Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Reduced Attentional Capture by Topological Changes in Children with Autism Spectrum Disorder: Evidence for a Perceptual Deficit
Authors Li J, Xi H, Zhang Q, Duan T, Li D, Shi L, Gan S, Li H, Zhu C
Received 17 April 2025
Accepted for publication 26 September 2025
Published 29 October 2025 Volume 2025:21 Pages 2401—2413
DOI https://doi.org/10.2147/NDT.S535054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Rakesh Kumar
Jing Li,1,* Huanjun Xi,2,* Qingqing Zhang,1 Tao Duan,1 Dandan Li,1,3,4 Lei Shi,5 Shuoqiu Gan,2 Hong Li,5 Chunyan Zhu1,3,4,6
1School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, 230032, People’s Republic of China; 2Institute of Artificial Intelligence, Hefei Comprehensive National Science Center, Hefei, 230088, People’s Republic of China; 3Anhui Province Key Laboratory of Cognition and Neuropsychiatric Disorders, Hefei, 230022, People’s Republic of China; 4Collaborative Innovation Center of Neuropsychiatric Disorders and Mental Health, Hefei, Anhui, 230022, People’s Republic of China; 5Department of Pediatric Rehabilitation, Anhui Hospital Affiliated to the Pediatric Hospital of Fudan University, Hefei, People’s Republic of China; 6Department of Psychology, The Second Affiliated Hospital of Anhui Medical University, Hefei, 230601, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunyan Zhu, School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei, 230032, People’s Republic of China, Tel +86 0551-65161249, Email [email protected] Hong Li, Department of Pediatric Rehabilitation, Anhui Hospital Affiliated to the Pediatric Hospital of Fudan University, Hefei, People’s Republic of China, Email [email protected]
Background: Deficits in the adaptive allocation of attention are considered a feature associated with autism spectrum disorder (ASD). It remains unclear whether the attention of children with ASD can be modulated involuntarily by stimulus-driven processes. Visual processing is believed to initiate with topological perception; thus, we investigate the modulation of attention shifts in children with ASD by altering topological properties. This approach aims to elucidate the mechanism underlying atypical attentional capture in ASD.
Methods: Our study recruited 32 ASD children and 30 age-matched typically developing (TD) children. Employing an attentional capture paradigm, we systematically documented the eye movement of both ASD and TD participants in response to stimuli that included non-topological change (nTC), topological change (TC) and abrupt onset.
Results: The results suggest that the attention of children with ASD fails to be captured by TC and onset stimuli, and the degree of attentional bias towards TC is significantly correlated with their scores on clinical diagnostic scales.
Conclusion: Our results suggest that atypical attentional capture in ASD children is likely a result of impaired processing of topological perception. This finding not only enhances our understanding of their attentional atypicality but also provides insights for intervention practices to improve global processing.
Keywords: autism spectrum disorder, attention capture, bottom-up attention, topological perception, eye-tracking
Background
Autism Spectrum Disorder (ASD) is a complex neurodevelopmental condition characterized by enduring impairments in social communication and interaction, as well as the presence of restricted, repetitive patterns of behavior. Although not a core diagnostic criterion for ASD, atypical attention has been recognised as being associated with ASD since the condition was first described in detail by Kanner.1 Evidence linking atypical attention to ASD includes: (1) early and persistent attentional differences,2–5 (2) atypical attentional patterns in infants with ASD-sibling history,2,4 and (3) attentional impairments in Fragile X syndrome frequently co-occurs with ASD.6–8 This connection suggests that attentional deficits may constitute a core neurobiological mechanism underlying ASD-related behavioral manifestations.
Consistent with this finding, impaired attentional orienting to salient environmental cues represents a widely reported feature of ASD.9–11 This atypical attention profile may stem from involuntary mechanisms, which develop earlier than voluntary control (peaking in early adulthood).12–14 In typical development, involuntary attention is automatically drawn to intrinsic stimulus properties.15,16 A canonical example is the abrupt onset, wherein the sudden appearance of a novel object reliably captures attention.17–19 However, the exact mechanism of onset capture remains controversial.20–26 Limited evidence further suggests that children with ASD exhibit selective deficits in prioritizing novel stimuli.27,28 Greenaway and Plaisted27 argued that the failure of abrupt onsets to capture the attention of ASD children may be related to impaired processing of dynamic stimuli. Whereas, Xu et al29 recently reported that ASD children also fail to orient to topological changes and attributed this failure to impaired topological perception. Collectively, these findings raise the unresolved question of how atypical attentional capture in ASD can be reconciled.
Notably, these seemingly disparate findings on attentional atypicalities in ASD may share a unified explanation: Both dynamic processing deficit and topological perception impairment could stem from a more fundamental mechanism elucidated by Chen’s topological perception theory30–32––specifically, reduced sensitivity to topological changes in ASD children, which compromises their prioritization of novel stimuli including abrupt onsets.
Chen’s framework offers a formal account of why abrupt onset should be treated as topological change. According to the theory, a perceptual object is defined as the set of properties that remain invariant under smooth, continuous transformations (eg, stretching, twisting) that do not tear or glue the object’s structure. Within this definition, the sudden appearance of objects (ie, abrupt onsets) fundamentally represents a topological transformation––that is, the emergence of a new perceptual object. In the analysis of topology, an abrupt onset is a transformation from zero to one, which represents a change in topological property. Crucially, such transformation (abrupt onset) captures attention not through low-level features (eg, luminance) but via the spontaneous generation of a new perceptual object.33,34 Chen’s seminal work first rigorously formalized this concept by defining a perceptual object by its topological invariants.32,35 Consequently, abrupt onsets and topological changes are integrated into a single theoretical framework in which both constitute inherently salient stimuli that automatically capture attention.
Building on this framework, we hypothesize that children with ASD will exhibit significantly reduced attentional capture (longer fixation latencies, fewer first saccades) for stimuli with topological changes and abrupt onsets compared to typically developing children, but no group differences will emerge for non-topological changes. This deficit will correlate with higher ASD symptom severity, supporting impaired topological perception as a mechanism.
