Back to Journals » Clinical Ophthalmology » Volume 16
Reduction of Myopic Progression Using a Multifocal Soft Contact Lens: A Retrospective Cohort Study
Authors Cooper J, O'Connor B, Aller T ![]() , Dillehay SM, Weibel K, Benoit D
, Dillehay SM, Weibel K, Benoit D ![]()
Received 14 April 2022
Accepted for publication 15 June 2022
Published 4 July 2022 Volume 2022:16 Pages 2145—2155
DOI https://doi.org/10.2147/OPTH.S370041
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jeffrey Cooper,1,2 Brett O’Connor,3 Thomas Aller,4,5 Sally M Dillehay,6 Katherine Weibel,7 Douglas Benoit8
1Cooper Eye Care, New York, NY, USA; 2State University of New York College of Optometry, New York, NY, USA; 3MyEyeDr – Mandarin, Jacksonville, FL, USA; 4Dr. Thomas Aller, Optometrist, Inc., San Bruno, CA, USA; 5University of California, Berkeley School of Optometry, Berkeley, CA, USA; 6ClintrialSolutions, LLC, Roswell, GA, USA; 7The Ohio State University College of Medicine, Department of Ophthalmology, Columbus, OH, USA; 8Visioneering Technologies, Inc., Alpharetta, GA, USA
Correspondence: Douglas Benoit, Visioneering Technologies, Inc, Alpharetta, GA, 30009, USA, Email [email protected]
Purpose: To evaluate myopia progression over an approximately 6-year follow-up period in children and young adults wearing a commercially available, daily disposable, soft multifocal contact lens with an extended depth of focus (center distance) design.
Methods: This retrospective cohort analysis included data from 196 patients of mean (SD) age 12.3 (2.7) years (range, 5– 20 years), fit with the NaturalVue Multifocal (NVMF) contact lens at 15 practices in the United States over 6 years. All patients showed at least − 0.50D of myopic progression in at least one eye prior to wearing the lens. Data from the right eye were analyzed. One-way ANOVA with Tukeys post-hoc t-tests were used for statistical analysis, with a significance level set at P < 0.05.
Results: After wearing these lenses for 6– 72 months, the average myopia progression slowed by approximately 0.84 D or 85% compared to baseline, which was statistically significant at all time points (P < 0.0001). Frequency distribution revealed that 91% of wearers showed a decrease in myopia progression compared to baseline, with 79% of wearers showing a ≥ 70% reduction in myopia progression. The average change in axial length in a subset of the population over 47 months of follow-up was approximately 0.10 mm/year. Compared with changes expected in an age- and ethnicity-matched myopic virtual control group obtained from published meta-analysis data, both myopic refractive error progression and axial elongation were significantly lower in NVMF wearers at 12, 24 and 36 months (P < 0.001). Analysis of the age- and ethnicity-matched virtual control group predicted that the Cumulative Absolute Reduction of axial Elongation (CARE) value over 3 years would be 0.45 mm.
Conclusion: Wearers of the soft multifocal contact lens displayed significant reductions in myopia progression throughout a follow-up period of 6 years.
Keywords: myopia, myopia progression control, soft multifocal contact lenses, peripheral hyperopia
Introduction
Myopia is the most frequent cause of distance vision impairment in the world.1 The prevalence of myopia is increasing markedly, and it is projected to affect 50% of the world population by 2050.1–3 The comorbidities associated with myopic axial elongation, including glaucoma, retinal detachment, cataract, and myopic macular degeneration, emphasize the importance of halting or slowing the progression of myopia.3–6 Clinical findings and animal studies have provided substantial support for various interventions for the treatment of myopia,3,7 including spectacles, orthokeratology, center-distance soft multifocal contact lenses, and atropine.8–10 Meta-analyses have shown that all of these slow the progression of myopia to some extent.11–15
Multiple soft multifocal contact lenses, which contain relative peripheral plus power of varying degrees, have been shown to slow the progression of myopia.16–24 Recent 3-year, randomized clinical trials have assessed the ability of MiSight dual-focus soft contact lenses (CooperVision, Victor, NY)18,25 and Biofinity center-distance multifocal soft contact lenses (CooperVision) to slow the progression of myopia.17 In data submitted to the US FDA for regulatory approval, MiSight contact lenses demonstrated an adjusted mean difference of 0.67 D from control lenses in refractive error change and an adjusted mean difference of 0.28 mm from control lenses in axial length change after 3 years.25 To date, MiSight remains the only US FDA approved treatment for slowing the progression of myopia.
The results obtained in the Bifocal Lenses in Nearsighted Kids (BLINK) trial of Biofinity center-distance multifocal soft contact lenses were similar to those of MiSight lenses, based on a broad overlap of the 95% confidence intervals (CI) for their primary outcomes.17,18,25 The BLINK trial tested Biofinity center-distance multifocal contact lenses (+1.50 D and +2.50 D add), and Biofinity single vision lenses (CooperVision), both of which are intended for monthly replacement. The +2.50 D add lenses demonstrated an adjusted mean difference of 0.46 D from control single vision lenses in refractive error change and an adjusted mean difference of 0.23 mm from control in axial length change after 3 years. This trial also showed that the higher add (+2.50 D) lenses were more effective than the medium add (+1.50 D) lenses for slowing the progression of myopia, suggesting a possible dose-response relationship between soft multifocal add power and myopic progression control, although this has only been shown in animal models.26
A retrospective case series analyzed a daily disposable soft multifocal lens with a distance center and a large amount of relative plus power surrounding the center (NaturalVue Multifocal [NVMF] 1 Day, Visioneering Technologies, Inc., Alpharetta, GA)27 in 32 myopic children, of mean (SD) age 10.98 (2.95) years, at 10 practice locations in the United States.16 The original study16 was developed after a small group of practitioners having an informal discussion of their methods for managing myopia discovered that they each were using NVMF with good success. Since these patients existed in each practice involved in the study, they decided to use a retrospective analysis. Every chart of any individual wearing NVMF for myopia control was evaluated, regardless of the outcome with the lenses.
