Back to Journals » Journal of Inflammation Research » Volume 18
Relationship Between Inflammation-Nutrition Composite Indices and Ovarian Endometrioma: A Retrospective Observational Study
Authors Zhang Y ![]() , Zeng NM, Fan JY, Qiu JP, Jiang FD, Wang Y
, Zeng NM, Fan JY, Qiu JP, Jiang FD, Wang Y
Received 29 April 2025
Accepted for publication 21 October 2025
Published 27 October 2025 Volume 2025:18 Pages 14871—14880
DOI https://doi.org/10.2147/JIR.S537407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yan Zhang,1 Ni Mei Zeng,1 Jing Yi Fan,1 Jian Ping Qiu,2 Fang Da Jiang,3 Yun Wang1
1Physical Examination Center, the Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou, Jiangsu, People’s Republic of China; 2Gynecological Department, the Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou, Jiangsu, People’s Republic of China; 3Internal Medicine Department, Aurora Oshkosh Medical Center, Oshkosh, Wisconsin, USA
Correspondence: Yun Wang, Physical Examination Center, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, No. 242, Guang Ji Road, Suzhou, 215008, People’s Republic of China, Email [email protected]
Objective: Endometriosis is a chronic inflammatory disease with impacts on reproduction, health and quality of life, yet its diagnosis is often delayed. Ovarian endometrioma (OMA) is the most common subtype of endometriosis. The establishment of simple predictive indicators could screen women at high risk of OMA, thereby potentially facilitating the early diagnosis and management of endometriosis. This study aimed to comprehensively evaluate the predictive performance of inflammation and inflammation-nutrition composite indices for ovarian endometrioma (OMA) among women of reproductive age in China.
Methods: A total of 333 women with diagnosed OMA and 506 controls were included in this study. Inflammation indices including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune inflammation index (SII) and inflammation-nutrition composite indices including neutrophil percentage‑to‑albumin ratio (NPAR), NLR/AGR, PLR/AGR, SII/AGR and neutrophil percentage/AGR(NP/AGR) were calculated. Multivariate logistic regressions were used to assess the associations of indices with OMA. Receiver operating characteristic (ROC) curves and areas under the curve (AUCs) were used to evaluate the predictive value of indices for OMA.
Results: Compared with women without OMA, inflammation indices (NLR, PLR, SII) and inflammation-nutrition composite indices (NPAR, NLR/AGR, PLR/AGR, SII/AGR, NP/AGR) in patients with OMA showed a significant increase. Subjects in the higher tertile of these indices had a significantly increased risk of OMA compared with those in the lower tertile (P < 0.01). NP/AGR had the greatest total AUC (AUC = 0.799) in the ROC curve analysis.
Conclusion: NPAR, NLR/AGR, PLR/AGR, SII/AGR and NP/AGR could provide additional clinical diagnostic value for OMA as non-invasive and cost-effective tests, and are better than inflammation indices (NLR, PLR, SII) alone. Among them, NP/AGR might be the best predictor.
Keywords: neutrophil-to-lymphocyte ratio, NLR, platelet-to-lymphocyte ratio, PLR, systemic immune inflammation index, SII, neutrophil-percentage-to-albumin ratio
Introduction
Endometriosis is a benign gynecological disease defined by the presence of endometrial-like tissues outside the uterus, which is thought to arise by retrograde menstruation typically, affecting 6–10% of women at reproductive age and up to 50% of women with infertility.1–3 Its common clinical symptoms include chronic pelvic pain, dysmenorrhea, dyspareunia, dysuria, dysphasia and infertility. Over 176 million women have suffered from endometriosis worldwide. However, 65% women were misdiagnosed initially, with the diagnosis time ranging from 4 to 11 years.3 Although the pathogenesis is unclear, endometriosis is certainly a chronic inflammation disorder that is associated with dysfunction in immune cells with a genetic component. Dysregulated immune cells, including neutrophils, lymphocytes, macrophages, natural killer (NK) cells and dendritic cells, play a crucial role in the pathogenesis of endometriosis and contribute to chronic inflammation and disease progression.4 Endometriosis is classified into three subtypes: superficial endometriosis, deep infiltrating endometriosis (DIE), and ovarian endometrioma (OMA), which is also known as chocolate cysts and accounts for 67%.5,6 Ultrasound is an effective method for diagnosing OMA (93% sensitivity and 95% specificity).3 New inflammation markers, such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune inflammation index (SII) and neutrophil-percentage-to-albumin ratio (NPAR), have emerged as promising tools for assessing and predicting systemic inflammation status.7–9 Among them, NPAR is a composite inflammation and nutrition biomarker at the same time. Higher NPAR indicates higher neutrophil-percentage or lower albumin, or both. Several studies suggested that NLR, PLR, SII, IL-6, IL-1β could provide additional diagnostic value for endometriosis.10–15 However, few focused on the relationship between inflammation-nutrition biomarkers and endometriosis. Serum albumin, globulin and albumin–globulin ratio (AGR) measurements reflect body’s nutrients and inflammatory. In inflammatory states, hypoalbuminemia and low AGR could be observed.16–18 Therefore, this study incorporated AGR into the formula to calculate NLR/AGR, PLR/AGR, SII/AGR and NP/AGR, thereby new inflammation-nutrition composite indicators were derived. We conducted an observational study to investigate whether these indices, including NPAR, NLR/AGR, PLR/AGR, SII/AGR, NP/AGR, could serve as predictive or supplementary markers for diagnosing ovarian endometrioma (OMA). If simple predictive indicators for OMA were identified, they would be used to screen women at high risk of OMA, thereby potentially facilitating the early diagnosis and management of endometriosis.
Materials and Methods
Study Population
The study participants were recruited from the Affiliated Suzhou Hospital of Nanjing Medical University. From 1st January 2017 to 31st March 2025, women who were initially diagnosed with endometriosis by ultrasound were selected as cases. Meanwhile, healthy women who came to our hospital for routine health examinations and did not have any infection within six months were chosen as controls. Exclusion criteria were as follows: 1) other known causes of chronic inflammatory disease; 2) active infections; 3) severe hematologic disorders; 4) recent use of anti-inflammatory or immunosuppressive drugs; 5) cancer; 6) pregnancy; 7) lactation; 8) major surgical interventions within the last 6 months; 9) missing or invalid data (Figure 1) Finally, a total of 333 cases and 506 controls were included in the analysis.