To empirically test this hypothesis, we employed a refined experimental paradigm grounded in the gap-overlap literature. The gap-overlap paradigm––widely utilized to investigate attentional disengagement in ASD36,37––has consistently revealed challenges in attentional shifting under overlap condition. Responsively, our study incorporated gap condition to mitigate this confound, enabling a cleaner investigation of attentional capture. Specifically, we implemented a change detection task designed to isolate the attentional effect of novel objects defined by topological properties, while systematically monitoring eye movement patterns throughout the visual search process in both ASD and typically developing children. This task represents a methodological advancement over the classic abrupt onset paradigm38 and gap paradigm, as it allows for direct comparison of eye movement indices between topological changes and the abrupt onsets––thereby directly probing the predicted differential attentional capture mechanisms.
Methods
Participants
All children with ASD were diagnosed by professional pediatric neurologists using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), and recruited from Anhui Hospital Affiliated to the Pediatric Hospital of Fudan University, China. Typically developing (TD) children were recruited from schools in the Hefei, Anhui province, China. Inclusion criteria for both groups of children were that they were aged between 4 years and 12 years, with normal or corrected-to-normal vision. Exclusion criteria for ASD group: (1) family history of monogenic disorders (to exclude genetic confounds), such as fragile X syndrome; (2) birth weight < 2000 g and gestational age < 32 weeks (to exclude developmental impairments of prematurity); and (3) current use of psychotropic medications (to exclude pharmacologic effects). Exclusion criterion for TD group: family history of ASD (to reduce the risk of undiagnosed ASD).
A total of 37 children with ASD and 33 typically developing (TD) children were recruited, with 32 ASD and 30 TD participants ultimately included in the study. Five children with ASD and three TD children were excluded from the formal analysis due to poor data quality (see detailed in the Analyses section). Consequently, the final analytic sample comprised 32 ASD children and 30 TD children. The ASD and TD children were well matched for gender and chronological age. Written informed consent was obtained from all parents or legal guardians for their children’s participation in this study. All procedures were conducted in compliance with the guidelines and regulations of the Declaration of Helsinki and were approved by the Ethics Committee of Anhui Hospital Affiliated to the Pediatric Hospital of Fudan University, China (approval number: EYLL-2023-026). Detailed characteristics of the participants are shown in Table 1.
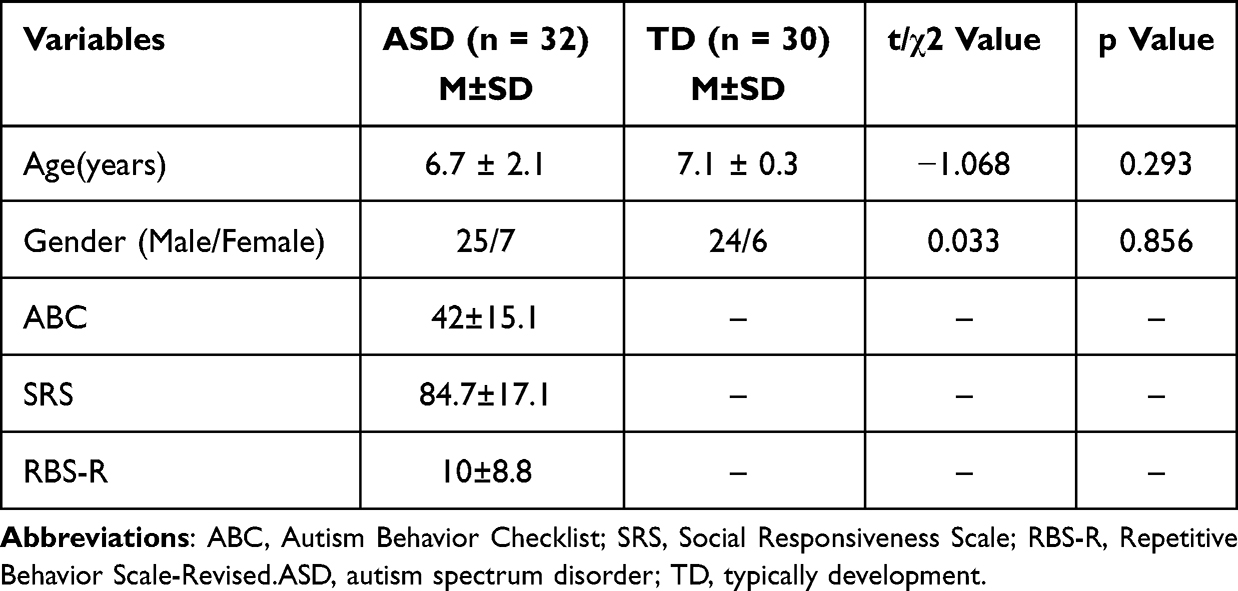 |
Table 1 Demographic Characterization Across Different Groups |
Apparatus and Stimuli
We used the iView X high-speed eye tracker, manufactured by the SensoMotoric Instruments (SMI Inc., German), to record the ocular movements of participants. The stimuli were displayed on a 30-inch monitor (refresh rate 250 Hz) with a resolution of 1680×960 pixels.
The stimuli consisted of cartoon images (2° × 2.6°) and geometric shapes (each 2° × 2°), as depicted in Figure S1. The role of cartoon images was to maintain the starting point of the children’s eye movements at the center of the screen. The place-holder frame consisted of five divisible circles. These circles were positioned at the eight-node position of the imaginary circle on the screen, whose center was positioned 8° from the center of the screen.
