Back to Journals » Clinical Ophthalmology » Volume 17
Refining the Diagnostic Technique to Determine Prevalence of Demodex Mites in Eyelash Hair Follicles Within Standard Ophthalmic Practice: A Single-Center Outpatient Clinical Study
Authors Boel C, Westerveld E, Kloos D, Goezinne F
Received 27 March 2023
Accepted for publication 17 June 2023
Published 17 July 2023 Volume 2023:17 Pages 2027—2036
DOI https://doi.org/10.2147/OPTH.S407898
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr John Miller
Charlotte Boel,1,2 Elianne Westerveld,3 Daniëlla Kloos,3 Fleur Goezinne1
1Eyescan Rijswijk, Rijswijk, the Netherlands; 2Department of Ophthalmology, University Hospital Brussels, Brussels, Belgium; 3Eyescan Warmond, Warmond, the Netherlands
Correspondence: Fleur Goezinne, Eyescan Rijswijk, Madame Curielaan 6, Rijswijk, 2289 CA, the Netherlands, Tel +31 88 1111 945, Email [email protected]
Purpose: A high density of Demodex infestation in human eyelids and eyelash follicles has been implicated in a variety of ocular surface conditions. However, Demodex infestation often goes undiagnosed and untreated, due to an overlap in signs and symptoms with other sources of ocular surface inflammation. We sought to refine the diagnostic technique for outpatient assessment for Demodex infestation and determine prevalence of Demodex mites in the hair follicles of eyelashes from patients in a standard ophthalmic practice.
Patients and Methods: Patients recruited from a single outpatient ophthalmology clinic were examined for the presence of Demodex mites following standard ophthalmic consultation. During anterior segment biomicroscopic examination, investigators searched for cylindrical dandruff and collarettes around the base of patient eyelashes. These were removed, and individual eyelashes manipulated with tweezers to reveal Demodex mites. Presence of Demodex, cylindrical dandruff and collarettes, time taken to identify the first Demodex mite, mean number of Demodex mites per hair shaft, and patient-reported symptoms of blepharitis were recorded and analyzed to determine potential correlations.
Results: A total of 173 patients were recruited, of whom 106 were included in Demodex prevalence analyses. Demodex infestation was identified in 100/106 (94%) patients, with a mean time of 2 minutes and 20 seconds taken to find the first Demodex mite and a mean number of 3 mites identified per hair shaft. Presence of Demodex significantly correlated with the presence of cylindrical dandruff (98/106 [92%] patients; p < 0.001), but not with the presence of collarettes (62/106 [58%] patients; p = 0.230) or symptoms of blepharitis (15/106 [14%] patients; p = 0.591).
Conclusion: These results highlight the pervasiveness of Demodex infestation, predicted by the presence of cylindrical dandruff, in the eyelashes of patients in a standard ophthalmic practice. They support the use of a non-invasive diagnostic technique to allow fast, simple identification of Demodex by ophthalmologists and optometrists in outpatient clinical practice.
Keywords: Demodex folliculorum, Demodex brevis, blepharitis, diagnosis, incidence, ophthalmic clinical practice
Plain Language Summary
This study is about a group of microscopic mites called Demodex that live in people’s eyelids and eyelashes. High numbers of Demodex mites can cause a variety of eye conditions that make people’s eyelids red, swollen, irritated, and itchy. While infestations of Demodex are often easy to treat once identified, they often go undiagnosed since their symptoms are similar to other causes of eye irritation. We wanted to simplify the techniques that eye doctors can use to diagnose Demodex infestations in order to find out how common Demodex mites are among patients visiting an eye clinic.
We refined a simple technique to diagnose Demodex infestation in human eyelids using an ophthalmic microscope and tweezers. Using this technique, we examined the eyelids of 106 eye clinic patients and found that almost all of them had Demodex mites in their eyelashes. We found an average of 3 Demodex mites per eyelash examined, taking an average time of 2 minutes and 20 seconds to find the first Demodex mite. Demodex mites were more likely to be found in patients who had cylinders of dandruff around the base of their eyelashes than in those who did not.
Our results suggest that Demodex mites are widespread in the eyelashes of eye clinic patients and that eye doctors can use a simple and quick technique to diagnose Demodex infestation in their patients. We propose that ophthalmologists and optometrists should consider using this diagnostic technique in patients with signs and symptoms of Demodex infestation.