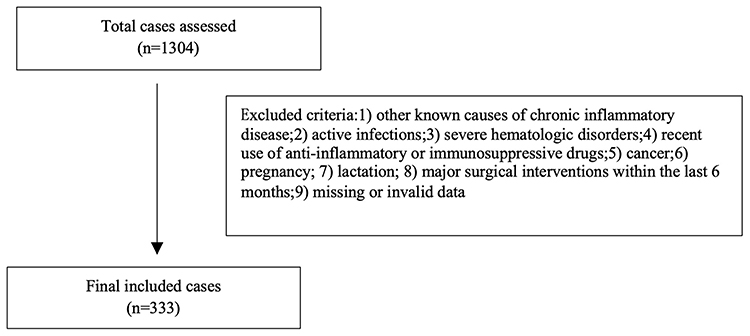 |
Figure 1 Flowchart of case selection for the study. |
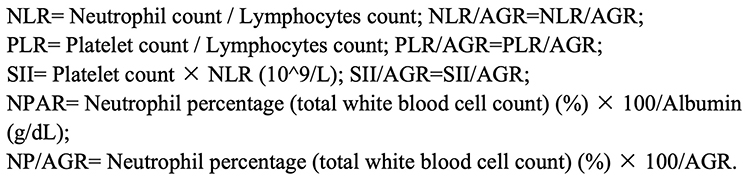 |
Figure 2 Equations of the inflammation indices and inflammation-nutrition composite indices. |
This study was conducted in accordance with the Declaration of Helsinki and approved by The Affiliated Suzhou Hospital of Nanjing Medical University Ethical Review Committee (KL901617).
Data Collection
Data including neutrophils, neutrophil percentage, monocytes, lymphocytes, platelets, albumin, globulin and AGR were retrospectively collected from the hospital information system. Inflammation indices (NLR, PLR, SII) and inflammation-nutrition composite indices (NPAR, NLR/AGR, PLR/AGR, SII/AGR, NP/AGR) were calculated by using the equations shown in Figure 2.7–9
OMA was diagnosed based on the ‘O-RADS US Risk Stratification and Management System: A Consensus Guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee’ by experienced ultrasonologists with expertise in OMA imaging. Images showed typical endometriomas: homogenous low-level or ground glass internal echoes, surrounding ovarian parenchyma is seen.19
Statistical Analysis
Numerical variables were expressed as medians and two specific percentiles (P25 and P75) for non-normally distributed data, and Mann–Whitney U-tests were used for comparison with two groups. Numerical variables were described as mean ± standard deviation for normally distributed data, and t-tests were used.
All inflammation and inflammation-nutrition composite indices were divided into 3 groups according to tertiles, respectively. Multivariate logistic regression analyses were used to evaluate the association between OMA and each index. Odds ratios (ORs) and 95% confidence intervals (CIs) were computed with the first tertile as a reference, adjusting for year. The trend across the tertiles of each index was conducted by using Cochran-Armitage trend test. Furthermore, we used receiver operating characteristic (ROC) curves and areas under the curves (AUC) to evaluate the predictive value of indices for OMA. All statistical analyses were performed with Statistical Package for the Sciences software (SPSS, version 29.0). A value of P < 0.05 in the two-tailed test was considered to be statistically significant.
Results
Baseline Characteristics in Both Groups
According to Table 1, subjects with OMA had increased levels of systolic blood pressure (SBP), diastolic blood pressure (DBP), body mass index (BMI), fasting blood glucose (FBG), triglycerides (TGs), uric acid (UA) (all P < 0.05). Table 1 also compared the inflammation and inflammation-nutrition indices of the individuals in both groups. Subjects with OMA had significantly higher globulin, total protein, PLT, Neutrophil counts (NC), Neutrophil percentage (NP), NLR, PLR, SII, NPAR, NLR/AGR, PLR/AGR, SII/AGR and NP/AGR than those in the control group (all P < 0.05), but had lower albumin, AGR, Lymphocyte counts (LC), Lymphocyte percentage (LP), Monocyte counts (MC) and Monocyte percentage (MP) (all P < 0.05).
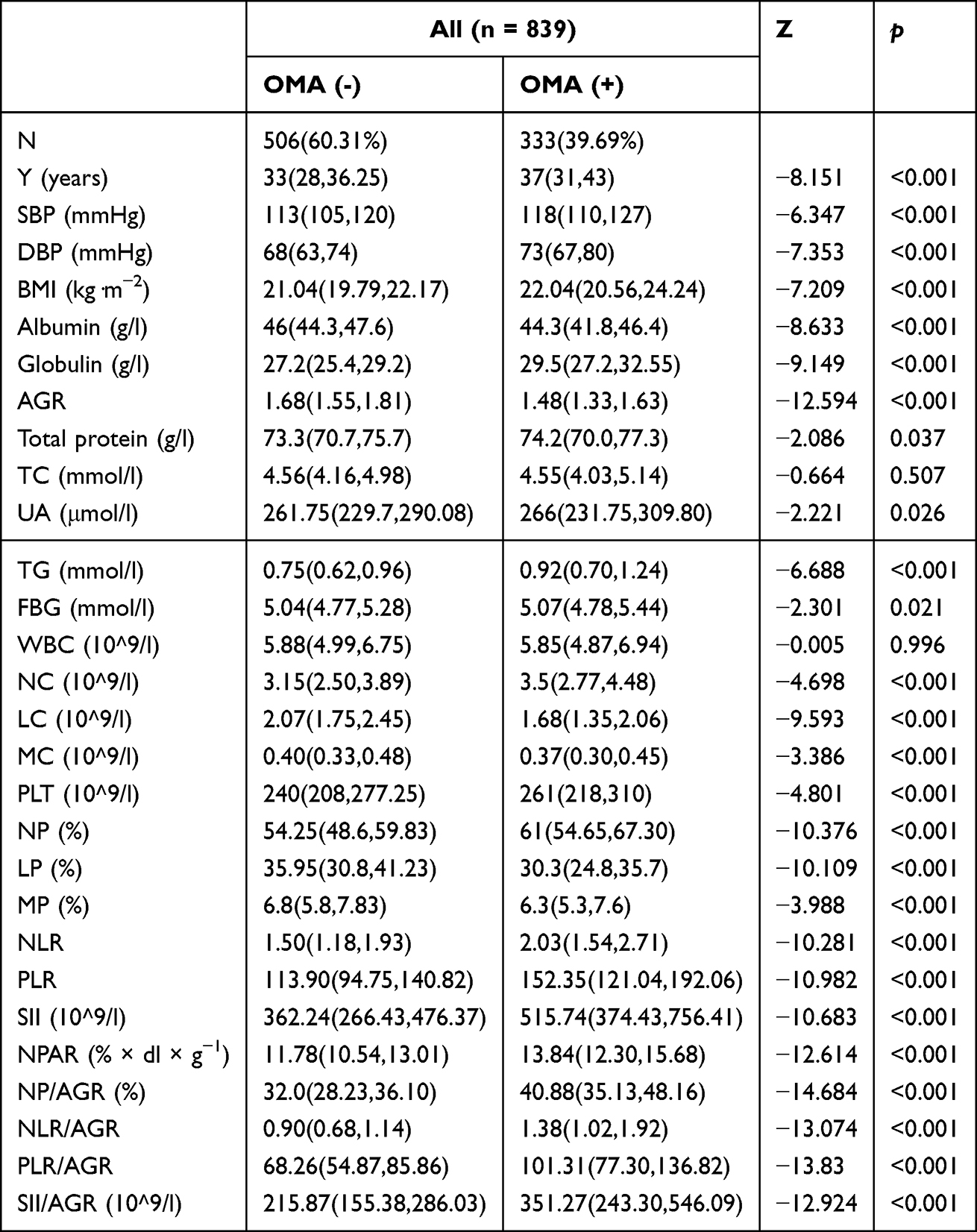 |
Table 1 Basic Characteristics in Two Groups |
Univariate and Multivariate Regression for Each Index with OMA
In Table 2, univariate and multivariate logistic regressions showed significant association (P < 0.01) between OMA and all indices (NLR, PLR, SII, NPAR, NLR/AGR, PLR/AGR, SII/AGR, NP/AGR) separately. According to multivariate logistic regression results, each index demonstrated a positive relation with OMA as the numerical variable. NLR/AGR had the maximum OR (OR = 4.43, 95% Cl 3.153–6.261, P < 0.001, Table 2).
