Back to Journals » International Journal of Women's Health » Volume 8
Reducing rural maternal mortality and the equity gap in northern Nigeria: the public health evidence for the Community Communication Emergency Referral strategy
Received 20 August 2015
Accepted for publication 12 January 2016
Published 16 March 2016 Volume 2016:8 Pages 77—92
DOI https://doi.org/10.2147/IJWH.S94823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
Susan B Aradeon,1 Henry V Doctor2
1Freelance International Consultant (Social and Behavioral Change Communication), Aventura, FL, USA; 2Department of Information, Evidence and Research, Regional Office for the Eastern Mediterranean, World Health Organization, Nasr City, Cairo, Egypt
Abstract: The Sustainable Development Goal (SDG) maternal mortality target risks being underachieved like its Millennium Development Goal (MDG) predecessor. The MDG skilled birth attendant (SBA) strategy proved inadequate to end preventable maternal deaths for the millions of rural women living in resource-constrained settings. This equity gap has been successfully addressed by integrating a community-based emergency obstetric care strategy into the intrapartum care SBA delivery strategy in a large scale, northern Nigerian health systems strengthening project. The Community Communication Emergency Referral (CCER) strategy catalyzes community capacity for timely evacuations to emergency obstetric care facilities instead of promoting SBA deliveries in environments where SBA availability and accessibility will remain inadequate for the near and medium term. Community Communication is an innovative, efficient, equitable, and culturally appropriate community mobilization approach that empowers low- and nonliterate community members to become the communicators. For the CCER strategy, this community mobilization approach was used to establish and maintain emergency maternal care support structures. Public health evidence demonstrates the success of integrating the CCER strategy into the SBA strategy and the practicability of this combined strategy at scale. In intervention sites, the maternal mortality ratio reduced by 16.8% from extremely high levels within 4 years. Significantly, the CCER strategy contributed to saving one-third of the lives saved in the project sites, thereby maximizing the effectiveness of the SBAs and upgraded emergency obstetric care facilities. Pre- and postimplementation Knowledge, Attitude, and Practice Survey results and qualitative assessments support the CCER theory of change. This theory of change rests on a set of implementation steps that rely on three innovative components: Community Communication, Rapid Imitation Practice, and CCER support structures. Innovative communication body tools and the rote learning Rapid Imitation Practice training methodology enabled low-literate volunteers to saturate their communities with informed group discussions transferring communication capacity and ownership to the discussion participants. CCER is especially efficient because virtually every timely, community referral for emergency maternal care results in a saved life, whereas on average, only one in every eight births delivered by an SBA (12%) is expected to be a delivery-associated complication requiring lifesaving care.
Keywords: Community Communication, rural maternal mortality equity gap, public health evidence, theory of change, three-delay model, emergency referral, delivery-associated complication, Nigeria
Introduction
Background
By increasing focus on the rural and impoverished women, safe motherhood programs addressing the Sustainable Development Goal (SDG) 3.1 can reduce the major equity gap that led to the significant underachievement of the Millennium Development Goal (MDG) 5 target with its skilled birth attendant (SBA) delivery indicator. This safe motherhood challenge mainly lies in countries with massive deprivation and large rural populations.1 According to conservative estimates, between 130 and 180 million women gave birth without the benefit of SBAs in South Asia and sub-Saharan Africa from 2011 to 2015 with 90% of these births occurring in the rural areas.2 These estimates imply that in the short and medium term, the vast majority of maternal lives cannot be saved by the SBA strategy alone. Moreover, this overmedicalized strategy requiring every woman to give birth in a facility fails to take into consideration the financial, transport, and cultural barriers to facility delivery that compound the barriers posed by the inadequate numbers and maldistribution of SBAs. Although intrapartum facility-based care is the appropriate long-term strategy, this one-size-fits-all strategy is not achievable with current resources and infrastructure. Consequently, alternative context-specific service- and community-based strategies need to be designed and validated.3
Against this background, our objective is to promote integration of the Community Communication for Emergency Referral (CCER) strategy into the SBA delivery strategy as an innovative community mobilization strategy that ensures timely access to emergency obstetric services in order to reduce maternal mortality and the safe motherhood equity gap that continues to be faced by rural women in resource-constrained environments. This community mobilization strategy empowers low- and nonliterate community leaders, volunteers, and informed discussion participants to become the communicators and to establish the maternal support systems required for timely emergency evacuation and healthier home deliveries to save the lives of thousands of rural women.
Methodology
We provide a case study of the integration of CCER into the safe motherhood component of a health systems strengthening project and show how CCER meets the criteria for Evidence-Based Public Health (EBPH).4 The Partnership for Reviving Routine Immunization in Northern Nigeria, Maternal Newborn and Child Health (PRRINN-MNCH), funded by the Department for International Development (UK aid) and the Government of Norway implemented CCER “at scale” in an extremely challenging rural environment in northern Nigeria over 4 years between 2009 and 2013. We justify the need for integration of this rural maternal emergency referral strategy into the PRRINN-MNCH SBA strategy and provide project household survey data and reports that demonstrate the effectiveness of the combined strategy. We rely on analysis from project sisterhood method data that demonstrates that PRRINN-MNCH reduced the maternal mortality ratio (MMR) by 16.8% in the intervention clusters. A value for money report underscores the effectiveness of CCER. Furthermore, the informal diffusion and tripling of communities taking responsibility for evacuating women in danger indicates the potential for CCER sustainability. Using documented information, we compare the estimated lifesaving effects of delivery-associated complications and timely emergency evacuations. We calculate that CCER contributed to one-third of the maternal lives saved in the intervention clusters. We then describe the CCER theory of change that underpins these successes. Finally, we substantiate the “posited causal pathway” with additional evidence from Knowledge Attitude and Practice (KAP) surveys and qualitative studies.
The equity gap for women in northern Nigeria
Northern Nigeria has one of the highest MMRs in the world – estimated at 1,271 deaths per 100,000 live births based on a 2011 project household survey in four states.5 The difficult terrain, widespread poverty, and the extremely harsh social environment for women compound health system issues that deprive most women, and especially rural women, from lifesaving safe motherhood services. Almost two-thirds of people living in the north east and north west zones of Nigeria fall within the two lowest wealth quintiles.6
The low social status of the majority of Hausa women in northern Nigeria affects their reproductive health and contributes to some of the highest levels of maternal mortality worldwide.7 Cultural norms and beliefs result in minimal autonomy for women, who accord total obedience to the male head of the compound, accept strict purdah (confinement to the residential compound), polygamy, and very early arranged marriages.8 A virtuous wife is secluded within the residential compound, requiring the husband’s permission to go outside and possesses “kunya”, which translates roughly as modesty, shame, or deference.7 The high value placed on “kunya” inhibits women from calling for timely assistance if a maternal complication arises7 and influenced over one-quarter (27.8%) of women to deliver alone in the 5 years prior to 2013 and to reject maternal services provided by a male health worker.6,9 The low levels of literacy among women (26.0%) and among men (62.2%) compound the negative effects of their normative dependency on their husbands (83.8%) for health-care expenditures and decisions.6
The Nigeria 2013 Demographic and Health Survey (DHS) also reports on the current social factors directly affecting the reproductive health status of Hausa women.6 It is important to note that these data are for the north west, which covers a geographic area populated by the Hausa/Fulani with a small percentage of migrants largely located in urban areas. The majority of women (87.5%) delivered at home. Further, cultural reasons for not delivering in a facility (husband/family did not allow, not necessary, not customary) ranged from more than one-third to more than two-thirds of the respondents depending upon the state in which they live. Husband’s refusal to permit facility delivery was cited as a reason by 23.7% of women in Zamfara State.6 In addition, the cultural norm of early marriage and childbirth at a young age continues to place Hausa girls at high risk for maternal mortality and morbidity. The median age at first marriage is 15.3 years and at first birth is 17.9 years. Slightly more than one-third (36%) of teenage women (15–19 years) were already mothers or currently pregnant.6 Since growth of pelvic dimensions occurs after growth height is largely completed,10 a significant percentage of girls are at risk for pelvic obstruction and, if untreated, are at risk for obstetric fistulas owing to their very young age at delivery.7 Furthermore, the high ideal number of children (8.4= mean) and low current family planning use (3.6%) contribute to very high total fertility rates (TFRs, ranging from 6.5 to 8.4) indicating that more women are at potential risk for maternal mortality than would be the case with lowered TFRs.6
High hospital MMRs have been attributed to community delays that compound any hospital-based delays. These delays include delayed decision to seek medical care while seeking more familiar and financially feasible local remedies and/or awaiting the return home of the husband along with delayed arrival at the facility, partially owing to overcoming transportation challenges (availability, cost, and difficult terrain).11
Traditional beliefs result in medical care-seeking delays. The first care for a maternal complication is often sought from a traditional birth attendant or a traditional healer. For instance, “pregnant women affected by eclamptic fits or seizures are believed to be possessed by evil spirits”.12,13 As such, only the traditional healers possess the remedy. Some danger signs are considered normal or even beneficial, therefore requiring no treatment. Such is the case with malpresentation where the cultural belief is that the baby will be born brave and strong (Saudatu Zahradeen, email communication, May 5, 2015). Moreover, previous bad experiences with hospital care for the high percentage of cases arriving too late undermines effective care-seeking behaviors. In a North Nigerian study, Adamu et al13 stated that “in many cases, such referrals [to a higher level of care from poorly staffed health facilities] are perceived by patients and their relatives as acts devoid of compassion or acts that simply delay the inevitable death of the mother”.
