Back to Journals » Infection and Drug Resistance » Volume 19
Refining the Clinical Utility of Plasma Microbial Cell-Free DNA Sequencing in High-Risk Population of Infection: A Narrative Review
Authors Li X, Li J, Zhang L ![]() , Huang S
, Huang S ![]() , Zhao L, Liu L, Yang S
, Zhao L, Liu L, Yang S ![]()
Received 21 August 2025
Accepted for publication 26 January 2026
Published 4 March 2026 Volume 2026:19 562107
DOI https://doi.org/10.2147/IDR.S562107
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Xinyi Li,1,* Junjie Li,2,* Linbo Zhang,1 Shifeng Huang,1 Lin Zhao,3 Liyao Liu,3 Shuangshuang Yang1
1Department of Laboratory Medicine, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Key Laboratory of Laboratory Medical Diagnostics, Ministry of Education, Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Emergency, the First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shuangshuang Yang, Department of Laboratory Medicine, The First Affiliated Hospital of Chongqing Medical University, No. 1 Youyi Road, Yuzhong District, Chongqing, 400016, People’s Republic of China, Email [email protected]
Abstract: Plasma microbial cell-free DNA sequencing (mcfDNA-seq) has emerged as a promising diagnostic and prognostic tool for infectious diseases, with early enthusiasm driven by its potential to outperform conventional microbiological assays in detection sensitivity. However, its anticipated clinical superiority has not consistently translated into transformative improvements in infection management, particularly in high-risk populations. Since its inception in 2015, key controversies have persisted regarding the optimal timing of mcfDNA-seq testing, clinical utility of longitudinal quantification, preferred testing modality (plasma mcfDNA-seq vs blood cell DNA sequencing), and integrative analysis of mcfDNA-seq data incorporating host immune biomarkers and antimicrobial resistance (AMR) gene profiling to enhance diagnostic precision. To address these unresolved questions, this review synthesizes the current evidence on the clinical applications of plasma mcfDNA-seq, critically evaluates its performance across diverse infectious disease contexts, and concludes by delineating future challenges and opportunities to optimize its translational utility for clinical practice.
Keywords: plasma mcfDNA, sequencing, quantification, time series, clinical impact
Introduction
Infection remains a leading cause of morbidity and mortality in immunocompromised patients, particularly those with hematologic malignancies, hematopoietic cell transplantation, or solid organ transplantation. Due to impaired immune responses and frequent atypical clinical presentations, the diagnosis of infections in this population is particularly challenging. Conventional microbiological tests (CMTs) identify pathogens in fewer than 30% of cases, a rate further reduced by the widespread use of antibiotic prophylaxis.1 Moreover, CMTs exhibit limited sensitivity in detecting fastidious bacteria, mycobacteria, and fungi, which are common etiological agents in immunocompromised individuals. Consequently, diagnostic uncertainty persists as a major impediment to optimal infection management in this vulnerable group, underscoring the urgent need for more precise pathogen detection methodologies.
Microbial cell-free DNA sequencing (mcfDNA-seq) has emerged as a promising tool to overcome the limitations of CMTs, offering a minimally invasive approach with superior sensitivity and the capacity to detect a broader spectrum of pathogens than CMTs. By sequencing millions of circulating microbial DNA fragments, mcfDNA-seq generates clinically actionable data. Several studies have demonstrated a higher rate of positive findings by mcfDNA-seq compared to culture or other diagnostic modalities.1–5 Critically, this technology has now transitioned into clinical practice, with commercially available kits (eg, Karius® Test) receiving regulatory FDA approval specifically for aiding infection diagnosis in immunocompromised patients, including those with hematologic malignancies, organ transplants, or advanced HIV.1,4,6–10 However, the interpretation and clinical utility of these results, particularly from sterile specimens such as plasma, remain a substantial challenge.
For instance, a recent prospective multicenter study reported that antimicrobial modifications were implemented in only 18.4% of immunocompromised patients with pneumonia based on plasma mcfDNA-seq results.11 Similarly, Shah et al found that while 71% of plasma mcfDNA-seq results were positive for microorganisms, only 24% had a positive clinical impact in solid organ transplant recipients with infectious syndromes.12 In contrast, Benamu et al reported that plasma mcfDNA-seq facilitated early antimicrobial optimization in 47% of patients with febrile neutropenia.7 And David et al observed changes in the clinical management of 85% of immunocompromised patients with COVID-19-associated secondary pulmonary infections based on mcfDNA-seq results.13 These disparate findings highlight the ongoing debate regarding the clinical utility of plasma mcfDNA-seq in infection management among immunocompromised patients, as well as uncertainty surrounding its optimal application in this context.
To address this gap, we conducted a narrative synthesis and critical evaluation of the current evidence on the clinical impact of plasma mcfDNA-seq in the management of infections, especially in immunocompromised patients, and proposed strategies to optimize its clinical utility. We searched PubMed and Web of Science using keywords including “plasma microbial cell-free DNA”, “mcfDNA-seq”, “immunocompromised”, and “clinical utility” from January 2015 to February 2025. Of note, studies focusing solely on diagnostic performance, quality control, or cost-effectiveness were not discussed in this review, as these aspects have been extensively addressed in recent meta-analyzes and reviews.5,14–19
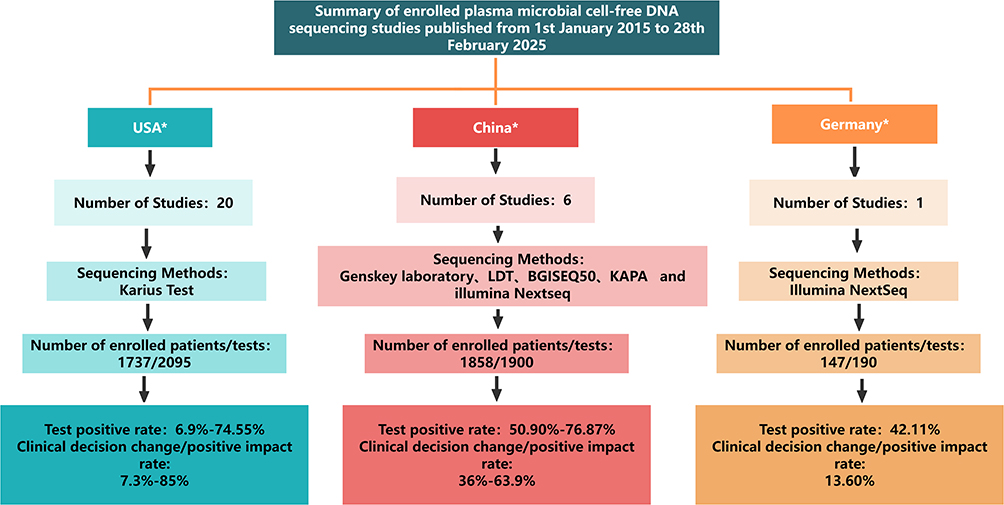 |
Figure 1 Summary of enrolled plasma mcfDNA-sequencing studies published from 1st January 2015 to 28th February 2025. USA*: Refer to.6,7,9,11–13,20–33 China*: Refer to.2,34–38 Germany*:Refer to.39 |
Clinical Impact of Plasma mcfDNA-Seq in Immunocompromised Patients
By summarizing the current application of plasma mcfDNA-seq in immunocompromised patients (Figure 1), most studies (20/27) were conducted in the United States, predominantly utilizing the commercial Karius test (KT) for plasma mcfDNA-seq, followed by studies from China (6) and Germany (1). Cumulatively, 3742 immunocompromised patients underwent 4185 mcfDNA-seq tests. Among these, 2521 tests yielded positive results for at least one microorganism, resulting in a positivity rate ranging from 6.9% to 76.87%. Notably, its positivity rates exhibited substantial variability across studies and differed by the sequencing platforms employed. Specifically, the commercial KT accounted for 2442 tests with positive rates ranging from 6.9%-74.55%, while laboratory-developed tests were performed in 1743 instances, yielding positive rates ranging from 42.11%-76.87%. The reported clinical impact of mcfDNA-seq results extended beyond alterations in antimicrobial therapy to encompass improvements in diagnostic efficiency, antimicrobial escalation or de-escalation, shortened treatment duration, guidance of patient management, and, in some cases, false diagnosis or unnecessary treatments. Generally, 7.3% to 85% of mcfDNA-seq results promoted changes in the clinical management or benefits of enrolled patients (Table 1).
