Back to Journals » Cancer Management and Research » Volume 12
Recurrence Patterns and Survival Outcomes in Chinese Patients with Surgically Treated Recurrent Ovarian Clear Cell Carcinoma: A Single Institutional Analysis of 45 Cases
Authors Ye S, Zhou S, Chen W ![]() , Xiang L, Wu X, Yang H
, Xiang L, Wu X, Yang H
Received 12 December 2019
Accepted for publication 29 January 2020
Published 7 February 2020 Volume 2020:12 Pages 913—919
DOI https://doi.org/10.2147/CMAR.S242129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Shuang Ye,1,2,* Shuling Zhou,2,3,* Wei Chen,1,2,4,* Libing Xiang,1,2 Xiaohua Wu,1,2 Huijuan Yang1,2
1Department of Gynecologic Oncology, Fudan University Shanghai Cancer Center, Shanghai, People’s Republic of China; 2Department of Oncology, Shanghai Medical College, Fudan University, Shanghai, People’s Republic of China; 3Department of Pathology, Fudan University Shanghai Cancer Center, Shanghai, People’s Republic of China; 4Department of Obstetrics and Gynecology, Minhang Hospital, Fudan University, The Central Hospital of Minhang District, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huijuan Yang
Department of Gynecologic Oncology, Fudan University Shanghai Cancer Center, Shanghai 200032, People’s Republic of China
Tel +86-21-65260535
Fax +86-21-64174774
Email [email protected]
Background: To evaluate the recurrence patterns and survival outcomes of surgically treated relapsed ovarian clear cell carcinoma (OCCC) patients.
Methods: We performed a comprehensive retrospective analysis of all the patients who underwent secondary debulking from 2004/10 to 2019/04.
Results: In total, 45 eligible patients were included. 75.6% of the patients had early-stage disease and platinum-sensitive recurrence accounted for 70.5%. The median progression-free survival after primary surgery (PFS 1) was 20 months (range, 2– 137). Of all, 64.4% patients had solitary recurrence and 86.7% patients had no residual disease after secondary surgery. Regarding tumor distribution, the most common site was pelvis (47.5%), followed by lymph node metastases (18.0%) and abdominal wall lesions (8.2%). For the entire population, the median disease-free survival after recurrence (PFS 2) and post-relapse survival (PRS) was 15 months (range, 0– 96), and 24 months (range, 3– 159), respectively. Eight patients (17.8%) had a prolonged PFS2 more than 30 months. Patients with localized relapse had better survival including PFS 2 (P=0.023), PRS (P=0.004), and overall survival (OS) (P=0.029). Patients who achieved complete resection tended to have longer PFS 2 (P=0.017). After multivariate analysis, complete resection at recurrence remained as an independent positive predictor for PFS 2 (P=0.022). The median OS was 50 months and was significantly associated with platinum response (P=0.003) and number of relapsed lesions (P=0.002).
Conclusion: A high rate of pelvic recurrence was noted in this population. Patients with focal recurrence had a favorable prognosis. Complete resection at secondary debulking proved to be an independent predictor for disease-free survival.
Keywords: ovarian neoplasms, clear cell carcinoma, recurrence, survival
Background
Ovarian clear cell carcinoma (OCCC), as a histological subtype of ovarian cancer, is more commonly seen in Asian women.1–3 OCCC represents a great challenge given its disease aggressiveness and chemotherapy resistance.1,2 To make it worse, recurrent patients have grave survival and limited effective systemic treatment options.4 According to a Japanese study including 113 recurrent cases, the 5-year post-recurrence survival rate was only 13.2%.5 The objective response rate to conventional chemotherapy is 9% in platinum-sensitive and 1% in platinum-resistant recurrence.6 Therefore, the effective treatment of recurrent OCCC is a largely unmet need. Recently, three Phase II trials have been published, which focused on evaluating novel biologic agents in the treatment of recurrent or persistent OCCC.7–9 It is disappointed, but within expectation, that oral multi-target kinases including sunitinib,7 cabozantinib8 and ENMD-20769 demonstrated minimal activity in the second- and third-line treatment as a single agent.
From a different perspective, what is the role of secondary debulking surgery in certain recurrent OCCC patients? Few publications have ever been reported. A most recent study from Japan evaluated the oncologic outcomes after secondary surgery in 25 recurrent OCCC cases.10
The aim of the current study was to characterize the recurrence patterns and survival outcomes in a population of surgically treated recurrent OCCC patients in our center. Besides, possible prognostic variables were assessed.