Low service uptake for antenatal care (ANC) and facility delivery also reflects the widespread perception that pregnancy and delivery are normal life events that require no special preventive measures or care. No perceived need is felt for ANC, extra rest, extra protein or anemia prevention, or SBA delivery.9 Moreover, ANC users are discouraged from planning on facility delivery, because many facilities cannot guarantee 24-hour services by a female SBA.14,15 In addition, almost half of the project household survey respondents reported concerns about the negative attitudes of the health workers, and the health workers themselves confirmed that since they were overworked, their ability to provide quality care was seriously undermined.9
The need for a combined SBA and Community Communication Emergency Referral strategy
Implementing the SBA strategy in northern Nigeria
PRRINN-MNCH, a health system strengthening project in northern Nigeria, achieved substantial reductions in the MMR by increasing availability of 24/7 SBAs in upgraded facilities and by integrating the rural maternal Community Communication Emergency Referral (CCER) intervention into the health system.
PRRINN-MNCH implemented a strong SBA training and facility-upgrading project that significantly increased the availability of SBAs utilizing the UNICEF/WHO/UNFPA cluster approach.16 Following the UNICEF/WHO/UNFPA recommendations, PRRINN-MNCH supported establishment of safe motherhood service clusters composed of one Comprehensive and four Basic Emergency Obstetric Care (C/BEmOC) facilities for populations of 500,000. PRRINN-MNCH added on eight primary health-care facilities (PHCs) per BEmOC. At the baseline, there were only two fully functioning CEmOCs and two BEmOCs. Before the end of the program, half of the 9.5 million people living in the three supported states (Katsina, Yobe, and Zamfara) lived in upgraded clusters: 19 EmOC facilities had four Life Saving Skills (LSS)-trained health workers while another 67 BEmOCs and PHCs had two LSS-trained health workers. Moreover, equipment and infrastructure improvements had been provided for two-thirds of these facilities with plans for the remaining one-third before the project closure. Significant gains were made in the number of midwives serving in public facilities (from 12 to 334), including midwives recruited from other parts of Nigeria under the Federal Government Midwife Scheme. In the immediate catchment area of facilities providing SBA services, Rapid Awareness Raising health promotion sessions were facilitated by health workers and trained lay persons using the Community Communication participatory methods. This urban health promotion work contributed to increased ANC attendance and SBA deliveries in the intervention clusters. Rates of ANC provided by SBAs doubled from 24.5% to 51.2%,17 indicating that up to one-quarter of the women were experiencing the benefits of maternal health services for the first time. Moreover, SBA deliveries in project clusters more than doubled from 11.3% to 26.8% between the 2009 baseline and the 2013 end line surveys.17
SBA services remain inaccessible to rural women
Despite these enormous project-driven gains in SBA service provision and uptake, the majority of rural dwellers still lacked access to midwives; only 49 PHCs had at least 1 midwife17 for the 9.5 million people residing in the 19 project clusters. In the PRRINN-MNCH-supported states, each cluster usually comprised 2–3 districts, depending on the population size.17 The scarcity of female health workers capable of providing SBA services can be reduced with continued donor projects and government efforts. Nevertheless, SBA services will remain inaccessible for the majority of rural women because of the practical impossibility of staffing even half of the PHCs with 24/7 SBA services. Cultural constraints have kept the number of local, female candidates eligible for LSS training at very low levels and have inhibited those trained from taking up or remaining in their rural postings.17 Too few girls attend schools and too few fathers permit their unmarried daughters to reside at an urban training institution. Most girls are married by the time they have completed their professional training. Young female professionals, even those with lower level training, marry successful men whose livelihood is based in the urban areas. As wives, they are expected to remain in the husband’s home with their children, who will necessarily attend one of the better urban schools. To accept a rural posting is to risk threatening a woman’s marriage or place within her family.16
Evidence of the effectiveness of the PRRINN-MNCH combined SBA with CCER strategy
A 16.8% MMR reduction achieved in PRRINN-MNCH intervention districts
Within 4 years, PRRINN-MNCH reduced the MMR as assessed by the sisterhood method from more than 1,271 to 1,190 deaths per 100,000 live births (Table 1). The MMR in the intervention districts declined significantly to 1,057, representing a 16.8% reduction (ie, 1,271–1,057=214; 214/1,271=16.8%), whereas the MMR in the control districts remained virtually the same even though they benefitted from almost the same percentage of SBA births (23.6% for the control districts and 26.8% for the intervention districts). In addition, the tripling of basic decision-making knowledge essential for arranging EmOC referrals (knowledge of four maternal danger signs) to almost 30% (29.4%) within the intervention communities from 10.2% reflects the critical increases CCER has brought about in the community capacity to save maternal lives. Moreover, it is likely that the actual levels of change in the MMR are greater than this estimate because the sisterhood method uses a historical reference period that is likely to go back more than 5 years.
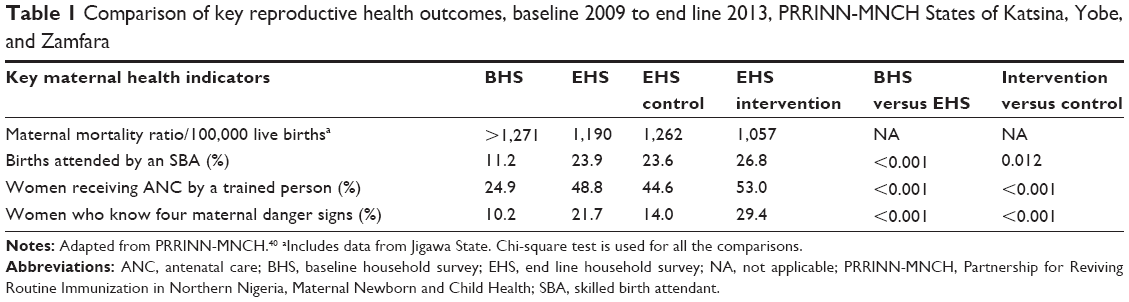 | Table 1 Comparison of key reproductive health outcomes, baseline 2009 to end line 2013, PRRINN-MNCH States of Katsina, Yobe, and Zamfara |
Good value for money with the CCER strategy
The CCER approach also appears to represent very good value for money (VfM). According to a 2012 VfM assessment using data collected for the first 2 years of rollout,18 the CCER mobilization approach was considered both efficient and effective and started generating cost–benefit data that demonstrated to the government that it was affordable. The cost–benefit data were useful in influencing policy and debates about VfM benchmarks.18 The VfM estimated additional cost of rolling out CCER was N85,037 (£340; US$529) per community based on the cost of the Community Communication (N66,730; £265; US$412) and the National Union of Road Transport Workers transport interventions (N18,291; £73 or US$114).18 In 2012 currency, the cost per life saved ranged from 10 to 18 UK pounds (about US$16–US$28) depending upon the cost-effectiveness of the implementation in each state with Katsina State being the most effective and Zamfara, the least (Table 2).