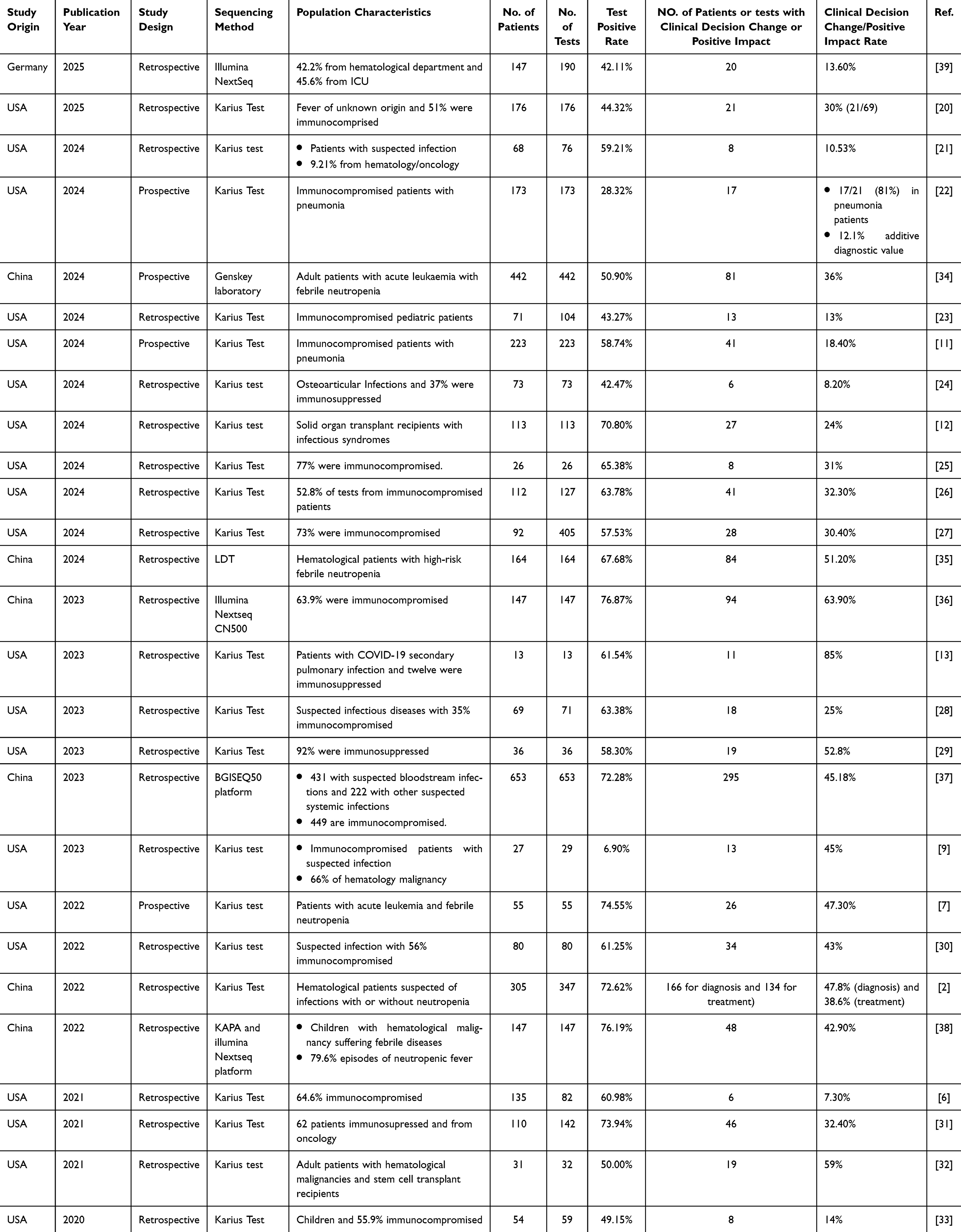 |
Table 1 Clinical Impact of Plasma mcfDNA Sequencing Among Immunocompromised Patients Suspected with Infection |
These findings underscore the significant heterogeneity observed in the clinical utility of plasma mcfDNA-seq in this patient population. Despite its initial promise, the test has not consistently achieved its full potential in improving infection management among immunocompromised individuals or high-risk population. Furthermore, the sub-optimal turnaround time and limited workflow efficiency of mcfDNA-seq diminish its utility in the timely detection of infection. These inherent limitations raise several critical questions regarding its clinical application: (1) What is the optimal timing for test administration, and is serial monitoring or time-series quantification of plasma mcfDNA necessary to enhance early clinical decision-making and improve patient outcomes? (2) What is the preferred testing modality: should plasma mcfDNA-seq be prioritized over blood cell DNA sequencing? (3) How can an integrative interpretation of mcfDNA-seq results, incorporating host response biomarkers and antimicrobial resistance gene profiling, augment its clinical value?
