Back to Journals » Clinical Ophthalmology » Volume 20
Refractive Outcomes of Cataract Surgery Using Zeiss Artificial Intelligence Calculator versus Barrett Universal II and Kane
Authors Cannon NT ![]() , Redden L
, Redden L ![]() , Riaz KM
, Riaz KM ![]() , Scruggs K, Pantanelli SM
, Scruggs K, Pantanelli SM ![]()
Received 17 November 2025
Accepted for publication 12 March 2026
Published 27 March 2026 Volume 2026:20 578393
DOI https://doi.org/10.2147/OPTH.S578393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Nathan T Cannon,1 Liam Redden,2 Kamran M Riaz,2 Kathleen Scruggs,1 Seth M Pantanelli1
1Department of Ophthalmology, Penn State College of Medicine, Hershey, PA, USA; 2Department of Ophthalmology, Dean McGee Eye Institute, Oklahoma City, OK, USA
Correspondence: Seth M Pantanelli, Department of Ophthalmology, Penn State College of Medicine, Hershey, PA, USA, Tel +1 717 531 5690, Email [email protected]
Purpose: To compare the performance of the Zeiss AI IOL Calculator (ZAIC) to that of Barrett Universal II (BUII) and Kane, using standard (K) and total keratometry (TK) as inputs.
Patients and Methods: This was a multicenter retrospective case series which included surgery-naïve eyes undergoing cataract surgery with preoperative optical biometry on the IOLMaster 700, monofocal IOL (Bausch & Lomb enVista MX60E) implantation, and 20/40 acuity or better measured at least 3 weeks postoperatively. After taking the difference between actual and predicted postoperative spherical equivalent (SE) for each eye, optimized outcome measures included the mean absolute error (MAE), standard deviation (SD) of the mean prediction error, root mean squared absolute error (RMSAE), median prediction error (MedAE), and proportion of eyes within 0.5 D of predicted. Statistical differences were identified using Wilcox-Holladay-Wang-Koch tests with Holm correction.
Results: A total of 246 eyes of 246 patients were analyzed. The MAE of ZAIC was significantly lower than that of BU2 TK [0.30 vs 0.32 D (p = 0.04)]. ZAIC had a lower SD and RMSAE than that of BU2 K and BU2 TK [0.38 vs 0.41 (p = 0.001) and 0.42 D (p = 0.002); 0.38 vs 0.41 (p = 0.008) and 0.42 (p = 0.008)]. ZAIC also had a larger proportion of eyes within 0.5 D of predicted compared to BU2 K [82% vs 76% (p = 0.02)], as well as a larger proportion of eyes within 0.75 D of predicted compared to BU2 TK [95% vs 91% (p = 0.02)]. There were no significant differences in MedAE or the proportion of eyes within 0.25 or 1 D of predicted.
Conclusion: Compared to BU2, ZAIC produces a lower MAE, SD, and RMSAE, and a higher proportion of eyes within 0.5 and 0.75 D of predicted but performs similarly to Kane across all outcome measures. This remains true regardless of whether K or TK is used as an input. This study is limited by its retrospective design and use of a single MX60E IOL model.
Plain Language Summary: This multi-institutional retrospective case series compares the prediction accuracy and precision of the Zeiss AI IOL Calculator (ZAIC) to the Barrett Universal II (BU2) and Kane intraocular lens power prediction formulas for cataract surgery. Results suggest ZAIC outperforms BU2 and performs at least as well as Kane. This holds true regardless of whether standard or total keratometry is used as formula inputs. This corroborates ZAIC as an accurate and precise tool for the preoperative selection of intraocular lens power, performing at least as well as other modern intraocular lens power calculation formulas.
Keywords: cataract extraction, intraocular lens, artificial intelligence
Introduction
The refinement of IOL power calculation formulas is a continually advancing cornerstone of refractive cataract surgery. Typically, IOL power calculation formulas require three basic inputs: preoperative biometric measurements, a target postoperative refraction, and a lens constant. The latter is a single unitless number intended to account for the effect of each individual IOL model’s specific geometry and optical properties.
