Back to Journals » OncoTargets and Therapy » Volume 11
Relationship between HER2 gene status and selected potential biological features related to trastuzumab resistance and its influence on survival of breast cancer patients undergoing trastuzumab adjuvant treatment
Authors Adamczyk A ![]() , Kruczak A, Harazin-Lechowska A, Ambicka A, Grela-Wojewoda A, Domagała-Haduch M, Janecka-Widła A
, Kruczak A, Harazin-Lechowska A, Ambicka A, Grela-Wojewoda A, Domagała-Haduch M, Janecka-Widła A ![]() , Majchrzyk K
, Majchrzyk K ![]() , Cichocka A, Ryś J, Niemiec J
, Cichocka A, Ryś J, Niemiec J
Received 1 March 2018
Accepted for publication 25 April 2018
Published 3 August 2018 Volume 2018:11 Pages 4525—4535
DOI https://doi.org/10.2147/OTT.S166983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Carlos E Vigil
Agnieszka Adamczyk,1 Anna Kruczak,1 Agnieszka Harazin-Lechowska,1 Aleksandra Ambicka,1 Aleksandra Grela-Wojewoda,2 Małgorzata Domagała-Haduch,2 Anna Janecka-Widła,1 Kaja Majchrzyk,1 Anna Cichocka,1 Janusz Ryś,1 Joanna Niemiec1
1Department of Tumour Pathology, 2Department of Systemic and Generalized Malignancies, Maria Sklodowska-Curie Memorial Cancer Centre and Institute of Oncology, Cracow Branch, Cracow, Poland
Background: The aim of the study was to investigate if parameters associated with human epidermal growth factor receptor type 2 (HER2) status (HER2 gene copy number, HER2/CEP17 ratio or polysomy of chromosome 17) are related to various biological features potentially responsible for trastuzumab resistance (PTEN, IGF-1R, MUC4, EGFR, HER3, HER4, and mutation status of PIK3CA) as well as their influence on survival of HER2-positive breast cancer patients treated with adjuvant chemotherapy and trastuzumab.
Patients and methods: The investigated group consisted of 117 patients with invasive ductal breast cancer (T≥1, N≥0, M0) with overexpression of HER2, who underwent radical surgery between 2007 and 2014. Status of ER, PR, and HER2 expression was retrieved from patients’ files. HER2 gene copy number was investigated by fluorescence in situ hybridization using PathVysion HER-2 DNA Probe Kit II. Expression of PTEN, IGF-1R, MUC4, EGFR, HER3, and HER4 was assessed immunohistochemically on formalin-fixed paraffin-embedded tissue sections. PIK3CA mutation status was determined by qPCR analysis.
Results: Overexpression of HER2 protein (IHC 3+) and ER negativity corresponded to higher HER2 copy number and HER2/CEP17 ratio (p<0.001). Tumors with polysomy were characterized by higher HER2 gene copy number but lower HER2/CEP17 ratio (p<0.026, p<0.001). Patients with tumors featuring HER3 immunonegativity or low HER2/CEP17 ratio (≤4) were characterized by 100% metastasis-free survival (p=0.018, p=0.062).
Conclusion: Presence of both unfavorable factors, ie, HER3 expression and high HER2/CEP17 ratio, allowed to distinguish a group of patients with worse prognosis (p=0.001).
Keywords: HER2-overexpressing breast cancer, HER2 amplification, HER2 gene copy number, HER2/CEP17 ratio, HER3 expression, trastuzumab
Introduction
Overexpression of human epidermal growth factor receptor type 2 (HER2) is observed in about 20%–25% of invasive breast cancer cases.1 HER2 is one of the most important oncogenes in breast cancer and plays an important role in the following cellular processes: proliferation, invasion, metastases, and enhanced survival of cancer cells.2 To block the activity of HER2, trastuzumab, which is a humanized monoclonal antibody against the IV domain of extracellular fragment of HER2, is currently implemented in treatment schedules applied for breast cancer. The inclusion of trastuzumab in the treatment regimen is determined by strong expression of HER2 protein or HER2 gene amplification defined according to the guidelines proposed by the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) from 2013.3 The immunohistochemistry (IHC) scoring system classifies HER2 expression status as positive (3+) if circumferential membrane staining is complete and intense in >10% of tumor cells. In the case of dual probe fluorescence in situ hybridization (FISH) technique, positive cases are defined as follows: HER2/CEP17 ratio ≥2.0 or when HER2/CEP17 ratio is <2.0 but mean HER2 copy number is ≥6.0 signals/cell.
The fact that after monotherapy with trastuzumab in patients with metastatic breast cancer objective response rate was 15%–26% suggests the presence of mechanisms determining trastuzumab resistance.4,5 Potentially, resistance to trastuzumab treatment could be caused by several events including 1) overexpression of MUC4 protein (that masks epitopes recognized by trastuzumab), 2) activation of HER2 signaling cascades: heterodimerization of HER2 with HER3, HER4, EGFR, activating mutations of PIK3CA (phosphatidylinositol 4,5-bisphosphate 3-kinase catalytic subunit), downregulation of PTEN protein expression.2,6,7 The influence of these potential factors on HER2-positive breast cancer patients survival is currently widely studied.
The status of HER2 was also investigated regarding its influence on breast cancer patients’ survival. It appears that in neoadjuvant setting and in the case of metastatic cancer higher level of HER2 amplification is related to higher rate of response to trastuzumab or longer survival.8–13 However, the role of HER2 amplification in adjuvant setting is controversial.8,14–18
Therefore, the aim of our study was to analyze the relationship between HER2 status (HER2/CEP17 ratio, gene copy number, and polysomy of chromosome 17) and potential factors related to trastuzumab resistance (PTEN, IGF-1Rβ, MUC4, HER3, HER4, EGFR expression, PIK3CA mutations) as well as its prognostic value for metastasis-free survival of HER2-positive breast cancer patients treated with trastuzumab in adjuvant setting. Studies investigating the abovementioned biological parameters and their relationship in a group of breast cancer patients treated with trastuzumab in adjuvant setting are sparse. Moreover, we investigated numerous parameters related to different mechanisms of trastuzumab resistance, and thus, the results of our study might be of interest to oncologists and pathologists.