The NaturalVue (etafilcon A) Multifocal 1 Day contact lens is a unique, patented, center-distance, extended depth of focus design, with an 8.3mm base curve, a 14.5mm lens diameter, a power range from +4.00D to −12.25D, and a universal add. The NVMF lenses incorporate an extended depth of focus design with up to 20 diopters (D) of relative peripheral plus power at their edges. Using specialized software required to measure their tangential power, the through the lens power at the edge of a child’s pupil, estimated at 5 mm, would be approximately 6–8D of relative plus power, building in 5 micron steps from the center of the lens design.28 It is theorized that this large amount of peripheral plus power may reduce peripheral hyperopic defocus and thus decrease the signal for axial elongation.7 NVMF lenses have received indications for myopia progression control in Europe, Australia, New Zealand, Hong Kong, Singapore, and Canada, but not yet in the USA.29
In the initial retrospective cohort analysis of NVMF lenses in 32 children, the mean (SD) duration was 10.94 (4.76) months, ranging from 6 to 25 months.16 The aim of the current study was to extend these findings over a longer period of time within a larger population of young myopes, and to contribute further to the knowledge base of myopia progression control using soft multifocal contact lenses for extended time periods.
Methods
This retrospective cohort analysis evaluated 196 patients of mean (SD) age at NVMF fitting of 12.3 (2.7) years (range, 5–20 years), from 15 practices in the United States fit with NVMF lenses between December 2014 and December 2020. Records from a total of 840 patient visits were reviewed. All the patients wore these lenses for a minimum of 6 months and were followed-up at regular 6 months intervals for up to 72 months. Patients were included if they had at least −0.50 D of myopic progression in at least one eye prior to NVMF correction, which was the clinical criterion used by most of these practitioners when prescribing an intervention for myopic progression. Only patients without prior myopic progression control treatment were included. To minimize bias in this type of retrospective cohort analysis, practitioners were required to provide data on all patients fit with NVMF during the study period, regardless of the outcomes of lens wear.
The NVMF lenses were prescribed at each clinical practice based on the best clinical judgment at each site. Parents and patients were advised that the lens design was able to control axial length growth in animal studies;26 that clinical and theoretical data supported its use to slow myopic progression in humans;7 and that real-world evidence showing efficacy in humans had been published.16 Patients and their parents provided verbal assent and consent, respectively, for the off-label use of these lenses, consistent with standard clinical practice. They were advised that they could refuse or discontinue treatment at any time. Fees for professional services and materials were billed and collected consistent with the practices’ fees for the services and materials.
Before the data were analyzed, they were de-identified and sent to one person for central analysis. Because of the retrospective nature of the data review and the use of deidentified data, the study met the Exempt Criteria per 45 CFR 46.101 (b)(4). Therefore, written informed consent/assent was not required, and a waiver was obtained from the Southwest Independent Institutional Review Board, Inc. (SI-17-10). The waiver for a retrospective study comports with the tenets of the Declaration of Helsinki.
Clinical Assessments
All options to slow the progression of myopia were discussed with the parents and children. Parents and children were also provided the option of simply continuing to monitor the child’s myopic progression with single vision glasses or contact lenses. The benefits and risks associated with each of these interventions were discussed. At each examination, a refraction was performed, and axial length was measured, if equipment was available at that practice location. Because this was not a randomized control trial with specific equipment requirements, instrumentation varied from practice to practice. Refraction techniques also varied between sites, with some doing cycloplegic autorefraction and some not. Generally, the same method for refraction was followed for all subjects within a practice. Refractions were performed at least annually, but more often if warranted. Visit frequency also varied from site to site based on the practitioner’s clinical judgement for each individual subject. Usually, subjects were seen every 3 to 6 months.
Assessing Effectiveness of Treatment
Baseline myopic progression was determined by annualizing the data due to the differing time frames of prior examination, whereas myopic progression with NVMF lens wear was determined by recording actual progression over time. Each child served as his/her own historical control, based on annualized myopic progression for the 12 months prior to wearing NVMF lenses. The initial analysis included data from the right eye of each subject.
Statistical Analysis
The study results were grouped into timeframe categories based on how long the child had worn the NVMF lenses. Statistical analyses were performed using one-way ANOVA with Tukey’s HSD post-hoc t-tests, with statistical significance set at P < 0.05.