Timing of Plasma mcfDNA-Seq Initiation
Since its initial introduction by De Vlaminck et al in 2015, mcfDNA-seq has garnered increasing attention as a valuable diagnostic and predictive modality for infectious diseases.40 However, the optimal timing of mcfDNA-seq testing to facilitate early diagnosis and effectively guide antimicrobial therapy remains a critical area of ongoing investigation. Recent studies have explored the predictive capacity of mcfDNA-seq at various temporal points during the course of infection. A seven-day sequential mcfDNA-seq study conducted in intensive care unit (ICU) patients demonstrated an overall predictive sensitivity of 87.5% for bloodstream infections (BSIs) prior to blood culture positivity, with daily sensitivity rates ranging from 81.82% to 92.31%.41 In a prospective pilot study involving pediatric patients with relapsed or refractory cancer, mcfDNA-seq predicted 75% of all BSIs and 80% of bacterial BSIs up to three days before the clinical onset of infection.8 Furthermore, in hematopoietic stem cell transplantation (HSCT) recipients with invasive mold infections (IMIs), mcfDNA-seq identified fungal pathogens as early as three weeks prior to clinical diagnosis, with positivity rates increasing from 11% to 38% over the preceding weeks.42
The utility of time-series detection was also investigated. A single-center prospective cohort study reported that pathogen-specific mcfDNA persisted significantly longer than conventional blood cultures (BCs) in patients with confirmed Staphylococcus aureus or gram-negative bacteremia. The median duration of detectability was 15 days for mcfDNA-seq compared to 2 days for BCs, respectively. Moreover, each additional day of mcfDNA positivity was associated with a 2.89-fold increased odds of metastatic infection.43 Similarly, another study on culture-confirmed BSIs found that mcfDNA-seq had a median detection duration of four days compared to one day for BCs. A detection duration of no less than 3 days was identified as an independent risk factor for septic shock.44 In cases of culture-negative infections, mcfDNA-seq demonstrated a 67% positivity rate in children with culture-negative musculoskeletal infections and detected pathogens over a longer duration than BCs (median: 2 days vs 1 day).45
Regarding the influence of antimicrobial treatment, mcfDNA remained detectable for a median of 38.1 days in patients with definite infective endocarditis (IE) following antibiotic initiation, compared to a mere 3.7 days for BCs.46 In another study on sepsis, mcfDNA-seq successfully detected pathogens even after 35 days of antibiotic treatment.47 A recent investigation into cardiac implantable electronic device-associated IE (CIED-IE) revealed that mcfDNA persisted in 90% of patients during antibiotic therapy, with a median detection duration of 11 days.48 In patients with sepsis who had received antibiotics within two weeks prior to presentation, mcfDNA-seq identified pathogens in approximately 50% of cases, compared to less than 20% by BCs.1 Similarly, a multicenter prospective study of 442 adult patients with acute leukemia and febrile neutropenia demonstrated that prior antibacterial exposure significantly reduced BC positivity but had a negligible impact on plasma mcfDNA-mNGS results.34 Concerning surgical interventions, mcfDNA-seq samples collected prior to surgery exhibited higher concordance with culture results (82%) compared to samples collected postoperatively (20%).45 A recent study on patients with IE further demonstrated a significant decline in mcfDNA levels following surgical source control.46
Collectively, these studies underscore the substantial potential of mcfDNA-seq for the early detection of pathogens, often preceding clinical diagnosis by up to a week, and its resilience in the context of ongoing antimicrobial therapy. This technology facilitates the identification of infections before the emergence of overt clinical symptoms and maintains reliability, even under antibiotic pressure, particularly in high-risk populations. To maximize the diagnostic yield, blood samples should ideally be collected prior to surgical procedures or implant removal. Notably, the prolonged persistence of mcfDNA in plasma following the initiation of antimicrobial therapy may serve as a valuable marker for the presence of metastatic infections, development of septic shock, or occurrence of unfavorable clinical outcomes.
Dynamic Quantification of mcfDNA in Infection Management
The application of plasma mcfDNA quantification for infection management was initially reported by Grumaz et al in 2016.49 Since then, numerous studies have investigated the clinical relevance of plasma mcfDNA levels in a diverse spectrum of infectious diseases, yielding several noteworthy observations.
Blauwkamp et al demonstrated that mcfDNA concentrations were significantly elevated in patients with confirmed sepsis compared to asymptomatic donors and individuals classified as unlikely to have sepsis.1 Similarly, Cao et al observed an increasing trend in pathogenic mcfDNA levels in the days preceding the onset of bloodstream infections (BSIs).41 Heldman et al reported a correlation between elevated plasma mcfDNA levels and both extrapulmonary dissemination and mortality in non-Aspergillus invasive mold infections (IMI).42 In patients with COVID-19, Lisius et al found that elevated mcfDNA levels, even in the absence of clinical suspicion of secondary infection, may indicate an undiagnosed secondary infection and predict poorer 90-day survival outcomes.50
In patients with implantable electronic device-related infective endocarditis (CIED-IE), Karchmer et al discovered that the persistence or early clearance of mcfDNA by the sixth day of antibiotic therapy could aid in differentiating between those with and without CIED-IE, thereby informing decisions regarding device extraction. This prospective cohort study enrolled 16 patients with staphylococcal bacteremia and CIED, who were classified according to the modified EHRA criteria into 11 with definite CIED-IE and 5 with possible CIED-IE A key finding was the significant divergence in mcfDNA kinetics between the two groups (Fisher’s exact test, P =0.001). In the definite CIED-IE group, mcfDNA remained detectable for a prolonged median duration of 11 days during antibiotic therapy and showed a marked increase in concentration in samples collected immediately after device extraction. In contrast, in the possible CIED-IE group, mcfDNA was uniformly undetectable after a median of 6 days of therapy and remained undetectable post-extraction. These patterns suggest that the persistence versus early clearance of mcfDNA can serve as a biomarker to differentiate patients with lead infection from those without it. Specifically, assessing mcfDNA clearance by day 6 of antibiotic therapy could inform the decision for device extraction. Furthermore, in cases where empirical extraction is performed, comparing mcfDNA concentrations before and immediately after the procedure may help clarify the presence or absence of intracardiac infection, thereby guiding post-extraction management, including the duration of antibiotic therapy.48
In the context of HSCT, Blair et al observed that mcfDNA dynamics varied according to the transplantation phase and differed significantly from those in healthy individuals.51 Specifically, this observational study reported that mcfDNA levels were significantly elevated during the post-neutropenic nadir period following HSCT compared to healthy individuals and exhibited considerable inter-patient variability. These mcfDNA dynamics not only reflect changes in microbiome composition but may also serve as functional indicators of gut barrier integrity. This link is based on the understanding that intensive conditioning regimens and post-transplant complications can compromise the intestinal mucosal barrier, leading to increased translocation of microbial components, including bacterial DNA, into the bloodstream of these patients. This suggests that mcfDNA not only reflects microbiome composition but may also serve as a functional indicator of gut barrier integrity, potentially predicting intestinal graft-versus-host diseases before the onset of clinical symptoms.
