Back to Journals » Advances in Medical Education and Practice » Volume 16
Reflecting on Students’ Experiences with Innovative Teaching Models in Clinical Placement: A Qualitative Study
Authors Feng S, Yang D, Zhang K, Yuan G, Tang H, Findlay D, Thomas AR, MacKinnon LS ![]() , Kuang M
, Kuang M ![]() , Xiao H, Xu D
, Xiao H, Xu D ![]()
Received 3 May 2025
Accepted for publication 4 July 2025
Published 1 October 2025 Volume 2025:16 Pages 1805—1814
DOI https://doi.org/10.2147/AMEP.S532673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Shaoting Feng,1,* Daya Yang,1,* Kunsong Zhang,1,* Gang Yuan,1 Hao Tang,1 Denise Findlay,2 Adam R Thomas,2 Lewis S MacKinnon,2 Ming Kuang,1 Haipeng Xiao,1 Dan Xu1,2
1First Affiliated Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Curtin Medical School, Faculty of Health Sciences, Curtin University, Perth, Australia
*These authors contributed equally to this work
Correspondence: Dan Xu, Email [email protected] Ming Kuang, Email [email protected]
Background: General practice (GP) placement teaching can be challenging because of time constraints, ineffective teaching models, and a lack of consensus approaches. GP clinics are more frequently used for undergraduate students’ learning to translate theoretical knowledge into clinical practice. Evidence suggests that a learner-centred approach is essential for facilitating deeper learning. “Student-led consultation under supervision” is one such learner-centred teaching model applied during GP placement, engaging both trainers and trainees in applying the core values of clinical thinking. This qualitative study intends to explore students’ learning outcomes when implementing the innovative teaching model “Student-led consultation under supervision during GP clinical placement” for potential quantitative introduction as a formal GP placement curriculum.
Methods: A convergent mixed-method approach was applied using validated surveys and pre-designed questionnaires for individual reflection when implementing innovative teaching models in medical students’ GP placements. Thirty-five medical students from China and Australia participated in the study. Survey and reflection data were collected for descriptive and semantic analysis.
Results: “Student-led consultation under supervision in a consultant’s chair with discussion” was the students’ most highly rated teaching model. Students’ reflections on the use of these teaching models were semantically analysed using a validated questionnaire. The students’ reflections highlighted the perceived academic benefits with identifying the enablers of and barriers to developing the formal GP placement curriculum.
Conclusion: This study shows that “Student-led consultation under supervision in a consultant’s chair with discussion” is innovative in GP teaching. The demonstrated innovation embraces the concept of cognitive apprenticeship for improving learning outcomes. These teaching models incorporate students’ reflection in curriculum design and extend the definitions of “cognitive apprenticeship” and “transfer of learning” in modern clinical teaching to improve trainees’ placement learning. The identified enablers of and barriers to implementing these innovative teaching models will pave the way for future studies to confirm the practicality of implementing them in real-life clinical practice.
Keywords: innovative training methods, general practice placement teaching, clinical thinking, clinical education, cognitive apprenticeship, action learning
Introduction
Training medical students in general practice (GP) placements can be problematic because of a lack of available time, ineffective teaching models, and a lack of standardised approaches.1,2 As didactic lectures and simulated teaching provide students with theoretical knowledge and simulated clinical experiences, bedside inpatient ward (BIW) teaching, general practice clinic (GPC), and hospital outpatient clinic (HOPC) teaching help to apply this knowledge and experience to real-life practical experience. BIW teaching, which takes place at the bedside on the inpatient ward, can deliver practical learning experiences but may be limited by the volume of patients and the lack of diversity of conditions presented.3,4 Recent evidence suggests that GPC and HOPC are frequently used in students’ teaching and learning to translate theoretical knowledge into practical learning experiences.5,6 Both GPC and HOPC have been shown to play important roles in undergraduate clinical placement.2,6 However, ineffective teaching models and a lack of standardised approaches have hindered students’ practical learning, and may widen the gap between theory and practice.1,2 The application of a learner-centred approach has been shown to narrow the gap and facilitate in-depth learning.7 Research shows that “Student-led consultation under supervision” is the ideal teaching model in clinical placements of HOPC and GPC.6,8 This teaching model is innovative in engaging both supervisors and students in exercising the core values of clinical reasoning: clinical thinking, clinical assessment, choosing wisely for investigation, problem list formulation and treatment plan, and consensus clinical decision-making, by letting students play the consultants’ roles.9 Our study uses validated surveys to rank students’ preferences for different teaching models and interviews students to ask them to reflect on the innovative teaching model of “Student-led consultation under supervision in a consultant’s chair with discussion”. The innovation extends the basic learner-centred model of “Student-led consultation under supervision” to “Student-led consultation under supervision in a consultant’s chair with discussion”, which enables students to experience a full consultation with a patient, with the observer being the supervising doctor. The analysis of students’ reflections will help to identify enablers and barriers and indicate the feasibility of implementation of the model as a formal GP placement curriculum. This study will also discuss students’ feedback regarding this teaching model’s limitations and barriers to implementation, with a plan for future research to determine whether it enhances academic performance and translates into clinical competence in career clinical practice.