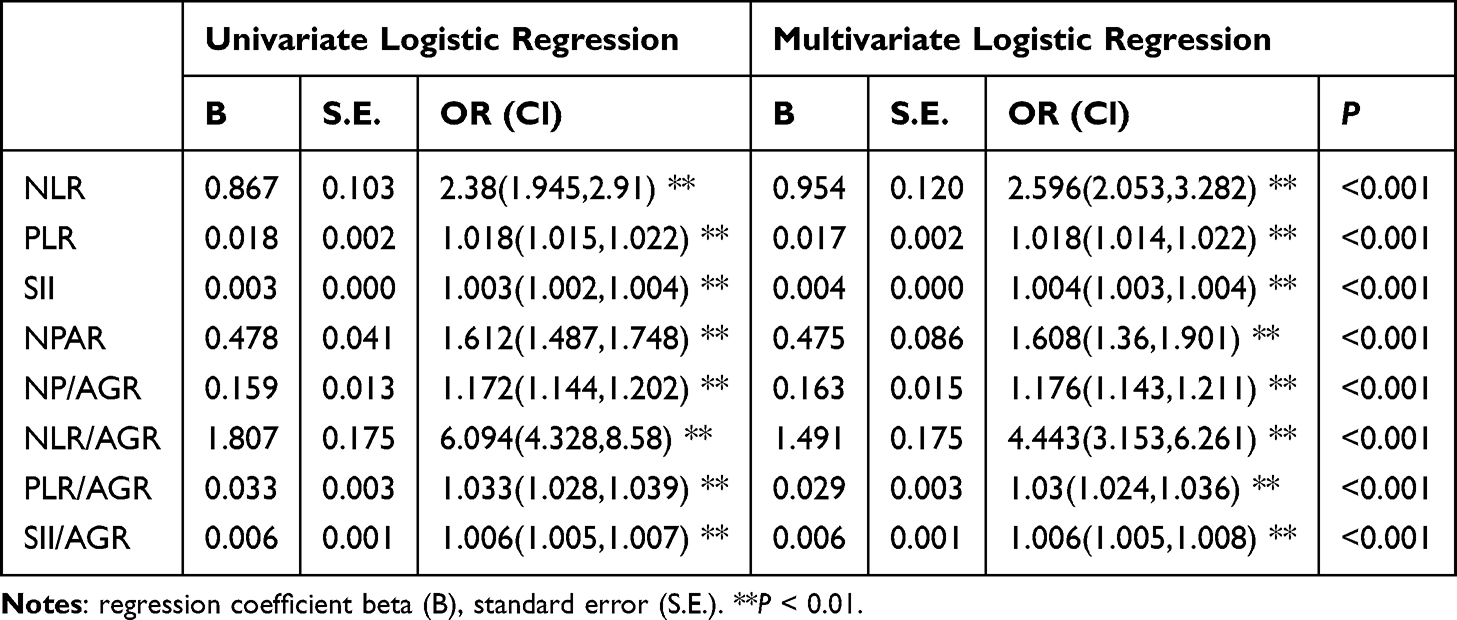 |
Table 2 Univariate and Multivariate Logistic Regression Analyses of Each Index |
Cochran–Armitage Trend Test of the Impact of Each Index on OMA Prevalence
In Table 3, increasing levels of NLR, PLR, SII, NPAR, NLR/AGR, PLR/AGR, SII/AGR and NP/AGR showed a significant linear trend with OMA, when concentrations were analyzed by a Cochran-Armitage trend test.
