Back to Journals » Journal of Blood Medicine » Volume 13
Relationship Between Initial Parenteral Iron Therapy Dosing and Treatment Effectiveness: A Real-World Retrospective Analysis
Authors LaVallee C ![]() , Bansal I, Kamdar S, Kwong WJ, Boccia RV
, Bansal I, Kamdar S, Kwong WJ, Boccia RV
Received 19 November 2021
Accepted for publication 17 February 2022
Published 8 March 2022 Volume 2022:13 Pages 133—142
DOI https://doi.org/10.2147/JBM.S349070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Chris LaVallee,1 Isha Bansal,2 Shilpa Kamdar,2 Winghan Jacqueline Kwong,3 Ralph V Boccia4
1Health Outcomes Research, Decision Resources Group, Burlington, MA, USA; 2Analytics, Decision Resources Group, Burlington, MA, USA; 3Health Economics & Outcomes Research, Daiichi Sankyo Inc., Basking Ridge, NJ, USA; 4Center for Cancer and Blood Disorders, P.C, Bethesda, MD, USA
Correspondence: Winghan Jacqueline Kwong, Daiichi Sankyo, Inc., 211 Mt Airy Road, Basking Ridge, NJ, 07920, USA, Tel +1 908 992 7063, Email [email protected]
Purpose: Replacement iron is the main treatment for iron deficiency, but the relationship between initial intravenous (IV) dose and need for additional treatment is unclear. This study explored patterns of IV iron dosing in US clinical practice.
Methods: Patient records were obtained for adults who received IV iron for anemia between 2015 and 2017. Patients were classified into four groups: those who received < 1500 mg and ≥ 1500 mg IV iron and those received ≤ 1000 mg and > 1000 mg within 3 weeks of their first dose. The proportion of patients requiring additional IV iron after 30 days of the initial dose was evaluated.
Results: Data were obtained for 2959 patients receiving iron sucrose (44.2%), ferric carboxymaltose injection (FCM) (25.8%), and ferumoxytol (FM) (14.3%). Overall, 567 patients (19%) received ≥ 1500 mg of IV iron and 942 (32%) received > 1000 mg of IV iron within the first 21 days. Mean (SD) baseline iron deficit was 1001 mg (312). Patients who received ≥ 1500 mg had a 32% lower probability of receiving additional IV iron than those who received < 1500 mg (adjusted hazard ratio [HR]: 0.68 [95% confidence interval (CI); 0.58, 0.81]) and incurred significantly fewer outpatient visits for all causes (p < 0.001) and IV iron treatment (p < 0.001). Patients who received an initial dose of > 1000 mg had a 41% lower probability of receiving additional IV iron than those who received ≤ 1000 mg (adjusted HR: 0.59 [95% CI; 0.52, 0.67]) and had significantly fewer outpatient visits for all causes (p < 0.001) and IV iron treatment (p < 0.001). Patients receiving FCM required fewer outpatient visits than those receiving FM and other treatments, including a subgroup of patients who initially received > 1000 mg IV iron.
Conclusion: Higher doses of IV iron within 3 weeks of first dose may reduce further IV iron treatment needs and outpatient visits.