Materials and Methods
Study Design
A convergent mixed-method approach was applied using validated surveys and pre-designed questionnaires for individual reflection when implementing innovative teaching models in medical students’ GP placements. Twenty participants from Australia and 15 participants from China participated in the study at five participating GPCs. All 35 participants read the provided participant information and agreed to participate by signing the consent form prior to the commencement of their clinical placements at the five participating GPCs. The informed consent particularly included the publishing of anonymised quotes captured during the individual reflection. The validated survey and interview reflection questionnaires were designed and modified by a few of the co-authors based on previously published studies.10–13 All data were collected from Australian students during their 4 weeks of GP placements from 2020 to 2024, whereas data from Chinese students were collected during their 4-week elective exchange placements at GPCs in Australia from 2017 to 2019. The detailed time schedules for the different teaching models for the students are given in Table 1; different exposure times to student-led teaching models existed between Australian students (30 hours per week) and Chinese students (20 hours per week) because of different university curriculum designs for GP placement. The supervisors observed and assessed the student-led consultations, while the participating students completed the survey on the teaching models at the end of the placement. The survey was completed anonymously and collected for data analysis by independent researchers. The individual interviews for reflection were conducted in English by the supervisor at the conclusion of the placement, with steps of semantic analysis including transcript review, data coding framework establishment, interpretation of coded data, and theme development and concept formulation. A detailed description of the various teaching models is presented in Table 2.
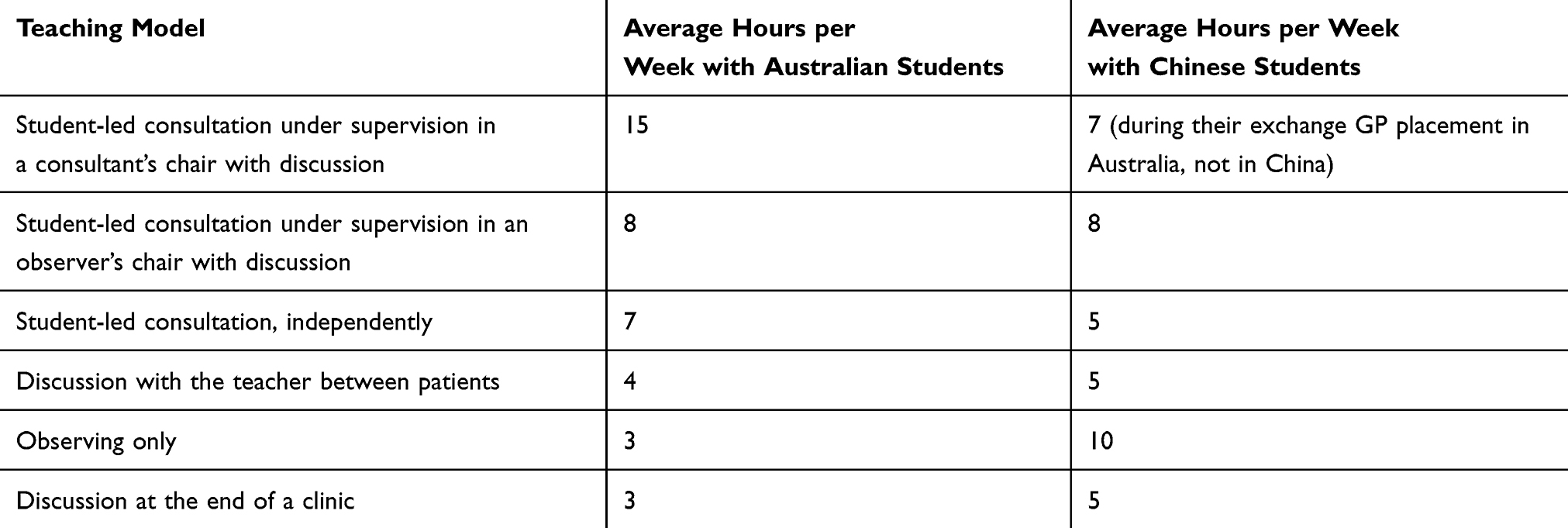 |
Table 1 Duration of Various Teaching Models Applied During General Practice (GP) Placements |
 |
Table 2 Ranking Survey and Detailed Description of the Six Different Teaching Models by Both Australian and Chinese Students |
Teaching Model Ranking and Individual Interview Reflection