Patients and methods
Patients
The investigated group consisted of 117 patients with invasive ductal breast cancer (T≥1, N≥0, M0) with overexpression of HER2, who underwent radical surgery between 2007 and 2014 at the Department of Surgical Oncology, Maria Sklodowska-Curie Memorial Cancer Centre and Institute of Oncology, Cracow Branch. The patients received neither neoadjuvant chemotherapy nor radiotherapy. After surgery, trastuzumab in adjuvant setting was applied as well as chemotherapy and radiotherapy in selected cases. Patients with tumors presenting estrogen/progesterone receptor (ER/PR) expression additionally received hormonotherapy. Data concerning clinical and histological parameters are presented in Table 1. The mean age of patients was 53.4 ± 0.9 years (mean ± standard errors of mean [SEM]), median was 56 years and range was from 31 to 79 years. The study received approval from the Ethical Committee at the Regional Medical Chamber in Cracow (decision from 4th December 2013). This was a retrospective study utilizing archived tissues, with no direct patient contact, no modification of diagnostic or treatment procedures, and no personal patients’ data revealed; in this case, no specific patient consent was needed.
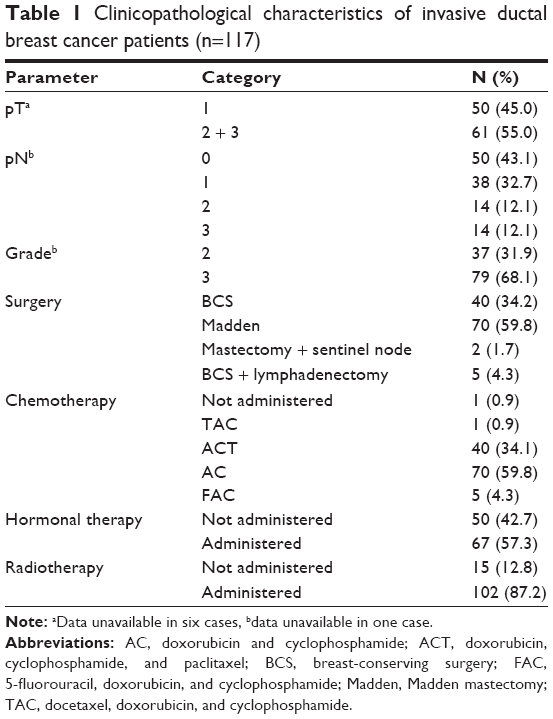 | Table 1 Clinicopathological characteristics of invasive ductal breast cancer patients (n=117) |
Material
The study was performed on archival formalin-fixed paraffin-embedded (FFPE) tissues. Tumor specimens were reexamined independently by two pathologists (A.H-L., A.A.) to confirm histological diagnosis and tumor grade as well as to assess tissue amount and quality needed for this study.
HER2 FISH testing
In the assessment of HER2 status, immunohistochemistry (IHC) was applied and followed by FISH in selected cases, ie, if the results of IHC were equivocal (the expression assessed as 2+) (Figure 1A). In the investigated group, we additionally assessed status of HER2 gene in cases with 3+ IHC score, which constituted most of the patients (77.4%) (Figure 1B). HER2 gene copy number was investigated by FISH using PathVysion HER-2 DNA Probe Kit II (Vysis, Abbott Laboratories) according to manufacturer’s protocol. The PathVysion HER-2 DNA Probe Kit consists of two labeled DNA probes. The LSI HER-2/neu probe that spans the HER2 gene (17q11.2-12) is labeled in SpectrumOrange, while the CEP17 probe that is labeled in SpectrumGreen hybridizes to the alpha satellite DNA located at the centromere of chromosome 17 (17p11.1–q11.1). Inclusion of the CEP17 probe allows detection of the relative copy number of HER2 gene.
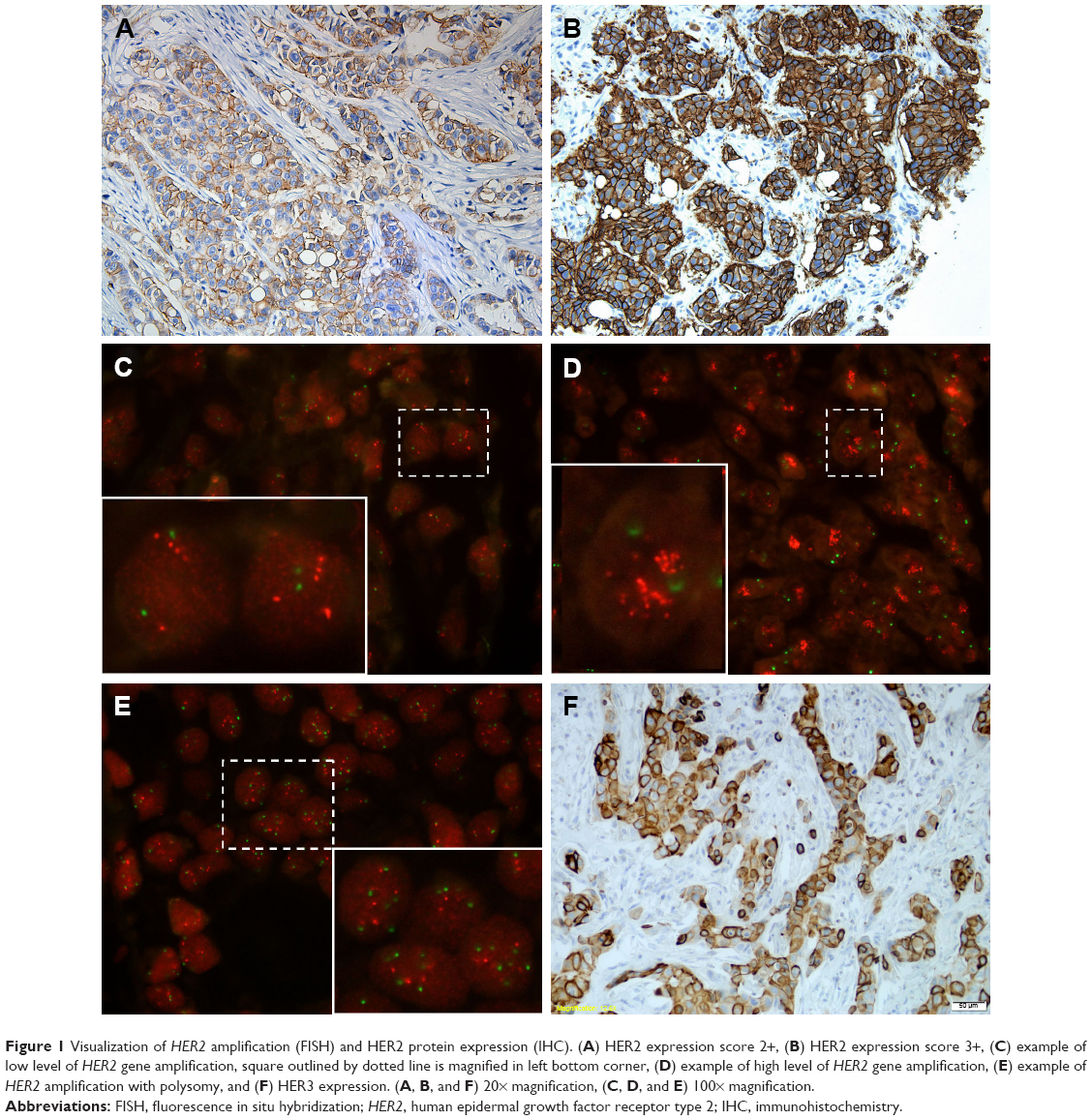 | Figure 1 Visualization of HER2 amplification (FISH) and HER2 protein expression (IHC). (A) HER2 expression score 2+, (B) HER2 expression score 3+, (C) example of low level of HER2 gene amplification, square outlined by dotted line is magnified in left bottom corner, (D) example of high level of HER2 gene amplification, (E) example of HER2 amplification with polysomy, and (F) HER3 expression. (A, B, and F) 20× magnification, (C, D, and E) 100× magnification. |
FISH signals were assessed with an Olympus fluorescence microscope BX41 by two independent investigators. Using 100× objective lens, 20–40 interphase tumor nuclei were examined for each specimen, and the numbers of fluorescent signals within tumor cells from HER2 gene and chromosome 17 centromere were recorded.
