Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Relationship Among Sensory Over-Responsivity, Problem Behaviors, and Anxiety in Emerging Adults with Autism Spectrum Disorder
Authors Syu YC, Huang PC, Wang TY, Chang YC, Lin LY ![]()
Received 1 July 2020
Accepted for publication 17 August 2020
Published 24 September 2020 Volume 2020:16 Pages 2181—2190
DOI https://doi.org/10.2147/NDT.S270308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Ya-Cing Syu,1 Pai-Chuan Huang,1 Tsui-Ying Wang,1 Yen-Ching Chang,1 Ling-Yi Lin1,2
1Department of Occupational Therapy, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 2Institute of Allied Health Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Correspondence: Ling-Yi Lin Tel +886-6-235-3535 ext. 5917
Fax +886-6-237-6604
Email [email protected]
Introduction: Despite the highly prevailing rate of sensory over-responsivity, problem behaviors, and anxiety among emerging adults with autism spectrum disorder (ASD), little is known about the nature of their experiences. While previous studies have indicated potential relationships among these conditions, their connections still need to be clarified. This study aimed to examine the relationships between sensory over-responsivity, problem behaviors, and anxiety.
Methods: Fifty-seven emerging adults with ASD (Mage = 21.4, SD = 2.5; males = 80.7%) were recruited. The Adult Sensory Profile – Chinese version, Problem Behavior Scale of Scales of Independent Behavior – Revised, and Generalized Anxiety Disorder-7 – Chinese version (GAD-7) were used.
Results: The percentage of emerging adults with ASD who scored more than most people in the two quadrants were sensation sensitivity = 33.3% and sensation avoiding = 26.3%. Approximately 66.7%, 27.5%, and 50.9% of participants had internalizing behaviors, externalizing behaviors, and asocial behaviors, respectively. Approximately, 64.9% of the participants scored on or above the cut-off score of 6 on the GAD-7. Sensation sensitivity and sensation avoiding were significantly correlated to problem behaviors; and anxiety was a mediating variable that accounts for the relationships between sensory over-responsivity and problem behaviors.
Conclusion: These results indicated that emerging adults with ASD showing problem behaviors might also report more exaggerated responses toward sensory inputs and experience more anxiety symptoms. The results indicate that sensory over-responsivity, problem behaviors, and anxiety may have common underlying mechanisms. Findings can be useful to understand the impacts of such difficulties for emerging adults with ASD.
Keywords: autism spectrum disorder, sensory over-responsivity, anxiety, problem behaviors
Introduction
Autism spectrum disorder (ASD) is a lifelong developmental disability that often presents persistent deficits in social communication and interaction problems, restricted or repetitive patterns of behavior and interests, and hyper- or hypo-reactivity to sensory input or unusual interests.1 A growing number of children diagnosed with ASD are aging into adolescence and toward adulthood. The transition from adolescence to adulthood is a critical stage in which youth experience changes in contextual and social roles, begin to take responsibility for their own choices, and learn and train for their occupation of choice. Research for adults with ASD is urgently warranted at the beginning of adulthood.2 Emerging adulthood (ages 18–25 years) is a period wherein youth may pursue further education, prepare to enter the workforce, participate in the community, or achieve a certain degree of independent living based on their level of functioning.3 Considering the cultural differences between Western and Eastern societies, evidence suggests that Chinese emerging adults may feel more obligated or responsible to their families and the society.4 Nevertheless, the core characteristics of ASD could greatly impact several aspects of their lives, including the ability to relate to things, events, and people. Emerging adults with ASD often face the responsibility of making their own decisions while not completely understanding their abilities or challenges, and they often feel alienated from their peer group.5 Clinical experiences suggest that problem behaviors and sensory over-responsivity are highly prevalent in individuals with ASD.6 These behaviors are barriers to employment, residential living, social opportunity, and community-based services.7
Problem behaviors (or maladaptive behaviors) are behaviors that interfere with everyday activities, including self-injurious behavior, withdrawal, uncooperative behavior, aggression, disruptive behavior, and destruction of property.8 Problem behaviors have been widely documented in studies on individuals with ASD and include a range of emotional and behavior problems including internalizing and externalizing behaviors.8–10 In a longitudinal study that was conducted for 24 years, the negative effects of problem behaviors persisted when not treated and were associated with poor adult outcomes.11 Recent longitudinal autism research has observed an overall decline in problem behaviors over time among adults with ASD.8,12,13 However, several studies have shown a high prevalence rate and high symptom stability of problem behaviors in adolescences and adults with ASD.12,13 In addition, problem behaviors are associated with vocational independence and activities of daily living, lower feelings of parent–child closeness, and a decreased sense of autonomy.14,15
Sensory processing refers to the ability to manage the sensory information received from the surroundings and from the body.16,17 Sensory over-responsivity is a sensory processing difficulty, which implies exaggerated or negative responses to sensory stimuli.18 Sensory over-responsivity reflects two behavior patterns according to Dunn’s model: sensation sensitivity and sensation avoiding.16,17 Some research findings suggest that sensory over-responsivity is common in individuals with ASD and is linked to sleep problems, lower levels of social skills and adaptive behaviors, and increased anxiety; moreover, when combined with anxiety, it predicts an increasing level of gastrointestinal problems.18–21 Among the few studies that included adults with ASD, the results have shown that sensory over-responsivity persists into adulthood.22–24 Sensory over-responsivity can affect an individual’s emotional states, education participation, social life, and work performance.22,23 Previous studies have also suggested that over-responsiveness to sensory stimuli may negatively impact on psychological well-being in children.18,19,21,25 However, little is known regarding this issue in emerging adults with ASD, thus indicating the need for further investigation.