Results
The study cohort consisted of 196 patients with myopia, of mean (SD) age at NVMF fitting of 12.3 (2.7) years (range, 5–20 years). These patients included 101 (51.5%) females and 95 (48.5%) males, with the population being 59% Caucasian, 20% Eastern Asian/Asian, and 21% other. At baseline, the range of spherical equivalent prescriptions was +0.10 to −11.60 D, and the average (SD) annual myopic progression was −0.98 (0.78) D. The average annual axial length change (SD) observed was 0.30 (1.2) mm. Of the 196 children, 152 (77.6%) completed at least 1 year of wear (range, 12–17 months), 101 (51.5%) completed at least 2 years (range 24–29 months), 64 (32.7%) completed at least 3 years (range, 36–41 months), 15 (7.7%) completed at least 4 years (range, 48–53 months), eight (4.1%) completed at least 5 years (range, 60–65 months), and seven (3.6%) completed 66–72 months of wear.
Treatment Outcomes
The annualized mean (SD) myopic progression prior to correction with NVMF was −0.98 (0.78) D/yr. Compared with baseline, each subsequent time point showed an approximately 85% (0.84 D/yr) reduction in average myopia progression, with these reductions being statistically significant at all time points (P < 0.0001; Figure 1). Overall, 91% of wearers showed reductions in myopic progression, with 79% showing ≥70% reductions in myopic progression and 69% having no increase in myopic progression from the time they started wearing the lenses through their last follow-up visit. These results are very similar to those of the original retrospective cohort analysis with 32 subjects wearing NVMF.16
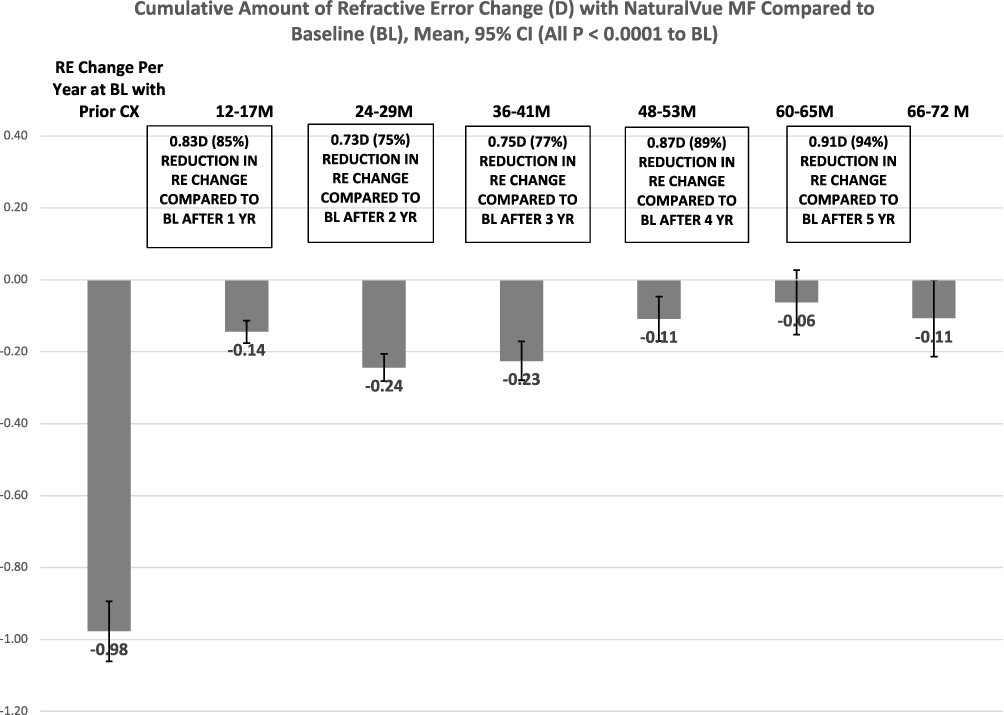 |
Figure 1 Change over time in refractive error (D) while wearing NaturalVue Multifocal lenses compared with baseline annualized myopic progression. Refractive error at all time points differed significantly when compared with baseline (P < 0.0001). |
From 6 through to 72 months, the average cumulative myopia progression while wearing NVMF never exceeded approximately 0.25 D from baseline. Only 14 (7.0%) lens wearers experienced an increase in myopia from baseline through their last follow-up examination, with on average (SD) increase of −0.26 (0.17) D (range: −0.02 to −0.50D; 95% CI −0.13, −0.39 D).
Not all of the clinical sites had instrumentation to measure axial length, with some acquiring this equipment during the study period. Baseline axial length was measured in only eight patients, with these having an average (SD) annual axial length change at baseline of 0.30 (1.2) mm. Axial length measured in 58 patients after 1 year of wearing NVMF lenses was found to increase a mean (SD) of 0.07 (0.2) mm. The mean (SD) cumulative axial length increases from baseline after 2 years in 32 subjects and 3 years in 14 subjects of NVMF wear, were 0.15 (0.18) mm and 0.14 (0.16) mm, respectively. The average axial length change after wearing NVMF for 47 months was approximately 0.10 mm per year. Because most of the children had not been examined prior to the onset of myopia and/or because axial length was not routinely measured in all young children, baseline axial length measurements were not generally available for this population.