In summary, mcfDNA levels exhibit dynamic and highly patient-specific variability, underscoring the importance of personalized monitoring and interpretation of results. Early quantification of plasma mcfDNA holds considerable promise for the timely detection of infections (eg, BSIs) and prediction of clinical outcomes (eg, mortality in sepsis, COVID-19-associated secondary infections, and invasive fungal infections). Moreover, mcfDNA dynamics can support clinical decision-making by distinguishing true infections from noninfectious conditions. In patients with implanted devices, mcfDNA levels may assist in guiding decisions regarding device removal and duration of antibiotic therapy. Finally, in HSCT recipients, mcfDNA levels may serve as a valuable biomarker for assessing gut microbiome composition and barrier integrity, potentially providing insights into infection risk, and recovery.
Plasma mcfDNA-Seq Versus Blood-Cell DNA Sequencing
While plasma mcfDNA levels can increase during infectious episodes, their concentrations remain relatively low compared to those of host-derived DNA, which can limit the analytical sensitivity of pathogen detection. To address this limitation, blood cell DNA sequencing has been developed as an alternative approach. This method involves the selective lysis of human cells to enrich microbial nucleic acids within the total nucleic acid pool.
Recent investigations have compared the diagnostic performance of plasma mcfDNA and blood-cell metagenomic next-generation sequencing (mNGS). Wu et al evaluated 253 patients with sepsis using both plasma and blood cell mNGS, with blood cultures (BCs) serving as the reference.52 Their findings indicated that blood-cell mNGS demonstrated the capacity to detect bacterial pathogens missed by plasma mNGS, whereas plasma mNGS exhibited superior efficacy in identifying viral pathogens. Overall, blood cell mNGS slightly outperformed plasma mNGS in terms of sensitivity, with detection rates of 72.13% and 67.21%, respectively. Similarly, Chen et al reported higher sensitivity for blood-cell mNGS than for plasma mcfDNA mNGS, using BCs as the reference standard.53 Wang et al further corroborated these findings, demonstrating that blood cell mNGS exhibited significantly higher clinical concordance than plasma mNGS, a result echoed in a recent sepsis study by Zhu et al47,54 Collectively, these studies suggest that blood cell DNA sequencing may offer an advantage over plasma mcfDNA-seq for the detection of culturable pathogens, potentially due to the detection of microbial DNA within circulating phagocytes (eg, neutrophils, monocytes), which serves as a biomarker of active immune engagement and may better differentiate true infection from colonization or non-pathogenic shedding.47,53–55
However, other investigations have yielded contrasting results. For instance, Zhu et al reported that in septic patients, plasma mcfDNA mNGS (p-mNGS), which detects microbial cell-free DNA circulating in plasma, demonstrated a sensitivity of 100% for bacteria/fungi and 97% for viruses when compared to blood cultures and viral PCR. This surpassed the performance of blood-cell mNGS (bc-mNGS), which enriches microbial nucleic acids from within blood cells (including those phagocytosed by immune cells) and showed sensitivities of 88% for bacteria/fungi and 71% for viruses.47 Wang et al also observed a higher positive detection rate for plasma mcfDNA mNGS (84.4%) compared to blood cell mNGS (46.9%).54 Given these inconsistencies, some researchers have explored the diagnostic potential of combined mNGS (co-mNGS), which integrates both plasma mcfDNA mNGS and blood cell mNGS. These studies demonstrated that co-mNGS can enhance diagnostic sensitivity and overall performance, yielding a higher area under the ROC curve (AUC = 0.9581) than either approach alone.53
In summary, the comparative diagnostic efficiency of plasma mcfDNA-seq and blood cell DNA sequencing remains controversial. While blood cell DNA sequencing appears to offer superior sensitivity for detecting culturable pathogens and demonstrates better clinical concordance in some studies, plasma mcfDNA-seq has proven highly effective for identifying unculturable pathogens (eg, DNA viruses, mycobacteria, and Pneumocystis). Notably, a critical consideration when interpreting these comparative studies is their common use of blood culture as the reference standard. Although this provides a practical benchmark for culturable bloodstream infections, it is an imperfect comparator. Blood cultures have limited sensitivity and a narrow taxonomic scope. Consequently, these comparisons may not fully capture the relative diagnostic value of plasma versus blood cell sequencing for the broad spectrum of unculturable pathogens that these technologies are uniquely capable of detecting. Despite a combined mNGS approach may represent a more comprehensive diagnostic strategy, potentially improving overall accuracy in the management of infectious diseases, the cost-effectiveness of a combined mNGS approach warrants further investigation, particularly in resource-limited settings.
Integrative Interpretation of Plasma mcfDNA-Seq Results
A major limitation of the clinical application of mcfDNA-seq as both a diagnostic and antimicrobial stewardship tool is the challenge of distinguishing between pathogenic organisms and colonizers. Given that mcfDNA can be recognized by Toll-like receptors, it has the potential to trigger systemic inflammatory responses.56 Consequently, the integration of mcfDNA data with host immune response profiles has been proposed as a valuable strategy for differentiating true infections from colonization.
Recent studies have explored this integrative approach by combining mcfDNA-seq data with host clinical parameters, immune biomarkers, and machine learning algorithms. A nested case–control study involving ICU patients with pneumonia reported significant and independent associations between mcfDNA levels and inflammatory biomarkers, including fractalkine, procalcitonin, pentraxin-3, and suppression of tumorigenicity-2.57 Similarly, Lisius et al observed a positive correlation between mcfDNA levels and established markers of inflammation, such as white blood cell count, interleukin-6, interleukin-8, and surfactant protein D.50
A recent transcriptomic study supports these findings. Among the samples positive for either plasma mcfDNA-mNGS or blood cell mNGS, elevated procalcitonin and C-reactive protein levels were observed. Notably, the study also revealed suppressed expression of interferon-induced genes and increased expression of genes within the Janus kinase-signal transducer and activator of transcription (JAK-STAT) pathway, indicating the activation of host immune responses.47
Grumaz et al introduced the Sepsis Indicating Quantifier (SIQ) score, which integrates normalized mcfDNA read counts with pathogen-specific reference values to facilitate bacteremia identification.49 Their results demonstrated strong concordance with blood culture findings, underscoring the potential of this integrated approach in sepsis diagnosis.
