Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
Recombinant Activated Factor VII in Aortic Surgery for Patients Under Hypothermic Circulatory Arrest
Authors Ise H ![]() , Ushioda R, Kanda H, Kimura F, Saijo Y, Akhyari P, Lichtenberg A, Kamiya H
, Ushioda R, Kanda H, Kimura F, Saijo Y, Akhyari P, Lichtenberg A, Kamiya H
Received 5 December 2021
Accepted for publication 15 March 2022
Published 5 April 2022 Volume 2022:18 Pages 337—348
DOI https://doi.org/10.2147/TCRM.S352609
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Hayato Ise,1,2 Ryohei Ushioda,1 Hirotsugu Kanda,3 Fumiaki Kimura,4 Yasuaki Saijo,5 Payam Akhyari,2 Artur Lichtenberg,2 Hiroyuki Kamiya1
1Department of Cardiac Surgery, Asahikawa Medical University, Asahikawa, Japan; 2Department of Cardiovascular Surgery, Heinrich Heine University, Düsseldorf, Germany; 3Department of Anesthesiology and Critical Care Medicine, Asahikawa Medical University, Asahikawa, Japan; 4Department of Cardiovascular Surgery, Kushiro Kojinkai Memorial Hospital, Kushiro, Japan; 5Division of Public Health and Epidemiology, Department of Social Medicine, Asahikawa Medical University, Asahikawa, Japan
Correspondence: Hirotsugu Kanda, Department of Anesthesiology and Critical Care Medicine, Asahikawa Medical University, Midorigaoka-Higashi 2-1-1-1, Asahikawa, 078-8510, Japan, Tel +81-166-68-2583, Fax +81-166-68-2589, Email [email protected]
Purpose: We aimed to identify the risk factors of critical bleeding and investigate the safety of recombinant activated factor VII (rFVIIa) in aortic surgery under hypothermic circulatory arrest (HCA).
Patients and Methods: The present single-center retrospective study compared the baseline characteristics of 144 patients who underwent aortic surgery under HCA at our institute. Among the total cohort of 144 patients, 42 received rFVIIa (rFVIIa group), while the remaining 102 patients did not (non-rFVIIa group). Perioperative bleeding and transfusions, postoperative 30-day mortality, and adverse events (AEs) were analyzed in 29 propensity score-matched pairs.
Results: Before surgery, the rFVIIa group demonstrated a greater number of shocks (p=0.019), higher JapanSCORE II mortality rate (p=0.033), low platelet count (p=0.015) and fibrinogen (p< 0.001) level, prolonged activated partial thromboplastin time (aPTT) (p=0.005) and prothrombin time international normalized ratio (PT-INR) (p=0.006), and longer aortic cross clamp time (p=0.049). Postoperative bleeding, transfusion, 30-day mortality, and AEs were comparable between the groups both in the entire-unmatched cohort and propensity score matching cohort.
Conclusion: Preoperative shock, higher JapanSCORE II mortality rates, low platelet and fibrinogen levels, prolonged aPTT and PT-INR, and longer aortic clamping time might be risk factors for excessive bleeding and indicate the need for rFVIIa treatment. The present study suggests that rFVIIa can be safely used to address critical and continuous bleeding in spite of adequate transfusion and supplementation of other coagulation factors in aortic surgery under HCA, without an increase in 30-day mortality and AEs.
Keywords: aortic surgery under hypothermic circulatory arrest, cardiac surgery, recombinant activated factor VII, retrospective study, uncontrollable bleeding
Introduction
Management of bleeding is an important and often urgent concern for anesthesiologists and cardiac surgeons, especially during aortic surgery. Currently, hypothermic circulatory arrest (HCA) with cerebral perfusion is a safe standard strategy in thoracic aortic surgery to lower the incidence of perioperative stroke.1–4 However, HCA causes coagulopathy because of both cardiopulmonary bypass (CPB) and hypothermia, which may result in life-threatening bleeding.5,6 In such cases of bleeding, massive transfusion of packed red blood cells (PRBC), fresh frozen plasma (FFP), and platelet concentrate (PC) is performed. Occasionally, the condition necessitates further administration of other hemostatic agents, such as fibrinogen concentrates, prothrombin complex, and recombinant activated factor VII (rFVIIa). However, researchers have not yet assessed the risk factors for such critical bleeding events even following adequate transfusion protocol and administration of other coagulation factors, ie fibrinogen concentrates and prothrombin complex, which necessitates rFVIIa treatment in aortic surgery under HCA.
rFVIIa was developed as a treatment agent for bleeding episodes in hemophilia. Nonetheless, its off-label use in cardiac surgery has increased since the first report in 2000.7 In 2008, rFVIIa was most frequently used in cardiac surgery (29%) and trauma (29%) in the USA, compared to its use for hemophilia A and B (2.7%).8 Numerous studies have investigated the efficacy and safety of rFVIIa in cardiac surgery.9,10 However, only few studies have focused on its off-label use in aortic surgery.11,12 Moreover, these studies only included patients with acute aortic dissection (AAD) or those who underwent aortic surgery without HCA. Therefore, the safety of rFVIIa for life-threatening bleeding in aortic surgery under HCA remains unclear.