Comparison to MiSight and BLINK Clinical Trial Data
The success of an intervention for myopia control may be assessed by comparing results to those of randomized controlled trials (RCTs), by determining average myopia progression in age-matched children wearing single vision corrective lenses.30 Therefore, a subgroup analysis was performed to compare the 3-year results with NVMF lenses with those of the MiSight and the BLINK high add (+2.50D) lenses.17,18 The enrollment criteria for the MiSight and BLINK trials differed slightly, with the MiSight trial assessing patients aged 8–12 yrs and with starting refraction of −0.75D to −4.00D and the BLINK trial enrolling patients aged 7–11 yrs and with starting refraction of −1.00D to −5.00D. NVMF wearers of the same age at enrollment as those in the MiSight trial were used for this comparison, and an all-available eyes analysis for 41 children of mean (SD) age 10.3 (1.3) years was used to match the data available for MiSight.25 The demographic characteristics of these groups of children are shown in Table 1.
 |
Table 1 Baseline Demographic Characteristics of Age-Matched NaturalVue Multifocal Wearers and Subjects in the MiSight and BLINK Trials17,18,25 |
The designs of the MiSight and BLINK RCTs allowed for use of their Control group data to directly compare MiSight, BLINK high add (+2.50D) and NVMF results for myopic progression through 3 years (Table 2).
 |
Table 2 Comparison of Myopic Progression Over 3 Years for Age-Matched NaturalVue Multifocal Wearers and Subjects in the MiSight and BLINK Trials17,18,25 |
To further evaluate the ability of NVMF lenses to slow the progression of myopia, refractive error and axial length progression in 66 NVMF lens wearers aged 8–12 years, of mean (SD) age 10.32 (1.3) years and including 32 (48%) children of Asian ethnicity, were compared with the refractive error and axial length progression in children matched by age and ethnicity (Asian or non-Asian) in published meta-analyses of data30–34 from 63 clinical trials. This approach of using an age and/or ethnicity matched virtual control group has been used in other studies to evaluate myopia control.37–41 The mean refractive error and axial length progression for each child in the age and ethnicity matched virtual control group were calculated based on the data in the meta-analyses.30–34
Both refractive error progression (P < 0.0001; Figure 2) and axial length elongation (P < 0.0001; Figure 3) were significantly lower throughout 3 years of wear of NVMF lenses compared with a virtual control group of age and ethnicity matched myopic children from published meta-analyses.30–34
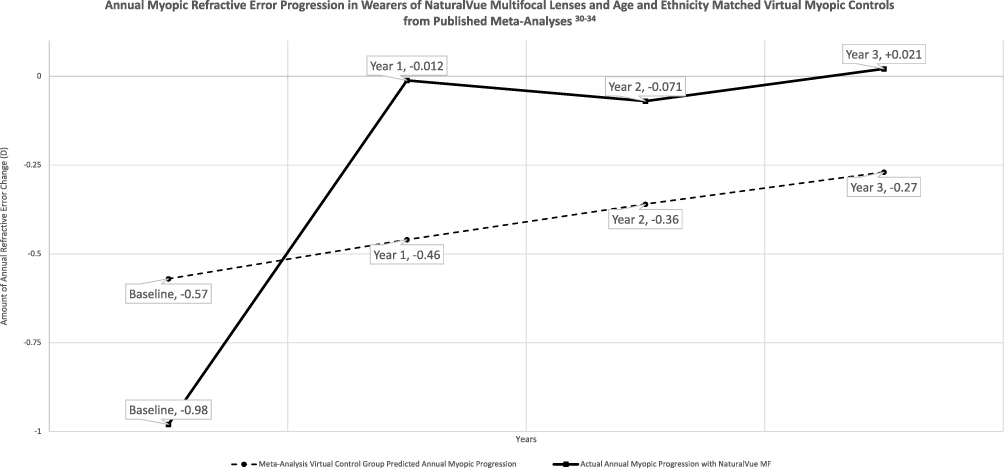 |
Figure 2 Annual myopic refractive error progression in wearers of NaturalVue multifocal lenses and age and ethnicity matched virtual myopic controls from published meta-analyses.30–34 |
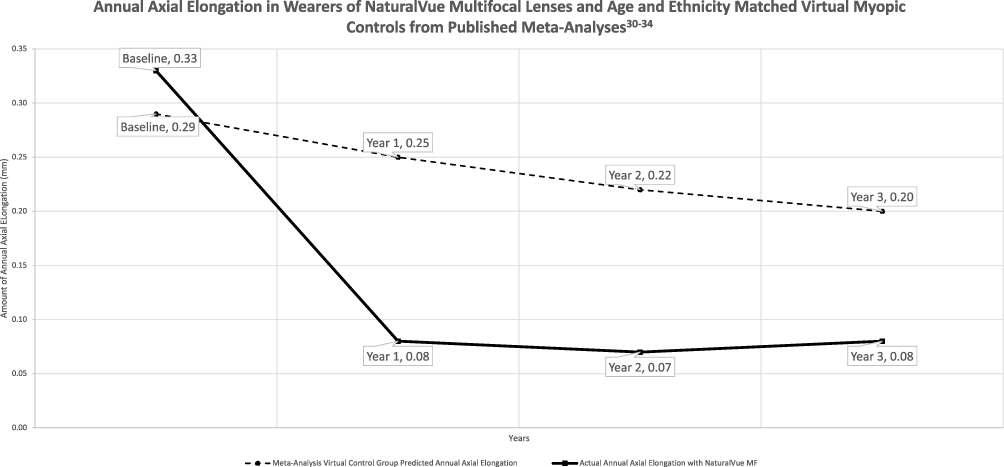 |
Figure 3 Annual axial elongation in wearers of NaturalVue multifocal lenses and age and ethnicity matched virtual myopic controls from published meta-analyses.30–34 |
Discussion
This real-world study assessed whether wearing NVMF contact lenses slowed myopic progression in myopic children. On average, NVMF lens wearers experienced ≤0.25D cumulative myopic progression from baseline throughout the 6 years of follow-up and those in whom axial length was measured showed approximately 0.10 mm of axial length progression per year through 4 years of follow-up.