This study applied a validated and modified survey instrument used in previously published studies10–13 for rating teaching models (Table 2) in GP placement, while reflections from individual interviews with all participating students were collected at the end of the placements.10–13 The trainers interacted with the trainees in such a way as to maximise the delivery of specific learning objectives (Table 2). The trainers booked three to five consultations per hour with students during their sessions (Table 2). A parallel convergent design14 was adopted in this research, as quantitative survey data and qualitative reflection were collected and analysed concurrently in the same phase of GP placement. Convergent parallel design includes the simultaneous execution of quantitative and qualitative components in the same stage of the research, weighs the methods equally, analyses the two components independently, and interprets the outcomes concurrently.14 This training approach, “Student-led consultation under supervision in a consultant’s chair with discussion”, demonstrates a three-way clinical communication, with the trainee doctor leading the clinical encounter; the training doctor overseeing as well as assisting with communication at critical decision-making points including focus history-taking, relevant physical examination, appropriate investigation, problem list definition and treatment; and the patient receiving a mutually agreeable treatment plan after patient-centred education by the student doctor’s explanation and reassurance. The approach applies either the training doctor or the trainee doctor starting a three-way clinical communication, as follows: 1) when finishing the history-taking and physical examination; 2) when formulating the required problem lists; and 3) when discussing the treatment plan to achieve patients’ understanding on the implementation of the novel approach.
The interview used pre-designed questionnaires published in previous studies10–13 to collect students’ reflections on the implementation of innovative teaching models (Table 3). The interviewers were independent researchers, instead of the students’ clinical supervisors, to ensure the validity and reliability of the reflection data. Prior to the interview, the supervisors confirmed the students’ understanding of clinical reasoning, learning, and clinical competence, as well as other medical educational concepts in the questionnaire.
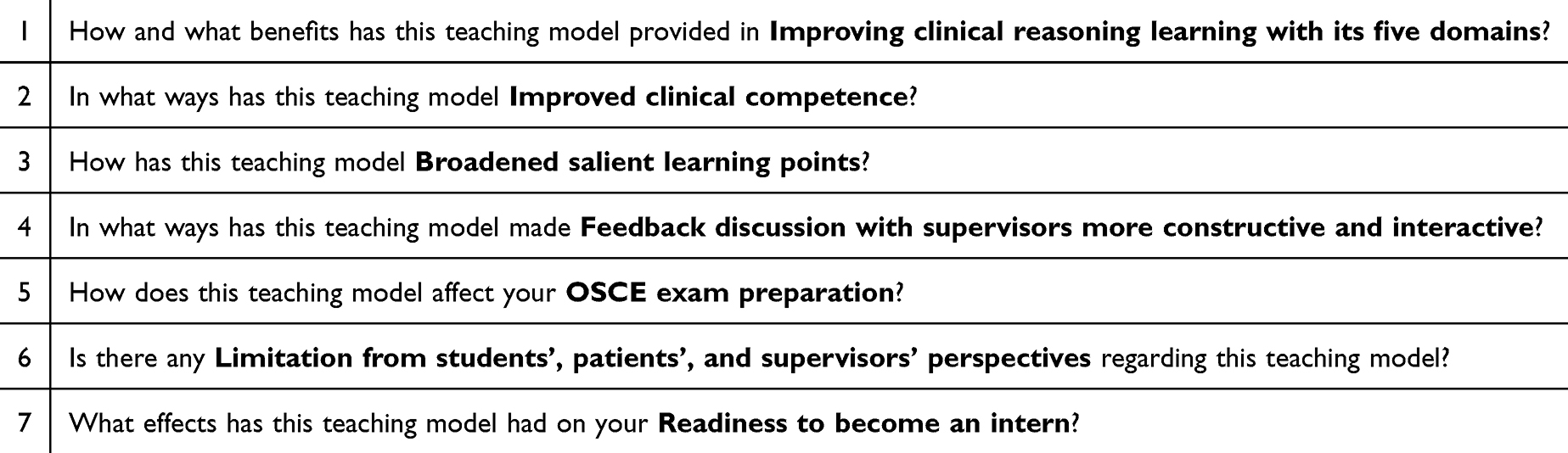 |
Table 3 Seven Pre-Designed Questions Included in the Interview Questionnaire |
Data Analysis
The authors undertook descriptive and semantic analysis of the qualitative reflections from the individual interviews.14 The qualitative reflection data from individual interviews were subjected to the steps of semantic analysis,15 including transcript review and data coding by two independent research co-authors, and interpretation of the coded data with the development of emerging themes by the main author.
