Back to Journals » International Medical Case Reports Journal » Volume 19
Recurrent Polymicrobial Bloodstream Infection in End-Stage Renal Disease: Co-Infection with Klebsiella pneumoniae, Enterobacter cloacae, Achromobacter xylosoxidans, and Achromobacter denitrificans in a Hemodialysis Patient
Authors Nabeta H ![]() , Northover NS, Neguemadji NN
, Northover NS, Neguemadji NN ![]() , Doddi S, Amoa AO, Akanyijuka A, Reina Limon R, Uday KA
, Doddi S, Amoa AO, Akanyijuka A, Reina Limon R, Uday KA
Received 29 December 2025
Accepted for publication 21 April 2026
Published 26 May 2026 Volume 2026:19 592417
DOI https://doi.org/10.2147/IMCRJ.S592417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Henry Nabeta,1 Nicole S Northover,2 Ngaba N Neguemadji,1 Swetha Doddi,1 Akua Oforiwa Amoa,1 Abel Akanyijuka,1 Raul Reina Limon,1 Kalpana A Uday1,3
1Department of Internal Medicine, BronxCare Health System, Bronx, NY, USA; 2Department of Medicine, American University of the Caribbean School of Medicine, Cupecoy, Sint Maarten; 3Department of Internal Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Correspondence: Henry Nabeta, Email [email protected]; [email protected]
Abstract: Polymicrobial infections in hemodialysis contribute to increased morbidity and mortality. We report a patient who was readmitted due to infection with multiple pathogens and was treated with favorable outcomes. A 51-year-old male with diabetes mellitus, hypertension, and end-stage renal disease was evaluated in the emergency room following fever and chills observed during hemodialysis via a right chest tunneled catheter 2 days before admission. Two months prior, a left forearm arteriovenous graft had been placed. Initial blood cultures at his dialysis center grew Gram-negative bacilli. Empiric vancomycin and gentamicin were initiated to cover both Gram-positive and Gram-negative pathogens commonly associated with catheter-related infections. When contacted, the dialysis center reported cultures had revealed Klebsiella pneumoniae and Enterobacter cloacae complex. Chest imaging suggested pneumonia, and antibiotics were changed to vancomycin and piperacillin-tazobactam. Blood cultures obtained at admission subsequently identified ESBL-producing Klebsiella pneumoniae, prompting escalation to meropenem. Following tunneled dialysis catheter removal and placement of a right femoral central venous catheter, subsequent cultures identified Achromobacter xylosoxidans sensitive to meropenem. He was discharged 3 weeks after negative cultures. One month later, he was readmitted with fever and worsening hypoxemia requiring oxygen supplementation. Hospital course was complicated by diarrhea, with stool analysis confirming Clostridioides difficile infection. Symptoms resolved with oral vancomycin. Blood cultures identified A. xylosoxidans, leading to meropenem treatment. The left internal jugular tunneled dialysis catheter was removed. He experienced spontaneous bleeding at the graft site. Angiography showed no pseudoaneurysm. An urgent graft excision revealed A. xylosoxidans in the resected arteriovenous graft, along with A. denitrificans in blood cultures. Antibiotics were switched to ceftazidime due to suspected meropenem-induced transaminitis and confirmed susceptibility of the organism. Following negative cultures, a left chest tunneled dialysis catheter was placed, and he was discharged. Infections with multiple microorganisms in hemodialysis require prompt and targeted antimicrobial therapy for favorable outcomes.
Keywords: polymicrobial bacteremia, vascular access infection, dialysis catheter infection, end-stage renal disease, opportunistic gram-negative pathogens
Introduction
Achromobacter xylosoxidans and Achromobacter denitrificans are ubiquitous gram-negative bacteria found in the environment and cause opportunistic infections in immunocompromised individuals.1,2
Infections with A. xylosoxidans have been identified among patients undergoing chemotherapy, individuals with diabetes, and those with chronic kidney disease.3 In these patients, complications like bacteremia and/or sepsis, endocarditis, and established catheter infections through biofilms4–6 contribute to morbidity and mortality. Treatment of these infections is complicated by both intrinsic and acquired antimicrobial resistance. Achromobacter xylosoxidans exhibits intrinsic resistance to several commonly used antibiotics, including aminoglycosides, aztreonam, and many cephalosporins, although susceptibility to ceftazidime and carbapenems has been reported.7–12 Antibiotics resistance by Achromobacter species involves multiple genes encoding β-lactamases, efflux pumps, and drug-modifying enzymes.2,13,14 Similarly, Klebsiella pneumoniae and Enterobacter cloacae possess intrinsic resistance mechanisms, including chromosomal β-lactamase production, which may limit susceptibility to certain β-lactam antibiotics and complicate antimicrobial selection in polymicrobial infections. Klebsiella pneumoniae also acquires additional resistance through transfer of plasmid-encoded β-lactamases (including carbapenemases and ESBLs) and efflux pumps.15–17 Enterobacter cloacae complex expresses chromosomal AmpC β-lactamases and demonstrates innate resistance to aminopenicillins, early generation cephalosporins, cephamycins, and other β-lactam/β-lactamase inhibitor combinations (except piperacillin-tazobactam).18,19 Additionally, inducible Amp expression confers additional resistance to certain β-lactams, including third-generation cephalosporins like cefotaxime and ceftriaxone.20,21
Interestingly, although a rare cause of human infections, A. denitrificans was identified in a patient undergoing hemodialysis with an indwelling non-tunneled central venous catheter (CVC).22,23 Infections with A. denitrificans often require multiple courses and doses of antibiotics for eradication, given their resistant nature and tolerance to drug microbicidal activity.2,24–26
Previous studies found that bacteremia with Achromobacter species was associated with a high all- cause 30-day mortality rate of 23%.27,28 There are no clinical guidelines that describe the treatment of patients with co-infection of both A. xylosoxidans and A. denitrificans, or those that present with any other infections. Co-infection with polymicrobial organisms is likely challenging and requires prompt management to prevent detrimental outcomes including mortality among patients undergoing hemodialysis.
