Back to Journals » Clinical Ophthalmology » Volume 17
Refractive Predictability of a Swept Source Optical Coherence Tomography Biometer in Long and Short Eyes Implanted with Extended Depth of Focus Intraocular Lenses
Received 14 July 2023
Accepted for publication 31 October 2023
Published 21 November 2023 Volume 2023:17 Pages 3525—3530
DOI https://doi.org/10.2147/OPTH.S430535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Clayton Blehm,1 Brad Hall2
1Gainesville Eye Associates, Gainesville, GA, USA; 2Sengi, Penniac, NB, Canada
Correspondence: Clayton Blehm, Gainesville Eye Associates, 2061 Beverly Road, Gainesville, GA, 30501, USA, Tel +1 770-532-4444, Email [email protected]
Purpose: To determine the refractive predictability of Argos (Movu, a Santec company) measurements and the Barrett Universal II formula in long and short eyes implanted with an extended depth of focus (EDOF) intraocular lens (IOL).
Methods: This retrospective, non-interventional study included 86 eyes (55 long and 31 short) of 55 patients. Preoperative biometry was performed using the Argos. Preoperative IOL power formulas were the preprogrammed Barrett Universal II (BUII). Data were collected for refractive outcomes, postoperative prediction error (directional and absolute), and monocular corrected distance visual acuity (CDVA, Snellen).
Results: The mean absolute prediction error for BUII was 0.27 ± 0.26 D overall, 0.24 ± 0.20 D in long eyes, and 0.33 ± 0.33 D in short eyes. Overall, the percentage of eyes with ≤ 0.5 D prediction error was 84% for BUII. In long eyes, the percentage of eyes with ≤ 0.5 D prediction error was 90% for BUII. In short eyes, the percentage of eyes with ≤ 0.5 D prediction error was 74% for BUII. The percentage of eyes with ≤ 0.5 D of MRSE was 89% for long eyes and 94% for short eyes. Visual acuities were excellent in both long and short eyes, with > 90% of eyes 20/25 or better in each group.
Conclusion: The prediction error of Argos using BUII was low in long and short eyes at one month after EDOF IOL implantation.
Plain Language Summary: An intraocular lens (IOL) is an artificial lens that can be implanted in the eye to replace a natural lens that has become opaque. The power of the IOL must be carefully chosen for clear vision after implantation. Cataract surgeons use devices called biometers to measure the eye and calculate the most appropriate IOL power to implant. A novel biometer is available that may offer good accuracy, for predicting the IOL power, in eyes that are longer or shorter than average. The purpose of this study was to determine the refractive predictability of this biometer in long and short eyes implanted with an extended depth of focus (EDOF) IOL. The results of this study suggest that the refractive predictability was excellent in long and short eyes at one month after EDOF IOL implantation, resulting in great vision postoperatively.
Keywords: Argos, biometry, SS-OCT
Introduction
The success of cataract surgery and intraocular lens (IOL) implantation can be measured by the postoperative refractive outcomes. Both patients and surgeons have high expectations for clear vision after surgery, and good refractive outcomes are key for clear vision. This is especially true with presbyopia-correcting lenses such as trifocals or extended depth of focus (EDOF) IOLs.1
Hitting the refractive target is influenced by accurate and precise preoperative measurements of the eye. Optical biometry is the standard of care to determine anterior chamber depth (ACD), axial length (AL), and keratometry (K). Currently available optical biometers include those based on partial coherence interferometry (PCI),2 optical low coherence reflectometry (OLCR),3 optical low coherence interferometry (OLCI),4 and swept-source optical coherence tomography (SS-OCT).5,6
Refractive accuracy is also influenced by the IOL power formula used. Many optical biometers are available preprogrammed with the latest generation IOL power formulas, and these newer IOL formulas are reported to result in excellent refractive outcomes.7–9 However, it can still be challenging to achieve the refractive target in eyes with long (≥ 24.5 mm) or short (≤ 22.5 mm) axial lengths.