Results
Thirty-five students ranked the different teaching methods (Table 2). “Student-led consultation under supervision in a consultant’s chair with discussion” was ranked best (33/35). “Student-led consultation under supervision in an observer’s chair with discussion” ranked second best (32/35). These two most preferred teaching models had a booking timeframe of three patients per hour, 15 minutes’ consultation, and 5 minutes’ discussion.
The emerging teaching and learning themes generated from students’ reflections highlight the core values of clinical thinking and reasoning.9 Individual student reflection following the semantic analysis is illustrated by the following emerging themes.
Clinical Thinking
Student 1: In contrast to the old style of being a shadow learner, I can formulate my own clinical thinking rather than trying to copy others, ultimately boosting applied knowledge and practical skill advancement and retention.
This learning style gave me confidence in my ability to tackle unfamiliar learning situations and environments. As a student, I am inclined to avoid learning opportunities in situations beyond my capability; however, I was repeatedly placed in situations [that were] unfamiliar, with the supervisor’s safety net. I learned that my initial poor performance was in a safe environment, which enabled me to improve on my mistakes. I felt uncomfortable, allowing me to throw myself into future learning opportunities. Another downside I perceived was the lengthy consultation time; however, I rarely observed any negative comments from the patients.
Clinical Assessment
Student 2: Student-led consultation at [the] consultant’s chair needs a succinct history-taking and relevant physical examination, in contrast to university-level full history and examination. By practising clinical skills in a time-aware manner with full involvement, I found the clinical signs and management more memorable, enabling the connection of pathology to real-life cases. Applicable knowledge is further cemented during the later study period owing to the supervisor’s application of this innovative teaching model. My negative comments were [that] the lack of prior knowledge and skill may compromise the efficiency of care delivery.
Choosing Wisely for Investigation
Student 3: Learning how to realistically plan investigations in the context of a patient’s clinical assessment without blindly accepting trainers’ comments on investigation choice. More precisely, aligning investigations target[ed] towards problem lists and treatment plan[s]. This teaching model enables my daily practice to apply the concept of “Choosing Wisely”. My only concern was the potential inadequate investigation, which may cause unnecessary anxiety to the patient.
Problem List Formulation and Treatment Plan
Student 4: Supervisors’ expertise feedback “fine-tunes” and consolidates the student’s clinical thinking of establishing a broad list of differential diagnoses with a clear outline of “common” and” not to be missed” diagnoses. Receptionists are appreciated for comforting the waiting patients because our problem list creation and management took extra time, which was one of my concerns with patient’s waiting time.
Consensus Clinical Decision-Making
Student 5: The unique training model enables multidisciplinary advice for [a] consensus treatment plan with most patients. Allied health has always made a significant contribution [to] the final consensus treatment plan. We appreciate these opportunities for clinical interaction with allied health staff and were prepared to take this learning in a culturally appropriate manner on board [to] our clinical practice in China to share with our colleagues. My only negative comment was of the potential cultural barriers [to] implementing this teaching and training model in China.
Clinical Competency
Student 6: Being in the consultant’s chair is an opportunity for the trainees; it consolidates their learning and identifies what [the] trainee needs to extend the learning. Practical skills that are often not taught in the classroom include note-taking, referral-writing, writing-investigation, prescribing medications, and minor procedures. Dedicated supervisors design up-to-date placement curriculum to empower trainees taking ownership of their learning for improving their clinical competencies. My only worry was [that] the extra time with the supervisors may interfere with their work schedule.
Important Take-Home Messages
Student 7: Assuming [the] GP’s role is a unique and well-designed model for trainees to improve their clinical conversation skills, such as how to deliver adverse outcomes, motivational counselling, and managing a diverse variety of challenging emotional issues. In assuming the consultant’s role, students assume responsibility for their patients with follow-up, making my learning productive and rewarding. However, my downside concern was the added time for both the supervisor and the patient.
Reflection Interview with a Trainer
Student 8: The reflection interview with trainers enables feedback on both the positive and negative aspects of the swapped chair method, demonstrating the most practical part where the trainer can discuss where I went wrong and fill in anything I may have missed. Finally, I anticipate the teaching model’s application to all placements to ensure our training standards. If I need to comment on the downside, my only concern was [that] the extra time added to the supervisor may affect the supervisor’s clinical duty.