To our knowledge, to date, there is no reported case of polymicrobial infections, including co-infection with A. xylosoxidans and A. denitrificans among patients with end -stage renal disease (ESRD) undergoing hemodialysis. Here, we describe a male patient with diabetes mellitus and ESRD undergoing hemodialysis who presented with recurrent polymicrobial infections with Klebsiella pneumoniae, Enterobacter cloacae complex, A. xylosoxidans, and A. denitrificans, which were successfully managed with appropriate antimicrobial therapy.
Case Report
We report a case of a 51-year-old male with a past medical history of diabetes mellitus, hypertension, chronic obstructive pulmonary disease, cerebrovascular accident with anoxic brain injury complicated by mild cognitive impairment, hyperparathyroidism, seizure disorder, and end-stage renal disease on maintenance hemodialysis (3 days weekly) via a tunneled dialysis catheter (TDC). He was transferred to the emergency room (ER) following positive blood culture results at an outside dialysis center. He lives independently and denied tobacco, alcohol, or illicit drug use. Two months prior to admission, an arteriovenous (AV) graft had been placed in the left forearm. Two days before admission, he developed fever with chills while undergoing dialysis via a right TDC. Blood was obtained for an infection work up. Cultures grew gram-negative bacilli. He received empiric broad-spectrum therapy with vancomycin and gentamicin at the dialysis unit to cover both Gram-positive and Gram-negative organisms while awaiting definitive identification and susceptibility results. He was transferred to our hospital for further management.
Vital signs at the ER were: Blood pressure, 130/75 mmHg, heart rate, 79 bpm, temperature, 98.4 0F (36.9 °C), and saturation, 97% on room air. Physical examination revealed an adult male in no acute distress. Laboratory evaluation found mildly decreased hemoglobin 10.1 g/dL; elevated white blood cell counts 15.3 k/uL, elevated neutrophil count 13.3 k/uL, with neutrophil % of 87.1%; blood urea nitrogen of 29 mg/dL; and elevated creatinine of 6.5 mg/dL. Table 1 is a summary of laboratory findings at admission. During dialysis at the ER, he was observed to spike a fever with chills. Hemodialysis was performed via a left upper chest TDC. Blood specimens were obtained for repeat culture. His outside dialysis Center was contacted and reported the initial blood culture had identified growth of Klebsiella pneumoniae and Enterobacter cloacae complex. There were no patients at the Center with similar symptoms. A chest X-ray at the ER revealed right lower lung opacity along the costophrenic and cardiophrenic angles, with features of infiltrates/pleural disease with atelectasis and pleural effusions. Antibiotics were switched to vancomycin and piperacillin-tazobactam to cover pneumonia with bacteremia.
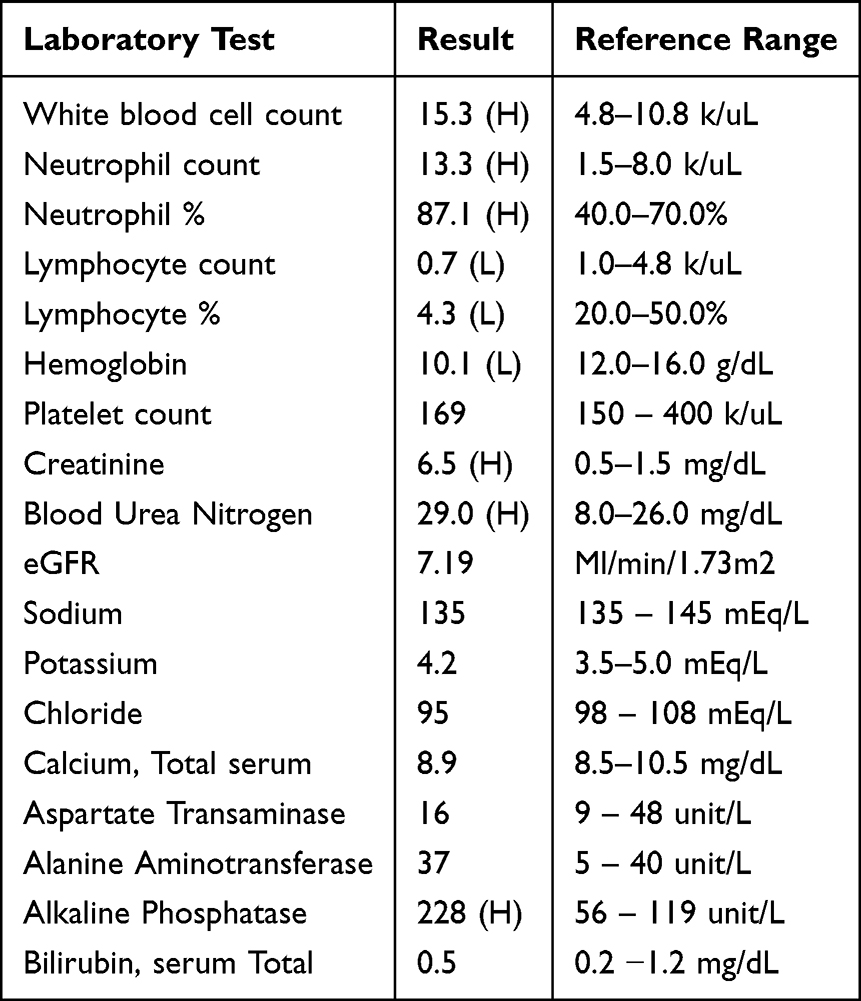 |
Table 1 Laboratory Parameters (Complete Blood Count, Renal Function Tests, Hepatic Function) at Initial Admission |
Infectious disease was consulted to evaluate for possible TDC infection and recommended changing the catheter after 2–3 negative blood cultures. Culture results from admission day 1 grew Klebsiella pneumoniae (ESBL) sensitive to meropenem. Table 2 shows the sensitivity of Klebsiella pneumoniae (ESBL) to different antibiotics tested. Antimicrobial susceptibility testing results were interpreted according to the Clinical and Laboratory Standards Institute (CLSI) 34th edition guidelines used by the institutional microbiology laboratory. Piperacillin/tazobactam was discontinued, and meropenem started. The TDC was removed, and a temporary right femoral non-tunneled CVC placed. On day 12, the white blood cell count decreased to 10.7 k/uL, within the normal range (4.8–10.8 k/uL). Culture results from blood specimens obtained on admission day 2 identified Achromobacter (Acaligenes) xylosoxidans. The patient continued to receive meropenem given the identified sensitivity to this antibiotic. Table 3 shows the sensitivity of A. xylosoxidans identified to different antibiotics tested.