Although before and after treatment comparisons have limitations, they have been used to evaluate other myopia control interventions, as they are the only method of evaluating the efficacy of treatment in individual patients.35–38 Comparisons to data in control groups17,18,25,39–41 and to the average progression of refractive error and axial length in virtual control groups of age and ethnicity matched patients from meta-analyses30–34 can help gauge the success of NVMF lenses for myopia control. Because treatment efficacy cannot be determined in individuals, the annual progression observed with NVMF lenses can be compared with the average annual progression in subjects from multiple clinical studies, thus setting better myopia control expectations for patients and their parents or guardians.
Data from the age and ethnicity matched virtual control group are of particular interest, as NVMF lens wearers showed greater initial rates of progression of both refractive error and axial elongation than predicted for their age and ethnicity. Despite these more rapid initial rates of progression, NVMF lens wearers showed much lower annual rates of refractive error and axial elongation progression than the age and ethnicity matched virtual control group.30–34
Recently, a new efficacy metric was introduced called the Cumulative, Absolute, Reduction in axial Elongation (CARE).42 It is an empirically demonstrated, evidence-based articulation of myopia control effect reasonably expected for a given treatment over a given time. It communicates the benefit that a child receiving a specific treatment might expect independently of age, progression rate, refractive error, and ethnicity over a stated time period. The projected CARE value in this group was 0.45 mm over 3 years, a result comparable to those of other interventions for which CARE values have been calculated.50 The CARE value can also be used to estimate the amount of reduction of refractive error change by multiplying it by 2.1.50 Therefore, using the virtual-control group data derived by Nixon and Brennan from over 63 randomized clinical trials as a comparison,42 the CARE value projects that NVMF would show 0.945D less myopic progression over 3 years than a child who was not treated with the lenses.
The patients in the present study may differ from those recruited for clinical trials. Parents seeking care to slow the progression of myopia are often high myopes themselves and thus more motivated to participate in treatment. Practitioners may also show selection bias, in that treatment of these children may be based on the amount of myopic progression observed at baseline. Also, these practitioners generally chose to treat children who had shown a ≥-0.50D progression of myopia since their previous examination.
It has been suggested that annual progression prior to an intervention for myopic progression should not be used as a baseline indicator of treatment efficacy.42 In clinical practice, however, this is the most available indicator to determine the efficacy of treatment. Similar to other treatments, both patients and clinicians are concerned with treatment-associated changes. For example, a recent 3-year study of atropine use in European children used a similar approach, comparing myopic progression after starting atropine treatment with baseline myopia.35 Although randomized clinical trials are required for submission to regulatory agencies, clinicians in real-world clinical practice can only compare pre- and post-intervention myopic progression on an individual basis. Comparisons of the performance of NVMF lenses with control groups and data from meta-analyses provide a more robust way of evaluating NVMF lenses as a potential intervention for myopic progression.
Yearly data on refractive error and axial length in the control groups from the MiSight and BLINK trials showed linear progression of myopia in children aged 7–12 years, a finding also observed in other control groups.43,44 Age has been found to be the primary factor driving myopic progression.9,45 For example, a recent 5-year analysis evaluated 6855 ethnically diverse Americans aged 12–25 years who were enrolled in the National Health and Nutrition Examination Survey.46 In the final multivariate models, age and female sex were the two most significant factors relative to the presence or absence of myopia as well as refractive error. These findings support the approaches used in the present study, comparing annual changes observed with NVMF lenses with an age-matched control group and data from meta-analyses.
Unlike data obtained from a randomized clinical trial (RCT), real-world data, such as those in the present study, allow clinicians to estimate likely outcomes when NVMF lenses are used to slow myopia progression. Regulatory agencies have begun to accept real-world evidence data regarding the usage, including the potential benefits and risks, of medical products, as traditional clinical trials have strict limitations that may not always apply to clinical practice.47 In clinical practice, the age and power limitations required in clinical trials are not considered, and patients/parents must pay for product and services out of pocket. Based on clinical experience, parents are generally not interested in the results of control groups in RCTs; rather, they are interested in what they can expect from treatment of their child. By matching sub-groups based on age at enrollment with the data from age-matched control groups in the MiSight and BLINK RCTs, it is possible to apply reasonable, albeit directional, comparison of the results observed with NVMF, MiSight and BLINK high add (+2.50D) lenses.
The MiSight and BLINK contact lenses differ in the amount of peripheral plus manifested in their optical profiles. MiSight lenses have +2.00D25 in the periphery in alternating bands, whereas BLINK lenses (“D” lenses) have a reported add of +2.50D.48 NVMF lenses are designed to have approximately 6–8D of additional plus power in the periphery at the edge of the pupil (estimated to be 5 mm).27,28 Clinical trials comparing NVMF with other lenses are required to directly determine differences in their effectiveness in slowing the progression of myopia.