Procedure
Change Detection Task
To ensure the accuracy of the data collected, all participants were seated at a distance of approximately 65 cm from the screen where they completed all tasks and corrections using the SMI Experimental Centre software. Upon successful completion of the 5-point eye movement calibration, participants proceeded immediately to the change detection task. The task was composed of an equal number of test trials across three categories: non-topological change (nTC), topological change (TC), and abrupt onset change (Onset). Hence, the entire experimental session comprised 51 trials, consisting of 3 practice trials and 48 test trials. Each trial initiated with the display of a central cartoon image, which was then succeeded by the place-holder frame. Throughout the place-holder frame presentation, as soon as the participant’s gaze was stabilized within an of 1.8° radius surrounding the fixation point for a minimum of 500 milliseconds, the experimenter had to press the keyboard to terminate the current display, or the place-holder frame would automatically change to the target frame after 5 seconds. The target frame was presented for 2 seconds, during which subjects were asked to immediately look at the part that differs from the rest, the target, as shown in Figure 1.
 |
Figure 1 Stimuli and Procedure of Change Detection Task. |
Symptom Measures
The Chinese versions of the Autism Behavior Checklist (ABC),39 the Social Responsiveness Scale (SRS)40 and the Repetitive Behavior Scale-Revised (RBS-R)41 were utilized for the assessment of autistic traits in children, with the questionnaires being completed by parents or primary caregivers. The ABC is composed of 57 items across five subscales: sensory, social, motor, verbal communication, and social adaptation. The SRS, a 65-item questionnaire with 4-point Likert scale ranging from 1 (not true) to 4 (almost always true), is a well-established parent-report measure designed to evaluate the severity of social impairment in autistic children. The RBS-R is a 43-item parent-report instrument that utilizes a 4-point Likert scale to evaluate the frequency of various behaviors characteristic of autism. The RBS-R contains six subscales that assess different aspects of repetitive and restrictive behaviors: stereotypic behavior, self-injurious behavior, obsessive-compulsive behavior, ritualistic behavior, repetitive behavior and restricted interests. Higher scores on all of these scales indicate more severe symptoms.
Analyses
Prior to commencing data analysis, two regions of interest (ROIs) were specified: the central ROI and the target ROI. The central ROI was defined as a circular region with a radius of 1.8°, centered on the fixation point. The target ROI was configured as a trapezoidal region encircling the target item (see Figure 2). Participants were excluded from the analysis if over 50% of their trials were classified as invalid, either due to the absence of central fixation at trial initiation, or if they had errors in 50% or more of the trials.42 Five children with ASD and three TD children were excluded from the statistical analysis.
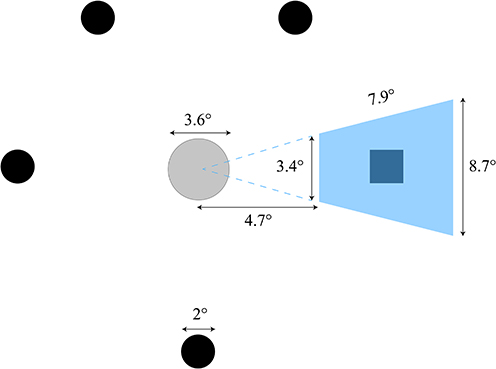 |
Figure 2 Two Regions of Interest (ROIs). |
We utilized four key eye tracking metrics––saccadic reaction time (SRT), visual search time (VS), first fixation dwell time (FFDT), and saccadic accuracy rates (AR)––as independent variables in our analysis. To evaluate the diagnostic classification potential of these behavioral features, linear discriminant analysis (LDA) was implemented. Post LDA, discriminant scores were calculated to quantify group differences. The classification performance of these discriminant scores in distinguishing children with ASD from TD peers was evaluated through receiver operating characteristic (ROC) curve analysis, employing non-parametric methods (Mann–Whitney U-test) to determine optimal sensitivity and specificity thresholds.
Eye-tracking data acquired from the SMI system were imported into the SPSS software (version 22.0; IBM Corp., USA). When the assumption of sphericity is violated, the Greenhouse-Geisser method is used to correct the ANOVA analysis.43 We performed mixed-effects ANOVAs to analyze the impact of stimulus type (nTC, TC, and Onset) and group (ASD and TD) on the saccadic indices (VS, SRT, FFDT and AR). Pairwise comparisons using the least significant difference (LSD) post hoc tests44 were conducted to identify significant group differences in responses to specific stimuli.
We also conducted Pearson correlation analysis to explore the associations between saccadic parameter (VS, SRT, FFDT and AR) and clinical rating scales (ABC, SRS and RBS-R). To account for multiple comparisons in Pearson correlation analysis, we applied False Discovery Rate (FDR) correction to control for the false-positive rate.45 GraphPad Prism software (version 9.5.0; GraphPad Prism Software Inc., USA) was used to generate all graphs.
Results
Visual Search Time (VS)
Visual search time is defined as the interval between target appearance and saccade landing within the target ROI. A repeated measures ANOVA was conducted to assess the effect of group (ASD, TD) and stimulus type (TC, nTC, Onset) on the VS There was a significant main effect for group [F (1, 60) = 36.347, p < 0.001, η2 = 0.377], suggesting that children with ASD exhibited a longer VS compared to TD children. Additionally, the interaction effect was also significant [F (2, 120) = 8.661, p < 0.01, η2 = 0.126]. Simple effects analysis revealed that ASD children showed no differential VS across stimuli. In contrast, the TD group exhibited significant differences in VS between TC and nTC (p < 0.001) as well as between nTC and Onset (p = 0.001), but not between TC and Onset. The mean values of eye-tracking measures (latency and accuracy) and the corresponding statistical values for the ASD and TD groups are shown in Table 2 and Figure 3.