Introduction
Demodex (Demodex folliculorum and Demodex brevis) is a genus of mites known to reside commonly in human hair follicles.1,2 These transparent mites are 0.3–0.4mm in length, with four short pairs of legs located on the anterior segment of the body, and a longer tubular-shaped posterior segment. They can be found in the sebaceous glands of the scalp, face, and ears, and in the meibomian glands of the eyelids and eyelash follicles, where they anchor themselves to the follicle head-downwards, with their posterior segment protruding.1,2
A high density of Demodex infestation has been implicated in a variety of ocular surface conditions such as blepharitis, an inflammation of the eyelids that can cause burning or itching sensations, redness and scaling.2–4 Demodex folliculorum infestation is also one of the key contributors in the pathogenesis of meibomian gland dysfunction (MGD) related dry eye, and a higher prevalence of chalazion was found in D. folliculorum infected patients.5,6 It is thought that Demodex folliculorum can cause anterior blepharitis through micro-abrasion and irritation of the eyelash follicles, while Demodex brevis can cause posterior blepharitis with meibomian gland dysfunction and keratoconjunctivitis through mechanical blockage.3,4 Indeed, a meta-analysis of blepharitis case–control studies, including a total of nearly 5000 participants, confirmed a stable and statistically significant association between Demodex infestation and blepharitis with a pooled odds ratio of 4.89 (95% confidence interval 3.00–7.97) in random effect models.7
Several local or systemic treatment options are available for Demodex blepharitis, which have been shown to be effective at reducing or eradicating Demodex mites and improving the symptoms of blepharitis.8 Treatment selection is usually based on the severity of the condition, with local treatments favored in the majority of cases due to fewer systemic side effects.3,8 While Demodex infestation is resistant to a wide range of common antiseptic solutions including 75% alcohol and 10% povidone–iodine and antimicrobials such as erythromycin and metronidazole, mites can dose-dependently be killed by tea tree oil, which forms the basis of several treatments for Demodex.9 In the literature, it is found that ivermectin (topical and systemic) and ivermectin-metronidazole (topical) are also good anti-Demodex interventions. In addition to traditional pharmacotherapy, light therapies, especially IPL and skin cleansing, could also be considered as effective methods to control Demodex mite infestation.10 Examination for Demodex infestation should therefore be considered in patients with symptomatic blepharitis and remedial treatment offered to patients in whom Demodex mites are found to be present.11
However, Demodex infestation often goes undiagnosed and untreated, due to a significant overlap in signs and symptoms with other ocular surface conditions including anterior or posterior blepharitis, evaporative or non-evaporative dry eye, and other sources of ocular surface inflammation.3 A conventional method of diagnosing Demodex infestation involves the epilation and microscopic evaluation of four nonadjacent lashes per eyelid, where mites can be visually identified by their characteristic morphology and motility.1 However, such procedures can be time-consuming to perform and uncomfortable for patients. In addition, random eyelash epilation has been shown to underestimate the density of Demodex infestation, since mite counts may vary based on the presence of cylindrical dandruff at the base of the epilated lash.3,12 Consequently, ophthalmologists and optometrists do not commonly diagnose and treat Demodex in routine practice.13
A need therefore exists for the incorporation of novel diagnostic techniques into standard outpatient practice, to allow ophthalmologists and optometrists to assess the prevalence of Demodex mites quickly, simply, and accurately. In clinical studies using epilation techniques, presence of cylindrical dandruff on the eyelashes has been shown to indicate a high‑density Demodex infestation.14 An alternative technique of identifying Demodex infestation has been previously described, in which mites can be identified in situ under 25–40x biomicroscopic magnification by the removal of cylindrical dandruff and application of rotation and lateral tension to eyelashes without epilation, in order to expose and visualize mites at the eyelash follicle.15,16
The aim of our study was to determine the prevalence of Demodex mites in the hair follicles of eyelashes from patients within a standard ophthalmic practice, using an in situ diagnostic technique. In order to do this, a pilot study was set up to refine the in situ diagnostic technique previously described by not epilating the hair follicle as was done by Muntz,15,16 and determine the easiest way for ophthalmologists and optometrists to identify and examine Demodex mites in outpatient clinical practice. This was followed by a larger study, which investigated the prevalence and density of Demodex infestation in the eyelash hair follicles of ophthalmic outpatients using the early described in situ diagnostic technique.
Materials and Methods
Study Population
For both the pilot and larger prevalence study, patients were recruited from a single outpatient ophthalmology clinic (Eyescan Rijswijk and Warmond, Rijswijk, the Netherlands; formerly Oogheelkunde Rijswijk). Patient recruitment occurred between November 2019 and January 2020. Consecutive consenting patients were recruited during a normal ophthalmic consulting hour, with no specific inclusion or exclusion criteria. Patients were subsequently excluded if they were unable to undergo a thorough eyelid examination due to conditions including excessive blinking, eyelid-squeezing, head-throwing, name-calling, light-headedness, or fainting. All other patients underwent an in-situ examination technique for the diagnosis of Demodex infestation.
This study followed the tenets of the Declaration of Helsinki and was approved by the Oogheelkunde Rijswijk institutional review board. Informed consent was obtained from all participants after explanation of the nature and possible consequences of the study. No patients refused to participate in the study.