Positive Input with OSCE Practice
Student 9: Every patient encounter is similar to that of an OSCE exam case, [but] better … owing to prompt discussion on students’ clinical performance. I strongly believe that there is no better form for preparation. Our GP supervisor should claim credit for applying this unique teaching model.
Limitations from Students’, Patients’, and Supervisors’ Perspectives
Student 10: The downside of this teaching is the length of consultations for patients with extra time for supervisor–student discussions. Another disadvantage of these consultations is that they require more pre-reading knowledge from students to perform the consultation at a satisfactory level, which can also be seen as an enabler for student-initiated proactive learning appreciated by supervisors and patients.
Positive Experiences for Competent Practice as Junior Doctors
Student 11: I feel that this experience has enabled me to progress my clinical competency to the level of a junior doctor, in particular [by] delivering more confident bedside care for initiating [an] investigation and establishing [a] treatment plan, as this responsibility will usually be the senior doctors’ responsibility. I acknowledge this teaching model as intern-readiness training to facilitate smooth transition to competent interns. My main concern was [that] the extra time needed from both supervisors and patients may, rarely, lead to unnecessary anxiety.
Enablers and Barriers
We identified several enablers, including dedicated supervisors, supportive administrative staff, cooperative patients, and appropriate consulting rooms. Barriers include a lack of time for supervisors, clinical safety, overloaded administrative staff, patients who are in a hurry, and inadequately equipped consulting rooms.
Discussion
The teaching model of “Student-led consultation under supervision in a consultant’s chair with discussion” has mirrored two closely aligned educational terms, namely, “cognitive apprenticeship” and “action learning”.
The concept of a cognitive apprenticeship can be summarised as an experience of cognitively obtaining and mastering practical knowledge and skills under supervision, rather than merely obtaining physical skills,16 and is about the ultimate development of the complete set of cognitive skills through authentic supervised practices.17 The process of cognitive apprenticeship needs to expose the clinical thinking to improve learners’ understanding, which is achieved by supervisors externalising their thinking to enable the learners’ eventual independent practice. Table 4 shows seven frameworks of the cognitive apprenticeship,16,18 centred on the definitions of situatedness and legitimate peripheral participation.19 The definition of “situatedness” corresponds to student-led consultation in a consultant’s chair in this study. In making the term “legitimate peripheral participation” relevant to this study, the training approach of “Student-led consultation under supervision in a consultant’s chair with discussion” has shown the use of three out of seven frameworks of cognitive apprenticeships by trainers for teaching students to practise proactive listening through observation, consultation in the GP’s chair under supervision, constant self-reflection, and exploration of their own clinical thinking. This training approach has also demonstrated an evidenced-based learner-centred approach7 in clinically legitimate settings, which has shown benefits in terms of students’ development of clinical thinking and reasoning.20 Stalmeijer et al20 introduced the concept of “cognitive apprenticeship” into clinical placement teaching owing to its positive outcomes in medical students’ placement learning. This concept has since been commonly applied in postgraduate specialist training.21 The ultimate goal of cognitive apprenticeship is to provide scaffolding support so that young practitioners can start to develop their own clinical thinking ability for career competent practice. Our teaching model of “Student-led consultation under supervision in a consultant’s chair with discussion” is similar to the concept of cognitive apprenticeship, with students’ feedback stating improved clinical reasoning skills and clinical competence. Furthermore, the students’ reflections demonstrated the constant use of frameworks of cognitive apprenticeships, including “reflection”, “articulation”, and “exploration”, for reviewing trainers’ feedback and reflecting on the interactive discussion with their supervisors to facilitate advanced learning. The removal of supervision is debatable owing to a number of factors compromising clinical care. One student reflects that most students worry about the management plan, especially during parallel consultations when students run independent consultations.