Keywords: anemia, ferric carboxymaltose injection, ferumoxytol, iron sucrose
Introduction
Iron deficiency anemia is the most prevalent form of anemia globally and can occur in patients with chronic diseases and inflammation, sometimes alongside anemia of chronic disease (ACD).1–3 Improved diets and living standards have resulted in the global burden of iron deficiency anemia decreasing over time, from 11.2% of all years of life with disability in 1990 to 8.8% in 2010.3 Anemia is now most prevalent in women of reproductive age (primarily due to menstruation) and in children, and a high prevalence of iron deficiency anemia also exists in people with gastrointestinal disorders.4,5 Symptoms of anemia include weakness and fatigue, and reduced aerobic capacity, which can impact work performance.3,6,7 If not properly treated, severe anemia can lead to hypoxia, potentially resulting in organ damage.8
Replacement iron is the mainstay therapy for iron deficiency anemia.5,8,9 Oral iron therapy is often prescribed for iron deficiency anemia, but its effectiveness is diminished and uptake from the gut is limited in patients with gastrointestinal diseases. Although blood transfusion is an effective treatment in patients with active bleeding, it only offers a temporary solution and does not address the underlying problem for iron deficiency anemia.5 Consequently, parenteral (intravenous [IV]) iron therapy is often necessary for patients with iron deficiency anemia associated with chronic diseases (often gastrointestinal diseases that make oral iron supplements ineffective), those with a large or sustained loss of iron, and those who cannot tolerate oral iron.5,8,10
Parenteral iron therapies that are currently available in the US vary in dose and administration schedule, and include ferric carboxymaltose (FCM), ferumoxytol (FM), iron sucrose, ferric derisomaltose, sodium ferric gluconate, and iron dextran.11
Currently, data on the association between initial IV iron dose given, durability of treatment effectiveness, and the risk of iron deficiency relapse are limited. In a previous investigation of initial IV iron dose and retreatment in patients treated with iron isomaltoside (Scandinavian NIMO study),12 an initial >1000 mg dose of iron isomaltoside significantly reduced the need for retreatment up to 12 months and had a higher treatment response rate compared to an initial dose of 1000 mg or lower.12 However, the evaluation was limited to a single IV iron product in a study sample mostly composed of patients with inflammatory bowel diseases. It remains unclear if the findings are generalizable to a broader patient population receiving parenteral iron replacement therapy in US clinical practice.
The objective of this analysis was to characterize patterns of IV iron dosing in US clinical practice and examine the association between initial IV iron dose and real-world treatment effectiveness as assessed by the need for additional IV iron treatment and serum hemoglobin normalization.
Methods
Patient Data Source and Eligibility
Records data were obtained from the DRG real-world evidence (RWE) data repository US database; this database includes medical and pharmacy claims and electronic health record (EHR) data for >300 million patients from 2011 to the time of the study, covering approximately 98% of US health plans. Data from all sources is linked via a direct-matching algorithm and then de-identified at the patient level, enabling longitudinal tracking of patients across data sources and sites of care. Linked claims data and EHRs were available for approximately 75 million patients.13
Patients were included if they were adults (aged ≥18 years) who received IV iron between 1st March 2015 and 28th February 2017 and had anemia, defined as a baseline serum hemoglobin (Hgb) level below normal (<12 g/dL for females and <13.5 g/dL for males) in the 30 days before or on the date of the index (first) IV iron claim. Patients were excluded if they had received IV iron within 6 weeks of index date, were on dialysis, or if their total iron dose exceeded 4000 mg (inclusive of index dose) over 21 days. Iron doses in excess of 4000 mg were deemed an unlikely and unsafe amount of iron, indicating a potential error in data reporting.
Analysis
The design of the study is summarized in Figure 1. Iron deficit was estimated using the modified Ganzoni equation.14 Eligible patients were classified into four dose groups (not mutually exclusive): 1) patients with a total IV iron dose ≥1500 mg, 2) patients with a total IV iron dose <1500 mg, 3) patients receiving a total IV iron dose of >1000 mg and 4) patients with a total IV iron dose ≤1000 mg, within 21 days of 1st dose. The 21-day cut-off was chosen because the US prescribing information for FM and FCM recommend completing a full course within 7–14 days; a further 7 days were allowed in order to account for potential scheduling issues arising in the real-world setting. In addition, patients were classified into three mutually exclusive treatment groups based on the index IV iron product that they received: 1) patients who received FCM; 2) patients who received FM; and 3) patients who received other IV iron products except FCM and FM.
 |
Figure 1 Study design. Abbreviation: Hgb, hemoglobin. |
Treatment effectiveness was assessed by the proportion of patients achieving normalized serum Hgb level within 12 months of index dose, defined as ≥12 g/dL for females and ≥13.5 g/dL for males. Durability of iron replacement therapy was operationally defined as the absence of additional IV iron dose 30 days after initial dose. As such, the proportion of patients receiving additional IV iron after 30 days of the initial dose was compared between dose groups of ≥1500 mg vs <1500 mg initial IV iron dose using Cox proportional hazards regression, adjusted for comorbidities, baseline serum Hgb and baseline iron deficit level. In addition, mean number of all-cause outpatient visits and visits associated with IV iron infusion were assessed. Similar analyses were performed comparing patients who received >1000 mg vs ≤1000 mg initial IV iron dose.