Sensory over-responsivity might correlate with problem behaviors. However, thus far, only three studies have examined the relationship between sensory processing dysfunction, emotion, and behavior problems in children with ASD. Tseng et al26 found that sensation avoiding and sensory sensitivity were significantly associated with internalizing and externalizing problem behaviors in 67 children with ASD aged 48–84 months. O’Donnell et al27 found that preschool children had higher levels of sensory processing difficulties are more likely to present problem behaviors, including irritability, lethargy, stereotypic behaviors, hyperactivity/noncompliance, and inappropriate speech. Similarly, Dellapiazza et al28 found that irritability is related to avoiding-sensation behaviors, while hyperactivity/noncompliance is related to seeking-sensation behaviors and sensory-sensitivity behaviors. Atypical sensory processing also explains a significant part of the variance of problem behaviors (from 16% to 39%) after controlling age and IQ. The results indicated that children with ASD having higher levels of sensory processing difficulties were more likely to present with problem behaviors, including irritability, lethargy, stereotypic behaviors, hyperactivity, and inappropriate speech. Yet, none has considered the relationship between sensory over-responsivity and problem behaviors in adults with ASD.
Anxiety is another co-occurring condition that has been proposed as being relevant to both problem behaviors and sensory over-responsivity. According to a review regarding the comorbid psychiatric symptoms of ASD, anxiety disorders are the most detected disorders in individuals with ASD, with the rates of 5–35% generalized anxiety reported in previous studies.29 Studies have shown that individuals with ASD who have higher levels of anxiety symptoms will also experience greater levels of difficulty with over-responsivity.18,19,21,30 However, the reviewed studies were limited because they (a) examined in children or adolescents with ASD but not in adults, and (b) used different measurements for anxiety which may cover several types of anxiety disorders, such as generalized anxiety, separation anxiety, or social anxiety. Compared to children with ASD who reported lower scores on anxiety, children with ASD with more severe anxiety and mood problems had more aggressive behaviors.31 Storch et al32 found that children and adolescents with ASD who had co-occurring behavior problems experienced higher levels of anxiety than youth with anxiety and ASD alone. In the few studies that have been conducted, youth with ASD demonstrated higher levels of anxiety also have more disruptive behaviors and are more likely to use antipsychotic medication.31,32 Though clinical experiences show that individuals with ASD often exhibit both anxiety and problem behaviors, the relationship has rarely been studied in adults.
Given the high prevalence of problem behaviors, anxiety, and sensory over-responsivity, it thereby highlights the need for further research on the relationships among problem behaviors, sensory processing, and anxiety in emerging adults with ASD. Regarding the core symptoms of ASD, a change in the physical and social environments may relate to anxiety, resulting in the emergence of problem behaviors. Despite the importance of understanding the potential relationships among these factors in emerging adults with ASD, no study has addressed these issues. Thus, the present study aimed to explore the relationships between sensory over-responsivity, problem behaviors, and anxiety in emerging adults with ASD. We, therefore, tested the following hypotheses: (1) Sensation sensitivity and sensation avoiding are associated with problem behaviors in emerging adults with ASD, (2) sensation sensitivity and sensation avoiding are associated with anxiety, and (3) anxiety is associated with problem behaviors.
Materials and Methods
Ethics Statement
The study protocol has been proved by the Institutional Review Board of National Cheng Kung University Hospital (B-ER-107-076) and followed the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects.
Participants
Fifty-seven adults with ASD (46 males/11 females) aged between 18 and 25 enrolled in the present study, giving a mean age of 21.4 years. All participants reported that they were diagnosed with ASD by a registered psychiatrist according to the Diagnostic and Statistical Manual V (DSM-5) criteria.1 The severity levels the psychiatrist assigns depend on the severity of the symptoms and the levels of support. A diagnosis on the autism spectrum was confirmed with a disability identification card. The disability identification card was issued by a health and welfare agency of the Taiwanese government after processes of evaluation and assessment by the committee composed of professionals from medicine, social work, special education and employment counseling. Participants with moderate and severe intellectual disability were excluded. Nine participants had an intelligence quotient between 53 and 69 (mild intellectual disability), three participants had an intelligence quotient between 73 and 85 (borderline intellectual functioning), and 45 participants had an intelligence quotient between 86 and 150. Table 1 provides sample characteristics of the participants with ASD.