Pilot Study Design and Procedures
The aim of the pilot study was to determine an optimal diagnostic technique for the identification and examination of Demodex mites in outpatient clinical practice. In order to do this, investigators replicated and refined the in-situ technique for identifying Demodex infestation previously described by Muntz et al.15 Briefly, investigators searched for characteristics of Demodex infestation, such as cylindrical dandruff and collarettes around the base of eyelashes, during an anterior segment biomicroscopy assessment. To identify the presence of Demodex infestation, cylindrical dandruff and collarettes were first removed from the eyelashes, then the eyelashes were manipulated with tweezers to reveal the Demodex mites (Figure 1).
 |
Figure 1 Technique for identifying the Demodex mite. Cylindrical dandruff (A) is sought and removed (B), then the hair follicle is manipulated (C) to reveal Demodex mites (D). |
Prevalence Study Design and Procedures
For the prevalence study, consecutive patients were examined using a refined in situ diagnostic technique whereby the presence of Demodex mites was investigated following standard ophthalmic examination. For each patient, the upper and lower eyelids of both eyes were examined at 40x magnification. Any patients unable to undergo a thorough eyelid examination due to excessive retraction, movement, or blinking were excluded from the study.
On each eyelid, eyelashes were examined for cylindrical dandruff and collarettes using tweezers. If found, cylindrical dandruff and collarettes were removed, and the hair was manipulated by laterally tensioning and twisting in such a way that one or more Demodex mites, if present, rose up the hair shaft. This technique was continued for one minute; if no eyelash hair could be grasped within this timeframe, the investigation was discontinued. Otherwise, investigation continued until the upper and lower eyelids of both eyes had been thoroughly examined.
Outcome Measures
In the pilot study, presence of Demodex mites, cylindrical dandruff and collarettes, and patient-reported symptoms of blepharitis were recorded for each patient. In addition, the time taken searching for Demodex infestation and the mean number of Demodex mites identified per hair shaft were recorded for each patient.
Similarly, presence of Demodex mites, cylindrical dandruff and collarettes, and patient-reported symptoms of blepharitis were recorded for each patient in the prevalence study. In addition, the time taken to find the first Demodex mite, mean number of Demodex mites identified per hair shaft, and mean amount of cylindrical dandruff identified per 40x magnification view were recorded for each patient. Patient baseline characteristics, including age, were also documented.
Statistical Analyses
For both the pilot and prevalence studies, examination results were statistically analyzed to determine potential correlations between the presence or density of Demodex infestation and the other clinical variables assessed. Statistical analyses were performed using SPSS statistics software version 28, and statistical significance was assigned to p-values of less than or equal to 0.05.
Categorical variables including the presence or absence of cylindrical dandruff and collarettes and continuous variables including patient age and mean time taken to identify Demodex were analyzed for potential associations with the presence or density of Demodex infestation. In addition, patient-reported symptoms of blepharitis were analyzed for potential associations with the presence of Demodex infestation, cylindrical dandruff, or collarettes. Fisher’s exact test was used to determine any potential associations between two categorical variables. Pearson’s correlation coefficient was used to analyze the correlation between two continuous variables and the statistical significance of any differences between the means of two continuous variables was analyzed using an independent T-test.
Results
Patients
Between November 2019 and January 2020, a total of 173 patients were recruited for in situ examination for the presence of Demodex infestation following a standard ophthalmic consultation. Patient disposition is shown in Figure 2. A total of 13 patients were included in the pilot study. Following the pilot study, a further 45 patients were assessed for Demodex infestation in order to improve the diagnostic technique and provide a learning curve for investigators. Results of this learning phase were not recorded.
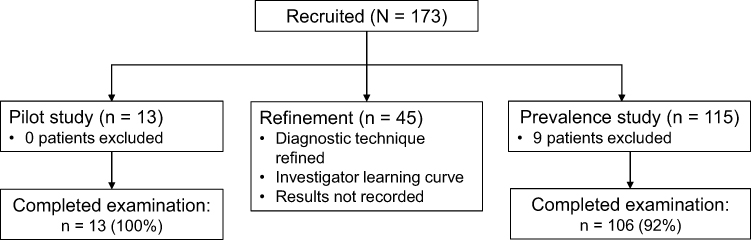 |
Figure 2 Patient disposition. |
A total of 115 patients were enrolled in the subsequent prevalence study. Of these, 9 patients were excluded from the study for conditions that prevented thorough eyelid examination including excessive blinking, eyelid-squeezing, head-throwing, name-calling, light-headedness, and fainting. The remaining 106 patients were included in the prevalence study analyses. The mean age of patients included in prevalence study analyses was 66.4 years (standard deviation ±14.6; range 20–86) and 60/106 (57%) patients were female. Eye drops were being used by 43/106 (41%) patients; the majority of patients had a history of eye surgery and/or other non-ophthalmological comorbidities. Patient baseline characteristics are presented in Table 1.
