Back to Journals » Advances in Medical Education and Practice » Volume 16
Reflections of Occupational Therapy Graduates on Their Educational Curriculum at Kuwait University: An Exploratory Study
Authors Alotaibi N ![]() , Alnaser MZ
, Alnaser MZ ![]() , Jasem ZA
, Jasem ZA ![]() , Alhamad H
, Alhamad H ![]() , Ahmad FM
, Ahmad FM ![]() , Almajran A, Nadar MS
, Almajran A, Nadar MS ![]()
Received 21 July 2025
Accepted for publication 22 October 2025
Published 6 November 2025 Volume 2025:16 Pages 2043—2061
DOI https://doi.org/10.2147/AMEP.S551187
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Naser Alotaibi,1 Musaed Z Alnaser,1 Zainab A Jasem,1 Hamad Alhamad,1 Feddah M Ahmad,1 Abdullah Almajran,2 Mohammed Sh Nadar1
1Occupational Therapy Department, Faculty of Allied Health Sciences, Health Science Center, Kuwait University, Jabriah, Kuwait; 2Department of Community Medicine, Faculty of Medicine, Health Science Center, Kuwait University, Jabriah, Kuwait
Correspondence: Naser Alotaibi, Email [email protected]
Introduction: Global trends in occupational therapy practice such as telehealth, community-based practice, and culturally safe care have become integral in occupational therapy. It highlights the need for curricula that integrate emerging practices alongside core competencies of practitioners. Thus, understanding occupational therapy graduates’ perspectives concerning their educational curriculum is important as it provides insights into their experiences, identifies gaps in education, and ensures alignment with evolving professional demands. These perspectives further assist in refining curricula to enhance competency and preparedness for clinical practice.
Purpose: This preliminary research studied the perspectives of occupational therapy graduates regarding their educational experiences at the occupational therapy department at Kuwait University.
Methods: A convergent parallel mixed-methods approach was utilized using a self-developed questionnaire (ie Curriculum Questionnaire) with close- and open-ended questions. Descriptive statistics, reliability analysis and t-test served as primary analyses of the quantitative data, and thematic analysis was used to analyze the qualitative data.
Results: The study included 83 participants, with the questionnaire demonstrating strong validity and internal consistency. Graduates reported moderate satisfaction with faculty support (mean=3.7 ± 1.1), with higher satisfaction among participants with more years of experience within practice (P=0.035). Conversely, satisfaction with laboratory classes was notably low, particularly concerning equipment and space (mean=2.7 ± 1.0). Graduates emphasized curriculum strengths such as professionalism, occupation-based models, and environmental adaptation; however, they highlighted gaps such as lack of specialty exposure (eg, dysphagia, assistive technology, and neonatal care), limited interprofessional education, and insufficient preparation for emerging areas like telehealth and culturally responsive practice.
Conclusion: Understanding graduates’ perspectives is crucial for advancing the educational curriculum, enhancing clinical learning environments, and ensuring that graduates are well-prepared for professional challenges. Linking findings to Kuwait’s healthcare priorities and university reform agenda underscores the practical significance of curriculum adaptation.
Keywords: curriculum development, higher education, telehealth, healthcare, interprofessional education, health promotion
Introduction
Healthcare clients have continuous and increasing demands and expectations of healthcare services.1,2 Healthcare institutions strive to deliver high-quality services that meet client satisfaction.3 Therefore, healthcare education programs have a great responsibility to meet the needs of healthcare clients and institutions. Preparing qualified, skilled, and competent graduates is an ongoing evaluated process to ensure the delivery of high-quality healthcare services across diverse patient populations and contexts. Because education programs serve as the backbone of the healthcare industry, evaluating the healthcare curriculum is a critical first step to identify both facilitators and challenges to quality care.
Occupational therapy is a healthcare profession providing healthcare services to various populations in different contexts. Due to the fast-growing healthcare technologies, healthcare demands, and increasing patient expectations, occupational therapy educational curricula must equip their students with the knowledge and skills necessary to ensure adequate preparedness to practice.
In order to ensure successful transition from the academic to the workplace environment, essential competency development areas within the occupational therapy educational curriculum are required. These essential competency development areas would include: 1. professional attitudes (ie cultural competency and personality traits); 2. Professional communication (ie effective and empathetic communication skills with patients), 3. collaboration (ie working collaboratively not only with occupational therapists but also within the whole rehabilitation team to support multidisciplinary practice and holistic care); 4. Delivery of quality service (ie the provision of evidence-based occupational therapy practice and applying client-centered approach to maximize therapeutic outcomes).4 Integrating these competency areas within the occupational therapy educational curriculum as a curricular framework along with addressing the World Federation of Occupational Therapists (WFOT) Minimum Standards for the Education of Occupational Therapists, can serve as a benchmark for assessing the effectiveness of the educational programs and identify areas for improvement.5
Evaluating occupational therapy curricula is particularly crucial because occupational therapy education uniquely integrates both biomedical and psychosocial aspects of care, requiring students to develop hands-on skills alongside theoretical knowledge. Unlike other health professions, occupational therapy students must demonstrate competence in a wider range of skill domains, such as activity analysis, environmental adaptation, occupation-based models, and client-centered approaches, which presents distinct challenges. Educational curricula are expected to prepare students to reconstruct their knowledge and contextualize it in the clinical practice after graduation. Such transition is expected to meet the changing demands of the clinical environment and support evidence-based practice.6–12 Therefore, ongoing evaluation of the occupational therapy curriculum is essential to ensure that the curriculum remains relevant to practice and aligns with student needs, healthcare trends, and client expectations.
However, occupational therapy curricula vary significantly across different countries and institutions due to differences in healthcare systems, professional regulations, and accreditation requirements. The evolution of occupational therapy practice, including the integration of technology, telehealth, and community-based rehabilitation, necessitates continuous curriculum updates to ensure alignment with global standards,6,8,13 while meeting local contextual needs. Hence, global trends and standards in occupational therapy education demands understanding of the competency requirements for occupational therapists worldwide.14 Notably, global advancements in occupational therapy necessitate curriculum updates to address challenges such as cultural humility, evidence-based practice, and critical reflexivity in practice. Western-influenced curricula may limit cultural responsiveness, requiring greater integration of non-Western perspectives.15 Additionally, barriers to evidence-based practice, including connotations of disability, time constraints, and resource accessibility, highlight the need for stronger emphasis in occupatonal therapy education.16,17 Lastly, global therapist shortages stress the importance of curricula that support workforce sustainability and skill retention.18
Due to the constant growth in understanding of the clinical environments, healthcare teams, diseases and disorders characteristics and demographics, the review of the occupational therapy curriculum is necessary. One important strategy to address that is through grasping the views of the occupational therapy graduates regarding their educational curriculum. It is essential to understand the perspectives of occupational therapy graduates regarding their educational curriculum and its relevance to the dynamic nature of the clinical practice.6,19,20 Such views can offer broader insights about the required changes to be made within the curriculum, thus facilitating the use of an occupational perspective across practice settings, maintaining the pace with current events, trends, changes, and developments, and upholding professional values.21,22 Understanding the graduates’ occupational therapy perspectives can stimulate curriculum redesign and therefore facilitate the process of curricular review and revision to meet the dynamic and ongoing nature of the clinical expectations in occupational therapy practice.8–11,13,19,20,22,23 This can also facilitate desired professional changes within the educational curriculum and improve knowledge acquisition and skills development for occupational therapy students and graduates.6,8,10,13,23 However, the perspectives of occupational therapy graduates regarding their educational curriculum in Kuwait were not explored.
The occupational therapy educational program at Kuwait University is newly developed and was established in 2009. As a relatively recent program, it faces unique challenges, including the need for ongoing curriculum refinement, faculty development, and alignment with evolving international standards. Unlike long-established programs in the United States, United Kingdom, Australia, and Canada, Kuwait’s program requires frequent assessments to refine clinical training, research integration, and teaching strategies. However, compared to longer-established programs, it may require more structured evaluation mechanisms to ensure it keeps pace with global advancements in occupational therapy education. Hence, it is accredited by the World Federation of Occupational Therapists (WFOT), which is the professionally recognized accrediting body for all international occupational therapy educational programs worldwide.24 Since the commencement of the program at Kuwait University, twelve batches have graduated and are currently working in different healthcare sectors to meet the needs of different patient populations.
Despite the significance of curriculum evaluation, there is a lack of research investigating the effectiveness and adequacy of occupational therapy education in Kuwait. This gap highlights the need for an empirical investigation into how well the curriculum prepares graduates for real-world clinical challenges and professional expectations. Refining the occupational therapy curriculum and ensuring that it meets the ongoing development in the profession demonstrate the key role of occupational therapists with post-graduate qualifications, thus producing desired and satisfactory patient outcomes in the future.25 Furthermore, evaluating the curriculum provides a professional competency guide for upholding ethical and legal standards, ensuring patient safety, collaborating across disciplines, and applying evidence-based practice. The challenges of theoretical transfer into effective clinical decision-making, client-centered practice, and cultural responsiveness are essential in the preparedness to adapt to complex healthcare environments.