In this current cohort analysis, 79% of wearers experienced a ≥70% reduction in myopia progression compared with their prior year progression. Over a three-year period, 91% of NVMF wearers and 41.3% of MiSight wearers progressed only 0.25D over 3 years; data on progression in the BLINK trial were only reported at the >1.00D level.
The amount of axial length change from baseline was measured in a subset of the patients wearing NVMF lenses. Compared with baseline, the average axial length increase over 47 months was approximately 0.10 mm/yr. This growth rate was similar to that expected in emmetropic children, ie, 0.10–0.13 mm/year for children aged 8–13 years,40,49 providing further evidence that NVMF lenses can reduce refractive error and axial length changes over an extended period of time.
Comparisons of the current cohort analysis of NVMF lens wearers with those in the previous study showed several important similarities and differences. For example, 32 children who wore NVMF lenses for 6 to 25-months showed a significant decrease in myopia progression from baseline of about 0.86 D, or an average 96% in both eyes, and 90% showed a ≥70% reduction in myopic progression.16 Although both analyses provide evidence of decreases in myopia progression with NVMF lens wear, the present study reported actual progression rates, whereas the previous study reported annualized rates. Also, in contrast to the previous study, the present study included subjects with no prior treatment for myopic progression. Differences in the results of the two studies may be due to the inclusion in the present study of a larger patient population (196 versus 32 subjects) and a longer maximum follow-up time (72 months versus 25 months).
Limitations
This current study is a retrospective cohort analysis capturing real-world data. Interventions for myopic progression were determined by the clinical judgment of each practitioner, which has the potential for selection bias. For example, some practitioners with awareness of certain interventions may have an unconscious bias to utilize that intervention in higher amounts of baseline myopia progression. Not all practitioners used cycloplegic autorefraction measurements to assess refractive error progression, although measurement methods were consistent within each practice. Different instruments were used in these clinical practices, which may have increased the variability of the data. Some of the sample sizes for axial length measurements were small, indicating the need for larger sample sizes to draw conclusions about axial length growth with NVMF lens wear.
When comparing these outcomes with those of parallel groups in RCTs,17,18,25 it should be noted that myopia progression decreases with age. Therefore, comparisons before and after treatment may show greater apparent efficacy than would be observed in studies having separate control groups. However, the virtual control group from published meta-analyses30–34 was both age and ethnicity matched, accounted for children aging throughout the 3 years of follow-up, and demonstrated significant slowing of both refractive error and axial length progression in the NVMF group.
Conclusion
The current cohort analysis demonstrated that wearers of NVMF daily disposable soft contact lenses exhibited significant reductions in myopia progression over an extended follow-up period of 6 years (72 months), complementing the original study. The results are in agreement with previous analyses of optical interventions to slow the progression of myopia. Although sample sizes were small for AL change due to equipment limitations at the clinical practices at baseline, the results showed significant inhibition of axial length elongation in that subset. Although more research is warranted, NVMF lenses appear to be effective in slowing the progression of myopia in children.
Acknowledgments
The authors thank Drs. Chad Carlsson, Kevin Chan, Alan Glazier, Jeff Jeruss, Viola Kanevsky, Jennifer Lee, Roy Park, Susan Resnick, David Sweeney, Danica Yang, Nadine Eisenberg and Amber Zaunbrecher for contributing data for this analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Visioneering Technologies, Inc., provided financial support for data collection and manuscript preparation for this research.
Disclosure
Jeffrey Cooper, MS, OD: Consultant to Visioneering Technologies, Inc.
Brett O’Connor, OD: Consultant to Visioneering Technologies, Inc.
Thomas Aller, OD: Consultant to Visioneering Technologies, Inc. Advisory board member for Treehouse Eyes, Haag-Streit, and Reopia Optics. Stockholder in Treehouse Eyes. Personal fees from Essilor, personal fees from Essilor Amera, LTD, other from Reopia Optics, Ic., grants, personal fees, non-financial support from BHVI, personal fees from Nevakar, outside the submitted work; In addition, Dr Thomas Aller has a patent 6752499 licensed to Vision CRC, a patent 10175502 licensed to Vision CRC, a patent 9477097 licensed to Vision CRC, a patent 8240847 licensed to Vision CRC, a patent 8672472 licensed to Vision CRC, a patent 20170010478 licensed to Vision CRC, a patent 20140132914 licensed to Vision CRC, a patent 2014078039 licensed to Vision CRC, a patent PI 20084968 licensed to Vision CRC, a patent 049.4323 licensed to Vision CRC.
Sally M. Dillehay, OD, EdD: Former employee of and Consultant to Visioneering Technologies, Inc. Listed on VTI patents.
Katherine Weibel, OD: Consultant to Visioneering Technologies, Inc.
Douglas P. Benoit, OD: Employee of and stockholder in Visioneering Technologies, Inc.
The authors report no other conflicts of interest in this work.
References
1. Holden B, Sankaridurg P, Smith E, Aller T, Jong M, He M. Myopia, an underrated global challenge to vision: where the current data takes us on myopia control. Eye. 2014;28(2):142–146. doi:10.1038/eye.2013.256
2. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
3. Cooper J, Tkatchenko AV. A review of current concepts of the etiology and treatment of myopia. Eye Contact Lens. 2018;44(4):231–247. doi:10.1097/ICL.0000000000000499
4. Mitchell P, Hourihan F, Sandbach J, Wang JJ. The relationship between glaucoma and myopia: the Blue Mountains Eye Study. Ophthalmology. 1999;106(10):2010–2015. doi:10.1016/S0161-6420(99)90416-5
5. Ogawa A, Tanaka M. The relationship between refractive errors and retinal detachment–analysis of 1166 retinal detachment cases. Jpn J Ophthalmol. 1988;32(3):310–315.