The slides were evaluated according to ASCO/CAP 2013 recommendations.3 The status of HER2 gene was defined as follows: 1) amplification of HER2 gene was defined as HER2/CEP17 ratio ≥2 (Figure 1C and D) or HER2 gene copy number ≥6 signals per cell and 2) polysomy was defined as average number of signals from centromere of chromosome 17 per cell ≥3 (Figure 1E).
IHC
Status of ER, PR, and HER2 expression was retrieved from patients’ files (diagnostic procedures). HER2 overexpression was assessed using HercepTest (Dako Agilent Pathology Solutions) according to recommended manufacturer’s procedure.
Presence of >1% of tumor cells expressing ER or PR (nuclear) and EGFR (membranous) classified tumor as immunopositive. Expression of PTEN, IGF-1R, MUC4, EGFR, HER3 (Figure 1F), and HER4 was assessed immunohistochemically. Table 2 contains details of IHC procedures. BrightVision detection system (Immunologic, Duiven, The Netherlands) and DAB (Vector Laboratories, Inc., Burlingame, CA, USA) were used for visualization.
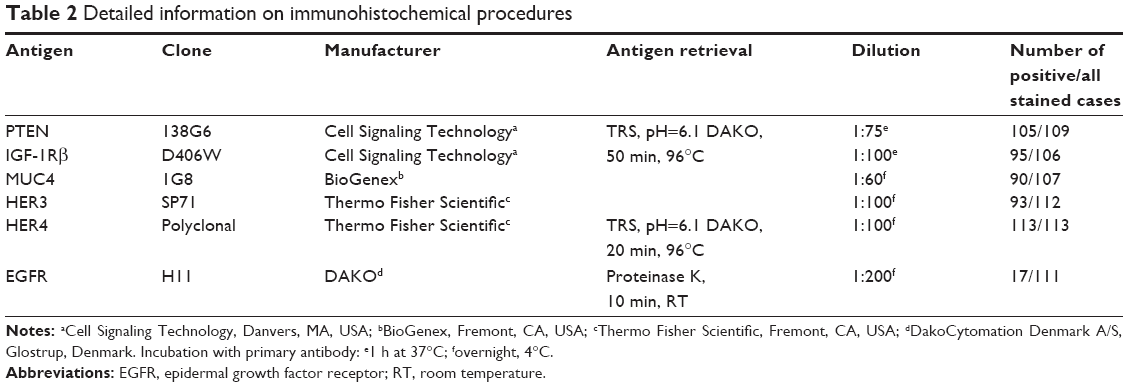 | Table 2 Detailed information on immunohistochemical procedures |
Expression of investigated proteins was evaluated only in the invasive component of the tumors. Cytoplasmic expression of HER3, HER4, IGF-1R, MUC4, and PTEN was estimated using histological score (H-score) calculated as:
H-score = (1 × percentage of weakly positive cells) + (2 × percentage of moderately strong positive cells) + (3 × percentage of strongly positive cells).
The whole panel of IHC results was not available for all cases due to insufficient amount of tissue in paraffin blocks or small fragments of tumor tissue, which hindered obtaining reliable results (Table 2).
qPCR analysis of PIK3CA mutation status
Details concerning DNA isolation and PCR procedure were described elsewhere.19 DNA was isolated from FFPE tumor tissue blocks using ReliaPrep FFPE gDNA Miniprep System from Promega Corp. qPCR reactions were performed to identify presence of H1047R and E545K PIK3CA mutations using assays manufactured by Thermo Fisher Scientific on ViiA 7 Real-Time PCR System (Thermo Fisher Scientific). Received data were analyzed using Mutation Detector Software.
Statistical analysis
For continuous variables, descriptive statistics were used to determine mean values and SE. Kruskal–Wallis ANOVA test with Bonferroni correction was applied for testing differences between groups. Relationships between categorical variables were analyzed using Yates test for 2×2 tables or Pearson χ2 (for variables with >2 categories). Pearson product-moment correlation coefficient was estimated to test correlation between continuous variables.
Metastasis-free survival was estimated as time from surgery to clinically or radiologically confirmed metastases. The probability of survival was estimated using the Kaplan–Meier method. The log-rank test was used to investigate the statistical significance of the differences observed between two groups and to establish the cutoff point for HER3, IGF-1R, MUC4, HER4, and PTEN expression (the minimal p-value method). Only for HER3 expression, there was a clearly statistically significant cutoff point. p<0.05 was considered significant in all statistical procedures. The statistical analysis was carried out using STATISTICA 12 software (StatSoft, Inc., Tulsa, OK, USA).