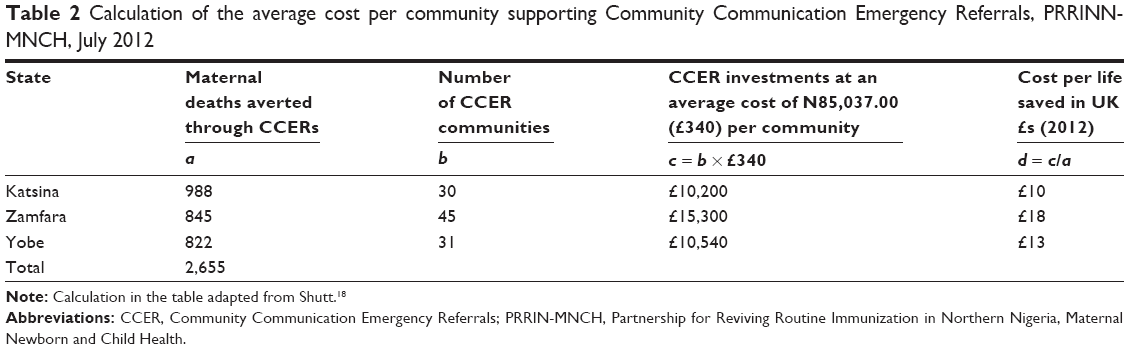 | Table 2 Calculation of the average cost per community supporting Community Communication Emergency Referrals, PRRINN-MNCH, July 2012 |
This CCER VfM extends beyond the cost per life saved. CCER communities maximize the utility of strengthened EmOCs and their SBAs. The C/BEmOCs are planned to provide safe motherhood services to large catchment areas covering populations of between 125,000 and 500,000 which necessarily include many rural communities. As discussed in the next section, every timely rural community referral gives the SBAs the opportunity to avert a maternal death whereas many of the facility deliveries are free of complications. CCER also catalyzes the formation of informed citizens and social capital within rural communities. As discussed in a later section, volunteers are trained and acquire experience leading peer group discussions that promote ANC and SBA delivery, newborn care and routine immunization. Moreover social capital is built and used to arrange for timely evacuations.
Evidence of the substantial role of CCER in reducing maternal deaths
The integration of the CCER strategy into the SBA strategy
The significant difference between the substantial MMR reduction in PRRINN-MNCH intervention sites and the minimal reduction in the control sites suggests that the innovative CCER strategy played a substantial role in saving women’s lives. Crucially, the intervention sites only reported 3.2% more SBA deliveries than the control sites despite their much greater maternal mortality reduction.
An estimate of the relative contribution of the CCER strategy versus the SBA strategy for reducing maternal deaths can be established, although available data do not provide the exact contribution of CCER to the reduction in the MMR. Clearly, the SBA services are essential for saving maternal lives. Thus both strategies depend upon a health system that supports well-equipped and supplied SBAs at the C/BEmOC levels. The major health system difference is that the CCER strategy only requires ensuring quality EmOC services along with very gradual, well-managed increases in the number and capacity of PHCs providing SBA services, whereas the SBA strategy focuses on supplementing EmOC services with rapid expansion of SBA delivery services to PHCs. Both strategies also depend upon informed citizens who ensure that 1) in the case of CCER, women experiencing an obstetric emergency reach the SBA facility in a timely manner, and 2) in the case of SBA deliveries, women give birth with an SBA and are ready to return after discharge should they experience a maternal danger sign.
Comparing CCER and SBA strategies for reducing maternal deaths
A comparison of the relative magnitude of maternal deaths averted by the CCER strategy and by the SBA strategy provides insight into the significant contribution of the CCER strategy to saving women’s lives. The CCER strategy empowers rural communities to save the lives of all women experiencing complications regardless of when they occur during pregnancy, delivery, or the postpartum period, whereas the SBA strategy saves the lives of the women who experience these life-threatening complications during delivery and the immediate postpartum period. Thus, the SBA strategy falls short of providing a lifesaving strategy for rural women who experience maternal emergencies during pregnancy and during most of the postpartum period. Our comparison defines SBA delivery-associated complications, as those complications that occur during delivery and extend through the first week postpartum, assuming that each woman who had an SBA delivery and then experienced a complication within 1 week returned to the facility for treatment.
The only available PRRINN-MNCH data is the number of SBA deliveries (297,349) reported by the project household survey respondents in the intervention sites.17 We rely on estimates of life-threatening complications and the timing of these complications throughout the maternal period to establish the number of births that result in life-threatening delivery-associated complications.
As a basis for the calculations, we establish the proportion of all births that are estimated to result in life-threatening complications. To this end, we rely on the estimates and the logic of the WHO Monitoring Obstetric Care Handbook. According to the Handbook, “the proportion of major direct obstetric complications throughout pregnancy, delivery and immediately postpartum is estimated to be 15% of expected births”.19 However, the Handbook also notes that the rate of obstetric complications may in fact be higher19 and that 68% of African maternal deaths are due to direct causes, 26.6% are due to indirect causes, and 5.4% are unclassified.19 To simplify our calculations, we made slight adjustments. We assigned the unclassified causes to direct and indirect causes. We calculated 70% for direct causes (versus the official estimate of 68%) and 30% for indirect causes (versus the official estimate of 26.6%).19 These estimations allowed us to estimate the proportion of deliveries that represent the total complications faced by women from both direct causes and indirect causes occurring throughout pregnancy, delivery, and immediately postpartum. To establish that the Total Complications (TC) equal 21% of the Total Births (TB), we rely on two formulae for Direct Causes (DC) provided by the Handbook; DC equal 15% of TB and DC equal 70% of TC (Table 3).
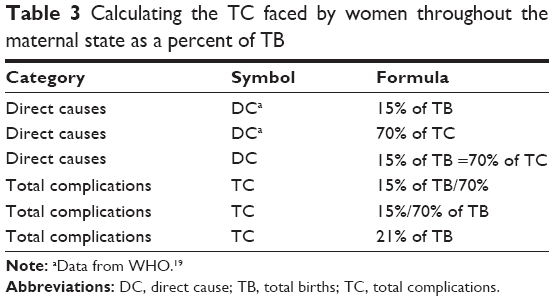 | Table 3 Calculating the TC faced by women throughout the maternal state as a percent of TB |
Next, we establish the estimated percentage of all delivery-associated complications. As indicated earlier, delivery-associated complications refer to those complications occurring while women are under the care of SBAs during delivery and the first week postpartum. We rely on two sets of published estimates. First, WHO experts established that 16% of deaths occur during delivery and that 60% occur during the postpartum period.20 Second, Nour21 further establishes that 66% of postpartum deaths occur within 1 week postpartum. Assuming that each woman who had an SBA delivery and then experienced a complication within 1 week returned to the SBA for treatment, 40% of the postpartum deaths (60%×66% =40%) can be treated by an SBA within the first week postpartum. The percentage of complications expected to occur during delivery (DD =16%) plus the percentage of complications expected to occur during the first week postpartum (CWPP =40%) provides the percentage of SBA delivery-associated preventable complications or deaths (DD + CWPP =56%; Table 4). Notably, the SBA delivery strategy only addresses slightly more than half of the expected complications.
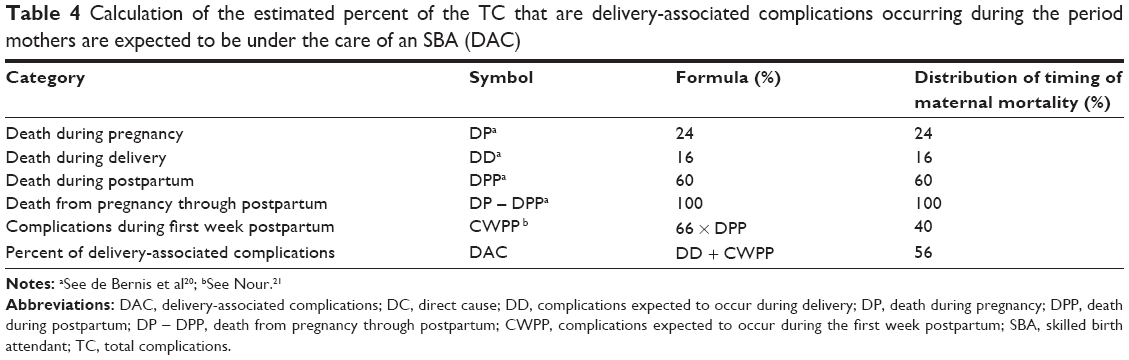 | Table 4 Calculation of the estimated percent of the TC that are delivery-associated complications occurring during the period mothers are expected to be under the care of an SBA (DAC) |
Using the percentages from Tables 3 and 4, we calculated the estimated percent of the total births that are delivery-associated complications along with the expected PRRINN-MNCH delivery-associated complications (Table 5). Thus, 62,443 women representing 21% of the mothers of the total births delivered by the SBAs (297,349) were at risk of life-threatening complications at some time during their pregnancy through the postpartum period (21%×297,349=62,443). Moreover, only 34,968 women representing 56% of the 62,433 women expected to have a life-threatening complication would have actually experienced a complication while under the care of an SBA (56%×62,433=34,968). Finally, we calculate that slightly less than 12% of the women delivered by the SBAs required their expertise to prevent a delivery-associated complication (56% of 21% =11.76%; 11.76% of 297,349=34,968).