While theoretical lens constants are provided by the IOL manufacturer, crowd-sourced empirically derived constants are available for most IOLs and power calculation formulas at IOLCon.org,1 the successor site of the User group for Laser Interference Biometry (ULIB).2 Empirical constants are generally regarded as more accurate than the manufacturer’s constant. However, they are still a significant source of prediction error, in part due to small sample sizes and variance in contributor methodologies. While lens constants aim to refine predictions of effective lens position (such as in the context of predictive modeling used by many modern power prediction formulas),3 it is also well-recognized that a single value cannot fully capture an IOL’s varied behavior across the spectrum of ocular biometries and especially in higher IOL powers.4,5
Recently, a novel IOL power calculation formula has emerged which attempts to replace the use of the lens constant. The Zeiss AI IOL Calculator (ZAIC) was developed by Carl Zeiss Meditec (Jena, Germany) and released in April, 2023. Its development involved artificial intelligence training to conform to physical optics principles and the behavior of real eyes. Using training data from the Veracity platform, residual errors are minimized for individual IOL models, thereby refining the formula’s ability to adjust IOL-specific predictions for each eye’s biometry and intended IOL power. ZAIC accepts either Standard (K) or Total (TK) Keratometry as inputs and is currently available for 13 IOL models within the Veracity platform and EQ Workplace, as detailed in Supplemental Table 1.6,7
There are only two original studies to date on ZAIC outcomes. Kenny et al demonstrated ZAIC outperforms Barrett Universal II (BU2), Kane, and several other modern formulas across multiple outcome measures in a population of 278 short eyes (axial length < 22 mm).8 Wang et al additionally corroborated ZAIC’s advantage over BU2 in a more representative population of 10,838 eyes, with a sub analysis of 2053 eyes implanted with MX60E IOLs (Bausch and Lomb, Bridgewater, NJ) that showed ZAIC outperformed both BU2 and Kane for this IOL model. The same study reinforced that for short eyes (axial length < 22.5 mm), ZAIC outperformed BU2 and Kane.9
While further corroboration of these early ZAIC outcomes is still needed, no study has yet examined whether these relationships hold true when using TK measurements. In contrast to K, TK accounts for the posterior corneal curvature by incorporating direct reflectance anterior K measurements and swept-source optical coherence tomography (OCT) corneal thickness measurements to estimate the overall contributions of the anterior and posterior cornea, theoretically providing a more accurate representation of overall corneal power. This can be particularly helpful in eyes where the normal anterior-to-posterior ratio of corneal powers has been altered, such as in keratoconic or post-laser vision correction eyes. In the latter set of eyes, it has been shown that incorporation of posterior corneal curvature measurements in formulas like Barrett True-K may improve accuracy.10 While most studies show no difference in outcomes, some studies suggest the use of TK inputs may improve outcomes for some modern formulas and thus might alter the performance of these formulas relative to that of ZAIC.11,12 BU2 and Kane were selected because they are among the most commonly used contemporary formulas and are widely regarded as highly accurate in modern IOL power calculations.
Therefore, the purpose of this study is to corroborate ZAIC’s performance and determine whether the use of K or TK as inputs alters the relative performance of ZAIC versus two other modern formulas, BU2 and Kane, in a population of eyes implanted with a single monofocal IOL model. We hypothesize that ZAIC will produce lower mean absolute error (MAE) and standard deviation (SD) of the SE prediction error (PE) for each formula, as well as lower median absolute error (MedAE) and root mean squared absolute error (RMSAE), with higher proportions of eyes within 0.25, 0.5, 0.75, and 1 D of predicted compared to BU2 and Kane, regardless of whether K or TK are used as inputs.
Methods
This multicenter retrospective case series was approved by the Penn State Institutional Review Board (STUDY00024103) and adhered to the Declarations of Helsinki and the Health Insurance Portability and Accessibility Act. Patient consent was not required because the information gathered on each patient was not sensitive in nature and had a very low probability of causing harm to subjects or affecting decisions on clinical care they had already received.