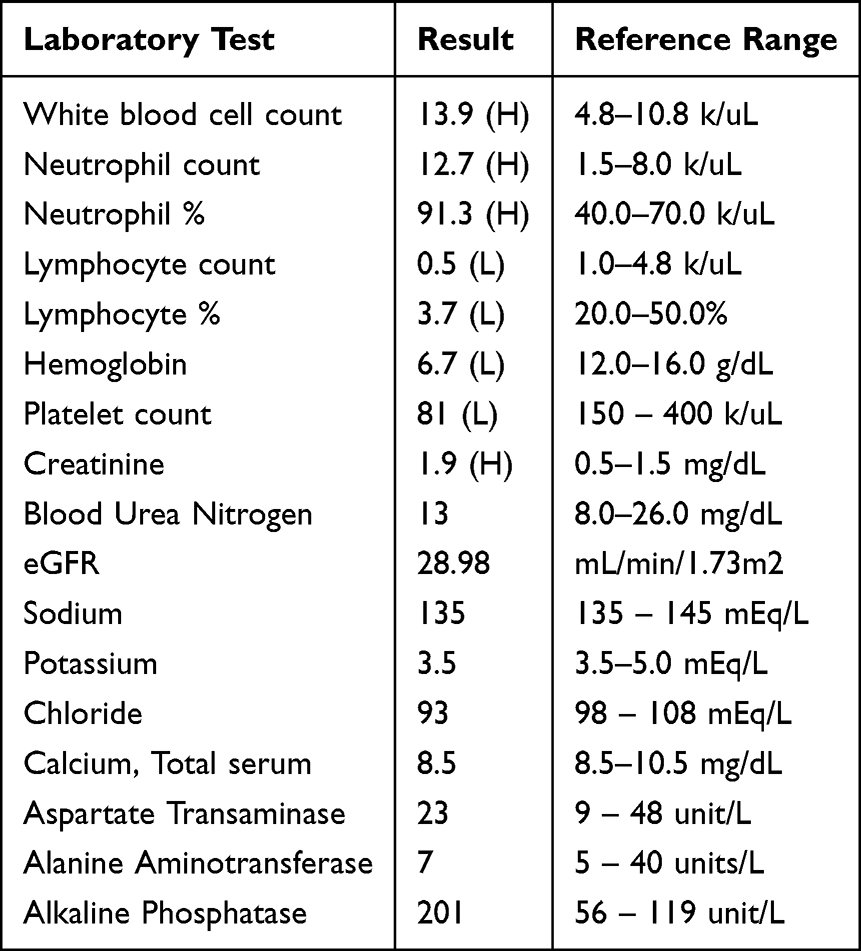 |
Table 2 Laboratory Parameters (Complete Blood Count, Renal Function Tests, Hepatic Function) at Re-Admission |
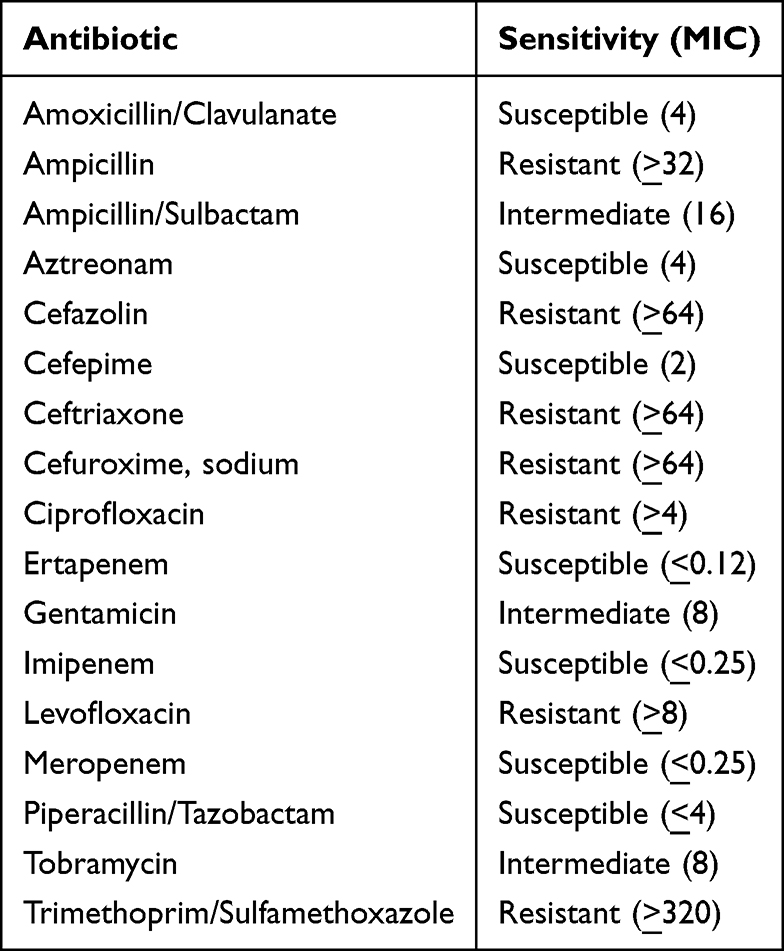 |
Table 3 Sensitivity Profile for Klebsiella pneumoniae (ESBL) with Respective Minimum Inhibitory Concentrations (MIC) for Tested Antibiotics |
Subsequent blood cultures on day 4 and day 5 grew A. xylosoxidans, while that on day 9 grew Achromobacter (Acaligenes) denitrificans with similar sensitivity to A. xylosoxidans. A transthoracic echocardiogram revealed no valvular vegetations. On day 16, the right non-tunneled CVC was removed due to ongoing infection. A left femoral non-tunneled CVC was placed on day 19. Blood cultures from day 18 and day 21 were subsequently negative and he was discharged on day 29.
