Back to Journals » Open Access Emergency Medicine » Volume 15
Reducing Door-In to Door-Out Time for Patients Receiving a Mechanical Thrombectomy Using AutoLaunch Protocol
Authors Howell DM ![]() , Li T, Quellhorst E, Katz JM, Arora R, Berkowitz J
, Li T, Quellhorst E, Katz JM, Arora R, Berkowitz J
Received 28 June 2023
Accepted for publication 11 October 2023
Published 17 October 2023 Volume 2023:15 Pages 367—371
DOI https://doi.org/10.2147/OAEM.S427945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Devin M Howell,1,2 Timmy Li,1 Elizabeth Quellhorst,2 Jeffrey M Katz,3 Rohan Arora,3 Jonathan Berkowitz2
1Department of Emergency Medicine, Northwell Health, Manhasset, NY, USA; 2Center for Emergency Medical Services, Northwell Health, Syosset, NY, USA; 3Department of Neurology, Northwell Health, Manhasset, NY, USA
Correspondence: Devin M Howell, Department of Emergency Medicine, Northwell Health, 300 Community Drive, Manhasset, NY, 11030, USA, Email [email protected]
Background: Door-in to door-out (DIDO) time for large vessel occlusion (LVO) stroke is an emerging stroke performance measure. Initial presentation at a non-Comprehensive Stroke Center (CSC) requires a transfer process that minimizes delays. Our objective was to assess whether DIDO time for stroke patients was reduced after implementation of an AutoLaunch protocol for interfacility transfers.
Methods: This was a pre-post analysis of an AutoLaunch protocol for all acute stroke patients transferred to a CSC for mechanical thrombectomy. The distribution of DIDO times between patients transferred via the AutoLaunch and traditional dispatch protocols were compared.
Results: We evaluated 92 interfacility transfers, with 22 utilizing the AutoLaunch protocol and 70 utilizing traditional dispatch. Among AutoLaunch transfers, the median DIDO time was 85 minutes (IQR: 71, 133), while the median DIDO time among the traditional transfers was 109 minutes (IQR, 84, 144) (p=0.044).
Conclusion: Implementation of an AutoLaunch protocol for patients with suspected LVO was associated with a reduction in DIDO time to CSCs. Further studies should evaluate patient outcomes based on transfer strategies.
Keywords: AutoLaunch, interfacility, transfer, EMS, stroke
Introduction
Transferring a patient between hospitals is a logistically complex and timely process. Prabhakaran et al evaluated 191 patients, demonstrating that transfer center contact time to ambulance request time and ambulance request to arrival time led to a combined average of 40.5 minutes in delayed transfer time.1 Another study demonstrated that transfer delays in up to 14% of Acute Ischemic Stroke (AIS) patients made them ineligible for intra-arterial treatment.2 In order to reduce interfacility transfer delays, Northwell Health’s Center for Emergency Medical Services (CEMS) implemented an AutoLaunch protocol on March 25, 2019. If a Large Vessel Occlusion (LVO) is identified via brain Computed Tomography Angiogram (CTA) at the Primary Stroke Center (PSC) and last known well time is <24 hours, the sending Emergency Department (ED) physician can initiate a tier 1 (immediate threat to life or limb) transfer to a Comprehensive Stroke Center (CSC). This process allows for an ambulance to be dispatched to the sending facility prior to acceptance of the patient by the receiving facility. The physician is simultaneously connected to an accepting physician at the CSC to discuss the patient and receive formal acceptance. A retrospective pre-post analysis of this process after its implementation found that the AutoLaunch protocol resulted in a 27.6% reduction in response time, or 7.6 minutes saved, among all interfacility transfers.3 Although this process is applied to all critical transfers requiring life-saving intervention or higher level of care, whether the protocol reduced Door-In to Door-Out (DIDO) time for stroke patients requiring thrombectomy was unknown.
DIDO time is an emerging clinical stroke performance measure, defined as the duration of time from initial patient presentation to discharge from the initial, non-stroke center hospital. Reduction in DIDO time was found to be one of the most modifiable factors in reducing recanalization time, where delays could propagate further neurologic damage due to brain tissue ischemia.4 Although most EDs have access to Alteplase (tPA) or Tenecteplase (TNK), not all are CSCs capable of post-thrombolytic monitoring and/or performing mechanical thrombectomy. LVO may be the cause of AIS in over 30% of cases,5 and mechanical thrombectomy has been well-studied as an early treatment for LVO that is capable of reducing disability in these patients.6–10 If CSC facilities are local and appropriate, any candidates for thrombectomy should be expeditiously transferred.