Building on this concept, Wang et al developed a machine learning model to predict bacterial sepsis.58 The model incorporated plasma mcfDNA copy number, procalcitonin, C-reactive protein, albumin level, and minimum systolic blood pressure. It achieved an average AUC of 0.85 and a precision of 0.91, demonstrating its promise as a tool for early diagnosis and risk stratification in bacterial sepsis.
Another challenge in the clinical application of mcfDNA-seq is the limited capacity to predict antimicrobial resistance (AMR), which is largely attributable to the typically low sequencing depth of clinical metagenomic workflows. However, new methods that enrich AMR genes within mcfDNA or selectively deplete host-derived cfDNA have shown promising results in improving detection capabilities. Christians et al developed a workflow that enriches ultrashort and rare mcfDNA fragments prior to Karius test sequencing, enabling the identification of key AMR genes, such as SCCmec, mecA, mecC, vanA, vanB, blaCTX-M, and blaKPC, with diagnostic yields ranging from 56.8% to 83.3%.10 Sonntag et al further advanced this field by developing suppression PCR-based selective enrichment sequencing approach (SUSPECTS), which selectively amplifies AMR gene targets (vanA, vanB, tet) using suppression adapter ligation and multiplex suppression PCR before nanopore sequencing. This approach enables the identification of both pathogen and AMR-specific sequencing reads within minutes of sequencing, potentially reducing the turnaround time to 11–13 hours.59
Taken together, these advancements effectively bridge the gap between pathogen identification and actionable resistance profiling, offering clinicians timely and tailored treatment options, particularly for high-risk patients. In conclusion, the integration of mcfDNA analysis with host immune biomarkers, machine learning models, and AMR profiling offers a powerful multidimensional toolkit for infection diagnosis, particularly in complex clinical scenarios such as sepsis and immunocompromised patients. Ongoing research and technological innovations are expected to further enhance the clinical utility of these integrative strategies.
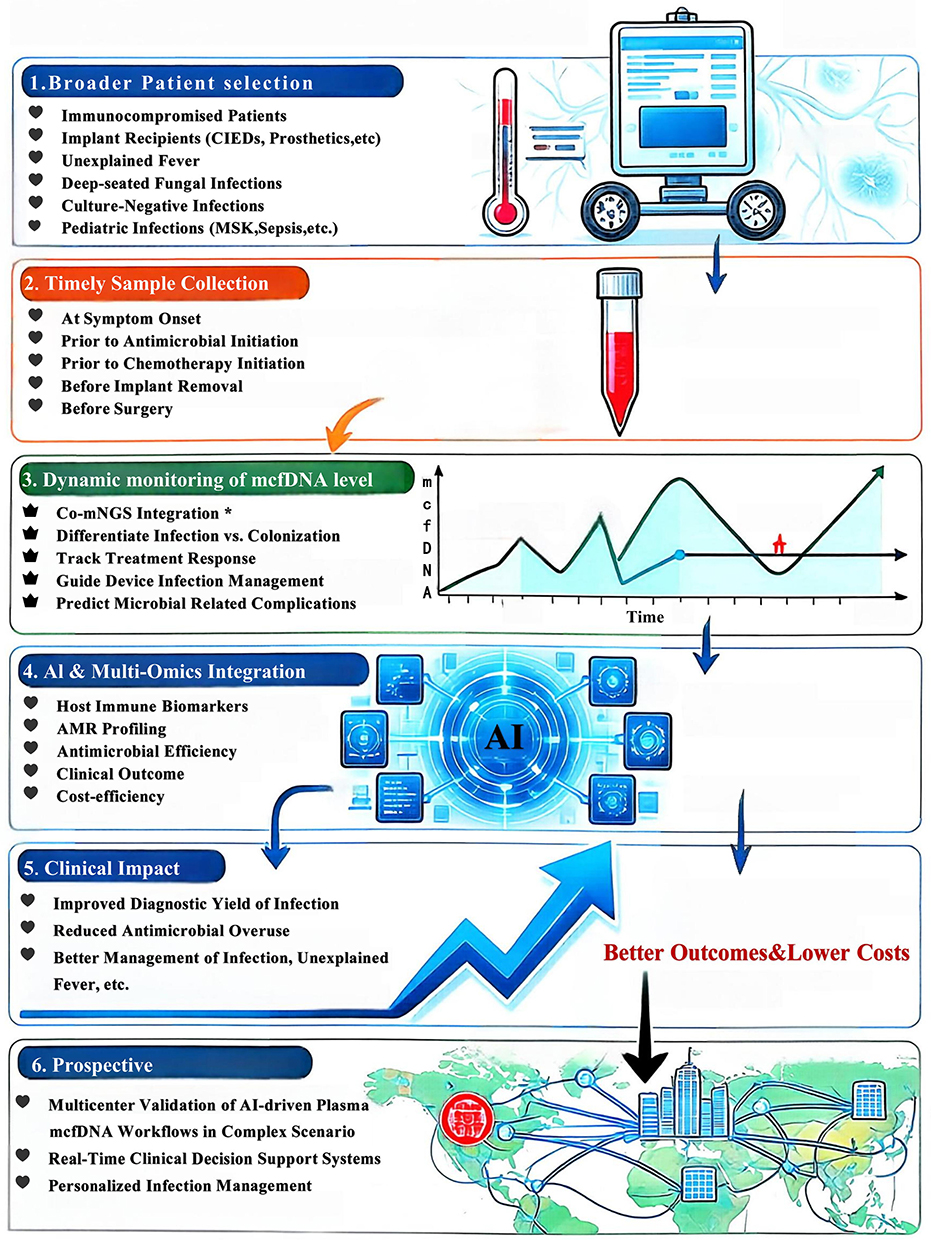 |
Figure 2 The refinement strategy of clinical utility of plasma mcfDNA sequencing and prospective. *Co-mNGS Integration (Plasma + Blood Cell DNA): Cost-effectiveness should be further investigated, particularly in resource-limited settings. Abbreviations: CIEDs, Cardiac implantable electronic devices; MSK, Musculoskeletal Infections; AMR, Antimicrobial Resistance. |
Conclusion and Future Prospective
Although the current clinical adoption rate of mcfDNA-seq is approximately 36%, suggesting the potential for broader implementation, its significant value, particularly in the management of high-risk patients, should not be underestimated. As an evolving diagnostic technology, existing evidence supports its role as a valuable complementary diagnostic tool, especially in clinical scenarios where conventional microbiological methods are inadequate. To optimize its clinical utility, we propose a four-step strategy for the implementation of plasma mcfDNA-seq, aimed at refining its application and improving patient management outcomes (Figure 2). The first strategy involves broadening the scope of patient selection. The application of plasma mcfDNA-seq should not be limited to immunocompromised individuals. Consideration should also be extended to patients with implanted medical devices, those presenting with unexplained fever, suspected deep-seated fungal infections, culture-negative infections, implanted devices (eg, cardiac implantable electronic devices, prosthetic joints), pediatric musculoskeletal infections or infections caused by fastidious microorganisms, etc. The second strategic imperative is to ensure the timely collection of blood samples. Early sample acquisition is crucial, particularly prior to antimicrobial/chemotherapy initiation or alteration, removing implants or surgery. This practical approach enhances the likelihood of detecting relevant microbial DNA, consequently improving the diagnostic yield. The third strategy involves dynamic monitoring of mcfDNA levels. Serial quantification of plasma mcfDNA both before and after antimicrobial treatment, transplantation, or surgical intervention can reveal critical trends in pathogen burden. The analysis of these temporal dynamics can help track treatment response, distinguish true infection from colonization, gut barrier function and guide decisions on device management, therapy duration, with persistence indicating complications like metastatic infection, septic shock or intestinal graft-versus-host diseases. Furthermore, the incorporation of co-mNGS, which encompasses both plasma and blood cell DNA sequencing, has the potential to enhance diagnostic sensitivity and clinical concordance. Controversies persist regarding comparator metrics and traditional blood cultures, with limited sensitivity and taxonomic scope, may undervalue plasma mcfDNA-seq’s unique ability to detect extracellular and fastidious pathogens. Meanwhile, blood cell sequencing excels at intracellular microbes, highlighting the complementary but not competitive roles of these modalities. The fourth strategic element focuses on integrating advanced data interpretation tools. The application of machine learning and AI-assisted models that incorporate plasma mcfDNA levels, host immune biomarkers, and antimicrobial resistance profiles can significantly enhance the accuracy and timeliness of early diagnosis and facilitate the implementation of targeted antimicrobial therapy.
