Back to Journals » Infection and Drug Resistance » Volume 12
Rectovaginal Colonization With Pathogenic Escherichia coli During Pregnancy And Neonatal Outcomes
Authors Liu TH, Wang HP, Cho FN, Wang JL ![]() , Hung CH, Chiou YH, Chen YS
, Hung CH, Chiou YH, Chen YS ![]() , Lee SSJ
, Lee SSJ ![]() , Cheng MF
, Cheng MF ![]()
Received 7 March 2019
Accepted for publication 13 September 2019
Published 30 September 2019 Volume 2019:12 Pages 3103—3112
DOI https://doi.org/10.2147/IDR.S207857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Tzu-Hao Liu,1,2 Hsiao-Ping Wang,1,3 Fu-Nang Cho,3,4 Jiun-Ling Wang,5,6 Chih-Hsin Hung,7 Yee-Hsuan Chiou,1,3 Yao-Shen Chen,3,8 Susan Shin-Jung Lee,3,8 Ming-Fang Cheng1,3,7,9
1Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung 81362, Taiwan; 2Department of Pediatrics, Zuoying Branch of Kaohsiung Armed Forces General Hospital, Kaohsiung 81342, Taiwan; 3School of Medicine, National Yang-Ming University, Taipei 11221, Taiwan; 4Department of Obstetrics and Gynecology, Kaohsiung Veterans General Hospital, Kaohsiung 81362, Taiwan; 5Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan 70101, Taiwan; 6Department of Medicine, College of Medicine, National Cheng Kung University, Tainan 70101, Taiwan; 7Department of Chemical Engineering and Institute of Biotechnology and Chemical Engineering, I-Shou University, Kaohsiung 84001, Taiwan; 8Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung 81362, Taiwan; 9School of Nursing, Fooyin University, Kaohsiung 83102, Taiwan
Correspondence: Ming-Fang Cheng
Department of Pediatrics, No. 386, Dazhong 1st Road, Zuoying District, Kaohsiung 813, Taiwan
Tel +886-7342-2121
Fax +886-7346-8207
Email [email protected]
Purpose: The role of pathogenic Escherichia coli colonization in asymptomatic pregnant women is not well understood. The purpose of this work was to determine the prevalence, antimicrobial susceptibility, and neonatal outcomes of pathogenic E. coli colonization in pregnant women.
Patients and methods: A total of 137 women from southern Taiwan with singleton pregnancies were enrolled between March 2016 and June 2017. The women were prospectively screened for E. coli colonization in the rectovaginal region during prenatal examination. The exclusion criteria are twin pregnancy of the mother and major anomaly of the neonate. All E. coli isolates were identified as either pathogenic or commensal strains, and their susceptibility to various antimicrobials was investigated. Clinical data of the infants were retrieved from their medical records.
Results: Results showed that 35.8% of asymptomatic pregnant women had pathogenic E. coli colonization in the rectovaginal region. Neonates born to such mothers showed significant morbidities, including hospitalization (OR= 3.74, 95% CI= 1.18∼11.87), hyperbilirubinemia (OR= 2.81, 95% CI= 1.24∼6.38), and gastrointestinal symptoms (OR= 5.53, 95% CI= 1.39∼21.94). Maternal colonization with pathogenic E. coli at rectoanal site was a risk factor for neonatal hyperbilirubinemia after Benjamini–Hochberg (BH) adjustment (52% vs 24%, adjusted P= 0.048).
Conclusion: The prevalence of pathogenic E. coli colonization in Taiwanese asymptomatic pregnant women was high, and the neonates born to colonized mothers exhibited potential neonatal morbidities. Larger studies are necessary to confirm these findings.
Keywords: maternal-neonatal transmission, respiratory distress, hyperbilirubinemia, gastrointestinal symptoms
Introduction
Escherichia coli is a commensal bacterium generally found in human and animal intestines. Most E. coli strains are harmless, but some strains that possess specific virulence factors are pathogenic and are associated with various infectious diseases in humans. Pathogenic E. coli strains are broadly classified based on the sites of infection into strains that primarily cause gastrointestinal diseases or extraintestinal infections. Based on the characteristics of clinical disease presentation and their virulence factors, these pathogenic E. coli strains can be further categorized into the following six pathotypes: 1) enteroaggregative E. coli (EAEC), 2) enterohemorrhagic E. coli (EHEC), 3) enteroinvasive E. coli (EIEC), 4) enteropathogenic E. coli (EPEC), 5) enterotoxigenic E. coli (ETEC), and 6) extraintestinal pathogenic E. coli (ExPEC).1
Group B Streptococcus (GBS) and E. coli are the leading causes of early-onset neonatal sepsis,2,3 resulting in severe complications and sequelae.4 Transmission of either of these pathogens from the colonized maternal genital tract to the fetus before or during labor is currently considered the route of bacterial acquisition in neonates.5–7 Accordingly, guidelines for the prevention of neonatal GBS infections by reducing vertical transmission from mothers colonized with GBS have been well established8,9 and have substantially reduced the incidence of neonatal GBS sepsis.10 However, E. coli remains the most significant pathogen of neonatal sepsis in preterm infants, who are more likely to develop a fulminant illness with fatality.3 As a definite relationship between neonatal morbidities and maternal–neonatal transmission of E. coli has not yet been established, protocols for preventing neonatal infections caused by E. coli are not currently available. To our knowledge, this is the first study to focus on maternal colonization with pathogenic E. coli and the subsequent neonatal outcomes. Therefore, we investigated the prevalence, antimicrobial susceptibility, and influences on subsequent neonatal outcomes of pathogenic E. coli colonization in pregnant women.
Materials And Methods
Study Design And Subjects
Annually, 600 children are delivered at the Kaohsiung Veterans General Hospital, a 1400-bed medical center in southern Taiwan that provides both primary and tertiary medical care. The hospital has a tertiary level Neonatal Intensive Care Unit, with an average of 400 admissions per year, and treats all infants from gestational week 23. The hospital’s Institutional Review Board approved this study (VGHKS16-CT2-04), and written informed consent was obtained from all the study participants. This study was conducted in accordance with the Declaration of Helsinki. The sample size was determined by using two population proportion formula with the assumption of 20% prevalence of preterm birth in case group, 10% prevalence of preterm birth in control group, 95% confidence level, and 80% POWER. The sample size was calculated to be 197.11,12 From March 2016 to June 2017, 161 pregnant women were enrolled after obtaining their informed consent in this prospective study. Vaginal and rectal samples were obtained from the participants during their routine prenatal examination from 7 to 39 weeks of gestation. Up to four samples were collected at different time points from each participant. When vaginal and rectal samples yielded positive results for E. coli, the participants were considered colonized with E. coli. Initially, 161 pregnant women participated in our study. Nineteen pregnant women were excluded before delivery because of elective abortion or loss of follow-up at our hospital. Five pregnant women were excluded after delivery because of twin pregnancies and major anomalies in the newborns (Figure 1). At the end of the study period, 137 qualified pregnant women were enrolled in our study. These women gave birth to singletons in our hospital between March 2016 and June 2017. The 137 neonates received routine newborn care in our baby room, and some were hospitalized in the sick-baby room and neonatal intensive care unit because of illness, according to their clinical condition, within 28 days of birth.