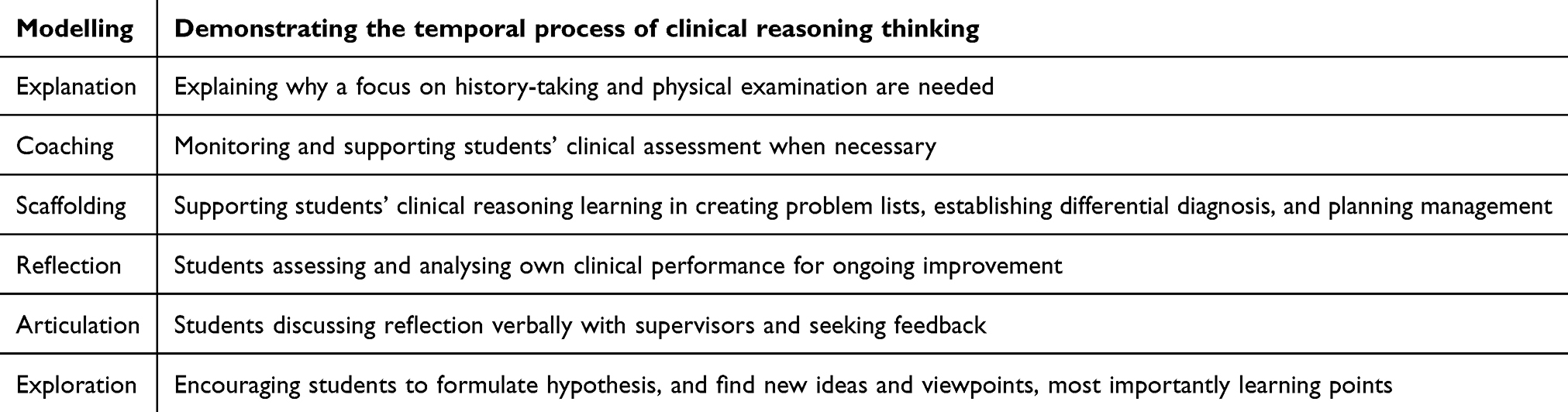 |
Table 4 Methods Supporting the Goals of Cognitive Apprenticeship |
Another outstanding point in trainees’ reflections highlights the capacity building of taking ownership of individual clinical thinking, and showcases the concept of “action learning” through the cognitive apprenticeship. Action learning is defined as the practical and productive application of prior learning and experience in novel contexts.22 This is part of the method in which we define a “novel context” as the practical application of the novel teaching model, a real-life consultation that differs from the original classroom setting.23
Action learning in medical education is a process of complex problem-solving in which the student constantly takes action and reflects on learning points. A previous study demonstrated that action learning may facilitate the successful transfer of learning into practice in learning clinical communication skills.24 In our study, the more precise definition is “supervised action learning”, with students taking action under supervision and undertaking excellent reflection on the novel teaching model. The Chinese students reflected that they would continue this teaching model into their junior doctor’s career learning and ongoing professional development to ensure the constant progression of clinical competency towards becoming a senior clinician. There was a slight difference in reflection between the Australian and Chinese students. Chinese students had more unique experiences with this teaching model during GP placement in Australia because they had not experienced this teaching model in China. They also reflected that they gained a more in-depth understanding of the core value of clinical thinking, especially in shared clinical decision-making, which features interprofessional and multidisciplinary discussion. Australian students highlighted their improvement in clinical thinking regarding clinical assessment, choosing wisely for investigation, problem list formulation and treatment plans, and consensus clinical decision-making. They were impressed by their clinical thinking for the focus history and physical examination during short GP consultation. In formulating the problem list and treatment plan, clinical thinking was highlighted in identifying “not to be missed” diagnoses. In reaching the consensus clinical decision-making, they gained a deeper understanding of safe clinical service delivery from ethical, medicolegal, and cultural perspectives. All students placed great value on the benefits of the teaching model in enhancing their clinical competency, objective structured clinical examination (OSCE) preparation, and intern readiness, with all students passing the final-year OSCE, recognising the significant contribution of their preparation using this teaching model. Chinese students reflected that cultural beliefs could limit the application of this training method because of the lack of trust in student doctors in Chinese communities.25 Another emerging limitation is a lack of time commitment, which could impair both patients’ safety and students’ learning. Previous research has shown that a lack of time commitment can be an obstacle to teaching in clinics, implying a need for dedicated clinical teaching time.26 However, our students positively reflected that this limitation could drive better-quality consultations and benefit patient education as a result of the extra time spent in ensuring the full comprehension of the treatment plan. Designated teaching clinics in GP placement have been proven to minimise these limitations for Australian students but not for Chinese students. Research in China indicates that this teaching model has been implemented in designated teaching clinics to train interns and junior doctors in their specialties.25
Furthermore, recent research on educational interventions has focused on improving clinical competencies in undergraduate settings, with structured interventions targeting clinical documentation.27 This review, by Emekli et al,27 supports the notion that focused educational efforts can enhance key aspects of clinical competence, such as medical record-keeping. The current study used verbal reflection in measuring the efficacy of this innovative teaching model on students’ progression of clinical competency, and the review by Franco et al28 on reflective writing similarly highlights the value of structured reflection in developing communication and professional skills for students in clinical placements. The final discussion point regarding clinical competency progression for our study lies in another review, by Pierce et al,29 showing that the effectiveness of structured models such as SNAPPS (Summarise, Narrow, Analyse, Probe, Plan, Select) and OMP (One-Minute Preceptor) in improving clinical reasoning aligns with the rationale for using supervised student-led consultations in real patient settings.