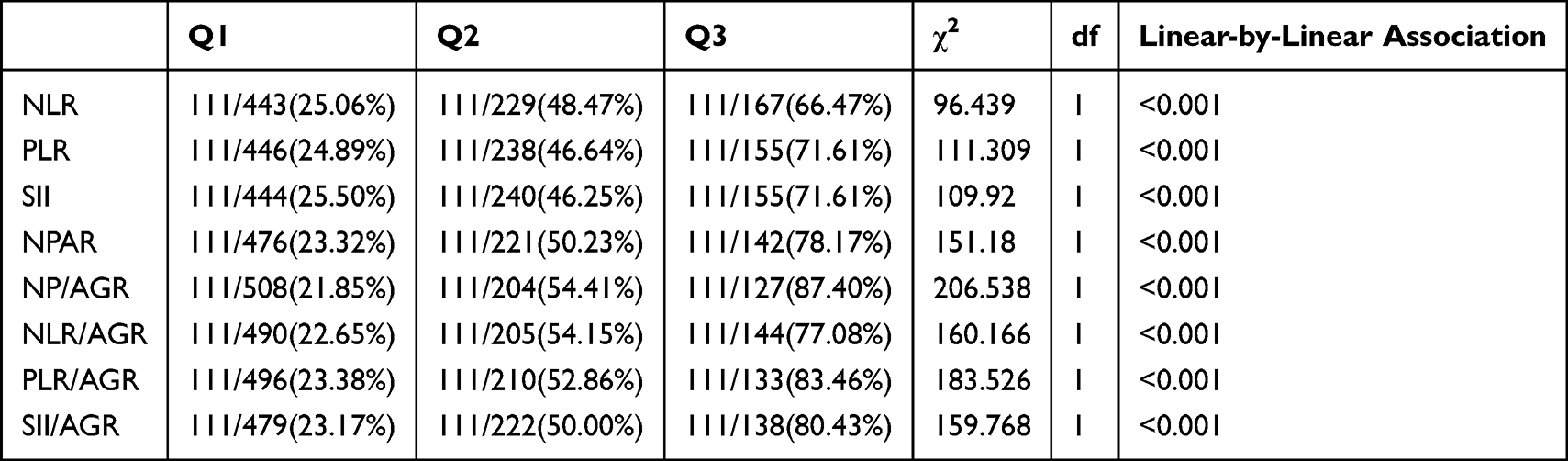 |
Table 3 Cochran–Armitage Trend Test of the Impact of Each Index on OMA Prevalence |
ORs for OMA Stratified by Tertiles of Each Index
Table 4 demonstrated that each index was significantly associated with OMA (P < 0.05). The ORs for OMA still increased across the tertiles of each index. Among all subjects, the NP/AGR showed the highest risk of OMA among all the indices, followed by PLR/AGR and SII/AGR.
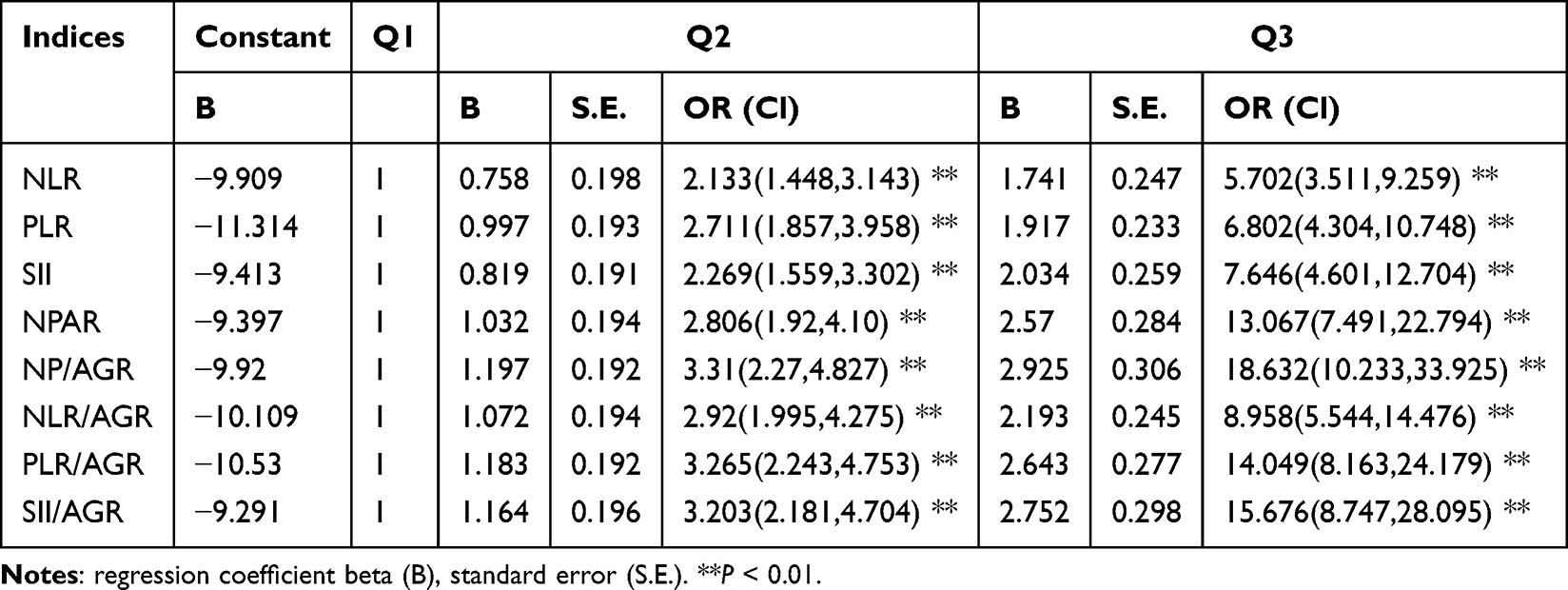 |
Table 4 ORs for OMA Stratified by Tertiles of Each Index |
ROC Curves and AUC for Indices in Identifying OMA
Table 5 showed that NP/AGR had the greatest AUC of 0.799, followed by PLR/AGR and NLR/AGR. Figure 3 presents the ROC curves and AUCs of all parameters for diagnosis of OMA.
