Back to Journals » International Journal of General Medicine » Volume 15
Red Cell Alloimmunization and Autoimmunization Among Sickle Cell Disease and Thalassemia Patients in Jazan Province, Saudi Arabia
Authors Halawani AJ ![]() , Mobarki AA, Arjan AH, Saboor M
, Mobarki AA, Arjan AH, Saboor M ![]() , Hamali HA
, Hamali HA ![]() , Dobie G
, Dobie G ![]() , Alsharif KF
, Alsharif KF ![]()
Received 28 January 2022
Accepted for publication 6 April 2022
Published 15 April 2022 Volume 2022:15 Pages 4093—4100
DOI https://doi.org/10.2147/IJGM.S360320
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Amr J Halawani,1 Abdullah A Mobarki,2 Ali H Arjan,3 Muhammad Saboor,2 Hassan A Hamali,2 Gasim Dobie,2 Khalaf F Alsharif4
1Department of Laboratory Medicine, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia; 2Department of Medical Laboratory Technology, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 3Department of Laboratory and Blood Bank, King Fahad Central Hospital, Ministry of Health, Jazan, Saudi Arabia; 4Department of Clinical Laboratory Science, College of Applied Medical Sciences, Taif University, Taif, Saudi Arabia
Correspondence: Amr J Halawani, Department of Laboratory Medicine, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Purpose: Sickle cell disease (SCD) and thalassemia are common inherited blood disorders in Saudi Arabia, especially in Jazan Province. Patients with these disorders require multiple blood transfusions, which may lead to alloimmunization because of mismatched blood group antigens. In this study, we examined the alloimmunization and autoimmunization rates in patients with SCD and thalassemia together with the involved antibodies.
Patients and Methods: A cross-sectional study was conducted to review the transfusion history records of patients with SCD and thalassemia at Prince Mohammed bin Nasser Hospital, Jazan Province, Saudi Arabia.
Results: Four-hundred thirty-eight patients (385 with SCD, 52 with β-thalassemia, and 1 with α-thalassemia) were received leukoreduced red cell transfusions. The alloimmunization and autoimmunization rates in patients with SCD were 12.98% and 0.52%, respectively. In patients with thalassemia, the alloimmunization and autoimmunization rates were 13.21% and 3.77%, respectively. The most prevalent antibodies in the study population were anti-E (17.19%) and anti-K (14.06%).
Conclusion: The alloimmunization and autoimmunization rates were determined in patients with SCD and thalassemia in Jazan Province, Saudi Arabia. The results highlight the need for extended phenotyping to include ABO, RH (D, C, c, E, e), K, Fya, Fyb, Jka and Jkb antigens in the screening panel. This will benefit patients to ensure better transfusion practices.
Keywords: red cell alloimmunization, sickle cell disease, thalassemia, autoimmunization
Introduction
Sickle cell disease (SCD) is an autosomal recessive blood disorder in which normal hemoglobin A is replaced by sickle hemoglobin because of a single point mutation in the hemoglobin subunit β gene.1 The incidence of SCD is highest in sub-Saharan Africa, the Middle East, and India.2 High frequencies of SCD have been reported in the Eastern and Southwestern Provinces of Saudi Arabia.3,4
In recent decades, substantial progress in the management of SCD has been achieved through early diagnosis and good medical care. However, acute and chronic complications of SCD, which largely contribute to hemolysis and vaso-occlusive crises, remain life-threatening.5 Red blood cell (RBC) transfusion remains the cornerstone of SCD management. In addition to the correction of anemia, blood transfusion greatly reduces inflammation and endothelial injuries in patients with SCD.6
Thalassemia is one of the most widespread inherited “monogenic” hemoglobin disorders caused by the decreased production or absence of one or more globin chains.7 The clinical severity of thalassemia varies depending on the number of affected α and/or β genes. Patients with thalassemia major require frequent blood transfusions. Conversely, many thalassemia carriers remain asymptomatic.8
Thalassemia is extremely prevalent in Mediterranean and Middle Eastern countries, including Saudi Arabia.9,10 The frequency of β-thalassemia per 1000 individuals in Saudi Arabia is 13.6%, with disease and carrier rates of 0.7% and 12.9%, respectively.11 Similar to SCD, β-thalassemia was found to be most prevalent in Jazan and the Eastern Province in a national premarital screening program.12
Alloimmunization occurs when patients receive incompatible blood units, which results in exposure to foreign antigens and the subsequent production of antibodies.13 These antibodies attach to donor RBCs, leading to their destruction in the patient’s circulation. RBC alloimmunization is a major complication in patients with SCD and can result in delayed hemolytic transfusion reactions (HTR) and hyperhemolysis.14 The alloimmunization risk is associated with several factors, including patient age, age at which transfusion was started, number of blood transfusions received, transfusion of non-leukodepleted packed RBCs, transfusion of old blood, and patient sex (females have higher rates than males).15–18 The alloimmunization rate among transfusion-dependent patients also varies based on the population.