Prospective validation of AI-driven liquid biopsy workflows to automate pathogen-AMR-host response integration, particularly in complex scenarios like unexplained fever, transplantation related complications, fungal device infections, pediatric infections or polymicrobial sepsis. As technical and analytical rigor advance, plasma mcfDNA-seq supported by ML and multi-compartmental sampling will redefine infectious disease diagnostics, offering culture-agnostic, time-sensitive insights to optimize targeted therapy across all patient populations.
Acknowledgments
This work was supported by the Natural Science Foundation of Chongqing, China (cstc2021 jcyj-msxmX0217) and the Chongqing Medical Scientific Research Project (Joint project of Chongqing Health Commission and Science and Technology Bureau, 2022QNXM002).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Blauwkamp TA, Thair S, Rosen MJ. et al. Analytical and clinical validation of a microbial cell-free DNA sequencing test for infectious disease. Nat Microbiol. 2019;4(4):663–12. doi:10.1038/s41564-018-0349-6
2. Xu C, Chen X, Zhu G, et al. Utility of plasma cell-free DNA next-generation sequencing for diagnosis of infectious diseases in patients with hematological disorders. J Infect. 2023;86(1):14–23. doi:10.1016/j.jinf.2022.11.020
3. Han DS, Li R, Shi JP, et al. Liquid biopsy for infectious diseases: a focus on microbial cell-free DNA sequencing. Theranostics. 2020;10(12):5501–5513. doi:10.7150/thno.45554
4. Park SY, Chang EJ, Ledeboer N, et al. Plasma Microbial Cell-Free DNA Sequencing from over 15,000 Patients Identified a Broad Spectrum of Pathogens. J Clin Microbiol. 2023;61(8):e0185522. doi:10.1128/jcm.01855-22
5. Hu Y, Zhao Y, Zhang Y, et al. Cell-free DNA: a promising biomarker in infectious diseases. Trends Microbiol. 2025;33(4):421–433. doi:10.1016/j.tim.2024.06.005
6. Hogan CA, Yang S, Garner OB, et al. Clinical Impact of Metagenomic Next-Generation Sequencing of Plasma Cell-Free DNA for the Diagnosis of Infectious Diseases: a Multicenter Retrospective Cohort Study. Clin Infect Dis. 2021;72(2):239–245. doi:10.1093/cid/ciaa035
7. Benamu E, Gajurel K, Anderson JN, et al. Plasma Microbial Cell-free DNA Next-generation Sequencing in the Diagnosis and Management of Febrile Neutropenia. Clin Infect Dis. 2022;74(9):1659–1668. doi:10.1093/cid/ciab324
8. Goggin KP, Gonzalez-Pena V, Inaba Y, et al. Evaluation of Plasma Microbial Cell-Free DNA Sequencing to Predict Bloodstream Infection in Pediatric Patients with Relapsed or Refractory Cancer. JAMA Oncol. 2020;6(4):552–556. doi:10.1001/jamaoncol.2020.0176
9. Weiss ZF, Pyden AD, Jhaveri TA, et al. The diagnostic and clinical utility of microbial cell-free DNA sequencing in a real-world setting. Diagn Microbiol Infect Dis. 2023;107(2):116004. doi:10.1016/j.diagmicrobio.2023.116004
10. Christians FC, Akhund-Zade J, Jarman K, et al. Analytical and clinical validation of direct detection of antimicrobial resistance markers by plasma microbial cell-free DNA sequencing. J Clin Microbiol. 2024;62(10):e0042524. doi:10.1128/jcm.00425-24
11. Madut DB, Chemaly RF, Dadwal SS, et al. Clinical Utility of Plasma Microbial Cell-Free DNA Sequencing Among Immunocompromised Patients With Pneumonia. Open Forum Infect Dis. 2024;11(8):ofae425. doi:10.1093/ofid/ofae425
12. Shah JR, Sohail MR, Lasco T, et al. Clinical utility of plasma microbial cell-free DNA sequencing in determining microbiologic etiology of infectious syndromes in solid organ transplant recipients. Therapeutic Advances in Infectious Disease. 2024;11:20499361241308643. doi:10.1177/20499361241308643
13. David JA, Kolipakkam B, Morales MK, et al. Cell-free plasma next-generation sequencing assists in the evaluation of secondary pneumonia in patients with COVID-19: a case series. Epidemiol Infect. 2023;151:e185. doi:10.1017/S0950268823001711
14. Vissichelli N, Degner N, Berman DM, et al. Meta-Analysis of Diagnostic Performance of Next Generation Sequencing of Plasma Microbial Cell-Free DNA for Infections in Hematopoietic Stem Cell Transplant Patients. Blood. 2022;140:13013–13014. doi:10.1182/blood-2022-167729
15. Filkins LM, Bryson AL, Miller SA, et al. Navigating Clinical Utilization of Direct-from-Specimen Metagenomic Pathogen Detection: clinical Applications, Limitations, and Testing Recommendations. Clin Chem. 2020;66(11):1381–1395. doi:10.1093/clinchem/hvaa183
16. Niles DT, Lee RA, Lamb GS, et al. Plasma cell-free metagenomic next generation sequencing in the clinical setting for the diagnosis of infectious diseases: a systematic review and meta-analysis. Diagn Microbiol Infect Dis. 2023;105(1):115838. doi:10.1016/j.diagmicrobio.2022.115838
