Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Relationship Between Glucose/Lipid Metabolism and Placental Biomarkers in Gestational Diabetes and Preeclampsia
Authors Zhou M, Feng Y, Zhang C, Tian X, Li M, Zheng Y ![]()
Received 4 November 2024
Accepted for publication 11 February 2025
Published 3 March 2025 Volume 2025:18 Pages 691—702
DOI https://doi.org/10.2147/DMSO.S504653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Meng Zhou,* Yapei Feng,* Chunxia Zhang, Xiangwen Tian, Mingde Li, Yujie Zheng
Department of Obstetrics and Gynecology, Shengli Oilfield Central Hospital, Dongying, Shandong, 257000, China
*These authors contributed equally to this work
Correspondence: Yujie Zheng, Email [email protected]
Objective: To investigate the significance and relationship of glucose and lipid metabolism, placental resistin, and human lipid carrier protein (LCN— 2) expression in pregnant women with gestational diabetes mellitus (GDM) complicated by severe preeclampsia (SPE).
Methods: A total of 89 patients with GDM and SPE (G+S group) and 89 patients with GDM alone (GDM group) were included. Blood samples were collected to measure glucose and lipid metabolism indicators [fasting blood glucose (FBG), fasting insulin (FINS), glycosylated hemoglobin (HbA1c), total cholesterol (TC), triglycerides (TG), HDL-C, and LDL-C], and immunohistochemistry was used to assess placental resistin and LCN— 2 levels. Delivery conditions and adverse maternal and neonatal outcomes were compared. Pearson correlation analysis was conducted to explore the relationship between placental resistin, LCN— 2, and glucose and lipid metabolism indicators.
Results: FBG, FINS, HbA1c, TC, and TG levels were higher, and HDL-C was lower in the G+S group compared to the GDM group (P< 0.05). The positive expression rates of resistin and LCN— 2 in placental tissue were also higher in the G+S group (P< 0.05). The G+S group had lower gestational weeks, neonatal birth weight, and higher postpartum hemorrhage than the GDM group (P< 0.05). The G+S group showed higher rates of adverse maternal outcomes (postpartum hemorrhage, intrauterine infection) and neonatal outcomes (preterm birth, fetal distress) (P< 0.05). Pearson analysis showed that placental resistin and LCN— 2 expression were positively correlated with FBG, FINS, TC, and TG, and negatively correlated with HDL-C (P< 0.05).
Conclusion: Pregnant women with GDM and SPE have higher risks of glucose and lipid metabolism disorders, placental resistin and LCN— 2 expression, and adverse maternal and neonatal outcomes compared to GDM patients. Resistin and LCN— 2 may influence glucose and lipid metabolism, affecting pregnancy outcomes.
Keywords: gestational diabetes mellitus, severe preeclampsia, placental resistin, human lipid carrier protein, correlation
Introduction
According to the International Diabetes Federation (IDF), the global prevalence of gestational diabetes mellitus (GDM) was approximately 14.0% in 2017, with North America at 12.6%, Africa at 9.0%, and Asia at 21.0%.1 With the development of China’s economy and the reform of its fertility policies, the prevalence of GDM has been increasing. Meta-analysis and systematic review results show that, based on the standards of the International Association of Diabetes and Pregnancy Study Groups (IADPSG), the overall prevalence of GDM in China is 14.8%.2 Preeclampsia (PE) is a pregnancy-related hypertensive disorder that severely impacts maternal and fetal health and is a leading cause of increased maternal and perinatal mortality. Reports indicate that the prevalence of GDM complicated by PE (GDM-PE) ranges from 6.0% to 15%.3 The pathophysiology of GDM-PE is complex and can lead to multi-organ dysfunction, causing severe harm to both the mother and the fetus. The earlier the onset of the disease, the greater the impact on maternal and fetal outcomes. Currently, the pathophysiology of GDM and PE is distinct, but there are some overlaps, especially in terms of the interactions between metabolism and the immune system. GDM is primarily caused by insulin resistance, insufficient insulin secretion, and changes in placental hormones.4 Severe Preeclampsia (SPE) is mainly caused by placental development abnormalities, poor blood flow perfusion, endothelial dysfunction, and immune response abnormalities. The connection between the two: metabolic disorders, inflammation, and oxidative stress are potential common points, with pregnant women with GDM being more likely to develop SPE.5 Studies6 have shown that GDM and SPE often coexist in late pregnancy, and their combined presence further aggravates maternal glucose and lipid metabolism disorders. The pathogenesis of GDM complicated by SPE is complex and involves significant multi-factorial interactions, with metabolic abnormalities and placental dysfunction at its core.7 Glucose and lipid metabolism imbalance not only exacerbates insulin resistance in pregnant women but also affects placental angiogenesis and structural function, thus adversely impacting fetal development.8 Therefore, an in-depth exploration of the glucose and lipid metabolism mechanisms and the role of placental factors in GDM combined with SPE not only helps to reveal the key pathological processes of its development but also provides new ideas for clinical prevention and intervention.
The placenta, as a key organ for maternal-fetal substance exchange, is considered to be a core factor in the occurrence of adverse maternal and neonatal outcomes due to its dysfunction.9 Recent studies10,11 have found that a significant increase in the expression of certain specific factors in the placenta is closely related to maternal metabolic imbalance, which may affect fetal development and maternal health by regulating the glucose and lipid metabolism function of the placenta. Resistin, an inflammatory factor secreted by adipose tissue, plays an important role in the occurrence and development of insulin resistance and metabolic syndrome.12 Previous studies13 have shown that elevated resistin levels are closely related to the pathological processes of GDM and SPE, suggesting that it may be one of the key regulatory factors of metabolic abnormalities in GDM complicated by SPE. Human Lipocalin-2 (LCN-2) is a secretory glycoprotein, and recent studies have found that LCN-2 is associated with the onset of pregnancy-related metabolic disorders,14 and studies15 have pointed out that its abnormal expression in pregnant women may affect lipid metabolism in the placenta, thereby interfering with lipid transfer between the mother and fetus. However, there are few domestic studies on the relationship between LCN-2, GDM, and PE. Therefore, in-depth research on the expression of resistin and LCN-2 in the placenta of patients with GDM and SPE, and their relationship with glucose and lipid metabolism disorders, not only aids in better understanding the mechanisms behind adverse pregnancy outcomes in these patients but also may provide new targets for clinical intervention. Based on the above reasons, this study detects the expression levels of resistin and LCN-2 in the placental tissues of patients with GDM and SPE in our hospital and analyzes their relationship with glucose and lipid metabolism indicators, aiming to provide a scientific basis for the prevention and treatment of glucose and lipid metabolism disorders in patients with GDM and SPE and to offer new research directions for reducing the risk of adverse pregnancy outcomes in these patients.