Of note, cultural norms are highly emphasized in occupational therapy education and practice, as it plays significant role in shaping the therapist’s therapeutic choices and patients’ outcomes.18 Therefore, cultural considerations, particularly reflecting the Middle Eastern culture, should be incorporated well within the occupational therapy education due to its unique beliefs and values.26 For example, understanding specific Middle Eastern cultural factors, such as gender differences, religious beliefs, strong family bonds, culturally tailored collaborative care and lifestyles, are fundamental elements to be considered within the assessment and intervention process.27 In particular, the integrations of factors influencing the local context and cultural relevance among people living in Kuwait, are expected to be covered through teaching and clinical placements within the occupational therapy curriculum at Kuwait University.
Having said that, the purpose of the current study was to investigate the perspectives of occupational therapy graduates regarding their educational experiences at the occupational therapy department at Kuwait University. This study has important implications for occupational therapy students, faculty, clinical supervisors, and clinicians. It will inform desired curricular changes that promote students’ positive learning experiences and support graduates’ needs to meet the dynamic challenges of the clinical environments. It will consequently support the desired service provision and patients’ therapeutic outcomes.
Methods
Design
The study utilized a convergent parallel mixed-methods approach, including both quantitative and qualitative approaches. This approach was chosen because it allows for the simultaneous collection and analysis of both types of data, thus providing a comprehensive deeper understanding of graduates’ perspectives relevant to their educational curriculum. Hence, combining both approaches allowed for cross datasets interpretation, consequently enhanced the study’s credibility and validity. The quantitative approach comprised closed-ended questions, while the qualitative approach included open-ended questions requiring coding and thematic analysis. Using this design, the study was able to integrate numerical data with rich narrative responses, ensuring that findings were well-rounded and reflective of the graduates’ experiences. For the purpose of this study, the questionnaire is called Curriculum Questionnaire (CQ).
Participants
Participants included occupational therapy graduates from twelve consecutive batches (n=291) who earned their Bachelor of Science degree in occupational therapy from Kuwait University. All twelve batches followed the same core curriculum, ensuring consistency in training content, credit requirements, and competency expectations across cohorts. Graduates were working in public or private sectors or pursuing higher education (in Kuwait or abroad). A convenience sampling method was used to recruit participants, as it allowed for efficient access to a large number of graduates via social media and professional networks. This approach was practical given the limitations of reaching all graduates through official records. Of note, the graduates who were practicing as occupational therapists were called “the experienced therapists”, whereas “the non-experienced therapists” were those who had only completed an internship of up to three months without officially practicing as occupational therapists. Occupational therapy students and non-Kuwait University graduates were excluded.
Instrumentation
Development and Validation of the Curriculum Questionnaire (CQ)
In order to develop a well-structured questionnaire that is appropriate, relevant, and inclusive to address the study’s main objective, an extensive literature search was performed concerning items, components, and/or other relevant issues and factors pertaining to occupational therapy educational curricula. Doing so contributed initially to the development and construction of the questionnaire components and items. Following that, due to their knowledge base and expertise in occupational therapy theory and education, the questionnaire was sent to seven occupational therapy experts who are academicians and researchers (Ph.D holders) with a wide range of teaching and research experience in the field of occupational therapy. For the purpose of obtaining holistic perspectives, these experts had different occupational therapy specialties and were from different countries including Kuwait (four experts), United States (one expert), India (One expert) Australia (one expert); they all provided inputs, feedback, and recommendations to ensure the relevance and appropriateness of its contents. A series of meetings and discussions were held to review and scrutinize the questionnaire components and items within the expert committee. Following several meetings with the experts, all feedback and inputs were addressed and incorporated. Finally, a consensus of the final questionnaire components and items was reached for the approval of its final version.
A pilot testing stage was undertaken with 20 occupational therapy graduates, who were from different occupational therapy specialties including pediatrics, neuro-rehabilitation, orthopedics, and mental health; they were conveniently selected (convenience sampling) with a wide range of working experience ranging from 1 to 7 years; the intent of this process was to ensure clarity and relevance of all questionnaire items. In order to support the content validity of the CQ, a content validity index (CVI) was developed. This index included two main components: (1) clarity of items (comprehensibility), (2) relevance of items (appropriateness). In addition, for each of these two components, there was a 4-point scale response to choose from for each item (1 – strongly disagree, 2 – disagree, 3 – agree, and 4 – strongly agree). A face validity form was also provided to the participants, which asked them whether this questionnaire serves its main intent of grasping their reflection of the taught educational curriculum. The response to this question was dichotomous with either yes or no response.
After reviewing and analyzing the results of the CVI, it was found that generally all items were relevant and appropriate. However, as suggested by few participants, several items were rewarded to ensure better readability and clarity of all items. With regards to the face validity of the CQ, face validity was supported by 85% (n=17) of the pilot study participants. Hence, it was demonstrated that the outcome of this pilot testing stage was positive thus supporting the validity of the CQ. On the other hand, the reliability of the CQ was assessed in later stage. Measuring reliability was through assessing the internal consistency of CQ; this was conducted when the actual data collection process was initiated with a larger sample size of occupational therapy graduates.
Structure of the CQ (Components and Items)
It included three components:
First Component
This first section addresses the characteristics and demographics of the study participants, including age, year of graduation, work experience, area of practice, setting, types of diagnoses seen, participation in continuing education, conference attendance, research involvement, and supervision of occupational therapy students.
Second Component
This second section includes two main subcomponents. First, there are seven close-ended questions that assess satisfaction with the occupational therapy curriculum, including didactic courses, laboratory courses, faculty teaching style, faculty support, and clinical placements/fieldwork training. Second, there are 24 questions regarding curriculum agreement, covering topics such as the occupational therapy process, research courses, occupation-based models, philosophical and theoretical concepts, emerging areas, health promotion, and interdisciplinary collaboration. Both satisfaction and agreement questions were measured using a 5-point Likert scale, with higher scores indicating greater satisfaction or agreement.
Third Component
This third section contains open-ended questions that explore the participants’ reflections on three main subcomponents including: 1. the theoretical courses of the occupational therapy educational program; 2. the occupational therapy laboratory courses of the occupational therapy educational program; 3. the clinical fieldwork placement and training of the occupational therapy educational program. There were three open ended questions for each subcomponent targeting a) strengths, b) weaknesses, and c) recommendations for improving occupational therapy theoretical courses, laboratory courses, and fieldwork placement and training, respectively. Thus, within the created Google Form of the questionnaire, participants were able to type in their responses in response to the open-ended questions to collect the qualitative data. Participants were also given the opportunity to provide additional comments on aspects of the curriculum not covered in previous questions.
For the readers’ convenience, the whole study developed curriculum questionnaire is attached in Supplementary File (S1).
Data Collection Procedure
The Institutional Review Board (IRB) approval (approval no/963) was obtained before data collection. Graduates were contacted through social media platforms (eg alumni WhatsApp groups) and emails using a Google Forms questionnaire to facilitate participation and improve response rates. The study rationale was explained, anonymity was assured, and informed consent was obtained from all participants. Hence, the participants informed consent included publication of anonymized responses/direct quotes. In addition, with regards to the open-ended questions, the written qualitative responses were collected through Google Forms in a separate file for its analysis and interpretations.
Data Analysis
Analysis was conducted using IBM® SPSS Statistics for Windows, Version 29.0 (IBM Corp., Armonk, NY, USA). The statistical significance level was set at 5% (α = 0.05) for all analyses. Descriptive analysis was used to calculate means, standard deviations, medians, and interquartile ranges (IQRs) for continuous variables, while categorical variables were summarized using frequencies and proportions. Additionally, score variables were analyzed using means, standard deviations, medians, and IQRs. Reliability (internal consistency) was measured using Cronbach’s alpha coefficient. Both parametric and non-parametric tests were employed to assess differences between experienced and non-experienced therapists: t-tests were used for normally distributed data, while the Mann–Whitney U-test was applied to compare medians in non-normally distributed variables.
Concerning the open-ended questions of the survey, a thematic analysis was conducted to identify the main themes of the graduates’ responses, followed by Braun and Clarke28 guidelines. Two independent coders applied Braun & Clarke’s six-step thematic analysis. A codebook was iteratively refined; discrepancies were resolved via discussion. Inter-coder reliability was calculated (Cohen’s κ=0.82), demonstrating strong agreement. Reflexivity was maintained via analytic memos and an audit trail. Hence, the coding process involved several steps: (1) data familiarization, (2) initial code generation, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the final analysis. A consensus was reached via discussion to formulate the study themes and subthemes accordingly. In other words, a thematic analysis was made qualitatively to confirm the inclusion of all relevant themes and subthemes obtained from the graduates’ perspectives.
Findings from both datasets were then integrated using “following a thread technique” to track identified key findings across the two datasets to allow for data interpretation.29,30 This was achieved by comparing the findings from the quantitative and qualitative data which allowed for interdependent explanations of the results.
