during the COVID-19 pandemic: a narrative review. Heliyon. 2022;8(12):e12489. In eng. doi:10.1016/j.heliyon.2022.e12489
37. Mazharian A, Panthier C, Courtin R, et al. Incorrect sleeping position and eye rubbing in patients with unilateral or highly asymmetric keratoconus: a case-control study. Graefes Arch Clin Exp Ophthalmol. 2020;258(11):2431–2439.In eng. doi:10.1007/s00417-020-04771-z
38. Najmi H, Mobarki Y, Mania K, et al. The correlation between keratoconus and eye rubbing: a review. Int J Ophthalmol. 2019;12(11):1775–1781.In eng. doi:10.18240/ijo.2019.11.17
39. Li X, Wei A, Yang Y, Hong J, Xu J. Effect of eye rubbing on corneal biomechanical properties in myopia and emmetropia. Front Bioeng Biotechnol. 2023;11:1168503. In eng. doi:10.3389/fbioe.2023.1168503
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characterization of Corneal Biomechanics Using CORVIS ST Device in Different Grades of Myopia in a Sample of Middle Eastern Ethnicity
El-Mayah E, Albalkini AS, Barrada OA
Clinical Ophthalmology 2024, 18:901-912
Published Date: 21 March 2024
Brillouin Metrics of the Crystalline Lens Comparison Between Low-Medium Myopia and High Myopia
Bao Y, Ma Y, Cao J, Yu Y, Fukuyama T, Zhang Z, Niu L, Yao P, Wang X, Zhou X, Zhao J
Clinical Ophthalmology 2025, 19:4001-4009
Published Date: 29 October 2025