Materials and Methods
Patients
The study was approved by the institutional review board and the requirement for written informed consent was waived due to its retrospective design. We searched the Electronic Medical Record system to include all the patients who received secondary debulking surgery at first recurrence in our institution. The patient data were identified and maintained with confidentiality, in accordance with the Declaration of Helsinki. A total of 48 patients fulfilled the criteria from 2004/10 to 2019/04. Three cases were excluded due to incomplete information: absence of stage at initial surgery (n=2) and no survival information after recurrent surgery (n=1). All the patients underwent open surgery. Data were collected regarding age, International Federation of Gynecology and Obstetrics (FIGO) stage at initial diagnosis,11 platinum-free interval, intro-operative findings in secondary surgery including recurrent tumor numbers and distributions, residual disease at secondary cytoreduction, and status at the date of last contact. Patients were considered to have platinum-sensitive disease if the interval time was more than 6 months from the completion of the last platinum-based chemotherapy to disease recurrence. Patients who had a recurrence at more than one site were considered to have multiple sites of recurrence. We further dichotomized the modes of recurrence into within pelvis and out of pelvis. Progression-free survival 1 (PFS 1) and overall survival (OS) was defined as the time interval from the date of the primary surgery to the date of first recurrence and death or last contact, respectively. PFS 2 was measured as the time interval from the date of the secondary surgery to the date of the next recurrence. Post-relapse survival (PRS) was calculated as the time interval from the date of diagnosis of relapsed disease to the date of death or last contact. Patients with PFS 2 > 30 months were considered to have a prolonged disease-free interval after the first recurrence in line with a previous study.4
Statistical Analysis
Descriptive statistics were used in presenting clinicopathological variables. Medians and ranges were employed for continuous variables, while proportions were used for categorical data. Survival time was evaluated using the Kaplan-Meier model, whereas Cox regression was conducted for multivariate analysis. Variables with statistical significance on univariate analysis were included in the multivariate one. All P values reported were two-tailed, and P<0.05 was considered statistically significant.
Kaplan–Meier curves were plotted using GraphPad Prism (Version 6.0, GraphPad Software, Inc., La Jolla, CA, USA). All other statistic analyses were performed with Statistical Package for Social Science (SPSS) (Version 20.0, SPSS, Inc., Chicago, IL, USA).
Result
Patient Information and Recurrence Patterns
Table 1 summarizes the demographic and clinical information of the 45 patients included in the study. About three quarters (75.6%) of the patients had early-stage disease (FIGO I+II) at primary surgery. Only one patient did not receive platinum-based adjuvant chemotherapy. Overall, platinum-sensitive recurrence accounted for 70.5% (31/44). The median PFS 1 was 20 months (range, 2–137).
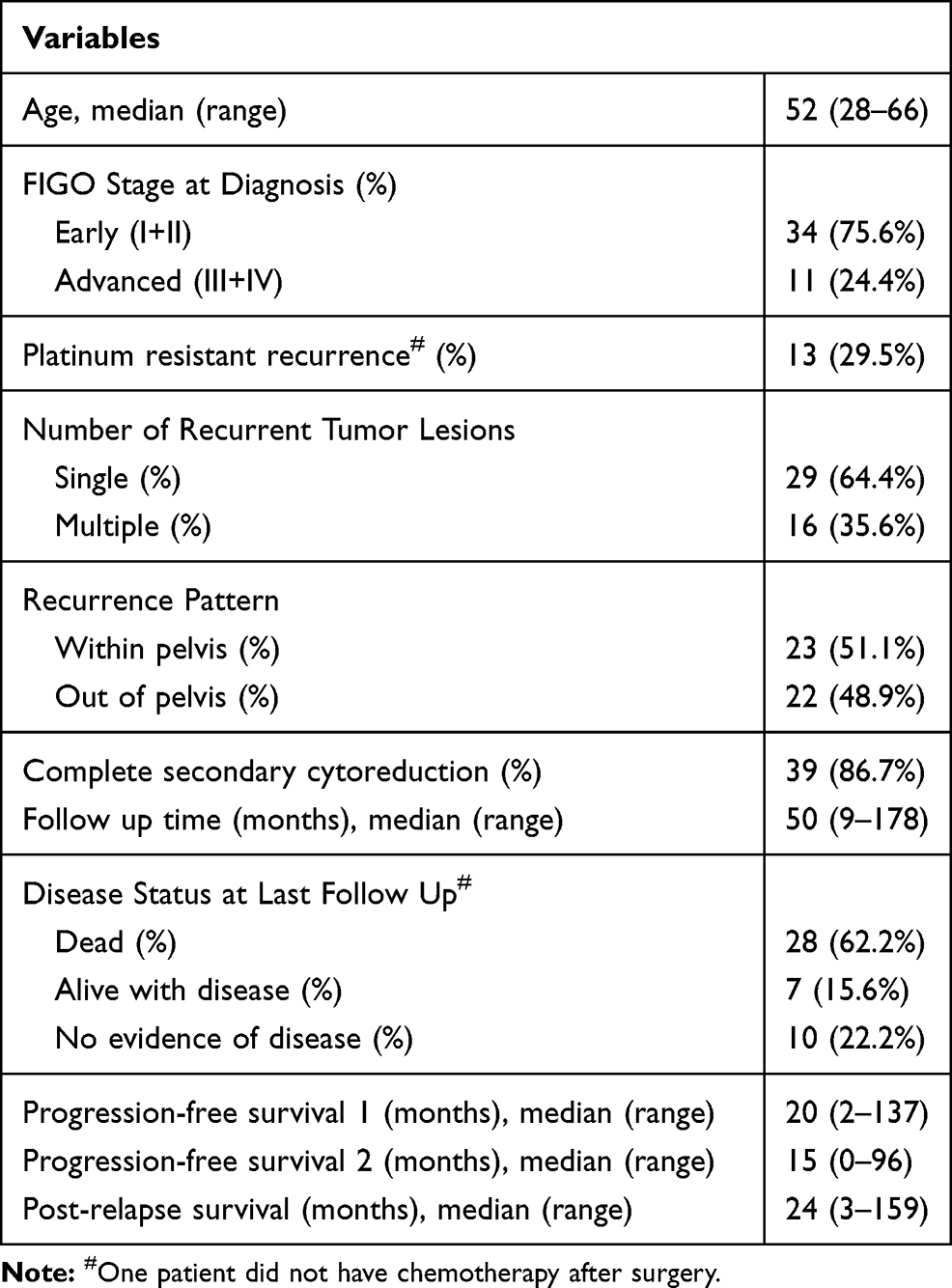 |
Table 1 Patient Characteristics (n=45) |
Concerning the number of recurrent tumor lesions, 29 (64.4%) patients presented with single-site recurrence. In terms of tumor distribution, 51.1% patients had initial recurrence involving the pelvis. Complete secondary cytoreduction was achieved in 39 (86.7%) of the patients.