 |
Table 2 Saccadic Indices of Change Detection Task in Different Groups |
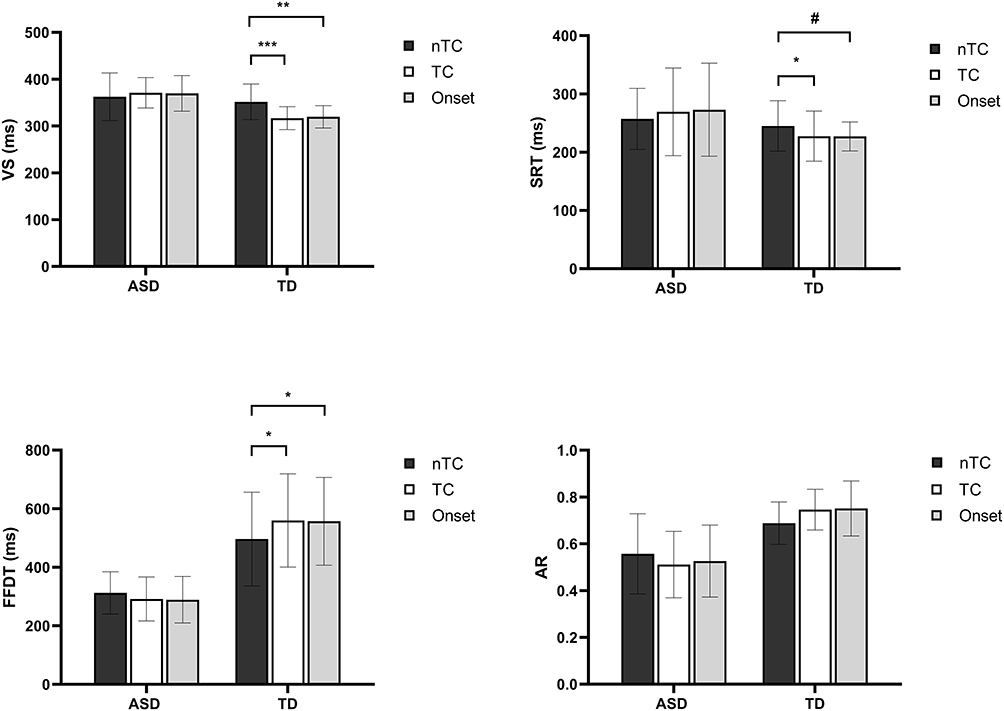 |
Figure 3 Saccadic Indices as a Function of Group and Stimulus Type; *p < 0.05, **p < 0.01, ***p < 0.001, #p = 0.056. |
Saccadic Reaction Time (SRT)
Saccadic reaction time was determined by the duration from the emergence of the target to the initiation of the first correct saccadic eye movement. Similarly, a repeated measures ANOVA was conducted to assess the effect of group (ASD, TD) and stimulus type (TC, nTC, Onset) on the SRT data. Analysis revealed that both the main effect of group [F (1, 60) = 6.907, p < 0.05, η2 = 0.103] and the interaction effect [F (2, 120) = 4.565, p < 0.05, η2 = 0.071] were significant. Post hoc analysis showed no significant effect of stimulus type on SRT was observed within the ASD group. However, TD children exhibited significant differences between TC and nTC (p = 0.043), marginal significance for nTC and Onset (p = 0.056), and no significant difference between TC and Onset, as demonstrated in Figure 3.
First Fixation Dwell Time (FFDT)
First fixation dwell time is measured by the time spent on the target ROI during the first gaze, which reflects the degree of attentional capture. We performed a repeated measures ANOVA to evaluate the effect of group (ASD, TD) and stimulus type (TC, nTC, Onset) on FFDT data. There was a main effect of group [F (1, 60) = 136.330, p < 0.0001, η2 = 0.694], indicating that the FFDT of children with ASD within the target ROI was shorter than that of TD children. In addition, the interaction effect was marginal significant [F (2, 120) = 2.961, p = 0.056, η2 = 0.047]. Analysis of simple effect indicated no stimulus-dependent variation in FFDT for ASD children. Nevertheless, TD children showed significant differences between TC and nTC (p = 0.018), and between nTC and Onset (p = 0.041), but not between TC and Onset, as depicted in Figure 3.
Saccadic Accuracy Rate (AR)
The ratio of saccades directly to the target was tested. A repeated measures ANOVA was employed to evaluate the AR data. The results indicated that both the main effect of group [F (1, 60) = 88.643, p < 0.0001, η2 = 0.596] and interaction effect were significant [F (2, 120) = 3.187, p = 0.045, η2 = 0.05]. Post hoc tests revealed no significant AR differences for both ASD and TD children across stimuli, as shown in Figure 3.
In summary, our eye-tracking analyses employing multiple metrics consistently demonstrated distinct response patterns between ASD and TD children across stimulus types (TC, nTC, Onset). TD children exhibited efficient processing of topological changes, as evidenced by their faster and more pronounced attentional capture by such stimuli. Conversely, children with ASD showed atypical attentional patterns, likely attributable to impaired topological perception that compromised their ability to accurately and rapidly detect topological changes, thereby resulting in divergent eye-movement profiles compared to their TD peers.
The results for AR in controls were not fully consistent with the latency findings, which may reflect weaker topological effects for accuracy vs latency. This dissociation may arise because topological effects primarily influence latency, rather than decision accuracy. Rapid early topological changes might not guarantee high decision accuracy. Consequently, we did not include AR as a potential variable in the subsequent discriminant analysis.
Receiver Operating Characteristic Curve (ROC)
Although not our primary aim, eye-tracking metrics show potential utility as screening tools. Critically, significant group differences emerged between TC and nTC across key saccadic indices (SRT, VS, and FFDT). We conducted discriminant analysis using the group-differentiated saccadic metrics (SRTtc-ntc, VStc-ntc, and FFDTtc-ntc). The overall accuracy of the discriminant model is 75.8%, and the discriminant score is obtained according to the following formula:

Figure 4 shows the ROC curve of the discriminant score between ASD and TD children. The area under the curve (AUC) of the ROC analysis in ASD vs TD was 0.803 (p < 0.001, 95% CI [0.694, 0.914]), indicating that discriminant score derived from saccadic indices in the change detection task enable moderate accuracy in differentiating children with ASD from TD peers. The Youden index identified an optimal cut-off value of –0.014, yielding 78.1% sensitivity and 76.7% specificity, as shown in see Figure 4. Notably, while these LDA/ROC models show promising diagnostic potential, their clinical applicability requires validation in larger, independent cohorts.