While there is not yet a gold standard for DIDO time, limiting it to <60 minutes in stroke patients with emergent LVO leads to significant reduction in morbidity and mortality.11 The objective of this study was to assess whether DIDO time for stroke patients requiring thrombectomy was reduced after implementation of the AutoLaunch protocol.
Methods
This was a pre-post analysis of DIDO time for patients transferred to our CSC. The pre-intervention period was January 1, 2019 to March 24, 2019, and the post-intervention period was March 25, 2019 to December 31, 2020. Our health system’s Institutional Review Board determined that this was a quality improvement project, and that IRB approval was not required. Patients were identified by querying our hospital’s medical record system for all patients who were transferred for thrombectomy. Patient characteristics were electronically pulled from our hospital’s electronic medical record system and their EMS medical records were reviewed to ascertain their DIDO times.
The CEMS at Northwell Health is a hospital system-based ambulance service in New York, handling approximately 85,000 emergency calls and 25,000 interfacility transfers (IFTs) annually. North Shore University Hospital (NSUH), part of Northwell Health, is a 756-bed quaternary care hospital and CSC in Manhasset, NY, US. All patients transferred to NSUH by a CEMS ambulance between January 1, 2019 and December 31, 2020 for thrombectomy were included in our analysis. In June, 30, 2020, our institution started a telestroke protocol; patients transferred under this protocol were excluded from our analysis.
The traditional dispatch protocol involves: the requesting provider discussing with a receiving facility provider, acceptance of the patient by the receiving provider, bed arrangement at the receiving facility, and transport to the receiving facility. Our AutoLaunch protocol dispatches an ambulance to the sending facility once an IFT request is made, prior to the acceptance of the patient by the receiving facility.
We used descriptive statistics to describe the study sample. Data were stratified by whether the ambulance was dispatched using the AutoLaunch protocol or traditional dispatch, and patient characteristics were compared using Wilcoxon rank, chi-square, or Fisher’s exact tests, as appropriate. The Wilcoxon rank sum test was used to determine whether the distribution of DIDO time was different according to whether the ambulance utilized the AutoLaunch protocol or traditional dispatch. Statistical significance was defined as p<0.05. Analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC, USA).
Results
Data from a total of 92 patients were analyzed, 57 from 2019 and 35 from 2020. As shown in Table 1, a total of 22 patients (11 in 2019 and 11 in 2020) were transferred with AutoLaunch and 70 patients (46 in 2019 and 24 in 2020) were transferred with traditional dispatch. The traditional dispatch transfers (24 in 2020) occurring during the post-analysis were due to backdoor transfers, or direct physician-to-physician transfer acceptance prior to contacting the CSC. The median age of the study sample was 69 years (IQR: 55, 79), 53.3% were male, 46.7% were white, and the majority (23.9%) of transfers occurred on Thursday. Median NIHSS score prior to the transfer was 17 (IQR: 14, 22). Demographic characteristics and NIHSS score were not significantly different between patients transferred via the AutoLaunch and traditional dispatch protocols.