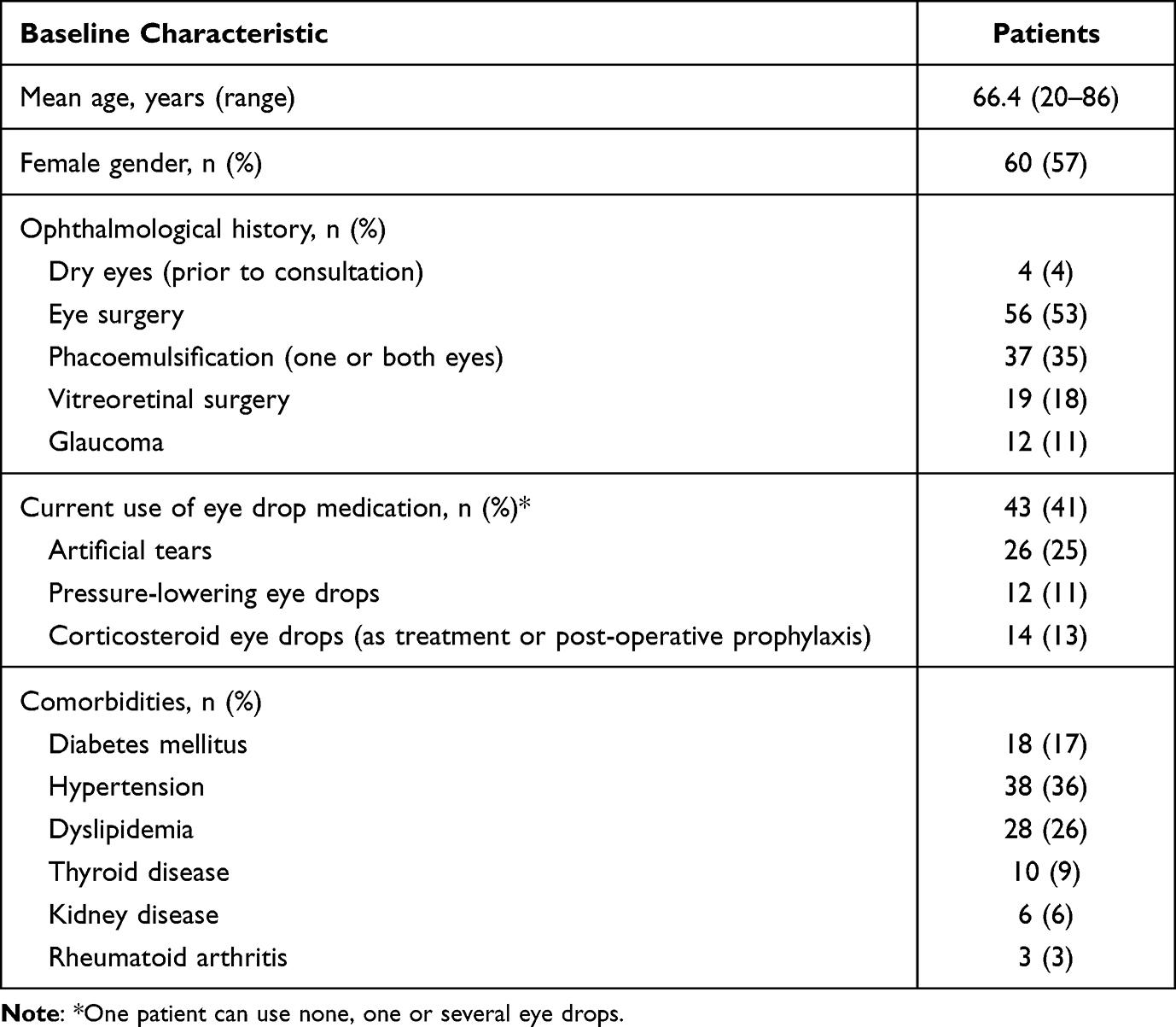 |
Table 1 Patient Baseline Characteristics (Prevalence Study, N = 106) |
Pilot Study Results
During the pilot study, investigators spent a total of 23 minutes and 30 seconds searching for Demodex infestation across all patients, spending a mean average time of 1 minute and 48 seconds (range 30 seconds to 3 minutes) searching each patient. Presence of Demodex infestation was identified in all 13 (100%) patients; the mean number of Demodex mites identified per hair shaft was 2 (range 1–4).
Cylindrical dandruff was identified in all 13 (100%) patients, and collarettes were identified in 7/13 (54%) patients. All patients who had cylindrical dandruff also had presence of Demodex infestation. However, since both of these examination results were constants, a statistical correlation between the two categorical variables could not be established. Statistical analysis found no significant correlation between presence of collarettes and the amount of Demodex per hair shaft (p = 0.8 by independent T-test).