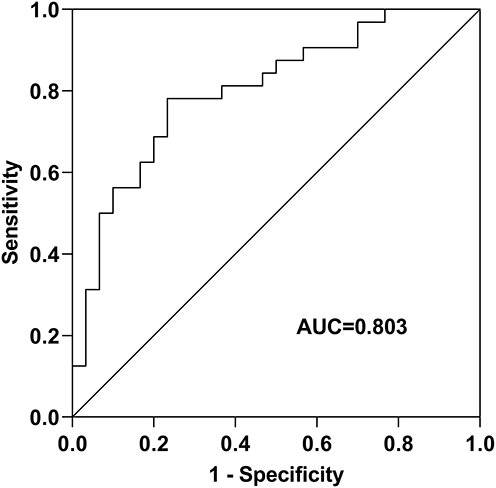 |
Figure 4 Receiver Operating Characteristic Curve. |
Correlation Analysis
Our findings suggest that topological changes fail to capture attention in children with ASD, indicating a potential association between this perceptual deficit and their clinical symptoms. This impairment in early-stage topological perception may progressively disrupt higher-level cognition functions in ASD, particularly social communication and repetitive behaviors. Quantitative analyses corroborate this relationship: (1) Pearson correlation revealed that the absolute difference in FFDT between the TC and Onset conditions was positively associated with the total score on the RBS-R (r = 0.443, p = 0.033), and (2) AR under Onset condition were significantly correlated with total SRS score (r = –0.557, p = 0.003), as demonstrated in Figure 5 and Table 3.
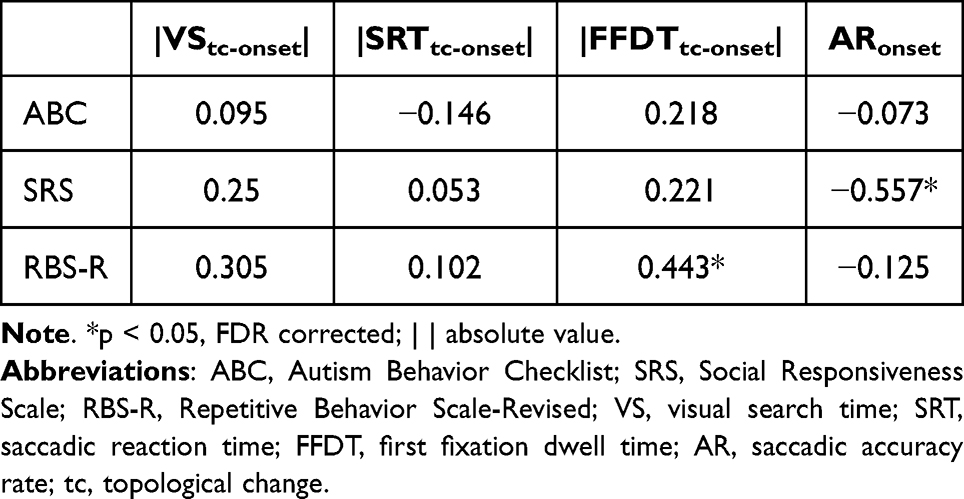 |
Table 3 Pearson Correlation Between Saccadic Indices and Clinical Scales |
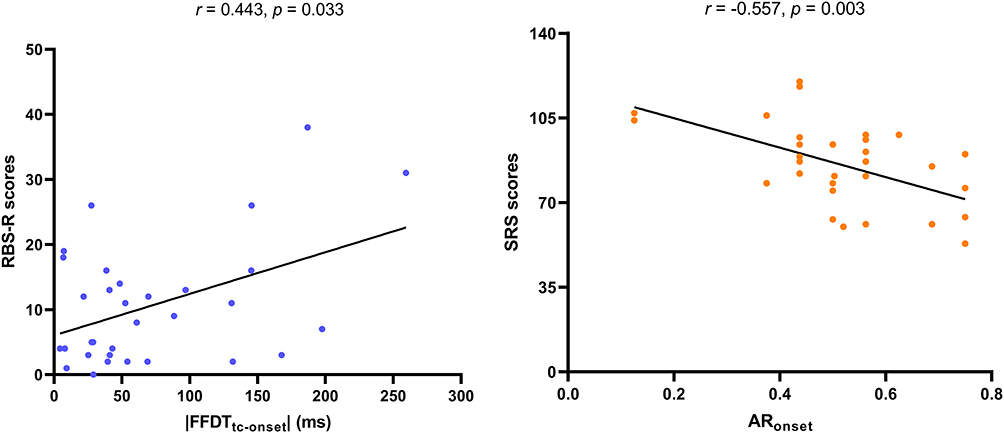 |
Figure 5 Pearson Correlations Between Saccadic Indices and Clinical Scales. |
Discussion
Several key findings emerged from this study. Firstly, children with ASD demonstrated a diminished capacity for attentional capture by abrupt onsets, aligning with previous studies.27,28 Secondly, these children also exhibited a reduced ability to allocate attention in response to topological changes, echoing recent results from Xu et al.29 Thirdly, the extent of attentional capture impairment by topological changes, including abrupt onsets, correlates with the severity of symptoms (repetitive behavior) in children with ASD. Collectively, our findings suggest that attention deficits in children with ASD may stem from abnormalities in early topological processing. Topological perception deficits may underlie both attentional and social phenotypes in ASD.
Our study explored the nexus between visual attention deficits at the lower levels and the impairments in higher-order social and communicative skills, a relationship underscored by previous research.46,47 We specifically investigated the correlation between attentional capture prompted by topological changes in children with ASD and the clinical symptoms quantified through the ABC, SRS, and RBS-R scales. Deficits in attention to topological changes/abrupt onsets may reduce the capture of social cues such as facial expressions, which might be attributed to impaired holistic processing (eg, perceiving faces as unified “perceptual objects”) forces an over-reliance on feature-based strategies (eg, mouth-focused gaze). This topological explanation consistent with weak central coherence accounts48,49 and predicts downstream deficits in joint attention. On another level, existing research indicates that attention deficits and repetitive behaviors share a common underlying impairment.50 In individuals with ASD, compromised topological perception leads to a cognitive style characterized by focal attention to local features. This cognitive style may constitute the foundation for rigid routines, restricted interests, and repetitive behaviors.51 Reduced sensitivities to environmental changes––such as alterations in topological structure––may drive ASD individuals to preferentially engage with highly familiar, non-novel stimuli (eg, repetitive patterns), thereby reinforcing stereotyped behaviors. This ultimately results in cognitive inflexibility among individuals with ASD.