Results
Relations between status of HER2 and clinical and biological parameters
In the examined group, 29 tumors presented expression of HER2 protein (based on IHC) classified as 2+, while 86 classified as 3+. FISH confirmed amplification of HER2 gene in 115 cases; however, in 2 cases with IHC assessed as 3+ we did not observe HER2 gene amplification. Mean CEP17 probe signal per cell was 2.8 ± 0.1 (mean ± SE) (range 1–8.2), HER2 copy number was 16.6 ± 0.8 (range 1.6–38.4), and HER2/CEP17 ratio was 6.7 ± 0.4 (range 1.2–17.5). Higher level of HER2 protein (IHC 3+) corresponded to higher HER2 copy number per cell and HER2/CEP17 ratio (Table 3). Steroid receptor-positive tumors presented lower HER2 copy number per cell and HER2/CEP17 ratio (Table 3). Other parameters including pT, pN, grade, mutations in PIK3CA gene, and EGFR expression were not associated with any parameters investigated by FISH technique (Table 3). In the case of other proteins, the following correlations were found: positive correlation between HER2 gene copy number and HER4 expression (r=0.201, p=0.033) and negative correlations between: 1) HER2 gene copy number and HER3 as well as IGF-1R expression (r=−0.278, p=0.003; r=−0.314, p=0.001, respectively) and 2) HER2/CEP17 ratio and IGF-1R (r=−0.227, p=0.019). MUC4 expression correlated with neither HER2 gene copy number nor HER2/CEP17 ratio.
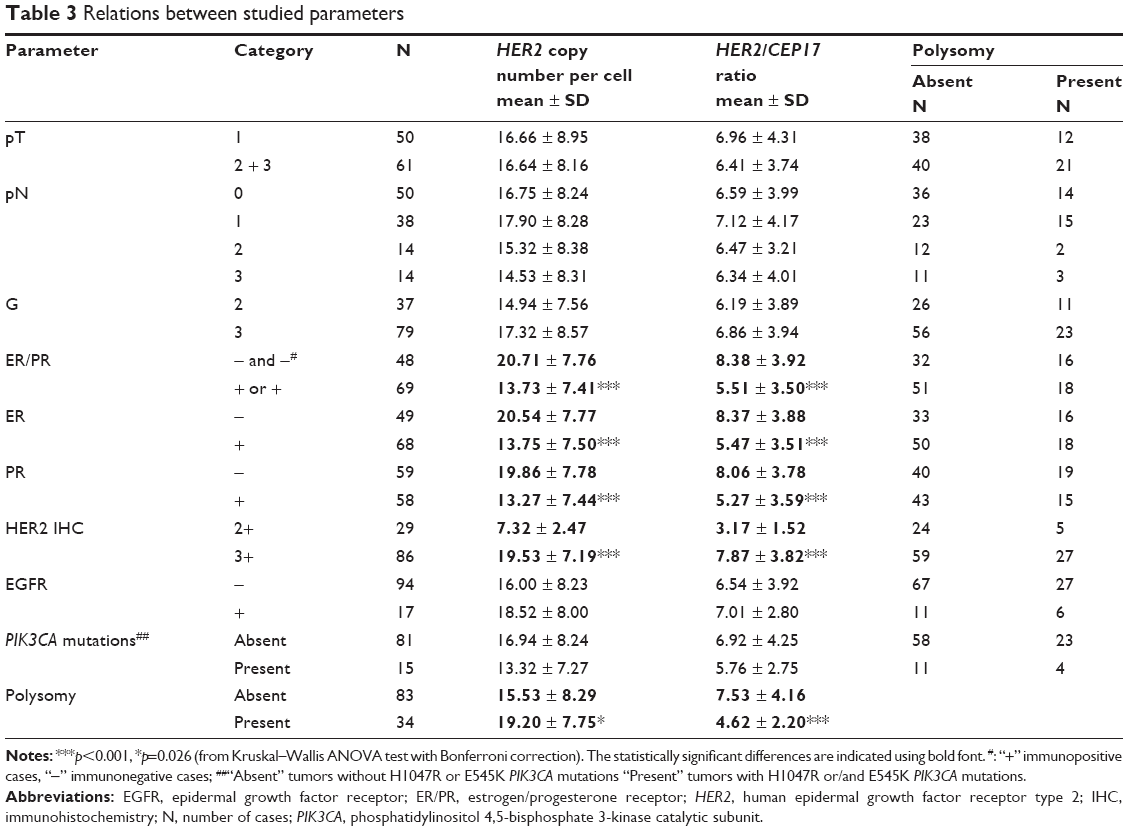 | Table 3 Relations between studied parameters |
We observed that tumors with polysomy were characterized by higher number of HER2 gene copy number per cell but lower HER2/CEP17 ratio (Table 3). Expression of HER3, IGF-1R, MUC4, HER4, and PTEN did not differ between groups of tumors with and without polysomy of chromosome 17.
Survival analysis
Survival analysis was carried out in a group of 117 patients, and the mean time of follow-up was 54.8 months (range 17.0–98.6 months, median 50.5 months).
Favorable metastasis-free survival was observed in patients with pN0+pN1 (vs pN2+pN3) pathological stage (Table 4) and in carcinomas with HER3 immunonegativity (Table 4, Figure 2A). Among parameters related to HER2 status, HER2/CEP17 ratio was the only factor with cutoff point (≤4) on the border of statistical significance (Table 4, Figure 2B). However, it is worth mentioning that patients with tumors featuring HER3 immunonegativity or low HER2/CEP17 ratio (≤4) were characterized by 100% metastasis-free survival. We also studied cumulative effect of HER3 expression and HER2/CEP17 ratio to determine if creating a group with two potentially negative factors can improve statistical significance. Patients with tumors presenting both strong HER3 positivity and high HER2/CEP17 ratio were characterized by a very high statistically significant poorer prognosis (p=0.001) (Table 4, Figure 2C).