Furthermore, the occurrence rate of thromboembolic complications following administration of rFVIIa in patients who underwent aortic surgery under HCA should be investigated. In a meta-analysis study, Levi et al reported that treatment with high dose rFVIIa on an off-label basis increased the risk of arterial thromboembolic events in patients due to several conditions, such as spontaneous central nervous system bleeding, trauma, spinal surgery, and cardiac surgery.13 In a particular cohort that underwent non-aortic cardiac surgery, ie coronary artery bypass grafting and/or valve surgery without HCA, Gill et al reported a trend towards an increased occurrence of adverse events, including stroke.9 However, massive coagulopathy would be exist in patients suffering from critical bleeding in aortic surgery under HCA, and association between thromboembolic complications and the use of rFVIIa in this particular cohort has not been well investigated.
Thus, we intended to identify the risk factors of uncontrollable bleeding in aortic surgery under HCA and to elucidate the safety of off-label rFVIIa use for life-threatening bleeding events.
Materials and Methods
Study Design and Patient Population
We retrospectively analyzed 162 patients who underwent aortic surgery under HCA between April 2014 and March 2019 at a single institution. Cases of redo and salvage surgeries (requiring cardiopulmonary resuscitation before surgery) were excluded. Of the remaining 144 patients, 42 patients received rFVIIa (rFVIIa group), while 102 patients did not (non-rFVIIa group). We analyzed the preoperative patient characteristics, perioperative bleeding and transfusions, postoperative adverse events (AEs), and 30-day mortality. Postoperative 30-day mortality and thrombosis-related AEs were the primary endpoints. In contrast, postoperative bleeding and transfusions were the secondary endpoints. AEs were defined as follows: disabling stroke (postoperative persistent neurological deficits caused by thromboembolic events, confirmed by computed tomography (CT) scan or magnetic resonance imaging); minor stroke (postoperative temporary neurological deficits with recovery at discharge or at transfer to another hospital), and renal failure (serum creatinine >2.0 mg/dl and doubling of the preoperative value, or the new onset of hemodialysis). Myocardial infarction (MI), pulmonary embolism (PE), deep venous thrombosis, and other AEs were comprehensively diagnosed by physical examinations, laboratory tests, CT, electrocardiography, echocardiography, or color Doppler sonography (where appropriate).
The Asahikawa Medical University Hospital approved the off-label use of rFVIIa. The Institutional Review Board of Asahikawa Medical University approved this study (No. 19078). While the need for written informed consent for enrollment in this study was waived due to the retrospective study design. The research content has been open for public consumption and the patients were granted the right to refuse participation in the present study. On the other hand, written informed consent to use rFVIIa had been obtained from the participants. In cases of elective or urgent surgery, written informed consent was obtained directly from the patients preoperatively. In cases of emergency surgery, written informed consent was obtained from a family member of the patient.
Anesthetic Methods
Once in the operating room, standard monitoring was performed using five-channel electrocardiography, pulse oximetry, and direct arterial or indirect blood pressure monitoring. General anesthesia was performed using the target-controlled intravenous infusion of propofol, continuous infusion of remifentanil, and single-dose administration of fentanyl. Propofol was infused to maintain a bispectral index within the range of 40–60. Sevoflurane or Desflurane were also administered if the attending anesthesiologist judged it to be necessary. Rocuronium was administered to facilitate endotracheal intubation and to provide adequate muscle relaxation during surgery when necessary. After intubation, a central venous catheter and transesophageal echocardiography probe were inserted. After completing the surgical procedures, the patients were sedated using a continuous infusion of propofol and dexmedetomidine while intubated and were transported to the intensive Care unit (ICU).
Surgical Procedures
Median sternotomy was performed in all cases. Before CPB, we administered heparin (300 U/kg) to maintain an activated clotting time of >480 s during CPB. CPB was established using bicaval venous cannulation. Arterial cannulation is generally performed at the level of the ascending aorta or femoral artery in some AAD cases. Following CPB establishment, mild (>28°C) to moderate (20.1–28°C) hypothermia was applied. Myocardial protection was achieved by antegrade or retrograde cardioplegia in cases of thoracic aortic aneurysm (TAA) or AAD, respectively. The ascending aorta was clamped and transected during systemic cooling, and proximal anastomosis of the aorta was performed. The rectal temperature upon reaching the target temperature induced HCA. Simultaneously, retrograde cerebral perfusion was initiated and eventually switched to antegrade selective cerebral perfusion by cannulation of the supra-aortic arch vessels. Moreover, the patients underwent distal anastomosis of the ascending aorta or aortic arch during the HCA. Following the end of the distal anastomosis, perfusion of the lower body was restarted from the side branch of the prosthesis, and rewarming was initiated. Moreover, anastomoses of the supra-aortic arch vessels were performed following distal anastomosis of the aorta in case of total arch replacement. Concomitant procedures were performed when required.
Intraoperative and Postoperative Management of Bleeding and Transfusion
Following weaning from CPB, heparin was antagonized by protamine administration (1:1 ratio to the applied heparin dosage). Subsequently, a transfusion was initiated. Hemoglobin <8 g/dL resulted in PRBC transfusion. Cell saver blood was also administered. In our institute, the cell saver blood was considered in the bleeding amount, although nearly all the cell saver blood was returned to the patients. Moreover, FFP was transfused upon detecting prolonged activated partial thromboplastin time (aPTT) or prothrombin time international normalized ratio (PT-INR). PC transfusion occurred when platelets (Plt) were <8 × 109. In addition, the patients were administered cryoprecipitate when fibrinogen was <1.5 g/L. Fibrinogen <1.5 g/L following cryoprecipitate transfusion resulted in fibrinogen concentrate administration. rFVIIa was administered on observing continuous excessive bleeding despite the correction of surgical bleeding, pH, temperature, and adequate transfusion. Cryoprecipitate, fibrinogen concentrate, and rVIIa were only used in the operating room. After achieving adequate hemostasis in the operative field, as assessed by the surgeon, the patients were transferred to the ICU. Re-exploration was considered in the ICU if the total bleeding amount from the chest tubes exceeded 400 mL/h regardless of adequate transfusion.