Data and Methods
Clinical Data
A total of 89 patients with gestational diabetes mellitus (GDM) complicated by severe preeclampsia (SPE) treated at our hospital between April 2022 and January 2024 were selected as the study subjects (G+S Group). Additionally, 89 patients with GDM alone during the same period were selected as controls (GDM Group). Inclusion criteria: ① Both GDM and SPE meet the relevant clinical diagnostic criteria: GDM is diagnosed according to the World Health Organization (WHO) and International Association of Diabetes and Pregnancy Study Groups (IADPSG) criteria, and SPE is diagnosed according to ACOG and FIGO criteria;16,17 ② Natural conception with singleton, cephalic pregnancy confirmed by ultrasound; ③ Normal structure and function of the birth canal; ④ Good cognitive and communication abilities, clear consciousness upon admission, high adherence to the study process, able to cooperate with the study requirements, and signed informed consent. Exclusion criteria: ① Severe organ dysfunction; ② Presence of immune, metabolic, or hematologic diseases; ③ Endocrine or infectious diseases; ④ Severe cardiovascular or cerebrovascular diseases; ⑤ History of adverse pregnancies or childbirth; ⑥ Other pregnancy complications; ⑦ Use of assisted reproductive technology; ⑧ Recent (within 1 month) use of medications affecting glucose and lipid metabolism; ⑨ Poor compliance, dropout, or loss to follow-up. This study was approved by the Medical Ethics Committee of Shengli Oilfield Central Hospital (Approval No.: YXLL202405801), and ethical standards were strictly followed throughout the research. Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki.
Main Reagents and Instruments
The main reagents used in this experiment include rabbit anti-human resistin polyclonal antibody and rabbit anti-human lipocalin (LCN-2) polyclonal antibody (Catalog No.: YK-RH001 and YK-LC001, Xiamen Yanke Biotechnology Co., Ltd)., ready-to-use high-efficiency immunohistochemistry kit (Catalog No.: AB-HIK001, Shanghai Absin Biotechnology Co., Ltd)., enzyme-linked immunosorbent assay (ELISA) kits (Catalog No.: ELISA-EL1001, Wuhan Elabscience Biotechnology Co., Ltd). Major equipment includes: ES-500 fully automatic tissue embedding machine (Catalog No.: XY-ES500, Shanghai Xinyu Biotechnology Co., Ltd)., RM2135 microtome (Catalog No.: Leica-RM2135, Leica, Germany), BS280 fully automated biochemical analyzer (Catalog No.: Mindray-BS280, Mindray Bio-Medical Electronics Co., Ltd., Shenzhen), and BX-41 optical microscope (Catalog No.: Olympus-BX41, Olympus, Japan).
Methods
Specimen Collection Method
Within 24 hours of admission, 5 mL of peripheral elbow venous blood was collected from each patient by healthcare personnel, and serum was separated after centrifugation at 1500 r/min for 5 minutes, then preserved aseptically for future use. Within 2 minutes after delivery, a 2.0 cm × 1.0 cm × 1.0 cm block of placental tissue near the root of the umbilical cord on the maternal surface was collected, rinsed with physiological saline, placed in a pathology bag containing fixative, and labeled accordingly.
Detection Methods
Measurement of Glucose and Lipid Metabolism
The levels of glucose and lipid metabolism-related indicators were measured using a fully automated biochemical analyzer. The levels of total cholesterol (TC) and triglycerides (TG) were measured by enzyme-based colorimetric methods; high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) were measured by precipitation techniques; fasting blood glucose (FBG) was measured by the glucose oxidase method; fasting insulin (FINS) was measured by chemiluminescence; glycated hemoglobin (HbA1c) was measured by high-performance liquid chromatography. All measurements were conducted according to equipment manuals and operational procedures to ensure data accuracy.
Determination of Resistin and LCN-2 in Placental Tissue
Immunohistochemistry was used to measure the expression levels of resistin and LCN-2 proteins in placental tissue. The specific steps are as follows: ① Specimen Fixation and Pretreatment: Placental tissue specimens were fixed in 4% paraformaldehyde solution, then rinsed with phosphate-buffered saline (PBS) to remove paraformaldehyde residues. The specimens underwent gradient alcohol dehydration to maintain tissue structure integrity and clear cell morphology. ② Sectioning and Staining: After dehydration, tissue blocks were continuously sectioned at a thickness of 5 μm using a microtome. After deparaffinization, hematoxylin-eosin (HE) staining was performed to observe the overall tissue structure, with eosin staining added after hematoxylin staining for 120 seconds. Samples were dehydrated in gradient alcohol, cleared with xylene, and finally mounted with neutral gum for microscopic observation. ③ Immunohistochemical Staining Steps: After deparaffinization, slides were incubated with 3% hydrogen peroxide deionized water to inhibit endogenous peroxidase activity, followed by heat antigen retrieval. Normal goat serum was added as a blocking solution to block nonspecific binding sites, incubated at room temperature for 10–15 minutes. ④ Primary Antibody Incubation: Rabbit anti-human resistin polyclonal antibody or rabbit anti-human LCN-2 polyclonal antibody was added, incubated at room temperature for 60 minutes, and the slides were stored overnight at 4°C. The next day, PBS was used to wash the slides 3 times for 3 minutes each to ensure the removal of nonspecific binding antibodies. ⑤ Secondary Antibody Incubation and Development: Biotin-labeled goat anti-rabbit IgG was added, incubated at room temperature for 60 minutes, washed again with PBS 3 times for 3 minutes each, and horseradish peroxidase-labeled solution was added, incubated at room temperature for 1 hour. After washing, a chromogenic agent was added for development, and if necessary, hematoxylin was added to enhance contrast. ⑥ Negative and Positive Controls: PBS buffer without primary antibody was used as a negative control to ensure experiment specificity, while known positive slides were used as positive controls to verify the staining accuracy. Staining results were observed and analyzed under a microscope.