17. Sutton AJ, Lupu DS, Bergin SP, et al. Cost-Effectiveness of Plasma Microbial Cell-Free DNA Sequencing When Added to Usual Care Diagnostic Testing for Immunocompromised Host Pneumonia. PharmacoEconomics. 2024;42(9):1029–1045. doi:10.1007/s40273-024-01409-4
18. Wang G, Lam WKJ, Ling L, et al. Fragment Ends of Circulating Microbial DNA as Signatures for Pathogen Detection in Sepsis. Clin Chem. 2023;69(2):189–201. doi:10.1093/clinchem/hvac197
19. Mzava O, Cheng AP, Chang A, et al. A metagenomic DNA sequencing assay that is robust against environmental DNA contamination. Nat Commun. 2022;13(1):4197. doi:10.1038/s41467-022-31654-0
20. Ranganath N, Bisono Garcia B, Vaillant J, et al. From Chart Biopsy to Liquid Biopsy: evaluating the Diagnostic Yield and Clinical Impact of Plasma Microbial Cell-Free DNA Next-Generation Sequencing in the Management of Fever of Unknown Origin. Open Forum Infect Dis. 2025;12(2):ofaf038. doi:10.1093/ofid/ofaf038
21. Almeida GG, Dumm R. Clinical Utility of Metagenomic Next-Generation Sequencing of Plasma Microbial Cell-Free DNA: a Single-Center Retrospective Study. Am J Clin Pathol. 2024;162:S170–S171. doi:10.1093/ajcp/aqae129.375
22. Bergin SP, Chemaly RF, Dadwal SS, et al. Plasma Microbial Cell-Free DNA Sequencing in Immunocompromised Patients With Pneumonia: a Prospective Observational Study. Clin Infect Dis. 2024;78(3):775–784. doi:10.1093/cid/ciad599
23. Lehman AC, Goren LR, Evans MD, et al. Clinical Performance of Plasma Metagenomic Sequencing in Immunocompromised Pediatric Patients. J Pediatric Infect Dis Soc. 2024;13(5):276–281. doi:10.1093/jpids/piae024
24. Petri F, Mahmoud OK, Ranganath N, et al. Plasma Microbial Cell-free DNA Next-generation Sequencing Can Be a Useful Diagnostic Tool in Patients With Osteoarticular Infections. Open Forum Infect Dis. 2024;11(7):ofae328. doi:10.1093/ofid/ofae328
25. Shean RC, Garrett E, Malleis J, et al. A retrospective observational study of mNGS test utilization to examine the role of diagnostic stewardship at two academic medical centers. J Clin Microbiol. 2024;62(9):e0060524. doi:10.1128/jcm.00605-24
26. Thompson RA-C, Donnelley MA, Trigg K, et al. Utility of microbial cell free DNA next-generation sequencing for diagnosis and management of infectious diseases. Diagn Microbiol Infect Dis. 2024;110(1):116334. doi:10.1016/j.diagmicrobio.2024.116334
27. Vinh Dong H, Saleh T, Kaur I, et al. Elucidating the Clinical Interpretation and Impact of a Positive Plasma Cell-Free DNA Metagenomics Test Result-A Single Center Retrospective Study. J Appl Lab Med. 2024;9(1):14–27. doi:10.1093/jalm/jfad083
28. Linder KA, Miceli MH. Impact of Metagenomic Next-Generation Sequencing of Plasma Cell-free DNA Testing in the Management of Patients With Suspected Infectious Diseases. Open Forum Infect Dis. 2023;10(8):ofad385. doi:10.1093/ofid/ofad385
29. Vissichelli NC, Morales MK, Kolipakkam B, et al. Cell-free next-generation sequencing impacts diagnosis and antimicrobial therapy in immunocompromised hosts: a retrospective study. Transpl Infect Dis. 2023;25(1):e13954. doi:10.1111/tid.13954
30. Shishido AA, Noe M, Saharia K, et al. Clinical impact of a metagenomic microbial plasma cell-free DNA next-generation sequencing assay on treatment decisions: a single-center retrospective study. BMC Infect Dis. 2022;22(1):372. doi:10.1186/s12879-022-07357-8
31. Wilke J, Ramchandar N, Cannavino C, et al. Clinical application of cell-free next-generation sequencing for infectious diseases at a tertiary children’s hospital. BMC Infect Dis. 2021;21(1):552. doi:10.1186/s12879-021-06292-4
32. Yu J, Diaz JD, Goldstein SC, et al. Impact of Next-Generation Sequencing Cell-free Pathogen DNA Test on Antimicrobial Management in Adults with Hematological Malignancies and Transplant Recipients with Suspected Infections. Transplant Cell Ther. 2021;27(6):500.e501–500.e506. doi:10.1016/j.jtct.2021.02.025
33. Lee RA, Al Dhaheri F, Pollock NR, et al. Assessment of the Clinical Utility of Plasma Metagenomic Next-Generation Sequencing in a Pediatric Hospital Population. J Clin Microbiol. 2020;58(7):e00419–20. doi:10.1128/JCM.00419-20
34. Feng S, Rao G, Wei X, et al. Clinical metagenomic sequencing of plasma microbial cell-free DNA for febrile neutropenia in patients with acute leukaemia. Clin Microbiol Infect. 2024;30(1):107–113. doi:10.1016/j.cmi.2023.05.034
35. Wang X, Zhang H, Zhang N, et al. Application value of metagenomic next-generation sequencing in hematological patients with high-risk febrile neutropenia. Front Cell Infect Microbiol. 2024;14:1366908. doi:10.3389/fcimb.2024.1366908
36. Han D, Yu F, Zhang D, et al. The Real-World Clinical Impact of Plasma mNGS Testing: an Observational Study. Microbiol Spectr. 2023;11(2):e0398322. doi:10.1128/spectrum.03983-22
37. Pang F, Xu W, Zhao H, et al. Comprehensive evaluation of plasma microbial cell-free DNA sequencing for predicting bloodstream and local infections in clinical practice: a multicenter retrospective study. Front Cell Infect Microbiol. 2023;13:1256099. doi:10.3389/fcimb.2023.1256099