A total of 7/13 (54%) patients reported symptoms of blepharitis, which included dry eyes and a “grain of sand” feeling. The presence of collarettes was associated with the reported symptoms of blepharitis (Figure 3).
 |
Figure 3 Correlation between presence of collarettes and patient-reported symptoms of blepharitis. |
Prevalence Study Results
During the prevalence study, the mean time taken for investigators to find the first Demodex mite was 2 minutes and 20 seconds (standard deviation ±20 seconds; range 30 seconds to 10 minutes) and a mean number of 3 Demodex mites were identified per hair shaft. The number of Demodex mites identified per hair shaft was found to be negatively correlated with the time taken to find the first Demodex mite (Pearson’s correlation coefficient of –0.402; p < 0.001). Therefore, the greater the number of Demodex mites per hair shaft, the less time it took for investigators to identify the first Demodex mite (Figure 4).
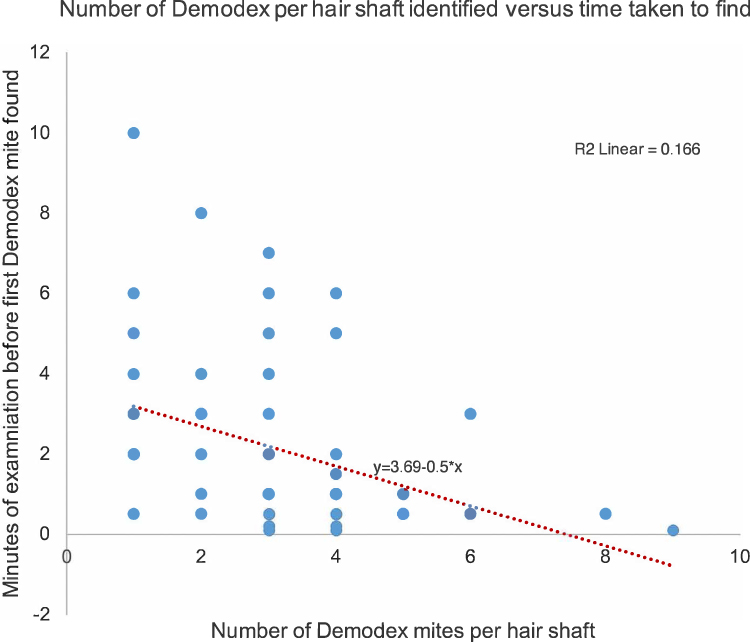 |
Figure 4 Correlation between the number of Demodex mites identified per hair shaft and the time taken to find the first Demodex mite (Pearson’s correlation coefficient –0.402; p<0.001). |
Overall, presence of Demodex infestation was identified in 100/106 (94%) patients, cylindrical dandruff was identified in 98/106 (92%) patients, and collarettes were identified in 62/106 (58%) patients. Presence of Demodex infestation was significantly associated with presence of cylindrical dandruff (p < 0.001 by Fisher’s exact test) but was not found to be associated with patient age (p = 0.117 by independent T-test) or presence of collarettes (p = 0.230 by Fisher’s exact test). Investigators identified a mean number of 3.35 cylindrical dandruffs per 40x magnification view across all patients and eyelids studied. There was a positive correlation between the mean number of Demodex mites identified per hair shaft and the amount of cylindrical dandruff seen per 40x magnification view (Pearson’s correlation coefficient of +0.537; p < 0.001). Therefore, the greater the amount of cylindrical dandruff present, the more Demodex mites were identified.
A total of 15/106 patients (14%) reported symptoms of blepharitis, including dry eyes and a “grain of sand” feeling. Some of these patients also reported additional symptoms including blurred vision, tearing eyes, and red or swollen eyelids (Table 2). No significant associations were found between patient-reported symptoms of blepharitis and presence of Demodex infestation (p = 0.591 by Fisher’s exact test), cylindrical dandruff, or collarettes (both p = 1.000 by Fisher’s exact test). Neither were patient-reported symptoms of blepharitis found to be associated with the mean number of Demodex mites identified per hair shaft (p = 0.08 by independent T-test) or the mean amount of cylindrical dandruff identified per 40x magnification view (p = 0.571 by independent T-test).