Evaluation of Staining Results
For each slide, five high-power field areas were randomly selected to observe the positive expression of resistin and LCN-2 in placental tissue. Positive staining for resistin and LCN-2 was mainly localized in the cell membrane or cytoplasm of placental trophoblasts, and positive staining was indicated by the presence of brownish-yellow granules. The evaluation criteria for staining results were based on the number of positive cells and staining intensity, with the following scoring system: ① Scoring of Positive Cell Number: Based on the proportion of positive cells in the section: less than 5% positive cells scored 0 points; 6%–25% scored 1 point; 26%–50% scored 2 points; 51%–75% scored 3 points; more than 75% scored 4 points. ② Scoring of Staining Intensity: Based on the staining intensity: no significant staining scored 0 points; light yellow staining slightly above background scored 1 point; moderate brownish-yellow granules scored 2 points; abundant, uniformly distributed brown or dark brown granules scored 3 points. The scores of positive cell number and staining intensity were added to obtain a final composite score: a score ≤3 points was considered negative expression, and a score >3 points was considered positive expression. The scoring system used for evaluating the staining results is based on the general principles of immunohistochemical assessment of protein expression, as outlined in Nielsen et al (2015) for external quality assessment of immunohistochemistry in NordiQC.18 The criteria for scoring positive cell number and staining intensity were adapted from standard practices in immunohistochemistry, which have been validated in various tissue types, including placental tissues.
Observation of Pregnancy Outcomes
Pregnancy outcome data for both groups were recorded, including gestational age at delivery, newborn weight, postpartum blood loss, and delivery mode. Maternal and neonatal adverse pregnancy outcomes were also recorded in detail. Maternal outcomes included complications such as postpartum hemorrhage, intrauterine infection, placental abruption, and premature rupture of membranes. Neonatal outcomes included preterm birth, neonatal asphyxia, neonatal hypoglycemia, fetal distress, fetal growth restriction, and macrosomia.
Statistical Analysis
Data were analyzed and visualized using GraphPad Prism 8, with analysis conducted using SPSS 22.0. Measurement data, assuming normal distribution and homogeneity of variance, are expressed as ( and were compared between groups using independent sample t-tests. Count data are expressed as n (%) and analyzed using chi-square (x²) tests. Pearson linear correlation analysis was used to analyze the correlation between resistin, LCN-2 expression, and glucose and lipid metabolism indicators. All tests were two-tailed, and a P-value <0.05 was considered statistically significant.
and were compared between groups using independent sample t-tests. Count data are expressed as n (%) and analyzed using chi-square (x²) tests. Pearson linear correlation analysis was used to analyze the correlation between resistin, LCN-2 expression, and glucose and lipid metabolism indicators. All tests were two-tailed, and a P-value <0.05 was considered statistically significant.
Results
Comparison of Basic Information
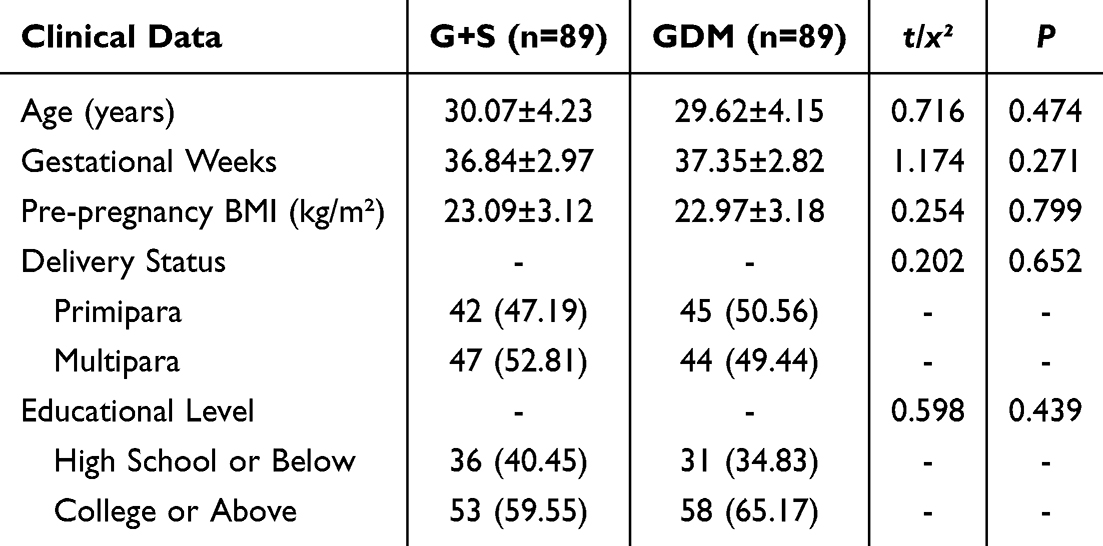
There were no statistically significant differences in age, gestational weeks, pre-pregnancy BMI, delivery status, or educational level between the two groups of pregnant women (P > 0.05), indicating comparability. See Table 1.
 |

Comparison of Lipid Metabolism Indicators
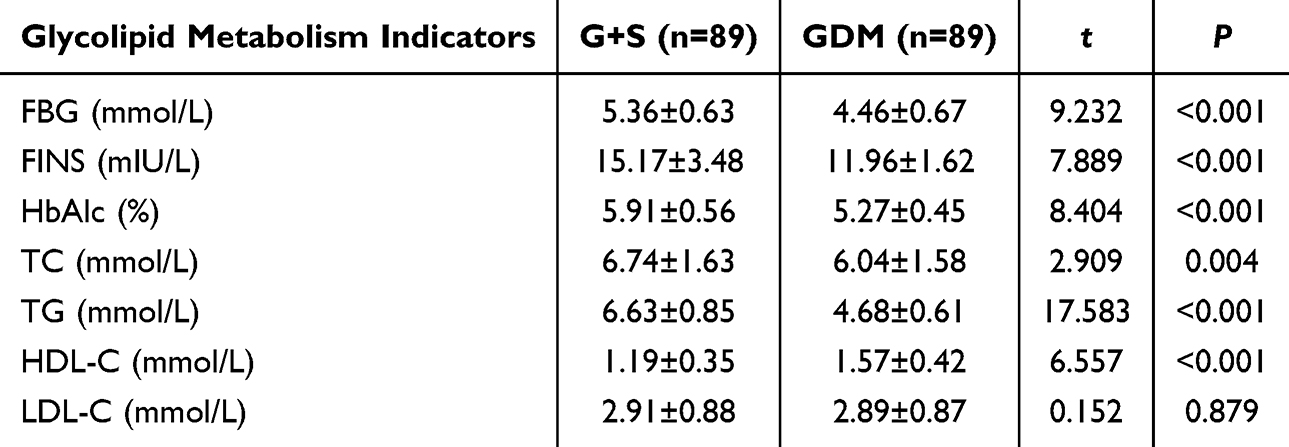
The G+S group had higher levels of FBG, FINS, HbAlc, TC, and TG compared to the GDM group, while HDL-C levels were lower than those in the GDM group (P < 0.05). There was no significant difference in LDL-C levels between the two groups (P > 0.05). See Table 2.