Patients that underwent small incision clear cornea cataract surgery with monofocal IOL implantation (enVista MX60E, Bausch & Lomb, Bridgewater, NJ) for visually significant cataract at the Penn State Eye Center (Hershey, PA, USA) or the Dean McGee Eye Institute (Oklahoma City, OK, USA) between December 2018 to August 2024 were included. These eyes additionally had preoperative optical biometry performed on the IOLMaster 700 (Carl Zeiss Meditec, Jena, Germany). Patients with more than one eye represented had one eye randomly excluded to include only one eye per patient. Also excluded were any eyes with a postoperative refraction measured less than 21 days following surgery, those with prior history of incisional corneal surgery, those undergoing combined procedures, or those with any significant coexisting ocular pathology known to impact the refractive predictability of cataract surgery (ie, prior laser corneal refractive surgery, Fuchs endothelial dystrophy, keratoconus, uveitis) or vision potential (ie, macular degeneration, diabetic retinopathy). To maintain higher quality postoperative refraction data, eyes with best corrected visual acuity (BCVA) worse than 20/40 were also excluded. Postoperative subjective refractions were obtained by multiple trained personnel without the use of cycloplegic agents.
Demographic information was collected on all eyes. BU2 and Kane postoperative spherical equivalent (SE) predictions were obtained from their respective websites,13–16 using standard (K) and total (TK) keratometries, respectively, as inputs, to give two sets of predictions for each formula (ie, BU2 K and BU2 TK; Kane K and Kane TK). ZAIC predictions were obtained by sharing deidentified data (sine postoperative refractions) directly with Carl Zeiss Meditec. The A-constant obtained from IOLCon.org used to perform the BU2 and Kane calculations was 119.2. Primary outcomes included MAE and SD of the SE PE for each formula. Secondary outcomes included MedAE, RMSAE, and the proportion of eyes within 0.25, 0.5, 0.75, and 1 D of predicted. PE was calculated by taking the difference between the actual and predicted postoperative SE for each formula; they were then