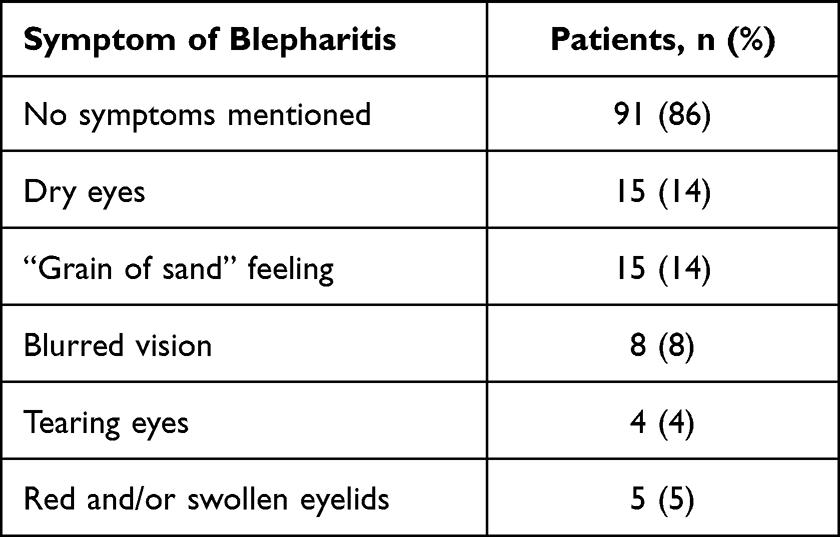 |
Table 2 Patient-Reported Symptoms of Blepharitis (Prevalence Study, N = 106) |
Discussion
Our study on the accurate diagnosis and prevalence of Demodex highlights the pervasiveness of Demodex infestation in a standard ophthalmic practice. We found an extremely high prevalence of Demodex mites in the eyelids of 94% of ophthalmology clinic outpatients. These findings are somewhat higher than those of prior studies, which have found that Demodex mites are present on the eyelashes of between 43% and 90% of patients with blepharitis,12,17 and between 18% and 55% of ophthalmology patients without blepharitis.12,18 However, our findings may be confounded by a bias in patient selection; this study may have identified a particularly high prevalence of Demodex infestation as all subjects were clinical outpatients with a wide range of pre-existing ocular conditions, whereas previous studies recruited subjects with a narrower range of ocular complaints12,17 or with no pre-existing ocular or lid and margin disease.12,18
The higher prevalence of Demodex infestation found in our study may also be due in part to the use of an improved in situ technique for Demodex identification, compared with prior studies which have used the technique of eyelash epilation for microscopic identification of Demodex mites.12,17,18 An alternative in situ technique for the clinical diagnosis and grading of Demodex infestation, described by Muntz et al, has previously been shown to identify a higher number of Demodex mites per eyelash than epilation techniques.15 Our study substantiates this technique, whereby investigators are able to visualize mites at the exposed eyelash follicle by removing cylindrical dandruff and applying static, lateral tension to the eyelash without epilation. The results of our study confirm that this method is convenient and clinically applicable, requiring only tweezers and 40x biomicroscope magnification, and allowing for rapid, efficient evaluation of large numbers of eyelashes with confirmation of Demodex infestation within 2–3 minutes. During our study, this technique was performed successfully both by optometrists and by ophthalmologists. We suggest that it could be carried out simply and effectively in standard outpatient practice.
The results of our study showed that the more Demodex mites present per hair shaft, the faster they were to be found. Demodex mites were not always found in both eyes or eyelids; in some patients they were found exclusively in the upper eyelids or in one eye. It was therefore important to conduct a thorough search during examination. Examination was highly dependent on patient cooperation. Some patients experienced cylindrical dandruff removal or eyelash pulling and twisting as itchy and painful, and thorough examination was not possible in 9 of the 115 patients enrolled in the prevalence study. In addition, a learning curve was needed in order for individual investigators to identify Demodex mites efficiently. Identification was more difficult in patients with light skin or hair because the transparent mites are less noticeable than on dark skin or hair. Based on these findings, we recommend that optometrists and ophthalmologists should receive training on in situ techniques for the accurate diagnosis of Demodex infestation, to inform treatment decisions for their patients with blepharitis.