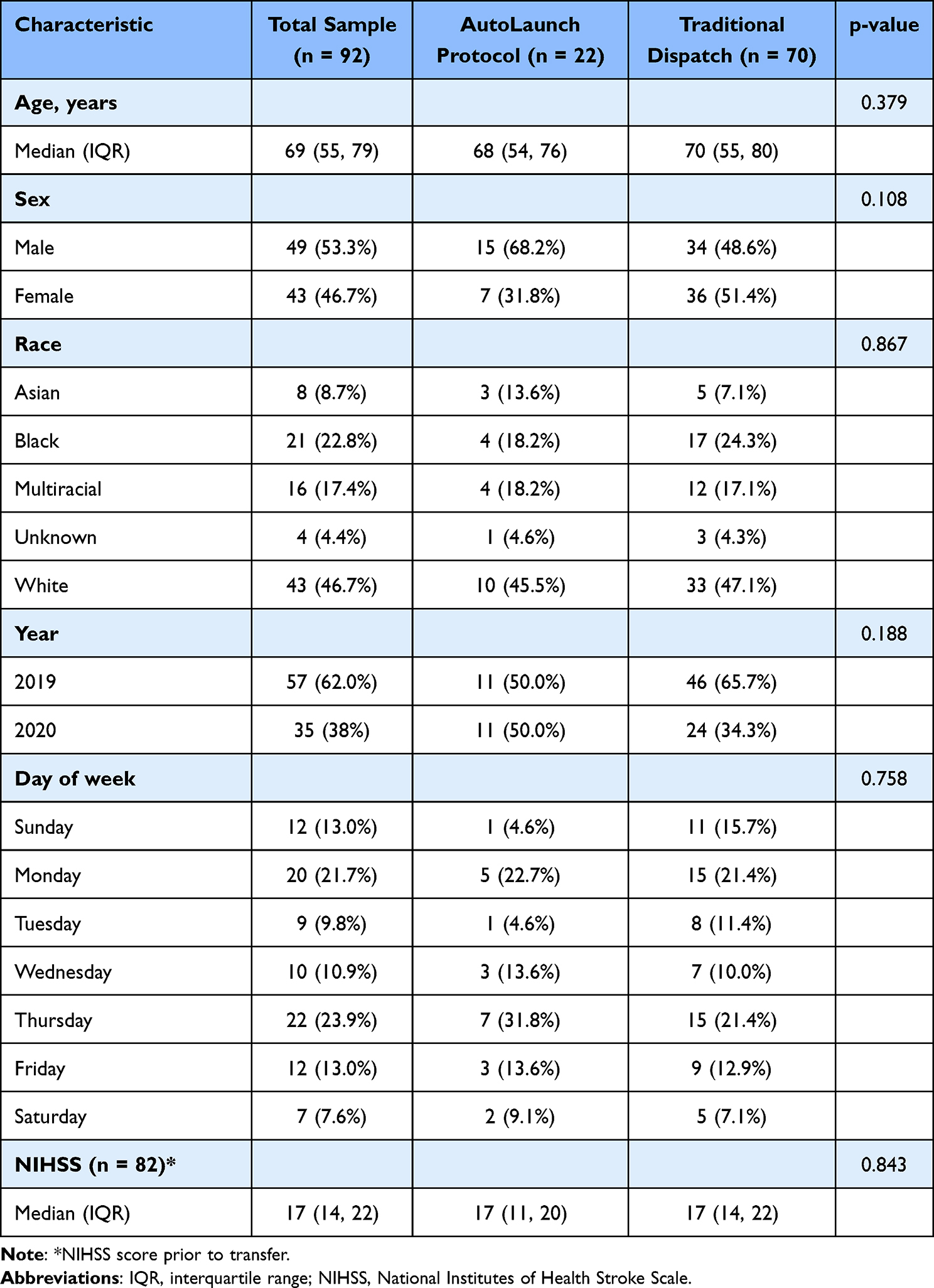 |
Table 1 Patient Characteristics |
As shown in Table 2, the distribution of DIDO times differed significantly based on protocol. Among the 22 patients transferred utilizing the AutoLaunch protocol, the median DIDO time was 85 minutes (IQR: 71, 133), while the median DIDO time among the 70 patients utilizing traditional dispatch was 109 minutes (IQR, 84, 144) (p=0.0435). There was substantial variability in DIDO among the traditional dispatch protocol, with DIDO times ranging from 34 minutes to 1234 minutes, while there was less variability among the AutoLaunch Protocol (range: 40 to 320 minutes).