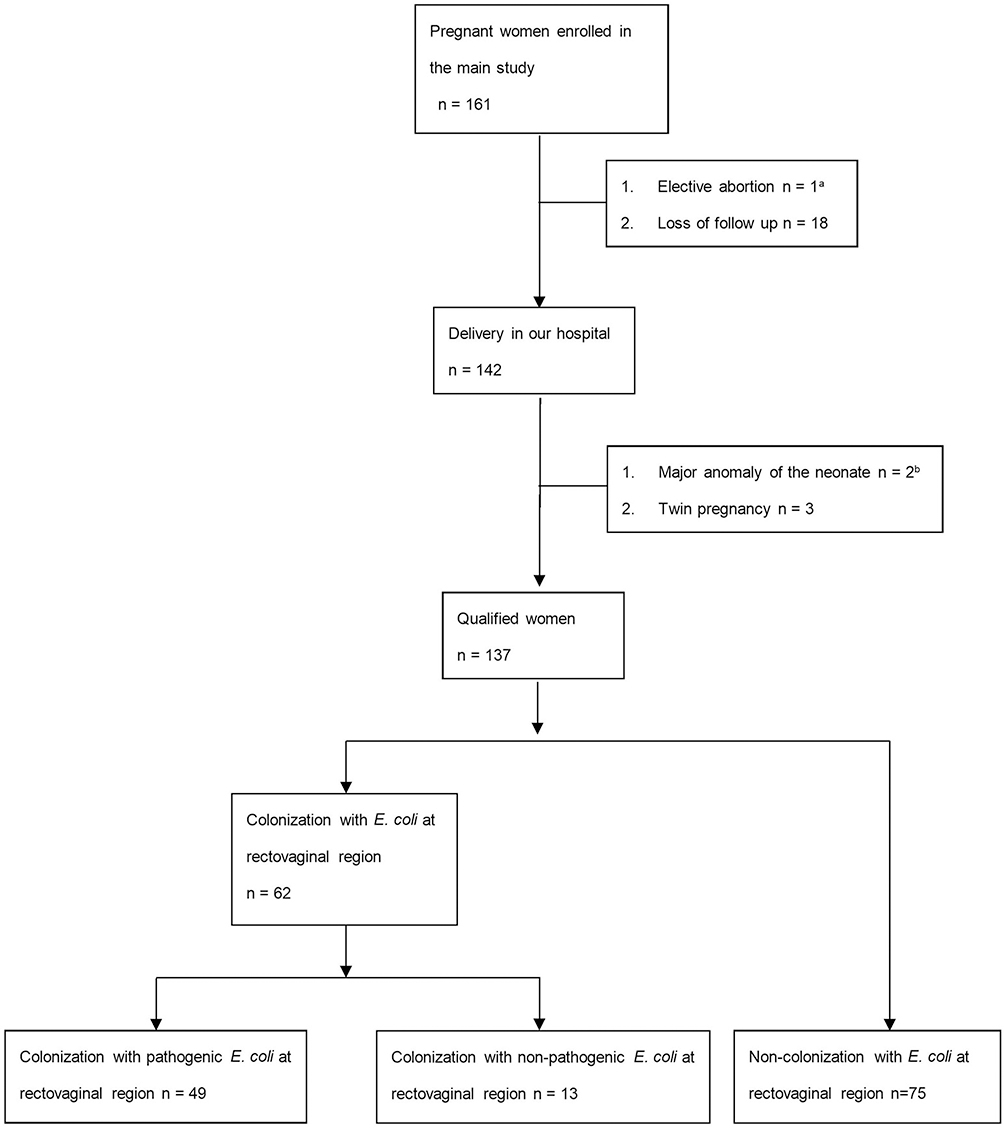 |
Figure 1 Patient flow diagram for E. coli screening among pregnant women. Notes: aElective abortion because of severe ventriculomegaly of the fetus. bMajor anomaly of two neonates due to (1) right lung aplasia and (2) hypoplastic left heart syndrome. |
Sampling And Culture Conditions
Vaginal and rectal samples from pregnant women were collected with cotton swabs. Sampling was performed by an obstetrician, and the swabs were transported in a COPAN Transystem® (Copan Diagnostics, Inc., Brescia, Italy). Initially, the swab samples were plated on CHROMagar Salmonella PLUS (Taiwan Prepared Media, Taipei, Taiwan) and incubated without CO2 for 12–16 hrs at 35–37°C. A selected colony was plated on agar plates (Oxoid, Basingstoke, UK) with Luria-Bertani medium (Sigma-Aldrich, St. Louis, USA) for purification. Each of these colonies were subcultured three more times. Five of the isolated strains were plated on E. coli CHROMagar (ECC) plates (CHROMagar, Paris, France) to reconfirm the presence of E. coli and incubated without CO2 for 12–16 hrs at 35–37°C. Finally, two colonies of E. coli were randomly selected for pathotype identification and antimicrobial susceptibility.