 |

Comparison of Positive Expression Rates of Resistin and LCN-2 Proteins in Placental Tissue
Among the 89 patients in the G+S group, 76 showed positive expression of resistin in placental tissue, and 72 showed positive expression of LCN-2 protein. In the GDM group, out of 89 patients, 53 had positive resistin expression and 50 had positive LCN—2 protein expression. The positive rates of resistin and LCN—2 in the G+S group were significantly higher than in the GDM group (P < 0.05). See Figure 1.
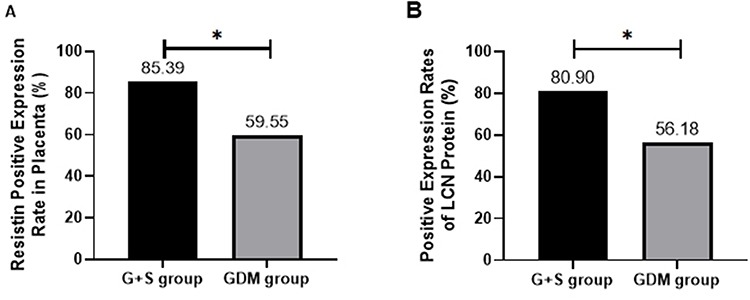 |
Figure 1 Comparison of Positive Expression Rates of Resistin and LCN—2 Proteins in Placental Tissue [n (%)]. (A) Positive Expression Rates of Resistin; (B) Positive Expression Rates of LCN—2 Protein. Note: * indicates P < 0.05. |
Comparison of Delivery Conditions
Among the 89 patients in the G+S group, 34 had natural deliveries. The gestational age at delivery in this group was (37.13±2.08) weeks, neonatal birth weight was (2907.48±356.82) g, and postpartum blood loss was (415.39±126.74) mL. In the GDM group, 60 patients had natural deliveries, with a gestational age at delivery of (38.24±1.76) weeks, neonatal birth weight of (3323.57±367.15) g, and postpartum blood loss of (338.46±101.97) mL. The G+S group had lower gestational age at delivery, neonatal birth weight, and proportion of natural delivery, but higher postpartum blood loss compared to the GDM group (P < 0.05). See Figures 2 and 3.
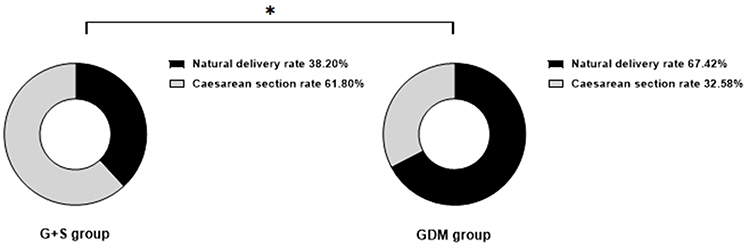 |
Figure 2 Comparison of Delivery Methods [n (%)]. Note: * indicates P < 0.05. |
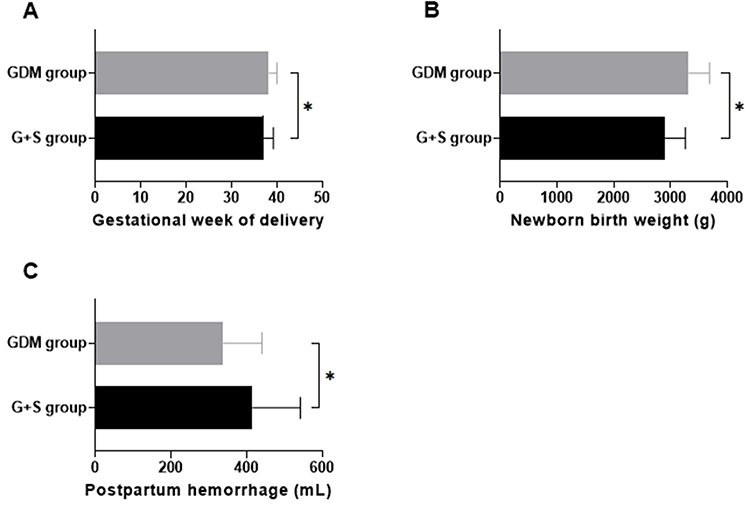 |
Figure 3 Comparison of Gestational Age at Delivery, Neonatal Birth Weight, and Postpartum Blood Loss. (A) Gestational week of delivery; (B) Newborn birth weight (g); (C) Postpartum hemorrhage (mL). Note: * indicates P < 0.05. |
Comparison of Adverse Maternal and Infant Outcomes
For maternal outcomes, the G+S group had higher rates of postpartum hemorrhage, intrauterine infection, and premature rupture of membranes compared to the GDM group (P < 0.05); there was no significant difference in the incidence of placental abruption between the two groups (P > 0.05). For neonatal outcomes, the G+S group had higher incidences of preterm birth, fetal distress, and fetal growth restriction compared to the GDM group (P < 0.05). There were no significant differences between the two groups in the incidences of neonatal asphyxia, neonatal hypoglycemia, and macrosomia (P > 0.05). See Tables 3 and 4.