The alloimmunization rate in patients with SCD ranges between 20% and 30%; however, this high rate was considerably reduced when blood from racially homogenous populations was utilized for transfusion.19–21 The rate of SCD alloimmunization in Arabian Gulf countries varies from 13.7% to 65.5%.22–25 The reported alloimmunization rates in patients with thalassemia were 33.57% in Saudi Arabia,24 20% in Oman,25 and 30% in Kuwait.26
Considering these findings, the present study assessed the prevalence of alloimmunization and autoimmunization in patients with SCD and thalassemia in Jazan Province, Saudi Arabia. Furthermore, the prevalence of the involved antibodies were determined.
Materials and Methods
Patients
A cross-sectional study was conducted by reviewing the transfusion history records between November 2014 to March 2017 from Prince Mohammed bin Nasser Hospital (PMBNH) in Jazan Province, Saudi Arabia. A total of 438 patients, including 385 with SCD, 52 with β-thalassemia major, and 1 with α-thalassemia were included in the study. All patients received leukoreduced red cell transfusions.
The patients were categorized into two groups: SCD (n = 385) and thalassemia (n = 53, among whom which 52 had β-thalassemia major and 1 had α-thalassemia). Ethical approval was obtained from the Institutional Review Board of Jazan Hospital, Ministry of Health, Kingdom of Saudi Arabia (No. 2015).
Transfusion Policy
The patients’ samples were screened for the following antigens: A, B, O, AB, D, C, c, E, e, and K. These antigens were investigated using ID System gel cards (Bio-Rad, Dreieich, Germany). The samples were tested using DiaClon ABO/D + Reverse Grouping and DiaClon Rh Subgroups + K gel cards (Bio-Rad, Dreieich, Germany). Antibody screening and identification were performed. Cross-matching was performed and antigen-negative matching blood units were provided for the recipients.
Statistical Analysis
The alloimmunization and autoimmunization rates were calculated as percentages. P-values were calculated using a Z-Test for two population proportions to compare differences in the alloimmunization rates in the present study with those reported in other Arabian countries.27 P-values <0.05 and <0.01 indicated significant and highly significant differences, respectively.
Results
In total, 438 transfusion-dependent patients (227 men and 211 women) admitted to PMBNH to receive blood transfusions were screened for the presence of irregular antibodies. The sociodemographic characteristic of these patients are presented in Table 1. All the patients were Saudi nationals, and they resided in Jazan Province. The ages of the SCD patients ranged from 7 to 67 years with the majority of these patients with the 25–45 year age group with 60.26%. Regarding the thalassemic patients, the ages ranged from 10 to 51 years, in which the most common for the 17–24 years age group at 52.84%.