The Argos (Movu, a Santec company) is an SS-OCT biometer that measures the eye utilizing a wavelength of 1060 nm.10 Rather than using one refractive index for the entire eye, the Argos uses refractive indices of 1.376 for the cornea, 1.410 for the lens, and 1.336 for the aqueous and vitreous, and a sum of these segments to determine the axial length.11,12 This allows for adjustments to the axial length calculation based on variability in the lengths of each segment. This sum-of-segments approach has been reported to result in excellent refractive outcomes compared to using a single refractive index.13–15 In addition, Shammas et al12 observed good refractive outcomes with the Argos in long and short eyes with a monofocal IOL. However, to date, there is minimal data on the refractive and visual outcomes of the Argos in long and short eyes with presbyopia correcting IOLs.
The purpose of this study was to determine the refractive predictability of Argos measurements in long and short eyes implanted with an EDOF IOL.
Methods
This was a non-interventional retrospective chart review of visual and refractive outcomes in long (≥ 24.5 mm) and short (≤ 22.5 mm) eyes using an SS-OCT biometer (Argos). An institutional review board reviewed the study (Salus IRB; approval CB-22-001). The IRB granted a waiver of informed consent as this was a non-interventional retrospective chart review of anonymized data. All data were maintained with confidentiality. This study followed the tenets of the Declaration of Helsinki, International Harmonization (ICH) guidelines, and Good Clinical Practice (GCP). There was no requirement to register this study in a clinical trials database (such as clinicaltrials.gov) as this was a retrospective chart review.
Charts were reviewed from subjects who had cataract surgery between December 2021 and January 2023. Eligible charts were those from adults who had previous uncomplicated cataract surgery with corrected distance visual acuity (CDVA) of 20/30 or better following implantation with AcrySof Vivity IOLs (Alcon Vision, LLC; toric and non-toric), and axial lengths ≤ 22.5 mm or ≥ 24.5 mm where biometry and IOL calculations were performed with the ARGOS SS-OCT device. Charts were excluded from subjects that had ocular pathology noted in patient chart, moderate-severe corneal or retinal pathology, severe dry eye disease, history of corneal refractive surgery, irregular astigmatism, or corneal astigmatism greater than 4.00 D.
Preoperative and ≥ 1 month postoperative data were collected. Visual acuities were collected in Snellen and converted to logMAR for analysis. Preoperative biometry was performed using the Argos biometer. The Barrett Universal II formula (BUII) was used with all eyes, and all eyes were targeted for plano or first minus. Using the data collected with the Argos, spherical equivalent predictions using the Barrett True Axial Length formula (BTAL) were back-calculated for exploratory analyses. Microincision phacoemulsification was performed by a single experienced surgeon (CB) in all eyes. The ORA System with Verifeye+ (Alcon Vision, LLC) was used intraoperatively, though the final implanted IOL was based on surgeon discretion. The primary endpoint was the mean absolute prediction error in long and short eyes. Secondary endpoints included the percentage of eyes within 0.50 D of predicted postoperative spherical equivalent in long and short eyes and postoperative CDVA in long and short eyes. Exploratory endpoints included median absolute prediction error in long and short eyes, mean and median absolute prediction error in long and short eyes using back-calculations with the Barrett True Axial Length formula, and the percentage of eyes within 0.50 D of predicted postoperative spherical equivalent in long and short eyes using back-calculations with the Barrett True Axial Length formula. Absolute prediction error was calculated as the absolute difference between predicted spherical equivalent and the postoperative manifest refraction spherical equivalent.
All statistical analyses were performed using the statistical software R version 4.2.2 (The R Foundation for Statistical Computing, Vienna, Austria). The study was intended to be descriptive in nature. A total sample size of 80 was considered sufficient to characterize the performance of the Argos in long and short eyes.
Results
The chart review identified 86 eyes (55 long and 31 short) of 55 patients that were eligible based on the inclusion and exclusion criteria above. Table 1 summarizes the preoperative and patient demographics.