Limitations
This pilot study has a few limitations in terms of setting and design because it is restricted to a small, non-random sample, drawn from only five GPCs with highly variable supervision structures. These limiting factors may compromise the transferability and credibility of our research findings. Furthermore, a 2018 study demonstrated that curricular designers have assigned clinical rotations for university-associated teaching clinics and multiple community clinics, with competent trainers taking on the role of undergraduate education.30 Thus, our study team is currently planning an extension study to address these limitations in order to improve the scientific credibility of the research findings. Other notable limitations are the study’s failure to address the cultural and institutional biases, interviewer influence, and response desirability bias. The cultural and institutional biases included the Chinese students in this pilot study having fewer hours in their placements than the Australian students because of the curriculum design. The Chinese students also reflected that the Chinese cultural influence may be a barrier to the implementation of the innovative teaching and training model. Our team is planning to include cultural factors in the extension study, with the aim of overcoming all of these limitations.
Conclusion
This pilot research shows that “Student-led consultation under supervision in a consultant’s chair with discussion” is innovative in GP teaching. The demonstrated innovation embraces the concept of cognitive apprenticeship for improving learning outcomes. With the implementation of this innovative model, trainees experience a better transfer of learning and are reassured in gaining confidence in their future career as competent medical practitioners. Considering the enablers of and barriers to implementation, future extension studies should recruit more senior-year students from the two universities to strengthen the evidence from this pilot study by overcoming the above-mentioned limitations, and also investigate whether cultural factors influence the implementation of the teaching innovation in Chinese GPCs and HOPCs. Ultimately, the results of this study could provide advice to education researchers and university academics on whether this innovative teaching model can be feasibly and quantitatively implemented in clinical placement.
Data Sharing Statement
The data for this research are not all publicly available, but are available upon reasonable request.
Ethics
This study was approved by the Human Ethics Research Committee at Curtin University and the First Affiliated Hospital of Sun Yat-sen University.
Acknowledgments
Shaoting Feng, Daya Yang and Kunsong Zhang are co-first authors for this study. The authors thank the staff at both Curtin Medical School of Curtin University and the First Affiliated Hospital of Sun Yat-sen University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Best J. Teaching medical students; Tips from the frontline. Aust Fam Physician. 2012;41:22–24.
2. Almoallim H, k A, Minguet J, Alotaibi M. Advantages and perspectives of teaching in outpatient clinics: a systematic review creative education. SciRes. 2015;6:1782–1789. doi:10.4236/ce.2015.616181
3. Dent J. Learning in ambulatory care. In: Walsh K, editor. Oxford Textbook of Medical Education. New York: Oxford University Press; 2013:221–231. doi:10.1093/med/9780199652679.003.0019
4. Denton G, Durning S, Hemmer P, Pangaro L. RESEARCH BASIC TO MEDICAL EDUCATION: a time and motion study of the effect of ambulatory medical students on the duration of general internal medicine clinics. Teaching Learning Med. 2005;17:285–289. doi:10.1207/s15328015tlm1703_15
5. General Medical Council. Recommendations on Undergraduate Medical Education. London: General Medical Council; 2009.
6. Ash JK, Walters LK, Prideaux DJ, Wilson IG. The context of clinical teaching and learning in Australia Medical. J Austr. 2012;196(7):1
7. Spencer JA, Jordan RK. Learner centred approaches in medical education. BMJ. 1999;318:1280–1283. doi:10.1136/bmj.318.7193.1280
8. Dallol B. Fruhstorfer B Is there a difference in the perception of outpatient clinic teaching, between medical students and teachers? A mixed method study. MedEd. 2019. doi:10.15694/mep.2019.000080.1
9. Cooper N, Bartlett M, Gay S, et al. On behalf of the UK clinical reasoning in medical education (CReME) consensus statement group Consensus statement on the content of clinical reasoning curricula in undergraduate medical education. Med Teach. 2021;43(2):152–159. doi:10.1080/0142159X.2020.1842343
10. Zhang J, Tang Y, Feng S, et al. Collaborative teaching and curricular integration in pre-intern clinical placements: insights from the Greater Bay area. Adv Med Educ Pract. 2024;15:1027–1037. doi:10.2147/AMEP.S471782
11. Feng S, Yang D, Zhang K, et al. Reflecting on experiences of senior medical students’ external clinical teaching visits in general practice placements: a pilot study. Adv Med Educ Pract. 2024;15:207–216. PMID: 38525099; PMCID: PMC10961076. doi:10.2147/AMEP.S454467
12. Feng S, Yang D, Zhang K, et al. Reflecting on experiences of GP trainees teaching senior medical students during GP placement: a pilot study. Aust J Gen Pract. 2024;2024:207–16.