Table 2 presents the specific details of the 61 recurrence sites identified in the entire cohort. Not surprisingly, the most common site was pelvis (n=29, 47.5%), and followed by lymph node metastases (n=11, 18.0%) and abdominal wall lesions (n=5, 8.2%). Parenchymal solid organ metastases were observed in liver (n=3, 4.9%), lung (n=2, 3.3%) and spleen (n=1, 1.6%), respectively. Among the 29 patients with solitary recurrence, more than half (18/29, 62.1%) of the patients had pelvis-confined tumor. The rest patients had recurrent tumors in lung (n=2), liver (n=1), spleen (n=1), abdominal wall (n=3), lymph node (n=2), hepatorenal recess (n=1), and right diaphragm (n=1).
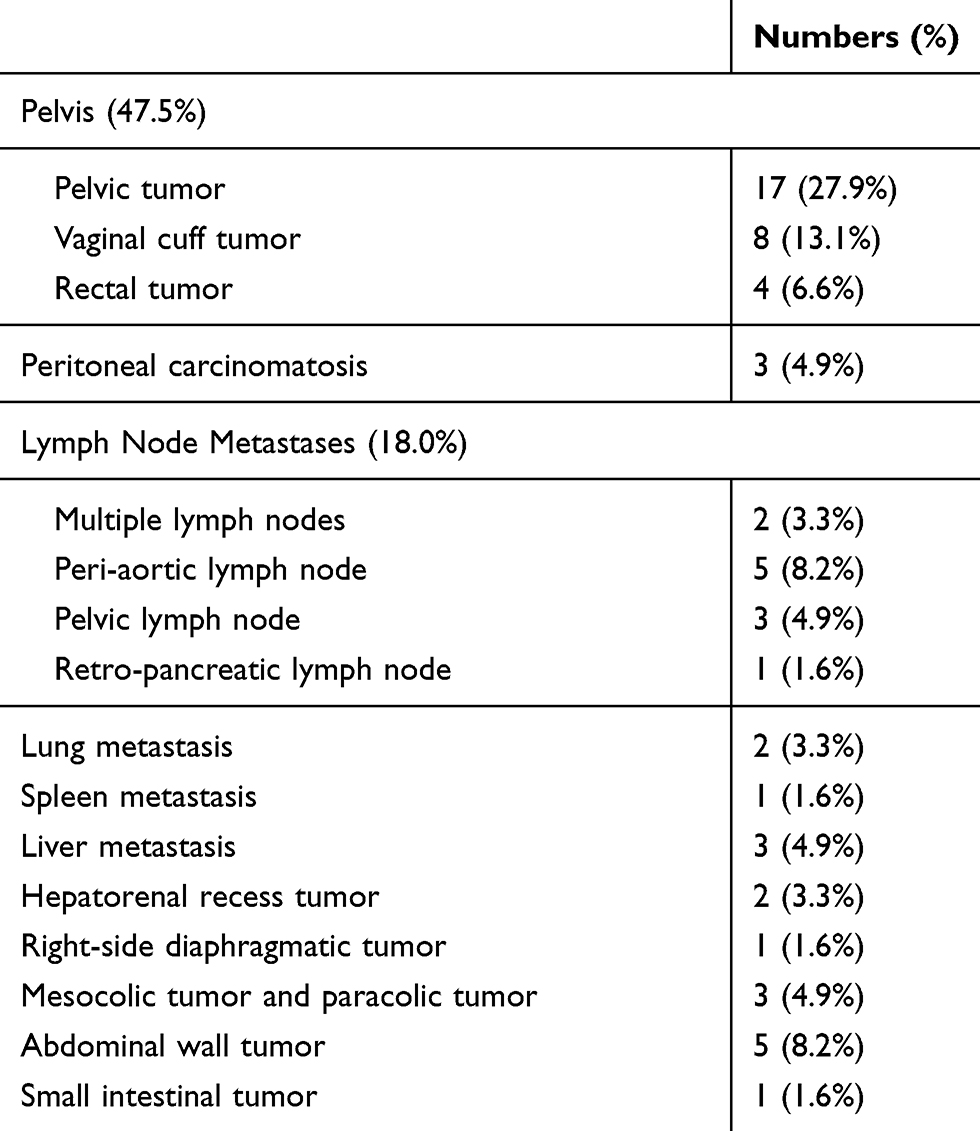 |
Table 2 Recurrent Tumor Distributions (n=61) |
Oncologic Outcomes After Recurrence
After a median follow-up time of 50 months (range, 9–178) after recurrence, 28 patients (62.2%) were dead from disease. Seven patients (15.6%) were still alive with disease while 10 patients (22.2%) remained disease-free. For the group as a whole, the median PFS 2 and PRS was 15 months (range, 0–96), and 24 months (range, 3–159), respectively. A total of eight patients (17.8%) had a prolonged disease-free interval after recurrence (PFS 2 > 30 months). Supplementary Table S1 shows the specific detail of the eight patients. Notably, three patients presented platinum-resistant recurrence.