Indication and Administration Dose of rFVIIa
As aforementioned, rFVIIa was administered upon observing continuous excessive bleeding despite the adjustments for surgical bleeding, pH, temperature, and adequate transfusion. In the early period of the present series, 5 mg of rFVIIa was administrated in most cases (n=20). However, with the accumulation of clinical experience, 2 mg or 1 mg of rFVIIa was mainly administered in the late period (n=22). Repetitive administration was warranted only in one patient (5 mg + 2 mg).
Statistical Analyses
While the categorical variables are presented as numbers and percentages, the continuous variables are presented as medians. We performed propensity score matching (PSM) to balance the risk factors for outcomes between the groups. The propensity score (PS) was obtained from a logistic regression model with forced entry method, including variables presented in Table 1, except for concomitant surgery and JapanSCORE II. JapanSCORE II was not considered for PS because it represents the risk-adjusted mortality and preoperatively expected morbidity, based on the Japan Cardiovascular Surgery Database (JCVSD).12 Thus, age, sex, BMI, AAD/TAA, emergency surgery, malperfusion, preoperative shock, cardiac tamponade, GCS<8, smoking, hypertension, diabetes mellitus, liver dysfunction, anticoagulant treatment, and laboratory data before surgery (Hb, Plt, APTT, PT-INR, fibrinogen, serum creatinine, total arch replacement, CPB time, aortic clamp time, lowest rectal temperature, and HCA time) were included in the logistic regression model with forced entry method to generate propensity score. Patients were matched 1:1 using the nearest neighbor matching method without replacement, and a caliper width of 0.2 of the standard deviation of the logit of the estimated PS. This resulted in 29 out of the possible 42 pairs. We calculated standardized mean differences before and after PSM to assess the balance of variables between the groups. Unmatched sub-cohorts were compared using the Fisher's exact test and Mann–Whitney U-test for categorical and continuous variables, respectively. Following PSM, we performed the McNemar test and Wilcoxon signed rank test for the categorical and continuous variables, respectively. PSM was performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria).14 All other statistical analyses were performed using Statistical Package for the Social Sciences for Windows (version 26.0; IBM Corp., Armonk, NY, USA). We analyzed the baseline characteristics in an unmatched population. Perioperative bleeding, transfusion, and postoperative outcomes were analyzed in the matched population. The statistical significance was defined as p<0.05.
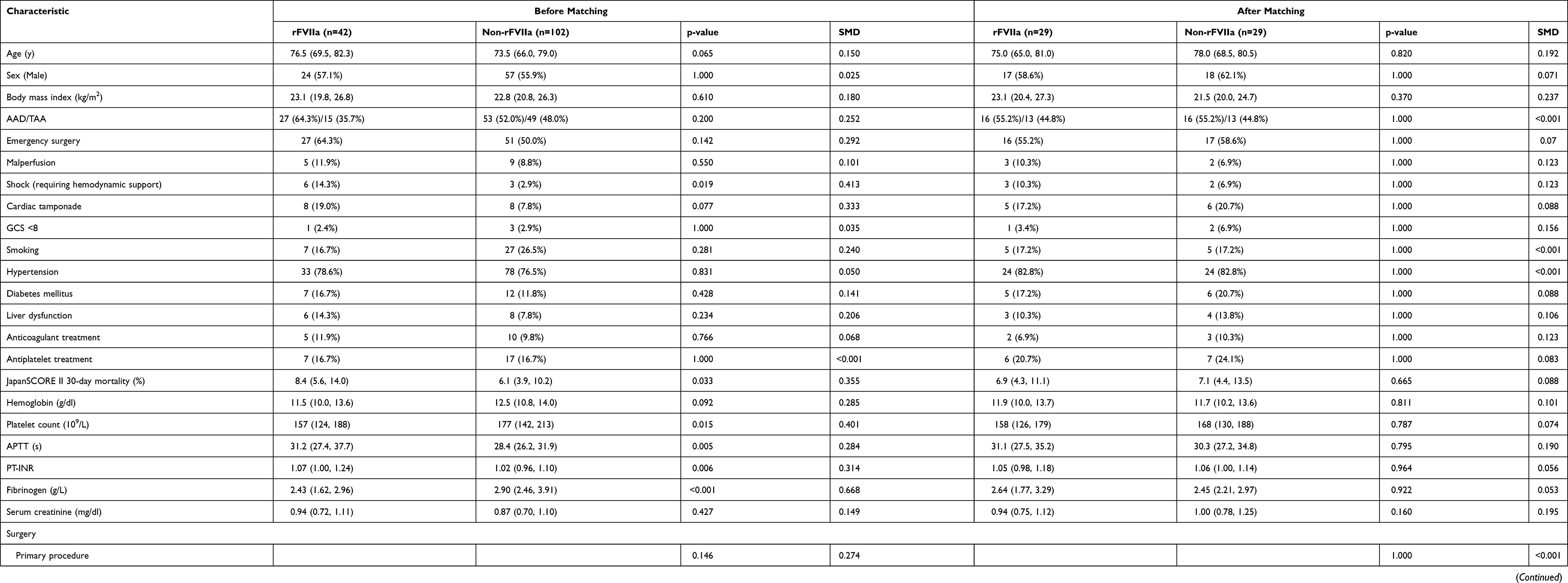 |
Table 1 Baseline and Operative Characteristics |
Results
Baseline and Operative Characteristics
Table 1 summarizes the baseline and operative characteristics. Before PSM, the number of shock patients (p=0.019) and JapanSCORE II 30-day mortality rates (p=0.033) were significantly higher in the rFVIIa group. While Plt (p=0.015) and fibrinogen (p<0.001) were significantly lower, aPTT (p=0.005) and PT-INR (p=0.006) were prolonged in the rFVIIa group. The rFVIIa group demonstrated longer aortic clamp time (p=0.049) and higher lowest body temperature (p=0.043). Following PSM, none of the characteristics were significantly different between the groups.