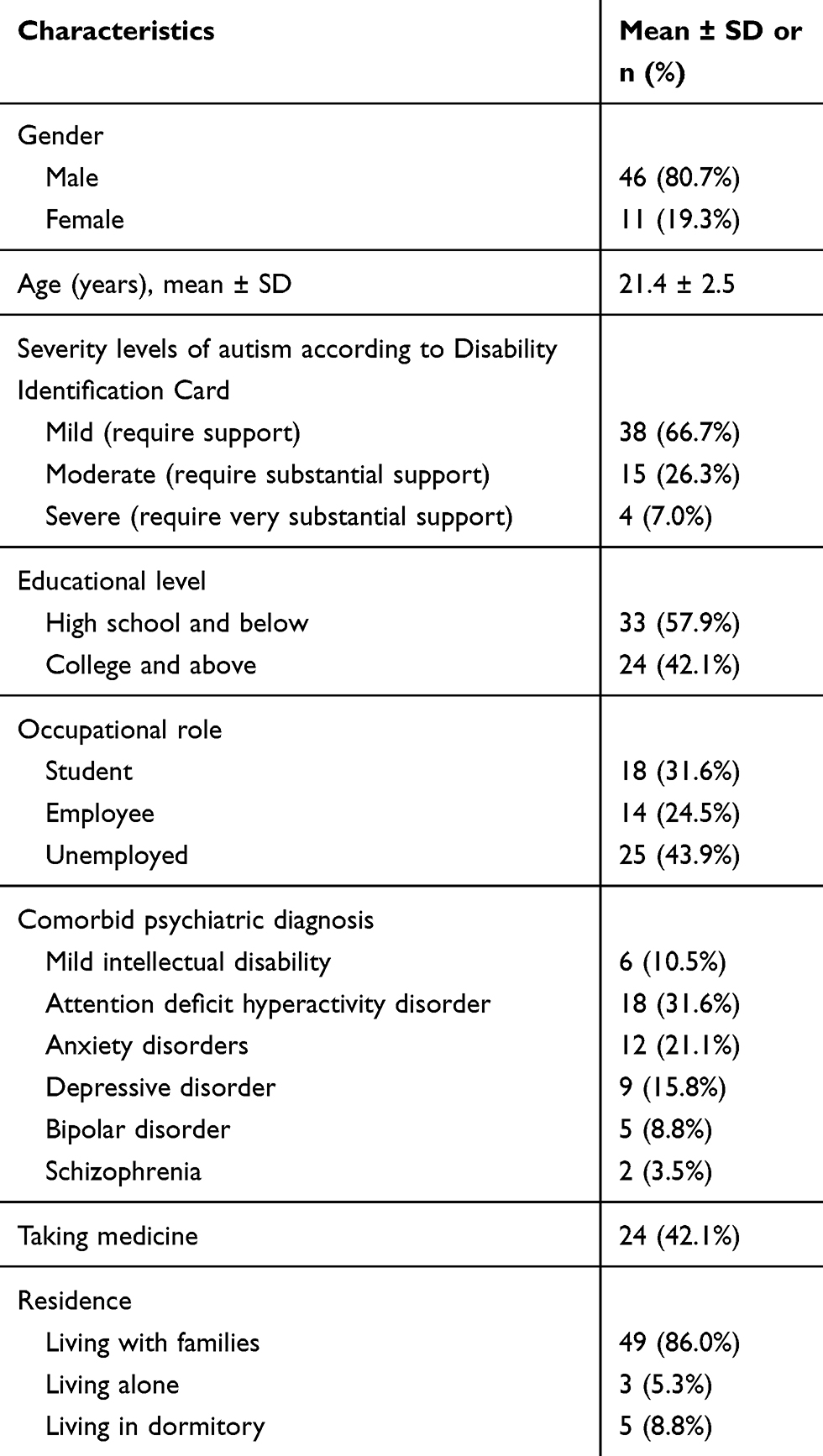 |
Table 1 Sample Characteristics (n = 57) |
Measurements
Demographic Information
Caregivers of participants with ASD provided background information, including age, gender, medical history (eg, diagnosis, comorbid psychiatric conditions, psychiatric medication, disability identification card), residential living, access to spoken language (formulate echolalia, words, phrases, sentences), the intellectual quotient, educational level, occupational status.
Adult Sensory Profile – Chinese Version (ASP)
The ASP is a 60-item questionnaire, which assesses behavior response to sensory processing experience in everyday life.33 The scale is designed for adolescents and adults aged 11 to 65 years. The questionnaire is based on Dunn’s sensory processing theory, which addresses neurological thresholds and behavioral responses. The scale consists of four quadrants: sensation sensitivity (shows over-response reactions with sensation but does not actively avoid them), sensation avoiding (engages in behaviors of avoidance or reduces everyday sensory events), low registration (fails to notice sensory stimuli and may act indifferent to the surroundings), and sensation seeking (actively seeks or craves sensory stimuli). The scale uses a 5-point scale to rate the frequency of the sensory experience, ranging from 1 (“almost never”) to 5 (“almost always”), leading to a total score for each quadrant of 15 to 75; higher scores indicate a higher frequency of certain sensory processing patterns. The study used the quadrants of sensation sensitivity and sensation avoiding. The cut-off scores that are similar to most people in the two quadrants are sensation sensitivity (31–45) and sensation avoiding (33–47) based on the Taiwanese norms of the test.34 Scores above the cut-off scores would be categorized as more than most people. The internal consistency of the four quadrants is between 0.71 and 0.80, indicating acceptable internal consistency of the Chinese version of the ASP.34 Alpha reliability was 0.93 for the sample in the present study, indicating an excellent internal consistency.
The Problem Behavior Scale of Scales of Independent Behavior – Revised (SIB-R)
The SIB-R evaluates the level of functioning in main behavior areas across settings, such as the home, school, workplace, and community.35 The scale contains 14 areas of adaptive behavior and eight areas of problem behavior. To fit the study purpose, the present study used only the problem behavior scale to measure the frequency and severity of participants’ problem behavior over 6 months. The scale consists of eight problem behaviors, which are divided into three domains: internalizing (eg, self-injury, stereotyped, withdrawn), externalizing (eg, disruptive, destructive, hurts others), and asocial (eg, socially offensive, uncooperative). The SIB-R uses a scale of 1 to 5 to determine the level of severity of the problem behaviors, ranging from 1 (“not a problem”) to 5 (“a critical problem”). The frequency of problem behaviors was assessed using a 5-point scale, ranging from 1 (“never”) to 5 (“1 or more times an hour”). The raw scores were converted into standard scores and maladaptive index scores. Standard scores with a mean of 100 and a standard deviation of 15 were utilized; higher scores imply a more severe problem behavior.35 The Taiwanese version of the SIB-R shows a good test–retest reliability (Cronbach’s alpha = 0.70), compared to the test–retest reliability of the English version, which is 0.80.35,36 Alpha reliability was 0.79 for the sample in the present study, indicating an acceptable internal consistency.