Results
A total of 83 participants participated in the study, with a response rate of 28.5%. This response rate was expected given the challenges in reaching all graduates, such as availability and willingness to participate. However, it may impact the representativeness of the findings, as those who responded may have stronger opinions about the curriculum compared to non-respondents. The final sample (n=83, ~28% response rate) represents approximately 30% of reachable alumni, which is considered acceptable for exploratory mixed-methods studies in small professional cohorts.31
The majority were female (95.2%), reflecting the gender distribution in the occupational therapy field. The participants held a bachelor’s degree (96.4%) and had an average age of 25.5 years. Their clinical experience averaged 2.6 years, and their GPA was on average 3.1. In addition, the practice settings varied, while attending different settings including rehabilitation hospitals (34.9%), general hospitals (18.1%), and specialized hospitals/centers 7.2%). To our knowledge, gender distribution, professional experience, and practice settings among respondents generally align well with the general OT graduate population in Kuwait, supporting the applicability of the findings. The main areas of practice included hand therapy (25.3%), pediatrics (20.5%), neurorehabilitation (18.1%), and mental health (3.6%). Regarding professional development, the data revealed that 59.8% of the participants had not participated in any research or published publications, and 66.3% had not supervised occupational therapy students. The majority had attended at least one scientific conference (63.4%), and a similar proportion had taken one or more certification courses. Descriptions of the participants’ characteristics are identified in Table 1.
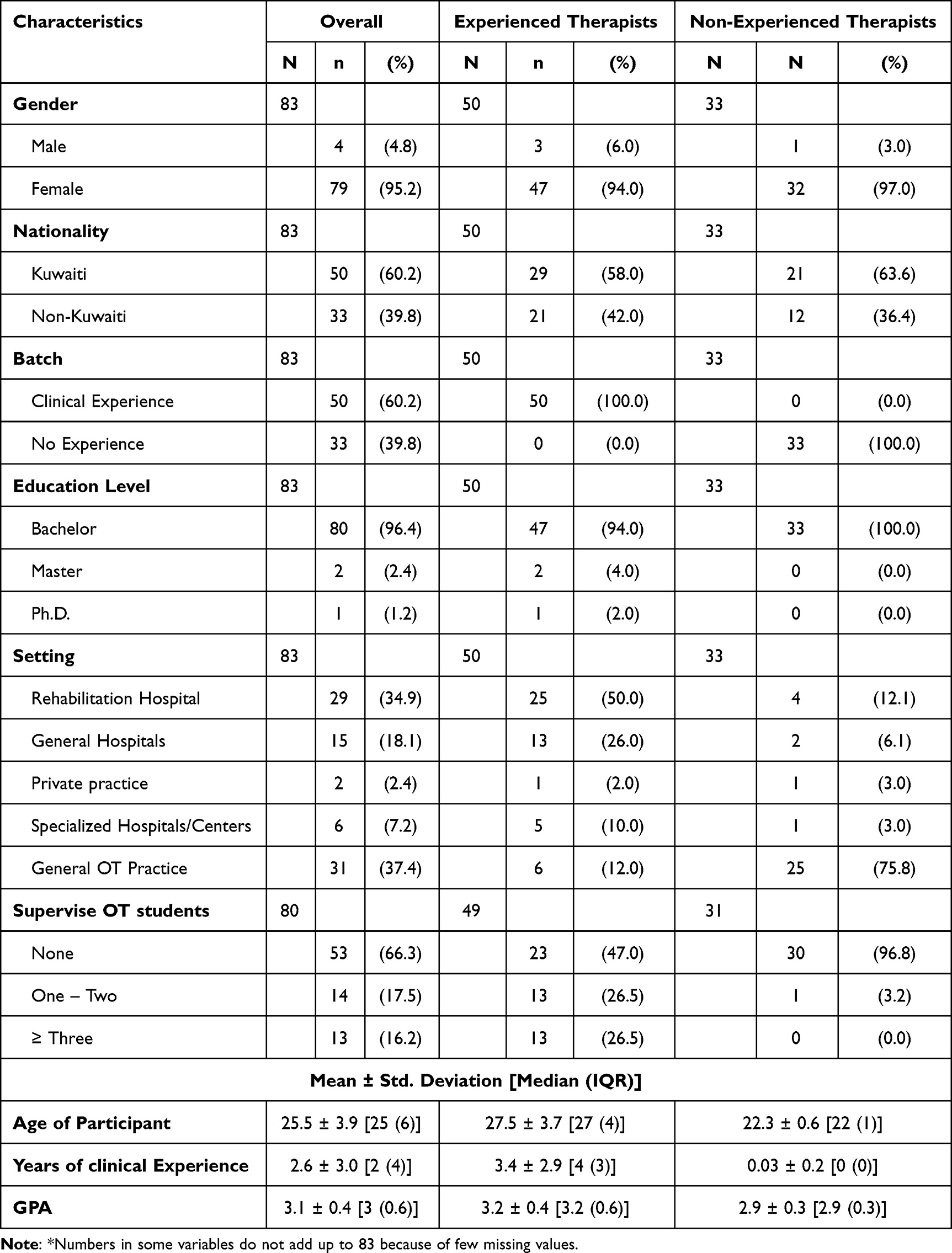 |
Table 1 Characteristics of the Study Participants (N=83) |
With regards of the reliability of the CQ, particularly the quantitative part of it, its reliability (internal consistency) was indicated for the study sample (n=83); the reliability analysis for satisfaction subcomponent (consisting of 7 items) was α = 0.88, while for agreement subcomponent (consisting of 24 items) was α = 0.95. The combined subcomponents together (consisting of 31 items) was α = 0.96. Such values indicate a satisfactory internal consistency of the CQ for its use with the occupational therapy graduates.
Satisfaction with the Occupational Therapy (OT) Educational Curriculum
With regards to the satisfaction with various aspects of the occupational therapy curriculum, the study participants had higher levels of satisfaction relevant to the support provided to students from the occupational therapy faculty members (3.7 ± 1.1). On the other hand, the lowest satisfaction level reported by the study participants was related to occupational therapy laboratory classes in terms of tools/equipment (2.7 ± 1.0) as well as occupational therapy laboratory classes in terms of space (2.8 ± 1.1). The dissatisfaction with lab spaces and equipment may indicate the need for infrastructure improvements to enhance practical learning experiences. Additionally, the participants exhibited an acceptable level of satisfaction with the clinical fieldwork placement and training (3.2 ± 0.9). Further details on satisfaction with the occupational therapy Educational Curriculum are reported in Figure 1.
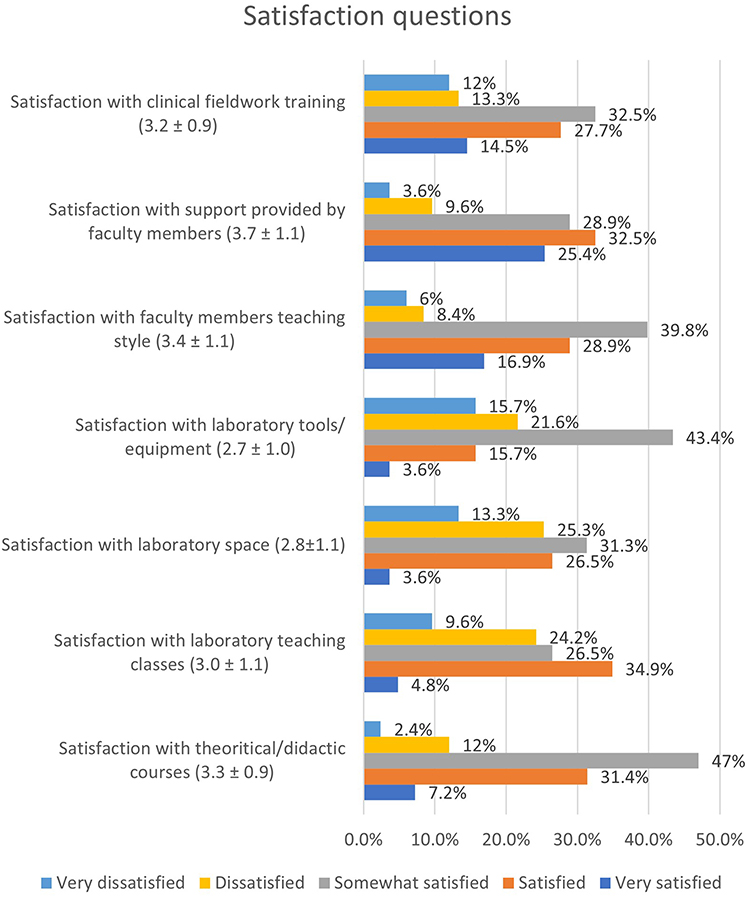 |
Figure 1 Satisfaction with the occupational therapy (OT) educational curriculum (n= 83). |
Agreement with the Content of the Occupational Therapy (OT) Educational Curriculum
As illustrated in Table 2, the agreement with the content of the educational curriculum varied based on the perspectives of the study participants. The most highly agreed-upon content areas within the curriculum included professional behavior (4.1 ± 0.9), occupation-based models (ie, frames of reference) (3.8 ± 0.9), and environmental adaptation (3.8 ± 0.9). These findings suggest that foundational aspects of occupational therapy practice are well covered and appreciated by graduates. Participants also reported adequate agreement with content such as occupation-based assessments that are culturally appropriate (3.6 ± 1.0), client-centered and functionally based intervention approaches (3.6 ± 0.9), health promotion and wellness (3.6 ± 1.1), disability rights (3.6 ± 1.1), and understanding and applying research concepts to support evidence-based practice (3.5 ± 1.2).