Perioperative Bleeding and Transfusion
Table 2 summarizes the perioperative amounts of bleeding and transfusion.
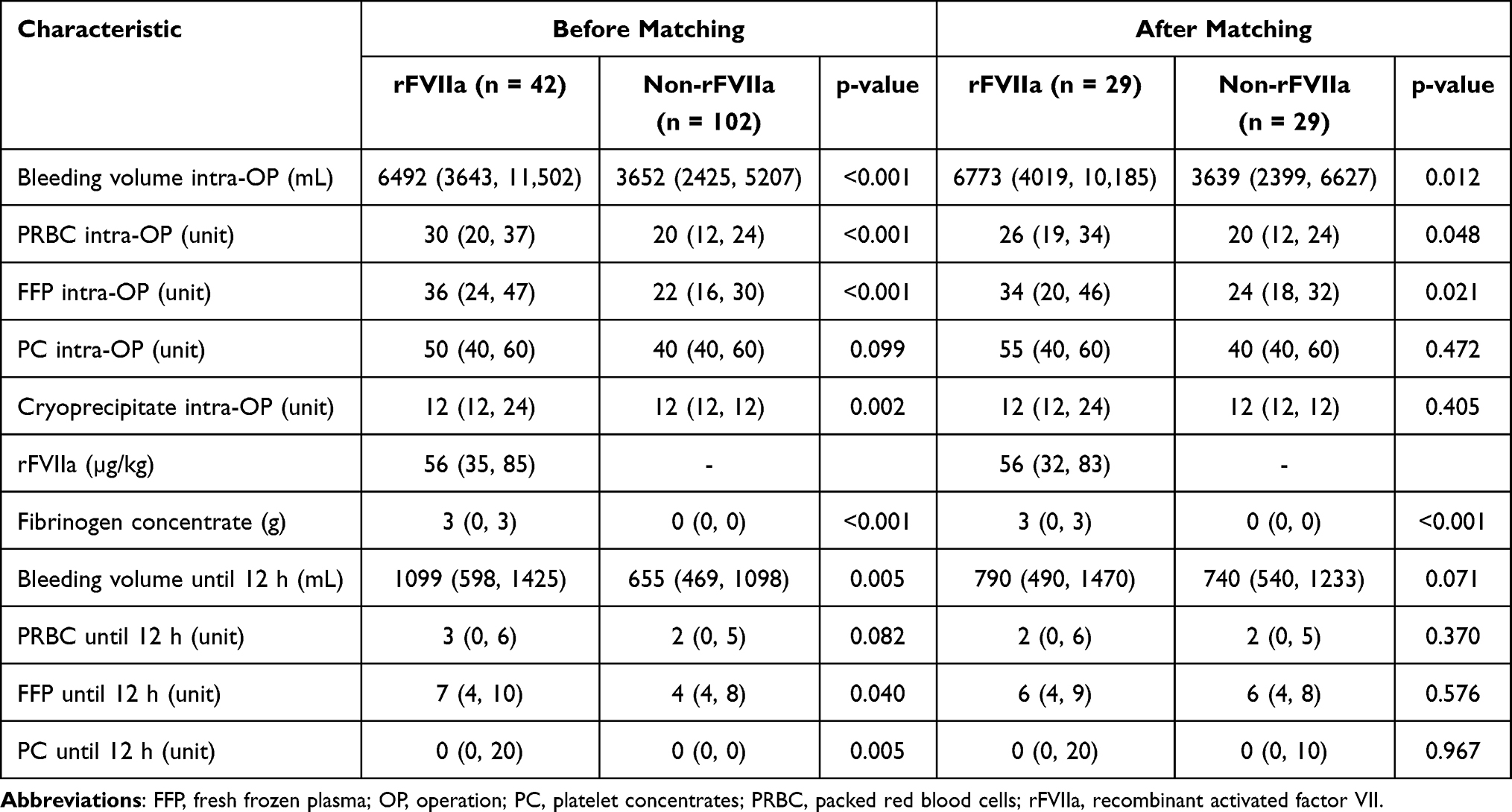 |
Table 2 Perioperative Bleeding and Blood Products in the Entire Unmatched and Propensity-Score Matched Populations |
In the entire unmatched cohort, intraoperative bleeding and amount of transfusion were significantly higher in the rFVIIa group than the non-rFVIIa group, as a matter of course because rFVIIa was administrated in patients with critical bleeding in the present series.