Study Definitions
Pathogenic E. coli strains were identified using a multiplex polymerase chain reaction (PCR) assay with primers for detecting genes encoding the following diarrheagenic virulence factors: heat labile enterotoxin (estA) and heat stabile enterotoxin (eltB) for ETEC, invasion plasmid antigen (ipaH) for EIEC, aggregative virulence regulator (aggR) for EAEC,1 and intimin (eae) plus shigatoxin (stx1 or stx2) for EHEC.13 ExPEC was defined as harboring more than two of the following five genes: P fimbriae (papA), S and F1C fimbriae (sfaS/focG), Dr-binding adhesins (afa), aerobactin system (iutA), and group 2 polysaccharide capsule (kpsM II).14
Clinical Data
Subject information regarding age, ethnicity, educational level, use of antimicrobials and probiotics, and pets at home for the past 3 months was obtained via questionnaires prior to sampling. Maternal GBS screening results and clinical data were retrieved from the maternal medical records. Clinical data on infants were retrieved from their medical records and were analyzed for the occurrence of any clinical symptoms within 28 days of birth. Neonatal outcome was defined as illness developed within 28 days after birth. Hospitalization was defined as hospitalization because of clinical illness in need of further evaluation and management. Perinatal infection was defined as the presence of clinical symptoms or signs of sepsis. Respiratory distress was defined as ground glass pattern observed via chest X-ray and clinically confirmed by a neonatologist. Hyperbilirubinemia was defined as