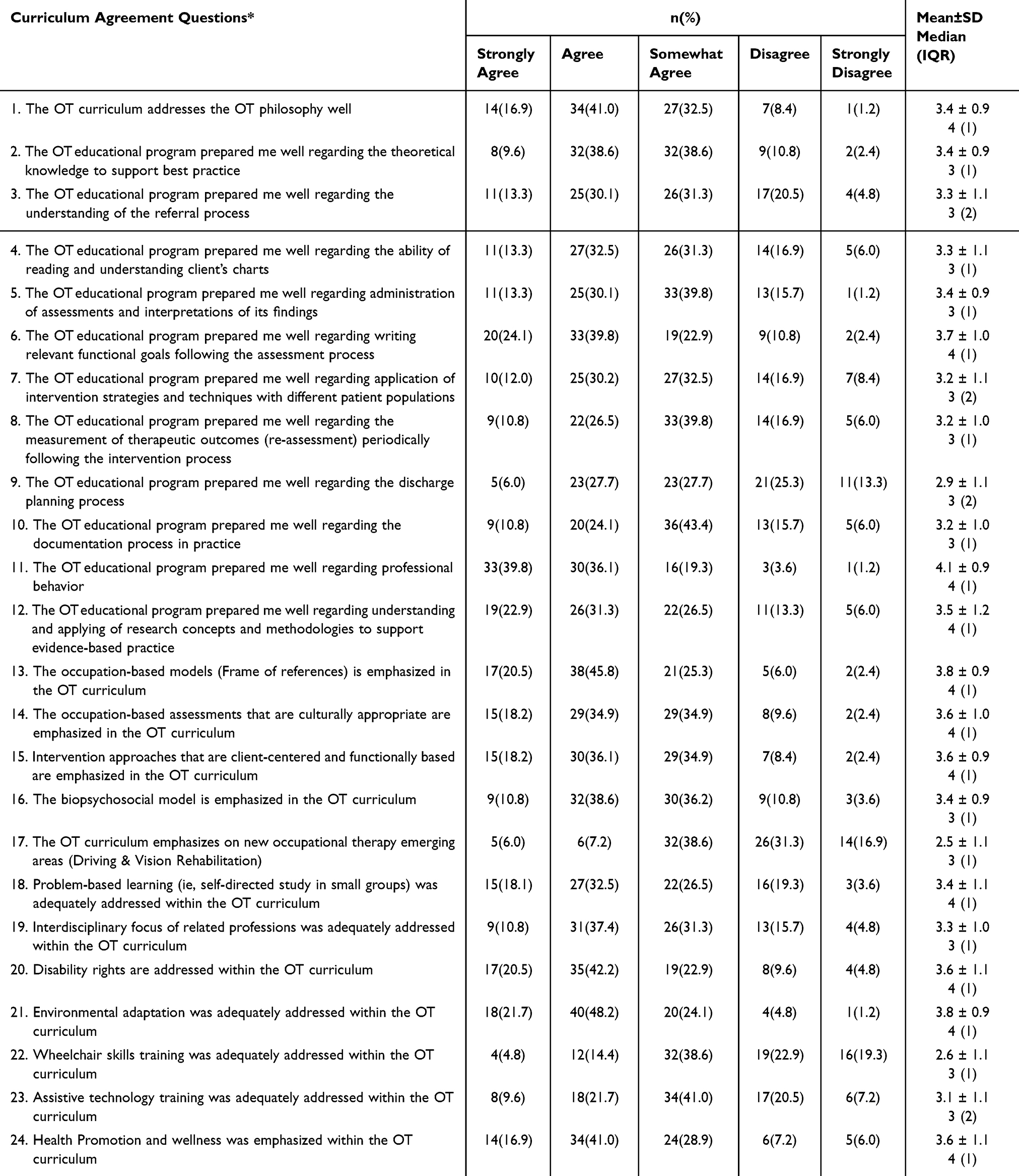 |
Table 2 Agreement with the Content of the Occupational Therapy (OT) Educational Curriculum (N=83) |
On the other hand, curriculum content related to emerging areas (2.5 ± 1.1) as well as wheelchair training (2.6 ± 1.1) was rated as inadequately addressed. The low scores in emerging areas highlight the necessity of curriculum updates to include modern occupational therapy practices such as telehealth and assistive technology. Additionally, interdisciplinary focus on related professions (interprofessional education) was not highly emphasized within the curriculum (3.3 ± 1.0). Further details concerning participants’ agreement with the occupational therapy curriculum content are illustrated in Table 2.
Comparison Between Experienced and Non-Experienced Therapists in Terms of Satisfaction and Agreement with the Occupational Therapy (OT) Educational Curriculum
In our study, non-experienced therapists were significantly less satisfied with laboratory classes in terms of space compared with experienced therapists (P=0.014). On the other hand, experienced therapists reported significantly higher satisfaction levels regarding the support provided by occupational therapy faculty members (P=0.035). This suggests that professional experience may positively influence graduates’ perceptions of faculty support, possibly due to increased appreciation of foundational training. Table 3 provides further details about the comparison between experienced and non-experienced therapists in this regard.
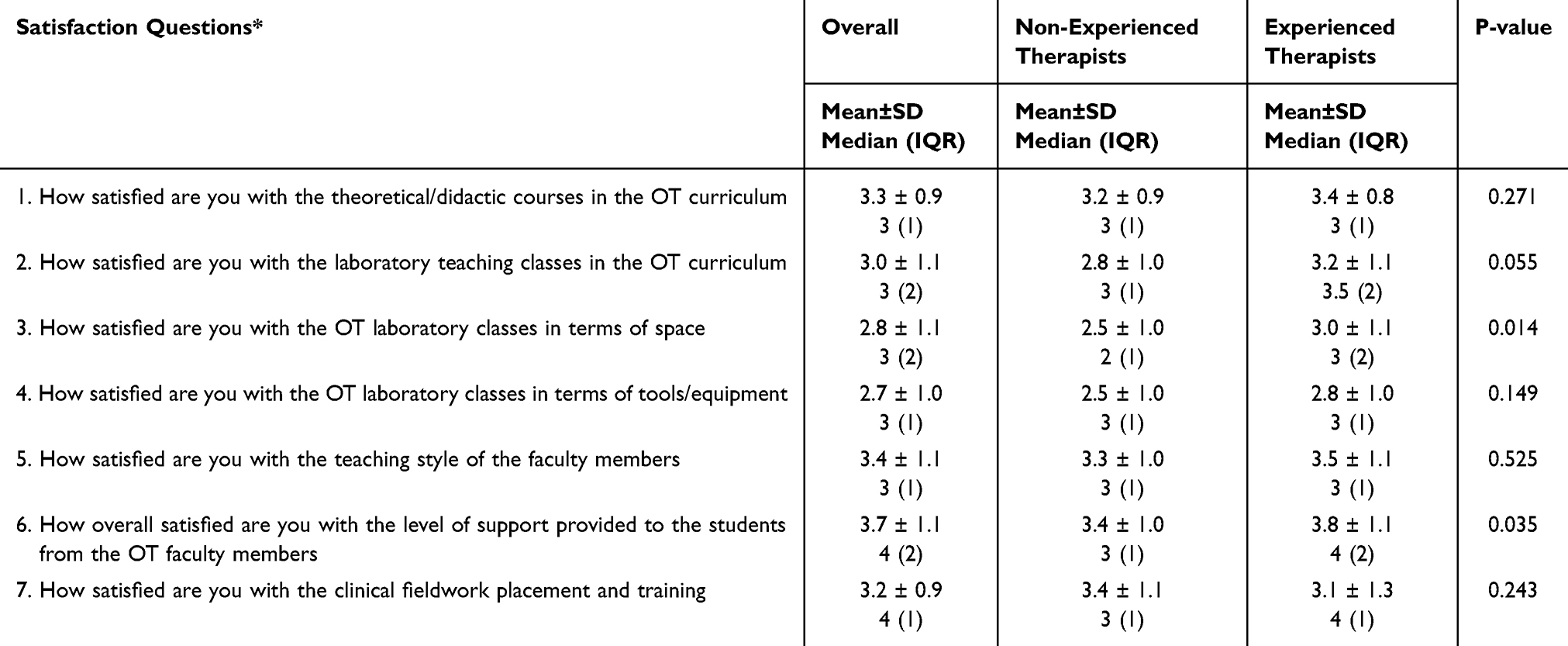 |
Table 3 Comparison Between the Experienced Therapists (N=50) and Non-Experienced Therapists (n=33) in Terms of Satisfaction with the Occupational Therapy (OT) Educational Curriculum |
Furthermore, experienced therapists believed that the biopsychosocial model was significantly better covered in the curriculum compared with non-experienced therapists (P=0.049). This difference may stem from the fact that experienced therapists have had the opportunity to apply these concepts in practice, reinforcing their relevance. Additional details about comparisons between experienced and non-experienced therapists concerning agreement with occupational therapy curriculum content are illustrated in Table 4.