Generalized Anxiety Disorder-7 – Chinese Version (GAD-7)
The GAD-7 measures the frequency of seven symptoms of anxiety by asking participants to rate how often they have been bothered by the symptoms in the last 2 weeks on a 4-point scale ranging from 0 (“not at all”) to 3 (“nearly every day”).37 The higher the sum score of the scale, the higher the level of anxiety. On the Taiwanese version of GAD-7, a cut-off score of 9 is used to determine a possible clinically significant condition of anxiety. The Chinese version of GAD-7 shows good reliability (Cronbach’s alpha = 0.89).38 Alpha reliability was 0.95 for the sample in the present study, indicating an excellent internal consistency.
Procedure
The principal investigator contacted and posted the advertisement via Facebook Groups, Foundations or Associations for Individuals with ASD, Resource Classrooms of Universities, and the hospitals. Data were collected using printed questionnaires and Google Online Forms. A written consent information was presented to the participants before they begin the questionnaires. After the participants have read the consent information and agree to participate, they filled in the informed consent online. Then, they would be directed to the research questionnaires. The participants who have voluntarily agreed to participate in this study were asked to complete the demographic information, the problem behavior scale of the ASP, the SIB-R, and the GAD-7. Completing the questionnaires took approximately 20 to 25 minutes on average.
Data Analysis
Data were analyzed using the IBM SPSS 22.0, with two-tailed p < 0.05 to identify statistically significant coefficients. Descriptive statistics were examined to ensure the basic properties of the demographic data. Pearson correlations were used to clarify the relationships between the outcome variables. Multivariate regression analysis was computed to identify significant relationships among all variables.
Results
Table 2 shows the scores for the sensory over-responsivity, problem behaviors, and anxiety levels of the participants. The mean scores (standard deviation [SD]) of the two sensory quadrants were sensation sensitivity = 41.4 (9.8) and sensation avoiding = 42.1 (11.8), which were similar to most people from a large normative sample of the sensory quadrants. The percentage of those who scored more than most people in the two quadrants were sensation sensitivity = 33.3% (n = 19) and sensation avoiding = 26.3% (n = 15). The mean scores for the problem behavior scale and three subscales were as follows: overall problem behaviors = 104.3 (SD = 9.4, range = 96–145); internalizing behaviors = 107.5 (SD = 11.1, range = 96–135); externalizing behaviors = 94.3 (SD = 7.5, range = 90–133); and asocial behaviors = 102.4 (SD = 11.2, range = 92–131). Analyses were also made using a cut-off value of 100. Approximately 57.9%, 66.7%, 27.5%, and 50.9% of participants scored above 100 for overall problem behaviors, internalizing behaviors, externalizing behaviors, and asocial behaviors, respectively. Regarding the types of problem behaviors experienced, 28.1% had no specific problem behaviors, 24.6% had at least one type, 31.6% had at least two types, and 15.8% had all three specific types. The mean score of the GAD-7 was 8.9 (6.7), and approximately 64.9% (n = 37) of the participants scored on or above the cut-off score of 6 on the GAD-7.