One month after discharge, the patient was readmitted following a febrile episode and shortness of breath during dialysis via left internal jugular (IJ) TDC at his center. Vancomycin and gentamicin were initiated, and he was transferred to the ER. Vitals were: Blood pressure, 142/86 mmHg, heart rate, 68 bpm, temperature, 98 °F, and saturation, 92% on room air. Laboratory tests revealed a low hemoglobin 6.7 g/dL; elevated white blood cell count 13.9 k/uL, neutrophil count 12.7 k/uL, with neutrophil % of 91.3%; blood urea nitrogen of 13 mg/dL; and elevated creatinine of 1.9 mg/dL. Hemoglobin A1c was 5.7%. Table 4 is a summary of laboratory test results at readmission. He was transfused with one unit of packed red blood cells. He was admitted to the intensive care unit (day 4 to day 6) due to worsening hypoxemia and placed on bilevel positive airway pressure ventilation. He developed worsening diarrhea and on day 4, stool analysis detected C. difficile Toxin B and GDH antigen. He was treated with oral vancomycin 250 mg every 6 hours daily for C. difficile colitis. Chest X-rays revealed obscured cardiac and mediastinal silhouettes, with left pleural effusion and moderate vascular congestion. Thoracocentesis was performed on day 5 for worsening pleural effusions. Blood cultures obtained at admission revealed A. xylosoxidans sensitive to meropenem, and the antibiotic was initiated. The left IJ TDC was removed on day 11. A decision was made to remove the AV graft due to recurrent infections. While vascular surgery planned for graft excision on day 13, he developed spontaneous bleeding at the left forearm graft site. CT angiography of the left upper extremity revealed no pseudoaneurysm or vaso-occlusive disease. He underwent urgent graft excision and patch repair on day 13. Blood cultures from day 11 grew A. denitrificans, while the resected AV graft grew A. xylosoxidans (day 14). Subsequently, blood cultures from day 16 and day 19 were negative for growth. At this stage, Klebsiella pneumoniae ESBL was no longer isolated, and the ongoing infection was attributed to Achromobacter species. On day 19, he developed worsening transaminitis (AST 1128 unit/L, ALT 202 unit/L, ALP 1155 unit/L), for which meropenem-drug induced liver injury was suspected. Meropenem was discontinued, and ceftazidime initiated. Final culture results from day 19 were reported negative 5 days later. A left chest TDC was placed on day 26, while transaminitis resolved on day 39. The non-tunneled CVC was subsequently removed. She improved and was discharged on day 43. A timeline of infection is presented in Figure 1.
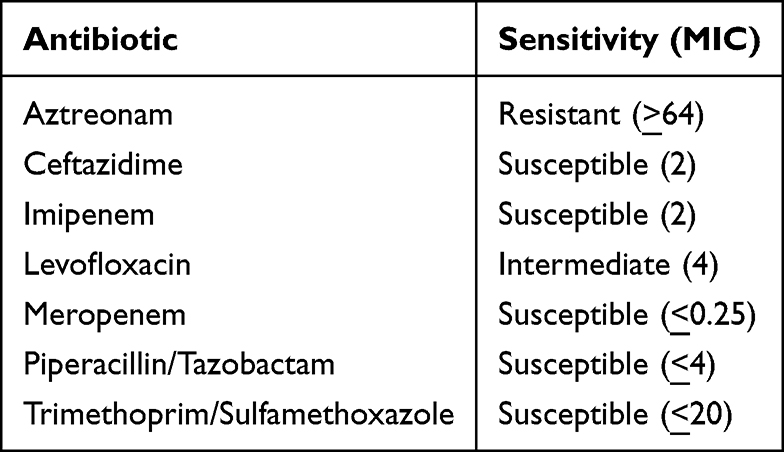 |
Table 4 Sensitivity Profile for Achromobacter xylosoxidans with Respective Minimum Inhibitory Concentration (MIC) for Tested Antibiotics |
 |
Figure 1 Timeline of bacterial species isolated. |
Discussion
This report describes infection with Enterobacter cloacae complex, Klebsiella pneumoniae (ESBL), and recurrent bacteremia with A. xylosoxidans and A. denitrificans in a patient undergoing hemodialysis. While A. xylosoxidans and A. denitrificans are considered low virulence opportunistic pathogens that may infect immunocompetent individuals, infections in immunocompromised states are associated with increased rates of readmissions,29 mortality and morbidity.30–32 Type 2 diabetes and ESRD are associated with immune dysfunction,33,34 predisposing to an increased risk of infections and other comorbidities, with poor outcomes,33,35,36 especially among patients like the case we present here.