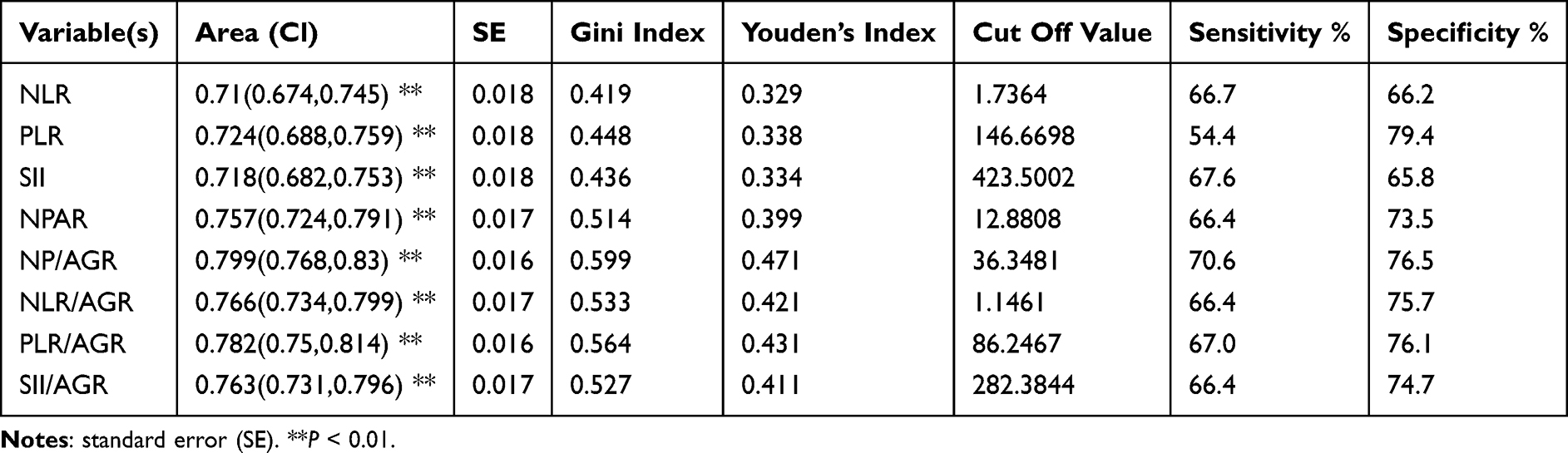 |
Table 5 AUC, Youden Index, Sensitivity, Specificity and Cut-off Point of Each Index for Predicting OMA |
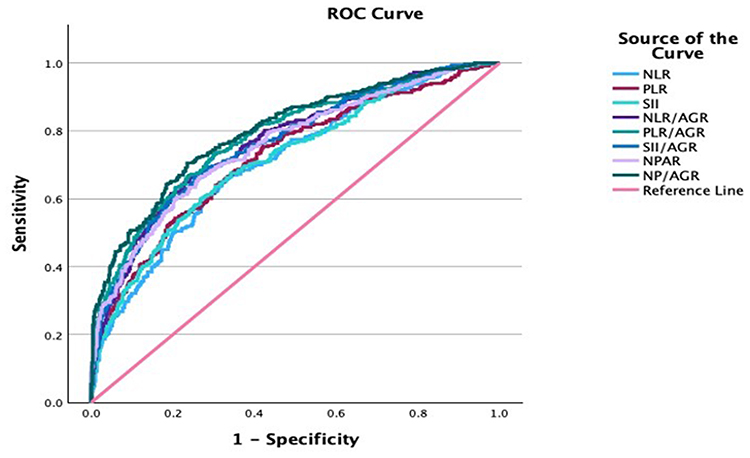 |
Figure 3 Comparison of the predictive value of all parameters for diagnosis of OMA. |
Discussion
Increasing evidence supported conceptualization of endometriosis as a systemic inflammatory disorder.3 A previous study showed that neutrophils (NT) are essential for the initial formation of endometriosis.20 In a mouse model of endometriosis, depletion of NT decreased the number of endometriotic lesions.20 NT produce angiogenic factors such as VEGF and pro-inflammatory cytokines, including IL-8 and CXCL10, and also reactive oxygen species, which may promote disease progression.21 Additionally, a defect in T-lymphocyte cytotoxicity occurs in women having endometriosis, which may contribute towards endometrial cell’s evasion from immune clearance.22 Neutrophilia and lymphocytopenia in endometriosis are often reported in the literature.12,23,24 However, the precise roles of lymphocyte cells in endometriosis, including B cells, T cells and NK cells, still require more investigations. In this study, higher neutrophil counts and neutrophils percentage, accompanied by lower lymphocyte counts, were seen in the cases compared to controls. Neutrophilia, along with a relative lymphocytopenia, yielded an increased NLR in patients with OMA, which is similar to the conclusion in another study.24
Inflammation and coagulation are two main host-defense systems that interact with each other.25 Inflammation activates coagulation, which modulates the inflammatory activity in many ways. Activated platelets were found to play a critical role in initiating inflammation.26
In OMA patients, more platelets were observed. This is supported by pathophysiological and clinical studies,27 which reported that platelets aggregated in endometriotic lesions and platelet depletion resulted in markedly reduced lesion size. Moreover, the elevated levels of PLR and SII in OMA patients are consistent with this notion in another study.28 Our data further confirmed an inflammatory status in OMA. Several studies suggested that NLR, PLR and SII could serve as adjunctive indicators for the severity of endometriosis.10,23,28 SII was also considered as a potential biomarker for predicting the risk of endometriosis.15,29
Additionally, endometriosis is a debilitating disease. Inflammation could lead to malnutrition in patients with sufficient nourishment. In addition, malnutrition may further induce an inflammatory response.18 Albumin can reflect not only the nutritional but also the inflammatory status. Monocyte products play an important role in reducing albumin production during inflammation.30 Globulin consists of many proteins related to inflammation, which also increases during the inflammatory process.18 Interleukin (IL)-6, one of the pro-inflammatory cytokines affecting OMA,14 increases immunoglobulin levels but reduces albumin production.31 Therefore, AGR indicates body’s nutritional and inflammatory status more accurately. These findings may explain the result that women with OMA have lower albumin and AGR but higher globulin. Therefore, in the case group, NPAR, NLR/AGR, PLR/AGR, SII/AGR and NP/AGR values considerably increased and had a greater diagnostic ability for OMA than NLR, PLR, SII.
This study also revealed that NP/AGR exhibited the greatest AUC among all indices. These findings align with a report,32 which reported that neutrophils accumulated in the OMA and the amounts of neutrophils were associated with the severity of OMA. Based on the above analysis, NP/AGR might describe the condition in OMA better.
In our study, inflammation-nutrition indices had receiver-operating characteristic areas under the curve ranging from 0.757 to 0.799, which had promising power for predicting OMA. While our study focused on the diagnosis abilities of inflammation-nutrition indices, based on the available literature,33–51 it is reasonable to infer that these indices could potentially be applied to innovative personalized medical care, which requires further research.
Firstly, inflammation-nutrition indices might serve as adjuncts to microRNAs (miRNAs) for the diagnosis of OMA. Several studies revealed that miRNAs have emerged as novel and potential biomarkers for endometriosis.33,34 Due to enhanced production IL-6, IL-1β and TNF-α involved in proinflammation, serum levels of miR125b-5p were upregulated, while let-7b-5p were downregulated in patients with endometriosis.35 A study suggested that let-7b had an AUC of 0.78, miR125b had an AUC of 0.73, and both combined with other miRNA makers (miR150, miR342, miRNA451a, miRNA3613) yielded an AUC of 0.93 (96% specificity and 83% sensitivity), thus demonstrating their potential as diagnostic biomarkers for endometriosis.36 Compared with relevant miRNAs, it is easier and cheaper to measure inflammation-nutrition composite indices. And these indices also have promising power for predicting OMA, especially NP/AGR having an AUC of 0.799. Therefore, inflammation-nutrition composite indices might serve as adjuncts to miRNAs for the diagnosis of OMA. In the future, based on relevant miRNAs and indices mentioned in our study, we will try to construct a risk nomogram model of women with OMA to better understand their diagnostic value. It is worth noting that, as the previous report revealed,36 let-7b might be a protective factor for endometriosis, which is similar to AGR in our study. On the other hand, increased miRNAs (miR125b, miR150, miR342, and miR451a), similar to inflammation indices, might be dangerous factors for endometriosis. Further studies are needed to explore the relationship between increased miRNAs and inflammation indices as well as the relationship between let-7b and AGR, respectively.