 |
Table 2 Scores of Problem Behaviors, Sensory Over-Responsivity, and Anxiety (n = 57) |
Table 3 presents the Pearson correlation coefficients between the two sensory quadrants and problem behaviors. Sensation sensitivity was found to correlate significantly with sensation avoiding (r = 0.737, p < 0.001), overall problem behaviors (r = 0.380, p = 0.004), internalizing behaviors (r = 0.360, p = 0.006), and asocial behaviors (r = 0.390, p = 0.003). Sensation avoiding was found to significantly correlate with overall problem behaviors (r = 0.356, p = 0.007), externalizing behaviors (r = 0.270, p = 0.042), and asocial behaviors (r = 0.366, p = 0.005). Given that higher sensory quadrants scores indicate greater levels of difficulty with over-responsivity, this positive correlation supported our first hypothesis.
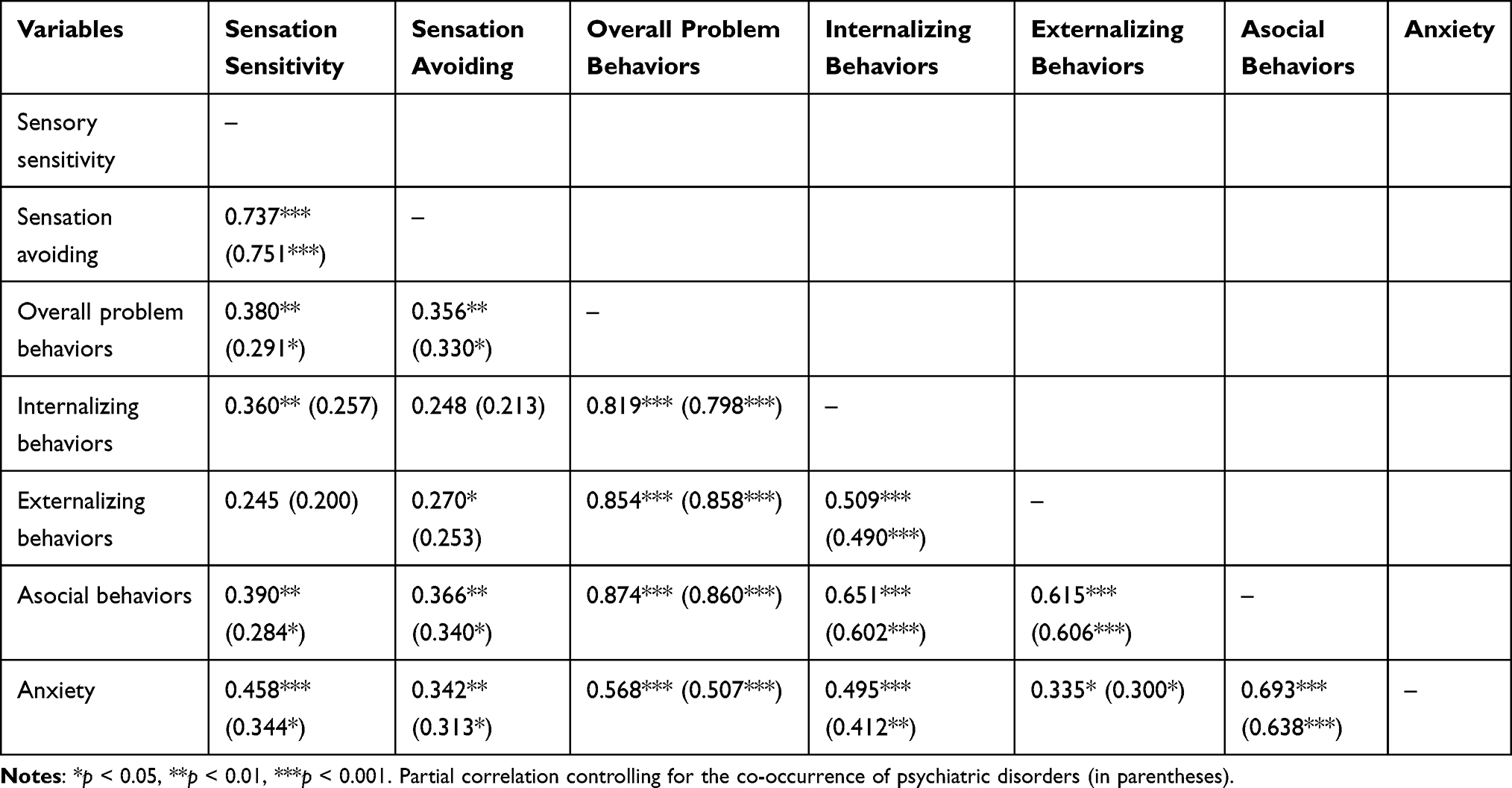 |
Table 3 Intercorrelations of Sensory Over-Responsivity, Problem Behaviors, and Anxiety (n = 57) |
Pearson’s correlations were conducted to investigate the relationship between the two sensory quadrants and anxiety. Anxiety was found to robustly and significantly correlate with sensation sensitivity (r = 0.458, p < 0.001) and sensation avoiding (r = 0.342, p = 0.009), suggesting that participants experienced greater anxiety when they more frequently reported being overwhelmed by sensation. Table 3 also presents the results of Pearson’s correlations to examine the relationship between anxiety and problem behaviors. Anxiety was found to be significantly associated with the overall problem behaviors (r = 0.568, p < 0.001), internalizing behaviors (r = 0.495, p < 0.001), externalizing symptoms (r = 0.335, p = 0.011), and asocial behaviors (r = 0.693, p < 0.001). The result indicates that the higher the level of reported anxiety, the greater the frequency of problem behaviors.
Partial correlation analysis was employed to detect possible effects of the co-occurrence of psychiatric disorders on the relationship between sensory quadrants, problem behaviors, and anxiety. The correlations between the sensation sensitivity, sensation avoiding, the overall problem behaviors, and anxiety remained significant after partialling the effects of psychopathological co-occurrence (Table 3).
The method outlined by Hayes39 was followed to examine whether anxiety was a mediating variable that accounts for the relationship between sensation avoiding and problem behaviors. This hypothesis was tested by a series of regression analyses. Sensation avoiding was significantly associated with problem behaviors and anxiety (Table 3). After controlling the relation between the problem behaviors and anxiety, the significant relationship between sensation avoiding and problem behaviors was reduced or became nonsignificant. A mediation effect would be supported. Figure 1 shows that anxiety was a mediator that accounts for the relationship between sensation avoiding and problem behaviors. Analyses using Sobel’s test40 indicated that the mediation effect was supported. This figure indicates that the greater problem behaviors in participants with greater sensation avoiding were mediating by their higher level of anxiety. A similar result was obtained in sensation sensitivity with a significant Sobel’s test (z = 2.896, p = 0.038). Table 4 presents the results of mediating effect.