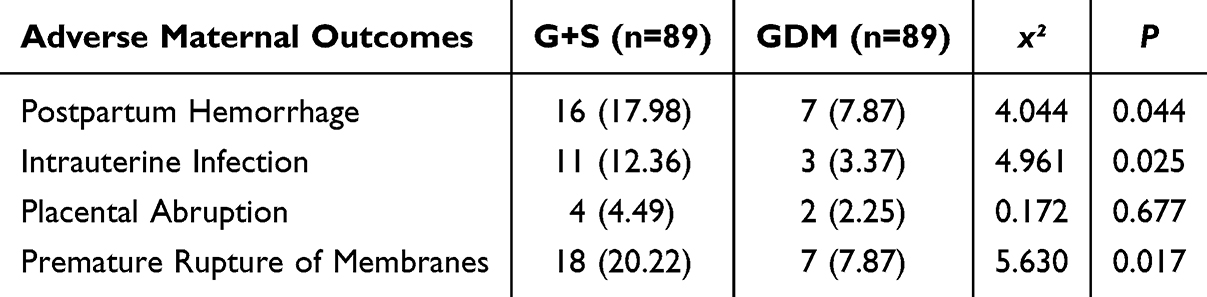 |
Table 3 Comparison of Adverse Maternal Outcomes [n (%)] |
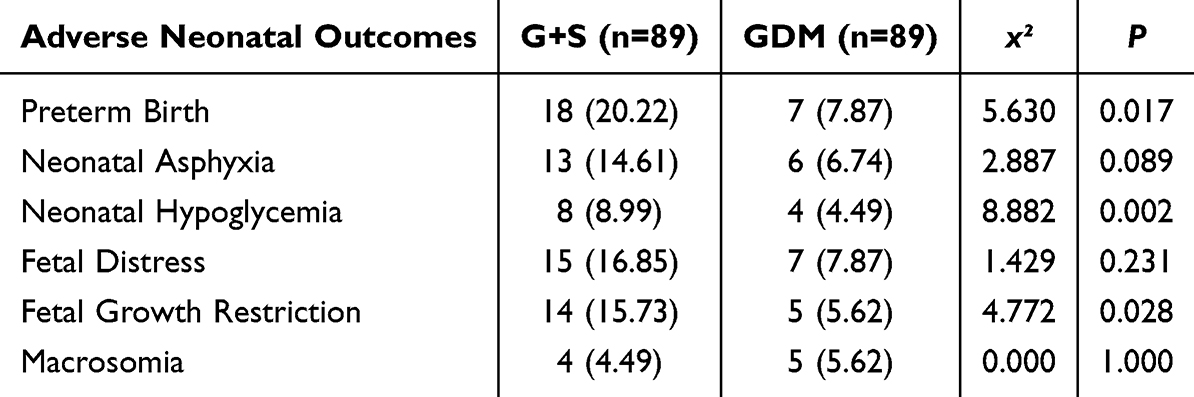 |
Table 4 Comparison of Adverse Neonatal Outcomes [n (%)] |
Correlation Analysis Between Positive Expression Rates of Resistin, LCN-2 Protein in Placental Tissue of Pregnant Women with GDM Complicated by SPE and Glycolipid Metabolism Indicators
Pearson correlation analysis showed that the positive expression of resistin and LCN-2 protein in the placental tissue of pregnant women with GDM complicated by SPE was positively correlated with FBG, FINS, TC, and TG, and negatively correlated with HDL-C (P < 0.05). See Table 5 and Figures 4 and 5.
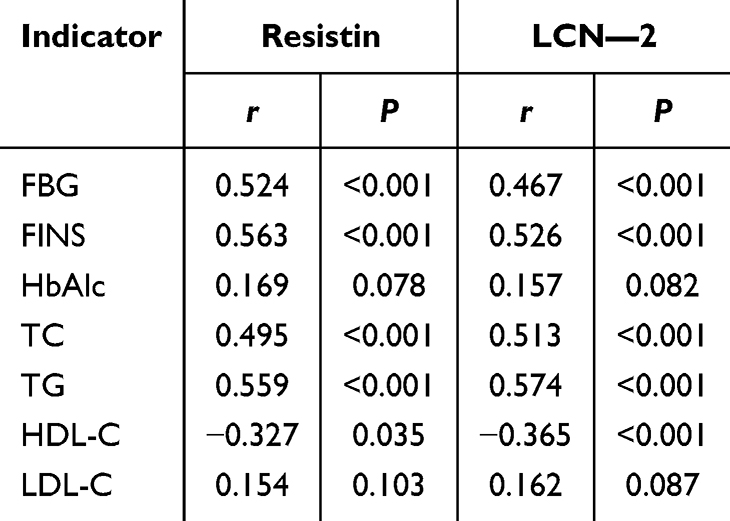 |
Table 5 Correlation Between Positive Expression Rates of Resistin, LCN—2 Protein in Placental Tissue of Pregnant Women with GDM Complicated by SPE and Glycolipid Metabolism Indicators |
 |
Figure 4 Correlation Between Positive Expression Rates of Resistin in Placental Tissue of Pregnant Women with GDM Complicated by SPE and Glycolipid Metabolism Indicators. |
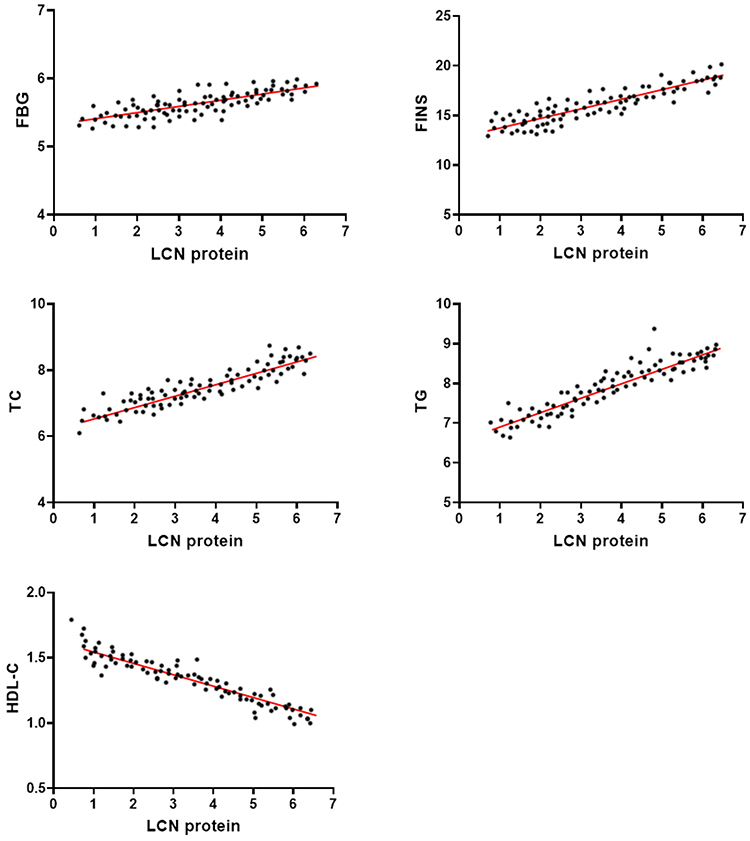 |
Figure 5 Correlation Between Positive Expression Rates of LCN—2 Protein in Placental Tissue of Pregnant Women with GDM Complicated by SPE and Glycolipid Metabolism Indicators. |
Discussion
Currently, the pathological mechanisms of GDM complicated by SPE are not fully understood, but increasing research19 suggests that adipokines secreted in placental tissue may play an important role in this process. Adipokines can exacerbate insulin resistance by influencing endothelial cell metabolism and activation, thereby creating conditions for the development of SPE.20 Resistin, a cysteine-rich protein secreted by adipose tissue, has the function of regulating insulin sensitivity.21 Specifically, resistin can reduce glucose uptake and utilization in peripheral tissues, resulting in disorders of glycolipid metabolism. Therefore, resistin is believed to play a crucial role in the pathogenesis of GDM complicated by SPE. Recent studies22 have shown that resistin can promote endothelial cell activation and smooth muscle cell proliferation, leading to endothelial dysfunction, which in turn contributes to the pathological processes of GDM and SPE. However, other studies23 have noted that, compared to normal pregnancy, serum resistin levels are lower in SPE patients, possibly reflecting individual differences or dynamic changes in the pathological process. Our study found that the positive expression rate of resistin in the placental tissue of patients with GDM complicated by SPE was significantly higher than in the GDM-only group, supporting the hypothesis that resistin may have a significant impact on vascular and metabolic regulation in patients with GDM complicated by SPE. In addition, our study further revealed that the degree of glycolipid metabolism disorder in GDM complicated by SPE is more severe than in GDM alone, as indicated by elevated levels of FBG, FINS, TC, TG, and decreased HDL-C. This finding is consistent with previous research,24 suggesting that patients with GDM complicated by SPE have higher insulin resistance and more pronounced glycolipid metabolism disorders. It can be inferred that high levels of resistin in placental tissue may exacerbate insulin resistance through a series of mechanisms in the pathological process of GDM complicated by SPE. Physiologically, resistin may directly act on insulin target organs, such as skeletal muscle and liver, inhibiting glucose uptake and thereby reducing glucose tolerance. Additionally, elevated resistin can activate multiple inflammatory signaling pathways, exacerbating endothelial dysfunction and causing excessive production of vasoconstrictors. With the proliferation of vascular smooth muscle cells and increased endothelial cell permeability, the vascular lumen gradually narrows and undergoes spasms, leading to elevated blood pressure and ultimately triggering SPE.