the level of total serum bilirubin (TSB) exceeding the normal range and in need of further phototherapy according to American Academy of Pediatrics guideline.15 Gastrointestinal symptoms were defined as the presence of vomiting, diarrhea, feeding intolerance, or gastrointestinal bleeding.
Statistical Analyses
All statistical analyses were performed using Stata/SE 12.1 for Windows 7 (StataCorp., College Station, Texas, USA). Continuous variables were expressed as mean value (standard deviation) and were compared using a two-tailed t-test. Categorical variables were expressed as number (percentage) and were compared using chi-square test or Fisher’s exact test. A P-value < 0.05 was considered statistically significant. Benjamini–Hochberg (BH) adjustment was applied for multiple comparison in Tables 3 and 4 separately.16
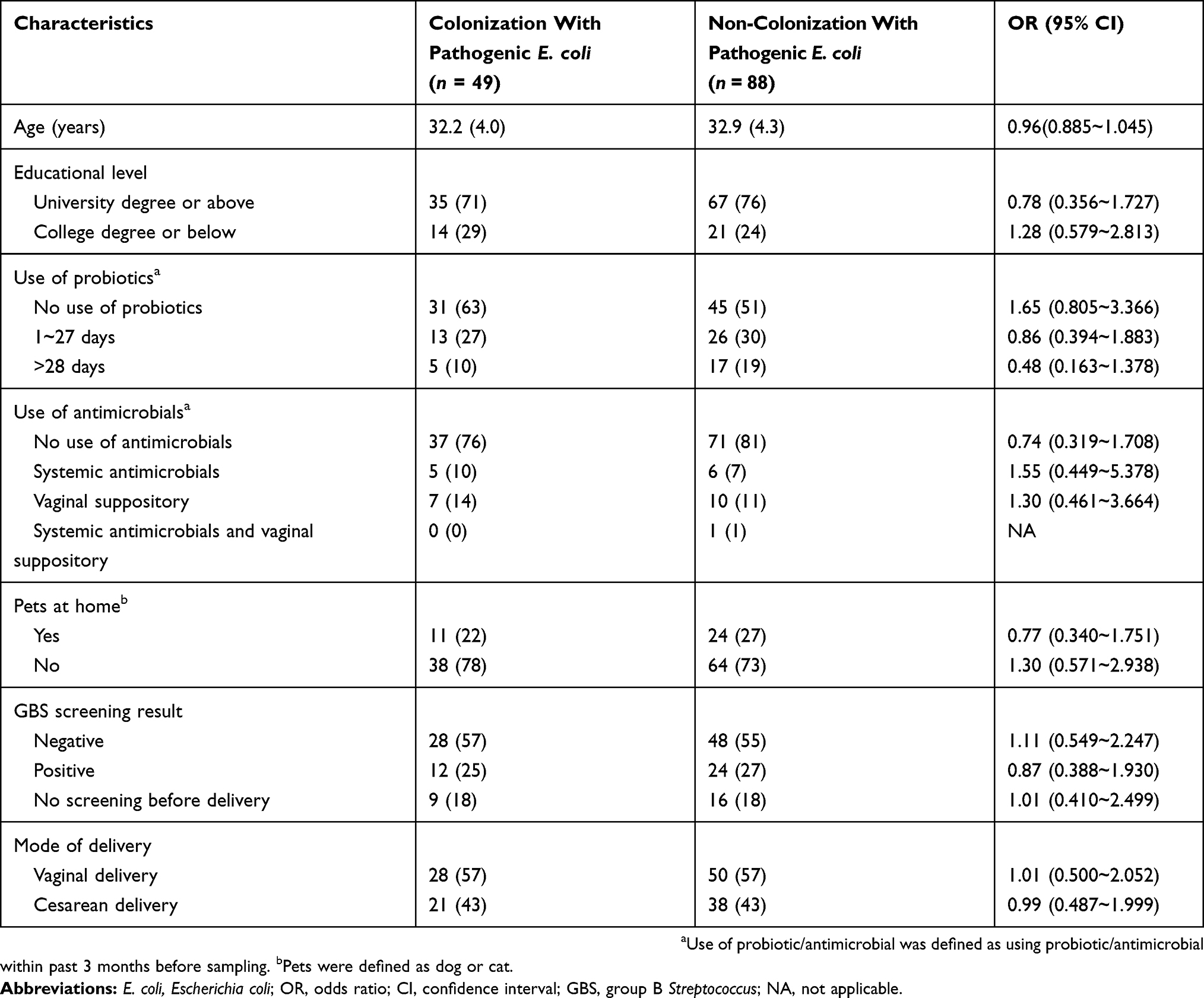 |
Table 1 Maternal Characteristics Of The Pregnant Women Included In This Study |
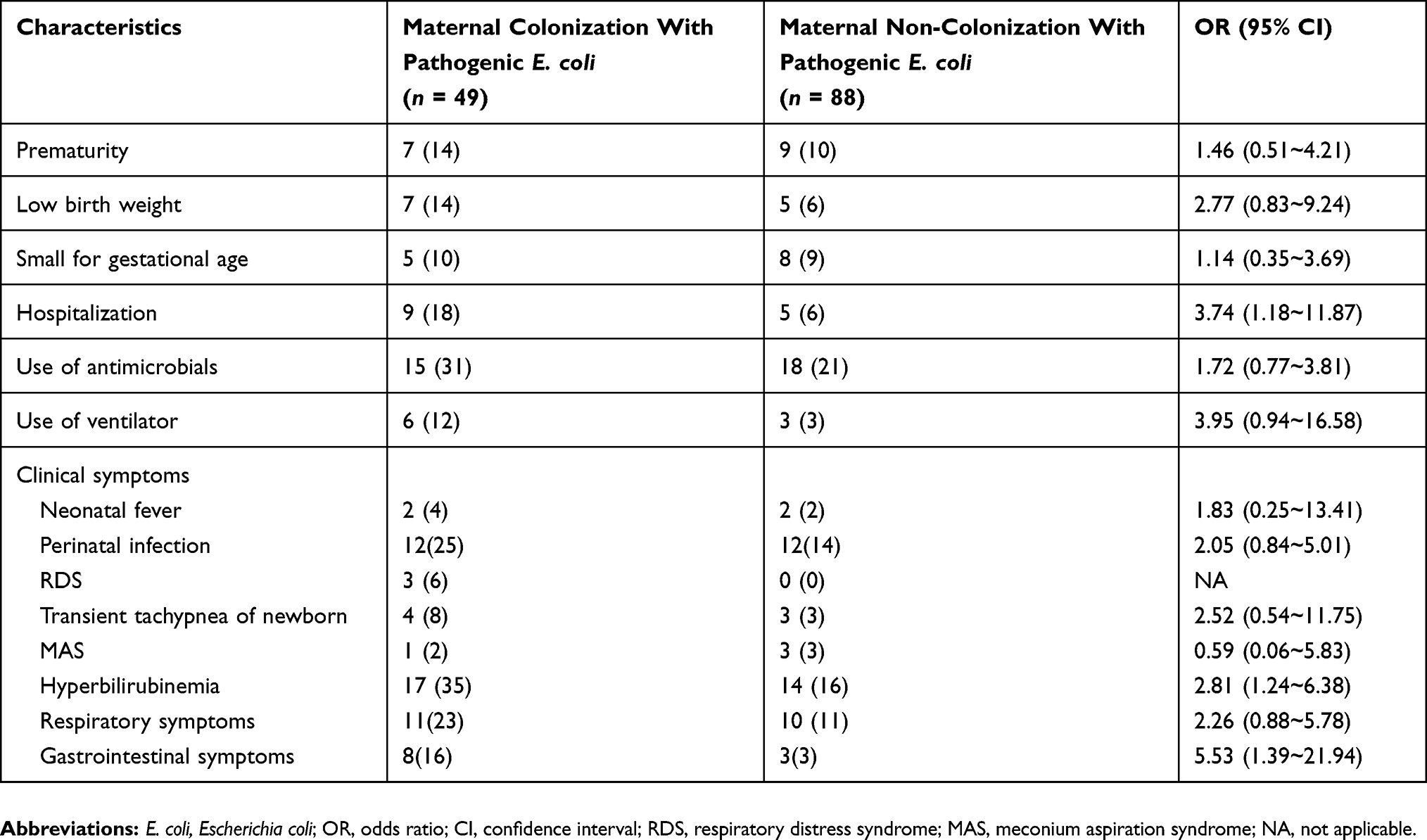 |
Table 2 Descriptive Analysis Of 137 Neonates With Maternal Colonization Of Pathogenic E. coli At Kaohsiung Veterans General Hospital Between March 2016 And June 2017 |
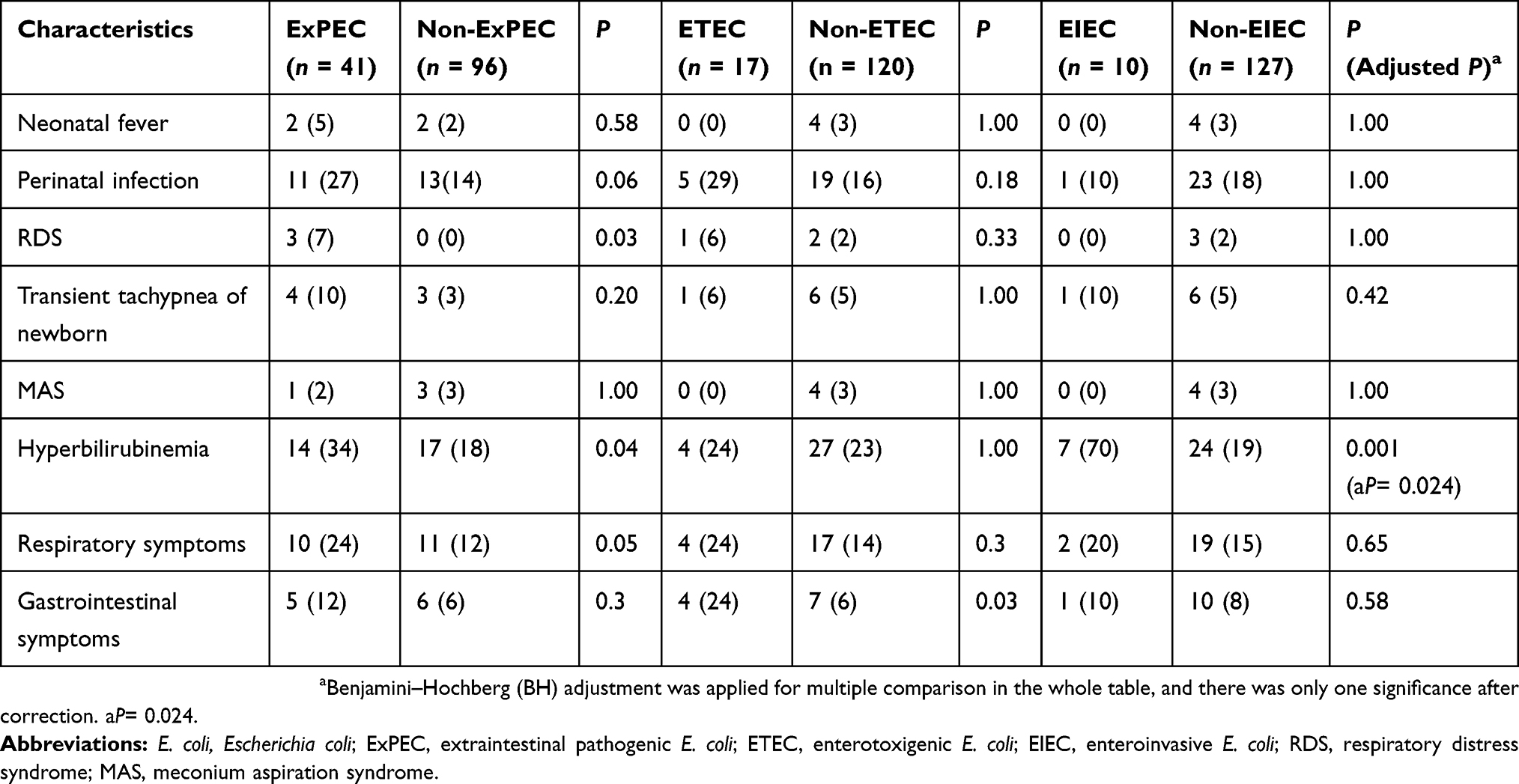 |
Table 3 Neonatal Morbidities According To Maternal Colonization With Each Pathotype Of E. coli Among 137 Pregnant Women |
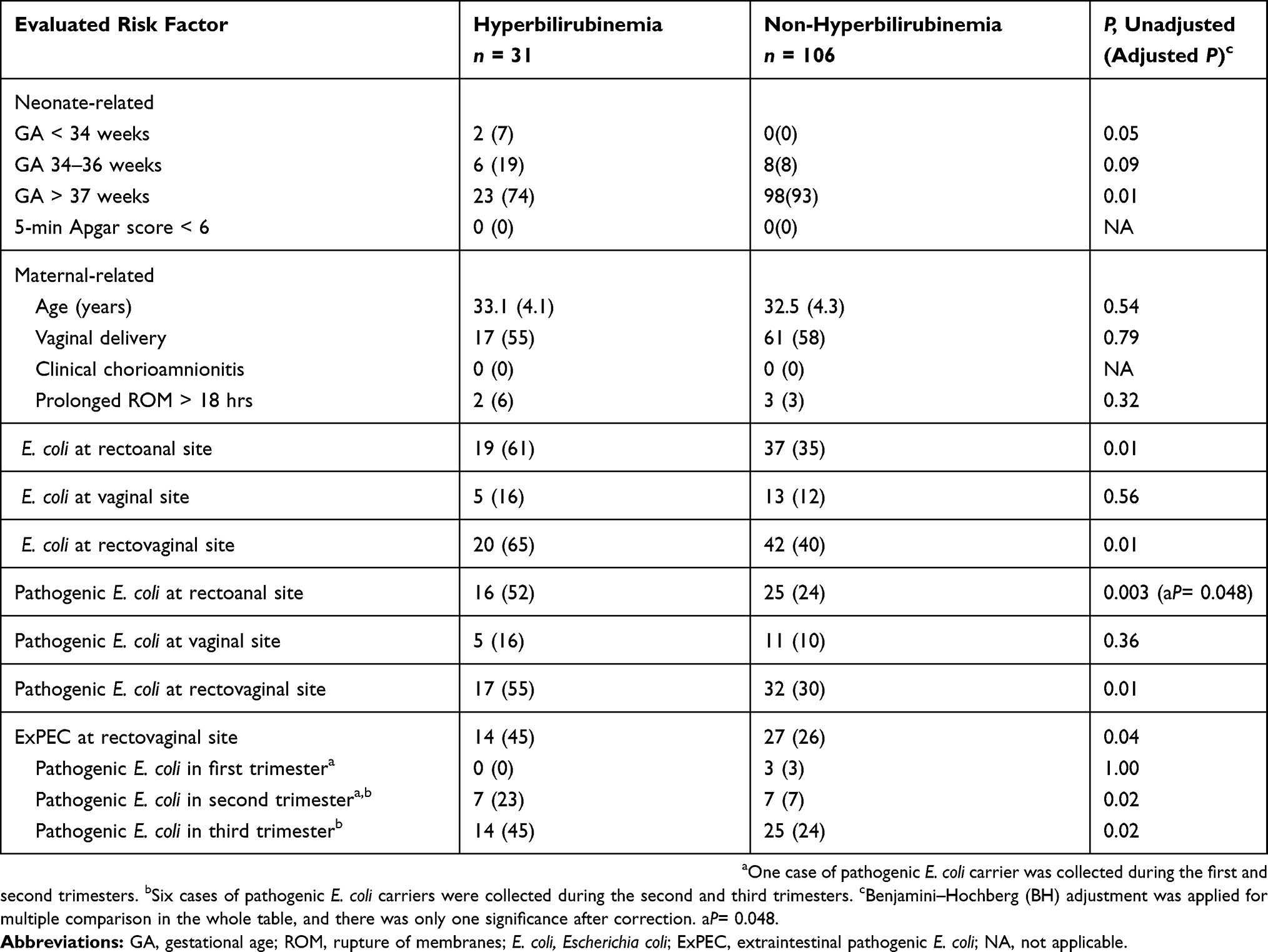 |
Table 4 Risk Factors For Hyperbilirubinemia Among 137 Singleton Neonates |
Results
Maternal Characteristics