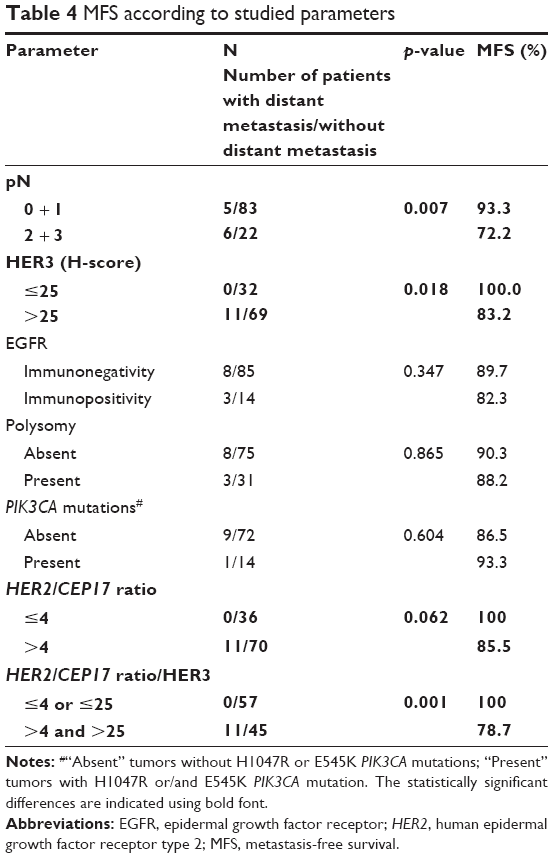 | Table 4 MFS according to studied parameters |
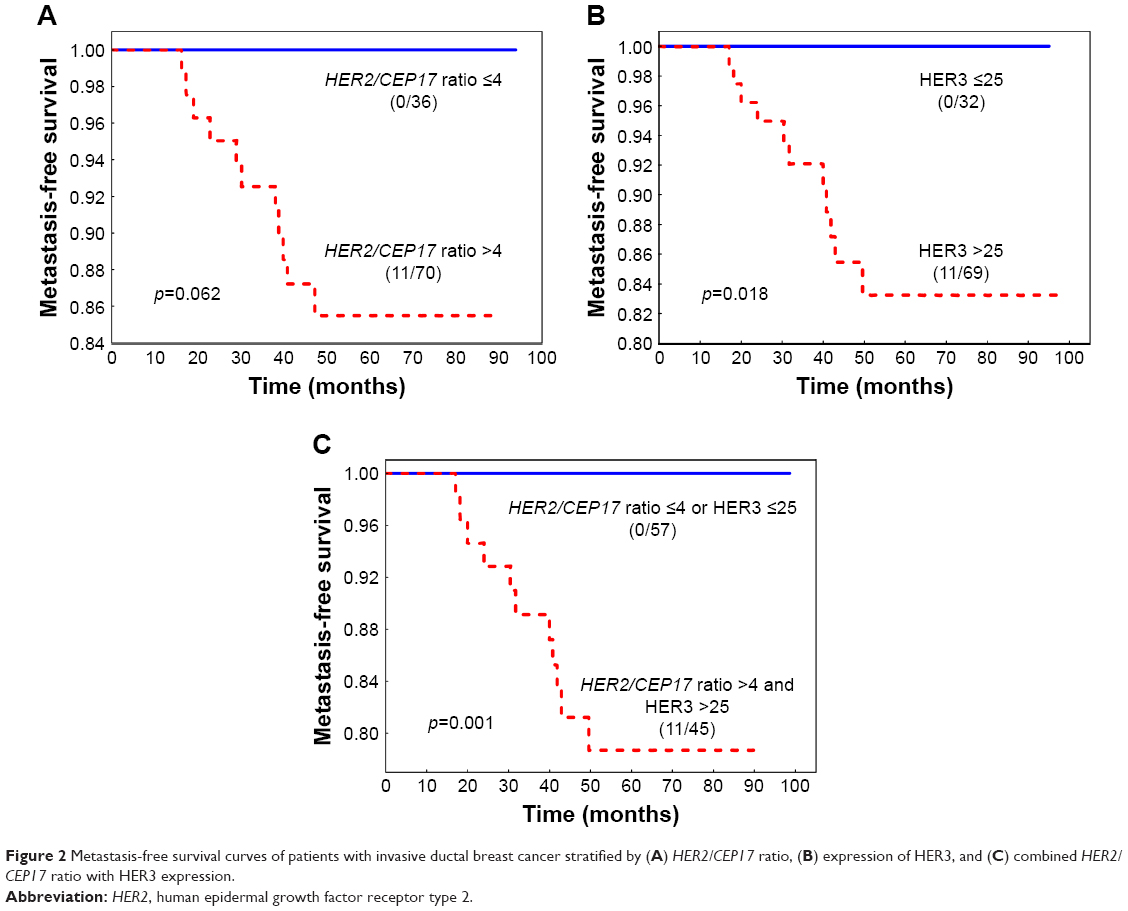 | Figure 2 Metastasis-free survival curves of patients with invasive ductal breast cancer stratified by (A) HER2/CEP17 ratio, (B) expression of HER3, and (C) combined HER2/CEP17 ratio with HER3 expression. |
Discussion
The studied group consisted of patients with HER2 IHC score 3+ and those with IHC score 2+ with confirmed HER2 amplification who received trastuzumab according to ASCO/CAP 2007 recommendations.20 At the end of 2013, the new ASCO/CAP recommendations were provided. These recommendations were less discriminating, and that is why some carcinomas previously classified as negative would be considered positive according to the new classification.21,22 Therefore, even if 2013 recommendations were applied in our group, all patients would still be considered as HER2 positive.
In the investigated group, we discovered two cases with HER2 overexpression (3+) but without HER2 amplification. The correlation between IHC and FISH results is well known, although there are some discordant cases. A study on 6,556 breast cancer tissue specimens showed that in the group of 707 patients with IHC scored as 3+, amplification was confirmed in 91.7% of cases.23 It is suggested that in IHC 3+/FISH− cases, discordance can be explained, at least partially, by polysomy24 or epigenetic/posttranscriptional events as suggested by Tsuda et al.25 It is worth mentioning that in our study one of the two IHC 3+/FISH− tumors was polysomic. On the other hand, in the case of tumors without HER2 expression but with HER2 amplification, this variance could be due to incomplete amplification of the smallest HER2 region of chromosome 17q11-12.26
In our study, we observed that tumors with polysomy were characterized by higher number of HER2 gene copy number per cell but lower HER2/CEP17 ratio. Probably in tumors without polysomy the increase of HER2 gene copies is caused only by amplification of HER2 gene on chromosome 17, while in tumors with polysomy (according to our observations) higher number of HER2 gene copy is caused mostly by polysomy of chromosome 17.
In the investigated group, HER2/CEP17 ratio values varied from 1.2 to 17.5 and HER2 copy number varied from 1.6 to 38.4, which is in the range reported by other authors.14,15
Data concerning relation between HER2/CEP17 ratio and HER2 copy number with clinical and biological features are sparse. To the best of our knowledge, our study is the first one to investigate relation between parameters associated with HER2 status (HER2 gene copy number, HER2/CEP17 ratio, and polysomy) and potential biological features related to trastuzumab resistance (expression of PTEN, IGF-1R, MUC4, EGFR, HER3, HER4, and mutation status of PIK3CA). For most of these factors, we did not note any relationships. However, similarly to other authors, we observed higher HER2/CEP17 ratio and HER2 copy number in ER-negative tumors.12,27,28 This relation was discovered not only if variables were dichotomous (the group divided to: ER-positive or ER-negative cases as well as HER2-overexpressing or non-HER2-overexpressing cases) but also then analyzed as continuous variables (ER and HER2 measured as quantitative value).28 Konecny et al assessed HER2/neu protein levels by ELISA and ER/PR (hormone receptor [HR]) expression by enzyme immunoassay in one cohort, while in the second cohort HER2/neu gene copy number was assessed by FISH and ER/PR expression by radioligand binding. They noted that not only levels of HER2 overexpression/gene amplification were negatively correlated with ER/PR levels, but even more importantly HR-positive/HER2-positive tumors had statistically significantly lower ER/PR levels than HR+/HER2-negative cases.28 This negative relation can be explained by the fact that HER2 overexpression can induce transcriptional repression of ER gene. Pietras et al demonstrated that HER2 overexpression in ER-dependent tumor cells promote ligand-independent downregulation of ER and a delayed autoregulatory suppression of ER transcripts.29 Moreover, Konecny et al showed that transfection of HR-positive human breast cancer cell lines with HER2 gene resulted in statistically significantly lower levels of ER and PR expression than in parental lines.28
Similarly to Varga et al, we did not observe any relationship between HER2/CEP17 ratio or HER2 copy number and tumor stage (pT) or nodal status.30 However, contrary to us, they found correlation between the abovementioned parameters and histological grade,30 which can be caused by differences in clinical characteristics of analyzed groups.