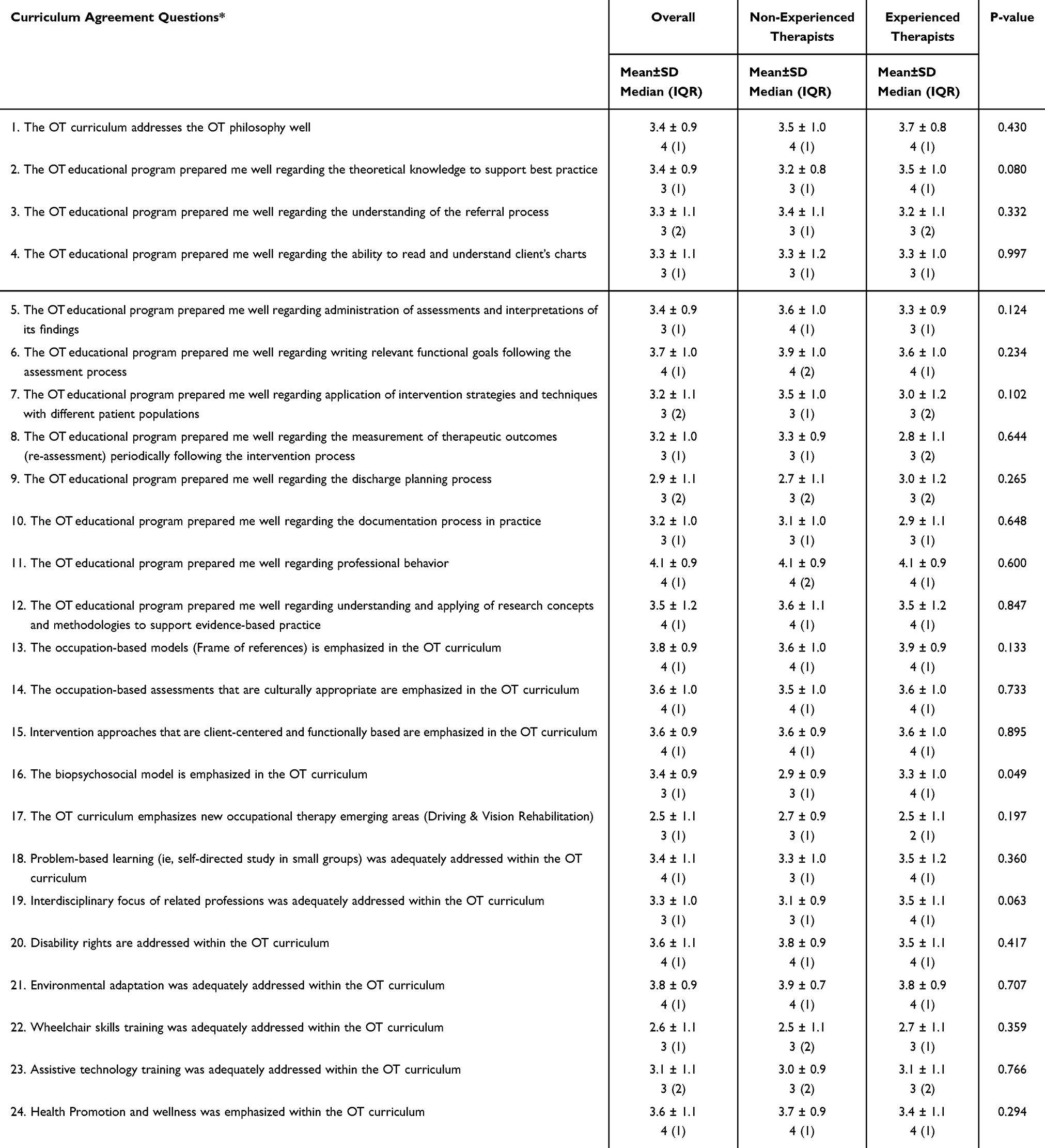 |
Table 4 Comparison Between the Experienced Therapists (N=50) and Non-Experienced Therapists (n=33) in Terms of Agreement with the Content of the Occupational Therapy (OT) Educational Curriculum |
Qualitative Findings
Analysis of the qualitative findings resulted in the emergence of two main themes: (1) the curricular aspect; and (2) teaching and learning resources. In addition, there were two subthemes for each theme. Hence, theme one has two subthemes including (a) curriculum coverage and depth of knowledge and (b) students’ skills development. On the other hand, the second theme has also two subthemes including (a) occupational therapy educators and (b) availability of resources to foster students’ practical training.
Theme One: Curricular Aspects
In this theme, participants discussed their educational curriculum in terms of the theoretical courses, practical training, and their clinical fieldwork training/experience.
Subtheme 1: Curriculum Coverage and Depth of Knowledge
Participants agreed on the comprehensive nature of the curriculum and its coverage of main topic areas “It covers all main areas of practice intensively such as Mental Health, Pediatrics, Neuro, and Ortho” P35; thus, ensuring a strong foundational knowledge in various areas of occupational therapy practice. This highlighted advantage was not limited to their theoretical education but also include their clinical trainings. P79 stated when was asked about their clinical fieldwork experience “We got knowledge from different cases. Apply the techniques and frames of references with real patient”. Accordingly, participants highly appreciated their practical trainings and fieldwork experiences that was diverse. P4 stated “Very practical, very occupational therapy based and related, and the chance of actually practicing and demonstrating different tests and techniques”.
However, participants showed their curiosity to have more content area in regard to specialty areas that were underrepresented content areas in the curriculum “Some of important areas (sub-specialty) of occupational therapy were not well taught (ex, dysphagia, seating, burns, assistive technology, women health, neonatal therapy)” P8. Despite the fact that variety of placements were available for their clinical training, “Some students are in the same placement for two courses and it’s not fair for the others who did not get to experience it” P11. This was also illustrated by P24 when asked about the main weaknesses within the clinical fieldwork placement “Duplication of areas or settings”.
Another area of concern was demonstrated in the findings related to the insufficient link that some participants experienced between the gained theoretical knowledge and its practical application. P18 mentioned “There is no connection between theoretical courses and fieldwork; there is always huge gap and not everything learned in classes can be applied in real practice settings. Also, most of evidence-based practices and frames of reference are not culturally based and not suitable to be applied in Kuwait practice”. Thus, the application of learned concepts was also not always possible, and not all learned knowledge were culturally sensitive.
Subtheme 2: Students’ Skills Development
Having a comprehensive curriculum assisted in enhancing students’ skills on a professional as well as personal levels. It promotes their professional awareness and fosters a strong identity development by its consideration of the occupational therapy’s historical and philosophical underpinnings. P37 mentioned as a main strength in the program its coverage of “Understanding the history and philosophy of occupational therapy”. Participants also highlighted that such focus is essential “Gives the whole picture of occupational therapy, includes most of theories and frames, can be relied on as basic knowledge” P43.
The occupational therapy curriculum also enhanced students’ professional growth and development by its focus on their skills of using research and evidence-based practice. P18 “[The curriculum is] rich in evidence-based practice, prepare graduates for strong self-educated people who always know how to make presentations and do research”. This enables them to be independent lifelong learners.
The fieldwork practice in addition to the theoretical courses enhances students’ skills of evaluation and intervention as well as their confidence and social skills. P9 illustrated that during the fieldwork “The students to handle patients with visual supervision is so good! To become more confident”. Nevertheless, the practical training assisted in “Strengthening practical skills, helping in building confidence in fieldwork, improving in presenting and in using standard assessments” P44. On the other hand, another group of students did not share the same experience in regard to their lab practical training. They demonstrated that it lacks to hands-on and many of the labs were the theoretical labs. P41 stated “Needs more hands-on implementation regarding the assessment and intervention… labs of occupational therapy are always theoretical, and nothing is practical to be learned to prepare students for real practice”. This disparity in opinions can be understood by looking at the second theme which discusses the available resources.
Theme Two: Teaching and Learning Resources
In the second found theme the focus was on assistance that the students received from the occupational therapy educators and in regard to the resources that were available to them to support their educational process.
Subtheme One: Occupational Therapy Educators
The occupational therapy educators included both the academics employed by the higher education institution (who delivered the didactic/theoretical teaching) and the clinical educators who were non-academics that delivered both the lab practical training and supervised students during their clinical fieldwork. Participants differentiated in their perspectives in regard to these two groups of educators. They were satisfied with the support provided by their academic educators, their diverse use of teaching techniques and the received guided instructions by them.
The participants illustrated that their practical training heavily depend on their clinical educators as some were very qualified. P12 “Some of them were good and some were not in terms of applying the theory part into clinical practice”. P81 described the fieldwork clinical educator “Was not always updated in knowledge, somehow weak with some instructions, repetitive even for trainees same knowledge was provided”. One of the participants suggested “Make sure that the supervisor wants or has knowledge and time about the area and is willing to teach” P26.
Another area of concern was with the inconsistency with the grading system and the received feedback from the clinical educators. P36 highlighted “Grades are different between clinical instructors, need more orientation, clinical instructors need training”. Nevertheless, the participants needed more constructive feedback on their work and practical application. P3 mentioned “Time was not enough for all the students to practice everything we took under the supervision of the teacher”.
Subtheme Two: Availability of Resources to Foster Students’ Practical Training
In this subtheme, two perspectives were found. A group of participants believed in the availability of useful resources of having adequate lab space and tools, and variety of practical materials and assessments available for practice. Whereas another group of participants used terms of crowded, inadequate equipment and limited time when asked about their lab training experience. P40 stated “Not enough time and space to let everyone practice sometimes”. P70 added “Limited space and equipment- no privacy when in neuro lab (partitions between beds)”. This second group had another concern in regard to their clinical fieldwork training about the number of students per their clinical educator, “many students with one supervisor” P43. P64 added “More than 3 students with one supervisor”.