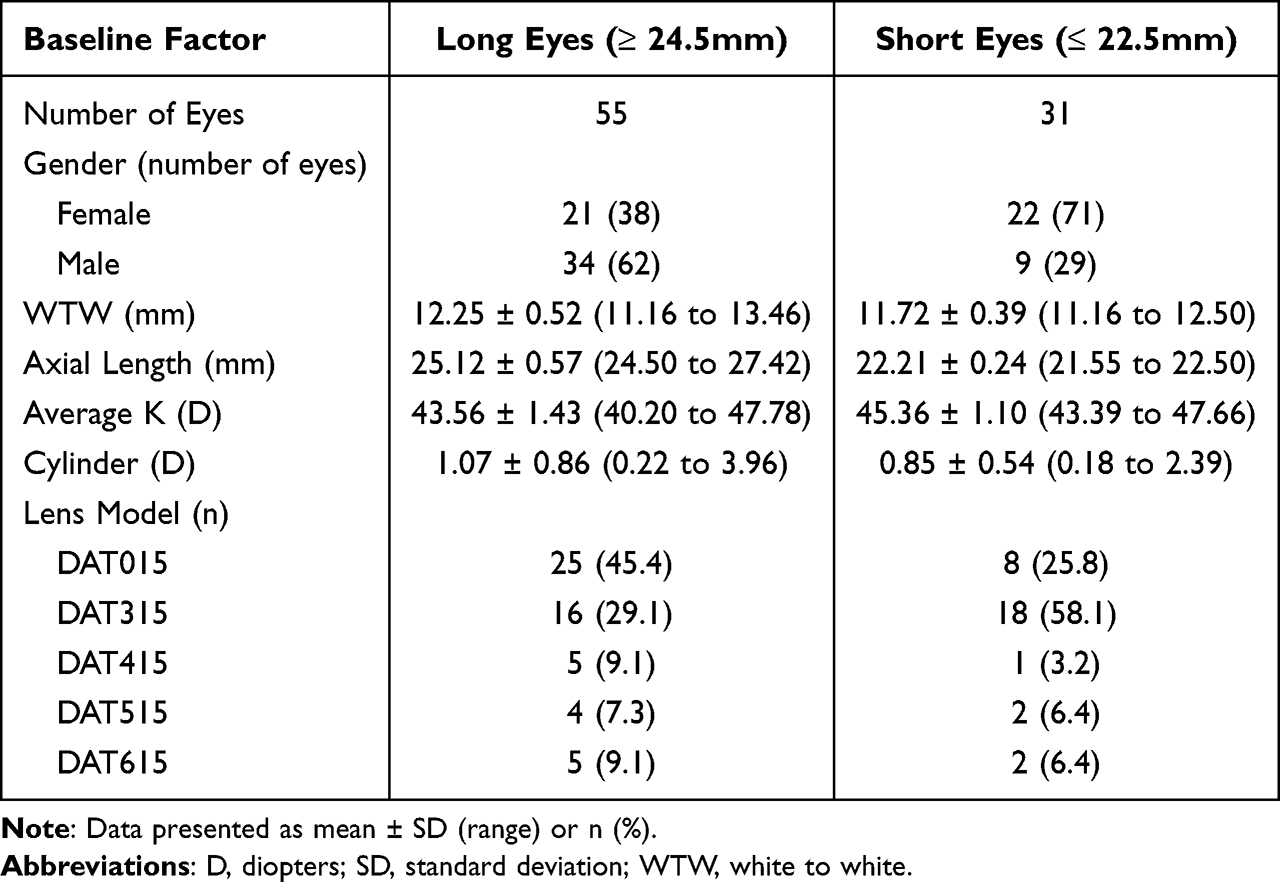 |
Table 1 Preoperative and Demographic Data |
A summary of the absolute prediction error for the BUII formula is shown in Table 2. Overall, mean absolute prediction error was 0.27 ± 0.26 D and the percentage of eyes with prediction error ≤ 0.5 D was 84%. In long eyes, mean absolute prediction error was 0.24 ± 0.20 D and the percentage of eyes with prediction error ≤ 0.5 D was 90%. In short eyes, mean absolute prediction error was 0.33 ± 0.33 D and the percentage of eyes with prediction error ≤ 0.5 D was 74%.