Secondly, it is plausible that inflammation-nutrition indices might serve as potential follow-up markers for let-7b treatment in OMA. For patients who want to conceive and would like to avoid the side effects associated with hormonal therapies, non-hormonal options such as immune-modulating agents, miRNA modulators, anti-IL-6 receptor monoclonal antibody, and stem-cell-based therapies may be available for these patients in the future.3,37
Among them, microRNA let‐7b is one of the popular miRNA modulators. Let-7b has anti-inflammatory effects and has been identified as a novel potential therapeutic target, which was supported by research in murine models of endometriosis.38 It is thought that let‐7b may regulate inflammation through its known target gene TLR4.39 According to a report based on animal experiments,38 a trend towards decreased levels of TLR4 was observed and IL‐6 levels were significantly suppressed in the let‐7b treatment group compared to controls. These results suggested that let‐7b treatment did reduce inflammation associated with endometriosis. Additionally, both TLR4 signaling and IL-6 are correlated with neutrophil activity. TLR4 signaling plays a significant role in the activation and lifespan of neutrophils.40 In addition, a recent study in murine models of endometriosis suggested that IL-6, together with G-CSF, promoted the involvement of neutrophils in the early formation of endometriotic lesions.41 Moreover, IL-6 could affect AGR levels as mentioned previously. As a result, it is plausible that let-7b might influence neutrophils and AGR levels through IL-6, thereby potentially affecting inflammation-nutrition indicators (especially NPAR, NP/AGR) in women with OMA. It remains to be investigated whether inflammation-nutrition indicators might serve as novel follow-up markers for let-7b treatment in women with OMA. Moreover, additional studies are required to determine whether let-7b leads to a reduction in neutrophils during the early stages of OMA through its regulation of TLR4 and IL-6.
Lastly, it is possible that the applications of these indices could be extended to cancer care as well. Evidence suggested that TLR-4 signaling might promote tumor growth in ovarian cancer and TLR-4-MyD88 signaling pathway might be a risk factor for developing cancer.42 In numerous clinical trials, TLR-4 has emerged as a potential target for cancer.43 IL-6 is dysregulated in the cancer microenvironment, where neutrophils and other various inflammatory cells are present.44 In addition, endometriosis and cancer share molecular characteristics because both pathologies include immune evasion, high proliferation and angiogenesis.45 Furthermore, miRNAs-let-7 family are some of the most common miRNAs involved in cell proliferation, invasion and apoptosis.34 Recently, several studies reported that let-7 could be used as a diagnostic or prognostic marker in lung and thyroid cancers.46,47 Let-7b could serve as an adjunctive biomarker for hormone therapy in breast cancer and NSCLC.48 Moreover, let-7b-5p has been identified to have different roles in regulating tumorigenesis and cancer progression.49 As a tumor suppressor, the anti-cancer roles of let-7b-5p were confirmed in several cancers, including human glioma, multiple myeloma, breast and gastric cancers.49 As a tumor-promoting factor, let-7b-5p is overexpressed in ovarian cancer.50 Additionally, a previous study showed that AGR and SII could serve as prognostic markers for women with cancer, and AGR was recommended to predict patient survival for young females.51 For the reasons above, it is possible that further studies in OMA regarding miRNAs-let-7 family and inflammation-nutrition indices might have some contributions toward cancer care.
Limitations of the Study
However, there are still some limitations. First, this is a retrospective observational study. Our findings need to be confirmed with prospective studies. Second, the data of other confounders, such as the menstrual cycle, history of gestation and production, lifestyle, were not included in the analysis because this information is not available. Third, compared with biopsy, ultrasonography diagnosis is a fast, reproducible and invasive method, but it is unable to assess the stage of OMA adequately, including the adhesion between the ovaries and surrounding organs.
Conclusion
This is the first study to combine NLR, PLR, SII, NP with AGR, obtain new inflammation-nutrition composite indices, and use these indices to support the diagnosis of OMA. This study indicated that NPAR, NLR/AGR, PLR/AGR, SII/AGR and NP/AGR could provide additional clinical diagnostic value for OMA as non-invasive and cost-effective tests and are better than inflammation indices (NLR, PLR, SII) alone. Among them, NP/AGR might be the best predictor.
Although our study focused on diagnosis abilities of inflammation-nutrition indices, based on the available literature,33–51 it is reasonable to infer that these indices could potentially be applied to innovative personalized medical care, including adjuncts to miRNAs for the diagnosis of OMA and follow-up markers for let-7b treatment in OMA. And all these inferences require further research, which might have some contributions toward cancer care.
Abbreviations
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index; FBG, fasting blood glucose; TC, total cholesterol; TGs, triglycerides; UA, uric acid; NC, Neutrophil counts; LC, Lymphocytes counts; MC, Monocyte counts; NP, Neutrophil percentage; LP, Lymphocyte percentage; MP, Monocyte percentage; AGR, albumin–globulin ratio; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SII, systemic immune inflammation index; NPAR, neutrophil-percentage-to-albumin ratio.
Data Sharing Statement
Data is available from the corresponding author on reasonable requests.