Data Integration
Integration of Quantitative and Qualitative Findings
To further understand the found key points regarding satisfaction and agreement with the curriculum, findings from both approaches were synthesized and illustrated (see Figure 2). To illustrate, the quantitative findings were supported by qualitative responses. For example, while participants appreciated the strong foundation in professional behaviors and occupation-based models, they expressed concerns in the qualitative data about the lack of exposure to certain specialty areas, including women’s health, assistive technology, and neonatal therapy. Similarly, though the participants were generally satisfied with clinical placements in qualitative responses, they further highlighted inconsistent clinical supervision as a major challenge. Despite this, participants acknowledged the availability of variety of clinical placements opportunities. With regards to their laboratory teaching, two perspectives emerged. The non-experienced therapists highlighted overcrowding in labs and were generally less satisfied with the availability of tools considering the number of students when compared with the experienced therapists.
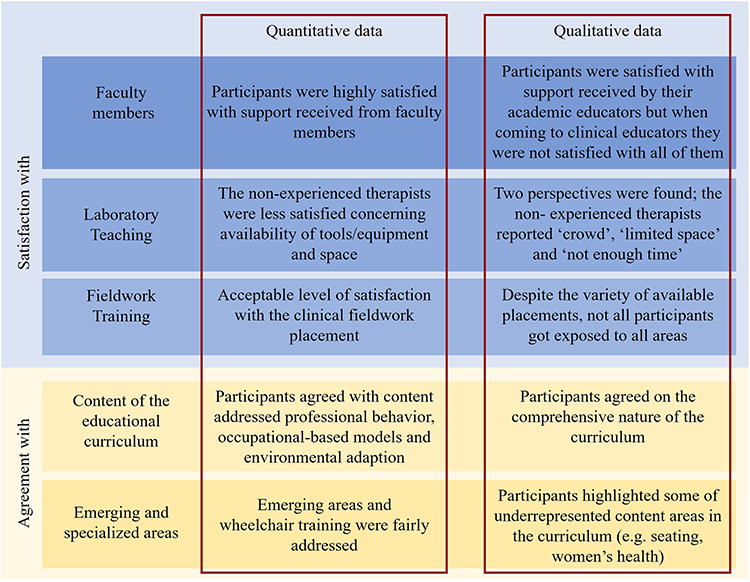 |
Figure 2 Integration of quantitative and qualitative findings. |
Discussion
In the present study, we investigated the perspectives of occupational therapy graduates regarding their occupational therapy educational program at Kuwait University; such perspectives were obtained through a mixed research design utilizing quantitative and qualitative methods. The study participants reported a high level of satisfaction with the support received from their faculty members during their educational experience. This finding aligns with established theories of student satisfaction, such as Tinto’s Student Integration Model and Astin’s Theory of Student Involvement, which suggest that strong faculty–student relationships contribute to enhanced learning outcomes and professional identity formation.32,33 Such support emerges from ongoing mentoring, listening to students’ concerns, exchanging feedback, and continuous guidance. Specific teaching methods, such as interactive learning strategies, personalized feedback, and mentorship practices, likely played a role in shaping this positive perception. Hence, the value of reflection and feedback, as well as mentor involvement, are important components of healthcare education; these components contribute positively to the competency development of graduates during their practice.34 In addition, the participants indicated that professional behavior was greatly emphasized within their curriculum. For example, dependability, organization, communication skills, interpersonal skills, and professional conduct were highly emphasized to students during their educational experiences whether in theoretical classes or when engaged in clinical training education. Professionalism is perceived as an integral part of occupational therapy education and considered a key factor for students’ learning and potentially contributes to the students’ personal changes in the future as practicing health care professionals.35,36 For the readers’ convenience, the professional behavior form utilized within the occupational therapy curriculum is provided in Supplementary File (S2).
Moreover, the educational program has adequately covered major theoretical underpinnings and concepts pertinent to occupational therapy. For example, the study participants agreed that occupation-based models and occupation-based assessments were incorporated and emphasized within their educational curriculum. Importantly, the emphasis on cultural contexts and social values of the Kuwaiti society is closely considered within the occupational therapy process, including the use of culturally relevant assessments in practice. Examples of these assessments include the Arabic versions of the Satisfaction with Daily Occupations (SDO) and Disability of Arm, Shoulder, and Hand (DASH), which are occupation-based, functionally oriented, culturally appropriate, and standardized outcome measures.37,38 Furthermore, in line with the published literature, some of the graduates indicated that the essence of intervention approaches that are client-centered, was incorporated in their educational curriculum.39 On the other hand, other graduates elaborated that most of evidence-based practices and frames of reference are not culturally based and not suitable to be applied in real practice, particularly within their clinical fieldwork experience. This raises a concern why some students observed limited application of culturally appropriate intervention in practice; this might be attributed to potential factors that acted as barriers of implementing interventions suitable for own culture, such as role of gender in therapy, patient’s belief of independence versus interdependence, self-awareness or bias about one’s own culture and/or limited understanding of others’ beliefs and cultural background.26,27,40 Thus, we recommend future studies to investigate the perspectives of students as well as occupational therapists concerning factors enabling and hindering the application of culturally based practice in Kuwait. Doing so would contribute to evidence-based occupational therapy practice that is scientifically driven and culturally appropriate.
Notably, as reported by the graduates, the emphasis on research skills and evidence-based practice were additionally emphasized within the curriculum. Having said that, the concepts of occupation-based, client-centered, and evidence-based practices are strongly believed to be central core concepts in occupational therapy theory and practice. As a result, these concepts continuously support the competency level of occupational therapy students and professionals, establish their professional identity and promote patients’ health and wellness.41 However, the curriculum showed limited coverage of emerging practice areas, such as dysphagia, seating, burns, assistive technology, women’s health, and neonatal therapy. While these areas are currently treated as subspecialties in our program, students expressed a desire for more content and practical exposure in these areas, highlighting a need to align the curriculum with evolving demands of the profession.42,43 To address this, we propose a structured review process involving practitioners and graduates to determine which emerging areas warrant integration as core competencies. The absence of sufficient content and hands-on training in these areas limits students’ exposure to specialized occupational therapy practices. Potential solutions could include specialized elective or certification modules, practical workshops, or targeted fieldwork placements in these sub-specialty areas to better equip students for emerging occupational therapy roles.
The study participants reported low satisfaction levels with the occupational therapy laboratory classes, particularly in terms of tools, equipment, and space. This limitation was echoed in both the quantitative and qualitative data, with participants highlighting the lack of hands-on implementation and the theoretical nature of many lab sessions. This inadequacy hinders the practical skills development necessary for effective clinical practice.44–46 To address the inadequacies in laboratory resources, it is essential to invest in upgrading the tools, equipment, and space available for occupational therapy laboratory classes. Implementing more practical, hands-on sessions will better prepare students for real-world clinical scenarios.45,47
The quality of clinical supervisors was an additional concern raised by participants. Inconsistencies in supervision may stem from variations in supervisor qualifications, clinical experience levels, and training in educational methodologies. Some students reported receiving strong mentorship, while others encountered supervisors who lacked up-to-date clinical knowledge or effective teaching skills. This inconsistency affected the participants’ clinical training experiences and their satisfaction with the feedback and grading system. Participants emphasized the need for clinical supervisors to be knowledgeable, willing to teach, and consistent in their evaluation methods.48–50 To enhance the quality of supervision, structured professional development programs should be implemented for clinical educators, focusing on teaching methodologies, evidence-based practices, and standardized assessment criteria. Additionally, reducing the student-to-supervisor ratio would allow for more personalized mentorship and practical skill development.
Furthermore, based on the present study results, compared with the non-experienced graduates, it was demonstrated that the experienced therapists significantly supported the notion that the biopsychosocial model was well-covered throughout the curriculum. This discrepancy may be linked to how the biopsychosocial model was introduced and reinforced during training. Experienced therapists, having applied this model in real-world settings, may recognize its practical integration within the curriculum, whereas non-experienced graduates may have found it difficult to contextualize in the absence of clinical exposure. In this regard, the literature supports the essence of incorporating the biopsychosocial model in practice, as it has been shown to enhance rehabilitation services and improve therapeutic outcomes.51
In addition, with relevance to the level of satisfaction among the graduates regarding occupational therapy laboratory classes in terms of space, the graduates with more clinical experience reported significantly higher satisfaction levels compared with non-experienced graduates (P=0.014). Similarly, the experienced graduates also indicated greater overall satisfaction concerning the support received from occupational therapy faculty members (P=0.035). This could be attributed to the fact that earlier batches of students experienced smaller class sizes and more individualized faculty attention, whereas later batches encountered larger student cohorts, leading to potential limitations in available faculty support.
Of note, though the academic faculty at the occupational therapy department are working extensively to manage these pragmatic issues, the increased number of students has led to faculty workload challenges, potentially impacting teaching quality and faculty well-being. In this regard, we strongly encourage the health sciences administration to consider providing more spacious labs as well as hiring additional faculty members to mitigate extra pressure and workload. Moreover, the university’s higher administration has a vital role in reviewing factors impacting the learning environment and providing legitimate solutions leading to quality teaching and a productive learning environment.