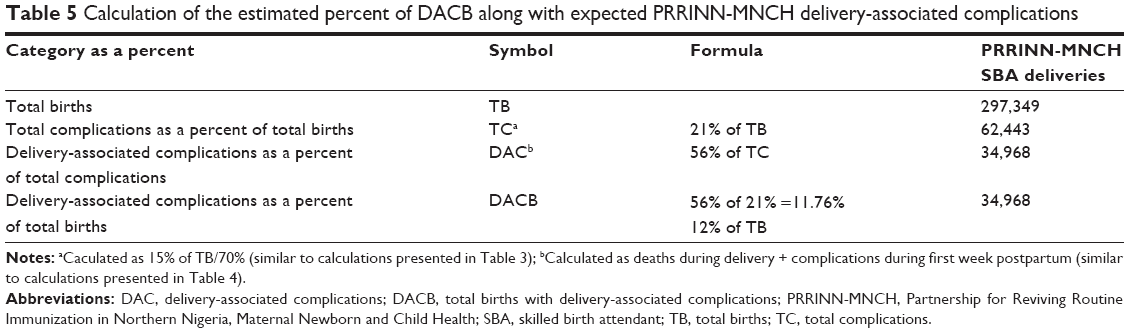 | Table 5 Calculation of the estimated percent of DACB along with expected PRRINN-MNCH delivery-associated complications |
Given the paucity of data, this comparison of the relative magnitude for deaths averted by the CCER and SBA strategies relied on proxies for both strategies. The proxy for the CCER strategy is the number of women transported from communities to the SBA facilities, whereas there is no facility confirmation that each woman was treated for a maternal emergency. PRRINN-MNCH cumulative data from monitoring and evaluation reports show that 17,227 women benefitted from CCER transport (after excluding women transported for normal delivery). The proxy for the SBA strategy is based on the household survey respondents’ reports of the category of person assisting at their most recent delivery and on the series of aforementioned calculations (Tables 3–5) that establish that an estimated 12% of births have a life-threatening complication during the SBA delivery-associated period. Based on these proxies, the CCER strategy contributed an estimated 17,227 maternal lives compared to an estimated 34,968 lives that were saved through the SBA strategy. Thus, the CCER strategy as implemented contributed to saving one-third (17,227/[17,227+34,968] =33%) of the lives saved during the 4-year PRRINN-MNCH period (Figure 1).
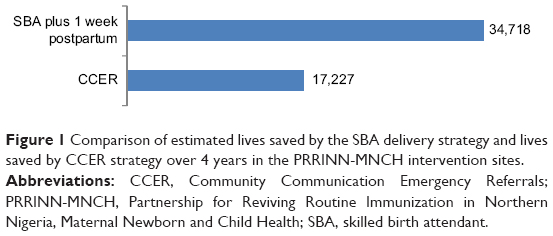 | Figure 1 Comparison of estimated lives saved by the SBA delivery strategy and lives saved by CCER strategy over 4 years in the PRRINN-MNCH intervention sites. |
The CCER theory of change
Reintroducing the three-delay model for reducing maternal deaths
To reduce rural maternal deaths in the near term, PRRINN-MNCH developed CCER, an innovative rural, mobilization intervention based on the three delay model for preventing maternal deaths.22 This model recognizes that virtually all deaths caused by direct obstetric emergencies could have been prevented by timely treatment at an EmOC. The first two delays occur at the community level (delayed decision to access facility care and delayed arrival at the facility), whereas the third delay is the delayed provision of quality care at the facility.22 PRRINN-MNCH integrated the CCER mobilization strategy that addresses the first two delays into the SBA strategy that addresses the third delay, thereby ensuring that rural women also benefited from this donor-funded maternal survival project.
The basic steps supporting the CCER theory of change are as follows: project and government change agents secure intervention support from the rural community gatekeepers (traditional leaders); the change agents facilitate a community forum to obtain buy-in resulting in the nomination of volunteer health promoters and agreement to establish the CCER support structures; four lead community volunteers (LCVs) are trained at district level; LCVs train 26 community volunteers (CVs) at community level; CVs lead 8–10 peer discussion groups weekly for 1 month, repeating this process if necessary to saturate the entire community; and, participants become community communicators spreading their new information and attitudes each week with the people in their social environment. Simultaneously, LCVs and community leaders establish and operate the CCER support structures.
Three innovative components underpinning the CCER theory of change
The CCER theory of change depends upon three innovative components: Community Communication including the community-based, informed group discussions and the communication body tools that empower their low-literate volunteer leaders; the Rapid Imitation Practice training methodology; and the community-based emergency referral support structures established by the community members themselves.
Community Communication23–25 is a form of community mobilization fully integrated with health communication that empowers community members to become the communicators spreading new health information and shared decision-making within their own social environment. Community Communication makes it easier for individuals to adopt healthier behaviors by saturating the community with informed discussions that increase social approval and pressure for change. Trained low- and nonliterate volunteers hold a series of discussions with small groups of peers encouraging the participants to discuss with people in their own social environment, so that everyone is talking about the new health information and considering its import. These community-based, informed discussions underpin the CCER transformation of rural apathy into social responsibility in the face of maternal emergencies.23,26
Community Communication depends upon innovative communication body tools23–25 that enable low-literate CVs and community members to learn, recall, share, and decide what to do about new health information with people in their own social environment. In the process, they generate their own health messages and decide themselves to change their own behaviors. For instance, in order to remember that fever is one of the nine maternal danger signs, you cross your hands over your chest while shivering and saying “fever” and for “severe bleeding” you push your hands away from your groin to represent the blood flow. Nine such “communication body tools” help people remember every danger sign rather than merely being aware of them so that they themselves can confidently become communicators, generating interpersonal discussions about these maternal danger signs and what to do about them.
Rapid Imitation Practice23,25 is the training methodology essential to Community Communication. This equitable methodology dispenses with print materials and relies on rote learning to empower nonliterate as well as literate community members to share new information and lead discussions about the import of the new information.23,25 This rote learning method involves small breakout groups with six trainees who act as community participants imitating their group leader. The leader models the danger sign with its body tool. Then each trainee has a turn as leader so that by the time everyone has acted as leader, each trainee has imitated multiple trainee-leaders, and everyone knows the new information by heart. Rapid Imitation Practice is also effective for building trainee skills to lead basic discussions among their peers. The group leader introduces a question and each trainee gives a response that represents a likely response from someone within their social environment. Everyone discusses the responses and then each trainee has the opportunity to act as the trainee-leader. In this way, the trainees become comfortable leading discussions about actions and issues arising from the new health information. Although Rapid Imitation Practice does not build the strong facilitation skills required for dialogues, it does enable nonliterate community members to own the Community Communication process. Any respected community member can become an effective CV and an effective community communicator regardless of literacy, education, wealth, sex, or social status. The CVs spread the new information along with opportunities for group reflection simultaneously to eight or more discussion groups that meet weekly. Participants are encouraged to share with their spouses, relatives, and friends and report back their interpersonal discussions to their discussion group.
CCER support structures to overcome barriers to timely emergency obstetric care were established with minimal program support after community buy-in was obtained during the initial community forum. Intervention communities established a savings scheme for emergency loans or outright gifts, an emergency transport scheme, and a blood donors group to accompany women referred to the C/BEmOC. Communities also effectively put social pressure on husbands to leave standing permission for wives to be taken to the hospital in an emergency and on families of pregnant women to ensure that a mother’s helper is present during delivery to call for help if needed. As a consequence, some communities had reported no maternal deaths for at least 2 years (Binta F Husseini 2014, personal email).
Supplementary religious leader and adolescent strategies
PRRINN-MNCH added on a religious leader communication intervention and integrated adolescent groups into the CCER communities. In 2011, PRRINN-MNCH reinforced the community-based peer group discussions with a religious leader health promotion component.27 Influential religious leaders met to develop social and behavior change communication messages reflecting the Islamic religious perspective. They developed booklets and taped cassettes, and trained more than 1,500 local religious leaders to disseminate the messages during Ramadan. More than 2 million people were reached with maternal, newborn, and child health messages using radio, television, and sermons in mosques and Islamuya schools. In addition, more than 2,000 Young Women’s Support Groups were established in CCER communities to ensure that the many young married women benefit from informed health discussions.28
Evidence from Knowledge, Attitude, and Practices Surveys
The Knowledge, Attitude, and Practices Survey respondents from within Community Communication intervention sites
Knowledge, Attitude, and Practices (KAP) changes occurred according to the intervention design based on catalyzing establishment of safe motherhood support structures and saturating the community rapidly with informed discussions to generate social approval and pressure for saving maternal lives. Rapid changes occurred around safe motherhood behaviors over a 14-month period between the baseline in November 2009 and the end line survey in February and March 2011. More than 2,000 respondents participated in each KAP survey.29 Respondents included community members who were critical targets for the CCER interventions: pregnant women, new mothers, older mothers, husbands of pregnant women, and new fathers. At end line, one-third of the respondents were “CE Light” community members who had actually received very little project support.29 Members from communities adjacent to the CCER communities requested their support, began contributing to the CCER maternal support structures, and benefitted from this new social capital for saving lives within their own communities.
