Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Reduction in apathy following epilepsy surgery
Authors Mah L, Swearer J, Phillips CA, Benjamin S ![]()
Received 31 January 2019
Accepted for publication 28 May 2019
Published 28 June 2019 Volume 2019:15 Pages 1679—1684
DOI https://doi.org/10.2147/NDT.S189603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Linda Mah,1–3 Joan Swearer,4 Catherine A Phillips,4 Sheldon Benjamin5
1Rotman Research Institute, Baycrest, Toronto, Canada; 2Department of Psychiatry, Baycrest Health Sciences, Toronto, Canada; 3Department of Psychiatry, Division of Geriatric Psychiatry, University of Toronto, Toronto, Canada; 4Department of Neurology, University of Massachusetts Medical School, Worcester, MA, USA; 5Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA, USA
Introduction: Surgical treatment for patients with epilepsy who do not respond to antiepileptic medication can lead to changes in behavior, including new onset of neuropsychiatric symptoms such as depression and anxiety. In other cases, neuropsychiatric symptoms present before surgery may be alleviated. Because application of diagnostic criteria for primary psychiatric disorders may not be valid in assessing behavior in epilepsy populations, we sought to determine the feasibility of measuring behaviors associated with frontal-subcortical dysfunction using the Frontal Systems Behavior Scale (FrSBe) in patients who had received surgical intervention for medically refractory epilepsy.
Materials and methods: Twenty-three patients who had previously undergone epilepsy surgery and their family member informants completed the FrSBe. The FrSBe includes separate forms for patients and informants to rate symptoms associated with three frontal lobe syndromes – executive dysfunction, disinhibition, and apathy – prior to and following a neurological condition. Patients and informants were asked to rate frontal lobe behaviors before and after epilepsy surgery using the FrSBe.
Results: Informants rated patients as showing a significantly greater reduction in apathy on the FrSBe compared to either disinhibition or executive dysfunction subscales. A trend in reduction of apathy following right hemisphere resection was found.
Conclusions: Patients who have undergone epilepsy surgery show a reduction in apathy but it is unclear whether this behavioral change is directly related to the surgical intervention. We suggest that these preliminary findings support the utility of implementing dimensional scales such as the FrSBe to study behavioral changes following epilepsy surgery.
Keywords: epilepsy surgery, apathy, frontal lobe, disinhibition, motivation, temporal lobe epilepsy
Plain language summary
Surgical treatment for patients with epilepsy who do not respond to antiepileptic medication leads to seizure freedom for the majority of cases, but can lead to changes in behavior, including new onset of neuropsychiatric symptoms such as depression or anxiety or reduction of neuropsychiatric symptoms that were present before epilepsy surgery. Because clinical criteria for primary psychiatric illnesses may not be valid in epilepsy populations, we assessed the feasibility of measuring behaviors associated with frontal-subcortical dysfunction using the Frontal Systems Behavior Scale (FrSBe) in patients who had received surgical intervention for medically-refractory epilepsy. The FrSBe includes separate forms for patients and for caregiver informants to rate symptoms associated with three frontal lobe syndromes: executive dysfunction, disinhibition, and apathy both prior to, and following, a neurological condition. For this study, we asked patients and caregivers to rate frontal lobe behaviors before and after epilepsy surgery using the FrSBe. Our results showed that informants rated greater reduction in apathy on the FrSBe compared to either disinhibition or executive dysfunction. Although we are unable to conclude that the reduction in apathy is directly related to the surgical intervention, these preliminary findings support the utility of using dimensional scales such as the FrSBe to assess behavioral changes following epilepsy surgery in future studies.