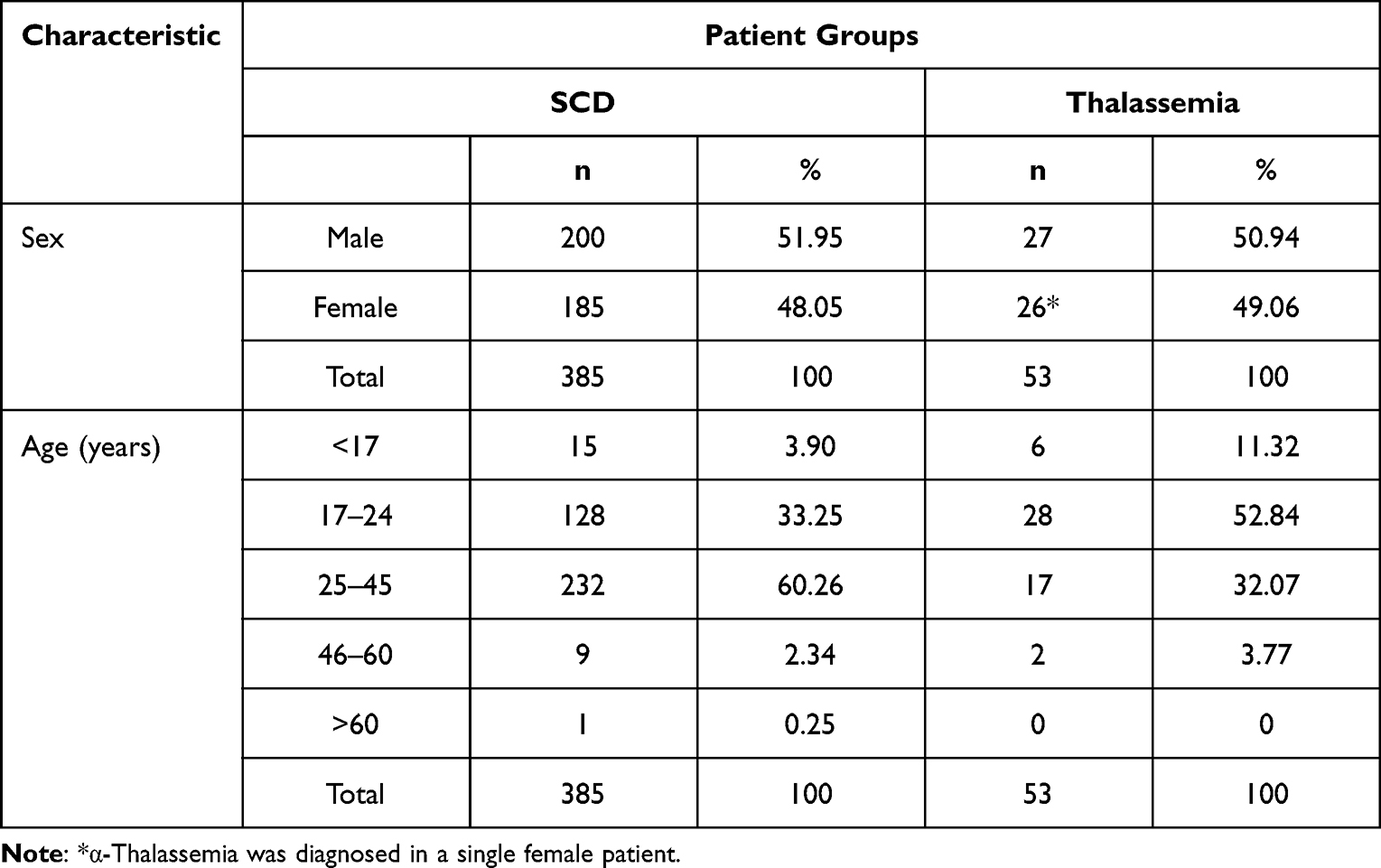 |
Table 1 Sociodemographic Characteristics of the Participants |
Among the 438 patients, 57 patients had positive antibody screening test results. The results of the comparative analysis of SCD and thalassemia between the present study and published data from Saudi Arabia and other Arabian Gulf countries are presented in Tables 2 and 3, respectively. The alloimmunization rate in patients with SCD was 12.98% and in those with thalassemia was 13.21%. The autoimmunization rates in patients with SCD and thalassemia were 0.52% and 3.77%, respectively.
 |
Table 2 Rates of SCD Alloimmunization in the Present Study and Studies Conducted in Saudi Arabia and Other Arabian Gulf Countries |
 |
Table 3 Rates of Thalassemia Alloimmunization in the Present Study and Those Conducted in Saudi Arabia and Other Arabian Gulf Countries |
Table 4 presents the frequencies of antibodies in patients with SCD and thalassemia. The most prevalent antibody in patients with SCD was anti-E (n = 11; 19.64%), followed by anti-K (n = 8; 14.28%). The frequencies of developed antibodies in seven patients with thalassemia are also presented in Table 4. Anti-D and anti-Jka were detected in two patients each (25%). Regarding the KEL blood group system, anti-K and anti-Kpa were observed in one patient each (12.50%). In addition, unidentified autoantibodies were reported in two patients (25%).