Communities saturated with effective discussions
Following an initial community forum, the volunteer health promoters effectively saturated the intervention communities with group and interpersonal discussions about CCER and key health decision-making information. The CVs reached one-third of the respondents directly or indirectly through group discussions (35.3%), which contributed to a multitude of interpersonal discussions with other community members including spouse (35.6%), friends (31%), relatives (30.1%), and others.29 Moreover, the group discussions effectively built individual and community capacity for and promoted timely community referrals to EmOC. Specifically, in accordance with the CCER causal pathways, the CVs increased knowledge about the need for preparing for maternal emergencies; encouraged participation in the operations of the newly established CCER structures; promoted individual, family, and community responsibility for timely CCER referrals; and promoted sharing the new information and attitudes toward timely emergency referrals with spouses, relatives, friends, and neighbors. Within 14 months, key decision-making knowledge, strengthened attitudes toward male and community responsibility to save maternal lives, and social capital supporting CCER referrals had become normative among the people most affected by recent and current pregnancies. In addition, actual safe pregnancy planning increased significantly even though the progress was uneven and much more progress is needed.29
Knowledge
By the KAP end line survey, key decision-making maternal, newborn, and child knowledge had become normative among pregnant women and their family decision-makers versus knowledge levels below one-third prior to the intervention (Table 6). Virtually, all respondents (91%) named without prompting four maternal danger signs, a proxy for the awareness of safe motherhood emergencies. More than two-thirds of the respondents named without prompting: three ANC benefits and the correct time for initiating breast-feeding (within 30 minutes). In addition, 60% knew the routine immunization schedule based on their knowledge of the proxy, correct timing for three of the five vaccination visits.
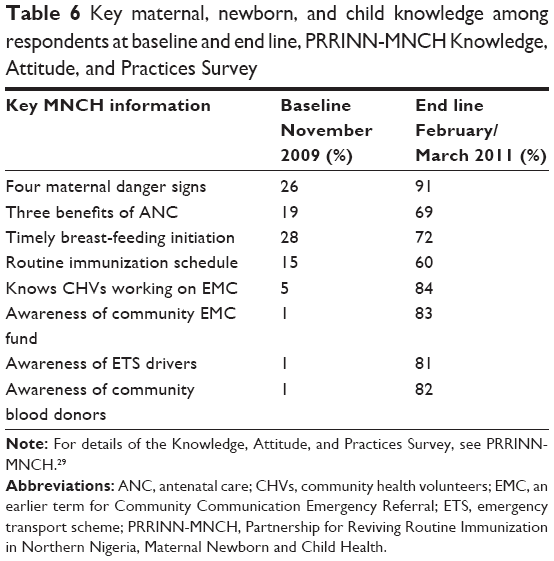 | Table 6 Key maternal, newborn, and child knowledge among respondents at baseline and end line, PRRINN-MNCH Knowledge, Attitude, and Practices Survey |
Furthermore, knowledge of the newly established CCER support systems had also become well established. Table 6 shows that 80% of respondents in the intervention communities cited multiple support systems including the community volunteers, savings fund, emergency drivers, and blood donors.29 Moreover, three-quarters of the respondents reported knowledge of particular women who had benefitted from these supports.29
Social capital built
The KAP end line survey also demonstrated that significant behavior changes had begun to take place in terms of social capital built for the CCER support structures. More than half of the end line KAP respondents reported that they had contributed to the community savings (Katsina 50%; Yobe 65%; Zamfara 48%).17 A substantial sum of money (N39 million Naira – £156,500) was saved for CCER by communities in Katsina, Yobe, and Zamfara States between December 2009 and September 2013. More than half of the women referred by the communities received a loan or outright grant to cover some or all of their emergency expenditures.17 Although not all maternal complications require blood, 25% of the maternal complications reported by the communities were supported by blood donors. Moreover, the community emergency transport schemes transported a small proportion of women for deliveries as well as those referred for emergencies.17 Many testimonies to the effectiveness of this social capital have been collected, including the following testimony from a village head.
Marariya Isa delivered at home and had a retained placenta: the husband was away from home. The chairman of the community volunteers was informed and he organised taking the woman to hospital. The chairman called an ETS driver and community volunteers accompanied the woman to Daura General Hospital [Village head, Yardaje, Katsina].30
Stronger attitudes toward spousal and community responsibility
Male involvement in safe motherhood increased significantly within the 14 months between the two KAP surveys. Men’s knowledge of four maternal danger signs increased from 19.5% to 91.7%.29 In addition, after the intervention, 77.5% of the respondents believed that community members held husbands responsible for saving maternal lives, whereas prior to the intervention only one-third (32.2%) perceived a community norm around the husband’s responsibility. Despite their perceptions of the community norms, prior to the intervention, 60.4% already held their husbands (or themselves as husbands) responsible and during the intervention, this increased to 84.4%. The belief that the community had backup responsibility for maternal emergency care was also widespread both before and after the intervention. However, a greater percentage of respondents strongly agreed at end line (52.5%) than at baseline (20.9%).29 Thus, the CCER intervention was able to build upon existing community beliefs about social responsibility.
Progress toward safe pregnancy planning
In addition, after the intervention, the percentage of parents who reported having planned for maternal emergencies themselves achieved normative levels among those directly involved in pregnancies moving from 46% to 82.1% among husbands of pregnant women and from 24.6% to 70.5% among pregnant women themselves.29 However, despite these increases in safe pregnancy planning, the 14 months period was insufficient to reach effective levels of safe pregnancy planning (at least four plans put in place) among new and pregnant parents in two of the three states. Virtually, all respondents in Katsina State (96.8%) reported having put in place at least four maternal planning actions (Table 7). In Yobe State, this percentage doubled from the baseline (11.6%–27.5%) but failed to reach higher levels most likely due to the increased insecurity. In Zamfara State, the planning actions increased in the largely nonliterate population from 0% to 23.5%.17
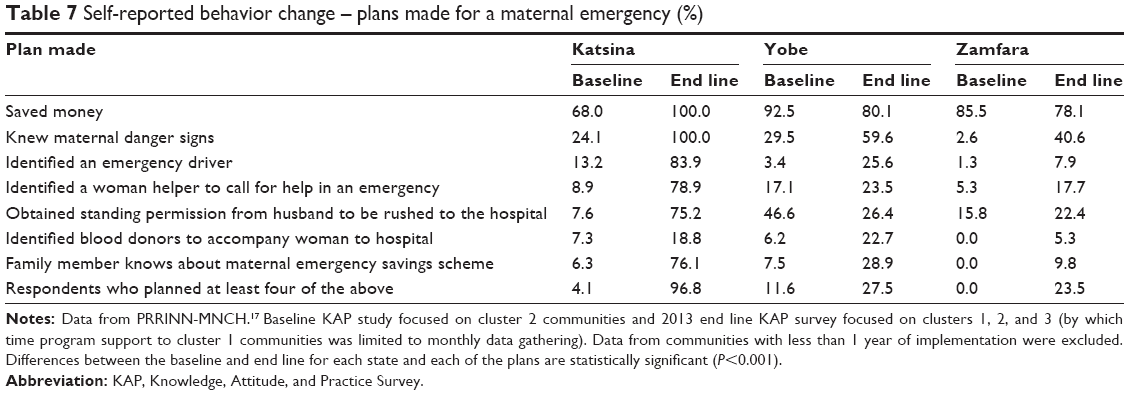 | Table 7 Self-reported behavior change – plans made for a maternal emergency (%) |
Evidence from qualitative studies
The qualitative baseline assessments
To inform CCER implementation, qualitative baseline assessments31 were undertaken in the PRRINN-MNCH states followed after 1 year of CCER implementation by a qualitative review of the Community Communication approach (formerly termed Community Engagement).32 The findings of the baseline assessments were similar to those presented in the literature cited earlier in the “The equity gap for women in northern Nigeria” section. Culturally, the husbands have sole financial and decision-making responsibility for maternal and child health, although their mothers often influence their decisions. Pragmatic concerns about the exorbitant costs relative to a man’s annual farming income inhibit timely decisions to transport a woman to a facility for emergency care. Traditional practices including a preference for birthing alone were recognized as contributing to delayed emergency care decisions. Moreover, traditional birth attendants cannot be deemed most appropriate as health promoters given their limited, postdelivery role (disposal of the placenta, cleaning of the baby, and ritual hot baths for the mother).