These significant differences were seen also in the PSM cohort. Intraoperative bleeding (p=0.012), PRBC transfusion (p=0.048), and FFP (p=0.021) were significantly higher in the rFVIIa group. Patients in the rFVIIa group received a significantly greater amount of fibrinogen concentrate (p<0.001). The median intraoperative dose of rFVIIa was 56 μg/kg.
Postoperative bleeding and amount of transfusion were significantly higher in the rFVIIa group than non-rFVIIa group in the entire unmatched cohort, however, those differences were not seen after PSM.
Mortality and Postoperative Adverse Events
The results of postoperative outcomes are shown in Table 3. Regarding laboratory data after surgery, Plt was significantly lower (p < 0.001) and PT-INR (p < 0.001) was shorter in rFVIIa group. There were no significant differences between the groups with regard to primary and secondary endpoints.
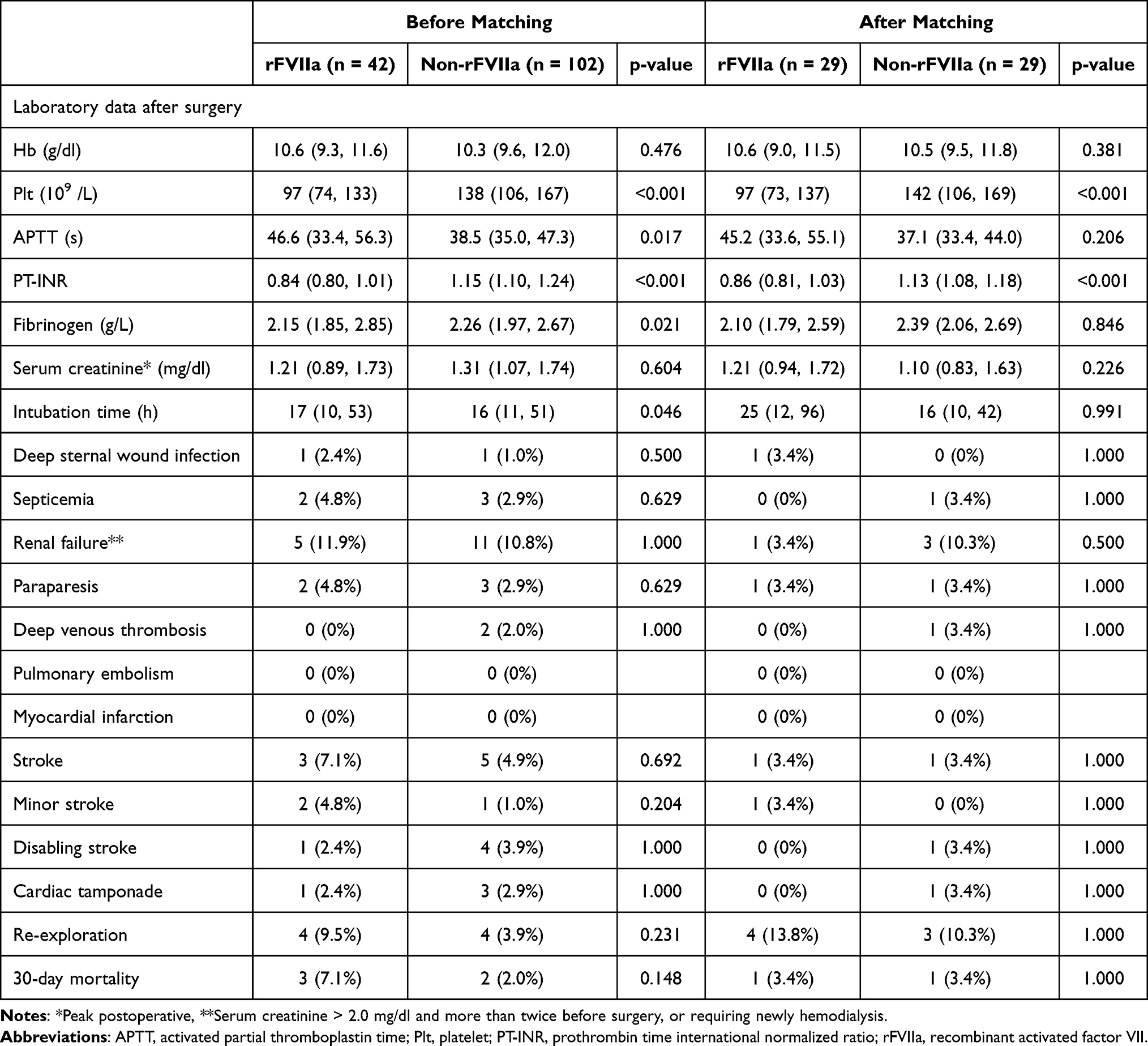 |
Table 3 Postoperative Data and Complications in the Entire Unmatched and Propensity-Score Matched Populations |
In the entire un-matched cohort, 30-day mortality was 7.1% in rFVIIa group and 2.0% in non-rFVIIa group (p=0.148). Stroke occurred in 3 patients (2 minor and 1 disabling stroke) in rFVIIa group and in 5 patients (1 minor and 4 disabling stroke) in non-rFVIIa group (p=0.692). There were no case of postoperative MI or PE in both groups. DVT occurred in 2 patients only in non-rFVIIa group (p=1.000) and cardiac tamponade occurred in one patient in rFVIIa group and in 3 patients in non-rFVIIa group (p=1.000). Re-exploration was performed 9.5% in rFVIIa group and 3.9% in non-rFVIIa group (p=0.231). All other postoperative adverse events were also comparable between the groups.