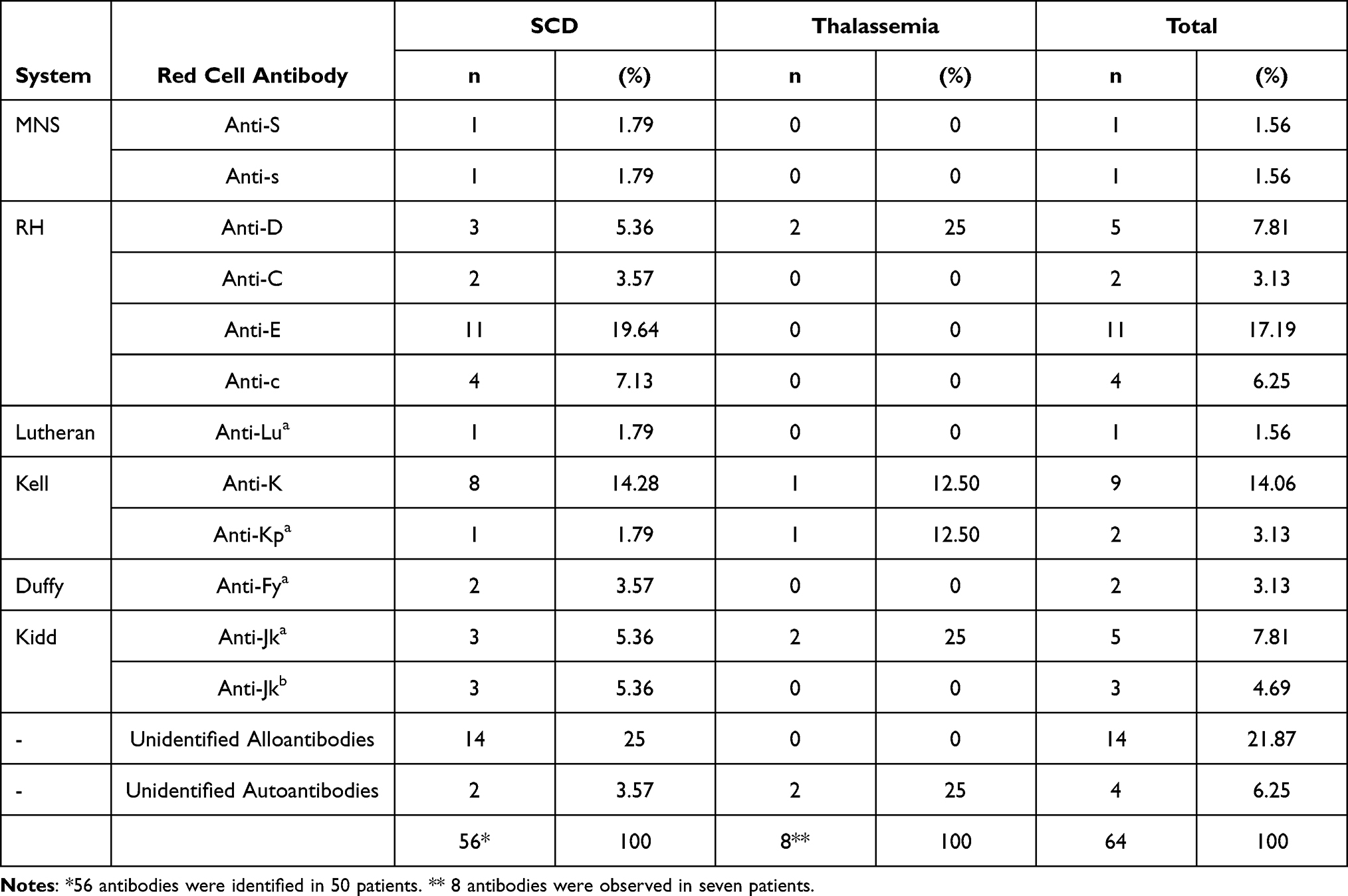 |
Table 4 Prevalence of Antibodies in Patients with SCD and Thalassemia |
The frequencies of A, B, AB, O, D, C, c, E, e, and K antigens among all patients are illustrated in Table 5. Concerning the ABO blood group system, the occurrence of the antigens was as follows: A, 126 (28.77%); B, 48 (10.96%); AB, 10 (2.28%); and O, 254 (57.99%). The most common antigens found in more than 90% of patients were D and e antigens. Specifically, the D antigen was present in 413 patients (94.29%), whereas the e antigen was detected in 438 patients (99.32%). The incidence of the E antigen was lowest among the RH blood group system, being present in 118 patients (26.76%). The K antigen was detected in 28 patients (6.34%).