Achromobacter species have increasingly been recognized as opportunistic pathogens in immunocompromised patients and those with indwelling vascular devices. Previous reports have described A. xylosoxidans bacteremia in patients with malignancy, cystic fibrosis, and chronic kidney disease, frequently associated with catheter-related infections.35,37,38 Several outbreaks and sporadic infections have also been reported in healthcare settings, including hemodialysis units, highlighting the organism’s ability to persist in aqueous environments and contaminated medical equipment.39–42 However, most reported cases involve monomicrobial infections caused by A. xylosoxidans. In contrast, the present case involved recurrent polymicrobial bloodstream infection with both A. xylosoxidans and A. denitrificans in addition to other Gram-negative pathogens.
Although no outbreaks were reported at the dialysis center, this infection was likely contracted through nosocomial contamination of equipment and catheter manipulation during hemodialysis, as previously reported by other groups.37,43 Infection prevention in dialysis units relies on strict adherence to established infection control practices, including hand hygiene, aseptic technique during catheter access and manipulation, routine disinfection of dialysis equipment, and monitoring of dialysis water treatment systems. Dialysis facilities follow standardized infection prevention protocols to reduce the risk of bloodstream infections associated with vascular access devices. In this case, communication with the dialysis center did not identify other patients with similar symptoms or evidence of an outbreak during the same period, and the unit reported adherence to standard infection control practices. This suggests that the infection likely represented an isolated event rather than a broader breach in infection prevention measures. Common sources of infection during dialysis using venous catheters include contaminated aquatic environments like deionized water in the dialysis system, and mishandling of saline flush, multidose heparin doses, antiseptics, intravenous fluids, and tap water.6,37–40
Indwelling intravascular catheters are a possible source of sustained bacteremia41,42,44 with Achromobacter spps45 when contaminated, and pose a challenge with eradication of infection.46,47 Often, patients may require a long duration of antibiotics,48 and/or combination therapy/antibiotics49,50 before the infection is cleared. This predisposes patients to the risk of drug-related adverse effects due to prolonged duration of treatment. This patient developed transaminitis following treatment with meropenem, which resolved with cessation of the drug and required switching to ceftazidime.
Treatment of Achromobacter infections can be challenging because these organisms demonstrate intrinsic and acquired resistance to multiple antimicrobial agents, including aminoglycosides, aztreonam, and several cephalosporins.9,10 Optimal therapy therefore relies on susceptibility-guided antimicrobial selection, and agents such as carbapenems, piperacillin-tazobactam, or ceftazidime may be required depending on the antimicrobial susceptibility profile.49
Despite numerous advantages like early maturity, synthetic AV grafts in hemodialysis are associated with several infectious and non-infectious complications that increase mortality and fatal outcomes.51,52 Dec B Nguyen et al,53 R A Bonome et al,54 IW Fong et al,55 and George M Nassar et al56 have observed that AV grafts have an intermediate risk of vascular access-related infection when compared to AV fistulas and CVCs. Upon excision, the graft from this patient grew A. xylosoxidans, while subsequent cultures were negative for infection. Although arteriovenous fistulas are generally preferred due to their lower infection risk, creation of a new fistula may not always be feasible because of patient-specific vascular anatomy, prior vascular access history, or the need for immediate dialysis access. In this case, the infected graft was excised to achieve source control, and vascular access decisions were made in consultation with vascular surgery to ensure continued dialysis while minimizing the risk of recurrent infection.
Blood stream infections in end-stage renal disease are associated with unfavorable outcomes,57–60 with polymicrobial infection described as an independent risk factor for death in hemodialysis.57 Prompt identification and management of patients with empirical antibiotics is required57 while awaiting sensitivity results for definitive management. Blood cultures at the initial admission identified Enterobacter cloacae complex and A. xylosoxidans. On readmission, cultures grew A. xylosoxidans and A. denitrificans. The patient was initiated on broad spectrum antibiotics, that were promptly changed as soon as sensitivity results were availed. Upon developing suspected meropenem-induced transaminitis during the subsequent readmission, the antibiotic regimen was changed, with improvement in hepatic function. Among patients undergoing hemodialysis who present with polymicrobial infections, prompt recognition and identification of the sensitivity profile of antibiotics, as well as close monitoring for related toxicity is required for favorable outcomes.
Limitations
This report has several limitations. As a single case report, the findings may not be generalizable to all patients with end-stage renal disease undergoing hemodialysis. Additionally, the exact source of infection could not be definitively established, although contamination of vascular access devices and dialysis-related equipment was suspected. Furthermore, microbiological analysis was limited to routine clinical cultures, and environmental or molecular investigations were not performed to confirm the precise source or transmission pathway. Despite these limitations, this case highlights the complexity of managing recurrent polymicrobial infections in immunocompromised patients and underscores the importance of early pathogen identification, targeted antimicrobial therapy, and timely vascular access management.
Conclusions
In summary, we report a case of recurrent polymicrobial bloodstream infection in a patient with ESRD undergoing hemodialysis involving Klebsiella pneumoniae, Enterobacter cloacae complex, A. xylosoxidans, and A. denitrificans. Successful management required prompt microbiological identification, targeted antimicrobial therapy including carbapenems and ceftazidime, and removal of infected vascular access devices (including TDCs) and an arteriovenous graft. This case highlights the importance of early pathogen identification, appropriate antimicrobial therapy, and vascular access management in treating complex polymicrobial infections in hemodialysis patients.
Ethics Approval
BronxCare Health System does not require ethical approval for reporting individual cases or case series. However, written informed consent was obtained from the patient for publication of this report.
Informed Consent
Written informed consent was obtained from the patient for publication of patient’s anonymized information in this article.