We also observed higher HER2 copy number in tumors with HER2 expression estimated by IHC as 3+. Positive relation between HER2 overexpression (IHC) and HER2 amplification (FISH) is well known and confirmed in large studies involving up to several thousand patients.23,31 Moreover, the level of HER2 mRNA (assessed by RT-PCR) was positively correlated with HER2 amplification (FISH)32 and HER2 expression,32,33 what translates into a straightforward pathway: more gene copy number, more mRNA transcripts and, in the end, higher level of protein expressed.
We did not observe relation between parameters associated with HER2 status (ie, HER2 gene copy number, HER2/CEP17 ratio or polysomy of chromosome 17) and PIK3CA mutation. It is confirmed by other authors who reported that mutations of PIK3CA gene were found in both HER2-negative and HER2-positive components.34 Janiszewska et al, who investigated co-occurrence of PIK3CA mutation and HER2 amplification, observed that most cells with His1047Arg mutation of PIK3CA did not contain amplified HER2 gene and suggested that these two alterations are independent genetic events.35
We also investigated if magnitude of HER2 amplification is related to patients’ survival after treatment with trastuzumab. According to HERA trial, adding trastuzumab to treatment schedule improves 10-year disease-free survival in the group of HER2-positive early breast cancer patients.36 Positivity of HER2 was defined as IHC score 3+ or HER2/CEP17 ratio ≥2 for tumors with IHC score 2+.14 FISH performed retrospectively for 3+ samples revealed a subgroup of 41 tumors with HER2/CEP17 ratio <2; however, due to small number of cases evaluation of possible benefit from trastuzumab treatment in this subgroup was not performed.14 In N9831 adjuvant trastuzumab trial, benefit from trastuzumab was observed in patients with IHC score 3+, with HER2/CEP17 ratio ≥2 and if those two parameters were simultaneously present. For patients with tumors characterized by IHC 0–2+ or HER2/CEP17 ratio <2, higher disease-free survival probability was observed but was not statistically significant.17 The relationship between HER2 status and HER2-positive breast cancer patients’ survival after trastuzumab therapy is still under investigation, and it is difficult to draw clear conclusions. One of the problems is the variety of treatment schedules (neoadjuvant/adjuvant) and of breast cancer stage (early/metastatic). It appears that in neoadjuvant setting HER2 amplification is positively correlated with more frequent pathological response to trastuzumab treatment,10,37 but not necessarily to higher survival rate.37 In case of metastatic breast cancer, most of the studies noted relationship between higher values of HER2/CEP17 ratio and longer time to progression9,11,12 or overall survival9 or higher probability of an objective response.13 However, Gullo et al reported that increased level of HER2 amplification in metastasis compared to primary tumor was associated with shorter overall survival.38
The situation regarding adjuvant treatment of HER2-positive breast cancer patients is even more complicated. In our study, high HER2/CEP17 ratio seems to be related to shorter metastasis-free survival (at the significance border). Meta-analysis published in 2016 stated that HER2 amplification is not a prognostic factor.8 However, this report was based on three studies, presenting inconsistent results:14–16 1) lack of statistically significant relation between HER2 amplification and disease-free survival,14 2) very high and low HER2 copy number associated with longer progression and overall survival,16 and 3) high HER2/CEP17 ratio and HER2 copy number related to shorter disease-free survival.15 In 2016, another article was published (not included in the meta-analysis), in which authors, similarly to us, reported poorer disease-free survival rate for patients with tumors characterized by high HER2/CEP17 ratio, although about 15% of those patients received neoadjuvant chemotherapy.18 Therefore, the role of HER2 amplification still seems to be undetermined in patients treated with trastuzumab in adjuvant setting. However, data obtained so far suggest that HER2 amplification is not a crucial factor for survival of HER2-positive breast cancer patients and its influence can be very slight.
In our study, HER3 expression was a significant tumor feature affecting patients’ survival. There are also other studies confirming that expression of HER3 is an indicator of shorter survival.39,40 Therefore, we analyzed combined effect of HER3 expression and HER2/CEP17 ratio and noted statistically significant (p=0.001) shorter metastasis-free survival in patients with tumors presenting HER3 expression together with high HER2/CEP17 ratio. It is not surprising, considering the fact that HER2 amplification is related to higher HER2 expression and HER2/HER3 heterodimer is considered the strongest activator of signaling pathways among EGFR family dimmers.41 Moreover, high level of HER2/HER3 dimers has been identified as an indicator of reduced relapse-free and overall survival.42
Therefore, the concept that blocking of HER2/HER3 heterodimerization can improve treatment outcome has a solid biological background. Pertuzumab is a monoclonal antibody against second domain of extracellular fragment of HER2, thus blocking its dimerization with other members of EGFR family.43 Many trials were conducted to evaluate efficiency of pertuzumab; however, its significance in adjuvant settings was confirmed only in the last year.44 Presented results showing HER3 expression as a marker of poorer survival after trastuzumab in adjuvant setting place them in clinical reality, suggesting the necessity of blocking of dimerization process, which is in agreement with recently published data from APHINITY trial. This clinical study concerned patients with nonmetastatic, adequately excised, node-positive or high-risk node-negative, histologically confirmed invasive HER2-positive breast cancer. The participants were randomly assigned to receive pertuzumab or placebo added to standard adjuvant chemotherapy plus 1 year of trastuzumab treatment. The trial demonstrated significantly higher 3-year rate of invasive disease-free survival in the pertuzumab group.44 It might lead to approval of using pertuzumab in adjuvant setting, as it has been approved in metastatic breast cancer or neoadjuvant treatment. CLEOPATRA study showed that adding pertuzumab to trastuzumab and docetaxel improved median duration of response, and based on those results, FDA approved in 2012 this treatment as first line for metastatic HER2-positive breast cancer.45 In 2013, based on NeoSphere trial data, pertuzumab was approved in neoadjuvant treatment (pertuzumab/trastuzumab/chemotherapy) for HER2-positive, locally advanced, inflammatory or early-stage high-risk breast cancers.45 Those data clearly demonstrated that dimerization of EGFR family members is a significant problem, influencing efficiency of trastuzumab treatment in all stages of cancer development and treatment schedule. Remembering that HER2/HER3 heterodimer is the most potent proliferation stimulator among all dimers of the EGFR family, it is not surprising that expression of HER3 is confirmed in some publications, including ours, as a marker of poorer survival.