In PSM cohort, 30-day mortality was 3.4% in both groups (p = 1). One patient (3.4%) in rFVIIa had postoperative minor stroke and one patient (3.4%) in non-rFVIIa had disabling stroke, respectively (p = 1.000). There were no case of postoperative MI or PE in both groups. DVT and cardiac tamponade were detected 1 case (3.4%) in non-rFVIIa group, respectively. Re-exploration was performed 13.8% in rFVIIa group and 10.3% in non-rFVIIa group (p = 1.000). All other postoperative adverse events were also comparable between the groups.
Association Between the Administered Dose of rFVIIa and Mortality/Stroke
Twenty patients who received 5 mg (n=19) or 7 mg (n=1) of rFVIIa were classified as group H and 22 patients who received 2 mg (n=19) or 1 mg (n=1) were classified as group L, and the mortality and thromboembolic complications were compared. Mortality was 10% (n=2/20) in group H and 4.5% (n=1/22) in group L (p=0.493). Stroke rates of 5% in group H (n=1/20, 2 minor strokes) and 9.1% in group L (n=2/22, 1 disabling and 1 minor stroke) were observed.
Comparison Between AAD and TAA Regarding the Detected Risk Factors for the Use of rFVIIa
As already described, 80 patients with AAD and 64 patients with TAA were included in the present study. rFVIIa was administrated in 27 (12.5%) patients with AAD and 15 (23.4%) patients with TAA, including three rupture cases. The results of this sub-analysis are shown in Table 4. Briefly, the preoperative condition, including indicators for coagulopathy, was worse in the AAD group than in the TAA group; however, the outcome was comparative.
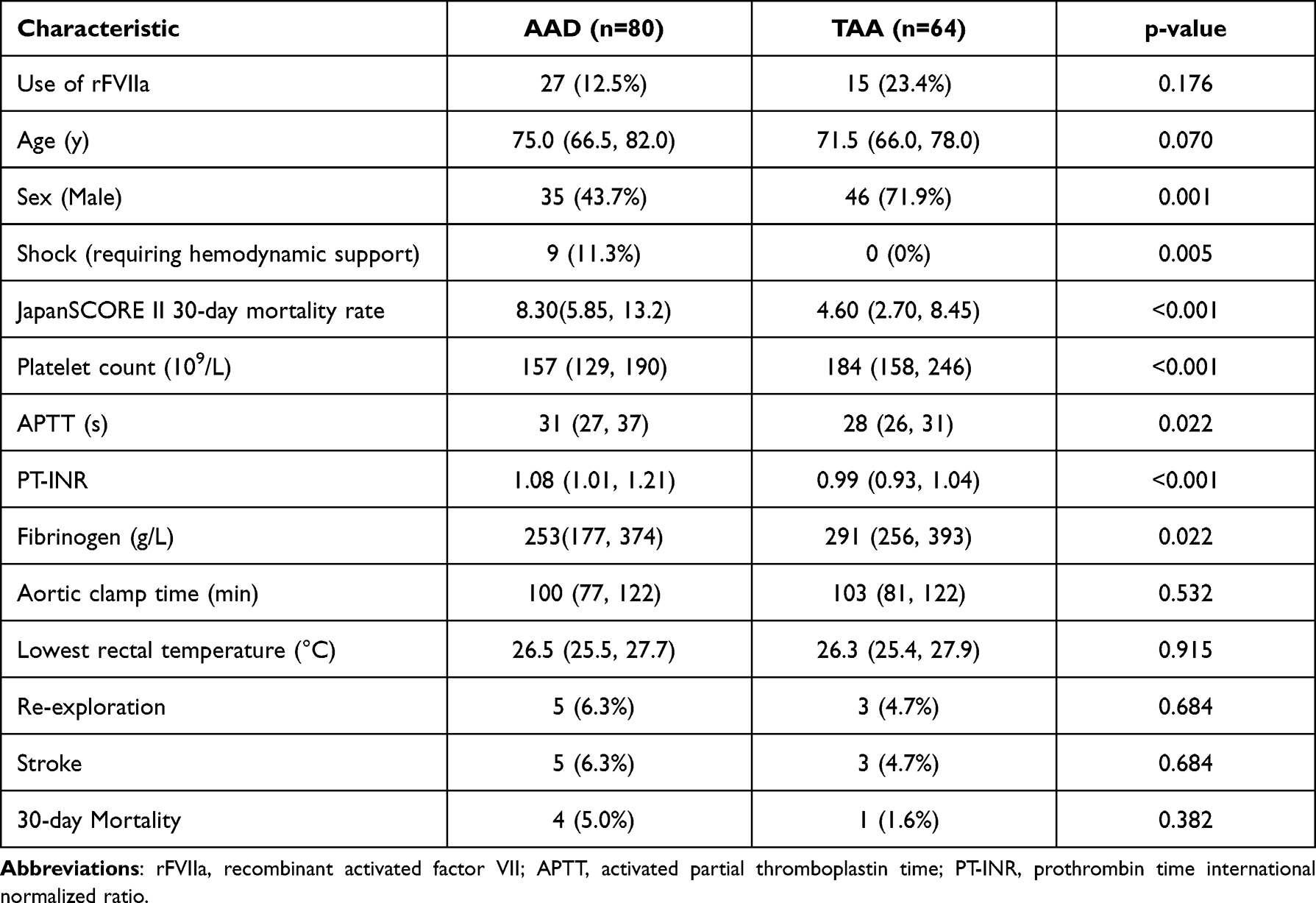 |
Table 4 Comparison Between Acute Aortic Dissection and Thoracic Aortic Aneurysm Regarding the Detected Risk Factors for rFVIIa Use and Outcomes |
Discussion
Few studies have reported on the off-label use of rFVIIa in aortic surgery, with no previous study focusing on the safety of rFVIIa in aortic surgery under HCA.10,11 However, the high possibility of massive bleeding necessitates an evaluation of the safety of off-label rFVIIa use in aortic surgery under HCA. The crucial findings of the present study were as follows: (i) preoperative shock, coagulopathic state in laboratory tests, higher JapanSCORE II 30-day mortality rate, and longer aortic clamp time might be associated with excessive bleeding in aortic surgery under HCA and (ii) rFVIIa application did not result in a significant increase in the postoperative 30-day mortality and AEs in aortic surgery under HCA.