Ethical Statement
The current retrospective study was approved by the ethical committee of the Affiliated Suzhou Hospital of Nanjing Medical University (ethical approval number: KL901617), which waived consent from study participants as it was not required due to the retrospective nature of the study. All patient data were anonymized during processing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Chantalat E, Valera MC, Vaysse C, et al. Estrogen receptors and endometriosis. Int J Mol Sci. 2020;21(8):2815. doi:10.3390/ijms21082815
2. Saunders PTK, Horne AW. Endometriosis: etiology, pathobiology, and therapeutic prospects. Cell. 2021;184(11):2807–2824. doi:10.1016/j.cell.2021.04.041
3. Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021;397(10276):839–852. doi:10.1016/S0140-6736(21)00389-5
4. Abramiuk M, Grywalska E, Małkowska P, Sierawska O, Hrynkiewicz R, Niedźwiedzka-Rystwej P. The role of the immune system in the development of endometriosis. Cells. 2022;11(13):2028. doi:10.3390/cells11132028
5. Gordts S, Koninckx P, Brosens I. Pathogenesis of deep endometriosis. Fertil Steril. 2017;108(6):872–885.e1. doi:10.1016/j.fertnstert.2017.08.036
6. Audebert A, Petousis S, Margioula-Siarkou C, Ravanos K, Prapas N, Prapas Y. Anatomic distribution of endometriosis: a reappraisal based on series of 1101 patients. Eur J Obstet Gynecol Reprod Biol. 2018;230:36–40. doi:10.1016/j.ejogrb.2018.09.001
7. Wang L, Liu L, Liu X, Yang L. The association between neutrophil percentage-to-albumin ratio (NPAR) and depression among US adults: a cross-sectional study. Sci Rep. 2024;14(1):21880. doi:10.1038/s41598-024-71488-y
8. Mandaliya H, Jones M, Oldmeadow C, Nordman II. Prognostic biomarkers in stage IV non-small cell lung cancer (NSCLC): neutrophil to lymphocyte ratio (NLR), lymphocyte to monocyte ratio (LMR), platelet to lymphocyte ratio (PLR) and advanced lung cancer inflammation index (ALI). Transl Lung Cancer Res. 2019;8(6):886–894. doi:10.21037/tlcr.2019.11.16
9. Wang N, Ren L, Li Z, et al. The association between SII and aging: evidence from NHANES 1999-2018. Front Public Health. 2024;12. 1418385. doi:10.3389/fpubh.2024.1418385
10. Gorun OM, Ratiu A, Citu C, et al. The role of inflammatory markers NLR and PLR in predicting pelvic pain in endometriosis. J Clin Med. 2024;14(1):149. doi:10.3390/jcm14010149
11. Tabatabaei F, Tahernia H, Ghaedi A, Bazrgar A, Khanzadeh S. Diagnostic significance of neutrophil to lymphocyte ratio in endometriosis: a systematic review and meta-analysis. BMC Womens Health. 2023;23(1):576. doi:10.1186/s12905-023-02692-7
12. Dominoni M, Pasquali MF, Musacchi V, et al. Neutrophil to lymphocytes ratio in deep infiltrating endometriosis as a new toll for clinical management. Sci Rep. 2024;14(1):7575. doi:10.1038/s41598-024-58115-6
13. Kokot I, Piwowar A, Jędryka M, Sołkiewicz K, Kratz EM. Diagnostic significance of selected serum inflammatory markers in women with advanced endometriosis. Int J Mol Sci. 2021;22(5):2295. doi:10.3390/ijms22052295
14. Mu F, Harris HR, Rich-Edwards JW, et al. A prospective study of inflammatory markers and risk of endometriosis. Am J Epidemiol. 2018;187(3):515–522. doi:10.1093/aje/kwx272
15. Peng L, Luo X, Cao B, Wang X. Exploring the link: systemic immune-inflammation index as a marker in endometriosis-insights from the NHANES 2001-2006 cross-sectional study. PLoS One. 2024;19(6):e0304591. doi:10.1371/journal.pone.0304591
16. Sheinenzon A, Shehadeh M, Michelis R, Shaoul E, Ronen O. Serum albumin levels and inflammation. Int J Biol Macromol. 2021;184:857–862. doi:10.1016/j.ijbiomac.2021.06.140
17. Chen Z, Song C, Yao Z, Sun J, Liu W. Associations between albumin, globulin, albumin to globulin ratio and muscle mass in adults: results from the national health and nutrition examination survey 2011-2014. BMC Geriatr. 2022;22(1):383. doi:10.1186/s12877-022-03094-4
18. Wu PP, Hsieh YP, Kor CT, Chiu PF. Association between albumin-globulin ratio and mortality in patients with chronic kidney disease. J Clin Med. 2019;8(11):1991. doi:10.3390/jcm8111991
19. Andreotti RF, Timmerman D, Strachowski LM, et al. O-RADS US risk stratification and management system: a consensus guideline from the ACR ovarian-adnexal reporting and data system committee. Radiology. 2020;294(1):168–185. doi:10.1148/radiol.2019191150
20. Takamura M, Koga K, Izumi G, et al. Neutrophil depletion reduces endometriotic lesion formation in mice. Am J Reprod Immunol. 2016;76(3):193–198. doi:10.1111/aji.12540
21. Vallvé-Juanico J, Houshdaran S, Giudice LC. The endometrial immune environment of women with endometriosis. Hum Reprod Update. 2019;25(5):564–591. doi:10.1093/humupd/dmz018
22. Agostinis C, Balduit A, Mangogna A, et al. Immunological basis of the endometriosis: the complement system as a potential therapeutic target. Front Immunol. 2021;11. 599117. doi:10.3389/fimmu.2020.599117
23. Cho S, Cho H, Nam A, et al. Neutrophil-to-lymphocyte ratio as an adjunct to CA-125 for the diagnosis of endometriosis. Fertil Steril. 2008;90(6):2073–2079. doi:10.1016/j.fertnstert.2008.03.061
24. Ottolina J, Bartiromo L, Dolci C, et al. Assessment of coagulation parameters in women affected by endometriosis: validation study and systematic review of the literature. Diagnostics. 2020;10(8):567. doi:10.3390/diagnostics10080567
25. Petäjä J. Inflammation and coagulation. An overview. Thromb Res. 2011;127 Suppl 2:S34–7. doi:10.1016/S0049-3848(10)70153-5
26. Sreeramkumar V, Adrover JM, Ballesteros I, et al. Neutrophils scan for activated platelets to initiate inflammation. Science. 2014;346(6214):1234–1238. doi:10.1126/science.1256478