6. Saw SM, Gazzard G, Shih-Yen EC, Chua WH. Myopia and associated pathological complications. Ophthalmic Physiol Opt. 2005;25(5):381–391. doi:10.1111/j.1475-1313.2005.00298.x
7. Smith EL. Prentice Award Lecture 2010: a case for peripheral optical treatment strategies for myopia. Optom Vis Sci. 2011;88(9):1029–1044. doi:10.1097/OPX.0b013e3182279cfa
8. Cooper J, Weibel K, Borukhov G. Use of atropine to slow the progression of myopia: a literature review and guidelines for clinical use. Vision Dev Rehabil. 2018;4(1):12–28.
9. Bullimore MA, Richdale K. Myopia control 2020: where are we and where are we heading? Ophthalmic Physiol Opt. 2020;40(3):254–270. doi:10.1111/opo.12686
10. Walline JJ, Lindsley KB, Vedula SS, et al. Interventions to slow progression of myopia in children. Cochrane Database Syst Rev. 2020;1(1):CD004916. doi:10.1002/14651858.CD004916.pub4
11. Gong Q, Janowski M, Luo M, et al. Efficacy and adverse effects of atropine in childhood myopia: a meta-analysis. JAMA Ophthalmol. 2017;135(6):624–630. doi:10.1001/jamaophthalmol.2017.1091
12. Huang J, Wen D, Wang Q, et al. Efficacy comparison of 16 interventions for myopia control in children: a network meta-analysis. Ophthalmology. 2016;123(4):697–708. doi:10.1016/j.ophtha.2015.11.010
13. Li SM, Wu SS, Kang MT, et al. Atropine slows myopia progression more in Asian than white children by meta-analysis. Optom Vis Sci. 2014;91(3):342–350. doi:10.1097/OPX.0000000000000178
14. Li SM, Kang MT, Wu SS, et al. Efficacy, safety and acceptability of orthokeratology on slowing axial elongation in myopic children by meta-Analysis. Curr Eye Res. 2016;41(5):600–608. doi:10.3109/02713683.2015.1050743
15. Li SM, Kang MT, Wu SS, et al. Studies using concentric ring bifocal and peripheral add multifocal contact lenses to slow myopia progression in school-aged children: a meta-analysis. Ophthalmic Physiol Opt. 2017;37(1):51–59. doi:10.1111/opo.12332
16. Cooper J, O’Connor B, Watanabe R, et al. Case series analysis of myopic progression control with a unique extended depth of focus multifocal contact lens. Eye Contact Lens. 2018;44(5):e16–e24. doi:10.1097/ICL.0000000000000440
17. Walline JJ, Walker MK, Mutti DO, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children: the BLINK randomized clinical trial. JAMA. 2020;324(6):571–580. doi:10.1001/jama.2020.10834
18. Chamberlain P, Peixoto-de-Matos SC, Logan NS, Ngo C, Jones D, Young G. A 3-year randomized clinical trial of MiSight lenses for myopia control. Optom Vis Sci. 2019;96(8):556–567. doi:10.1097/OPX.0000000000001410
19. Ruiz-Pomeda A, Perez-Sanchez B, Valls I, Prieto-Garrido FL, Gutiérrez-Ortega R, Villa-Collar C. MiSight Assessment Study Spain (MASS). A 2-year randomized clinical trial. Graefes Arch Clin Exp Ophthalmol. 2018;256(5):1011–1021. doi:10.1007/s00417-018-3906-z
20. Anstice NS, Phillips JR. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology. 2011;118(6):1152–1161. doi:10.1016/j.ophtha.2010.10.035
21. Sankaridurg P, Bakaraju RC, Naduvilath T, et al. Myopia control with novel central and peripheral plus contact lenses and extended depth of focus contact lenses: 2 year results from a randomised clinical trial. Ophthalmic Physiol Opt. 2019;39(4):294–307. doi:10.1111/opo.12621
22. Walline JJ, Greiner KL, McVey ME, Jones-Jordan LA. Multifocal contact lens myopia control. Optom Vis Sci. 2013;90(11):1207–1214. doi:10.1097/OPX.0000000000000036
23. Aller TA, Liu M, Wildsoet CF. Myopia control with bifocal contact lenses: a randomized clinical trial. Optom Vis Sci. 2016;93(4):344–352. doi:10.1097/OPX.0000000000000808
24. Aller TA, Wildsoet C. Bifocal soft contact lenses as a possible myopia control treatment: a case report involving identical twins. Clin Exp Optom. 2008;91(4):394–399. doi:10.1111/j.1444-0938.2007.00230.x
25. US Food & Drug Administration. MiSight 1 day (omafilcon A) soft (hydrophilic) contact lenses for daily wear. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf18/P180035B.pdf.