Table 3 demonstrates the survival analyses. On univariate analysis, patients with single-site recurrence had significantly better survival outcome including PFS 2 (P=0.023), PRS (P=0.004), and OS (P=0.029). Patients who achieved complete resection at secondary debulking tended to have longer PFS 2 with statistic significance (P=0.017). Regarding overall survival, FIGO stage, platinum response and number of relapsed lesions were significant predictors. Figure 1 depicts the representative Kaplan-Meier survival curves. Specifically, the median disease-free survival of patients with R0 resection was 17.0 months. Concerning patients with localized recurrence, the median PFS 2 and PRS were 19.0 months, 43.0 months, respectively. In contrast, the median PFS 2 and PRS were 11.0 months and 23.0 months for patients with multiple tumors. There was no difference in survival between patients who recurred within and those out of pelvis. The prognostic relevance of the site of relapse was not assessed due to small sample size.
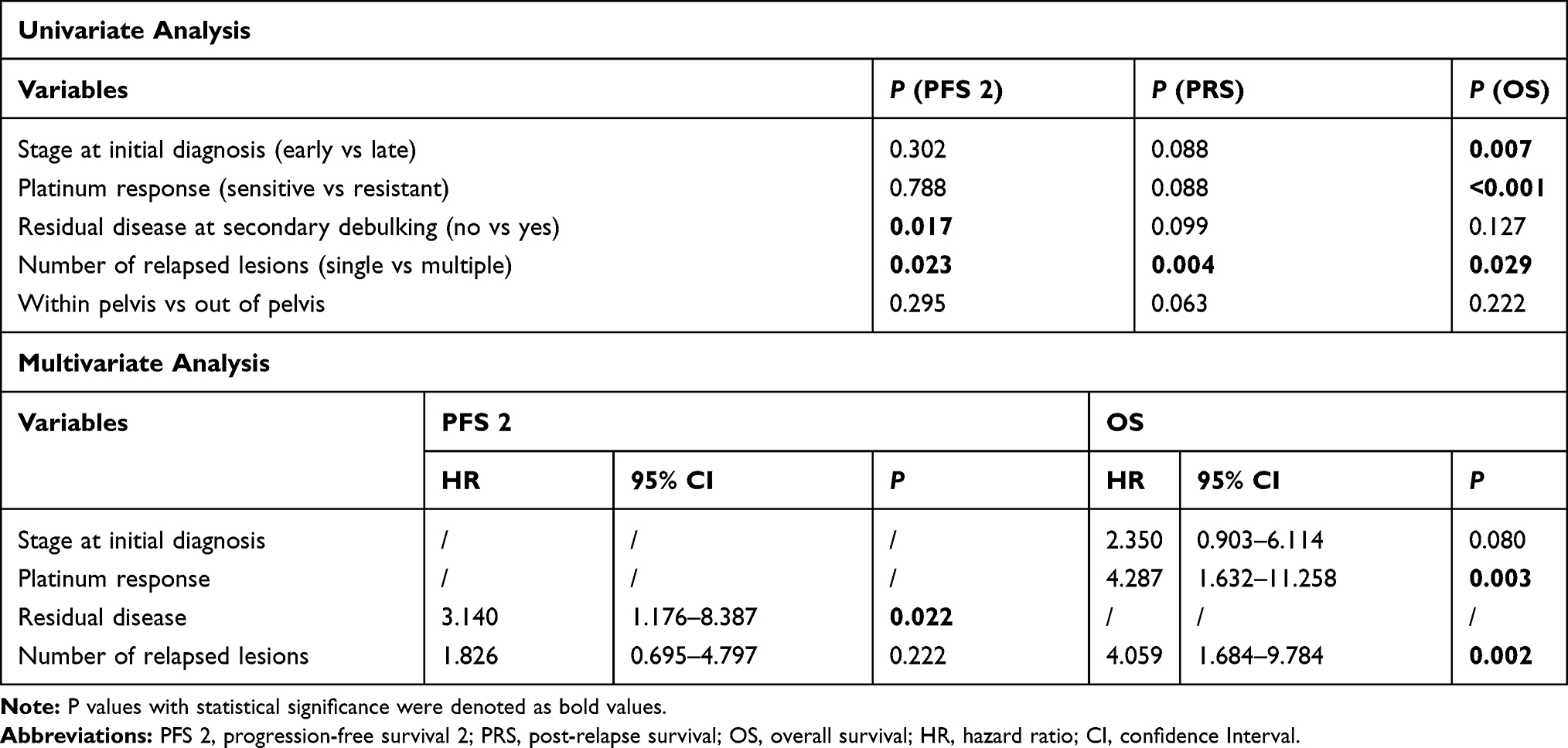 |
Table 3 Survival Analyses |
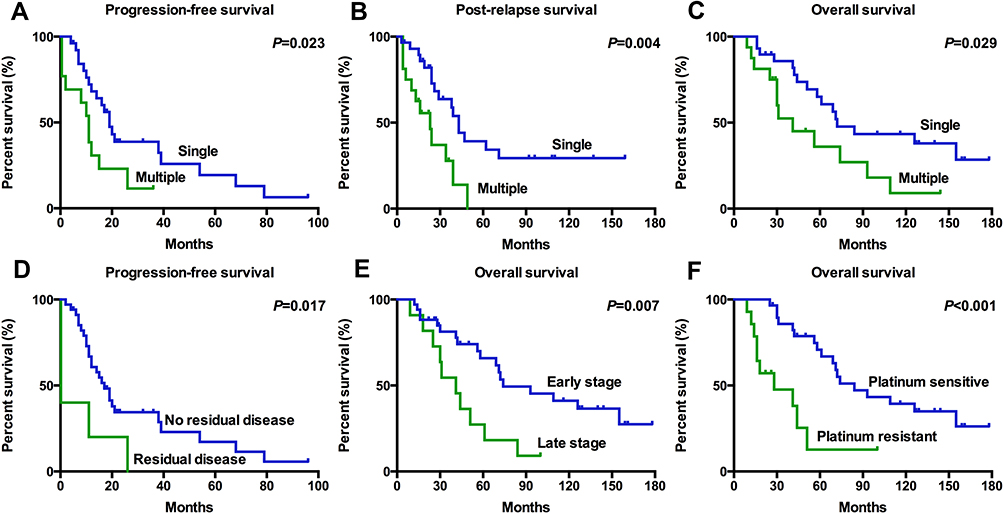 |
Figure 1 Representative Kaplan-Meier survival curves. (A–C), patients with single-site recurrence had better survival concerning progression-free survival after first recurrence (A), post-relapse survival (B) and overall survival (C). (D) Patients who achieved complete resection at secondary debulking had longer progression-free survival after recurrence. (E, F), patients with early-stage disease (E) and platinum-sensitive recurrence (F) had better overall survival. |
In the Cox regression analysis, complete resection at recurrence remained as an independent positive predictor for PFS 2 (P=0.022, Hazard Ratio [HR] 3.140, 95% Confidence Interval [CI]=1.176–8.387). For overall survival, both platinum response (P=0.003, HR 4.287, 95% CI=1.632–11.258) and number of relapsed lesions (P=0.002, HR 4.059, 95% CI=1.684–9.784) retained significance.
We noted that there were 10 patients who underwent two or three operations for recurrent disease. Supplementary Table S2 illustrates the clinicopathological characteristics and survival outcome of the 10 patients. Interestingly, six patients experienced solitary pelvic recurrence at each time. Two patients had unique recurrence site: one in vulvar (patient No. 2) and another in breast (patient No. 5).