Recent studies25 indicate that as an important molecular regulatory factor, adipokine LCN-2 may play a key role in the pathogenesis of GDM complicated by SPE. LCN-2 can not only promote placental trophoblast invasion and placental formation by synergizing with matrix metalloproteinase-9 (MMP-9),26 but also participates in regulating inflammatory responses, insulin metabolism, and ischemia-reperfusion injury.27 Research by Schröder et al28 observed significant overexpression of LCN-2 in the serum and placental tissue of SPE patients. Our study similarly found that compared with the GDM-only group, the positive expression rate of LCN-2 in the placental tissue of the GDM complicated by SPE (G+S) group was significantly higher (P < 0.05), further supporting the prevalence and physiological relevance of this phenomenon. This suggests that LCN-2 may play an important role in the pathological process of GDM complicated by SPE, and its high expression may be closely related to disease progression. It is speculated that the high expression of LCN-2 may exacerbate insulin resistance and endothelial damage through various mechanisms, thus playing a key role in the pathological process of GDM complicated by SPE. First, high LCN-2 expression may induce insulin resistance in hepatocytes, which in turn increases adipocyte activity by activating peroxisome proliferator-activated receptor γ (PPARγ) in adipocytes.29,30 PPARγ activation accelerates fat metabolism, leading to excessive production of lipid breakdown products and inducing lipid peroxidation reactions, thereby causing endothelial damage. This damage not only increases vascular permeability but also raises blood pressure. Meanwhile, high LCN-2 levels may inhibit nitric oxide synthesis, which plays an essential role in vasodilation. Its reduction can exacerbate glycolipid metabolism disorders and increased vascular resistance, further intensifying the extent of elevated blood pressure and insulin resistance. Additionally, our study revealed that GDM complicated by SPE may have a significant impact on maternal and fetal outcomes. Data showed that neonatal weight in the G+S group was significantly lower than in the GDM-only group, and the rate of preterm birth was higher, along with increased postpartum hemorrhage and elevated incidences of fetal distress, premature rupture of membranes, and fetal growth restriction. These findings suggest that GDM complicated by SPE may significantly increase the risk of adverse maternal and fetal outcomes. The potential reasons may be related to the exacerbation of glycolipid metabolic disorders and increased insulin resistance. These metabolic abnormalities may cause spasms in small arteries throughout the body, reducing blood supply to the placenta, resulting in placental ischemia and hypoxia, hindering nutrient and oxygen exchange between mother and fetus, and ultimately leading to adverse outcomes such as fetal growth restriction and low neonatal birth weight. Further analysis indicates that endothelial dysfunction in pregnant women with GDM complicated by SPE is relatively severe. This endothelial dysfunction may not only lead to preterm birth but also increase the risk of postpartum hemorrhage due to uterine atony. The hypertension and small artery spasms caused by SPE may reduce blood supply, affect placental perfusion, and lead to decreased placental function.31,32 Therefore, pregnant women with GDM complicated by SPE often face a higher risk of postpartum hemorrhage, requiring more active monitoring and intervention measures during the perinatal period to reduce the incidence of adverse pregnancy outcomes. However, it is important to emphasize that glycolipid metabolic disorders and placental factors, such as increased expression of resistin and LCN-2, are not the only risk factors for adverse outcomes in GDM complicated by SPE. Other factors, including genetic predisposition, lifestyle choices (eg, diet and physical activity), and environmental influences, also contribute to the development of these conditions. For instance, genetic polymorphisms related to insulin resistance and vascular function could predispose individuals to more severe GDM and preeclampsia. Additionally, maternal obesity, lack of prenatal care, and poor diet may worsen metabolic disturbances and increase the risk of complications. Environmental factors like stress and pollution may also play a role. Therefore, a multifactorial approach is needed to fully understand the risk factors for GDM complicated by SPE. Future studies should explore these additional factors, as they could provide a more comprehensive understanding of the mechanisms underlying adverse maternal and neonatal outcomes.