26. Woods J, Guthrie SE, Keir N, et al. Inhibition of defocus-induced myopia in chickens. Invest Ophthalmol Vis Sci. 2013;54(4):2662–2668. doi:10.1167/iovs.12-10742
27. Griffin RA. Ophthalmic lenses with induced aperture and redundant power regions; multifocal ophthalmic lens with induced aperture. US patent 7,178,918; 6,474,814. 2007 Feb 20.
28. Visioneering Technologies Inc. The naturalvue multifocal power profile. Available from: https://vtivision.com/wp-content/uploads/2020/05/MKTNVMWEQ1r0_NVMF_PowerProfileWeb_FNL.pdf.
29. Visioneering Technologies Inc. Redefine their tomorrow. Available from: https://global.vtivision.com/practitioner/products/multifocal-myopia/.
30. Myopia Profile. How can we set myopia control expectations? Available from: https://www.myopiaprofile.com/how-can-we-set-myopia-control-expectations/.
31. Brennan N, Cheng X, Toubouti Y, Bullimore M. Influence of age and race on axial elongation in myopic children. Optom Vis Sci. 2018;95:180072.
32. Meng W, Butterworth J, Malecaze F, Calvas P. Axial length of myopia: a review of current research. Ophthalmologica. 2011;225(3):127–134. doi:10.1159/000317072
33. Parssinen O, Kauppinen M, Viljanen A. The progression of myopia from its onset at age 8–12 to adulthood and the influence of heredity and external factors on myopic progression. A 23-year follow-up study. Acta Ophthalmol. 2014;92(8):730–739. doi:10.1111/aos.12387
34. Johnson & Johnson Vision. Managing myopia A clinical response to the growing epidemic. Available from: https://s3-us-west-2.amazonaws.com/covalentcreative/jjv/media/documents/Managing_Myopia_Clinical_Guide_Dec_2020.pdf.
35. Polling JR, Tan E, Driessen S, et al. A 3-year follow-up study of atropine treatment for progressive myopia in Europeans. Eye. 2020;34(11):2020–2028. doi:10.1038/s41433-020-1122-7
36. Turnbull PRK, Munro OJ, Phillips JR. Contact lens methods for clinical myopia control. Optom Vis Sci. 2016;93(9):1120–1126. doi:10.1097/OPX.0000000000000957
37. Michaud L. The Montreal Experience: a retrospective study of the management of myopia and axial length progression on 469 subjects. Invest Ophthalmol Vis Sci. 2019;60(9):5817.
38. Michaud L, Simard P, Marcotte-Collard R, Ouzzani M, Sinnott LT. The Montreal experience: a retrospective study part I—basic principles and treatment algorithm. Appl Sci. 2021;11(16):7455. doi:10.3390/app11167455
39. Aller T, Achenbach P, Cooper J, et al. Myopia management with naturalvue (etafilcon a) multifocal 1 day contact lenses: continuing evidence from clinical practice. Cont Lens Anterior Eye. 2019;42(6):e24. doi:10.1016/j.clae.2019.10.079
40. Chamberlain P, Lazon de la Jara P, Arumugam B, Bullimore MA. Axial length targets for myopia control. Ophthalmic Physiol Opt. 2021;41(3):523–531. doi:10.1111/opo.12812
41. Lam CS, Tang WC, Lee PH, et al. Myopia control effect of defocus incorporated multiple segments (DIMS) spectacle lens in Chinese children: results of a 3-year follow-up study. Br J Ophthalmol. 2021. doi:10.1136/bjophthalmol-2020-317664
42. Brennan NA, Toubouti YM, Cheng X, Bullimore MA. Efficacy in myopia control. Prog Retin Eye Res. 2021;83:100923. doi:10.1016/j.preteyeres.2020.100923
43. Hyman L, Gwiazda J, Hussein M, et al. Relationship of age, sex, and ethnicity with myopia progression and axial elongation in the correction of myopia evaluation trial. Arch Ophthalmol. 2005;123(7):977–987. doi:10.1001/archopht.123.7.977
44. Donovan L, Sankaridurg P, Ho A, Naduvilath T, Smith EL, Holden BA. Myopia progression rates in urban children wearing single-vision spectacles. Optom Vis Sci. 2012;89(1):27–32. doi:10.1097/OPX.0b013e3182357f79
45. Coviltir V, Burcel M, Cherecheanu AP, et al. Update on myopia risk factors and microenvironmental changes. J Ophthalmol. 2019;2019:4960852. doi:10.1155/2019/4960852
46. Harb EN, Wildsoet CF. Nutritional factors and myopia: an analysis of National Health and Nutrition Examination survey data. Optom Vis Sci. 2021;98(5):458–468. doi:10.1097/OPX.0000000000001694
47. US Food & Drug Administration. Use of real-world evidence to support regulatory decision-making for medical devices guidance for industry and food and drug administration staff; August 31, 2017. Available from: https://www.fda.gov/media/99447/download.
48. CooperVision. Biofinity multifocal lens fitting guidelines. Available from: https://coopervision.com/sites/coopervision.com/files/practitioner-fitting-guides/1131_biofinity_mf_fitting_guide_4.15_mech.pdf.
49. Zadnik K, Mutti DO, Mitchell GL, Jones LA, Burr D, Moeschberger ML. Normal eye growth in emmetropic schoolchildren. Optom Vis Sci. 2004;81(11):819–828. doi:10.1097/01.OPX.0000145028.53923.67
50. Brennan NA. Why “CARE” for myopia? Review of myopia management; October 1, 2020.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.