Discussion
The role of secondary debulking surgery for recurrent ovarian cancer has been evaluated in two large-scale multi-center surgical trials (DESKTOP III12 and GOG-021313). The median PFS increased from 14.0 to 19.6 months in DESKTOP III12 while only 16.5 to 18.2 months in GOG-0213.13 The difference might be due to different clinical practice and patient population.14 It is not hard to understand that these prospective studies included a limited number of recurrent OCCC patients due to disease rarity.15,16 One recent retrospective study collected recurrent OCCC cases from Tokai Ovarian Tumor Study Group (Nagoya University Hospital and 13 affiliated institutions) between 1990/01 and 2015/12.10 A total of 25 patients who received secondary surgery and 144 patients with medical treatment only were analyzed.10 They concluded that patients with intraperitoneal recurrence or incomplete tumor resection had the worst survival after secondary debulking.10 Besides, patients who received secondary cytoreductive surgery tended to have longer post-recurrent survival compared to those who received salvage chemotherapy only (21.2 months vs 15.7 months) although statistic significance was not achieved.10
Our study is one of the largest retrospective series of OCCC patients to explore the pattern of first recurrence and the value of secondary surgery. Quite in line with our previous work, the most common sites of first recurrence were pelvis and lymph node.17 Given that only surgical candidates were involved in the study, the recurrence pattern could not represent the whole picture. Hogen et al studied the recurrence mode of 61 OCCC patients to find that 38 (62%) patients had multiple-site recurrence, 12 (20%) had single-site recurrence, and 11 (18%) had nodal recurrence only.4 Interestingly, we observed unique recurrence sites including abdominal wall, vulvar and breast. In terms of post-recurrent oncologic outcome, we confirmed the favorable prognosis of OCCC patients with localized relapse, reporting a median PFS 2 and PRS of 19 and 43 months, respectively. In other words, 50% of patients had a median PRS 2 times longer than PFS 2. Besides, complete resection at recurrence proved to be an independent positive predictor for PFS 2. It is noteworthy that 10 patients received two to three operations for recurrent disease. Six patients experienced localized pelvic relapse at each time, which might support the concept that OCCC has a predilection for pelvic failure in line with previous publications.18,19
However, we should be aware that the conclusions from this study could not be extrapolated to all recurrent OCCC patients. A significant part of the patients were not suitable for secondary surgery and might receive systematic treatment. We reviewed the publications and listed some representative studies focusing on the treatment of recurrent OCCC in Table 4. Westhoff et al reported radiation therapy in a well-selected group of patients (n=24) and the five-year survival after recurrence was 62.9%.20 Of all, 62.5% patients had focal recurrence and 73.9% underwent surgery with or before their treatment.20 Quite a few relatively large-size retrospective studies evaluated different regimens and combinations of chemotherapy for recurrent or persistent OCCC.21–24 Disappointedly, similar conclusions were arrived that most chemotherapeutic regimens have little or no effect.21–24 Recently, three prospective clinical trials have been published, focusing on the efficacy of novel biologic agents for recurrent OCCC.7–9 Sunitinib is a highly potent, selective tyrosine kinase inhibitor (TKI), including vascular endothelial growth factor receptor (VEGF-R) and platelet-derived growth factor receptor (PDGF-R).25 The response rate of sunitinib monotherapy in second-line treatment of metastatic renal cell cancer is 34%.25 Nonetheless, in GOG-254 study including 30 recurrent OCCC cases, sunitinib demonstrated minimal activity in the second- and third-line treatment. The median PFS and OS were 2.7 months and 12.8 months, respectively.7 Cabozantinib, another TKI targeting mesenchymal–epithelial transition factor (MET) and VEGF-R, showed minimal activity in 13 OCCC patients in NRG-GY001 trial.8 ENMD-2076, a novel agent targeting Aurora A and VEGF-R, failed to meet the preset bar for efficacy in recurrent OCCC.9 However, the authors noticed that loss of AT-Rich Interactive Domain 1A (ARID1A) expression correlated with better PFS on ENMD-2076 and might warrant further investigation.9