Ethical Considerations
This study was conducted in accordance with ethical guidelines outlined in the Declaration of Helsinki. The research protocol followed in this retrospective study used de-identified secondary administration claims and electronic medical records (EMRs) that were collected for routine medical care and billing purposes. These data were compliant with the Health Insurance Portability and Accountability Act (HIPAA) Privacy rule, and thus the study did not require institutional review board (IRB) review. The claims and EHR data are linked together by a HIPAA-compliant encrypted patient key generated by a third party. It was not possible to contact patients to obtain informed consent as the data were de-identified.
Results
Patient Characteristics
In total, 2959 patients were included in the analysis (Figure 2; Table 1). At baseline, 58.4% were aged ≥65 years; 68.1% were female; mean (standard deviation [SD]) baseline Hgb was 9.7 g/dL (1.4); and median (SD) follow-up period length was 107 weeks (27.8). In total, 43% of patients (1285) had an iron deficit of >1000 mg.
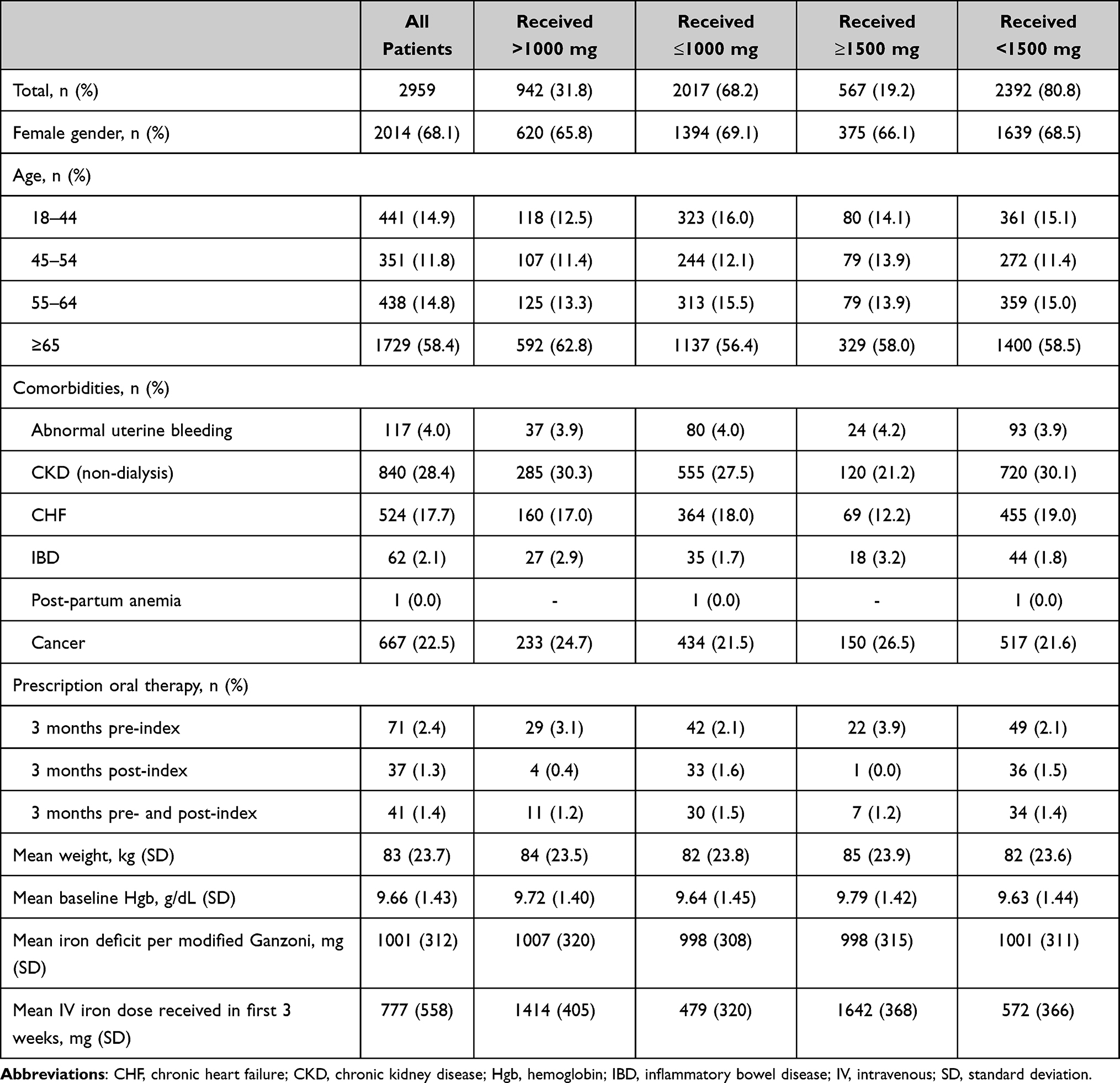 |
Table 1 Cohort Demographics and Characteristics |
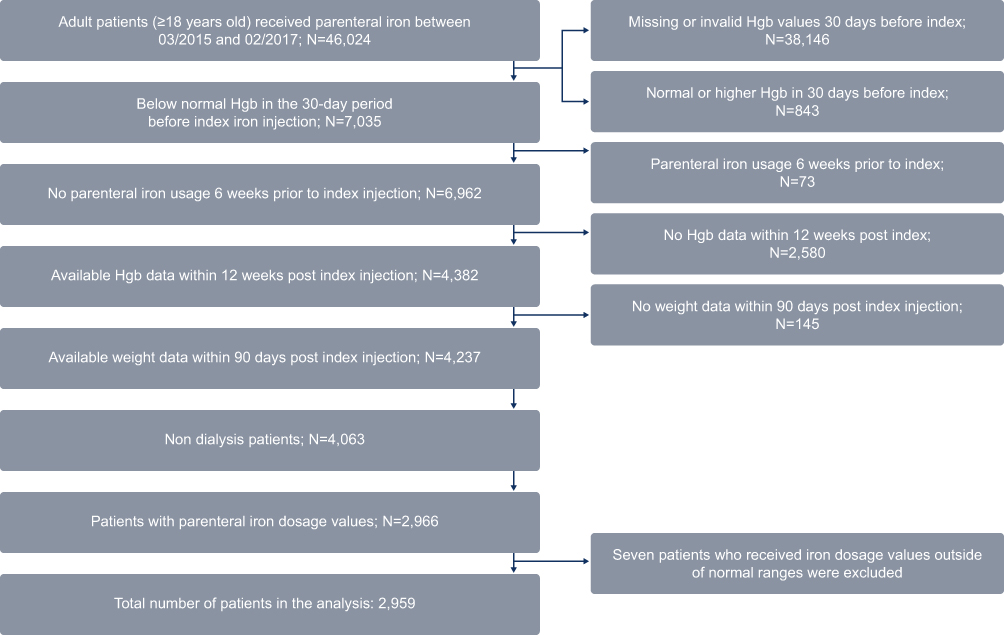 |
Figure 2 Patient sample attrition. Abbreviation: Hgb, hemoglobin. |
IV Iron Treatment Received
Iron sucrose was the most frequently used treatment type, received by 1309 patients (44.2%), followed by FCM (n = 763; 25.8%) and FM (n = 422; 14.3%; Table 2). Only 567 patients (19%) received ≥1500 mg of total IV iron, and 942 patients (32%) received >1000 mg total IV iron within the first 21 days.
 |
Table 2 Type of IV Iron Treatments Received by Cohort |
Mean (SD) index dose was 743 mg (148) for FCM, 466 mg (154) for FM, and 197 mg (222) for patients receiving other IV iron products. Two-thirds (66%) of patients treated with FCM received ≥1500 mg of total IV iron during the first 21 days (Figure 3), compared with 6% of patients treated with FM and 2% of patients receiving other iron products. Approximately 73% of patients treated with FM received >1000 mg of total IV iron during the first 21 days (Figure 3), compared with 66% of FCM patients and 7% of patients receiving other iron products.