Although there is a lack of direct neurocognitive evidence, we propose that these behavioral deficits may stem from impaired subcortical pathways in ASD. Subcortical pathways mediate rapid sensory processing52 and motor regulation.53 The evidence supporting subcortical pathway impairment primarily stems from the following neuroimaging studies: (1) Structural and functional abnormalities in the superior colliculus-pulvinar-amygdala pathway have been identified in individuals with ASD, characterized by compromised structural integrity54–56 and aberrant functional connectivity.55 (2) Animal models (valproic acid induced ASD mice) similarly exhibit synaptic connectivity deficits in this pathway, demonstrating cross-species consistency.57,58 Such structure-function coupling abnormalities may underlie the atypical gaze patterns observed in ASD (eg, preferential attention to local features). Notably, the subcortical pathway also serves as a critical circuit for topological property processing, as topological features selectively activate the superior colliculus56,59,60 and anterior temporal lobe.35,61 Therefore, when information processing within these pathways is disrupted, children with autism show diminished attentional capture by changes in topological properties and display stereotypic behaviors. However, direct causal links between impaired topological perception and clinical symptoms require further neuroimaging and electrophysiological studies.
While the majority of research supports the concept of bottom-up attention, there is still considerable debate regarding the specific attributes or attribute changes that involuntarily command attention. The theory of attentional capture by the abrupt onset of new physical stimuli is widely documented.62 However, this hypothesis is largely congruent with object-based attention studies that have not yet provided a precise definition of the perceptual object. Chen’s topological theory of perception offers a clear delineation, positing that the emergence of new objects is characterized by a transition from “nothing” to “something”, which is indicative of a change in topological properties.32 This representation of a new object necessitates attentional resources for processing, leading to a shift or reallocation of attention. In this study, we compared the search efficiency of topological changes and abrupt onsets between ASD and TD children, and discovered that both stimuli exert equivalent effects on attention. Besides, Pearson analysis revealed a significant positive correlation between the TC - nTC and Onset – nTC (see Figure S2 and Figure S3), which supports our hypothesis that both topological changes and onsets represent perceptual object manifestations based on topology.
Our study provides novel insights for clinical intervention. We propose a phased intervention approach for ASD children: initially implementing basic figure perception training that systematically reinforces global perceptual processing,e.g., perceptual organization tasks63 to ameliorate their excessive focus on local features. The intervention could subsequently be advanced by strengthening perceptual biases within social contexts to improve social functioning. However, the realization of this intervention model requires both empirical validation through further research and interdisciplinary collaboration between researchers and clinicians.
Limitations
This study, while illuminating, also has several limitations. Firstly, although efforts were made to match ASD and TD children on age and gender, nonverbal IQ may act as a confounding factor. Future studies should control for nonverbal IQ (eg, WISC-V or Raven’s Progressive Matrices), as these may covary with topological perception yet reflect distinct mechanisms. Secondly, the participants in this study were primarily Han Chinese from mainland China. Future research with larger and more diverse samples across different cultural backgrounds (eg, Westerns) is needed to validate and generalize these findings. Thirdly, given the profound heterogeneity of ASD, it remains unclear whether impairments in topological perception are a specific feature of the disorder. Future studies should incorporate additional control groups, such as individuals with Asperger syndrome, idiopathic language development disorder, and intellectual disability, to ascertain the specificity of the current study’s outcomes.
Conclusion
Despite some limitations, we identify topological perception deficits may be a transdiagnostic marker linking low-level (attentional capture) and high-level (social/behavioral) ASD features. Targeting these deficits through perceptual training may improve both attentional biases and downstream social outcomes. Future work should clarify their neurocognitive mechanisms and therapeutic potential.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from Chunyan Zhu on reasonable request.
Ethics Approval and Consent to Participate
Ethics approval was obtained from the Ethics Committee of Anhui Hospital Affiliated to the Pediatric Hospital of Fudan University, China (approval number: EYLL-2023-026). All procedures were conducted in accordance with the Declaration of Helsinki. All participants, both children and parents, signed informed consent after receiving a full description of the study, an explanation of its purpose, and information about the confidentiality of the data.
Funding
This work was supported by the STI2030-Major Projects (2021ZD0203803), the National Natural Science Foundation of China (32271134, 91432301), Anhui Province Natural Science Foundation (2408085MC081) and Anhui Provincial University Collaborative Innovation Program (GXXY-2021-003).
Disclosure
The authors declare that they have no competing interests.
References
1. Kanner L. Autistic disturbances of affective contact. Nervous Child. 1943;2(3):217–250.
2. Elsabbagh M, Volein A, Holmboe K, et al. Visual orienting in the early broader autism phenotype: disengagement and facilitation. J Child Psychol Psychiatr. 2009;50(5):637–642. doi:10.1111/j.1469-7610.2008.02051.x