 |
Table 2 Absolute Prediction Error for the BUII Formula |
Table 3 summarizes the postoperative refractive outcomes using the BUII formula. The refractive outcomes were excellent in both long and short eyes. The percentage of eyes with ≤ 0.5 D of residual cylinder was 90% for long eyes and 74% for short eyes. The percentage of eyes with ≤ 0.5 D of MRSE was 89% for long eyes and 94% for short eyes.
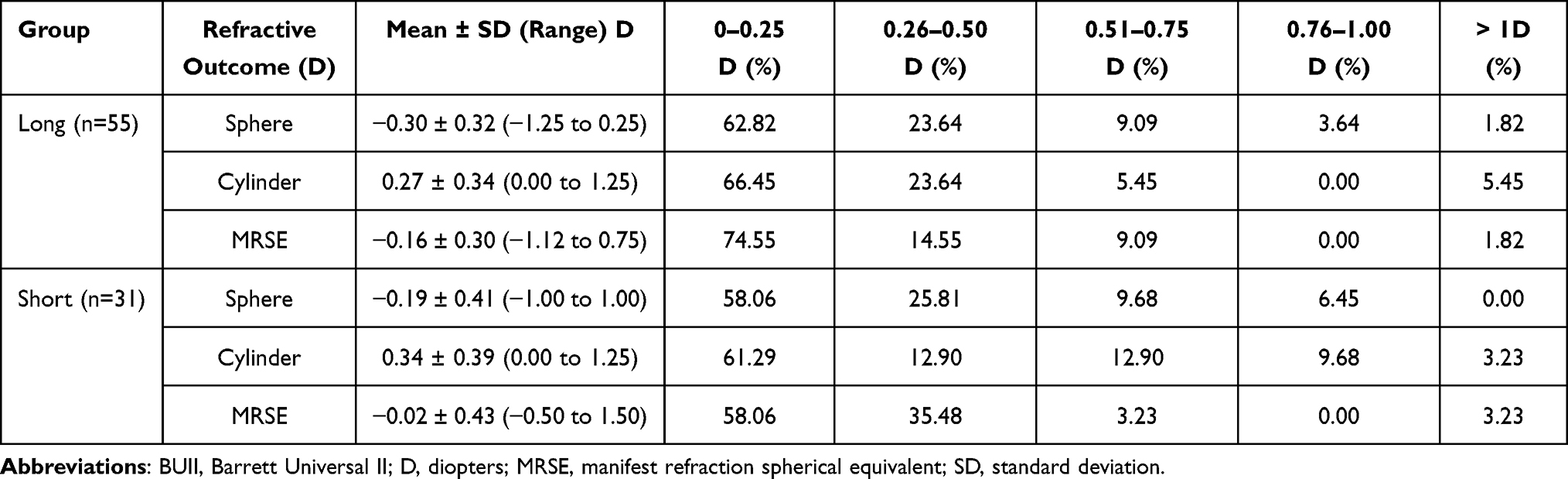 |
Table 3 Refractive Outcomes in Long (n=55) and Short Eyes (n=31) Using the BUII Formula |
Postoperative monocular CDVA for long and short eyes is summarized in Figure 1. Visual acuities were similarly excellent in both long and short eyes, with > 90% of eyes 20/25 or better in each group.