Additionally, this study further revealed that the expression levels of resistin and LCN-2 protein in the placental tissue of patients with GDM complicated by SPE were significantly correlated with various glycometabolic and lipid parameters. Specifically, the expression of resistin and LCN-2 in the placenta was positively correlated with FBG, FINS, TC, and TG, while negatively correlated with HDL-C (P < 0.05). These correlations suggest that resistin and LCN-2 may increase the risk of adverse pregnancy outcomes in patients with GDM complicated by SPE by influencing glycometabolism and lipid metabolism. It is speculated that when TC and TG levels rise and HDL-C levels decrease, lipid peroxidation reactions are induced in the body, resulting in vascular endothelial dysfunction and an increased risk of cardiovascular disease. The high expression of resistin and LCN-2 may exacerbate this metabolic disorder, further advancing insulin resistance. The aggravation of insulin resistance can lead to increased levels of FBG and FINS, forming hyperinsulinemia, which worsens lipid metabolism disorders in the body.33 As lipid metabolism becomes unbalanced, inflammatory responses in the body increase, potentially affecting the synthesis of important physiological regulators such as prostaglandin E2.34 Prostaglandin E2 plays an essential role in maintaining normal vascular function and regulating vascular tension; however, its reduced synthesis may worsen peripheral vascular resistance, exposing the vascular walls to higher pressure and potentially inducing hypertension. Furthermore, this disorder in glycometabolism and lipid metabolism affects not only the body’s energy metabolism but also has far-reaching negative impacts on endothelial cell function, causing structural and functional damage to vascular endothelium. As endothelial injury worsens, resistin and LCN-2 further aggravate the patient’s condition by enhancing insulin resistance and exacerbating metabolic disorders.
The limitations of this study include the following: ① Limited sample size: The relatively small sample size of this study may restrict the general applicability of the results. ② Short observation period: The observation period in this study may be relatively limited, failing to cover all stages of pregnancy or long-term follow-up, which may affect understanding of the dynamic changes in placental adipokines across different stages of pregnancy and their long-term impact on maternal and fetal outcomes. ③ Single-center data: This study is a single-center analysis, and the regional and population limitations may affect the generalizability of the findings. ④ Lack of inclusion of more potential influencing factors: Besides resistin and LCN-2, this study did not evaluate other adipokines or inflammatory factors that may affect GDM complicated by SPE, such as leptin and adiponectin. These factors may also participate in regulating glycometabolism, lipid metabolism, and vascular endothelial function, impacting the pathological progression of GDM complicated by SPE. ⑤ Insufficient depth in mechanism research: This study is primarily observational and did not conduct an in-depth exploration of the mechanisms of action of resistin and LCN-2, lacking in vitro or animal experimental data to support their physiological and molecular mechanisms. ⑥ Lack of consideration of individual patient differences: Variations in constitution, medical history, and lifestyle among patients may affect adipokine expression levels and disease progression, and this study did not fully control for or explore the influence of these individual differences, potentially limiting the interpretation of the results. These limitations suggest that future studies should aim to enhance the depth and generalizability of research by expanding sample sizes, extending follow-up periods, increasing research variables, and using multicenter data.
Conclusion
The high expression of resistin and LCN-2 may promote the imbalance of glycometabolism and lipid metabolism through multiple pathways, directly affecting maternal vascular health and leading to a series of adverse pregnancy outcomes. This finding not only reveals the potential mechanisms for the exacerbation of GDM complicated by SPE but also suggests that resistin and LCN-2 may become therapeutic targets in the future for regulating glycometabolism and protecting the vasculature. Based on the results of this study, further research on whether inhibition of resistin and LCN-2 expression can alleviate metabolic disorders in patients with GDM complicated by SPE and improve pregnancy outcomes may be a promising direction for future exploration.
In addition, future studies could focus on exploring gene expression profiles, such as through the analysis of long non-coding RNAs (lncRNAs) in this field. Investigating the role of lncRNAs in regulating the expression of resistin and LCN-2, as well as their potential involvement in the pathogenesis of GDM complicated by SPE, could provide valuable insights. This could help to identify novel biomarkers or therapeutic targets and advance our understanding of the molecular mechanisms underlying these conditions.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics and Consent Statements
This study was approved by the ethics committee of Shengli Oilfield Central Hospital. Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Sweeting A, Wong J, Murphy HR, et al. A clinical update on gestational diabetes mellitus. Endocr Rev. 2022;43(5):763–793. doi:10.1210/endrev/bnac003
2. Hauspurg A, Jeyabalan A. Postpartum preeclampsia or eclampsia: defining its place and management among the hypertensive disorders of pregnancy. Am J Obstet Gynecol. 2022;226(2s):S1211–s1221. doi:10.1016/j.ajog.2020.10.027
3. Joo EH, Kim YR, Kim N, et al. Effect of endogenic and exogenic oxidative stress triggers on adverse pregnancy outcomes: preeclampsia, fetal growth restriction, gestational diabetes mellitus and preterm birth. Int J mol Sci. 2021;22(18):10122. doi:10.3390/ijms221810122