There were no significant differences in maternal age, educational level, use of antimicrobials or probiotics within 3 months before sampling, pets at home, colonization with GBS, and mode of delivery between pregnant women with pathogenic E. coli colonization and those with no pathogenic E. coli colonization (Table 1).
Pathogenic E. Coli Colonization In Pregnant Women
Among the 137 pregnant women enrolled, 62 (62/137, 45.3%) were colonized with E. coli in the rectovaginal region, with 18 women (18/137, 13.1%) showing vaginal colonization, 56 women (56/137, 40.9%) showing rectal colonization (Table S1). Among the 62 colonized pregnant women, 49 women were colonized with pathogenic E. coli. Among these 49 women, the predominant E. coli pathotype was ExPEC (n = 41, 41/137, 29.9%), followed by ETEC (n = 17, 17/137, 12.4%), EIEC (n = 10, 10/137, 7.3%), EHEC (n = 5, 5/137, 3.6%), and EAEC (n = 2, 2/137, 1.5%) (Table S2).
Antimicrobial Susceptibility
All E. coli isolates from the 62 colonized women were analyzed for susceptibility to 18 antimicrobial agents. All isolates were found to be susceptible to cefepime, ertapenem, imipenem, amikacin, tigecycline, and colistin. The 62 E. coli-colonized women were classified into two groups based on colonization with pathogenic E. coli (n = 49) or non-pathogenic E. coli (n = 13). Compared to the non-pathogenic E. coli colonization group, antimicrobial susceptibilities were lower in the pathogenic E. coli colonization group, especially for ampicillin/sulbactam (55.1% vs 84.6%, P = 0.05), piperacillin (46.9% vs 69.2%, P = 0.15), and trimethoprim/sulfamethoxazole (63.3% vs 92.3%, P = 0.05) (Figure 2).