Preoperative shock and coagulopathy increased the risk of intraoperative bleeding, which might require rFVIIa administration. Preoperative shock in our patients was caused by AAD. Guan et al reported that intense prothrombin generation and excessive systemic fibrinolysis occur in AAD before surgery, thereby leading to prolonged consumption coagulopathy, excessive bleeding, and complications.15 On the other hand, researchers have also described coagulopathy in aortic aneurysms with increased intensity upon rupture.16 In the present study, there were three ruptured TAA cases and all the patients received rFVIIa therapy. Regardless of the underlying pathology, the rFVIIa group demonstrated significantly lower Plt and fibrinogen levels, prolonged aPTT, and PT-INR before PSM. This resulted in a significantly greater amount of intraoperative bleeding and transfusion.
In the present study, JapanSCORE II was used to estimate operative mortality because it is routinely calculated in all patients in our institute. JapanSCORE II is a calculated operative risk similar to EuroSCORE. However, it is based on JCVSD. JapanSCORE II more precisely reflects operative risk in Japan than EuroSCORE.17 In the present study, the higher frequency of AAD, emergent surgery, and shock might result in higher operative risk in the rFVIIa group. Despite a lower actual mortality rate than the calculated value, JapanSCORE II appeared to be a reliable risk predictor.
The clinical impact of HCA-induced coagulopathy is well known. However, the underlying mechanism is still unclear. Hypothermia and CPB are factors that cause coagulopathy. However, several studies have reported that the lowest body temperature is not associated with bleeding.2,4 In the present study, the lowest temperature was significantly higher in the rFVIIa group. Nevertheless, intraoperative bleeding was significantly higher in the rFVIIa group than that in the control group. In other words, the lowest temperature was not strongly associated with coagulopathy. Meanwhile, the aortic clamp time in the present study was significantly longer and supposedly associated with excessive bleeding. There are few reports on the relationship between coagulopathy and aortic clamp time. Moreover, longer aortic clamp time reportedly causes both fibrinogen consumption and accumulation of tissue plasminogen activator. Nonetheless, the underlying mechanism is unclear.18
The efficacy of off-label rFVIIa use has been repeatedly reported. However, most of the latter studies involved patients who underwent cardiac surgery,7–10 where the efficacy was demonstrated with respect to the amount of perioperative bleeding, transfusion, and re-exploration.7–10 However, a previous study on AAD surgery reported on significantly greater perioperative bleeding, transfusion, and re-exploration, following rFVIIa administration.19 In the present study, the rFVIIa group demonstrated significantly higher intraoperative bleeding and transfusion, in addition to significantly lower postoperative Plt. The severity of coagulopathy in aortic surgery under HCA is expectedly much higher than that in general cardiac surgery. Therefore, consumption coagulopathy may have persisted even after rFVIIa treatment. According to Paparella et al, intense thrombin generation in patients with AAD stimulates platelet activation and dysfunction, and promotes coagulation factor consumption and excessive fibrinolysis, which collectively result in excessive bleeding.20 Consumption coagulopathy and platelet dysfunction have been not only reported in AAD but also in TAA.21 Patients in the rFVIIa group in aortic surgery under HCA might continue to suffer from life-threatening bleeding and require a greater amount of transfusion if not treated with rFVIIa. Therefore, rFVIIa in aortic surgery under HCA plays an important role in rescue therapy.
The safety of rFVIIa, especially regarding thromboembolic complications, is still unclear and depends on several factors, such as patient characteristics, transfusion, and the dose of rFVIIa utilized. A randomized trial reported no significant increase in mortality, rather a numeric increase in AEs including stroke.9 Alfirevic et al reported higher mortality and renal morbidity in the rFVIIa group.22 The aforementioned studies focused on complex cardiac surgery. Other studies on AAD or aortic surgery demonstrated no significant increase in postoperative mortality or AEs.11,19 From these previous studies, one may assume that the prophylactic use of rFVIIa in patients with preserved coagulation condition could increase thromboembolic complications, but therapeutic use in patients having coagulation disorder would be safe. The results of the present study support this hypothesis. Intense thrombin generation in aortic surgery under HCA causes platelet dysfunction, consumptive coagulopathy, and excessive fibrinolysis. Based on the above-mentioned factors, a low frequency of thromboembolic AEs might result from rFVIIa therapy in aortic surgery.