3. Osterling JA, Dawson G, Munson JA. Early recognition of 1-year-old infants with autism spectrum disorder versus mental retardation. Dev Psychopathol. 2002;14(2):239–251. doi:10.1017/s0954579402002031
4. Zwaigenbaum L, Bryson S, Rogers T, Roberts W, Brian J, Szatmari P. Behavioral manifestations of autism in the first year of life. Int J Dev Neurosci. 2005;23(2–3):143–152. doi:10.1016/j.ijdevneu.2004.05.001
5. Allen G, Courchesne E. Attention function and dysfunction in autism. Front Biosci. 2001;6:D105–19. doi:10.2741/allen
6. Cornish K, Cole V, Longhi E, Karmiloff-Smith A, Scerif G. Does attention constrain developmental trajectories in fragile x syndrome? A 3-year prospective longitudinal study. Am J Intellect Dev Disabil. 2012;117(2):103–120. doi:10.1352/1944-7558-117.2.103
7. Roberts JE, Hatton DD, Long AC, Anello V, Colombo J. Visual attention and autistic behavior in infants with fragile X syndrome. J Autism Dev Disord. 2012;42(6):937–946. doi:10.1007/s10803-011-1316-8
8. Scerif G, Longhi E, Cole V, Karmiloff-Smith A, Cornish K. Attention across modalities as a longitudinal predictor of early outcomes: the case of fragile X syndrome. J Child Psychol Psychiatr. 2012;53(6):641–650. doi:10.1111/j.1469-7610.2011.02515.x
9. Landry O, Mitchell PL, Burack JA. Orienting of visual attention among persons with autism spectrum disorders: reading versus responding to symbolic cues. J Child Psychology Psychiatry. 2009;50(7):862–870. doi:10.1111/j.1469-7610.2008.02049.x
10. Murphy ER, Norr M, Strang JF, Kenworthy L, Gaillard WD, Vaidya CJ. Neural basis of visual attentional orienting in childhood autism spectrum disorders. J Autism Dev Disord. 2017;47(1):58–67. doi:10.1007/s10803-016-2928-9
11. Renner P, Grofer Klinger L, Klinger MR. Exogenous and endogenous attention orienting in autism spectrum disorders. Child Neuropsychol. 2006;12(4–5):361–382. doi:10.1080/09297040600770753
12. Enns JT, Brodeur DA. A developmental study of covert orienting to peripheral visual cues. J Exp Child Psychol. 1989;48(2):171–189. doi:10.1016/0022-0965(89)90001-5
13. Pearson DA, Lane DM. Visual attention movements: a developmental study. Child Dev. 1990;61(6):1779–1795. doi:10.2307/1130837
14. Scheerer NE, Birmingham E, Boucher TQ, Iarocci G. Attention capture by trains and faces in children with and without autism spectrum disorder. PLoS One. 2021;16(6):e0250763. doi:10.1371/journal.pone.0250763
15. Brosch T, Pourtois G, Sander D, Vuilleumier P. Additive effects of emotional, endogenous, and exogenous attention: behavioral and electrophysiological evidence. Neuropsychologia. 2011;49(7):1779–1787. doi:10.1016/j.neuropsychologia.2011.02.056
16. Theeuwes J. Visual selective attention: a theoretical analysis. Acta psychol. 1993;83(2):93–154. doi:10.1016/0001-6918(93)90042-p
17. Franconeri SL, Hollingworth A, Simons DJ. Do new objects capture attention? Psychol Sci. 2005;16(4):275–281. doi:10.1111/j.0956-7976.2005.01528.x
18. Lamy D, Egeth HE. Attentional capture in singleton-detection and feature-search modes. J Exp Psychol Hum Percept Perform. 2003;29(5):1003–1020. doi:10.1037/0096-1523.29.5.1003
19. Sunny MM, von Mühlenen A. Attention capture by abrupt onsets: re-visiting the priority tag model. Front Psychol. 2013;4:958. doi:10.3389/fpsyg.2013.00958
20. Jonides J, Yantis S. Uniqueness of abrupt visual onset in capturing attention. Percept Psychophys. 1988;43(4):346–354. doi:10.3758/bf03208805
21. Hillstrom AP, Yantis S. Visual motion and attentional capture. Percept Psychophys. 1994;55(4):399–411. doi:10.3758/bf03205298
22. Donk M, Theeuwes J. Prioritizing selection of new elements: bottom-up versus top-down control. Percept Psychophys. 2003;65(8):1231–1242. doi:10.3758/bf03194848
23. Hunt AR, von Mühlenen A, Kingstone A. The time course of attentional and oculomotor capture reveals a common cause. J Exp Psychol Hum Percept Perform. 2007;33(2):271–284. doi:10.1037/0096-1523.33.2.271
24. Schreij D, Theeuwes J, Olivers CN. Abrupt onsets capture attention independent of top-down control settings II: additivity is no evidence for filtering. Atten Percept Psychophys. 2010;72(3):672–682. doi:10.3758/APP.72.3.672
25. Becker SI, Lewis AJ. Oculomotor capture by irrelevant onsets with and without color contrast. Ann N Y Acad Sci. 2015;1339:60–71. doi:10.1111/nyas.12685
26. Schmid RR, Ansorge U. Novel tests of capture by irrelevant abrupt onsets: no evidence for a mediating role of search task difficulty during color search. Atten Percept Psychophys. 2023;85(3):667–684. doi:10.3758/s13414-022-02623-y
27. Keehn B, Joseph RM. Impaired prioritization of novel onset stimuli in autism spectrum disorder. J Child Psychol Psychiatr. 2008;49(12):1296–1303. doi:10.1111/j.1469-7610.2008.01937.x
28. Greenaway R, Plaisted K. Top-down attentional modulation in autistic spectrum disorders is stimulus-specific. Psychol Sci. 2005;16(12):987–994. doi:10.1111/j.1467-9280.2005.01648.x
29. Xu H, Xi H, Duan T, et al. The impairment attention capture by topological change in children with autism spectrum disorder. Prog Biochem Biophys. doi:10.16476/j.pibb.2024.0160
30. Chen L. Topological structure in visual perception. Science. 1982;218(4573):699–700. doi:10.1126/science.7134969
31. Chen L, Zhang S, Srinivasan MV. Global perception in small brains: topological pattern recognition in honey bees. Proc Natl Acad Sci U S A. 2003;100(11):6884–6889. doi:10.1073/pnas.0732090100
32. Chen L. The topological approach to perceptual organization. Vis Cogn. 2005;12(4):553–637. doi:10.1080/13506280444000256
33. Davoli CC, Suszko JW, Abrams RA. New objects can capture attention without a unique luminance transient. Psychon Bull Rev. 2007;14(2):338–343. doi:10.3758/bf03194074
34. Yantis S, Hillstrom AP. Stimulus-driven attentional capture: evidence from equiluminant visual objects. J Exp Psychol Hum Percept Perform. 1994;20(1):95–107. doi:10.1037//0096-1523.20.1.95