Of course, we are aware of the limitations of our study. First limitation is the size of the group. However, we investigated a very specific cohort: HER2-positive breast cancer patients treated with adjuvant chemotherapy combined with trastuzumab. This was a single institution retrospective study, which might be treated both as a disadvantage and as an advantage. The investigated group consisted of a smaller number of patients, but all patients included in our study were diagnosed by the same team of pathologists and evaluation of FISH was done by the same person, who performed the assessment of HER2 gene status for diagnostic purposes. Also, all patients were operated at our institution, and we can have a long follow-up. In the future, we intent to enlarge the investigated group.
Although the degree of HER2 amplification might not be a decisive factor for survival of HER2-positive breast cancer patients, it probably could be analyzed with other parameters and help in distinguishing patients with worse prognosis.
Conclusion
- Lower HER2 copy number per cell and HER2/CEP17 ratio is associated with ER receptor positivity and lower level of HER2 protein (IHC 2+).
- Tumors with chromosome 17 polysomy are characterized by higher number of HER2 gene copy number per cell but lower HER2/CEP17 ratio.
- Presence of both unfavorable factors: HER3 expression and high HER2/CEP17 ratio are related to statistically significant shorter metastasis-free survival.
Acknowledgment
The study was financed by the National Science Centre, based on decision numbered DEC-2013/09/B/NZ5/00764.
Disclosure
The authors report no conflicts of interest in this work.
References
Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177–182. | ||
De P, Hasmann M, Leyland-Jones B. Molecular determinants of trastuzumab efficacy: what is their clinical relevance? Cancer Treat Rev. 2013;39(8):925–934. | ||
Wolff AC, Hammond ME, Hicks DG, et al; American Society of Clinical Oncology; College of American Pathologists. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013;31(31):3997–4013. | ||
Cobleigh MA, Vogel CL, Tripathy D, et al. Multinational study of the efficacy and safety of humanized anti-HER2 monoclonal antibody in women who have HER2-overexpressing metastatic breast cancer that has progressed after chemotherapy for metastatic disease. J Clin Oncol. 1999;17(9):2639–2648. | ||
Vogel CL, Cobleigh MA, Tripathy D, et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J Clin Oncol. 2002;20(3):719–726. | ||
Mukohara T. Mechanisms of resistance to anti-human epidermal growth factor receptor 2 agents in breast cancer. Cancer Sci. 2011;102(1):1–8. | ||
Luque-Cabal M, García-Teijido P, Fernández-Pérez Y, Sánchez-Lorenzo L, Palacio-Vázquez I. Mechanisms behind the resistance to trastuzumab in HER2-amplified breast cancer and strategies to overcome it. Clin Med Insights Oncol. 2016;10 (Suppl 1):21–30. | ||
Xu QQ, Pan B, Wang CJ, et al. HER2 amplification level is not a prognostic factor for HER2-positive breast cancer with trastuzumab-based adjuvant treatment: a systematic review and meta-analysis. Oncotarget. 2016;7(39):63571–63582. | ||
Lee HJ, Seo AN, Kim EJ, et al. HER2 heterogeneity affects trastuzumab responses and survival in patients with HER2-positive metastatic breast cancer. Am J Clin Pathol. 2014;142(6):755–766. | ||
Singer CF, Tan YY, Fitzal F, et al; Austrian Breast and Colorectal Cancer Study Group. Pathological complete response to neoadjuvant trastuzumab is dependent on HER2/CEP17 ratio in HER2-amplified early breast cancer. Clin Cancer Res. 2017;23(14):3676–3683. | ||
Kim JW, Kim JH, Im SA, et al. HER2/CEP17 ratio and HER2 immunohistochemistry predict clinical outcome after first-line trastuzumab plus taxane chemotherapy in patients with HER2 fluorescence in situ hybridization-positive metastatic breast cancer. Cancer Chemother Pharmacol. 2013;72(1):109–115. | ||
Fuchs EM, Köstler WJ, Horvat R, et al. High-level ERBB2 gene amplification is associated with a particularly short time-to-metastasis, but results in a high rate of complete response once trastuzumab-based therapy is offered in the metastatic setting. Int J Cancer. 2013;135(1):224–231. | ||
Giuliani R, Durbecq V, Di Leo A, et al. Phosphorylated HER-2 tyrosine kinase and Her-2/neu gene amplification as predictive factors of response to trastuzumab in patients with HER-2 overexpressing metastatic breast cancer (MBC). Eur J Cancer. 2007;43(4):725–735. | ||
Dowsett M, Procter M, McCaskill-Stevens W, et al. Disease-free survival according to degree of HER2 amplification for patients treated with adjuvant chemotherapy with or without 1 year of trastuzumab: the HERA Trial. J Clin Oncol. 2009;27(18):2962–2969. | ||
Xuan Q, Ji H, Tao X, Xu Y, Zhang Q. Quantitative assessment of HER2 amplification in HER2-positive breast cancer: its association with clinical outcomes. Breast Cancer Res Treat. 2015;150(3):581–588. | ||
Borley A, Mercer T, Morgan M, et al. Impact of HER2 copy number in IHC2+/FISH-amplified breast cancer on outcome of adjuvant trastuzumab treatment in a large UK cancer network. Br J Cancer. 2014;110(8):2139–2143. | ||
Perez EA, Reinholz MM, Hillman DW, et al. HER2 and chromosome 17 effect on patient outcome in the N9831 adjuvant trastuzumab trial. J Clin Oncol. 2010;28(28):4307–4315. | ||
Stocker A, Hilbers ML, Gauthier C, et al. HER2/CEP17 ratios and clinical outcome in HER2-positive early breast cancer undergoing trastuzumab-containing therapy. PLoS One. 2016;11(7):e0159176. | ||
Adamczyk A, Niemiec J, Janecka A, et al. Prognostic value of PIK3CA mutation status, PTEN and androgen receptor expression for metastasis-free survival in HER2-positive breast cancer patients treated with trastuzumab in adjuvant setting. Pol J Pathol. 2015;66(2):133–141. | ||