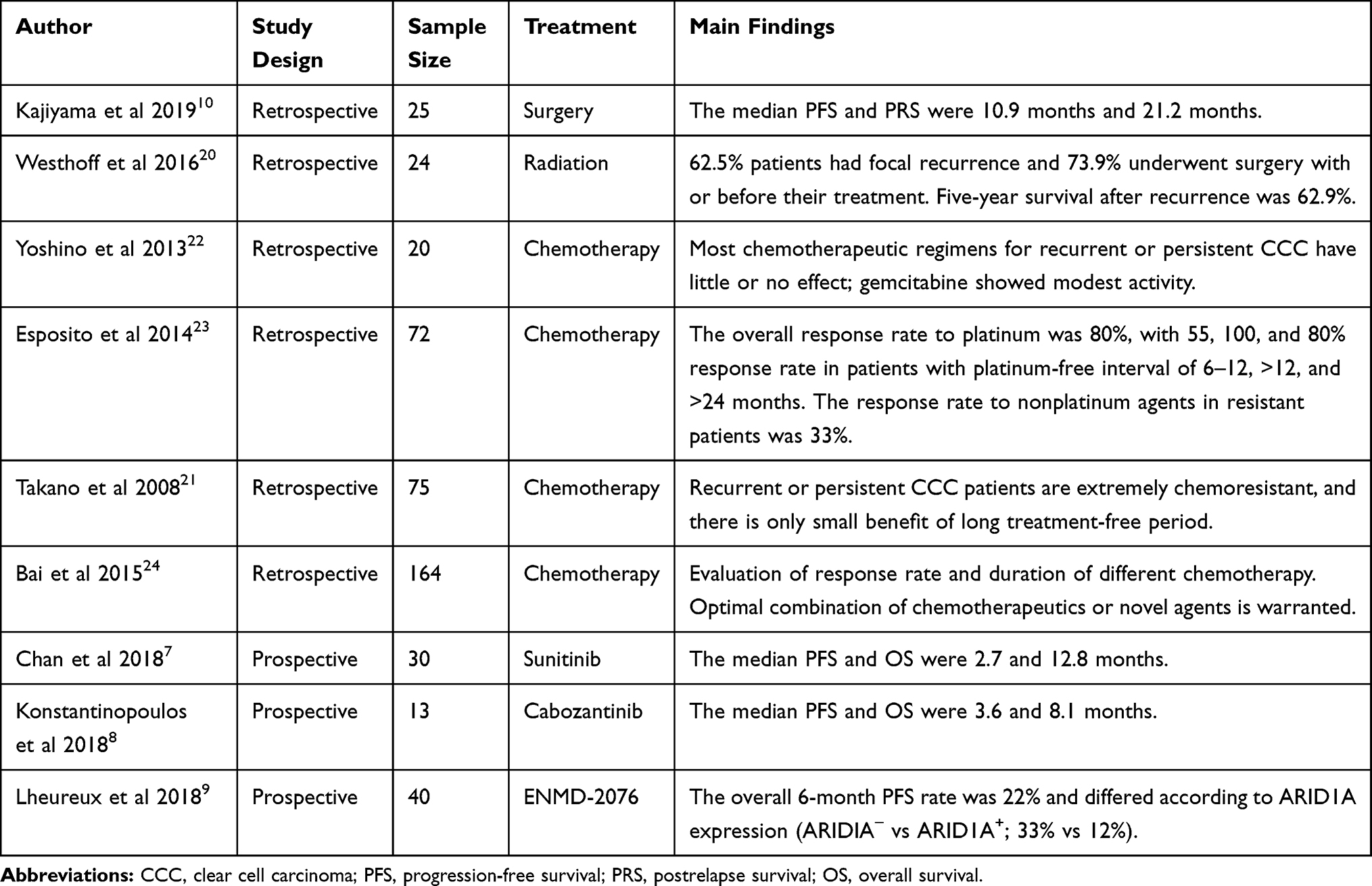 |
Table 4 A Review of Representative Studies Focusing on the Treatment of Recurrent Ovarian Clear Cell Carcinoma |
The study has several limitations. First, the cohort was limited by the selection and surveillance biases often associated with studies from a single academic institution. Second, given that some patients received post-operative treatment in local hospitals, the specific information of second-line chemotherapy was not evaluated in the study, which might be a confounding factor. Last, considering disease rarity, we collected the cases over a long period of time, which might lead to treatment heterogeneity and inconsistency.
Conclusion
We demonstrated the value of secondary cytoreductive surgery in a well-selected population of recurrent OCCC patients. Recurrence in a single anatomic site is associated with a favorable survival. Complete resection of tumors at recurrence might warrant a clinical benefit of longer disease-free survival.
Abbreviations
OCCC, ovarian clear cell carcinoma; FIGO, The International Federation of Gynecology and Obstetrics; PFS, Progression-free survival; OS, overall survival; PRS, post-relapse survival; HR, hazard ratio; CI, confidence interval; TKI, tyrosine kinase inhibitor; VEGF-R, vascular endothelial growth factor receptor; PDGF-R, Platelet-Derived Growth Factor Receptor; MET, mesenchymal–epithelial transition; ARID1A, AT-Rich Interactive Domain 1A.
Ethics Approval and Consent to Participate
The study was approved by the Fudan University Shanghai Cancer Center review board and the requirement for written informed consent was waived due to its retrospective design.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Anglesio MS, Carey MS, Kobel M, Mackay H, Huntsman DG. Clear cell carcinoma of the ovary: a report from the first Ovarian Clear Cell Symposium, June 24th, 2010. Gynecol Oncol. 2011;121:407–415. doi:10.1016/j.ygyno.2011.01.005
2. Del Carmen MG, Birrer M, Schorge JO. Clear cell carcinoma of the ovary: a review of the literature. Gynecol Oncol. 2012;126:481–490. doi:10.1016/j.ygyno.2012.04.021
3. Sung P-L, Chang Y-H, Chao K-C, Chuang C-M. Global distribution pattern of histological subtypes of epithelial ovarian cancer: a database analysis and systematic review. Gynecol Oncol. 2014;133:147–154. doi:10.1016/j.ygyno.2014.02.016
4. Hogen L, Vicus D, Ferguson SE, et al. Patterns of recurrence and impact on survival in patients with clear cell ovarian carcinoma. Int J Gynecol Cancer. 2019;29:1164–1169. doi:10.1136/ijgc-2019-000287
5. Kajiyama H, Shibata K, Mizuno M, et al. Postrecurrent oncologic outcome of patients with ovarian clear cell carcinoma. Int J Gynecol Cancer. 2012;22:801–806. doi:10.1097/IGC.0b013e3182540145
6. Crotzer DR, Sun CC, Coleman RL, Wolf JK, Levenback CF, Gershenson DM. Lack of effective systemic therapy for recurrent clear cell carcinoma of the ovary. Gynecol Oncol. 2007;105:404–408. doi:10.1016/j.ygyno.2006.12.024
7. Chan JK, Brady W, Monk BJ, et al. A phase II evaluation of sunitinib in the treatment of persistent or recurrent clear cell ovarian carcinoma: an NRG Oncology/Gynecologic Oncology Group Study (GOG-254). Gynecol Oncol. 2018;150:247–252. doi:10.1016/j.ygyno.2018.05.029
8. Konstantinopoulos PA, Brady WE, Farley J, Armstrong A, Uyar DS, Gershenson DM. Phase II study of single-agent cabozantinib in patients with recurrent clear cell ovarian, primary peritoneal or fallopian tube cancer (NRG-GY001). Gynecol Oncol. 2018;150:9–13. doi:10.1016/j.ygyno.2018.04.572