13. Xu D, Feng S, Yang D, et al. Reflecting on students’ experiences of an innovative teaching model during aged care visit in clinical placements: a qualitative pilot study. Adv Med Educ Pract. 2023;14:1339–1346. PMID: 38046262; PMCID: PMC10693279. doi:10.2147/AMEP.S436905
14. Creswell J, Clark V. Designing and Conducting Mixed Method Research.
15. Naeem M, Ozuem W, Howell K, Ranfagni S. A step-by-step process of thematic analysis to develop a conceptual model in qualitative research. Int J Qual Meth. 2023;22. doi:10.1177/16094069231205789.
16. Collins A, Brown JS, Newman SE. Cognitive apprenticeship: teaching the crafts of reading, writing, and mathematics. In: Resnick L, editor. Knowing, Learning, and Instruction: Essays in Honor of Robert Glaser. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.; 1989.
17. Collins A, Brown JS, Holum A. Cognitive apprenticeship: making things visible. Am Educ. 1991;15(3):38–46.
18. Enkenberg J. Instructional design and emerging models in higher education. Computers Human Behav. 2001;17:495–506. doi:10.1016/S0747-5632(01)00021-8
19. Lave J. Wenger E Situated Learning: Legitimate Peripheral Participation. Cambridge: Cambridge university press; 1991.
20. Stalmeijer RE, Dolmans DHJM, Wolfhagen IHAP, Scherpbier AJJA. Scherpbier AJJA Cognitive apprenticeship in clinical practice: can it stimulate learning in the opinion of students? Adv Health Sci Educ. 2009;14:535–546. doi:10.1007/s10459-008-9136-0
21. Merritt C, Daniel M, Munzer BW, Nocera M, Ross JC, Santen SA. A cognitive apprenticeship-based faculty development intervention for emergency medicine educators. West J Emerg Med. 2018;19(1):198–204. doi:10.5811/westjem.2017.11.36429
22. Roediger III HL, Butler AC. The critical role of retrieval practice in long-term retention. Trends Cognitive Sci. 2011;15(1):20–27. doi:10.1016/j.tics.2010.09.003
23. Pan SC, Rickard TC. Transfer of test-enhanced learning: meta-analytic review and synthesis. Psychol Bull. 2018;144(7):710–756. doi:10.1037/bul0000151
24. Dowson J. Transferring knowledge into practice? Exploring the feasibility of action learning for improving knowledge, skills and confidence in clinical communication skills. BMC Med Educ. 2019;19(37). doi:10.1186/s12909-019-1467-4
25. Zeng Y, Zhu B, Tang D, Feng X, Zhang Y, Zhan Y. The application of teaching clinic in resident training. China Continuing Med Edu. 2020;12:
26. Franco RLO, Machado JLM, Grinbaum RS, Porfírio GJM. Barriers to outpatient education for medical students: a narrative review. Int J Med Educ. 2019;10:180–190. doi:10.5116/ijme.5d76.32c5
27. Emekli E, Ö C, Ii B. Medical record-keeping educational interventions for medical students and residents: a systematic review. Health Inf Manag. 2025;54(2):177–189. PMID: 39138837. doi:10.1177/18333583241269031
28. Franco RS, Franco CAGDS, Severo M, Ferreira MA, Karnieli-Miller O. Reflective writing in the teaching of communication skills for medical students: a systematic review. Patient Educ Couns. 2022;105(7):1842–1851. PMID: 35063310. doi:10.1016/j.pec.2022.01.003
29. Pierce C, Corral J, Aagaard E, Harnke B, Irby DM, Stickrath C. A BEME realist synthesis review of the effectiveness of teaching strategies used in the clinical setting on the development of clinical skills among health professionals: BEME Guide No. 61. Med Teach. 2020;42(6):604–615. PMID: 31961206. doi:10.1080/0142159X.2019.1708294
30. Moore K, Bacon R, Bevitt T, et al. Student-led clinical services within the university health clinic: Definition, educational practices and outcome. Focus Health Prof Educ. 2018;19(2):1–13. doi:10.11157/fohpe.v19i2.213
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.