optimized for each formula by subtracting the mean PE from each individual PE to drive the mean PE to zero. Significant differences between ZAIC and the other formulas were identified for all outcome measures using the appropriate Wilcox-Holladay-Wang-Koch (WHWK) heteroscedastic statistical test, with Holm correction for multiple comparisons.17 A priori sample size calculation was not conducted; hence, the analysis has the potential to lack sufficient power to detect small differences between formulas.
Results
In total, 246 eyes of 246 patients were included in the study. Table 1 enumerates the demographic details on these eyes. Notably, the average subject age was 69, and the majority of patients were white/Caucasian. Postoperative LogMAR BCVA was 0.04 ± 0.08, with relatively unremarkable average biometry values including AL 23.9 ± 1.2 mm and Mean K 44.1 ± 1.6 D.
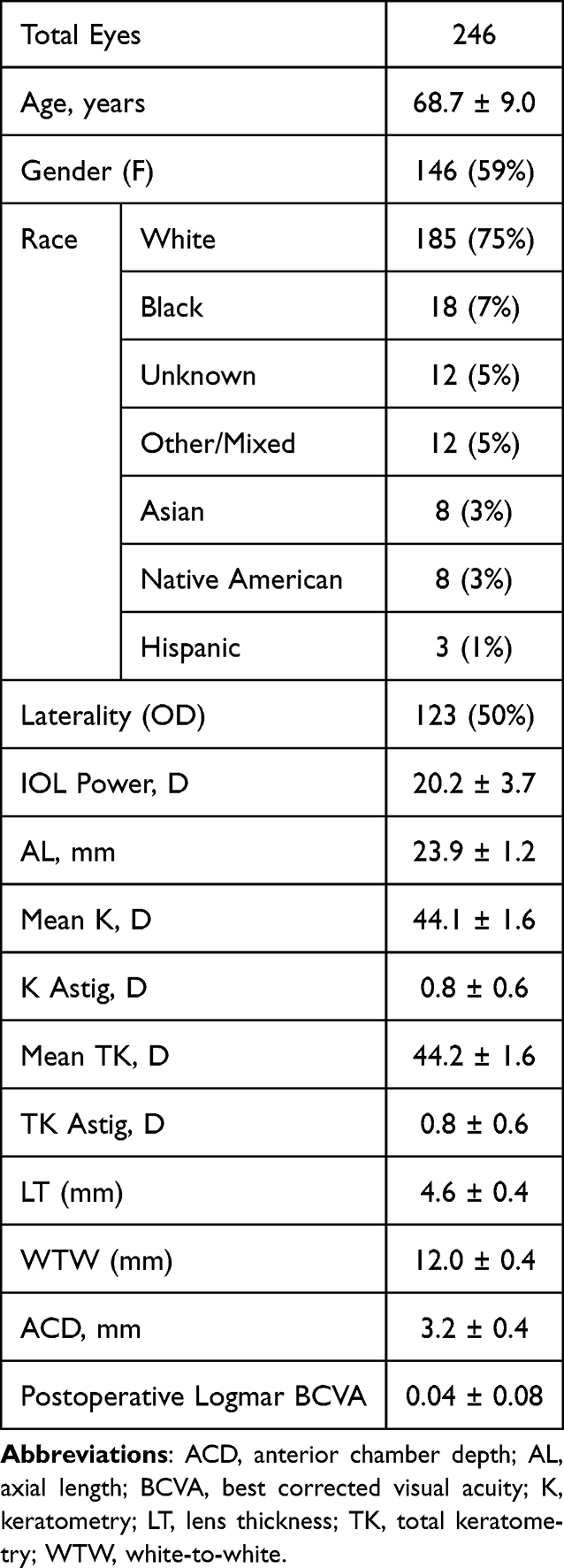 |
Table 1 Patient Demographics |
Primary and secondary outcomes are given in Table 2, and thresholds are reflected visually in Figure 1. ZAIC had a significantly lower SD of the PE compared to that of BU2 K (0.381 D versus 0.411 D; p = 0.001) and BU2 TK (0.381 D versus 0.417 D; p = 0.002). Likewise, ZAIC had a lower MAE compared to that of BU2 TK (0.296 ± 0.048 D versus 0.321 ± 0.052 D; p = 0.044) as shown in Figure 2. After Holm correction, there was no statistically significant difference found between ZAIC and BU2 K (0.296 ± 0.048 D versus 0.315 ± 0.051 D; p = 0.084). ZAIC had a lower RMSAE compared to that of BU2 K (0.380 D versus 0.410 D; p = 0.008) and BU2 TK (0.380 D versus 0.416 D; p = 0.008). There was also a higher number of eyes within 0.5 D of predicted for ZAIC [202 (82.1%)] versus for BU2 K [188 (76.4%); p = 0.022] and a higher proportion within 0.75 D for ZAIC [234 (95.1%)] versus for BU2 TK [224 (91.1%); p = 0.018]. There were no significant differences between ZAIC and other formulas for MedAE or for thresholds within 0.25 or 1 D. There were also no differences detected between ZAIC and Kane K or Kane TK outcomes. Unoptimized outcomes are provided in Supplemental Table 2. There were no significant differences in MAE between the two centers.