The widespread but partial knowledge of maternal danger signs as well as partial knowledge of their severity was recognized as contributing to the risk of delayed decisions to seek emergency care. Some of the interviewee beliefs about maternal complications reported in the assessment inhibit timely decisions to access EmOC. For example, “lower abdominal pain and bleeding after childbirth were considered normal, and fever after childbirth was considered a common sign of mild illness”.29 Thus, the studies confirmed the need for widely informed communities as a basis for changing safe motherhood practices and the need to provide financial and transport support for emergency referrals.
The qualitative Community Communication implementation review
The very comprehensive implementation review determined that overall, the strategy had been extremely successful.32 The reviewers used semistructured interviews at all levels along with transect walks in 30 participating communities as well as reviews of the relevant documents. They noted the commitment of the volunteers with very few dropouts, the establishment of operational CCER support structures, and the increased awareness of the danger signs and need to prepare for maternal emergencies. In addition, they found that there was virtually no longer any problem with obtaining standing permission from male partners to attend a health facility.32 As one male community member observed, “initially people were resistant but gradually, as they are also seeing the benefits, majority of them have changed their minds and joined us in contributing to the various CE activities”.32
The reviewers determined that CCER was successful largely because the program’s community entry forum catalyzed the establishment of the support structures and the CVs effectively spread knowledge and commitment to action through informed group discussions. One female community member explained that, “The danger signs are things we are used to seeing but we did not know they are dangers associated with them until the program came. Now we know how to deal with the danger signs”.32 The reviewers noted the effectiveness of the communication body tools in empowering both CVs and community members despite their low literacy levels. The people “have control over the information”, and one CV asserted that “We do not need posters – we are the posters”.32 The reviewers also described the lifesaving chain of events established by CCER (Figure 2).
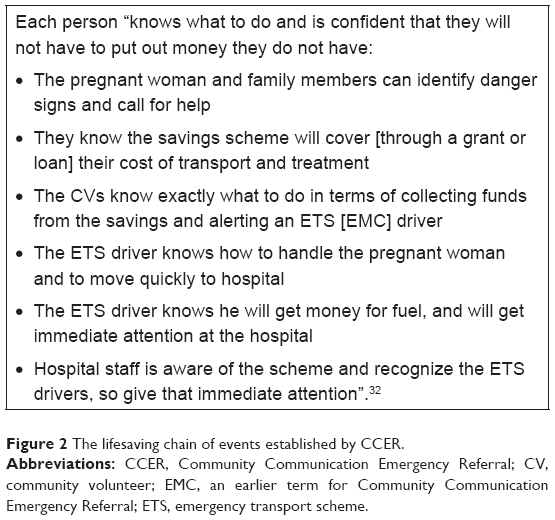 | Figure 2 The lifesaving chain of events established by CCER. |
One of the case studies cited by the reviewers exemplifies the effectiveness of the CCER intervention (Figure 3).
 | Figure 3 Case study 11, Latifa, aged 18 years. |
The reviewers assessed the key components of success, affirming that,
It is clear that the program provides communities with knowledge in a way that they understand; assists them in developing mechanisms to act on that knowledge and builds the community capacity to organise and act for themselves.32
The donor program catalyzed community establishment of CCER within the community, built the capacity of the CVs, and left the communities to implement CCER with weekly and then monthly coaching support and data gathering. Consequently, there was considerable variation in the implementation details across communities. Both community members and leaders reported that CCER implementation had increased community cohesion and responsibility. As one leader stated proudly, “the challenges and solutions belong to us all”.
According to the assessment, where CVs followed the implementation plan by holding a series of informed discussions with a small group of 8–15 of their peers, social approval and the capacity to take emergency action appeared to be better established. Where implementation was less systematic (holding ad hoc discussions with the captive but distracted audience among women during naming ceremonies or having difficulties retaining the same participants for the four discussions), social approval seemed to be well established. However, the community was more dependent upon the CVs to identify complications and take action.32(p16) The reviewers recommended increasing direct CV coverage to at least 50% of adults to effectively saturate the communities, noting that the transect walks revealed that some segments of some communities had not benefitted from the CCER intervention. The reviewers also recommended increasing technical coaching support to the CVs while cautioning that excessive support could undermine community ownership of CCER.
Discussion
This CCER case study provides large-scale evidence for an emergency obstetric care strategy to reduce maternal mortality,33 evidence that was missing in the early MDG years.34 Moreover, unlike the home-based intrapartum care strategies with skilled or lay persons, this community-based strategy does not divert scarce medical expertise from facility-based services.34 Instead, CCER relies on communication and community mobilization experts to catalyze and support community members to arrange timely emergency referrals. Although CCER has been replicated by the UK aid-funded Partnership for Transforming Health Systems II strengthening project in three northern Nigerian states, the public health evidence base still needs to be strengthened with a more robust monitoring and evaluation plan that directly links the community mobilization with the EmOC services. Nevertheless, the real-world effectiveness of CCER has been established.
Every timely emergency referral maximizes the utility of the expenditures on strengthening the SBAs and EmOCs. CCER reliance on upgraded EmOC facilities allows low-resource health systems to ensure every woman has access to lifesaving quality of care, while the health system very gradually expands quality 24/7 SBA services to the PHCs. The CCER strategy helps save lives and scarce resources without promoting an institutional delivery strategy, thereby avoiding the failure to achieve a “significant association between the proportion of institutional births and the MMR at district levels” as has been reported for the major Indian demand-side cash incentive program.35 Further, the key benefit of CCER is the prevention of maternal death or long-term harm for the majority of rural women in low-resource environments for whom the SBA strategy will not be feasible in the near and medium term.
The SBA delivery strategy is constrained by the focus on delivery and the immediate postpartum period. Only slightly more than half the complications (56% of births) occur during this period, according to calculations based on published estimates (Table 5). More than 17,000 rural women benefitted from emergency referrals to SBA services that directly averted a maternal death. To save the same number of lives through SBA deliveries, the midwives would have had to deliver more than 130,000 rural women because they could only expect one maternal emergency on average for every eight deliveries (Table 3; 17,000×8=136,000). This would have required an enormous level of effort and cost on the part of the rural communities and government.
Public health evidence has established the effectiveness of integrating the CCER strategy into the SBA strategy to save rural lives at scale. The success of the combined SBA and CCER strategy is established by the reduction in the MMR by 16.8% within 4 years versus the minimal control group reduction. The comparison of the lives saved with the CCER strategy versus the SBA strategy established that CCER contributed to saving one-third of the lives saved. In addition, the emergency referrals maximized the effectiveness of the SBAs and the strengthened EmOCs. The qualitative reviews and the KAP survey data “showed how it [CCER] can be made to work practicably at scale”.4 They demonstrate that the CCER theory of change operates effectively using the “posited causal pathway” that follows community steps to overcome the first two delays that threaten maternal lives. The CCER theory of change also relies on three innovative communication components to empower communities to decide for themselves to carry out timely maternal emergency referrals.
The qualitative reviews found that CCER was successful largely because the project’s community entry forum catalyzed the establishment of support structures including the community-based, informed group discussions led by the CVs that effectively spread knowledge and commitment to action. The reviewers also recognized the power of the Community Communication methodologies (the body tools, the Rapid Imitation Practice, and the saturation of the community with small group, informed discussions) to rapidly generate widespread behavioral change. They noted that community ownership led to some variation from the original implementation plan resulting in reduced community ownership. However, even in these cases, there was substantial social approval and reliance on the CVs when emergency complications were suspected.32
The KAP changes demonstrated that low- and nonliterate CVs using Community Communication methods saturated the intervention communities with effective, informed discussions. They generated a multitude of interpersonal discussions with spouses (35.6%), friends (31%), relatives (30.1%), and others.29 In accordance with the CCER design, the communication body tools enabled community members to become community communicators. They learned, recalled, shared, and discussed the benefits of the healthier behaviors with people in their social environment. KAP respondents reported being reached directly during volunteer group discussions and indirectly during interpersonal discussions with people in their own social environment. Since neither the supplementary religious leader and adolescent strategies nor the mass media radio spots and programs had been introduced during this period, the substantial health knowledge gains can be attributed to the informed discussions led by the volunteers and by health workers for the small percentage of rural women who did attend ANC.