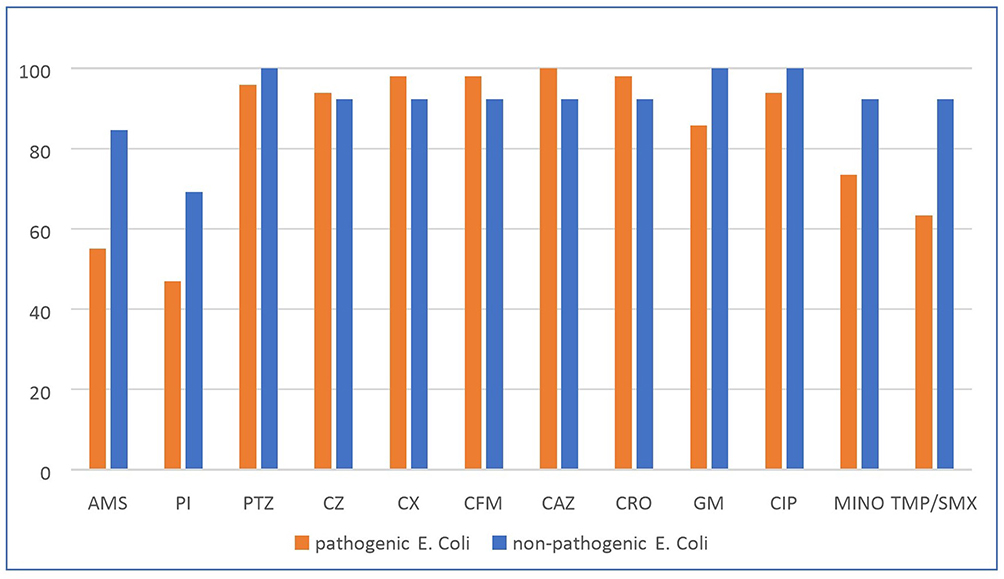 |
Figure 2 Antimicrobial susceptibility rate among pathogenic E. coli and non-pathogenic E. coli groups. Abbreviations: AMS, ampicillin/sulbactam; PI, piperacillin; PTZ, piperacillin/tazobactam; CZ, cefazolin; CX, cefoxitin; CFM, cefixime; CAZ, ceftazidime; CRO, ceftriaxone; GM, gentamicin; CIP, ciprofloxacin; MINO, minocycline; TMP/SMX, trimethoprim/sulfamethoxazole. |
Neonatal Outcomes
Among the 137 neonates, neonatal morbidities were more prevalent among neonates born to mothers with pathogenic E. coli colonization during pregnancy than among those born to mothers without pathogenic E. coli colonization (Table 2). These neonatal morbidities included prematurity, low birth weight, hospitalization (OR = 3.74, 95% CI= 1.18~11.87), respiratory distress syndrome, hyperbilirubinemia (OR= 2.81, 95% CI= 1.24~6.38), respiratory symptoms, and gastrointestinal symptoms (OR= 5.53, 95% CI= 1.39~21.94).
To better understand the relationship between neonatal outcome and each pathotype of E. coli in maternal colonization, the 137 neonates were divided into two groups for each pathotype (Table 3). Maternal colonization with EIEC during pregnancy was significantly associated with neonatal hyperbilirubinemia (adjusted P = 0.024).
Next, the association between hyperbilirubinemia and neonate- and maternal-related factors was evaluated using chi-square test or Fisher’s exact test and t-test in the 137 neonates (Table 4). There were no significant differences between hyperbilirubinemia and non-hyperbilirubinemia group in maternal age, mode of delivery, prolonged rupture of membranes, or gestational age. In addition, maternal colonization with pathogenic E. coli in the rectoanal region was a significant risk factor for hyperbilirubinemia (adjusted P = 0.048).
Among the 62 neonates born to E. coli-colonized mother, there was no significant difference in maternal preterm premature rupture of membranes and neonatal morbidities between pathogenic E. coli group and non-pathogenic E. coli group. Among the 49 neonates born to mothers with pathogenic E. coli colonization, only one case yielded E. coli colony from a pus culture obtained from a colostomy caused by necrotizing enterocolitis at 24 days of age. For the other 48 neonates, blood and cerebrospinal fluid cultures did not show positive results.
Discussion
Pathogenic E. coli include E. coli strains that possess specific virulence factors and can cause illnesses in healthy individuals, resulting in gastrointestinal diseases and extraintestinal infections.17 However, little is known about the prevalence of pathogenic E. coli colonization in the rectovaginal region during pregnancy and its subsequent neonatal outcomes. In our study, among 137 asymptomatic pregnant women, 35.8% (49/137) women were found to be colonized with pathogenic E. coli. Furthermore, pathogenic E. coli colonization was associated with neonatal morbidities. This is the first study to describe the potential companions between maternal pathogenic E. coli colonization and the neonatal outcomes. Vaginal colonization with E. coli is associated with maternal complications during pregnancy, such as premature rupture of membrane, chorioamnionitis, and preterm birth.18,19 However, these reports did not include relevant information regarding pathogenic E. coli colonization.
Several factors influence maternal E. coli colonization during pregnancy, including living with dogs and cats and the use of antibiotics during pregnancy.20,21 However, these factors did not correlate significantly with pathogenic E. coli colonization in our study. In our study, the prevalence of colonization with E. coli in the vagina was 13.1%, which was similar to data reported in earlier studies18,19 but lower than the prevalence reported in one particular study.22
Studies have shown that maternal–neonatal transmission of E. coli represents a substantial risk for infant colonization and can possibly cause further morbidity.7,22,23 The maternal–neonatal transmission rate of E. coli reportedly ranges from 21% to 35.7%22,24,25 and 17% in the setting of maternal premature rupture of membrane.26 These E. coli and even pathogenic E. coli transmitted from colonized mother may be colonized on the body surface or gastrointestinal tract of the neonate, or become pathogenic bacteria potentially, or even affect the distribution of normal flora in the respiratory tract, gastrointestinal tract or body surface. One study revealed that the presence of E. coli in the intrauterine meconium resulted from its translocation from the maternal gut.27 Due to an immature immune system and decreased placental transmission of maternal antibodies, neonates are relatively immunocompromised and more susceptible to pathogenic E. coli, resulting in severe neonatal infection.28 Approximately one-third of the pregnant women in our study were colonized with pathogenic E. coli in the rectovaginal region. Although these colonized pregnant women were asymptomatic, their neonates may be exposed to these pathogenic E. coli strains during or before vaginal delivery if pathogenic E. coli invaded the chorioamnion or the amniotic fluid.