 |
Figure 3 Proportion of patients receiving IV iron products within 21 days of index by dose (A) <1500 mg and ≥1500 mg and (B) ≤1000 mg and >1000 mg. Abbreviations: FCM, ferric carboxymaltose; FM, ferumoxytol; IV, intravenous; OTH, other. |
Patient demographics, comorbidities, and mean baseline serum Hgb were similar for those receiving >1000 mg and ≤1000 mg of IV iron within the first 21 days. Patients receiving ≥1500 mg of IV iron had a lower proportion of chronic kidney disease and congestive heart failure but a higher proportion of inflammatory bowel disease and cancer compared with patients who received <1500 mg of IV iron within the first 21 days. Mean (SD) baseline iron deficit for the overall study sample was 1001 mg (312) and it was similar for those receiving >1000 mg, ≤1000 mg, ≥1500 mg and <1500 mg of IV iron within the first 21 days. Mean (SD) total IV iron dose was 777 mg (558) over the first 21 days after the index dose in the overall study sample. Mean (SD) doses were 1414 mg [405] for those receiving >1000 mg and 1642 mg [368] for those receiving ≥1500 mg of IV iron. For those receiving ≤1000 mg and <1500 mg of IV iron, the mean (SD) doses were 479 mg (320) and 572 mg (366), respectively, over the first 21 days.
Serum Hemoglobin Normalization and Further IV Iron Treatment Requirements
Within 12 months of the index dose, the proportion of patients achieving normalized serum Hgb was highest for those receiving ≥1500 mg (62%), followed by patients receiving >1000 mg (56%) as compared to those receiving <1500 mg (45%) and ≤1000 mg (44%) over the first 21 days (p < 0.001; Figure 4). The mean (standard error [SE]) number of all-cause outpatient visits and the mean (SE) number of outpatient visits for IV iron treatment were significantly lower in patients receiving ≥1500 mg than <1500 mg iron (all-cause visits: 10 [0.59] and 13 [0.33], respectively [p < 0.001]; IV iron treatment visits: 2 [0.08] and 4 [0.06], respectively [p < 0.001]; Figure 4). Similarly, the mean (SE) number of all-cause outpatient visits and the mean (SE) number of outpatient visits for IV iron treatment was significantly lower in patients receiving >1000 mg than ≤1000 mg iron required significantly fewer outpatient visits (all-cause visits: 11 [0.46] vs 14 [0.37], respectively, p < 0.001; IV iron treatment visits: 3 [0.08] vs 4 [0.07], respectively, p < 0.001; Figure 4). During the 12-month period after index IV dose, the proportion of patients requiring ≥3 IV iron infusions was lowest among patients who received an initial dose of ≥1500 mg during the first 21 days (39%), followed by patients who received an initial dose of >1000 mg (43%), patients who received <1500 mg (56%) and those who received <1000 mg (57%) over the first 21 days.
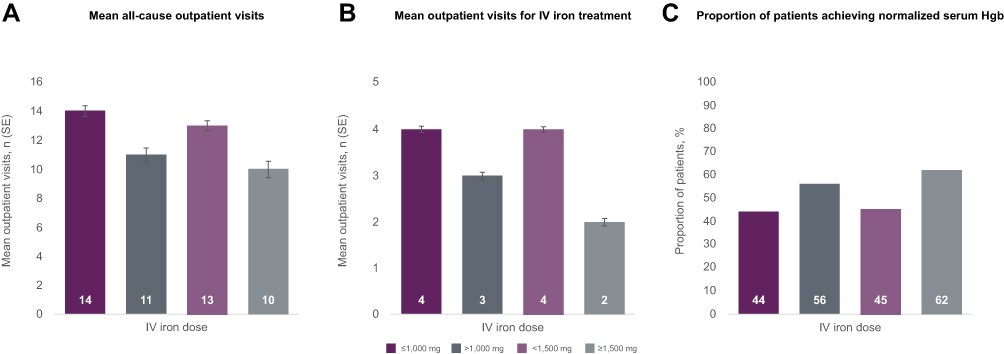 |
Figure 4 Outcomes in patients receiving an initial dose of IV iron. (A) Mean all-cause outpatient visits, (B) mean outpatients visits for IV iron treatment and (C) proportion of patients achieving normalized serum Hgb. Abbreviations: IV, intravenous; SE, standard error. |
After adjusting for comorbidities, baseline serum Hgb level and baseline iron deficit level, patients who received an initial dose of ≥1500 mg had a 32% lower probability of receiving additional IV iron 30 days after index IV iron dose than those who received <1500 mg (adjusted hazard ratio [HR]: 0.68 [95% confidence interval (CI); 0.58, 0.81]; Figure 4) during the entire study follow-up period. For those who received an initial dose of >1000 mg during the first 21 days after index IV iron dose, the probability of receiving additional IV iron 30 days after index IV iron dose was 41% lower than for those who received ≤1000 mg (adjusted HR: 0.59 [95% CI; 0.52, 0.67]; Figure 5).