Introduction
Surgical resection for medically intractable epilepsy achieves seizure freedom in 59–89% of cases,1 but carries a risk of adverse neurocognitive outcomes, such as language and memory deficits,2,3 and neuropsychiatric complications, such as de novo or worsening of mood or anxiety symptoms following surgery.4 However, other observational studies report improvement in neuropsychiatric symptoms based on self or clinician-rated scales, even while rates of psychiatric diagnoses remain unchanged. In the few controlled studies available, patients with epilepsy who underwent surgical resection did not show increased rates of neuropsychiatric symptoms5 and may have improved overall mental health based on quality of life measures, when compared to medically treated epilepsy patients.6
In addition to neuropsychiatric symptoms such as depression and psychosis, behavioral changes associated with frontal-subcortical damage have been reported following temporal lobe resection for seizures. Hill et al7 from the Maudsley Hospital in London reported that patients with a “history of aggressiveness” prior to surgery showed a reduction in aggression following temporal lobe resection for seizures, while other patients were noted to show increased sexual drive and social behavior, an outcome that appears more frequently for right-sided seizure foci.8 Given that epilepsy surgery may lead to behavioral changes that cannot be ascribed to a psychiatric condition, we sought to assess the feasibility of measuring changes in behaviors associated with frontal-subcortical dysfunction in patients who had previously undergone surgical treatment for epilepsy.
Frontal-subcortical dysfunction may occur due to structural or functional changes within prefrontal-subcortical circuits in neurological illness, but are also implicated in primary psychiatric conditions such as depression, mania, and psychosis.9 Three distinct frontal lobe neurobehavioral syndromes corresponding to a region of origin of one of the three prefrontal-subcortical circuits have been described.10 The dorsolateral prefrontal syndrome is characterized by executive function deficits and motor programming impairment. These executive function deficits include difficulty in persisting with or changing behavior (i.e., maintaining and shifting set) when required by the situation, reduced verbal and design fluency, and poor planning abilities. Motor programming abnormalities are found during alternating and reciprocal motor tasks. The orbitofrontal syndrome features prominent changes in personality which typically include disinhibition, labile or irritable mood, and socially inappropriate behavior. Patients with the orbitofrontal syndrome are also described as being “stimulus-bound” and respond to environmental cues through automatic imitation of other individuals’ gestures or use of objects in the immediate environment. The anterior cingulate syndrome is typified by marked apathy with a reduction in initiation of speech and behavior and limited displays of emotion.
To measure behavioural changes associated with these frontal lobe syndromes, we implemented the Frontal Systems Behavior Scale (FrSBe) (formally called the Frontal Lobe Personality Scale) which was developed to assess frontal lobe behaviors.11 The FrSBe includes a self-rated (patient) form and an informant (e.g., a family member) form to rate key symptoms associated with the three frontal lobe neurobehavioural syndromes – executive dysfunction, disinhibition, and apathy – both prior to and following a neurological condition. The goal of the current pilot study was to evaluate the feasibility of the FrSBe to measure changes in behavior following epilepsy surgery. We asked patients who had previously undergone surgical treatment for epilepsy and a family member informant to retrospectively rate frontal lobe behaviors before and after epilepsy surgery using the FrSBe. Based on clinical reports of increased sexual drive and social behavior,7,8 we predicted that apathy would decrease and disinhibition would increase following surgery. These effects were predicted to be greater in patients with right-sided resections since disinhibition and manic-like behavior are more frequently reported after right hemisphere damage.12
Materials and methods
Participants
The study was approved by the Institutional Review Board at University of Massachusetts Medical School, Worcester, MA, USA. A description of the study and FrSBe forms were sent to patients who had undergone surgical resection for intractable epilepsy over a 7-year period. Completion and return of the questionnaire was considered informed consent. In patients with temporal lobe epilepsy, amygdalohippocampectomy was performed. Questionnaires were returned for 27 out of 45 patients. Demographic and clinical variables are summarized in Table 1.