Study Implications and Future Directions
This study has notable strengths and implications that deserve future considerations. It is the first study addressing the perspectives of graduates concerning their occupational therapy educational program, as part of Kuwait University Health Science programs. This study therefore serves as the start for the curricular evaluation and monitoring among health sciences educational programs. Such assessments of various educational programs significantly add to the value of academic improvement and positive learning outcomes for university students.52 Thus, we suggest that occupational therapy programs, whether regional or international, should periodically review their educational programs to ensure an updated and scientifically driven of their programs. Doing so supports the dynamic change and trends within the occupational therapy profession.
In addition, the study’s findings open further avenues for research, particularly in curriculum enhancement and design and incorporation of practical culturally safe hands-on training. Moreover, as indicated in our study findings relevant to less emphasis on interprofessional education (IPE), we support the need for developing role playing and team-based case discussions among health science students for the purpose of improving their knowledge base toward each other’s professions. This facilitates positive IPE learning outcomes and support the professional identity and contributions of occupational therapy within the future rehabilitation team members.53 It can also provide quality learning experience for supervisors and students alike in diverse clinical settings.54–56 Most importantly, in order to promote replication of this study within different occupational therapy curricula globally, we recommend regional and international occupational therapy educators and researchers to utilize our study developed questionnaire as a guide for reviewing and assessing their educational curricula from the perspectives of students, graduates and/or clinicians thereby understanding and scrutinizing its scope, strengths, and weaknesses accordingly. Of note, we encourage examining further psychometric properties of the developed questionnaire as well as adding/modifying specific items to meet the tailored academic and cultural aspects particular to those occupational therapy educational programs. This will eventually contribute to the monitoring of occupational therapy educational curricula, guarantee better academic performance of students, and support desired clinical outcomes in the future.
Also, by identifying limitations relevant to clinical education within the occupational therapy curriculum, it drives academicians and researchers to address these weaknesses and consider proposing desired practical solutions accordingly. For example, train the trainers should be implemented to minimize differences and inconsistencies among clinical educators while evaluating students’ performance and providing consistent educational objectives. In other words, the clinical learning environment is a complex and multi-layered social environment in which educational institutions, academics and healthcare professionals should consider while developing curricula and teaching.57 Thus, academic educators have a great responsibility to develop a shared language to bridge the gap between pedagogy and clinical practice while considering the context of the clinical environment and ensuring alignment and conformity relevant to the taught curriculum, students’ clinical education experiences and the key roles of clinical educators within the process of clinical education.54,57 Notably, this study emphasizes the value of exchanging feedback between educators and students or graduates of the occupational therapy program. Doing so supports the essence of educational alliance between graduates (ie learners) and faculty members or clinical educators (teachers) to promote collaboration and provide invaluable insights into the advancement of educational curriculum and clinical learning environment.58 Preparedness for working in diverse healthcare environments enables new professionals to adapt to complex healthcare environments, uphold ethical and legal standards, collaborate across disciplines, and apply evidence-based practice ensuring patient safety, professional competency, and effective clinical decision-making. Nevertheless, it will improve further exploration on key aspects needed for further readiness and increased faculty resources in the alignment with international standards.
Study Limitations
The current study has several limitations that deserve attention. The developed questionnaire was not comprehensive regarding items relevant to the clinical supervisor support, or the types of support provided by the clinical supervisors within the clinical environment. This should be clearly indicated in future curriculum evaluation. Hence, clinical supervisors’ support can have profound impact on students’ learning and emotional wellbeing.59 Also, the sample of graduates was not randomly chosen thus limiting the generalizability of the study findings. In addition, due to the nature of the data collection process while administering the questionnaire through social media platforms, the timings of administering the questionnaire was not controllable as the participants filled it out in different timings. This could bring about bias and possibly affect the study findings. Therefore, future studies are encouraged to pay closer attention for such issue to minimize bias and ensure controlled outcomes. Moreover, though qualitative findings were utilized, relying only on general content analysis of the occupational therapy curriculum to analyze the results could be limited and less inclusive. For example, the specific emphasis on the role of culture in practice was overlooked and not fully elaborated upon. Having said that, future studies are therefore recommended to address the limitations of this exploratory study and build upon its shortcomings thereby ensuring improved students’ learning outcomes in classrooms as well as in clinical placements. Despite these limitations, we strongly believe that this study will contribute to the nature of curricular design, advancement of students’ academic learning and effective monitoring of educational curricula within the health science center.
Conclusions
To the best of our knowledge, this exploratory study was the first in the Health Science Center in Kuwait to investigate the perspectives of occupational therapy graduates regarding their educational curriculum. It was documented in the literature that exchanging feedback between educators and students or graduates can contribute to the advancement of educational curricula as well as improvements in the clinical learning environment. In this study, the perspectives of the graduates concerning their curriculum were satisfactory, mainly regarding theoretical courses, support received from faculty members, emphasis on professionalism, the value of applying occupation-based models, integration of occupation-based assessments, the use of intervention approaches that are client-centered, and the importance of utilizing the biopsychosocial model in practice.
On the other hand, the graduates emphasized areas requiring improvement, particularly in laboratory courses and clinical education in practice. Enhancing these aspects through increased hands-on training, updated laboratory resources, and structured clinical mentorship programs may be important for better preparing graduates. In addition, addressing the study limitations and building upon the study findings could strengthen the quality of occupational therapy education both locally and internationally. Future research is encouraged to explore the perspectives of other key stakeholders, such as employers, clinical supervisors, and patients, on graduate preparedness. Understanding employer expectations and patient outcomes may offer a more comprehensive evaluation of curriculum effectiveness and its impact on professional practice. Moreover, the study implications can also guide occupational therapy educational programs globally to conduct periodic reviews and assessments of their curricula, thereby supporting desired educational outcomes for their graduates. In turn, this may better position graduates who are well-equipped to meet the demands of occupational therapy practice within various clinical environments. Finally, this exploratory study will open a research avenue in the area of curriculum evaluation and monitoring, aiming to improve students’ learning experiences and support future rehabilitation outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. El-Haddad C, Hegazi I, Hu W. Understanding patient expectations of health care: a qualitative study. J Patient Exp. 2020;7(6):1724–1731. doi:10.1177/2374373520921692
2. Oster A, Wiking E, Nilsson GH, Olsson CB. Patients’ expectations of primary health care from both patients’ and physicians’ perspectives: a questionnaire study with a qualitative approach. BMC Primary Care. 2024;25(1):128. doi:10.1186/s12875-024-02389-2
3. Kalaja R. Determinants of patient satisfaction with health care: a literature review. Eur J Nat Sci Med. 2023;6(1):43–54. doi:10.2478/ejnsm-2023-0005
4. Chun I, Taff SD, Mehta A, Chang C-H. Identifying essential competency areas for occupational therapy education: a scoping review. J Occup Ther Educ. 2020;4(4):2. doi:10.26681/jote.2020.040402
5. World Federation of Occupational Therapists. Minimum Standards for the Education of Occupational Therapists 2016.
6. Naidoo D, Van Wyk JM. Competencies required to deliver a primary healthcare approach in the occupational therapy: a South African perspective. Occup Ther Int. 2023;2023(1):4965740. doi:10.1155/2023/4965740
7. Thomas A, Al Zoubi F, Mayo NE, et al. Individual and organizational factors associated with evidence‐based practice among physical and occupational therapy recent graduates: a cross‐sectional national study. J Eval Clin Pract. 2021;27(5):1044–1055. doi:10.1111/jep.13518
8. Braveman B. Population health and occupational therapy. Am J Occup Ther. 2016;70(1):7001090010p1–7001090010p6. doi:10.5014/ajot.2016.701002
9. Craik C, McKay EA. Consultant therapists: recognising and developing expertise. Br J Occup Ther. 2003;66(6):281–283. doi:10.1177/030802260306600608
10. Robertson LJ, Griffiths S. Graduates’ reflections on their preparation for practice. Br J Occup Ther. 2009;72(3):125–132. doi:10.1177/030802260907200307
11. Liddiard K, Batten R, Wang Y, Long K, Wallis A, Brown CA. Job club: a program to assist occupational therapy students’ transition to practice. Educ Sci. 2017;7(3):70. doi:10.3390/educsci7030070
12. Naidoo D, Van Wyk J, Waggie F. Occupational therapy graduates’ reflections on their ability to cope with primary healthcare and rural practice during community service. South Afr J Occup Ther. 2017;47(3):39–45. doi:10.17159/2310-3833/2017/v47n3a7
13. Hodgetts S, Hollis V, Triska O, Dennis S, Madill H, Taylor E. Occupational therapy students’ and graduates’ satisfaction with professional education and preparedness for practice. Can J Occup Ther. 2007;74(3):148–160. doi:10.1177/000841740707400303
14. von Zweck C, Ledgerd R, Shann S, Mlambo T. A global survey on occupational therapy education: findings and implications for diploma level education. World Federat Occup Therap Bull. 2023;79(2):173–182. doi:10.1080/14473828.2023.2174653
15. Hammell KRW. Occupation, well-being, and culture: theory and cultural humility/Occupation, bien-être et culture: la théorie et l’humilité culturelle. Can J Occup Ther. 2013;80(4):224–234. doi:10.1177/0008417413500465
16. Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol. 2001;27(1):363–385. doi:10.1146/annurev.soc.27.1.363
17. Mahoney WJ, Kiraly-Alvarez AF. Challenging the status quo: infusing non-Western ideas into occupational therapy education and practice. Open J Occup Ther. 2019;7(3):1–10. doi:10.15453/2168-6408.1592
18. American Occupational Therapy Association. Occupational therapy practice framework: domain and process (4th ed.). Am J Occup Ther. 2020;74(Suppl. 2):1.