 |
Figure 5 Probability of receiving an additional IV iron dose during study follow-up period in patients receiving (A) <1500 mg and ≥1500 mg and (B) ≤1000 mg and >1000 mg. Abbreviation: IV, intravenous. |
Among the three IV iron product groups, FCM had the highest proportion of patients achieving normal serum Hgb level (61%) and the lowest proportion of patients requiring ≥3 IV iron infusions within 12 months of index IV iron dose (27%) (Figure 6). The mean number of all-cause outpatient visits and visits related to IV infusion within 12 months of treatment was highest among patients treated with “other” IV iron therapies, and the lowest proportion was of those treated with FCM (Figure 6). Treatment group differences were similar in the subgroup of patients with a >1000 mg deficit.
 |
Figure 6 Post-infusion resource use by treatment type. (A) Patients requiring ≥3 injections within 12 months, (B) proportion of patients achieving normalized serum Hgb within 12 months, (C) mean all-cause outpatient visits, (D) mean outpatient visits for iron infusion. Abbreviations: FCM, ferric carboxymaltose; FM, ferumoxytol; Hgb, hemoglobin; IV, intravenous. Notes: *Statistically significant difference vs FM (p < 0.001); †statistically significant difference vs other (p < 0.001). |
Discussion
This analysis showed that high doses of IV iron within three weeks of first dose may offer an effective treatment option that is convenient for patients with iron deficiency anemia in need of parenteral therapy. By reducing the need to return for further treatment, high iron doses may minimize the risk of treatment ineffectiveness due to patient non-compliance and reduce healthcare resource utilization in patients with iron deficiency anemia receiving IV iron therapy.
Results of these data suggest that underdosing is common in real-world practice and it should be a consideration when initiating treatment. Despite a mean iron deficit of 1001 mg in the study sample, the mean IV iron dose received during the 3 weeks from index was only 777 mg. Mean iron deficit levels did not differ across dose groups, corroborating previous findings that baseline iron deficits are often not considered when choosing between IV iron products and determining IV iron dose for repletion in real-world practice.15 Moreover, our data suggested that many patients did not receive IV iron consistent with a product’s dosing recommendations. For example, during the first 21 days of treatment, our study showed that one in three patients treated with FCM received total cumulative IV iron dose lower than the recommended dose of 1500 mg of total IV iron. Similarly, approximately 1 in 4 of patients treated with FM received IV iron dose lower than the recommended cumulative total dose of 1020 mg. Although the reason for underdosing is unclear, possible barriers to adequate dosing might be poor follow-up or patients not returning to clinic after their first dose of IV iron.
At the time of this study, FCM and FM were the only IV iron products available on the US market providing a total cumulative dose >1000 mg in an initial course of IV iron therapy. In this study, treatment with IV iron of ≥1500 mg and >1000 mg was associated with significant reduction in the likelihood of additional IV iron treatment after 30 days. Treatment with FCM was also associated with lowest number of outpatient visits and the highest likelihood of normalized Hgb recovery among the three IV product groups, across both the overall cohort and the subgroup of patients with an iron deficit of >1000 mg. This indicates that the clinical benefit of high-dose IV iron is not only limited to patients with a high estimated iron deficit; rather, full replenishment of iron with a high dose IV product in the first 3 weeks of treatment appears to be important in reducing the clinical and economic burden of patients with iron deficiency anemia, irrespective of deficit. The mean number of infusion-related office visits in the low-dose IV iron group was highest and doubled that of patients treated with FCM and FM, but the proportion of patients achieving normalized serum Hgb was lowest for the low-dose IV iron group. These results suggest that giving low dose IV iron more frequently may be ineffective to provide sufficient iron repletion.