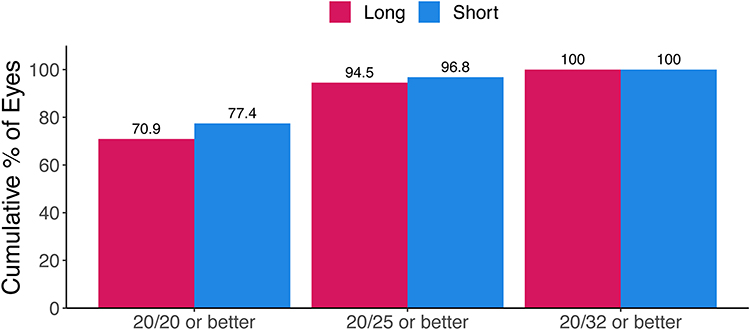 |
Figure 1 Cumulative postoperative monocular CDVA between groups. |
Absolute prediction error for the BTAL formula was back-calculated for exploratory analyses. A summary is shown in Table 4. Overall, mean absolute prediction error was 0.28 ± 0.27 D, and the percentage of eyes with prediction error ≤ 0.5 D was 85%. In long eyes, mean absolute prediction error was 0.26 ± 0.26 D, and the percentage of eyes with prediction error ≤ 0.5 D was 84%. In short eyes, mean absolute prediction error was 0.31 ± 0.28 D, and the percentage of eyes with prediction error ≤ 0.5 D was 87%.
 |
Table 4 Absolute Prediction Error for the BTAL Formula |
Discussion
Achieving the refractive target following cataract surgery is crucial for good postoperative visual outcomes. The UK National Health Service (NHS) released benchmark standards in 2009 of 55% and 85% of patients to be within 0.5 D and 1.0 D of the predicted refraction, respectively.16 It has been estimated that refractive outcomes are within 0.5 D of target refraction in only 73% of eyes.17 Refractive accuracy is influenced by the accuracy and precision of the preoperative biometry measurements, and also by the IOL power formula selected. In long eyes, missing the refractive target often leaves residual hyperopia.18,19 In short eyes, small changes in the final position of the implanted IOL can have large effects on the residual refractive error compared to average or long eyes.20 In this study, we determined the predictive accuracy of the BUII and BTAL formulas, which were available preprogrammed on the Argos biometer, in long and short eyes that were implanted with an EDOF IOL.
We used the cutoffs for long (24.50 mm) and short eyes (22.50 mm) reported by Shammas and Jabre,21 although axial lengths of exactly 22.50 and 24.50 mm were included in the short eye and long eye groups, respectively, in our study. For long eyes, the percentage of eyes with prediction error ≤ 0.5 D was 90% for BUII and 84% for BTAL. Shammas et al12 also reported on the refractive outcomes using the Argos in long and short eyes using a variety of IOL power formulas (including BUII and BTAL) after implantation with a monofocal IOL. The authors observed that the percentage of long eyes with prediction error ≤ 0.5 D was approximately 86% for BUII and 85% for BTAL (n=155). In another study, Shammas et al13 reported that the percentage of long eyes (defined as axial length ≥ 25 mm) with prediction error ≤ 0.5 D was approximately 91% using the Argos and the BUII formula (n=57). Yang et al6 observed that the percentage of long eyes (defined as axial length ≥ 26 mm) with prediction error ≤ 0.5 D was approximately 82% using the Argos and the Haigis formula (n=12). In addition, Omoto et al22 reported that the percentage of long eyes (defined as axial length ≥ 26 mm) with ≤ 0.5 D prediction error was approximately 70% using the Argos and the BUII formula (n=30). The outcomes reported in other studies are similar to those reported in our study, though the differences could be due to the differences in sample size, A-constant optimization, or surgical technique. The results of our study and other studies suggest that using the Argos with the BUII or BTAL formulas in long eyes results in excellent refractive outcomes.
For short eyes, we observed that the percentage of eyes with prediction error ≤ 0.5 D was 74% for BUII and 87% for BTAL. Shammas et al12 reported that the percentage of short eyes with prediction error ≤ 0.5 D was approximately 71% for BUII and 72% for BTAL (n=120). Yang et al6 observed that the percentage of short eyes with prediction error ≤ 0.5 D was approximately 71% using the Argos and the Haigis formula (n=12). Shammas et al13 reported that the percentage of short eyes (defined as axial length < 22 mm) with prediction error ≤ 0.5 D was approximately 72% using the Argos and the BUII formula (n=43). These reported percentages in other studies are less than those reported in our study, though the differences are likely due to differences in sample size and definition of short eyes. The results of our study and other studies suggest that using the Argos with the BUII or BTAL formulas in short eyes results in good refractive outcomes, however this remains a challenge compared to long eyes.