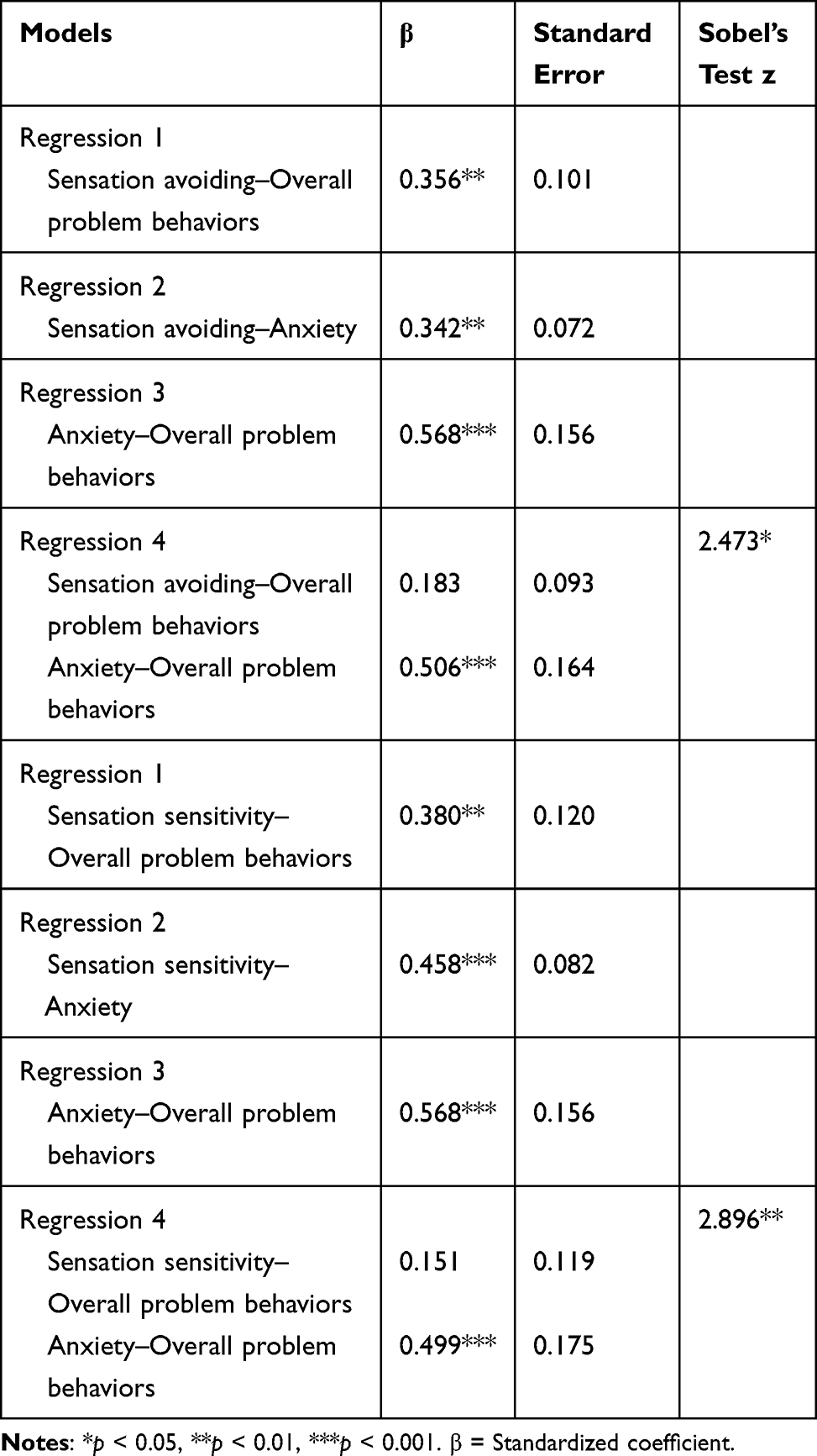 |
Table 4 Analysis Results of Mediation Effect |
 |
Figure 1 Results of testing for mediation by anxiety on relationship between sensation avoiding and problem behaviors. |
Discussion
Sensory processing difficulty is a prevalent condition in adults with ASD, but its association with their psychological well-being and behaviors has not been well explored. While previous studies have suggested some associations between sensory over-responsivity, problem behaviors, and anxiety, the present study is the first to use a cross-sectional design to examine all three conditions in Taiwanese emerging adults with ASD. The current study adds to the existing literature of adults with ASD by exploring the relationship between these two common conditions with problem behaviors. This research provides the following three findings: (1) sensation sensitivity and sensation avoiding are associated with problem behaviors in emerging adults with ASD; (2) sensation sensitivity and sensation avoiding are associated with anxiety; and (3) anxiety is associated with problem behaviors.
One of the core ASD symptoms includes a range of symptoms potentially related to sensory processing difficulties.1 In this sample, more than 25% of participants scored more than most people in the sensation sensitivity and sensation avoiding quadrants. This result is consistent with those of a study by Clince et al.22 Consistent with previous studies, emerging adults with ASD who exhibit more severe overall problem behaviors also have more exaggerated responses to sensory stimuli.41,42 Atypical sensory processing is a strong predictor of self-injury behaviors within a large ASD sample during childhood and adolescence.42 Our findings support the results of another study that used caregiver-reported data of high-functioning autism and found that the presence of stereotyped behaviors, a type of internalizing behavior, correlated with sensory processing issues.41 Our findings were also in line with those of Tseng et al26 who showed that a significant correlation exists between sensation sensitivity and internalizing behaviors and between sensation avoiding and externalizing behaviors. Furthermore, our findings extend the findings from preschool children to emerging adults with ASD.
Consistent with our hypotheses, individuals with problem behaviors evidenced higher levels of both sensory over-responsivity and anxiety. Consistent with prior studies,18,21 this study found that sensation sensitivity, sensation avoiding, and anxiety are highly correlated, suggesting that adults with ASD who have higher levels of anxiety more frequently respond to sensory inputs with exaggerating response. In line with the studies of Kim et al32 and Storch et al31 the results of this study show that individuals with ASD having higher levels of anxiety present greater and more frequent problem behaviors, including internalizing, externalizing, and asocial behaviors. Little attention has been given to the presence of problem behaviors within the context of anxiety among individuals with ASD. Nevertheless, the data support that clinicians should concern clients’ comorbid anxiety symptoms which may be related to their problem behaviors; however, more research is needed to support this relationship.
Notably, significant relationships were found between asocial behaviors and sensory over-responsivity as well as anxiety. Miller et al43 indicated that children who are sensation avoiding may present with asocial behaviors. Kring et al44 reported that adolescents and adults with ASD having a co-morbid psychiatric disorder (eg, schizophrenia, bipolar disorder, major depression, anxiety disorder, or obsessive-compulsive disorder) are more likely to have higher levels of asocial behaviors. However, no existing studies have been undertaken to determine the relationships between asocial behaviors and sensory over-responsivity or anxiety directly. Future longitudinal studies with more representative samples are needed to fully address these issues.
The study examined the bivariate relationships among the three conditions of interest. It is critical to consider the impacts of problem behaviors for emerging adults with ASD, who also have problems regulating their response to sensory inputs and emotions. The results of this study provide insights into the associations among sensory over-responsivity, problem behaviors, and anxiety in emerging adults with ASD. The lack of strategies for dealing with sensory over-responsivity could also affect their emotional status and may lead to them exhibiting more severe problem behaviors. However, these three conditions might share a reciprocal and complex relationship requiring significant investigation. With the findings of this study, unraveling the common underlying mechanisms is needed.