E. coli is one of the major pathogens causing neonatal sepsis and meningitis.3 The mortality rate of neonatal meningitis in developing countries is estimated to range from 40% to 58%, compared to the mortality rate of 10% in developed countries.29 ExPEC is the main E. coli pathotype responsible for extraintestinal infections in humans and usually causes meningitis in the neonatal period.30 In our study, ExPEC was the predominant pathotype in colonized pregnant women. Neonates born to mothers with ExPEC colonization may acquire the pathogen via vertical transmission or vaginal delivery. Reports show that the virulence factor hemolysin produced by ExPEC causes surfactant dysfunction and lung injury.31 The trend in neonatal respiratory symptoms between maternal colonization and non-colonization with pathogenic E. Coli in our study might be attributed to a similar mechanism.
Diarrheagenic E. coli are easily transmitted between humans and through contaminated water in countries with a high burden of diarrheal illnesses.32 There was no epidemic spread of diarrheal illness in the period of our study; however, we observed that maternal colonization with pathogenic E. coli was associated with neonatal gastrointestinal illness. Further studies are required to determine whether the pathogenic strain of E. coli is better adapted to the colonization of neonates. In addition, we also observed a significant correlation between maternal colonization with pathogenic E. coli, especially with EIEC strains, and neonatal hyperbilirubinemia. The pathogenetic causes of neonatal unconjugated hyperbilirubinemia include increased production of bilirubin, deficiency of hepatic uptake, impaired conjugation of bilirubin, and increased enterohepatic circulation of bilirubin.33 In our study, neonates born to mothers colonized with these strains tended to show neonatal infection and were more likely to exhibit gastrointestinal symptoms. Neonatal infection was a risk factor for hyperbilirubinemia. Increased destruction of red blood cells, which are more vulnerable to damage because of the elevated oxidative stress during sepsis, may explain this phenomenon.34 The progression of gastrointestinal symptoms, including vomiting, diarrhea, poor feeding, dehydration, and fasting, in neonates leads to the increased enterohepatic circulation of bilirubin.33,35 This may explain the relationship between neonatal hyperbilirubinemia and maternal colonization with pathogenic E. coli.
The incidence of neonatal infection increases in the case of maternal infection, risk factors for infection, and colonization.24,36 Our study demonstrated that maternal pathogenic E. coli colonization, especially at rectoanal region, is a risk factor for hyperbilirubinemia in the neonatal period. In the present study, the lack of culture-proven sepsis and neonatal colonization profile restricts us to have a reasonable and valid conclusion regarding the choice of empiric antibiotic therapy for the ill neonate delivered by the pathogenic E. coli colonized mother. The evidence to screen of pathogenic E. coli colonization on pregnant women and further use of prophylactic antibiotic treatment is also not enough to establish a cost-effectiveness protocol in view of our data despite the significant correlation between maternal colonization with pathogenic E. coli and neonatal morbidity.
This study had some limitations. First, we did not perform sampling for each participant at every trimester of pregnancy. As pathogenic E. coli can colonize transiently, a positive culture in only the first or second trimester may not affect infant outcomes. Therefore, stratified data on E. coli colonization in each trimester for correlation with the neonatal outcomes were not available in our study and should be established in a future research. Second, despite we had collected the meconium of the neonate among about half of the neonates enrolled in our study after the middle period of our study, and found there were no E. coli in the meconium (unpublished data). However, we did not routinely check the colonization status of the newborns; a routine check might have provided further evidence regarding the relation between maternal–neonatal transmission of E. coli and neonatal morbidity. Third, the data on neonatal outcomes were retrieved from the medical records of the newborns. However, for 14 infants, data could not be obtained as outpatient follow-up was discontinued after the age of 1 month. Fourth, this is a single-center study, and all of the participants were from one single obstetrician’s out-patient department. Therefore, the selection bias might still exist and could not fully represent Taiwan population or other region outside of Taiwan. Finally, the study was ended early due to funding factor and long study period, and then our sample size might be too small to perform multivariate analysis to identify the true independent factor, such as respiratory distress syndrome. These issues reinforce the necessity of a larger-scale, multi-center reservoir surveillance, particularly including more comprehensive data obtained from questionnaires in addition to medical records.
Conclusion
Approximately one-third of 137 asymptomatic pregnant women in our study presented with pathogenic E. coli colonization in the rectovaginal region. Neonates born to these colonized mothers had potential neonatal morbidities, including hospitalization, hyperbilirubinemia, and gastrointestinal symptoms. Further large studies are necessary to confirm the companions between maternal colonization with pathogenic E. coli and the development of neonatal morbidities to establish a suitable protocol for screening maternal colonization to prevent neonatal illnesses.
Acknowledgments
This work was supported by grants from the Ministry of Science and Technology, Taiwan [grant number MOST 107-2314-B-075B-004] and Kaohsiung Veterans General Hospital in Taiwan [grant number VGHKS107-180]. The funders did not play any role in the study design, data collection, and interpretation, or the decision to submit the study for publication.
Disclosure
The authors reports no conflicts of interest in this work.
References
1. Franz E, Veenman C, van Hoek AH, et al. Pathogenic Escherichia coli producing extended-spectrum β-lactamases isolated from surface water and wastewater. Sci Rep. 2015;5:14372. doi:10.1038/srep14372
2. Vergnano S, Sharland M, Kazembe P, et al. Neonatal sepsis: an international perspective. Arch Dis Child Fetal Neonatal Ed. 2005;90:F220–F224. doi:10.1136/adc.2002.022863
3. Stoll BJ, Hansen NI, Sanchez PJ, et al. Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics. 2011;127:817–826. doi:10.1542/peds.2010-2217
4. Ouchenir L, Renaud C, Khan S, et al. The epidemiology, management, and outcomes of bacterial meningitis in infants. Pediatrics. 2017;140:e20170476. doi:10.1542/peds.2017-0685
5. Knowles SJ, O’Sullivan NP, Meenan AM, et al. Maternal sepsis incidence, aetiology and outcome for mother and fetus: a prospective study. Bjog. 2015;122:663–671. doi:10.1111/1471-0528.12892
6. Barcaite E, Bartusevicius A, Tameliene R, et al. Prevalence of maternal group B streptococcal colonisation in European countries. Acta Obstet Gynecol Scand. 2008;8:260–271. doi:10.1080/00016340801908759
7. Watt S, Lanotte P, Mereghetti L, et al. Escherichia coli strains from pregnant women and neonates: intraspecies genetic distribution and prevalence of virulence factors. J Clin Microbiol. 2003;41:1929–1935. doi:10.1128/JCM.41.5.1929-1935.2003
8. Schrag SJ, Zywicki S, Farley MM, et al. Group B streptococcal disease in the era of intrapartum antibiotic prophylaxis. N Engl J Med. 2000;342:15–20. doi:10.1056/NEJM200001063420103
9. Verani JR, McGee L, Schrag SJ. Prevention of perinatal group B streptococcal disease: revised guidelines from CDC, 2010. MMWR Recomm Rep. 2010;59:1–32.