A limitation of this study was the sample size. The study was intended to be descriptive, and we did not power the study to be able to perform statistical comparisons between the BUII and BTAL formulas. However, our results suggest that both formulas perform well in long and short eyes. Another limitation of this study was the retrospective design. A randomized and prospective study designed to compare IOL power formulas would be better, however, given that such a study may require at least 400 eyes,12,13 a retrospective study offers significant cost and time advantages.
In conclusion, the prediction error of Argos using BUII was low in long and short eyes at one month after EDOF IOL implantation.
Acknowledgment
This paper was presented at the 2023 American Society of Cataract and Refractive Surgery (ASCRS) Annual Meeting as a conference talk with interim findings.
Funding
This study was supported with an investigator-initiated study grant (75040681) from Alcon Vision, LLC, Fort Worth, TX, USA.
Disclosure
Brad Hall reports that he has received consulting fees from Ace Vision Group outside the submitted work. The authors report no other conflict of interest for this work.
References
1. Schallhorn JM. Multifocal and extended depth of focus intraocular lenses: a comparison of data from the United States food and drug administration premarket approval trials. J Refract Surg. 2021;37(2):98–104. doi:10.3928/1081597X-20201111-02
2. Vogel A, Dick BH, Krummenauer F. Reproducibility of optical biometry using partial coherence interferometry: intraobserver and interobserver reliability. J Cataract Refract Surg. 2001;27(12):1961–1968. doi:10.1016/S0886-3350(01)01214-7
3. Hoffer KJ, Shammas JH, Savini G. Comparison of 2 laser instruments for measuring axial length. J Cataract Refract Surg. 2010;36(4):644–648. doi:10.1016/j.jcrs.2009.11.007
4. Hoffer KJ, Shammas HJ, Savini G, Huang J. Multicenter study of optical low-coherence interferometry and partial-coherence interferometry optical biometers with patients from the United States and China. J Cataract Refract Surg. 2016;42(1):62–67. doi:10.1016/j.jcrs.2015.07.041
5. Montes-Mico R, Pastor-Pascual F, Ruiz-Mesa R, Tana-Rivero P. Ocular biometry with swept-source optical coherence tomography. J Cataract Refract Surg. 2021;47(6):802–814. doi:10.1097/j.jcrs.0000000000000551
6. Yang CM, Lim DH, Kim HJ, Chung TY. Comparison of two swept-source optical coherence tomography biometers and a partial coherence interferometer. PLoS One. 2019;14(10):e0223114. doi:10.1371/journal.pone.0223114
7. Barrett GD. An improved universal theoretical formula for intraocular lens power prediction. J Cataract Refract Surg. 1993;19(6):713–720. doi:10.1016/S0886-3350(13)80339-2
8. Cheng H, Kane JX, Liu L, Li J, Cheng B, Wu M. Refractive predictability using the IOLMaster 700 and Artificial Intelligence-based IOL power formulas compared to standard formulas. J Refract Surg. 2020;36(7):466–472. doi:10.3928/1081597X-20200514-02
9. Melendez RF, Smits G, Nguyen T, Ruffaner-Hanson CD, Ortiz D, Hall B. Comparison of astigmatism prediction accuracy for toric lens implantation from two swept-source optical coherence tomography devices. Clinical Ophthalmology. 2022;16:3795–3802. doi:10.2147/OPTH.S378019
10. Shammas HJ, Ortiz S, Shammas MC, Kim SH, Chong C. Biometry measurements using a new large-coherence-length swept-source optical coherence tomographer. J Cataract Refract Surg. 2016;42(1):50–61. doi:10.1016/j.jcrs.2015.07.042