The study has several limitations. First, the study was a retrospective analysis of claims and EMR data from an open network. Claims data are often adjudicated on an ongoing basis. Healthcare services provided by out-of-network providers may not be captured by the database, which could lead to imprecision in the healthcare resource utilization results. Additionally, use of concomitant over-the-counter oral iron replacement medications was not captured by the database. We cannot completely rule out possible confounding from patient self-administered oral iron supplementation. Because the study required serum Hgb data, patients who did not have complete Hgb data recorded in EMRs were excluded, which could limit the generalizability of the study findings. A higher proportion of cancer patients and lower proportions of patients having non-dialysis dependent chronic kidney disease and congestive heart failure were observed among patients receiving ≥1500 mg dose group than the <1500 mg group. Future studies are needed to determine the effect of these comorbidities on study results. Because ferritin data were limited in the database, we were unable to assess iron stores to further understand the durability of iron repletion. Ferric derisomaltose was recently approved in the US and its data were not available at the time of the study. Future studies including data from ferric derisomaltose will provide a more comprehensive assessment on the effect of high dose IV iron on clinical and economic burden of iron deficiency anemia among US patients. A longer-term assessment could provide better insights into long-term patient outcomes.
Conclusion
In a real-world US setting, initial treatment with higher total dose of IV iron was associated with improved serum hemoglobin levels, reduced need for further iron treatment and lower healthcare resource utilization.
Funding
This research was funded by Daiichi Sankyo Inc.
Disclosure
CL, IB, and SK were employees of Clarivate, a healthcare analytics consultancy, at the time of the study. WJK is an employee of Daiichi Sankyo Inc. RVB was a consultant to Daiichi Sankyo, Amgen, Bristol Myers Squibb, AMAG, SecuraBio, and was on the speaker’s bureau of Rigel and Celgene during the time of this study. The authors report no other conflicts of interest in this work.
References
1. Camaschella C. New insights into iron deficiency and iron deficiency anemia. Blood Rev. 2017;31(4):225–233. doi:10.1016/j.blre.2017.02.004
2. Poggiali E, Migone De Amicis M, Motta I. Anemia of chronic disease: a unique defect of iron recycling for many different chronic diseases. Eur J Intern Med. 2014;25(1):12–17. doi:10.1016/j.ejim.2013.07.011
3. Kassebaum NJ, Jasrasaria R, Naghavi M, et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood. 2014;123(5):615–624. doi:10.1182/blood-2013-06-508325
4. World Health Organization (WHO). The global prevalence of anaemia in 2011; 2015. Available from: https://apps.who.int/iris/handle/10665/177094.
5. Jimenez K, Kulnigg-Dabsch S, Gasche C. Management of iron deficiency anemia. Gastroenterol Hepatol (N Y). 2015;11(4):241–250.
6. Haas JD, Brownlie T. Iron deficiency and reduced work capacity: a critical review of the research to determine a causal relationship. J Nutr. 2001;131(2s–2):
7. Lasch KF, Evans CJ, Schatell D. A qualitative analysis of patient-reported symptoms of anemia. Nephrol Nurs J. 2009;36(6):
8. Johnson-Wimbley TD, Graham DY. Diagnosis and management of iron deficiency anemia in the 21st century. Therap Adv Gastroenterol. 2011;4(3):177–184. doi:10.1177/1756283X11398736
9. Goddard AF, James MW, McIntyre AS, Scott BB. Guidelines for the management of iron deficiency anaemia. Gut. 2011;60(10):1309. doi:10.1136/gut.2010.228874
10. De Franceschi L, Iolascon A, Taher A, Cappellini MD. Clinical management of iron deficiency anemia in adults: systemic review on advances in diagnosis and treatment. Eur J Intern Med. 2017;42:16–23. doi:10.1016/j.ejim.2017.04.018
11. Auerbach M, Macdougall I. The available intravenous iron formulations: history, efficacy, and toxicology. Hemodial Int. 2017;21(Suppl 1):S83–s92. doi:10.1111/hdi.12560
12. Frigstad SO, Haaber A, Bajor A, et al. The NIMO Scandinavian study: a prospective observational study of iron isomaltoside treatment in patients with iron deficiency. Gastroenterol Res Pract. 2017;2017:4585164. doi:10.1155/2017/4585164
13. Decision Resources Group (DRG). Real world evidence US data repository; 2015. Available from: https://clarivate.com/products/real-world-data/.
14. Koch TA, Myers J, Goodnough LT. Intravenous iron therapy in patients with iron deficiency anemia: dosing considerations. Anemia. 2015;2015:763576. doi:10.1155/2015/763576
15. LaVallee C, Cronin P, Bansal I, Kwong WJ, Boccia RV. Effectiveness of parenteral iron therapy in the real-world setting: a retrospective analysis. J Clin Haematol. 2020;1(1).
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.