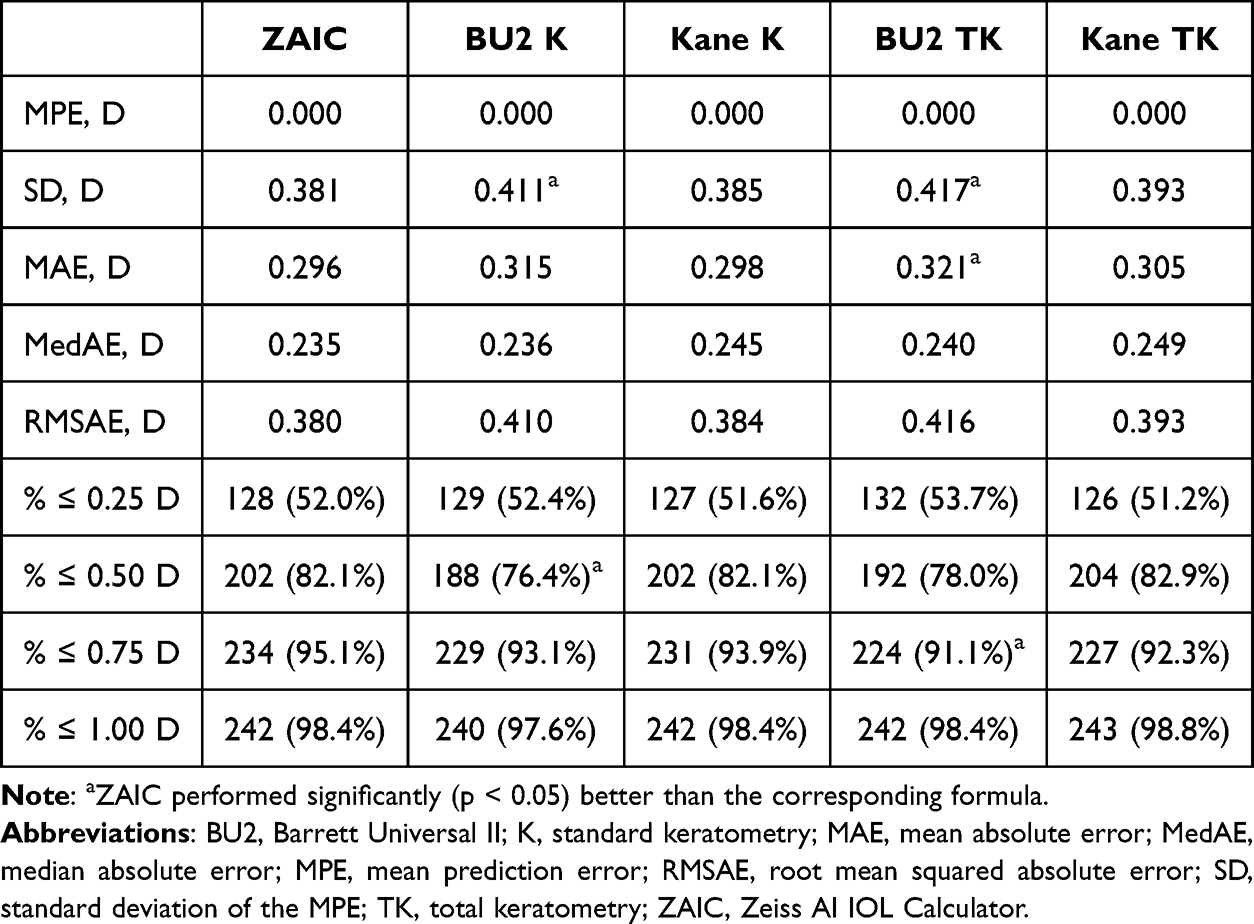 |
Table 2 Relative Formula Performance for Optimized Spherical Equivalent Prediction Errors |
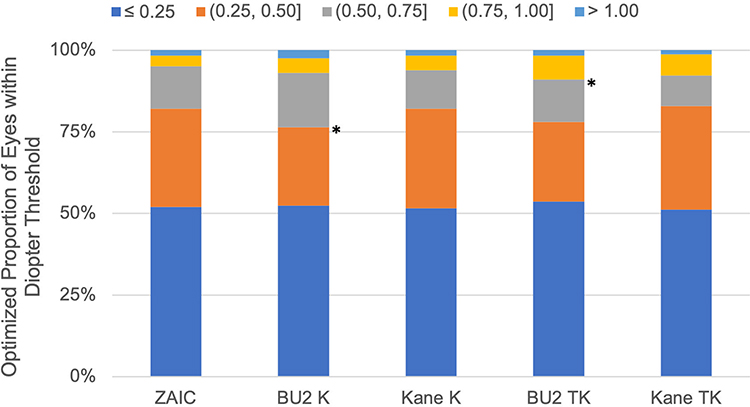 |
Figure 1 Optimized Thresholds. *p < 0.05. ZAIC has a significantly (p < 0.05) higher proportion of eyes within 0.50 D compared to BU2 K, and a higher proportion of eyes within 0.75 D compared to BU2 TK. Abbreviations: BU2, Barrett Universal II; K, standard keratometry; TK, total keratometry; ZAIC, Zeiss AI IOL Calculator. |
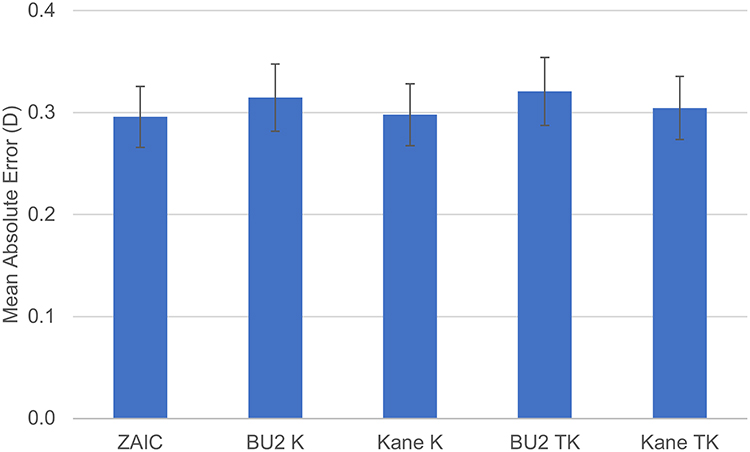 |
Figure 2 Optimized mean absolute errors with confidence intervals. ZAIC had a significantly (p < 0.05) lower mean absolute error compared to BU2 TK. Abbreviations: BU2, Barrett Universal II; K, standard keratometry; TK, total keratometry; ZAIC, Zeiss AI IOL Calculator. |
Discussion
ZAIC is a hybrid ray tracing- and artificial intelligence-based IOL power calculation formula and is currently the only formula to use artificial intelligence to replace the use of the traditional lens constant. Its outcomes are tailored for 13 IOL models within the Veracity platform. In the present study, we examined the performance of ZAIC relative to two other modern power calculation formulas found in Veracity: a vergence-based formula (BU2); and a hybrid vergence- and artificial intelligence-based formula (Kane). We also examined whether the use of standard versus total keratometry as formula input impacts the performance of the latter two formulas relative to ZAIC. We reported optimized outcomes, which are the most accurate way to measure formula performance because it helps minimize the effect of systematic PE offsets due to lens constant selection or from systematically skewed pre- or post-operative measurements in the test dataset.