9. Lheureux S, Tinker AV, Clarke BA, et al. A clinical and molecular Phase II trial of oral ENMD-2076 in ovarian clear cell carcinoma (OCCC): a study of the Princess Margaret Phase II Consortium. Clin Cancer Res. 2018:
10. Kajiyama H, Suzuki S, Yoshikawa N, et al. Oncologic outcomes after secondary surgery in recurrent clear-cell carcinoma of the ovary. Int J Gynecol Cancer. 2019;29:910–915. doi:10.1136/ijgc-2018-000142
11. FIGO Committee on Gynecologic Oncology. FIGO staging for carcinoma of the vulva, cervix, and corpus uteri. Int J Gynaecol Obstet. 2014;125:97–98. doi:10.1016/j.ijgo.2014.02.003
12. Du Bois A, Vergote I, Ferron G, et al. Randomized controlled Phase III study evaluating the impact of secondary cytoreductive surgery in recurrent ovarian cancer: AGO DESKTOP III/ENGOT ov20. J Clin Oncol. 2017;35 suppl:5501. doi:10.1200/JCO.2017.35.15_suppl.5501
13. Coleman RL, Spirtos NM, Enserro D, et al. Secondary surgical cytoreduction for recurrent ovarian cancer. N Engl J Med. 2019;381:1929–1939. doi:10.1056/NEJMoa1902626
14. Zang R, Zhu J. Which patients benefit from secondary cytoreductive surgery in recurrent ovarian cancer? J Gynecol Oncol. 2019;30:e116. doi:10.3802/jgo.2019.30.e116
15. Coleman RL, Brady MF, Herzog TJ, et al. Bevacizumab and paclitaxel-carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic Oncology Group study GOG-0213): a multicentre, open-label, randomised, Phase 3 trial. Lancet Oncol. 2017;18:779–791. doi:10.1016/S1470-2045(17)30279-6
16. Bommert M, Harter P, Heitz F, Du Bois A. When should surgery be used for recurrent ovarian carcinoma? Clin Oncol (R Coll Radiol). 2018;30:493–497. doi:10.1016/j.clon.2018.04.006
17. Ye S, Liu S, Xiang L, Wu X, Yang H. (18)F-FDG PET/CT-based metabolic metrics in recurrent tumors of ovarian clear cell carcinoma and their prognostic implications. BMC Cancer. 2019;19:226. doi:10.1186/s12885-019-5441-7
18. Hoskins PJ, Le N, Gilks B, et al. Low-stage ovarian clear cell carcinoma: population-based outcomes in British Columbia, Canada, with evidence for a survival benefit as a result of irradiation. J Clin Oncol. 2012;30:1656–1662. doi:10.1200/JCO.2011.40.1646
19. Macrie BD, Strauss JB, Helenowski IB, et al. Patterns of recurrence and role of pelvic radiotherapy in ovarian clear cell adenocarcinoma. Int J Gynecol Cancer. 2014;24:1597–1602. doi:10.1097/igc.0000000000000270
20. Westhoff GL, Fuh KC, Longacre TA, et al. Radiation therapy for recurrent clear-cell cancer of the ovary. Int J Gynecol Cancer. 2016;26:1608–1614. doi:10.1097/IGC.0000000000000810
21. Takano M, Sugiyama T, Yaegashi N, et al. Low response rate of second-line chemotherapy for recurrent or refractory clear cell carcinoma of the ovary: a retrospective Japan clear cell carcinoma study. Int J Gynecol Cancer. 2008;18:937–942. doi:10.1111/j.1525-1438.2007.01158.x
22. Yoshino K, Enomoto T, Fujita M, et al. Salvage chemotherapy for recurrent or persistent clear cell carcinoma of the ovary: a single-institution experience for a series of 20 patients. Int J Clin Oncol. 2013;18:148–153. doi:10.1007/s10147-011-0357-5
23. Esposito F, Cecere SC, Magazzino F, et al. Second-line chemotherapy in recurrent clear cell ovarian cancer: results from the multicenter italian trials in ovarian cancer (MITO-9). Oncology. 2014;86:351–358. doi:10.1159/000358730
24. Bai H, Sha G, Cao D, et al. Salvage chemotherapy for patients with recurrent or persistent ovarian clear cell carcinoma: a retrospective study of 164 cases. Medicine (Baltimore). 2015;94:e1121. doi:10.1097/MD.0000000000001121
25. Motzer RJ, Michaelson MD, Redman BG, et al. Activity of SU11248, a multitargeted inhibitor of vascular endothelial growth factor receptor and platelet-derived growth factor receptor, in patients with metastatic renal cell carcinoma. J Clin Oncol. 2006;24:16–24. doi:10.1200/JCO.2005.02.2574
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.