The present study has some limitations. First, our samples were volunteers or people who connected to the supporting resources or service systems, which may not represent the general population of emerging adults with ASD. Another limitation was the cross-sectional design. Despite the preliminary findings we provided regarding the associations between sensory processing, anxiety, and problem behaviors in emerging adults with ASD, it is difficult to clarify the causal relationship within these variables. Third, we did not have a direct clinical diagnosis of ASD. Future research using additional measurement tools for confirming an ASD diagnosis is therefore warranted. Future studies would benefit from using different types of sampling and a larger sample size to draw more confident conclusions. Objective measurements for participants who report their conditions reliably may be more sensitive.
Conclusions
The current study is the first to examine the relationships among sensory over-responsivity, problem behaviors, and anxiety in emerging adults with ASD in Taiwan. These findings indicate that emerging adults with ASD who experience problem behaviors may also have difficulties modulating their sensory input; their sensory over-responsivity was associated with their anxiety. Sensory over-responsivity was found to be associated with greater problem behaviors indirectly through elevated levels of anxiety. Given the unique symptoms of adults with ASD, a comprehensive intervention might be required for changing the modulation of sensory inputs, emotional regulation, and problem behaviors. Directions for future research may further investigate the underlying mechanisms and form an integrated treatment for these three conditions.
Acknowledgment
Support for this study was provided by grants MOST 107-2410-H-006-091 from the Ministry of Science and Technology in Taiwan.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub; 2013.
2. Murphy CM, Wilson CE, Robertson DM, et al. Autism spectrum disorder in adults: diagnosis, management, and health services development. Neuropsychiatr Dis Treat. 2016;12:1669–1686. doi:10.2147/NDT.S65455
3. Arnett JJ. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol. 2000;55:469–480. doi:10.1037/0003-066X.55.5.469
4. Nelson LJ, Chen X. Emerging adulthood in China: the role of social and cultural factors. Soc Res Child Dev. 2007;1:86–91.
5. Kapp SK, Gantman A, Laugeson EA. Transition to adulthood for high-functioning individuals with autism spectrum disorders. In Mohammadi M-R, editor, A Comprehensive Book on Autism Spectrum Disorders. Intech. 2011;451–478. doi:10.5772/21506
6. Matson JL, Sipes M, Fodstad JC, Fitzgerald ME. Issues in the management of challenging behaviours of adults with autism spectrum disorder. CNS Drugs. 2011;25(7):597–606. doi:10.2165/11591700-000000000-00000
7. Graetz JE. Autism grows up: opportunities for adults with autism. Disabil Soc. 2010;25(1):33–47. doi:10.1080/09687590903363324
8. Shattuck PT, Seltzer MM, Greenberg JS, et al. Change in autism symptoms and maladaptive behaviors in adolescents and adults with an autism spectrum disorder. J Autism Dev Disord. 2007;37(9):1735–1747. doi:10.1007/s10803-006-0307-7
9. Bauminger N, Solomon M, Rogers SJ. Externalizing and internalizing behaviors in ASD. Autism Res. 2010;3(3):101–112. doi:10.1002/aur.131
10. Walsh CE, Mulder E, Tudor ME. Predictors of parent stress in a sample of children with ASD: pain, problem behavior, and parental coping. Res Autism Spectr Disord. 2012;7:256–264. doi:10.1016/j.rasd.2012.08.010
11. Reef J, Diamantopoulou S, van Neurs I, et al. Predicting adult emotional and behavior problems from externalizing problem trajectories in a 24-year longitudinal study. Eur Child Adolesc Psychiatry. 2010;19:577–585. doi:10.1007/s00787-010-0088-6
12. Gray K, Keating C, Taffe J, Brereton A, Einfeld S, Tonge B. Trajectory of behavior and emotional problems in autism. Am J Intellect Dev Disabil. 2012;117(2):121–133. doi:10.1352/1944-7588-117-2.121
13. Woodman AC, Mailick MR, Greenberg JS. Trajectories of internalizing and externalizing symptoms among adults with autism spectrum disorders. Dev Psychopathol. 2016;28:565–581. doi:10.1017/S095457941500108X
14. Taylor JL, Smith LE, Mailick MR. Engagement in vocational activities promotes behavioral development for adults with autism spectrum disorders. J Autism Dev Disord. 2014;44(6):1447–1460. doi:10.1007/s10803-013-2010-9
15. Dieleman LM, DePauw SSW, Soenens B, Mabbe E, Campbell R, Prinzie P. Relations between problem behaviors, perceived symptom severity and parenting in adolescents and emerging adults with ASD: the mediating role of parental psychological need frustration. Res Dev Disabil. 2018;73:21–30. doi:10.1016/j.ridd.2017.12.012
16. Dunn W. The impact of sensory processing abilities on the daily lives of young children and their families: a conceptual model. Infant Young Child. 1997;9:23–35. doi:10.1097/00001163-199704000-00005
17. Ben-Sasson A, Hen L, Fluss R, et al. A meta-analysis of sensory modulation symptoms in individuals with autism spectrum disorders. J Autism Dev Disord. 2009;39(1):1–11. doi:10.1007/s10803-008-0593-3
18. Pfeiffer B, Kinnealey M, Reed C, et al. Sensory modulation and affective disorders in children and adolescents with asperger’s disorder. Am J Occup Ther. 2005;59(3):335–345. doi:10.5014/ajot.59.3.335