Our findings are in agreement with the current literature. Wang et al found that for 2053 eyes implanted with the MX60E IOL, ZAIC outperforms BU2 and Kane in terms of SD, root mean squared absolute error (RMSAE), MAE, and select thresholds. Likewise, we also found that ZAIC produced a significantly lower SD and RMSAE and higher proportion of eyes within 0.5 D of predicted compared to BU2 K. In addition, ZAIC outperformed BU2 TK in terms of SD, RMSAE, MAE, and the proportion of eyes within 0.75 D of predicted. For all formulas, our data showed higher thresholds and lower SD, MAE, and MedAE outcomes compared to the same measures for eyes implanted with MX60Es in the Wang et al study. Our BU2 outcomes were highly comparable to benchmark results reported by Melles et al for the SN60WF IOL, with differences of 0.007 D (1.7%) in SD, 0.004 D (1.3%) in MAE, and 4.4% in the proportion of eyes within 0.50 D of predicted,18 suggesting that our dataset demonstrates performance consistent with established standards of refractive accuracy. This is likely because our data was derived from only two sites, where lane lengths and careful protocols for measuring post-operative manifest refractions were clearly established. Wang et al used data which came from many more surgeons with probable heterogeneous lane lengths and more variable protocols for obtaining refraction. However, unlike Wang et al, we did not detect any significant differences between ZAIC and Kane K or Kane TK, possibly because our study of 246 eyes was underpowered relative to the 2053 eyes they examined.