The effectiveness of CCER in ensuring timely access to EmOC illustrates the value of integrating ownership of knowledge into community mobilization. Accessibility of services does not suffice. People must perceive the benefits of the services in order to access them. As pointed out by Thaddeus and Maine,22 recognition and perception of illness severity “may well be an overriding factor in the decision to seek appropriate care”. Failure to recognize a danger sign results in delayed appropriate care-seeking regardless of how near or far the SBA services are from the woman’s residence. This Community Communication intervention mitigated the fatalistic proverb that a pregnant woman has “one foot in heaven and one foot on earth” by correcting misconceptions about danger signs and modifying traditional beliefs in the normalcy of pregnancy. The very high levels of knowledge of maternal danger signs with virtually all KAP respondents (91% of those most affected by safe motherhood issues versus 26% at baseline) naming four maternal danger signs without prompting appears to have been a major factor in the changed behaviors. However, for most rural women, this knowledge would have been superfluous if it had not been combined with the CCER support structures that ensured timely, community-arranged transport for every woman experiencing a maternal emergency. The CCER integration of new, decision-making knowledge with “actual accessibility of services”22 meant that women were being rushed to EmOC facilities and returning alive after maternal emergencies. Three-quarters of the KAP respondents were aware of women who had benefitted from the CCER supports. The dramatic instances of maternal survival appear to have functioned as an extremely powerful communication event that contributed to the rapid 14-month change from apathy to social responsibility for saving women’s lives.23,26
The CCER social approval and cohesive community involvement built social capital. More than half of the KAP respondents contributed to the savings schemes promoted during the group discussions. Significantly, more than half of the women who benefitted from community emergency referrals received funds from the scheme in addition to transport and a quarter benefitted from community blood donors. Stronger attitudes about men’s responsibility for maternal health care appear associated with widespread knowledge of women benefitting from the maternal support structures – recognition that with community support men can fulfill their role as protectors of their family health.
Despite the effectiveness of CCER, this emergency referral strategy for reducing maternal mortality requires further strengthening. CCER is only effective in places where the health system provides upgraded SBA services at EmOCs. Thus, effective CCER interventions will always depend upon effective health system strengthening. For most obstetric complications, the community intervention will suffice to ensure timely care, because the interval between the onset of a major obstetric complication and death lasts 1 or more days depending upon the complication.20 Postpartum hemorrhage is the exception because it can result in a maternal death within 2 hours (Maine, unpublished data) especially if the woman is anemic. Although some CCER communities have reported 2 years without any maternal deaths (Hussaini 2014, personal communication), most communities can expect to continue to experience some deaths, especially postpartum hemorrhage deaths. In order to prevent these deaths, CCER needs to incorporate community-based distribution of misoprostol.36,37
Given its strong community ownership, the CCER intervention has the potential to adapt to diverse environments in order to ensure that poor women have timely access to lifesaving medical services regardless of their chosen delivery site. The CCER strategy will benefit from further adaptations. In places where rainy season results in impassable, swollen rivers, alternative strategies will be required, possibly including maternity waiting homes or informal arrangements. Adaptations will also be necessary for the many women living in small, widely dispersed communities where community mobilization is much more costly and where available volunteer health promoters and support structures may live very far away. More targeted integration with existing religious and social groups can also reinforce the shared knowledge and social cohesion. Moreover, all CCER communities will need to ensure that they reach out to the vulnerable women who have already lost children. Research across the project states has demonstrated a clustering of multiple child deaths among 20% of women suffering “just over 80% of all deaths”.38 Over time, following the lead of many existing CCER communities, promotion of and utilization of ANC, facility delivery, postpartum services, and child spacing needs to take greater prominence. Given the costs for good quality SBA services, and the savings in terms of cost and level of effort associated with CCER, adaptations of CCER also have the potential to benefit vulnerable impoverished women in urban areas. Even in urban environments with sufficient and well-distributed midwives, increased demand for SBA delivery may produce severe overcrowding of the available facility beds. Moreover, without any adaptations, this CCER community mobilization intervention can be expected to be even more effective in the original CCER states given the strengthened health systems and experience gained by the implementers and communities.
Limitations
The base data used for the comparison between the SBA strategy (number of SBA deliveries) and the CCER strategy (number of women transported to EmOC facilities) is only valid to demonstrate the order of magnitude differential between the two strategies. The specifics of the base data (297,349 women delivered by SBAs and 17,227 women benefitting from CCER for timely treatment of complications) are inexact. The SBA delivery data depend upon project household survey respondents’ reports on the category of the service provider who assisted at their deliveries. However, their assertion of having a skilled birth attendant at delivery may be a misunderstanding. They may not have been able to distinguish the correct cadre of staff with supplementary lifesaving skills training.39 The CCER data depend upon community reports of maternal emergencies and transport records. However, these records were not cross-checked against EmOC admissions. Moreover, the depth of data collected by the project’s monitoring and evaluation team on obstetric emergencies treated was limited. In addition, the comparison of the lifesaving strategies relies on approximations of relative percentages of direct, indirect, and unclassified causes of maternal emergencies, although the percentages are held constant for both strategies.
The KAP surveys indicate clear trends toward healthier, safe motherhood knowledge, attitudes, and practices arising from the CCER intervention. However, the KAP samples were partially purposive to explore the responses of the people most directly involved with maternal emergencies rather than the general population. Furthermore, the survey communities were equally divided among the three types of intervention communities: CE Complete, CE Complete Plus, and CE Light. Thus, one-third of the respondents lived in communities where other interventions reinforced the Community Communication work, while another one-third lived in communities with minimal project support.29 During the analysis stage, some data collected, especially data related to the use of the community support structures, appeared unreliable and were deleted from the end line results. This constrained the program’s ability to report on selected outcomes.29 In addition, the data are based on the respondents’ self-reports, which may be influenced by social desirability bias causing them to respond according to their perception of the interviewer’s beliefs rather than their own reality.
Conclusion
Global programs for ending preventable maternal mortality have the responsibility to develop safe motherhood programs that address the majority of women, especially rural women. The public health evidence4 presented here records the successful PRRINN-MNCH implementation of the CCER intervention at scale in a very challenging environment. This community-based, emergency obstetric care strategy ensured the timely referral and arrival of women experiencing maternal emergencies at upgraded SBA facilities essential for saving their lives. Integration of the CCER strategy into the SBA strategy contributed to saving more than one-third of the lives saved. CCER is an equitable, efficient, and culturally appropriate approach for saving the lives of rural women experiencing maternal emergencies in resource-constrained countries. CCER is especially efficient because virtually every timely, community referral for emergency maternal care results in a saved life, whereas only one in every eight births delivered by an SBA is expected to be a delivery-associated complication requiring lifesaving care. Although the available evidence fails to meet rigorous randomized controlled trial standards and lacks data directly linking women benefitting from community referrals to their EmOC treatment, the evidence indicates that CCER warrants further implementation in northern Nigeria and elsewhere. In order to establish a strong public health evidence base,4 CCER interventions and adaptations with well-integrated monitoring and evaluation programs will be essential in diverse, low-resource settings.
Acknowledgments
Most of the data reported in this study were collected as part of the PRRINN-MNCH project activities and are published on the PRRINN-MNCH website (www.prrinn-mnch.org). The authors acknowledge the support of the government, community leaders and members, staff, consultants, and senior technical advisors who participated in a number of surveys, assessments, and discussions and led the design of some of the interventions reported here. We also acknowledge the support of Dr Rodion Kraus, Deputy National Program Manager and the entire PRRINN-MNCH team.
The views expressed in this paper are those of the authors and do not represent the views of their previous or current institutions or organizations.