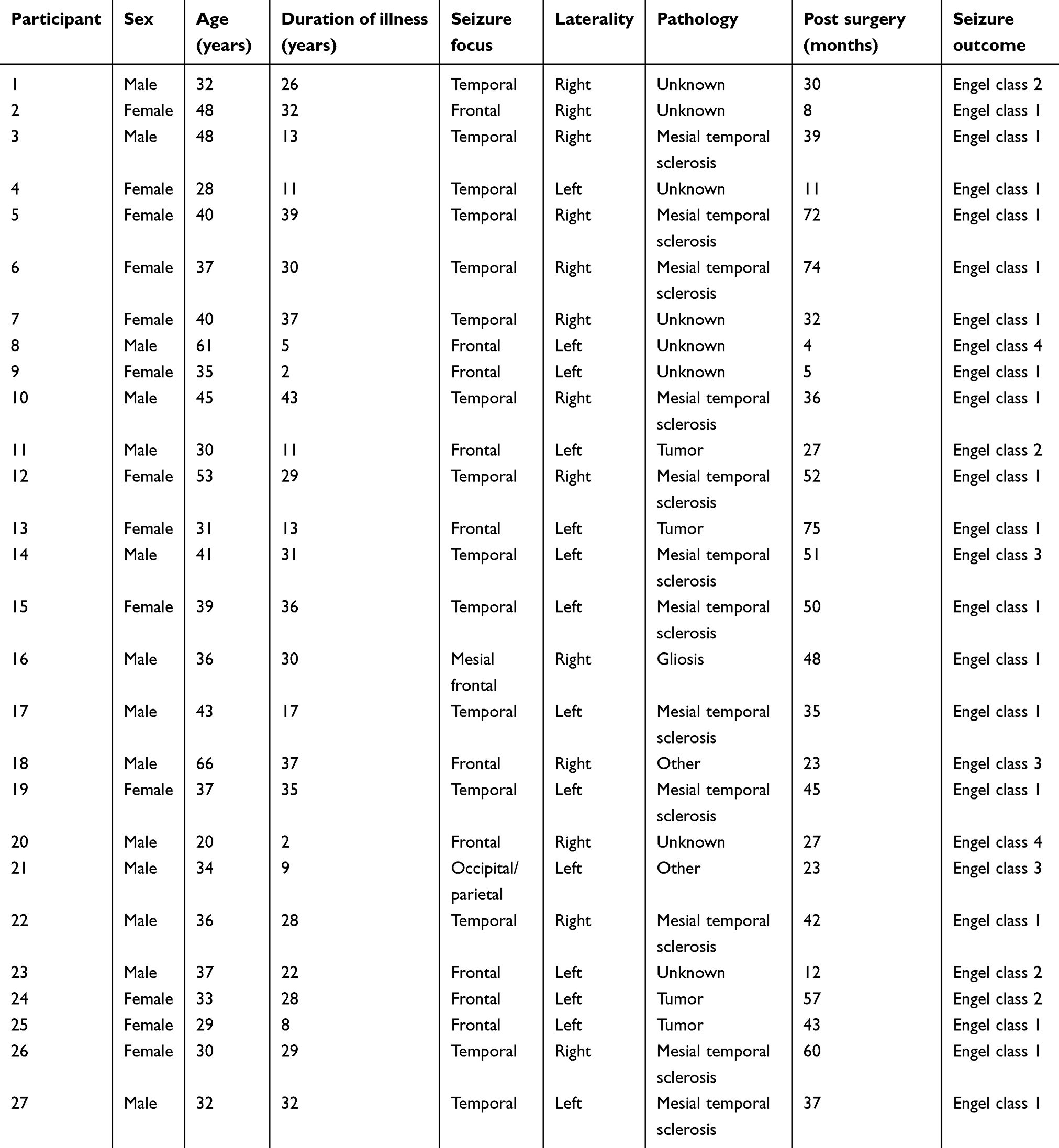 | Table 1 Demographic and clinical characteristics of participants with medically intractable epilepsy disorder |
Frontal Systems Behavior Scale
The FrSBe is a 46-item questionnaire that assesses behaviors associated with frontal-subcortical damage, including apathy, disinhibition, and executive dysfunction. Behaviors are rated on a 1–5 Likert-type scale at two time points: “before the illness or injury” (Before) and “at the present time” (Current). Three subscale scores on the FrSBe are calculated (Apathy, Disinhibition, and Executive Dysfunction), with higher scores on each subscale indicating greater dysfunction. The FrSBe includes a self-rated version and an informant-rated version. Both versions were mailed to patients. Of the 27 patients included in the current study, 23 informant-rated FrSBe forms were returned.