38. Zhang P, Zhang Z-H, Liang J, et al. Metagenomic next-generation sequencing for the diagnosis of fever of unknown origin in pediatric patients with hematological malignancy. Clin Chim Acta. 2022;537:133–139. doi:10.1016/j.cca.2022.10.008
39. Esse J, Träger J, Steininger P, et al. Metagenomic analysis of microbial cell-free DNA from plasma of patients with suspected infections: performance and therapeutic impact in clinical routine. Clin Microbiol Infect. 2025;31(6):1018–1025. doi:10.1016/j.cmi.2025.02.016
40. De Vlaminck I, Martin L, Kertesz M, et al. Noninvasive monitoring of infection and rejection after lung transplantation. Proc Natl Acad Sci U S A. 2015;112(43):13336–13341. doi:10.1073/pnas.1517494112
41. Cao YH, Jiang TT, Lin YF, et al. Time-series prediction and detection of potential pathogens in bloodstream infection using mcfDNA sequencing. Front Cell Infect Microbiol. 2023;13:1144625. doi:10.3389/fcimb.2023.1144625
42. Heldman MR, Ahmed AA, Liu W, et al. Serial Quantitation of Plasma Microbial Cell-Free DNA Before and After Diagnosis of Pulmonary Invasive Mold Infections After Hematopoietic Cell Transplant. J Infect Dis. 2024;229(2):576–587. doi:10.1093/infdis/jiad255
43. Eichenberger EM, de Vries CR, Ruffin F, et al. Microbial Cell-Free DNA Identifies Etiology of Bloodstream Infections, Persists Longer Than Conventional Blood Cultures, and Its Duration of Detection Is Associated With Metastatic Infection in Patients With Staphylococcus aureus and Gram-Negative Bacteremia. Clin Infect Dis. 2022;74(11):2020–2027. doi:10.1093/cid/ciab742
44. Xu Y, Peng M, Zhou T, et al. Diagnostic performance of metagenomic next-generation sequencing among hematological malignancy patients with bloodstream infections after antimicrobial therapy. J Infect. 2025;90(2):106395. doi:10.1016/j.jinf.2024.106395
45. Wood JB, Russell K, Davis TE, et al. Plasma Microbial Cell-Free DNA Sequencing for Pathogen Detection and Quantification in Children With Musculoskeletal Infections. J Pediatric Infect Dis Soc. 2024;13(3):211–219. doi:10.1093/jpids/piae012
46. Eichenberger EM, Degner N, Scott ER, et al. Microbial Cell-Free DNA Identifies the Causative Pathogen in Infective Endocarditis and Remains Detectable Longer Than Conventional Blood Culture in Patients with Prior Antibiotic Therapy. Clin Infect Dis. 2023;76(3):E1492–E1500. doi:10.1093/cid/ciac426
47. Zhu Y, Miao H, Zhang J, et al. Role of plasma and blood-cell co-metagenomic sequencing in precise diagnosis and severity evaluation of sepsis, a prospective cohort study in sepsis patients. J Infect. 2025;90(3):106434. doi:10.1016/j.jinf.2025.106434
48. Karchmer AW, Kaufman NJ, Park SY, et al. Quantitative Microbial Cell-Free DNA Sequencing from Plasma: a Potential Biomarker for the Diagnosis of Staphylococcal Infection of Cardiac Implantable Electronic Devices. Clin Infect Dis. 2025:ciaf113. doi:10.1093/cid/ciaf113.
49. Grumaz S, Stevens P, Grumaz C, et al. Next-generation sequencing diagnostics of bacteremia in septic patients. Genome Med. 2016;8(1):73. doi:10.1186/s13073-016-0326-8
50. Lisius G, Duttagupta R, Ahmed AA, et al. Noninvasive diagnosis of secondary infections in COVID-19 by sequencing of plasma microbial cell-free DNA. iScience. 2023;26(11):108093. doi:10.1016/j.isci.2023.108093
51. Blair LM, Akhund-Zade J, Katsamakis ZA, et al. Circulating microbial cell-free DNA is increased during neutropenia after hematopoietic stem cell transplantation. Blood Adv. 2023;7(21):6744–6750. doi:10.1182/bloodadvances.2023010208
52. Wu C, Yu X, Gai W, et al. Diagnostic value of plasma and blood cells metagenomic next-generation sequencing in patients with sepsis. Biochem Biophys Res Commun. 2023;683:149079. doi:10.1016/j.bbrc.2023.10.011
53. Chen H, Zheng Y, Zhang X, et al. Clinical evaluation of cell-free and cellular metagenomic next-generation sequencing of infected body fluids. J Adv Res. 2024;55:119–129. doi:10.1016/j.jare.2023.02.018
54. Wang D, Zhang Z, Shen H, et al. Comparison of plasma and blood cell samples in metagenomic next-generation sequencing for identification of the causative pathogens of fever. Heliyon. 2024;10(11):e31677. doi:10.1016/j.heliyon.2024.e31677
55. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341–355. doi:10.1038/s41576-019-0113-7
56. Mogensen TH. Pathogen recognition and inflammatory signaling in innate immune defenses. Clin Microbiol Rev. 2009;22(2):240–273. doi:10.1128/CMR.00046-08
57. Yang HP, Haidar G, Al-Yousif NS, et al. Circulating microbial cell-free DNA is associated with inflammatory host-responses in severe pneumonia. Thorax. 2021;76(12):1231–1235. doi:10.1136/thoraxjnl-2020-216013
58. Wang LL, Tian WJ, Zhang WJ, et al. A Machine learning model for predicting sepsis based on an optimized assay for microbial cell-free DNA sequencing. Clin Chim Acta. 2024;559:119716. doi:10.1016/j.cca.2024.119716
59. Sonntag M, Elgeti VK, Vainshtein Y, et al. Suppression PCR-Based Selective Enrichment Sequencing for Pathogen and Antimicrobial Resistance Detection on Cell-Free DNA in Sepsis-A Targeted, Blood Culture-Independent Approach for Rapid Pathogen and Resistance Diagnostics in Septic Patients. Int J Mol Sci. 2024;25(10):5463. doi:10.3390/ijms25105463
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.