11. Wang Q, Chen M, Ning R, et al. The precision of a new anterior segment optical coherence tomographer and its comparison with a swept-source OCT-based optical biometer in patients with cataract. J Refract Surg. 2021;37(9):616–622. doi:10.3928/1081597X-20210610-02
12. Shammas HJ, Taroni L, Pellegrini M, Shammas MC, Jivrajka RV. Accuracy of newer IOL power formulas in short and long eyes using sum-of-segments biometry. J Cataract Refract Surg. 2022;48(10):1113–1120. doi:10.1097/j.jcrs.0000000000000958
13. Shammas HJ, Shammas MC, Jivrajka RV, Cooke DL, Potvin R. Effects on IOL power calculation and expected clinical outcomes of axial length measurements based on multiple vs single refractive indices. Clin Ophthalmol. 2020;14:1511–1519. doi:10.2147/OPTH.S256851
14. Wang L, Cao D, Weikert MP, Koch DD. Calculation of axial length using a single group refractive index versus using different refractive indices for each ocular segment: theoretical study and refractive outcomes. Ophthalmology. 2019;126(5):663–670. doi:10.1016/j.ophtha.2018.12.046
15. Cooke DL, Cooke TL. Approximating sum-of-segments axial length from a traditional optical low-coherence reflectometry measurement. J Cataract Refract Surg. 2019;45(3):351–354. doi:10.1016/j.jcrs.2018.12.026
16. Gale RP, Saldana M, Johnston RL, Zuberbuhler B, McKibbin M. Benchmark standards for refractive outcomes after NHS cataract surgery. Eye. 2009;23(1):149–152. doi:10.1038/sj.eye.6702954
17. Lundstrom M, Dickman M, Henry Y, et al. Risk factors for refractive error after cataract surgery: analysis of 282 811 cataract extractions reported to the European Registry of Quality Outcomes for cataract and refractive surgery. J Cataract Refract Surg. 2018;44(4):447–452. doi:10.1016/j.jcrs.2018.01.031
18. Zaldivar R, Shultz MC, Davidorf JM, Holladay JT. Intraocular lens power calculations in patients with extreme myopia. J Cataract Refract Surg. 2000;26(5):668–674. doi:10.1016/S0886-3350(00)00367-9
19. Wang L, Shirayama M, Ma XJ, Kohnen T, Koch DD. Optimizing intraocular lens power calculations in eyes with axial lengths above 25.0 mm. J Cataract Refract Surg. 2011;37(11):2018–2027. doi:10.1016/j.jcrs.2011.05.042
20. Hoffer KJ, Savini G. IOL power calculation in short and long eyes. Asia Pac J Ophthalmol. 2017;6:330–331.
21. Shammas HJ, Jabre JF. Validating e-norms methodology in ophthalmic biometry. BMJ Open Ophthalmol. 2020;5(1):e000500. doi:10.1136/bmjophth-2020-000500
22. Omoto MK, Torii H, Masui S, Ayaki M, Tsubota K, Negishi K. Ocular biometry and refractive outcomes using two swept-source optical coherence tomography-based biometers with segmental or equivalent refractive indices. Sci Rep. 2019;9(1):655. doi:10.1038/s41598-019-42968-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Astigmatism Prediction Accuracy for Toric Lens Implantation from Two Swept-Source Optical Coherence Tomography Devices
Melendez RF, Smits G, Nguyen T, Ruffaner-Hanson CD, Ortiz D, Hall B
Clinical Ophthalmology 2022, 16:3795-3802
Published Date: 17 November 2022
Randomized Trial Comparing Prediction Accuracy of Two Swept Source Optical Coherence Tomography Biometers
Multack S, Plummer N, Smits G, Hall B
Clinical Ophthalmology 2023, 17:2423-2428
Published Date: 17 August 2023
A Retrospective Trial Comparing Prediction Accuracy of Three Biometers in Short, Medium, and Long Eyes
Multack S, Plummer N, Marneris A, Hall B
Clinical Ophthalmology 2025, 19:577-583
Published Date: 17 February 2025