Author contributions
All the authors provided substantial contribution to the conception and design, acquisition of data, analysis and interpretation, revision of drafts, and gave their final approval for the final version of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Koblinsky M, Matthews Z, Hussein J, et al. Maternal survival 3: going to scale with professional skilled care. Lancet. 2006;368:1377–1386. | ||
Crowe S, Utley M, Costello A, Page C. How many births in sub-Saharan Africa and South Asia will not be attended by a skilled birth attendant between 2011 and 2015? BMC Pregnancy Childbirth. 2012;12:4. | ||
Costello A, Azad K, Barnett S. An alternative strategy to reduce maternal mortality. Lancet. 2006;368:1478–1479. | ||
Shelton JD. Evidence-based public health: not only whether it works, but how it can be made to work practicably at scale. Glob Health Sci Pract. 2014;2(3):253–258. | ||
Doctor HV, Findley SE, Afenyadu GY. Estimating maternal mortality level in rural northern Nigeria by the sisterhood method. Int J Popul Res. 2012;2012:464657. | ||
National Population Commission (NPC) [Nigeria], ICF International. Nigeria Demographic and Health Survey 2013. Abuja, Nigeria and Rockville, MD: NPC and ICF International; 2014. | ||
Wall LL. Dead mothers and injured wives: the social context of maternal morbidity and mortality among the Hausa of northern Nigeria. Stud Fam Plann. 1998;29:341–359. | ||
Trevor J. Family change in Sokoto, a traditional Moslem Fulani/Hausa city. In: Caldwell JC, Igun AA, Gaisie SK, Addo NO, Olusanya PO, editors. Population Growth and Social Change in West Africa. New York, NY: The Population Council; 1975. | ||
Doctor HV, Findley SE, Ager A, et al. Using community-based research to shape the design and delivery of maternal health services in Northern Nigeria. Reprod Health Matters. 2012;20(39):104–112. | ||
Moerman ML. Growth of the birth canal in adolescent girls. Am J Obstet Gynecol. 1982;143(5):528–532. | ||
Tukur BM, Bawa U, Odogwu K, Adaji S, Suleiman I, Passano P. Praying for divine intervention: the reality of “the three delays” in northern Nigeria. Afr J Reprod Health. 2010;14(3):113–120. | ||
Ahmad BM. Women Perception of Eclampsia in Kano [Bachelor of Science Degree Project]. Kano, Nigeria: Department of Geography, Bayero University; 1999. | ||
Adamu YM, Salihu HM, Sathiakumar N, Alexander GR. Maternal mortality in Northern Nigeria: a population-based study. Eur J Obstet Gynecol Reprod Biol. 2003;109:153–159. | ||
Fatusi AO, Ijadunola KT. National Study on Essential Obstetric Care Facilities in Nigeria. Abuja, Nigeria: Federal Ministry of Health and UNFPA; 2003. | ||
Babalola S, Fatusi A. Determinants of use of maternal health services in Nigeria – looking beyond individual and household. BMC Pregnancy Childbirth. 2009;9:43. | ||
PRRINN-MNCH. Health Service Delivery Using the Cluster Approach in Summary: Health Service Delivery. 2013. Available from: http://www.prrinn-mnch.org/documents/PRRINN-MNCH2ClusterApproachSummary.pdf. Accessed July 11, 2015. | ||
PRRINN-MNCH. Final Report 2013: Better Maternal Child and Newborn Health in Northern Nigeria. 2013. Available from: http://www.prrinn-mnch.org/documents/PRRINN-MNCHFinalReport2013.pdf. Accessed July 11, 2015. | ||
Shutt C. Value for Money – Qualitative Analysis, PRRINN-MNCH: A Report to Health Partners International. 2012. Available from: http://www.prrinn-mnch.org/documents/VFMQualitativereportfinal28May12_21.pdf. Accessed June 30, 2015. | ||
WHO, UNFPA, UNICEF, Mailman School of Public Health – Averting Maternal Death and Disability (Columbia University). Monitoring Emergency Obstetric Care: A Handbook. 2009. Available from: http://www.amddprogram.org/sites/default/files/emochandbook_revisedaug10_eng.pdf. Accessed July 15, 2015. | ||
de Bernis L, Sherratt DR, Abou Zahr C, Van Lerberghe W. Skilled attendants for pregnancy, childbirth and postnatal care. Br Med Bull. 2003;67(1):39–57. | ||
Nour NM. An introduction to maternal mortality. Rev Obstet Gynecol. 2008;1(2):77–81. | ||
Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med. 1994;38(8):1091–1110. | ||
Aradeon SB, Soyoola M. Part 0: Community Communication. In e-Manual for Community Communication: MNCH Interactive Health Promotion Sessions. 2014. Available from: http://healthcommcapacity.org/health-compass. Accessed January 18, 2016. | ||
PATHS2. Communication Body Tools for Safe Motherhood [a DVD short: in Hausa with English subtitles]. Abuja, Nigeria: PATHS2; 2012. Available from: www.youtube.com/watch?v=3lUcbHHMvWY. Accessed August 11, 2015. | ||
Aradeon SB, Abdullahi MI, Hussaini BF. Rapid entertainment education. In: Onueke CE, editor. Entertainment-Education for Health Behaviour Change: Issues and Perspectives in Africa. Victoria, BC, Canada: FriesenPress; 2015:175–198. | ||
Aradeon SB, Aminu A, Doctor HV. Towards Better Solutions for Reducing Maternal Mortality and the associated Handout, Integrating Community Communication into the SBA Model for Reducing Maternal Mortality. Presented at: American Public Health Association Annual Meeting, November 15–19, 2014, New Orleans, LA. Available from: https://apha.confex.com/apha/142am/webprogram/Paper315565.html. Accessed February 7, 2016. | ||
Ben Umar H, Gill-Bailey A. Technical Brief on Collaboration with Religious Leaders. 2012. Available from: http://www.prrinn-mnch.org/documents/EngagingwithReligiousLeaders_final_May12_26.pdf. Accessed January 18, 2016. | ||
PRRINN-MNCH. Young Women’s Support Groups: Empowering Young Women and Improving Maternal Health. Technical Brief 5 of Community Engagement. 2013. Available from: http://www.prrinn-mnch.org/documents/PRRINN-MNCH3YWSGBrief.pdf. Accessed July 11, 2015. | ||
PRRINN-MNCH. Engaging with Communities to Increase Demand for MNCH Services: Summary of Results from the Endline MNCH KAP Survey in Katsina, Yobe and Zamfara States. 2011. Available from: www.prrinn-mnch.org/documents/Results_MNCHKAP_combine_Nov11_000.pdf. Accessed July 10, 2015. | ||
PRRINN-MNCH. Community Emergency Transport in Technical Brief 3 of Community Engagement. 2013. Available from: http://www.prrinn-mnch.org/documents/PRRINN-MNCH3EmergencyTransportBrief.pdf. Accessed July 11, 2015. | ||
PRRINN-MNCH. PRRINN-MNCH Baseline Studies Summary Report. 2009. Available from: http://www.prrinn-mnch.org/documents/PRRINN-MNCHBaselineStudiesSummaryReport2009.pdf. Accessed July 14, 2015. | ||
Surridge M, Bashir A, Amzat J. Unpublished Report to PRRINN-MNCH Program: Review and Documentation of Community Engagement Approach and Interventions (Assignment No: M.NT.6.1.1.G), January – March, 2011. | ||
Paxton A, Maine D, Freedman L, Fry D, Lobis S. The evidence for emergency obstetric care. Int J Gynaecol Obstet. 2005;88:181–193. | ||
Campbell OM, Graham WJ. Strategies for reducing maternal mortality: getting on with what works. Lancet. 2006;368:1284–1299. | ||
Randive B, Diwan V, De Costa A. India’s conditional cash transfer programme (the JSY) to promote institutional birth: is there an association between institutional birth proportion and maternal mortality? PLoS One. 2013;8(6):e67452. | ||
WHO. WHO Recommendations for the Prevention and Treatment of Postpartum Haemorrhage. 2012. Available from: http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/9789241548502/en/. Accessed December 31, 2015. | ||
Geller S, Carnahan L, Akosah E, et al. Community-based distribution of misoprostol to prevent postpartum haemorrhage at home births: results from operations research in rural Ghana. BJOG. 2014;121:319–326. | ||
PRRINN-MNCH. Clustering of Child Mortality in Northern Nigeria – Implications for Policy and Practice. 2012. Available from: http://www.prrinn-mnch.org/documents/clusteringstudy_childmortality_24.pdf. Accessed July 14, 2015. | ||
Warren C, Kimani J, Kivunaga J, et al. Validating the Indicators of the Quality of Maternal Health Care: Final Report, Kenya. Nairobi, Kenya: Population Council; 2014. Available from: http://www.popcouncil.org/uploads/pdfs/2014RH_MHTF-Kenya.pdf. Accessed December 20, 2015. | ||
PRRINN-MNCH. Baseline to Endline Changes in Maternal Health Outcomes. Technical Brief 2 of Evidence for Action. 2013. Available from: http://www.prrinn-mnch.org/documents/PRRINN-MNCH4EndlineMNCHOutcomesBrief.pdf. Accessed 11 July 2015. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.