Statistical analyses
Change in frontal behaviors
To evaluate observed changes in frontal behaviors, the informant-rated Executive Dysfunction, Disinhibition, and Apathy subscale scores were analyzed using a mixed ANOVA (between-group factors=frontal domain, laterality of resection; within-group factor=time). Laterality was included in the analyses based on reports of disinhibition following right-sided resections. Planned comparisons of change in apathy and change in disinhibition according to laterality for informant ratings of disinhibition and apathy were performed using the Mann–Whitney U-test due to small sample sizes.
Rater effects
To assess effects of the rater, we computed the % change score relative to baseline ((current–before)/before×100%) for each of the subscales (∆Apathy, ∆Disinhibition, and ∆Executive Dysfunction) and used a mixed ANOVA (between-group factors=frontal domain, laterality of resection; within-group factor=rater).
Results
Change in frontal behaviors
Mixed ANOVA (between-group factors=frontal domain, laterality of resection; within-group factor=time) showed a significant domain×time interaction (F(1, 42)=3.48, p=0.040). Paired t-tests showed that improvement in apathy was greater than change in either executive function or level of disinhibition (t(22)=2.19, p=0.04; t(22)=2.14, p=0.044), respectively (Figure 1). There were no main or interaction effects of laterality in the ANOVA.
 | Figure 1 Changes in frontal lobe symptoms (executive function, disinhibition, and apathy) following surgical resection for medically refractory epilepsy as rated by informants. Higher scores on the Frontal Systems Behavior Scale indicate greater dysfunction. Apathy was judged to decrease after epilepsy surgery. This change was greater than that found for disinhibition or executive dysfunction. |
Although not statistically significant, planned comparisons by laterality showed greater improvement in apathy in patients with right-sided resection (p=0.088, one-sided).
Rater effects
Mixed ANOVA (between-group factors=frontal domain, laterality of resection; within-group factor=rater) showed a rater×laterality effect (F(1, 20)=4.87, p=0.039). A domain×rater interaction fell short of statistical significance (F(1. 40)=2.74, p=0.077). The rater×laterality interaction was explained by greater discrepancy between self-ratings and informant ratings for patients with left-sided resections (p=0.029) compared to those with right-sided resections. Greater discrepancy in self-ratings versus informant ratings on the apathy subscale fell short of statistical significance (p=0.069).
Conclusions
The current study investigated the utility of assessing changes in behavior using the FrSBe retrospectively in a cohort of patients who had received surgical intervention for intractable seizure disorder. The main finding was that family member informants, but not patients themselves, rated apathy as reduced in patients who had undergone epilepsy surgery, while disinhibition and executive function were unchanged. We also found a nonsignificant trend for greater reduction in apathy in patients with right-sided resection. Contradictory to the hypotheses, no change in disinhibition was observed following epilepsy surgery.
These findings suggest that the FrSBe may have adequate sensitivity to measure changes in apathy following epilepsy surgery. Our findings of reduction in apathy are compatible with early descriptions of behavioral changes following anteromedial temporal section for seizures, which included increased sexual drive and enhanced social behavior.7,8 While not statistically significant, the pattern of greater reduction in apathy in patients with seizure foci in the right hemisphere is consistent with increases in goal-directed behavior more frequently reported following right temporal resection and right hemisphere damage.8,12
It is tempting to conclude that surgical intervention for epilepsy resulted in a reduction in apathy in our cohort; however, multiple factors likely contributed to the finding of decreased apathy following epilepsy surgery. For example, a reduced frequency of seizures and lower dosages or discontinuation of seizure medications may have improved the overall level of alertness and resulted in a reduction of apathy. It is also possible that mood improvement following surgery contributed to lowering of apathy since low motivation is a component of major depressive disorder. Further, because this study was conducted retrospectively with patients and informants completing the FrSBe an average of 35 months after the surgery date, their responses may not accurately capture the clinical presentation of patients pre and post surgery. Lastly, we are unable to conclude that surgical resection led to a reduction in apathy because our sample included patients with both temporal and extra-temporal (frontal) seizure foci. Due to the small sample size, it was not possible to perform any meaningful analyses to compare behavioral changes following temporal versus frontal resection.