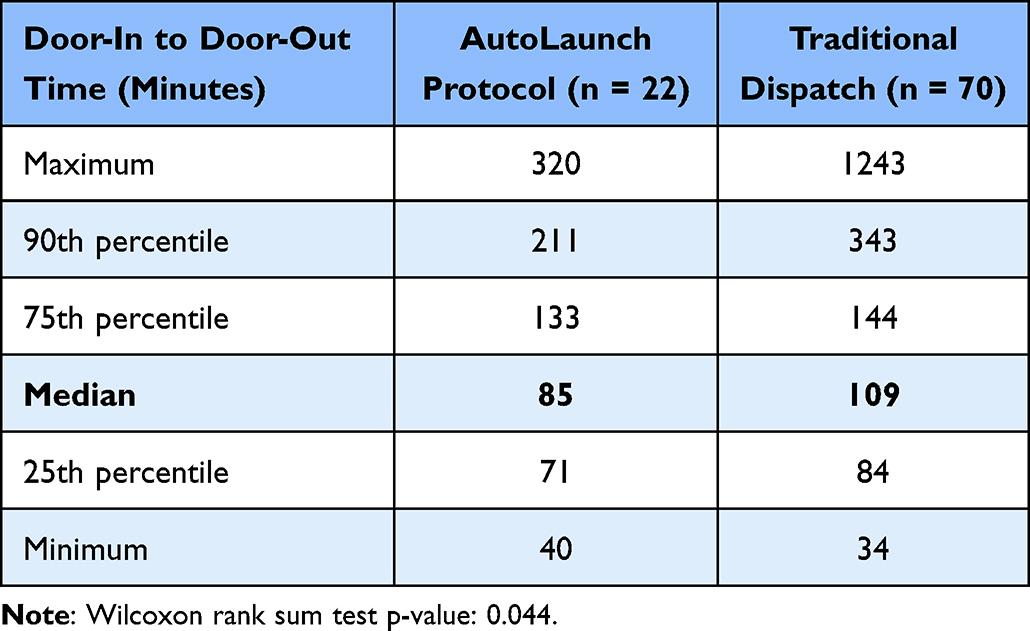 |
Table 2 DIDO Time Among AutoLaunch vs Traditional Dispatch Protocols |
Discussion
Our study examined the impact of an EMS AutoLaunch protocol on DIDO times for stroke transfers. Stroke transfers utilizing the EMS AutoLaunch protocol were associated with a median DIDO time reduction of 34 minutes. This is consistent with our findings that AutoLaunch reduced the response time (time from transfer request to EMS pickup) for all critical transfers.3 Although patient outcomes were not evaluated in this study, the relationship between time to reperfusion and patient outcomes has been well studied.12–14 DIDO has been also suggested as a predictor of stroke outcome for patients requiring endovascular treatment.
Gaynor et al used a stay-in-place approach to reduce DIDO for acute stroke patients; ambulance crews would wait at the sending facility with the patient until the decision to transfer was made.15 Although this was highly effective at reducing DIDO (47% reduction as opposed to 30%) and was associated with improved door to needle (DTN) and door to CT times, it is not feasible in EMS systems where emergency calls (ie, calls to a scene of patient) are managed by different EMS crews than interfacility calls. This later description applies to much of the US health system. When the reductions in DTN and door to CT times are considered, the impacts of this protocol are very similar to what was found in our analysis. In addition, the median staging time for the AutoLaunch protocol was 10.1 minutes, suggesting that AutoLaunch consumes fewer unit hours of EMS time than does the stay in place protocol.2
Bedside time, defined as the time it takes for EMS to prepare a patient for transport, is another target for reduction to improve DIDO times. Katz et al demonstrated that a stroke rescue program was able to reduce the bedside time in the initial ED by 9 minutes.16 It would be expected that the impacts of AutoLaunch and a rescue program be summative and not mutually exclusive. We therefore propose each system may require multiple changes to their interfacility transfer process to achieve DIDO goals.
The strength of this study was our ability to merge data from both our EMS agency and our receiving hospital. Despite this, there were several limitations. First, our data are representative of a single healthcare system that has an integrated EMS agency; therefore, it may be challenging to reproduce these results in other systems. Second, this was a retrospective, pre-post analysis. Although there were no changes to the stroke protocol in our health system during the study timeframe, there has been a consistent effort to improve stroke quality metric times and thus, it is possible that other factors may have contributed to the reduction in DIDO time. However, that would not explain the previously documented finding that the AutoLaunch protocol is associated with a reduction in interfacility transfer time among critical transfers overall.3 Finally, the study partially eclipsed the COVID-19 pandemic, which may have affected times due to changes in ED workflow.
Reducing the time for endovascular treatment in stroke transfers is a complex, multi-factorial problem. Our prior research has shown that AutoLaunch significantly reduces EMS response time for interfacility transfers, and the goal of this study was to demonstrate its impact on DIDO for stroke patients requiring thrombectomy. Overall, we found that AutoLaunch was associated with a significant reduction in DIDO for thrombectomy stroke transfers. Future studies should evaluate patient outcomes based on transfer strategies.
Abbreviations
DIDO, door-in to door-out; LVO, large vessel occlusion; CSC, comprehensive stroke center; CEMS, Center for Emergency Medical Services; IFT, interfacility transfer; NSUH, North Shore University Hospital; IQR, interquartile range; DTN, door to needle.
Acknowledgments
All views expressed in the submitted article are our own and not an official position of the institution or funder.
Funding
There is no funding to report.