Acknowledgments
We appreciate the care provided to the patient by the BCHS dialysis unit, Infectious Disease team, and nursing staff on the renal floor. We thank FNU Veena MD, BCHS Department of Internal Medicine, for reviewing the initial submission, incorporating reviewer edits, and proofreading the revised manuscript for correctness and relevance of edits made.
Funding
No funding was used during the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chávez-Valencia V, Aguilar-Bixano O, Orizaga-De-la-Cruz C, Lagunas-Rangel FA. Bacteraemia by Achromobacter denitrificans in Hemodialysis. Indian J Nephrol. 2021;31(5):500–9. doi:10.4103/ijn.IJN_317_20
2. Al-Asadi SA, Al-Kahachi RES, Alwattar WMA, Bootwala J, Sabbah MA. Genomic insights into achromobacter mucicolens IA antibiotic resistance. Microbiol Spectrum. 2022;10(2):e01916–21. doi:10.1128/spectrum.01916-21
3. Donderski R, Grajewska M, Mikucka A, Sulikowska B, Gospodarek-Komkowska E, Manitius J. Achromobacter xylosoxidans relapsing peritonitis and Streptococcus suis peritonitis in peritoneal dialysis patients: a report of two cases. Case Rep Nephrol. 2018;2018(1):9454520. doi:10.1155/2018/9454520
4. Ahmed M, Nistal C, Jayan R, Kuduvalli M, Anijeet H. Achromobacter xylosoxidans, an emerging pathogen in catheter-related infection in dialysis population causing prosthetic valve endocarditis: a case report and review of literature. Clin Nephrol. 2009;71(3):350–354. doi:10.5414/CNP71350
5. Rehman ZU, Chaudhari AP, Baumstein DI, Tahir MK. Achromobacter xylosoxidans: a potentially serious occult dialysis catheter-related infection: FR-PO481. J Am Soc Nephrol. 2023;34(11S):535–536. doi:10.1681/ASN.20233411S1535d
6. Kim MJ, Bancroft E, Lehnkering E, Donlan RM, Mascola L. Alcaligenes xylosoxidans bloodstream infections in outpatient oncology office. Emerg Infect Dis. 2008;14(7):1046. doi:10.3201/eid1407.070894
7. Gahrn-Hansen B, Siboni K. Studies on ampicillin resistance in Achromobacter xylosoxidans. APMIS. 1988;96(1–6):185–187. doi:10.1111/j.1699-0463.1988.tb05288.x
8. Nicolosi D, Nicolosi V, Cappellani A, Nicoletti G, Blandino G. Antibiotic susceptibility profiles of uncommon bacterial species causing severe infections in Italy. J Chemother. 2009;21(3):253–260. doi:10.1179/joc.2009.21.3.253
9. Hu Y, Zhu Y, Ma Y, et al. Genomic insights into intrinsic and acquired drug resistance mechanisms in Achromobacter xylosoxidans. Antimicrob Agents Chemother. 2015;59(2):1152–1161. doi:10.1128/AAC.04260-14
10. Almuzara M, Limansky A, Ballerini V, Galanternik L, Famiglietti A, Vay C. In vitro susceptibility of Achromobacter spp. isolates: comparison of disk diffusion, Etest and agar dilution methods. Int J Antimicrob Agents. 2010;35(1):68–71. doi:10.1016/j.ijantimicag.2009.08.015
11. Glupczynski Y, Hansen W, Freney J, Yourassowsky E. In vitro susceptibility of Alcaligenes denitrificans subsp. xylosoxidans to 24 antimicrobial agents. Antimicrob Agents Chemother. 1988;32(2):276–278. doi:10.1128/AAC.32.2.276
12. Holmes B, Snell J, Lapage S. Strains of Achromobacter xylosoxidans from clinical material. J Clin Pathol. 1977;30(7):595–601. doi:10.1136/jcp.30.7.595
13. Sandner-Miranda L, Vinuesa P, Cravioto A, Morales-Espinosa R. The genomic basis of intrinsic and acquired antibiotic resistance in the genus Serratia. Front Microbiol. 2018;9:828. doi:10.3389/fmicb.2018.00828
14. Ray S, Flemming LK, Scudder CJ, et al. Comparative phenotypic and genotypic antimicrobial susceptibility surveillance in Achromobacter spp. through whole genome sequencing. Microbiol Spectrum. 2025;13(4):e02527–24. doi:10.1128/spectrum.02527-24
15. Tsang KK, Lam MM, Wick RR, et al. Diversity, functional classification and genotyping of SHV β-lactamases in Klebsiella pneumoniae. Microbial Genomics. 2024;10(10):001294. doi:10.1099/mgen.0.001294
16. Maclean AK, Morrow S, Niu F, Hanson ND. What contributes to the minimum inhibitory concentration? Beyond β-lactamase gene detection in Klebsiella pneumoniae. J Infect Dis. 2024;230(4):e777–e788. doi:10.1093/infdis/jiae204
17. Kumar V, Sun P, Vamathevan J, et al. Comparative genomics of Klebsiella pneumoniae strains with different antibiotic resistance profiles. Antimicrob Agents Chemother. 2011;55(9):4267–4276. doi:10.1128/AAC.00052-11
18. Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious diseases society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clinl Infect Dis. 2024;ciae403. doi:10.1093/cid/ciae403
19. Macesic N, Uhlemann A-C, Peleg AY. Multidrug-resistant gram-negative bacterial infections. Lancet. 2025;405(10474):257–272. doi:10.1016/S0140-6736(24)02081-6
20. Matsuo A, Matsumura Y, Mori K, Noguchi T, Yamamoto M, Nagao M. Molecular epidemiology and β-lactam resistance mechanisms of Enterobacter cloacae complex isolates obtained from bloodstream infections, Kyoto, Japan. Microbiol Spectrum. 2025;13(4):e02485–24. doi:10.1128/spectrum.02485-24
21. Paterson DL. Resistance in gram-negative bacteria: enterobacteriaceae. Am J Infect Control. 2006;34(5):S20–S28. doi:10.1016/j.ajic.2006.05.238
22. Reis AC, Kroll K, Gomila M, Kolvenbach BA, Corvini PF, Nunes OC. Complete genome sequence of Achromobacter denitrificans PR1. Genome Announcements. 2017;5(31). doi:10.1128/genomea.00762-17