27. Ding D, Liu X, Duan J, Guo SW. Platelets are an unindicted culprit in the development of endometriosis: clinical and experimental evidence. Hum Reprod. 2015;30(4):812–832. doi:10.1093/humrep/dev025
28. Li MM, Tang XH, Wang LM. Study on the predictive significance of PLR, SII and RPR in ovarian endometriotic cyst. Zhonghua Fu Chan Ke Za Zhi. 2023;58(9):672–679. Chinese. doi:10.3760/cma.j.cn112141-20230504-00200
29. Zhou Y, Liu G, Yuan L, Qiao Y, Chen Q. Evaluating systemic immune-inflammation indices as predictive markers for endometriosis diagnosis: a retrospective observational study. J Reprod Immunol. 2025;167:104416. doi:10.1016/j.jri.2024.104416
30. Moshage HJ, Janssen JA, Franssen JH, Hafkenscheid JC, Yap SH. Study of the molecular mechanism of decreased liver synthesis of albumin in inflammation. J Clin Invest. 1987;79(6):1635–1641. doi:10.1172/JCI113000
31. Choe H, Kamono E, Abe K, et al. Accuracy of albumin, globulin, and albumin-globulin ratio for diagnosing periprosthetic joint infection: a systematic review and meta-analysis. J Clin Med. 2023;12(24):7512. doi:10.3390/jcm12247512
32. Xu H, Zhao J, Lu J, Sun X. Ovarian endometrioma infiltrating neutrophils orchestrate immunosuppressive microenvironment. J Ovarian Res. 2020;13(1):44. doi:10.1186/s13048-020-00642-7
33. Cho S, Mutlu L, Grechukhina O, Taylor HS. Circulating microRNAs as potential biomarkers for endometriosis. Fertil Steril. 2015;103(5):1252–60.e1. doi:10.1016/j.fertnstert.2015.02.013
34. Pant A, Moar K, Arora TK, et al. Deciphering the role of circulating miRNAs in the etiology and pathophysiology of endometriosis: an updated compiled review. Exp Cell Res. 2025;446(2):114482. DOI:10.1016/j.yexcr.2025.114482
35. Nematian SE, Mamillapalli R, Kadakia TS, Majidi Zolbin M, Moustafa S, Taylor HS. Systemic inflammation induced by microRNAs: endometriosis-derived alterations in circulating microRNA 125b-5p and Let-7b-5p regulate macrophage cytokine production. J Clin Endocrinol Metab. 2018;103(1):64–74. doi:10.1210/jc.2017-01199
36. Moustafa S, Burn M, Mamillapalli R, Nematian S, Flores V, Taylor HS. Accurate diagnosis of endometriosis using serum microRNAs. Am J Obstet Gynecol. 2020;223(4):
37. El-Zayadi AA, Mohamed SA, Arafa M, et al. Anti-IL-6 receptor monoclonal antibody as a new treatment of endometriosis. Immunol Res. 2020;68(6):389–397. doi:10.1007/s12026-020-09153-5
38. Sahin C, Mamillapalli R, Yi KW, Taylor HS. microRNA Let-7b: a novel treatment for endometriosis. J Cell Mol Med. 2018;22(11):5346–5353. doi:10.1111/jcmm.13807
39. Bao MH, Feng X, Zhang YW, Lou XY, Cheng Y, Zhou HH. Let-7 in cardiovascular diseases, heart development and cardiovascular differentiation from stem cells. Int J Mol Sci. 2013;14(11):23086–23102. doi:10.3390/ijms141123086
40. Mattke J, Darden CM, Lawrence MC, et al. Toll-like receptor 4 in pancreatic damage and immune infiltration in acute pancreatitis. Front Immunol. 2024;15:1362727. doi:10.3389/fimmu.2024.1362727
41. Guo F, He Y, Fan Y, et al. G-CSF and IL-6 may be involved in formation of endometriosis lesions by increasing the expression of angiogenic factors in neutrophils. Mol Hum Reprod. 2021;27(11):gaab064. doi:10.1093/molehr/gaab064
42. Kelly MG, Alvero AB, Chen R, et al. TLR-4 signaling promotes tumor growth and paclitaxel chemoresistance in ovarian cancer. Cancer Res. 2006;66(7):3859–3868. DOI:10.1158/0008-5472.CAN-05-3948
43. Litak J, Grochowski C, Litak J, et al. TLR-4 signaling vs. immune checkpoints, miRNAs molecules, cancer stem cells, and wingless-signaling interplay in glioblastoma multiforme-future perspectives. Int J Mol Sci. 2020;21(9):3114. doi:10.3390/ijms21093114
44. Khandia R, Munjal A. Interplay between inflammation and cancer. Advances in Protein Chemistry and Structural Biology. 2019;199–245. doi:10.1016/bs.apcsb.2019.09.004
45. Pollacco J, Sacco K, Portelli M, Schembri-Wismayer P, Calleja-Agius J. Molecular links between endometriosis and cancer. Gynecol Endocrinol. 2012;28(8):577–581. doi:10.3109/09513590.2011.650761
46. Mahmoudian-Sani MR, Mehri-Ghahfarrokhi A, Asadi-Samani M, Mobini GR. Serum miRNAs as biomarkers for the diagnosis and prognosis of thyroid cancer: a comprehensive review of the literature. Eur Thyroid J. 2017;6(4):171–177. doi:10.1159/000468520
47. Wang S, Wang Z, Wang Q, Cui Y, Luo S. Clinical significance of the expression of miRNA-21, miRNA-31 and miRNA-let7 in patients with lung cancer. Saudi. J Biol Sci. 2019;26(4):777–781. doi:10.1016/j.sjbs.2018.12.009
48. Asavasupreechar T, Saito-Koyama R, Miki Y, et al. PRB inhibited cell proliferation through let-7b-E2F1 in breast cancer. Endocr Relat Cancer. 2023;30(7):e220204. DOI:10.1530/ERC-22-0204
49. Li L, Zhang X, Lin Y, et al. Let-7b-5p inhibits breast cancer cell growth and metastasis via repression of hexokinase 2-mediated aerobic glycolysis. Cell Death Discov. 2023;9(1):114. doi:10.1038/s41420-023-01412-2
50. Huang X, Dong H, Liu Y, et al. Silencing of let-7b-5p inhibits ovarian cancer cell proliferation and stemness characteristics by Asp-Glu-Ala-Asp-box helicase 19A. Bioengineered. 2021;12(1):7666–7677. doi:10.1080/21655979.2021.1982276
51. Yang M, Zhang Q, Ge Y, et al. Prognostic roles of inflammation- and nutrition-based indicators for female patients with cancer. J Inflamm Res. 2022;15:3573–3586. doi:10.2147/JIR.S361300
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association and Comparison of Systemic Inflammation Indicators and Myocardial Injury After Noncardiac Surgery in Older Patients
Meng B, Zhang K, Liu C, Yao S, Li Z, Lou J, Fu Q, Liu Y, Cao J, Mi W, Li H
Journal of Inflammation Research 2025, 18:3499-3510
Published Date: 10 March 2025