Prior clinical studies have suggested that presence of cylindrical dandruff in a patient’s eyelashes is indicative of high‑density Demodex infestation.12,14,19–21 Our study found a significant association between the presence and density Demodex infestation and the presence and density of cylindrical dandruff. The greater the amount of cylindrical dandruff present, the more Demodex mites were identified, suggesting that presence of cylindrical dandruff is predictive of Demodex infestation. It is therefore important for optometrists and ophthalmologists to conduct a thorough examination for cylindrical dandruff, as well as Demodex mites themselves. The following clinical sequence has been previously suggested to identify Demodex infestation: (1) Confirm clinical history of blepharitis, dry eyes, and/or ocular allergy; (2) Slit-lamp examination of cylindrical dandruff; (3) Confirmation of Demodex infestation using light microscope evaluation of epilated lashes.22 We recommend replacing the final step in this sequence with the diagnostic technique conducted in our study of removing cylindrical dandruff and manipulating the hair follicle to reveal Demodex mites in situ, to enable quick and easy identification and examination of Demodex in standard outpatient practice. Conducting such examinations in routine clinical practice should alert clinicians to treat concomitant Demodex infestation in patients with blepharitis.12
The exact pathogenesis of blepharitis is unknown but is suspected to be multifactorial, with causes including bacterial infection of the ocular surface, infestation with organisms such as Demodex, and inflammatory skin conditions such as atopy and seborrhoea.23 Whether Demodex is commensal or parasitic remains an area of dispute, as mites are found in both symptomatic and asymptomatic individuals.3,4 Although few guidelines exist for the diagnosis and treatment of Demodex in clinical practice, the TFOS DEWS II management and therapy report recommends tea tree oil treatment for patients in whom Demodex infestation is present if the initial management of blepharitis is inadequate.11 Topical tea tree oil-based treatments (5% or 50%) such as terpinen-4-ol (25%) have been shown to be effective in eradicating Demodex mites and alleviating the symptoms of blepharitis and may also exert antibacterial, antifungal, and anti-inflammatory actions.8,23 Demodex eradication is not entirely successful with terpinen 4 old derivatives. The main goal is to reduce the amount of demodex and the complaints that patients experience from the mite.24 It is therefore important that optometrists and ophthalmologists know how to check their patients for Demodex infestation, so they can offer appropriate treatment to those with symptoms. For patients with symptoms of blepharitis, Demodex infestation can be treated in standard outpatient practice with tea tree oil or terpinen-4-ol, initially for one month or until these symptoms resolve.6,11 Once symptoms resolve, normal eyelid hygiene is advised to keep eyelids clean and in good condition. It is likely that Demodex infestation will eventually return, and if symptoms recur then intermittent use of topical treatment may be needed.25
Prior clinical studies have shown that prevalence of Demodex infestation is higher in patients with blepharitis than in those without,12,18 and appears to be associated with advancing age.17,26 Our study, however, did not find any correlation between presence of Demodex infestation and either patient age or reported symptoms of blepharitis. This lack of correlation may be due in part to the limited size and wide range of pre-existing ocular conditions in the patient population studied. However, it supports previous observations that Demodex mites are found in both symptomatic and asymptomatic individuals, suggesting that Demodex infestation does not cause symptoms for everyone. We found that the skin of older patients was more hardened, making Demodex mites easier to see, although the mite was also found in younger patients. However, these results should be interpreted with caution since our study was limited to a select group of patients within a single ophthalmology practice and was not representative of the wider population. The proposed technique could be a basis for the future studies for the diagnosis and follow-up of current treatments or proposed treatments. The mean age of patients in the prevalence study was over 65 years and few patients aged under 50 took part. Furthermore, not all enrolled patients were able to be examined, potentially introducing further selection bias to the study results.
Conclusion
In conclusion, our study demonstrated a very high prevalence of Demodex infestation, predicted by the presence of cylindrical dandruff, in the eyelashes of patients in a standard ophthalmic practice and use an in situ diagnostic technique for ophthalmologists and optometrists to determine the prevalence and density of Demodex mites in outpatient clinical practice. This study demonstrates that with a short-time investment, Demodex can be diagnosed and treated specifically and quickly. Future studies to explore the potential benefits of outpatient identification and treatment of symptomatic Demodex infestation would be welcomed, including assessment of optimal conditions for treatment initiation, length of treatment, and need for re-treatment should infestation or symptoms reoccur.
Acknowledgments
Medical writing support for manuscript development was provided by Jennie Pollard of Chill Pill Media Ltd, funded by Théa Pharma B.V.
Disclosure
F.G. declares honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events (not related to this study) from AbbVie, Horus Pharma, Novartis, Ophtec, Théa Pharma B.V., and Tramedico, and a leadership or fiduciary role in Visitatie Commissie Nederlands Oogheelkundig Gezelschap (NOG) and Adviescommissie Kwaliteitsvisitatie Federatie Medisch Specialisten (FMS) advisory groups. All other authors report no conflicts of interest in this work.
References
1. Coston TO. Demodex folliculorum blepharitis. Trans Am Ophthalmol Soc. 1967;65:361–392.
2. Rufli T, Mumcuoglu Y. The hair follicle mites Demodex folliculorum and Demodex brevis: biology and medical importance. Dermatologica. 1981;162:1–11. doi:10.1159/000250228
3. Fromstein SR, Harthan JS, Patel J, et al. Demodex blepharitis: clinical perspectives. Clin Optom. 2018;10:57–63. doi:10.2147/OPTO.S142708
4. Liu J, Sheha H, Tseng SCG. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010;10:505–510. doi:10.1097/ACI.0b013e32833df9f4
5. Hao Y, Zhang X, Bao J, Tian L, Jie Y. Demodex folliculorum infestation in meibomian gland dysfunction related dry eye patients. Front Med. 2022;9:833778. doi:10.3389/fmed.2022.833778
6. Huang J, Guo MX, Xiang DM, et al. The association of demodex infestation with pediatric chalazia. BMC Ophthalmol. 2022;22(1):124. doi:10.1186/s12886-022-02261-w
7. Zhao YE, L-P W, Hu L, et al. Association of blepharitis with Demodex: a meta-analysis. Ophthalmic Epidemiol. 2012;19:95–102. doi:10.3109/09286586.2011.642052
8. Navel V, Mulliez A, d’Azy CB, et al. Efficacy of treatments for Demodex blepharitis: a systematic review and meta-analysis. Ocul Surf. 2019;17(4):655–669. doi:10.1016/j.jtos.2019.06.004
9. Gao -Y-Y, Di Pascuale MA, Li W, et al. In vitro and in vivo killing of ocular Demodex by tea tree oil. Br J Ophthalmol. 2005;89:1468–1473. doi:10.1136/bjo.2005.072363
10. Li J, Wei E, Reisinger A, French LE, Clanner-Engelshofen BM, Reinholz M. Comparison of different anti-Demodex strategies: a systematic review and meta-analysis. Dermatology. 2023;239(1):12–31.