23. Aundhakar S, Mane M, Bharadiya A, Pawar S. Watch out! Pneumonia secondary to achromobacter denitrificans. Ann Med Health Sci Res. 2014;4(1):22–24. doi:10.4103/2141-9248.131700
24. Reis PJ, Reis AC, Ricken B, et al. Biodegradation of sulfamethoxazole and other sulfonamides by Achromobacter denitrificans PR1. J Hazard Mater. 2014;280:741–749. doi:10.1016/j.jhazmat.2014.08.039
25. Pandit P, Sahni A, Grover N, Dudhat V, Das N, Biswas A. Catheter-related blood stream infections: prevalence, risk factors and antimicrobial resistance pattern. Med J Armed Forces India. 2021;77(1):38–45. doi:10.1016/j.mjafi.2019.07.002
26. Doi Y, Shimizu M, Fujita T, Nakamura A, Takizawa N, Takaya N. Achromobacter denitrificans strain YD35 pyruvate dehydrogenase controls NADH production to allow tolerance to extremely high nitrite levels. Appl Environ Microbiol. 2014;80(6):1910–1918. doi:10.1128/AEM.03316-13
27. Crone CG, Rezahosseini O, Schultz HHL, et al. Achromobacter spp. in a cohort of non-selected pre-and post-lung transplant recipients. Pathogens. 2022;11(2):181. doi:10.3390/pathogens11020181
28. Barragán EP, Pérez JS, Corbella L, Orellana MÁ, Fernández-Ruiz M. Achromobacter xylosoxidans bacteremia: clinical and microbiological features in a 10-year case series. Revista Española de Quimioterapia. 2018;31(3):268.
29. Zilberman-Itskovich S, Cohen E, Ploshansky L-A, et al. The epidemiology of Stenotrophomonas maltophilia and Achromobacter xylosoxidans infections. Antimicrob Steward Healthc Epidemiol. 2024;4(1):e18. doi:10.1017/ash.2024.11
30. Habib S, Fuca N, Azam M, Siddiqui AH, Rajdev K, Chalhoub M. Achromobacter xylosoxidans/denitrificans bacteremia and subsequent fatal Escherichia coli/Streptococcus anginosus pleural empyema. Respirat Med Case Rep. 2018;25:311–313. doi:10.1016/j.rmcr.2018.10.010
31. Awadh H, Mansour M, Aqtash O, Shweihat Y. Pneumonia due to a rare pathogen: achromobacter xylosoxidans, subspecies denitrificans. Case Rep Infect Dis. 2017;2017:3969682. doi:10.1155/2017/3969682
32. Karanth SS, Gupta A, Prabhu M. Community acquired bilateral upper lobe pneumonia with acute adrenal insufficiency: a new face of Achromobacter Xylosoxidans. Australas Med J. 2012;5(10):531. doi:10.4066/AMJ.2012.1279
33. Berbudi A, Rahmadika N, Tjahjadi AI, Ruslami R. Type 2 diabetes and its impact on the immune system. Current Diabetes Rev. 2020;16(5):442–449. doi:10.2174/1573399815666191024085838
34. Tessaro FH, Ayala TS, Nolasco EL, Bella LM, Martins JO. Insulin influences LPS-induced TNF-α and IL-6 release through distinct pathways in mouse macrophages from different compartments. Cell Physiol Biochem. 2017;42(5):2093–2104. doi:10.1159/000479904
35. Abbott K, Agodoa L. Etiology of bacterial septicemia in chronic dialysis patients in the United States. Clin nephrol. 2001;56(2):124–131.
36. Singh K, Prasad KN, Mishra P, et al. Toll-like receptors TLR4 (Asp299Gly and Thr399Ile) and TLR2 (Arg677Trp and Arg753Gln) gene polymorphisms in end-stage renal disease patients on peritoneal dialysis. Int Urol Nephrol. 2015;47(12):2031–2037. doi:10.1007/s11255-015-1124-8
37. Gómez-Cerezo J, Suárez I, Ríos J, et al. Achromobacter xylosoxidans bacteremia: a 10-year analysis of 54 cases. Eur J Clin Microbiol Infect Dis. 2003;22(6):360–363. doi:10.1007/s10096-003-0925-3
38. Bonis BM, Hunter RC. JMM Profile: achromobacter xylosoxidans: the cloak-and-dagger opportunist. J Med Microbiol. 2022;71(5):001505. doi:10.1099/jmm.0.001505
39. Tena D, Carranza R, Barberá J, et al. Outbreak of long-term intravascular catheter-related bacteremia due to Achromobacter xylosoxidans subspecies xylosoxidans in a hemodialysis unit. Eur J Clin Microbiol Infect Dis. 2005;24(11):727–732. doi:10.1007/s10096-005-0028-4
40. Reverdy M, Freney J, Fleurette J, et al. Nosocomial colonization and infection by Achromobacter xylosoxidans. J Clin Microbiol. 1984;19(2):140–143. doi:10.1128/jcm.19.2.140-143.1984
41. Castellanos JLV, Villagrana EDC, Mendoza BMGT, Durazo DLG, Plascencia JG, Mejía-Zárate AK. First bacteremia outbreak due Achromobacter spp. in hemodialysis patients in Mexico. Nefrologia. 2022;42(1):101–103. doi:10.1016/j.nefroe.2022.03.003
42. Günther F, Merle U, Frank U, Gaida MM, Mutters NT. Pseudobacteremia outbreak of biofilm-forming Achromobacter xylosoxidans–environmental transmission. BMC Infect Dis. 2016;16(1):584. doi:10.1186/s12879-016-1909-0
43. Duggan JM, Goldstein SJ, Chenoweth CE, Kauffman CA, Bradley SF. Achromobacter xylosoxidans bacteremia: report of four cases and review of the literature. Clinl Infect Dis. 1996;23(3):569–576. doi:10.1093/clinids/23.3.569
44. Hugon E, Marchandin H, Poirée M, Fosse T, Sirvent N. Achromobacter bacteraemia outbreak in a paediatric onco-haematology department related to strain with high surviving ability in contaminated disinfectant atomizers. J Hosp Infect. 2015;89(2):116–122. doi:10.1016/j.jhin.2014.07.012
45. Yoon S, Kim H, Lim S, Kang J-M. Nosocomial outbreak of Achromobacter spp. bacteremia due to germicide contamination: a systematic review. Eur Rev Med Pharmacol Sci. 2022;26(17).