35. Zhou K, Luo H, Zhou T, Zhuo Y, Chen L. Topological change disturbs object continuity in attentive tracking. Proc Natl Acad Sci U S A. 2010;107(50):21920–21924. doi:10.1073/pnas.1010919108
36. Keehn B, Kadlaskar G, Bergmann S, McNally Keehn R, Francis A. Attentional disengagement and the locus coeruleus - norepinephrine system in children with autism spectrum disorder. Front Integr Neurosci. 2021;15:716447. doi:10.3389/fnint.2021.716447
37. Sacrey LA, Armstrong VL, Bryson SE, Zwaigenbaum L. Impairments to visual disengagement in autism spectrum disorder: a review of experimental studies from infancy to adulthood. Neurosci Biobehav Rev. 2014;47:559–577. doi:10.1016/j.neubiorev.2014.10.011
38. Yantis S, Jonides J. Abrupt visual onsets and selective attention: evidence from visual search. J Exp Psychol Hum Percept Perform. 1984;10(5):601–621. doi:10.1037//0096-1523.10.5.601
39. Kat S, Xu L, Guo Y, et al. Reliability and validity of the simplified chinese version of the aberrant behavior checklist in chinese autism population. Front Psychiatry. 2020;11:545445. doi:10.3389/fpsyt.2020.545445
40. Frazier TW, Youngstrom EA, Embacher R, et al. Demographic and clinical correlates of autism symptom domains and autism spectrum diagnosis. Autism. 2014;18(5):571–582. doi:10.1177/1362361313481506
41. Mirenda P, Smith IM, Vaillancourt T, et al. Validating the repetitive behavior scale-revised in young children with autism spectrum disorder. J Autism Dev Disord. 2010;40(12):1521–1530. doi:10.1007/s10803-010-1012-0
42. DiCriscio AS, Miller SJ, Hanna EK, et al. Brief report: cognitive control of social and nonsocial visual attention in autism. J Autism Dev Disord. 2016;46(8):2797–2805. doi:10.1007/s10803-016-2804-7
43. Blanca MJ, Arnau J, García-Castro FJ, Alarcón R, Bono R. Repeated measures ANOVA and adjusted F-tests when sphericity is violated: which procedure is best? Front psychol. 2023;14:1192453. doi:10.3389/fpsyg.2023.1192453
44. Harrison AJ, Slane MM. Examining how types of object distractors distinctly compete for facial attention in autism spectrum disorder using eye tracking. J Autism Dev Disord. 2020;50(3):924–934. doi:10.1007/s10803-019-04315-3
45. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B Methodol. 1995;57(1):289–300. doi:10.1111/j.2517-6161.1995.tb02031.x
46. Elsabbagh M, Holmboe K, Gliga T, et al. Social and attention factors during infancy and the later emergence of autism characteristics. Prog Brain Res. 2011;189:195–207. doi:10.1016/B978-0-444-53884-0.00025-7
47. Mottron L, Dawson M, Soulières I, Hubert B, Burack J. Enhanced perceptual functioning in autism: an update, and eight principles of autistic perception. J Autism Dev Disord. 2006;36(1):27–43. doi:10.1007/s10803-005-0040-7
48. Burnette CP, Mundy PC, Meyer JA, Sutton SK, Vaughan AE, Charak D. Weak central coherence and its relations to theory of mind and anxiety in autism. J Autism Dev Disord. 2005;35(1):63–73. doi:10.1007/s10803-004-1035-5
49. Frith U, Happé F. Autism: beyond “theory of mind”. Cognition. 1994;50(1–3):115–132. doi:10.1016/0010-0277(94)90024-8
50. Ravizza SM, Solomon M, Ivry RB, Carter CS. Restricted and repetitive behaviors in autism spectrum disorders: the relationship of attention and motor deficits. Dev psychopathol. 2013;25(3):773–784. doi:10.1017/S0954579413000163
51. Chen YH, Rodgers J, McConachie H. Restricted and repetitive behaviours, sensory processing and cognitive style in children with autism spectrum disorders. J Autism Dev Disord. 2009;39(4):635–642. doi:10.1007/s10803-008-0663-6
52. Phillips JM, Kambi NA, Saalmann YB. A subcortical pathway for rapid, goal-driven, attentional filtering. Trends Neurosci. 2016;39(2):49–51. doi:10.1016/j.tins.2015.12.003
53. Rae CL, Hughes LE, Anderson MC, Rowe JB. The prefrontal cortex achieves inhibitory control by facilitating subcortical motor pathway connectivity. J Neurosci. 2015;35(2):786–794. doi:10.1523/JNEUROSCI.3093-13.2015
54. Hu Y, Chen Z, Huang L, et al. A translational study on looming-evoked defensive response and the underlying subcortical pathway in autism. Sci Rep. 2017;7(1):14755. doi:10.1038/s41598-017-15349-x
55. Huang Y, Vangel M, Chen H, et al. The impaired subcortical pathway from superior colliculus to the amygdala in boys with autism Spectrum disorder. Front Integr Neurosci. 2022;16:666439. doi:10.3389/fnint.2022.666439
56. Zuo C, Wang D, Tao F, Wang Y. Changes in the development of subcortical structures in autism spectrum disorder. Neuroreport. 2019;30(16):1062–1067. doi:10.1097/WNR.0000000000001300
57. Contestabile A, Kojovic N, Casarotto G, et al. Translational research approach to social orienting deficits in autism: the role of superior colliculus-ventral tegmental pathway. Mol Psychiatry. 2025;30(8):3729–3739. doi:10.1038/s41380-025-02962-w
58. Meng Q, Huang Y, Cui D, et al. The dissociations of visual processing of “hole” and “no-hole” stimuli: an functional magnetic resonance imaging study. Brain Behav. 2018;8(5):e00979. doi:10.1002/brb3.979
59. Huang Y, Li L, Dong K, et al. Topological shape changes weaken the innate defensive response to visual threat in mice. Neurosci Bull. 2020;36(4):427–431. doi:10.1007/s12264-019-00454-w
60. Wang W, Zhou T, Chen L, Huang Y. A subcortical magnocellular pathway is responsible for the fast processing of topological properties of objects: a transcranial magnetic stimulation study. Hum. Brain Mapp. 2023;44(4):1617–1628. doi:10.1002/hbm.26162
61. Zhuo Y, Zhou TG, Rao HY, et al. Contributions of the visual ventral pathway to long-range apparent motion. Science. 2003;299(5605):417–420. doi:10.1126/science.1077091
62. Rauschenberger R, Yantis S. Attentional capture by globally defined objects. Percept Psychophys. 2001;63(7):1250–1261. doi:10.3758/bf03194538
63. Bian Z, Wang B, Wu X, Wang K, Jiang Y. Development and validation of paradigms based on the global-first topological approach for alzheimer’s disease severity staging. Neuropsychiatr Dis Treat. 2024;20:1225–1234. doi:10.2147/NDT.S460421
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.