 |
Table 5 Frequencies of ABO, RH, and K Antigens Among All Patients |
Discussion
We reported the alloimmunization and autoimmunization rates in Saudi SCD and thalassemia patients in Jazan Province, Saudi Arabia. The alloimmunization rate in patients with SCD was 12.98%, which is similar to that in the Eastern Province reported by Bashawri23 (13.7%, Table 2). Conversely, the alloimmunization rate in Jazan Province was significantly lower (P < 0.05) than that reported in studies conducted in Jeddah, Saudi Arabia (39.42%),24 Oman (31.6%),25 and Kuwait group 1 (65.5%) and Kuwait group 2 (23.6%).22 The alloimmunization rate in patients with thalassemia was 13.21% (Table 3). This rate was significantly lower than that reported in Jeddah city (35.57%, P < 0.01),24 Arabian populations (Kuwaiti and Non-Kuwaiti; 30%, P < 0.05),26 and Oman (20%).25
A possible explanation for the low alloimmunization rate in Jazan Province may be the phenotyping conducted at PMBNH for both donors and recipients. This phenotyping includes screening for ABO, RH (D, C, c, E, e) and K antigens. In contrast, in previous studies by Ameen et al and Hindawi et al,22,24 only ABO and D antigens were typed and considered for blood transfusion. This hypothesis is supported by a study conducted in Kuwait, which found that group 2, in which matching for ABO, RH (D, C, c, E, e), and K antigens was conducted, had a significantly lower alloimmunization rate (23.6%) than group 1 (65.5%), in which matching was performed only for ABO and D antigens.22
Moreover, a study by Castro et al found that different protocols of blood group phenotyping could affect the alloimmunization rate in patients with SCD receiving multiple units of transfused blood. They reported that the protocol of providing blood matched for the ABO, RH (D, C, c, E, e) and K antigens would decrease the alloimmunization rate by 53.3%.28 In addition, matching the RH (D, C, c, E and e) and K antigens was shown to significantly reduce the alloimmunization rate in patients with thalassemia.29
In the study population, 56 antibodies were detected in 50 immunized patients due to receiving multiple blood transfusion units. Although the transfusion protocol used for phenotyping includes ABO, D, C, c, E, e and K antigens, the most prevalent antibodies were anti-E and anti-K, at 17.9% and 14.06%, respectively. This is because these patients received compatible blood transfusion units for ABO and D antigens only and not for C, c, E, e, and K antigens. These transfusions were conducted at different hospitals in emergency situations and before referral to PMBNH. The same findings were reported by Hindawi et al, in which anti-E and anti-K were the most frequent alloantibodies.24
The reasons for the alloimmunization rate in the present study could be attributed to racial variations among the blood donors compared with the transfusion recipients. This may be associated with non-Saudi blood donors living in Jazan Province who donate blood to local blood banks. Moreover, patients with multiple antibodies have difficulties in obtaining antigen-negative blood. Furthermore, female patients with SCD and thalassemia comprised 48.17% of the study population, in which female patients normally have greater alloimmunization risks than male patients due to previous pregnancies.16
The autoimmunization rates in the current study were significantly lower than that reported by Ameen et al, which was 11% in thalassemia patients.26 Interestingly, autoantibody formation has been associated with blood transfusion.30 However, the incidence of autoantibodies has been reported to be lower than that of alloantibodies.31 Despite their lower frequency, autoantibodies may reduce the life span of RBCs, hamper cross-matching and lead to hyperhemolysis.29 In addition, autoantibodies might impede the compatibility of donated blood units with the recipients’ blood.32 Indeed, the development of those autoantibodies follows the formation of alloantibodies.33
The frequencies of the various blood groups among Saudi blood donors were determined in Jazan Province, Saudi Arabia.34–38 There were similarities between the blood donors in Jazan area and the patients in the present study. Five patients were produced alloanti-D, in which four male patients and one female. This female was a 35-years-old and might produce alloanti-D due to previous pregnancies. The formation of alloanti-D in the four male patients could be attributable to the presence of partial D antigen in the recipients, which has some missing D epitopes and. Consequently, this may lead to the production of alloanti-D against the missing parts of the intact D antigen, when receiving normal D-positive blood units containing all the D epitopes. Such a phenotype must be treated as D-negative phenotype and receive D-negative blood, which sometimes cannot be feasible due to the shortage in supply of this phenotype. Blood group genotyping may be the gold standard for overcoming the complexity of D antigen and its variants.39 It is highly recommended to investigate the D antigen among the Saudi Arabian population, especially in Jazan Province.