46. Turgutalp K, Kiykim A, Ersoz G, Kaya A. Fatal catheter-related bacteremia due to Alcaligenes (Achromobacter) xylosoxidans in a hemodialysis patient. Int Urol Nephrol. 2012;44(4):1281–1283. doi:10.1007/s11255-011-0003-1
47. Houlihan E, Lucey M, Pandian A, et al. Case of recurrent Achromobacter xylosoxidans bacteraemia and PICC (peripherally-inserted central catheter) line infection in an immunocompromised patient. Infect Prevent Pract. 2022;4(1):100202. doi:10.1016/j.infpip.2022.100202
48. Casazza R, De Leonardis R, Cozzolino M, Dialisi A, Borromeo CPSC. A. xylosoxidans and R. radiobacter-induced polimicrobic peritonitis in peritoneal dialysis: a case report. Giornale italiano di nefrologia. 2025;42(1). doi:10.69097/42-01-2025-07
49. Isler B, Kidd TJ, Stewart AG, Harris P, Paterson DL. Achromobacter infections and treatment options. Antimicrob Agents Chemother. 2020;64(11). doi:10.1128/AAC.01025-20
50. Turel O, Kavuncuoglu S, Hosaf E, et al. Bacteremia due to Achromobacter xylosoxidans in neonates: clinical features and outcome. Braz J Infect Dis. 2013;17(4):450–454. doi:10.1016/j.bjid.2013.01.008
51. Lawson JH, Niklason LE, Roy-Chaudhury P. Challenges and novel therapies for vascular access in haemodialysis. Nat Rev Nephrol. 2020;16(10):586–602. doi:10.1038/s41581-020-0333-2
52. Beathard GA. The treatment of vascular access graft dysfunction: a nephrologist’s view and experience. Adv Renal Replace Therap. 1994;1(2):131–147. doi:10.1016/S1073-4449(12)80044-6
53. Nguyen DB, Arduino MJ, Patel PR. Hemodialysis-associated infections. In: Chronic Kidney Disease, Dialysis, and Transplantation. 2018:389.
54. Bonomo RA, Rice D, Whalen C, Linn D, Eckstein E, Shlaes DM. Risk factors associated with permanent access-site infections in chronic hemodialysis patients. Infect Control Hosp Epidemiol. 1997;18(11):757–761. doi:10.1086/647530
55. Fong IW, Capellan JM, Simbul M, Angel J. Infection of arterio-venous fistulas created for chronic haemodialysis. Scand J Infect Dis. 1993;25(2):215–220. doi:10.3109/00365549309008487
56. Nassar GM, Ayus JC. Infectious complications of the hemodialysis access. Kidney Int. 2001;60(1):1–13. doi:10.1046/j.1523-1755.2001.00765.x
57. Fysaraki M, Samonis G, Valachis A, et al. Incidence, clinical, microbiological features and outcome of bloodstream infections in patients undergoing hemodialysis. Int J Med Sci. 2013;10(12):1632. doi:10.7150/ijms.6710
58. Tozawa M, Iseki K, Fukiyama K. Prevalence of hospitalization and prognosis of patients on chronic dialysis. Clin Experi Nephrol. 2000;4(3):236–240. doi:10.1007/s101570070028
59. Liu J, Su YK, Liu C-F, Chen J. Nosocomial blood-stream infection in patients with end-stage renal disease: excess length of hospital stay, extra cost and attributable mortality. J Hosp Infect. 2002;50(3):224–227. doi:10.1053/jhin.2001.1162
60. Hoen B, Paul-Dauphin A, Hestin D, Kessler M. EPIBACDIAL: a multicenter prospective study of risk factors for bacteremia in chronic hemodialysis patients. J Am Soc Nephrol. 1998;9(5):869–876. doi:10.1681/ASN.V95869
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevention of Intradialytic Hypotension in Hemodialysis Patients: Current Challenges and Future Prospects
Hamrahian SM, Vilayet S, Herberth J, Fülöp T
International Journal of Nephrology and Renovascular Disease 2023, 16:173-181
Published Date: 1 August 2023
Clinical Characteristics and Risk Factors for Multidrug-Resistant Enterobacter cloacae Complex Bacteremia in a Chinese Tertiary Hospital: A Decade Review (2013–2022)
Han M, Hua M, Xie H, Li J, Wang Y, Shen H, Cao X
Infection and Drug Resistance 2025, 18:427-440
Published Date: 22 January 2025
Effect of Hemodialysis on Glaucoma Patients
Hendricks TM, Quist TS, Wang K, Antes LM, Boese EA
Clinical Ophthalmology 2025, 19:827-834
Published Date: 12 March 2025