4. Askin L, Abus S, Tanriverdi O. Resistin and cardiovascular disease: a review of the current literature regarding clinical and pathological relationships. Curr Cardiol Rev. 2022;18(1):e290721195114. doi:10.2174/1573403X17666210729101120
5. Liu Y, Li D, Bolatai A, et al. Progress in research on biomarkers of gestational diabetes mellitus and preeclampsia. Diabetes Metab Syndr Obes. 2023;16:3807–3815. doi:10.2147/DMSO.S433179
6. Pankiewicz K, Szczerba E, Fijałkowska A, et al. The impact of coexisting gestational diabetes mellitus on the course of preeclampsia. J Clin Med. 2022;11(21):6390. doi:10.3390/jcm11216390
7. Samanth R, Shenoy V, Sreedharan S, et al. Effect of preeclampsia and gestational diabetes mellitus on neonatal distortion product otoacoustic emissions: a tertiary care center study. Ann Otol Rhinol Laryngol. 2023;132(9):985–995. doi:10.1177/00034894221126259
8. Frankevich N, Tokareva A, Chagovets V, et al. COVID-19 infection during pregnancy: disruptions in lipid metabolism and implications for newborn health. Int J mol Sci. 2023;24(18):13787. doi:10.3390/ijms241813787
9. Cindrova-Davies T, Sferruzzi-Perri AN. Human placental development and function. Semin Cell Dev Biol. 2022;131:66–77. doi:10.1016/j.semcdb.2022.03.039
10. Ng SW, Lee C, Ng A, et al. Ferroportin expression and regulation in human placenta/fetal membranes: implications for ferroptosis and adverse pregnancy outcomes. Reprod Biol. 2023;23(4):100816. doi:10.1016/j.repbio.2023.100816
11. Redline RW, Roberts DJ, Parast MM, et al. Placental pathology is necessary to understand common pregnancy complications and achieve an improved taxonomy of obstetrical disease. Am J Obstet Gynecol. 2023;228(2):187–202. doi:10.1016/j.ajog.2022.08.010
12. Floeck A, Ferrari N, Joisten C, et al. Resistin in pregnancy: analysis of determinants in pairs of umbilical cord blood and maternal serum. Cytokine X. 2021;3(2):100052. doi:10.1016/j.cytox.2021.100052
13. Nava-Salazar S, Flores-Pliego A, Pérez-Martínez G, et al. Resistin modulates low-density lipoprotein cholesterol uptake in human placental explants via PCSK9. Reprod Sci. 2022;29(11):3242–3253. doi:10.1007/s43032-022-00943-w
14. Jaberi SA, Cohen A, D’Souza C, et al. Lipocalin-2: structure, function, distribution and role in metabolic disorders. Biomed Pharmacother. 2021;142:112002. doi:10.1016/j.biopha.2021.112002
15. Li L, Ling B, Mei J, et al. Expression and significance of serum soluble fms-like tyrosine kinase 1 (sFlt-1), CXC chemokine ligand 16 (CXCL16), and lipocalin 2 (LCN-2) in pregnant women with preeclampsia. Ann Palliat Med. 2021;10(7):7866–7871. doi:10.21037/apm-21-1553
16. Sert UY, Ozgu-Erdinc AS. Gestational Diabetes Mellitus Screening and Diagnosis. Adv Exp Med Biol. 2021;1307:231–255.
17. Gestational hypertension and preeclampsia: ACOG practice bulletin, number 222. Obstet Gynecol. 2020;135(6):e237–e260. doi:10.1097/AOG.0000000000003891
18. Nielsen S. External quality assessment for immunohistochemistry: experiences from NordiQC. Biotech Histochem. 2015;90(5):331–340. doi:10.3109/10520295.2015.1033462
19. Jiao B, Wang Y, Li S, et al. Dissecting human placental cells heterogeneity in preeclampsia and gestational diabetes using single-cell sequencing. Mol Immunol. 2023;161:104–118. doi:10.1016/j.molimm.2023.07.005
20. Dai C, Fei Y, Li J, et al. A novel review of homocysteine and pregnancy complications. Biomed Res Int. 2021;2021:6652231. doi:10.1155/2021/6652231
21. Tripathi D, Kant S, Pandey S, et al. Resistin in metabolism, inflammation, and disease. The FEBS Journal. 2020;287(15):3141–3149. doi:10.1111/febs.15322
22. Shi Y, Zhu N, Qiu Y, et al. Resistin-like molecules: a marker, mediator and therapeutic target for multiple diseases. Cell Commun Signal. 2023;21(1):18. doi:10.1186/s12964-022-01032-w
23. Chandrasekaran S, Barry D, Melhorn S, et al. Evaluating relationships between visceral fat measures and adipokines concentrations among women with a history of preeclampsia. Am J Perinatol. 2020;37(11):1140–1145. doi:10.1055/s-0039-1692454
24. Miehle K, Stepan H, Fasshauer M. Leptin, adiponectin and other adipokines in gestational diabetes mellitus and pre-eclampsia. Clin Endocrinol. 2012;76(1):2–11. doi:10.1111/j.1365-2265.2011.04234.x
25. Yang HH, Wang X, Li S, et al. Lipocalin family proteins and their diverse roles in cardiovascular disease. Pharmacol Ther. 2023;244:108385. doi:10.1016/j.pharmthera.2023.108385
26. Wang X, Li A, Guo Y, et al. iTRAQ-based proteomics screen identifies LIPOCALIN-2 (LCN-2) as a potential biomarker for colonic lateral-spreading tumors. Sci Rep. 2016;6(1):28600. doi:10.1038/srep28600
27. Tan Q, Zhang C, Rao X, et al. The interaction of lipocalin-2 and astrocytes in neuroinflammation: mechanisms and therapeutic application. Front Immunol. 2024;15:1358719. doi:10.3389/fimmu.2024.1358719
28. Schröder SK, Gasterich N, Weiskirchen S, et al. Lipocalin 2 receptors: facts, fictions, and myths. Front Immunol. 2023;14:1229885. doi:10.3389/fimmu.2023.1229885
29. Jung M, Brüne B, von Knethen A, et al. Lipocalin-2 abrogates epithelial cell cycle arrest by PPARγ inhibition. Lab Invest. 2018;98(11):1408–1422. doi:10.1038/s41374-018-0098-4
30. Yousuf M, Shakir S, Khan I, Mammadova K, Ishrat U Diabetes management through α-glucosidase inhibitors challenges and current perspectives. J Mod Biol Drug Discov. 2023;2:9. doi:10.53964/jmbdd.20230092
31. Jena MK, Sharma NR, Petitt M, et al. Pathogenesis of preeclampsia and therapeutic approaches targeting the placenta. Biomolecules. 2020;10(6):953. doi:10.3390/biom10060953
32. Tang H, Liu X, He P, et al. Lipid accumulation product is a novel index associated with osteoporosis: evidence from two Independent Cross-sectional Chinese populations. Clin Mol Epidemiol. 2024;1:3. doi:10.53964/cme.2024003
33. Lee SH, Park SY, Choi CS. Insulin resistance: from mechanisms to therapeutic strategies. Diabetes Metab J. 2022;46(1):15–37. doi:10.4093/dmj.2021.0280
34. Lu C, Jiang Y, Xu W, et al. Sestrin2: multifaceted functions, molecular basis, and its implications in liver diseases. Cell Death Dis. 2023;14(2):160. doi:10.1038/s41419-023-05669-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.