Two patients among the study population produced anti-Fya. Halawani et al found that the Fy(a−b−) was the most prevalent phenotype (78.32%) in Jazan Province.36 Individuals with this phenotype may be prone to develop anti-Fya and anti-Fyb if they receive blood units containing the Duffy antigens. Regarding the Kidd blood group, five patients produced anti-Jka, while three patients produced anti-Jkb. This may reflect the prevalence of Jk(a+b−) and Jk(a−b+) in Jazan Province with 34.96% and 12.59%, respectively.37 Anti-S and anti-s were observed in a single patient each. The frequency of S and s antigens in Jazan Province were 61.07% and 82.55%, respectively.38
According to the frequencies of red cell antigens among the Saudi population in Jazan Province, it is highly recommended to extend the red cell phenotyping protocol to include the following antigen; ABO, RH (D, C, c, E, e), K, Fya, Fyb, Jka and Jkb for SCD and thalassemia patients. A protocol by Lasalle-Williams et al was applied to SCD patients and was reduced the alloimmunization risk to 7%. The matching was for the following antigens; ABO, RH (D, C, c, E, e), K, Kidd and Fya.40
A national registry for the blood donor phenotypes is extremely essential. This can help to establish a database of rare blood donors phenotypes around the Kingdom of Saudi Arabia and benefit different patients by reducing the risk of HTR. The limitation of this study was regarding the SCD patients with the unidentified antibodies, which were antibodies whose specificity could not be determined. This was due to the antibody identification panel was insufficient to identify the specificity.
Conclusion
We reported the alloimmunization and autoimmunization rates in patients with SCD and thalassemia in Jazan Province, Saudi Arabia. The most prevalent antibodies among the study population were anti-E and anti-K. It is highly recommended to perform extended phenotyping for the ABO, RH (D, C, c, E, e), K, Fya, Fyb, Jka and Jkb antigens and include them in the screening panel. This might provide compatible blood units for patients requiring multiple transfusions to ensure safety and reduce the alloimmunization risk.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Institutional Review Board (IRB) of Jazan Hospital, Ministry of Health, Kingdom of Saudi Arabia (No. 2015). Informed consent of the patients were waived by the IRB because of the retrospective nature of the research, which focused on reviewing the patients’ medical records. The patients’ details were held in a secure computerised database. Data were received with medical record numbers only and maintained with confidentiality. Therefore, the patients cannot be identified and there are no implications for the patient’s health and welfare. The study is in compliance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Taif University Researchers Supporting Program (Project number:TURSP-2020/153), Taif University, Saudi Arabia.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Steinberg MH, Sebastiani P. Genetic modifiers of sickle cell disease. Am J Hematol. 2012;87(8):795–803. doi:10.1002/ajh.23232
2. Piel FB, Patil AP, Howes RE, et al. Global epidemiology of sickle haemoglobin in neonates: a contemporary geostatistical model-based map and population estimates. Lancet. 2013;381(9861):142–151. doi:10.1016/S0140-6736(12)61229-X
3. Alhamdan NA, Almazrou YY, Alswaidi FM, Choudhry AJ. Premarital screening for thalassemia and sickle cell disease in Saudi Arabia. Genet Med. 2007;9(6):372–377. doi:10.1097/gim.0b013e318065a9e8
4. Hamali HA, Saboor M. Undiagnosed hemoglobinopathies: a potential threat to the premarital screening program. Pak J Med Sci. 2019;35(6):1611–1615. doi:10.12669/pjms.35.6.976
5. Hyacinth HI, Adams RJ, Greenberg CS, et al. Effect of chronic blood transfusion on biomarkers of coagulation activation and thrombin generation in sickle cell patients at risk for stroke. PLoS One. 2015;10(8):e0134193. doi:10.1371/journal.pone.0134193
6. Hyacinth HI, Adams RJ, Voeks JH, Hibbert JM, Gee BE. Frequent red cell transfusions reduced vascular endothelial activation and thrombogenicity in children with sickle cell anemia and high stroke risk. Am J Hematol. 2014;89(1):47–51. doi:10.1002/ajh.23586
7. Taher AT, Weatherall DJ, Cappellini MD. Thalassaemia. Lancet. 2018;391(10116):155–167. doi:10.1016/S0140-6736(17)31822-6
8. Cappellini M-D, Cohen A, Porter J, Taher A, Viprakasit V. Guidelines for the Management of Transfusion Dependent Thalassaemia (TDT). Nicosia, Cyprus: Thalassaemia International Federation; 2014.