19. Fortune T, Ryan S, Adamson L. Transition to practice in supercomplex environments: are occupational therapy graduates adequately prepared? Austr Occup Ther J. 2013;60(3):217–220. doi:10.1111/1440-1630.12010
20. Scanlan JN, Meredith PJ, Haracz K, et al. Mental health education in occupational therapy professional preparation programs: alignment between clinician priorities and coverage in university curricula. Austr Occup Ther J. 2017;64(6):436–447. doi:10.1111/1440-1630.12397
21. Walder K, Bissett M, Molineux M, Whiteford G. Understanding professional identity in occupational therapy: a scoping review. Scand J Occup Ther. 2022;29(3):175–197. doi:10.1080/11038128.2021.1974548
22. Cho E, Osenga S, Forwell S, Lee Bunting K. Understanding occupation in Canada: recent graduates’ perspectives. Scand J Occup Ther. 2023;30(4):488–496. doi:10.1080/11038128.2023.2173646
23. Kirke P, Layton N, Sim J. Informing fieldwork design: key elements to quality in fieldwork education for undergraduate occupational therapy students. Austr Occup Ther J. 2007;54:S13–S22.
24. World Federation of Occupational Therapists. Kuwait University Bachelor of Science. 2024. Available from: https://wfot.org/education-programmes/bachelor-of-science-4.
25. Öhlböck E, Stinson M, McClintock K, Turtle B. Evaluating the effectiveness of key components of Zones of Regulation™ curriculum training on teachers’ self‐efficacy at managing self‐regulation needs in autistic pupils. Brit J Special Educ. 2024;51(1):111–122. doi:10.1111/1467-8578.12501
26. Malkawi SH, Alqatarneh NS, Fehringer EK. The influence of culture on occupational therapy practice in Jordan. Occup Ther Int. 2020;2020(1):1092805. doi:10.1155/2020/1092805
27. Babish YR, Nammoura L, Abu-Asabeh K. The effects of culture and gender on occupational therapy practice for adults: from palestinian therapists’ perspective. Occup Ther Health Care. 2025;39(3):593–612. doi:10.1080/07380577.2024.2366331
28. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
29. Moran-Ellis J, Alexander VD, Cronin A, et al. Triangulation and integration: processes, claims and implications. Qual Res. 2006;6(1):45–59. doi:10.1177/1468794106058870
30. O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ. 2010;341:c4587. doi:10.1136/bmj.c4587
31. Mertens DM. Research and Evaluation in Education and Psychology: Integrating Diversity with Quantitative, Qualitative and Mixed Methods.
32. Astin AW. Student involvement: a developmental theory for higher education. 1999.
33. Astin AW. Student involvement: a developmental theory for higher education. J College Student Personnel. 1984;25:297–308.
34. Janssens O, Andreou V, Embo M, et al. The identification of requirements for competency development during work-integrated learning in healthcare education. BMC Med Educ. 2024;24(1):427. doi:10.1186/s12909-024-05428-9
35. Chien C-W, Chloe Mo SY, Chow J. Using an international role-modeling pedagogy to engage first-year occupational therapy students in learning professionalism. Am J Occup Ther. 2020;74(6):7406205060p1–7406205060p11. doi:10.5014/ajot.2020.039859
36. Gurley TA, DeCleene Huber KE, Chen A, et al. Professional behavior attributes: a survey of occupational therapy faculty perspectives. J Occup Ther Educ. 2022;6(1):9. doi:10.26681/jote.2022.060109
37. Manee F, Alotaibi N, Alobaidly F, Abu Tariah H, Hamed R, Eklund M. The psychometric properties of the Arabic version of the Satisfaction with Daily Occupations. Br J Occup Ther. 2015;78(4):260–267. doi:10.1177/0308022614557629
38. Alotaibi NM, Aljadi SH, Alrowayeh HN. Reliability, validity and responsiveness of the Arabic version of the disability of arm, shoulder and hand (DASH-Arabic). Disability Rehabil. 2016;38(25):2469–2478. doi:10.3109/09638288.2015.1136846
39. Wallengren C, Billig H, Björkman I, et al. Person-centered care content in medicine, occupational therapy, nursing, and physiotherapy education programs. BMC Med Educ. 2022;22(1):492. doi:10.1186/s12909-022-03502-8
40. Sonn I, Vermeulen N. Occupational therapy students’ experiences and perceptions of culture during fieldwork education. South Afr J Occup Ther. 2018;48(1):34–39. doi:10.17159/2310-3833/2018/vol48n1a7
41. O’Mahony SE, Joosten AV, O’Brien J. An exploratory study: undergraduates’ perspectives on how threshold concepts influence professional identity. Can J Occup Ther. 2023;90(4):374–383. doi:10.1177/00084174231154747
42. Tokolahi E, Robinson R. A scoping review of role-emerging, school-based fieldwork placements in occupational therapy education. New Zealand J Occup Ther. 2021;68(2):26–33.
43. Murphy CJ, Calk PT. Creating evidence-based practitioners: bridging the gap between the classroom and clinic. J Interprofessional Pract Collaboration. 2020;2(1):2.
44. Kriegseisen-Peruzzi M. Bridging theory and practice in OT education at the university of applied sciences for health professions upper Austria. World Federat Occup Therap Bull. 2016;72(1):49–50. doi:10.1080/14473828.2016.1151687
45. Zahedi H, Rowe S-J. Evaluation of an on-campus program bridging the theory-practice gap in occupational therapy education: student perspective. J Occup Ther Educ. 2021;5(3):1. doi:10.26681/jote.2021.050301
46. Howarth JT, Morris K, Cox DL. Challenges of teaching occupation: introduction of an occupation focused teaching tool. J Occup Sci. 2018;25(1):142–148. doi:10.1080/14427591.2017.1397535
47. Espiritu EW, McClain H, Phillippi RD. Recommendations for academic programs to best support occupational therapy students: student perspectives. J Occup Ther Educ. 2024;8(2):3. doi:10.26681/jote.2024.080203
48. Pashmdarfard M, Mehraban AH, Shafaroodi N, Arabshahi KS, Parvizy S. Strategies to promote the quality of occupational therapy fieldwork education: a qualitative study. Med J Islamic Republic Iran. 2022;36:1.
49. King C, Edlington T, Williams B. The “ideal” clinical supervision environment in nursing and allied health. J Multidisciplinary Healthcare. 2020;13:187–196. doi:10.2147/JMDH.S239559
50. Roberts MJ, Fitzgerald D, Molineux M. Educating occupational therapists in the use of theory and evidence to enhance supervision practice. Open J Occup Ther. 2017;5(4):10. doi:10.15453/2168-6408.1356
51. Liddiard KJ, Raynor AJ, DeJong H, Brown CA. The experience of meaningful rehabilitation as perceived by people with chronic pain: a phenomenological study. Work. 2023;75(2):689–701. doi:10.3233/WOR-220119
52. Forero DA, Adan A, Perry G, Majeed MH. Global perspectives and recommendations for curriculum design in academic programs in the health sciences. Educación Médica. 2022;23(2):100728. doi:10.1016/j.edumed.2022.100728
53. Ciani GJ, Grimaldi G, Macalintal M, Orner D. the impact of interprofessional education on health profession students’ professional identity. Educ Sci. 2023;13(5):494. doi:10.3390/educsci13050494
54. Remesh A. Curriculum design principles for developing a module in medical education. Pro Med Sci. 2017;1(1):34–37. doi:10.5455/pms.20171223064024
55. Komenda M, Karolyi M, Pokorná A, Vaitsis C. Medical and healthcare curriculum exploratory analysis. In: Informatics for Health: Connected Citizen-Led Wellness and Population Health. IOS Press; 2017:231–235.
56. Khanna P, Roberts C, Lane AS. Designing health professional education curricula using systems thinking perspectives. BMC Med Educ. 2021;21:1–8. doi:10.1186/s12909-020-02442-5
57. Ahmady S, Khani H. The situational analysis of teaching-learning in clinical education in Iran: a postmodern grounded theory study. BMC Med Educ. 2022;22(1):520. doi:10.1186/s12909-022-03577-3
58. Bing-You R, Ramani S, Ramesh S, et al. The interplay between residency program culture and feedback culture: a cross-sectional study exploring perceptions of residents at three institutions. Med Educ Online. 2019;24(1):1611296. doi:10.1080/10872981.2019.1611296
59. Javornická D, Kisvetrová H, Prušová E, Váverková R, Greaves PJ, Steven A. The influence of supervisory support on clinical learning as experienced by Czech Nursing and health professional students in the context of patient safety events: a qualitative study. Nurse Educ Pract. 2024;79:104041. doi:10.1016/j.nepr.2024.104041
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.