Our results did show a nonsignificant trend towards ZAIC outperforming both Kane K and Kane TK, consistent with the literature. While we did not have sufficient data to analyze a subset of short eyes, our results are consistent with Kenny et al, as our data demonstrate that ZAIC performs at least comparably to BU2 and Kane across multiple outcome measures. Our study additionally demonstrates no improvement in the performance of BU2 or Kane relative to that of ZAIC, regardless of whether K or TK are used as inputs, likely because we had a relatively normal dataset of eyes that reflects the general population, rather than overrepresenting subpopulations with abnormal or extreme keratometries. Although the absolute difference in MAE between ZAIC and BU2 TK (0.025 D) may be considered clinically small on an individual patient level, incremental improvements in prediction error can translate into meaningful gains at a population level. For example, modest increases in the proportion of eyes within 0.50 D of predicted refraction – often regarded as a clinically relevant threshold below which additional distance refractive correction is typically necessary – may still be of practical significance in routine cataract surgery.
There are clear theoretical advantages to a power calculation formula that bypasses the use of traditional lens constants and instead accounts for the nuanced interactions of each IOL model with preoperative biometries and implanted lens powers. Traditional lens constants, whether nominal or empirical, cannot account for these complex interactions as dynamically as artificial intelligence. However, a downside of using artificial intelligence for replacing lens constants is that it requires large, high-quality datasets of real-world refractive outcomes for each IOL model, which may (at least initially) limit its application to a smaller subset of IOL models which are used most frequently in practice. Further expansion of the IOL models available for use with ZAIC would be welcomed.
Conclusion
There are several strengths to the present study. First, because it is a multicenter study, results should be generalizable for eyes of normal ocular health implanted with MX60E IOLs. Second, our cohort demonstrated higher proportions within refractive prediction thresholds and lower dispersion metrics (SD, RMSAE, MAE, and MedAE) compared to prior studies evaluating ZAIC performance. In contrast, BU2 outcomes in our study were similar to those reported in large benchmark formula studies (eg, Melles et al), suggesting that the stringent exclusion criteria and data curation may have contributed to the observed performance metrics. This enables the identification of significant differences between ZAIC and BU2, even in a relatively small sample size representative of the population. Thirdly, we used robust heteroscedastic statistical methods in our analysis which have been shown to be sensitive in detecting significant differences while maintaining a high level of self-consistency.19
Weaknesses of this study include its retrospective nature and relatively small sample size, which may limit its ability to detect a real difference in performance between ZAIC and Kane. In addition, the small sample size also limits our ability to examine subsets of interest, such as eyes with short axial lengths. Other IOL models may also behave differently than the MX60E, which could limit generalizability.
In summary, we found that ZAIC outperforms BU2 in terms of SD, RMSAE, MAE, and select thresholds, regardless of whether K or TK are used as inputs. The present study reinforces this by detecting significant differences in outcomes even in a small, high-quality dataset of 246 eyes which are representative of the population. Finally, our data did not show that the use of TK alters the relative performance of BU2 or Kane compared to ZAIC. Future studies are needed to compare ZAIC to a broader range of modern formulas using expanded sets of IOL models.
Data Sharing Statement
This study was approved by the Penn State Institutional Review Board (STUDY00024103) and adhered to the Declarations of Helsinki and the Health Insurance Portability and Accessibility Act. Patient consent was not required because the information gathered on each patient was not sensitive in nature and had a very low probability of causing harm to subjects or affecting decisions of clinical care they had already received. Deidentified demographics and postoperative outcome measures on individual subjects are available upon written request by contacting the corresponding author for up to 3 years after publication.
Funding
This study was unfunded.
Disclosure
Dr Nathan Cannon receives consultant fees from Carl Zeiss Meditec, unrelated to the present work. Dr Kamran M Riaz serves as a consultant for AbbVie/ImmunoGen, Ambrx, Inc., Bausch & Lomb, Exelixis, Inc., and Neumora Therapeutics. He has received research support from Nova Eye. He receives royalties from Elsevier Publishing, Springer Publishing, and Wolters Kluwer Publishing. He has received speaking fees from AbbVie, AudioDigest, Bausch and Lomb, Brightstar Therapeutics, Carl Zeiss Meditec, Inc., CorneaGen, and Medscape. He has received travel fees from Aurion Therapeutics. None of these disclosures are related to the present work. Seth M Pantanelli is a consultant for Bausch & Lomb and Carl Zeiss Meditec, and additionally receives research support from Bausch & Lomb and Carl Zeiss Meditec, all unrelated to the present work. The authors report no other conflicts of interest in this work.