9. Weatherall DJ. The inherited diseases of hemoglobin are an emerging global health burden. Blood. 2010;115(22):4331–4336. doi:10.1182/blood-2010-01-251348
10. Al-Awamy BH. Thalassemia syndromes in Saudi Arabia. Meta-analysis of local studies . Saudi Med J. 2000;21:8–17.
11. Alsaeed ES, Farhat GN, Assiri AM, et al. Distribution of hemoglobinopathy disorders in Saudi Arabia based on data from the premarital screening and genetic counseling program, 2011–2015. J Epidemiol Glob Health. 2018;7(Supplement 1):S41–S47. doi:10.1016/j.jegh.2017.12.001
12. Memish ZA, Owaidah TM, Saeedi MY. Marked regional variations in the prevalence of sickle cell disease and β-thalassemia in Saudi Arabia: findings from the premarital screening and genetic counseling program. J Epidemiol Glob Health. 2011;1(1):61–68. doi:10.1016/j.jegh.2011.06.002
13. Blumberg N, Ross K, Avila E, Peck K. Should chronic transfusions be matched for antigens other than ABO and Rho (D)? Vox Sang. 1984;47(3):205–208. doi:10.1111/j.1423-0410.1984.tb01587.x
14. Vichinsky EP. Current issues with blood transfusions in sickle cell disease. Semin Hematol. 2001;38(Supplement 1):14–22. doi:10.1016/s0037-1963(01)
15. Murao M, Viana MB. Risk factors for alloimmunization by patients with sickle cell disease. Braz J Med Biol Res. 2005;38(5):675–682. doi:10.1590/s0100-879x2005000500004
16. Bauer MP, Wiersum-Osselton J, Schipperus M, Vandenbroucke JP, Briët E. Clinical predictors of alloimmunization after red blood cell transfusion. Transfusion. 2007;47(11):2066–2071. doi:10.1111/j.1537-2995.2007.01433.x
17. Desai PC, Deal AM, Pfaff ER, et al. Alloimmunization is associated with older age of transfused red blood cells in sickle cell disease. Am J Hematol. 2015;90(8):691–695. doi:10.1002/ajh.24051
18. Schonewille H, Van De Watering LMG, Loomans DSE, Brand A. Red blood cell alloantibodies after transfusion: factors influencing incidence and specificity. Transfusion. 2006;46(2):250–256. doi:10.1111/j.1537-2995.2006.00708.x
19. Natukunda B, Schonewille H, Ndugwa C, Brand A. Red blood cell alloimmunization in sickle cell disease patients in Uganda. Transfusion. 2010;50(1):20–25. doi:10.1111/j.1537-2995.2009.02435.x
20. Yazdanbakhsh K, Ware RE, Noizat-Pirenne F. Red blood cell alloimmunization in sickle cell disease: pathophysiology, risk factors, and transfusion management. Blood. 2012;120(3):528–537. doi:10.1182/blood-2011-11-327361
21. Olujohungbe A, Hambleton I, Stephens L, Serjeant B, Serjeant G. Red cell antibodies in patients with homozygous sickle cell disease: a comparison of patients in Jamaica and the United Kingdom. Br J Haematol. 2001;113(3):661–665. doi:10.1046/j.1365-2141.2001.02819.x
22. Ameen R, Al Shemmari S, Al-Bashir A. Red blood cell alloimmunization among sickle cell Kuwaiti Arab patients who received red blood cell transfusion. Transfusion. 2009;49(8):1649–1654. doi:10.1111/j.1537-2995.2009.02185.x
23. Bashawri LAM. Red cell alloimmunization in sickle-cell anaemia patients. East Mediterr Health J. 2007;13(5):1181–1189. doi:10.26719/2007.13.5.1181
24. Hindawi S, Badawi M, Elfayoumi R, et al. The value of transfusion of phenotyped blood units for thalassemia and sickle cell anemia patients at an academic center. Transfusion. 2020;60(Supplement 1):S15–S21. doi:10.1111/trf.15682