19. Mazurek MO, Petroski GF. Sleep problems in children with autism spectrum disorder: examining the contributions of sensory over-responsivity and anxiety. Sleep Med. 2015;16(2):270–279. doi:10.1016/j.sleep.2014.11.006
20. Nieto C, Lopez B, Gandia H. Relationships between atypical sensory processing patterns, maladaptive behaviour and maternal stress in Spanish children with autism spectrum disorder. J Intellect Disabil Res. 2017;61:1140–1150. doi:10.1111/jir.12435
21. Mazurek MO, Vasa RA, Kalb LG, et al. Anxiety, sensory over-responsivity, and gastrointestinal problems in children with autism spectrum disorders. J Abnorm Child Psychol. 2013;41(1):165–176. doi:10.1007/s10802-012-9668-x
22. Clince M, Connolly L, Nolan C. Comparing and exploring the sensory processing patterns of higher education students with attention deficit hyperactivity disorder and autism spectrum disorder. Am J Occup Ther. 2016;70(2):1–9. doi:10.5014/ajot.2016.016816
23. Robertson AE, Simmons DR. The sensory experiences of adults with autism spectrum disorder: a qualitative analysis. Perception. 2015;44(5):569–586. doi:10.1068/p7833
24. Tavassoli T, Miller LJ, Schoen SA, et al. Sensory over-responsivity in adults with autism spectrum conditions. Autism. 2014;18(4):428–432. doi:10.1177/1362361313477246
25. Green SA, Ben-Sasson A, Soto TW, et al. Anxiety and sensory over-responsivity in toddlers with autism spectrum disorders: bidirectional effects across time. J Autism Dev Disord. 2012;42(6):1112–1119. doi:10.1007/s10803-011-1361-3
26. Tseng M-H, Fu C-P, Cermak SA, et al. Emotional and behavioral problems in preschool children with autism: relationship with sensory processing dysfunction. Res Autism Spectr Disord. 2011;5(4):1441–1450. doi:10.1016/j.rasd.2011.02.004
27. O’Donnell S, Deitz J, Kartin D, et al. Sensory processing, problem behavior, adaptive behavior, and cognition in preschool children with autism spectrum disorders. Am J Occup Ther. 2012;66(5):586–594. doi:10.5014/ajot.2012.004168
28. Dellapiazza F, Michelon C, Oreve M-J, et al. The impact of atypical sensory processing on adaptive functioning and maladaptive behaviors in autism spectrum disorder during childhood: results from the ELENA cohort. J Autism Dev Disord. 2019;49:1–11. doi:10.1007/s10803-018-3679-6
29. Skokauskas N, Gallagher L. Psychosis, affective disorders and anxiety in autistic spectrum disorder: prevalence and nosological considerations. Psychopathology. 2009;43(1):8–16. doi:10.1159/000255958
30. Bitsika V, Sharpley CF, Mills R. How are sensory features associated with seven anxiety disorders in boys with autism spectrum disorder? Int J Dev Neurosci. 2016;50(1):47–54. doi:10.1016/j.ijdevneu.2016.03.005
31. Storch EA, Arnold EB, Jones AM, et al. The role of co-occurring disruptive behavior in the clinical presentation of children and adolescents with anxiety in the context of autism spectrum disorders. Child Psychiatry Hum Dev. 2012;43:734–746. doi:10.1007/s10578-012-0294-1
32. Kim JA, Szatmari P, Bryson SE, et al. The prevalence of anxiety and mood problems among children with autism and asperger syndrome. Autism. 2000;4(2):117–132. doi:10.1177/1362361300004002002
33. Brown C, Dunn W. Adolescent-Adult Sensory Profile. Tucson, AZ: Therapy Skill Builders; 2002.
34. Tseng MH, Chen WS. Chinese Version of Adolescent-Adult Sensory Profile. Taipei: Chinese Behavioral Science Corporation; 2009.
35. Bruininks RH, Woodcock RW, Weatherman RF, et al. Scales of Independent Behavior – Revised. Itasca, II: Riverside Publishing; 1996.
36. Lin LY Families of adolescents and adults with autism spectrum disorders in Taiwan (Unpublished doctoral dissertation). Boston University, USA, 2008.
37. Spitzer RL, Kroenke K, Williams JBW, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
38. Tong X, An D, McGonigal A, et al. Validation of the Generalized Anxiety Disorder-7 (GAD-7) among Chinese people with epilepsy. Epilepsy Res. 2016;120:1–36. doi:10.1016/j.eplepsyres.2015.11.019
39. Hayes AF. PROCESS: a versatile computational tool for observed variable mediation, moderation, and conditional process modeling. [White paper]; 2012. Retrieved from http://www.afhayes.com/public/process2012.pdf.
40. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36(4):717–731. doi:10.3758/BF03206553
41. Boyd BA, McBee M, Holtzclaw T, et al. Relationships among repetitive behaviors, sensory features, and executive functions in high functioning autism. Res Autism Spectr Disord. 2009;3(4):959–966. doi:10.1016/j.rasd.2009.05.003
42. Duerden EG, Oatley HK, Mak-Fan KM, et al. Risk factors associated with self-injurious behaviors in children and adolescents with autism spectrum disorders. J Autism Dev Disord. 2012;42(11):2460–2470. doi:10.1007/s10803-012-1497-9
43. Miller LJ, Anzalone ME, Lane SJ, et al. Concept evolution in sensory integration: a proposed nosology for diagnosis. Am J Occup Ther. 2007;61(2):135–140. doi:10.5014/ajot.61.2.135
44. Kring SR, Greenberg JS, Seltzer MM. Adolescents and adults with autism with and without co-morbid psychiatric disorders: differences in maternal well-being. J Ment Health Res Intellect Disabil. 2008;1(2):53–74. doi:10.1080/19315860801988228
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.