References
1. IOL Con. Available from: iolcon.org.
2. User Group for Laser Interference Biometry. Available from: ocusoft.de/ulib.
3. Olsen T, inventor. Methods of predicting the postoperative position of an IOL and uses of such methods. 2016.
4. Preussner PR. Okulix: ray tracing calculation for the pseudophakic eye. Available from: okulix.de/okulix-en.pdf.
5. Farsakoglu OF, Atik II, Kocabas H. Correlation of thin lens approximation to thick lens design by using context based method in optics education. In: Martins Costa MFPC, Zghal M, eds.
6. Koch D. Introducing the new ZEISS AI IOL Calculator. In:
7. Zeiss AI IOL Calculator. Available from: zeiss.com/meditec/en/products/data-management-software/zeiss-eq-workplace/zeiss-ai-iol-calculator-for-eq-workplace.html.
8. Kenny PI, Kozhaya K, Truong P, et al. Efficacy of segmented axial length and artificial intelligence approaches to intraocular lens power calculation in short eyes. J Cataract Refract Surg. 2023;49(7):697–8. doi:10.1097/j.jcrs.0000000000001185
9. Wang L, Burwinkel H, Bensaid N, Koch DD. Evaluation of an artificial intelligence-based intraocular lens calculator: AI-based IOL-optimized formula. J Cataract Refract Surg. 2024;51(4):332–336. doi:10.1097/j.jcrs.0000000000001603
10. Savini G, Hoffer KJ, Barrett GD. Results of the Barrett True-K formula for IOL power calculation based on Scheimpflug camera measurements in eyes with previous myopic excimer laser surgery. J Cataract Refract Surg. 2020;46(7):1016–1019. doi:10.1097/j.jcrs.0000000000000205
11. Qin Y, Liu L, Mao Y, et al. Accuracy of intraocular lens power calculation based on total keratometry in patients with flat and steep corneas. Am J Ophthalmol. 2023;247:103–110. doi:10.1016/j.ajo.2022.11.011
12. Ryu S, Jun I, Kim TI, Seo KY, Kim EK. Prediction accuracy of conventional and total keratometry for intraocular lens power calculation in femtosecond laser-assisted cataract surgery. Sci Rep. 2021;11(1):12869. doi:10.1038/s41598-021-92354-1
13. Barrett Universal II Formula. Available from: calc.apacrs.org/barrett_universal2105/.
14. Barrett GD. Intraocular lens calculation formulas for new intraocular lens implants. J Cataract Refract Surg. 1987;13(4):389–396. doi:10.1016/s0886-3350(87)80037-8
15. Barrett GD. An improved universal theoretical formula for intraocular lens power prediction. J Cataract Refract Surg. 1993;19(6):713–720. doi:10.1016/s0886-3350(13)80339-2
16. Kane Formula. Available from: iolformula.com.
17. Holladay JT, Wilcox RR, Koch DD, Wang L. Astigmatism analysis and reporting of surgically induced astigmatism and prediction error. J Cataract Refract Surg. 2022;48(7):799–812. doi:10.1097/j.jcrs.0000000000000871
18. Melles RB, Holladay JT, Chang WJ. Accuracy of intraocular lens calculation formulas. Ophthalmology. 2018;125(2):169–178. doi:10.1016/j.ophtha.2017.08.027
19. Cannon NT, Savini G, Pantanelli SM, et al. Which test is best: evaluation of traditional and contemporary statistical tests for analysis of spherical equivalent prediction error. Am J Ophthalmol. 2025;273:33–42. doi:10.1016/j.ajo.2025.01.022
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.