25. Alkindi S, AlMahrooqi S, AlHinai S, et al. Alloimmunization in patients with sickle cell disease and thalassemia: experience of a single centre in Oman. Mediterr J Hematol Infect Dis. 2017;9:e2017013. https://doi.org/10.4084/MJHID.2017.013
26. Ameen R, Al-Shemmari S, Al-Humood S, Chowdhury RI, Al-Eyaadi O, Al-Bashir A. RBC alloimmunization and autoimmunization among transfusion-dependent Arab thalassemia patients. Transfusion. 2003;43(11):1604–1610. doi:10.1046/j.1537-2995.2003.00549.x
27. Lawley DN. A generalization of Fisher’s z test. Biometrika. 1938;30(1–2):180–187. doi:10.1093/biomet/30.1-2.180
28. Castro O, Sandler SG, Houston-Yu P, Rana S. Predicting the effect of transfusing only phenotype-matched RBCs to patients with sickle cell disease: theoretical and practical implications. Transfusion. 2002;42(6):684–690. doi:10.1046/j.1537-2995.2002.00126.x
29. Thedsawad A, Taka O, Wanachiwanawin W. Prevalence and clinical significances of red cell alloimmunization and red cell bound immunoglobulin G in polytransfused patients with thalassemias. Hematology. 2019;24(1):208–214. doi:10.1080/16078454.2018.1549818
30. Garratty G. Autoantibodies induced by blood transfusion. Transfusion. 2004;44(1):5–9. doi:10.1111/j.0041-1132.2004.00658.x
31. Poole J, Daniels G. Blood group antibodies and their significance in transfusion medicine. Transfus Med Rev. 2007;21(1):58–71. doi:10.1016/j.tmrv.2006.08.003
32. Singer ST, Wu V, Mignacca R, Kuypers FA, Morel P, Vichinsky EP. Alloimmunization and erythrocyte autoimmunization in transfusion-dependent thalassemia patients of predominantly Asian descent. Blood. 2000;96(10):3369–3373. doi:10.1182/blood.V96.10.3369
33. Young PP, Uzieblo A, Trulock E, Lublin DM, Goodnough LT. Autoantibody formation after alloimmunization: are blood transfusions a risk factor for autoimmune hemolytic anemia? Transfusion. 2004;44(1):67–72. doi:10.1046/j.0041-1132.2003.00589.x
34. Halawani AJ, Arjan AH. ABO, RH, and KEL1 antigens, phenotypes and haplotypes in southwestern Saudi Arabia. Clin Lab. 2021;67(2). doi:10.7754/clin.lab.2020.200633
35. Saboor M, Zehra A, Hamali HA, et al. Prevalence of A2 and A2B subgroups and anti-A1 antibody in blood donors in Jazan, Saudi Arabia. Int J Gen Med. 2020;13:787. doi:10.2147/IJGM.S272698
36. Halawani AJ, Saboor M, Abu-Tawil HI, Mahzari AA, Mansor AS, Bantun F. Prevalence of duffy blood group antigens and phenotypes among Saudi blood donors in Southwestern Saudi Arabia. Clin Lab. 2021;67(1). doi:10.7754/clin.lab.2020.200505
37. Halawani AJ, Saboor M, Abu-Tawil HI, et al. The frequencies of Kidd blood group antigens and phenotypes among Saudi blood donors in Southwestern Saudi Arabia. Saudi J Biol Sci. 2021;29(1):251–254. doi:10.1016/j.sjbs.2021.08.081
38. Halawani AJ, Habibullah MM, Dobie G, et al. Frequencies of MNS blood group antigens and phenotypes in southwestern Saudi Arabia. Int J Gen Med. 2021;14:9315–9319. doi:10.2147/IJGM.S344826
39. Chou ST, Westhoff CM. The role of molecular immunohematology in sickle cell disease. Transfus Apher Sci. 2011;44(1):73–79. doi:10.1016/j.transci.2010.12.014
40. LaSalle‐Williams M, Nuss R, Le T, et al. Extended red blood cell antigen matching for transfusions in sickle cell disease: a review of a 14‐year experience from a single center (CME). Transfusion. 2011;51(8):1732–1739. doi:10.1111/j.1537-2995.2010.03045.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.