Wolff AC, Hammond ME, Schwartz JN, et al; American Society of Clinical Oncology; College of American Pathologists. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J Clin Oncol. 2007;25(1):118–145. | ||
Tchrakian N, Flanagan L, Harford J, Gannon JM, Quinn CM. New ASCO/CAP guideline recommendations for HER2 testing increase the proportion of reflex in situ hybridization tests and of HER2 positive breast cancers. Virchows Arch. 2016;468(2):207–211. | ||
Polónia A, Leitão D, Schmitt F. Application of the 2013 ASCO/CAP guideline and the SISH technique for HER2 testing of breast cancer selects more patients for anti-HER2 treatment. Virchows Arch. 2016;468(4):417–423. | ||
Owens MA, Horten BC, Da Silva MM. HER2 amplification ratios by fluorescence in situ hybridization and correlation with immunohistochemistry in a cohort of 6556 breast cancer tissues. Clin Breast Cancer. 2004;5(1):63–69. | ||
Petroni S, Addati T, Mattioli E, et al. Centromere 17 copy number alteration: negative prognostic factor in invasive breast cancer? Arch Pathol Lab Med. 2012;136(9):993–1000. | ||
Tsuda H, Akiyama F, Terasaki H, et al. Detection of HER-2/neu (c-erb B-2) DNA amplification in primary breast carcinoma. Interobserver reproducibility and correlation with immunohistochemical HER-2 overexpression. Cancer. 2001;92(12):2965–2974. | ||
Luoh SW, Ramsey B, Hanlon Newell A, et al. HER-2 gene amplification in human breast cancer without concurrent HER-2 over-expression. Springerplus. 2013;2:386. | ||
Loi S, Dafni U, Karlis D, et al. Effects of estrogen receptor and human epidermal growth factor receptor-2 levels on the efficacy of trastuzumab: a secondary analysis of the HERA trial. JAMA Oncol. 2016;2(8):1040–1047. | ||
Konecny G, Pauletti G, Pegram M, et al. Quantitative association between HER-2/neu and steroid hormone receptors in hormone receptor-positive primary breast cancer. J Natl Cancer Inst. 2003;95(2):142–153. | ||
Pietras RJ, Arboleda J, Reese DM, et al. HER-2 tyrosine kinase pathway targets estrogen receptor and promotes hormone-independent growth in human breast cancer cells. Oncogene. 1995;10(12):2435–2446. | ||
Varga Z, Tubbs RR, Moch H. Concomitant detection of HER2 protein and gene alterations by immunohistochemistry (IHC) and silver enhanced in situ hybridization (SISH) identifies HER2 positive breast cancer with and without gene amplification. PLoS One. 2014;9(8):e105961. | ||
Press MF, Sauter G, Buyse M, et al. HER2 gene amplification testing by fluorescent in situ hybridization (FISH): comparison of the ASCO-College of American Pathologists Guidelines with FISH scores used for enrollment in Breast Cancer International Research Group clinical trials. J Clin Oncol. 2016;34(29):3518–3528. | ||
Perez EA, Baehner FL, Butler SM, et al. The relationship between quantitative human epidermal growth factor receptor 2 gene expression by the 21-gene reverse transcriptase polymerase chain reaction assay and adjuvant trastuzumab benefit in Alliance N9831. Breast Cancer Res. 2015;17(1):133. | ||
Lehmann-Che J, Amira-Bouhidel F, Turpin E, et al. Immunohistochemical and molecular analyses of HER2 status in breast cancers are highly concordant and complementary approaches. Br J Cancer. 2011;104(11):1739–1746. | ||
Ng CK, Martelotto LG, Gauthier A, et al. Intra-tumor genetic heterogeneity and alternative driver genetic alterations in breast cancers with heterogeneous HER2 gene amplification. Genome Biol. 2015;16:107. | ||
Janiszewska M, Liu L, Almendro V, et al. In situ single-cell analysis identifies heterogeneity for PIK3CA mutation and HER2 amplification in HER2-positive breast cancer. Nat Genet. 2015;47(10):1212–1219. | ||
Cameron D, Piccart-Gebhart MJ, Gelber RD, et al; Herceptin Adjuvant (HERA) Trial Study Team. 11 years’ follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer: final analysis of the HERceptin Adjuvant (HERA) trial. Lancet. 2017;389(10075):1195–1205. | ||
Guiu S, Gauthier M, Coudert B, et al. Pathological complete response and survival according to the level of HER-2 amplification after trastuzumab-based neoadjuvant therapy for breast cancer. Br J Cancer. 2010;103(9):1335–1342. | ||
Gullo G, Bettio D, Zuradelli M, et al. Level of HER2/neu amplification in primary tumours and metastases in HER2-positive breast cancer and survival after trastuzumab therapy. Breast. 2013;22(2):190–193. | ||
Park YH, Jung HA, Choi MK, et al. Role of HER3 expression and PTEN loss in patients with HER2-overexpressing metastatic breast cancer (MBC) who received taxane plus trastuzumab treatment. Br J Cancer. 2014;110(2):384–391. | ||
Ocana A, Vera-Badillo F, Seruga B, Templeton A, Pandiella A, Amir E. HER3 overexpression and survival in solid tumors: a meta-analysis. J Natl Cancer Inst. 2013;105(4):266–273. | ||
Zaczek A, Brandt B, Bielawski KP. The diverse signaling network of EGFR, HER2, HER3 and HER4 tyrosine kinase receptors and the consequences for therapeutic approaches. Histol Histopathol. 2005;20(3):1005–1015. | ||
Spears M, Taylor KJ, Munro AF, et al. In situ detection of HER2:HER2 and HER2:HER3 protein-protein interactions demonstrates prognostic significance in early breast cancer. Breast Cancer Res Treat. 2012;132(2):463–470. | ||
Zagouri F, Sergentanis TN, Chrysikos D, et al. Pertuzumab in breast cancer: a systematic review. Clin Breast Cancer. 2013;13(5):315–324. | ||
von Minckwitz G, Procter M, de Azambuja E, et al; APHINITY Steering Committee and Investigators. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer. N Engl J Med. 2017;377(2):122–131. | ||
Gerratana L, Bonotto M, Bozza C, et al. Pertuzumab and breast cancer: another piece in the anti-HER2 puzzle. Expert Opin Biol Ther. 2017:17(3):365–374. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.