Exploratory analyses showed that self-ratings and informant ratings were less in agreement in patients who had resection of the left hemisphere compared to those with right-sided surgery. However, the significance of this is unclear, given the small sample size and previous observations of impaired awareness of illness or anosognosia as a consequence of left hemisphere dominance due to right hemisphere dysfunction.13
We emphasize that the study design and other methodological considerations do not allow us to conclude that a reduction in apathy is the direct result of surgical intervention for epilepsy. Nevertheless, our finding of change in apathy supports the utility of using a dimensional scale such as the FrSBe to prospectively assess neuropsychiatric outcomes following epilepsy surgery. Reduction in apathy in patients who have undergone epilepsy surgery has not have been previously reported, although improved mental health has been observed in patients randomized to epilepsy surgery as opposed to medical treatment.6 Prospective studies using dimensional scales to assess behavior will increase our knowledge of the impact of surgical treatment for refractory epilepsy on neuropsychiatric outcomes, in addition to achieving seizure freedom. This knowledge will allow patients and their families to make more informed decisions regarding surgical intervention for intractable seizure disorder.
Acknowledgments
We thank the patients and their family members for participating in our research.
Disclosure
Sheldon Benjamin is a partner in and one of the authors for Brain Educators LLC, publisher of a neuropsychiatry pocket card, “The Brain Card®”. The authors report no other conflicts of interest in this work.
References
1. Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal-lobe epilepsy. N Engl J Med. 2001;345:311–318. doi:10.1056/NEJM200108023450501
2. Helmstaedter C, Elger CE. Cognitive consequences of two-thirds anterior temporal lobectomy on verbal memory in 144 patients: a three-month follow-up study. Epilepsia. 1996;37:171–180.
3. Ives-Deliperi VL, Butler JT. Naming outcomes of anterior temporal lobectomy in epilepsy patients: a systematic review of the literature. Epilepsy Behav. 2012;24:194–198. doi:10.1016/j.yebeh.2012.04.115
4. Foong J, Flugel D. Psychiatric outcome of surgery for temporal lobe epilepsy and presurgical considerations. Epilepsy Res. 2007;75:84–96. doi:10.1016/j.eplepsyres.2007.05.005
5. Ramos-Perdigués S, Baillés E, Mané A, et al. A prospective study contrasting the psychiatric outcome in drug-resistant epilepsy between patients who underwent surgery and a control group. Epilepsia. 2016;57:1680–1690. doi:10.1111/epi.13497
6. Fiest KM, Sajobi TT, Wiebe S. Epilepsy surgery and meaningful improvements in quality of life: results from a randomized controlled trial. Epilepsia. 2014;55:886–892. doi:10.1111/epi.12625
7. Hill D, Pond DA, Mitchell W, Falconer MA. Personality changes following temporal lobectomy for epilepsy. 1957. Epilepsy Behav. 2004;5:603–610. doi:10.1016/j.yebeh.2004.05.002
8. Baird AD, Wilson SJ, Bladin PF, Saling MM, Reutens DC. Sexual outcome after epilepsy surgery. Epilepsy Behav. 2003;4:268–278. doi:10.1016/S1525-5050(03)00085-4
9. Cummings JL. Anatomic and behavioral aspects of frontal-subcortical circuits. Ann N Y Acad Sci. 1995;769:1–13.
10. Cummings JL. Frontal-subcortical circuits and human behavior. Arch Neurol. 1993;50:873–880. doi:10.1001/archneur.1993.00540080076020
11. Carvalho JO, Buelow MT, Ready RE, Grace J. Associations between original and a reduced Frontal Systems Behavior Scale (FrSBe), cognition, and activities of daily living in a large neurologic sample. Appl Neuropsychol Adult. 2016;23:125–132. doi:10.1080/23279095.2015.1012759
12. Starkstein SE, Berthier ML, Lylyk PL, Casasco A, Robinson RG, Leiguarda R. Emotional behavior after a Wada test in a patient with secondary mania. J Neuropsychiatry Clin Neurosci. 1989;1:408–412. doi:10.1176/jnp.1.4.408
13. Ramachandran VS. Anosognosia in parietal lobe syndrome. Conscious Cogn. 1995;4:22–51. doi:10.1006/ccog.1995.1002
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.