11. Jones L, Downie LE, Korb D, et al. TFOS DEWS II management and therapy report. Ocul Surf. 2017;15:575–628.
12. Bhandari V, Reddy JK. Blepharitis: always remember demodex. Middle East Afr J Ophthalmol. 2014;21(4):317–320. doi:10.4103/0974-9233.142268
13. Sharma N, Martin E, Pearce EI, Hagan S, Purslow C. Demodex blepharitis: a survey-based approach to investigate knowledge, attitudes, and practices among optometrists in India. Clin Optom. 2023;15:55–64.
14. Gao -Y-Y, Di Pascuale MA, Li W, et al. High prevalence of Demodex in eyelashes with cylindrical dandruff. Invest Ophthalmol Vis Sci. 2005;46(9):3089–3094. doi:10.1167/iovs.05-0275
15. Muntz A, Purslow C, Wolffsohn JS, et al. Improved Demodex diagnosis in the clinical setting using a novel in situ technique. Cont Lens Anterior Eye. 2020;43:345–349.
16. Mastrota KM. Method to identify Demodex in the eyelash follicle without epilation. Optom Vis Sci. 2013;90(6):e172–e174. doi:10.1097/OPX.0b013e318294c2c0
17. Demirkazık M, Koltaş İS. Blepharitis caused by Demodex. Turkiye Parazitol Derg. 2020;44:21–24. doi:10.4274/tpd.galenos.2019.6476
18. Kabataş N, Doğan AŞ, Kabataş EU, et al. The effect of Demodex infestation on blepharitis and the ocular symptoms. Eye Contact Lens. 2017;43(1):64–67. doi:10.1097/ICL.0000000000000234
19. Shah PP, Stein RL, Perry HD. Update on the management of demodex blepharitis. Cornea. 2022;41(8):934–939. doi:10.1097/ICO.0000000000002911
20. Zhong J, Tan Y, Li S, et al. The prevalence of Demodex folliculorum and Demodex brevis in cylindrical dandruff patients. J Ophthalmol. 2019;2019:8949683. doi:10.1155/2019/8949683
21. Aumond S, Bitton E. Palpebral and facial skin infestation by Demodex folliculorum. Cont Lens Anterior Eye. 2020;43(2):115–122.
22. Hom MM, Mastrota KM, Schachter SE. Demodex. Optom Vis Sci. 2013;90(7):e198–e205. doi:10.1097/OPX.0b013e3182968c77
23. Lindsley K, Matsumura S, Hatef E, et al. Interventions for chronic blepharitis. Cochrane Database Syst Rev. 2012;2012:CD005556. doi:10.1002/14651858.CD005556.pub2
24. Cheung IMY, Xue AL, Kim A, Ammundsen K, Wang MTM, Craig JP. In vitro anti-demodectic effects and terpinen-4-ol content of commercial eyelid cleansers. Cont Lens Anterior Eye. 2018;41(6):513–517. doi:10.1016/j.clae.2018.08.003
25. Evren KÖ, Karaca EE, Özek D. Efficacy of cyclic therapy with terpinen-4-ol in Demodex blepharitis: is treatment possible by considering Demodex’s life cycle? Eur J Ophthalmol. 2021;31:1361–1366. doi:10.1177/1120672120919085
26. Murphy O, O’ Dwyer V, Lloyd-McKernan A. The effect of lid hygiene on the tear film and ocular surface, and the prevalence of Demodex blepharitis in university students. Cont Lens Anterior Eye. 2020;43:159–168. doi:10.1016/j.clae.2019.09.003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association Between Acne Vulgaris, Acne Vulgaris with Nonspecific Facial Dermatitis, and Demodex Mite Presence
Paichitrojjana A, Chalermchai T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:137-146
Published Date: 22 January 2024
Evaluating the Efficacy of Oral Ivermectin on Clinical Symptoms and Demodex Densities in Patients with Demodicosis
Paichitrojjana A, Chalermchai T
Drug Design, Development and Therapy 2024, 18:5299-5306
Published Date: 19 November 2024