10. Van Dyke MK, Phares CR, Lynfield R, et al. Evaluation of universal antenatal screening for group B streptococcus. N Engl J Med. 2009;360:2626–2636. doi:10.1056/NEJMoa0806820
11. Purisch SE, Gyamfi-Bannerman C. Epidemiology of preterm birth. Semin Perinatol. 2017;41(7):387–391. doi:10.1053/j.semperi.2017.07.009
12. Wang H, Chow S-C. Sample Size Calculation for Comparing Proportions. Wiley Encyclopedia of Clinical Trials. American Cancer Society; 2007.
13. Fagan PK, Hornitzky MA, Bettelheim KA, et al. Detection of Shiga-like toxin (stx1 and stx2), intimin (eaeA), and enterohemorrhagic Escherichia coli (EHEC) hemolysin (EHEC hlyA) genes in animal feces by multiplex PCR. Appl Environ Microbiol. 1999;65:868–872.
14. Johnson JR, Gajewski A, Lesse AJ, et al. Extraintestinal pathogenic Escherichia coli as a cause of invasive nonurinary infections. J Clin Microbiol. 2003;41:5798–5802. doi:10.1128/JCM.41.12.5798-5802.2003
15. Maisels MJ, Bhutani VK, Bogen D, et al. Hyperbilirubinemia in the newborn infant > or =35 weeks’ gestation: an update with clarifications. Pediatrics. 2009;124:1193–1198. doi:10.1542/peds.2009-0329
16. Benjamini Y. Discovering the false discovery rate. J R Statist Soc B. 2010;72(4):405–416. doi:10.1111/j.1467-9868.2010.00746.x
17. Kaper JB, Nataro JP, Mobley HL. Pathogenic Escherichia coli. Nat Rev Microbiol. 2004;2:123–140. doi:10.1038/nrmicro818
18. Sáez-López E, Guiral E, Fernández-Orth D, et al. Vaginal versus obstetric infection Escherichia coli isolates among pregnant women: antimicrobial resistance and genetic virulence profile. PLoS One. 2016;11:e0146531. doi:10.1371/journal.pone.0146531
19. Carey JC, Klebanoff MA. Is a change in the vaginal flora associated with an increased risk of preterm birth? Am J Obstet Gynecol. 2005;192:1341–1346. doi:10.1016/j.ajog.2004.11.001
20. Stokholm J, Schjørring S, Pedersen L, et al. Living with cat and dog increases vaginal colonization with E. coli in pregnant women. PLoS One. 2012;7:e46226. doi:10.1371/journal.pone.0046226
21. Stokholm J, Schjørring S, Eskildsen CE, et al. Antibiotic use during pregnancy alters the commensal vaginal microbiota. Clin Microbiol Infect. 2014;20:629–635. doi:10.1111/1469-0691.12742
22. Tamelienė R, Barčaitė E, Stonienė D, et al. Escherichia coli colonization in neonates: prevalence, perinatal transmission, antimicrobial susceptibility, and risk factors. Medicina (Kaunas). 2012;48:71–76.
23. Birgy A, Mariani-Kurkdjian P, Bidet P, et al. Characterization of extended-spectrum-beta-lactamase-producing Escherichia coli strains involved in maternal-fetal colonization: prevalence of E. coli ST131. J Clin Microbiol. 2013;51:1727–1732. doi:10.1128/JCM.00749-13
24. Chan GJ, Lee AC, Baqui AH, et al. Prevalence of early-onset neonatal infection among newborns of mothers with bacterial infection or colonization: a systematic review and meta-analysis. BMC Infect Dis. 2015;15:118. doi:10.1186/s12879-015-0813-3
25. Rettedal S, Löhr IH, Bernhoff E, et al. Extended-spectrum beta-lactamase-producing Enterobacteriaceae among pregnant women in Norway: prevalence and maternal-neonatal transmission. J Perinatol. 2015;35:907–912. doi:10.1038/jp.2015.82
26. Asindi AA, Archibong EI, Mannan NB. Mother-infant colonization and neonatal sepsis in prelabor rupture of membranes. Saudi Med J. 2002;23(10):1270–1274.
27. Jiménez E, Marin ML, Martin R, et al. Is meconium from healthy newborns actually sterile? Res Microbiol. 2008;159:187–193. doi:10.1016/j.resmic.2008.07.003
28. Camacho-Gonzalez A, Spearman PW, Stoll BJ. Neonatal infectious diseases: evaluation of neonatal sepsis. Pediatr Clin North Am. 2013;60:367–389. doi:10.1016/j.pcl.2012.12.003
29. Furyk JS, Swann O, Molyneux E. Systematic review: neonatal meningitis in the developing world. Trop Med Int Health. 2011;16:672–679. doi:10.1111/j.1365-3156.2010.02704.x
30. Russo TA, Johnson JR. Proposal for a new inclusive designation for extraintestinal pathogenic isolates of Escherichia coli: ExPEC. J Infect Dis. 2000;181:1753–1754. doi:10.1086/jid.2000.181.issue-5
31. Russo TA, Wang Z, Davidson BA, et al. Surfactant dysfunction and lung injury due to the E. coli virulence factor hemolysin in a rat pneumonia model. Am J Physiol Lung Cell Mol Physiol. 2007;292:L632–L643. doi:10.1152/ajplung.00326.2006
32. Croxen MA, Law RJ, Scholz R, et al. Recent advances in understanding enteric pathogenic Escherichia coli. Clin Microbiol Rev. 2013;26:822–880.
33. Dennery PA, Seidman DS, Stevenson DK. Neonatal hyperbilirubinemia. N Engl J Med. 2001;344:581–590. doi:10.1056/NEJM200102223440807
34. Martin RJ, Fanaroff AA, Walsh MC. Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant.
35. Lauer BJ, Spector ND. Hyperbilirubinemia in the newborn. Pediatr Rev. 2011;32:341–349. doi:10.1542/pir.32-8-341
36. Chan GJ, Lee AC, Baqui AH, et al. Risk of early-onset neonatal infection with maternal infection or colonization: a global systematic review and meta-analysis. PLoS Med. 2013;10:e1001502. doi:10.1371/journal.pmed.1001502
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.