Disclosure
Dr Jeffrey Katz reports personal fees from Medtronic, XCath, Inc; grants from Siemens Healthineers, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Prabhakaran S, Khorzad R, Parnianpour Z, et al. Door-In-Door-out process times at primary stroke centers in Chicago. Ann Emerg Med. 2021;78(5):674–681. doi:10.1016/j.annemergmed.2021.06.018
2. Prabhakaran S, Ward E, John S, et al. Transfer delay is a major factor limiting the use of intra-arterial treatment in acute ischemic stroke. Stroke. 2011;42(6):1626–1630. doi:10.1161/STROKEAHA.110.609750
3. Howell D, Li T, De Bono J, Berkowitz J. Reduction in interfacility transfer response time after implementation of an autolaunch protocol. Prehospital Emerg Care. 2022;26(5):739–745. doi:10.1080/10903127.2021.1954271
4. McTaggart RA, Moldovan K, Oliver LA, et al. Door-in-Door-Out time at primary stroke centers may predict outcome for emergent large vessel occlusion patients. Stroke. 2018;49(12):2969–2974. doi:10.1161/STROKEAHA.118.021936
5. Lakomkin N, Dhamoon M, Carroll K, et al. Prevalence of large vessel occlusion in patients presenting with acute ischemic stroke: a 10-year systematic review of the literature. J Neurointerv Surg. 2019;11(3):241–245. doi:10.1136/neurintsurg-2018-014239
6. Fransen PS, Beumer D, Berkhemer OA, et al. MR CLEAN, a multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke in the Netherlands: study protocol for a randomized controlled trial. Trials. 2014;15(1):343. doi:10.1186/1745-6215-15-343
7. Goyal M, Demchuk AM, Menon BK, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372(11):1019–1030. doi:10.1056/NEJMoa1414905
8. Saver JL, Goyal M, Bonafe A, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 2015;372(24):2285–2295. doi:10.1056/NEJMoa1415061
9. Campbell BC, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372(11):1009–1018. doi:10.1056/NEJMoa1414792
10. Jovin TG, Chamorro A, Cobo E, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015;372(24):2296–2306. doi:10.1056/NEJMoa1503780
11. Choi PMC, Tsoi AH, Pope AL, et al. Door-in-Door-Out Time of 60 minutes for stroke with emergent large vessel occlusion at a primary stroke center. Stroke. 2019;50(10):2829–2834. doi:10.1161/STROKEAHA.119.025838
12. Ma G, Yu Z, Jia B, et al. Time to endovascular reperfusion and outcome in acute ischemic stroke: a Nationwide Prospective Registry in China. Clin Neuroradiol. 2022;32(4):997–1009. doi:10.1007/s00062-022-01178-7
13. Jahan R, Saver JL, Schwamm LH, et al. Association between time to treatment with endovascular reperfusion therapy and outcomes in patients with acute ischemic stroke treated in clinical practice. JAMA. 2019;322(3):252–263. doi:10.1001/jama.2019.8286
14. Nogueira RG, Smith WS, Sung G, et al. Effect of time to reperfusion on clinical outcome of anterior circulation strokes treated with thrombectomy: pooled analysis of the MERCI and Multi MERCI trials. Stroke. 2011;42(11):3144–3149. doi:10.1161/STROKEAHA.111.624163
15. Gaynor E, Griffin E, Thornton J, et al. Ambulance waiting and associated work flow improvement strategies: a pilot study to improve door-in-door-out time for thrombectomy patients in a primary stroke center. J Neurointerv Surg. 2022;14(6):573–576. doi:10.1136/neurintsurg-2021-017653
16. Kodankandath TV, Wright P, Power PM, et al. Improving transfer times for acute ischemic stroke patients to a Comprehensive Stroke Center. J Stroke Cerebrovasc Dis. 2017;26(1):192–195. doi:10.1016/j.jstrokecerebrovasdis.2016.09.008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Admission Hyperglycemia with Clinical Outcomes in Patients with Symptomatic Intracranial Hemorrhage After Endovascular Treatment for Large Vessel Occlusive Stroke
Yan J, Huang J, Pu T, Song J, Yang J, Li L, Li F, Zi W, Guo C, Peng Z
Clinical Interventions in Aging 2024, 19:1545-1556
Published Date: 23 September 2024
Association Between Liver Fibrosis Markers and Hemorrhagic Transformation Following Endovascular Treatment for Acute Ischemic Stroke: A Chinese Stroke Center Study
Gao W, Zhao Y, She J, Wu Z, Cai L, Chen X, Zhu R
International Journal of General Medicine 2025, 18:6107-6122
Published Date: 8 October 2025