The safety dose or optimal protocol for rFVIIa in cardiac surgery is still unknown. Researchers have reported on the safety and efficacy of a dose ranging between 35 μg/kg to 70 μg/kg in general cardiac surgery.23 Several studies have described the efficacy of low-dose rFVIIa <20 μg/kg.10 However, considering the severity of coagulopathy in aortic surgery under HCA, a higher dose may also be acceptable A dose <90 μg/kg is considered safe in patients without hemophilia.24 In the present study, the median dose of rFVIIa was 56 μg/kg, and patients did not demonstrate an increase in mortality or thromboembolic AEs. Moreover, the sub-analysis conducted in the present study demonstrated that the administration of a high dose of rFVIIa (more than 5 mg) was not associated with an increased mortality and stroke rate. This finding suggests that the administration dose is not associated with the postoperative complications, and that rFVIIa could be used repeatedly until adequate hemostasis is obtained. However, the present study does not determine the sufficient dose for adequate hemostasis in patients who experience critical bleeding during aortic surgery under HCA, which warrants further investigation. We administered rFVIIa following the correction of other hemostatic parameters, which was in compliance with current recommendations.22
Since rFVIIa is considered expensive, its cost effectiveness should also be discussed. In Japan, the cost of 1 mg rFVIIa is 85,276 yen. On the other hand, the cost of 2 units of PRBC (400 mL), 2 units of FFP (240 mL), and 20 units of PC (250 mL) are 17,194; 18,322; and 163,471 yen, respectively. It indicates that the cost of 2 mg rFVIIa is comparable to additional 20 units of PC in a situation of critical intraoperative bleeding. From the perspective of cost effectiveness and patients’ safety, administration of rFVIIa as a rescue therapy for critical bleeding in aortic surgery under HCA could be justified.
Limitations
Our study had several limitations. First, this was a single-center, retrospective, observational study with a small sample size. Second, the decision to use rFVIIa and its timing as a rescue therapy was made by the individual anesthesiologists and operating surgeons; thus, a definite criterion for the use of rFVIIa could not be clarified in the present study. Third, we performed PSM based on different characteristics before rFVIIa treatment. Nevertheless, there were several unmeasured confounders. Fourth, we observed a difference in intraoperative transfusions, which might have affected the amount of intraoperative bleeding and rFVIIa administration. However, it was impossible to equalize the number of intraoperative transfusions because of the retrospective observational study design. Despite the aforementioned limitations, this is the first study to focus on the use of rFVIIa in aortic surgery under HCA and could serve as a basis for further, large-volume studies focusing on coagulopathy during aortic surgery under HCA.
Conclusion
Preoperative shock, higher JapanSCORE II mortality rates, low Plt and fibrinogen, prolonged aPTT and PT-INR, and longer aortic clamp time might be risk factors for excessive bleeding, thus necessitating rFVIIa treatment. The present study suggests that rFVIIa can be used for critical and continuous bleeding in spite of adequate transfusion and supplementation of other coagulation factors during aortic surgery under HCA, without an increase in 30-day mortality and AEs. Nevertheless, further prospective randomized studies are warranted owing to the critical limitations of the present study.
Abbreviations
AAD, acute aortic dissection; AEs, adverse events; aPTT, activated partial thromboplastin time; CPB, cardiopulmonary bypass; CT, computed tomography; FFP, fresh frozen plasma; HCA, hypothermic circulatory arrest; ICU, intensive care unit; JCVSD, Japan Cardiovascular Surgery Database; MI, myocardial infarction; PC, platelet concentrate; PE, pulmonary embolism; Plt, platelets; PRBC, packed red blood cells; PS, propensity score; PSM, propensity score matching; PT-INR, prothrombin time international normalized ratio; rFVIIa, recombinant activated factor VII; TAA, thoracic aortic aneurysm.
Ethics Approval and Informed Consent
The Institutional Review Board of Asahikawa Medical University approved this study (No. 19078). While the need for written informed consent for enrollment in this study was waived due to the retrospective study design.
Acknowledgments
HI is supported by a research fellowship award from the Japanese Society on Thrombosis and Haemostasis.
Funding
There is no funding to report.
Disclosure
Payam Akhyari reveived speaker honoraria from Abiomed, Jotec-Cryolife, and Medtronic, reports grants and as the clinical study principal investigator for Edwards Lifesciences and Abbott, outside the submitted work. The authors declare that they have no other competing interests in this work.
References
1. Gupta P, Harky A, Jahangeer S, Adams B, Bashir M. Varying evidence on deep hypothermic circulatory arrest in thoracic aortic aneurysm surgery. Tex Heart Inst J. 2018;45(2):70–75. doi:10.14503/THIJ-17-6364
2. Keenan JE, Wang H, Gulack BC, et al. Does moderate hypothermia really carry less bleeding risk than deep hypothermia for circulatory arrest? A propensity-matched comparison in hemiarch replacement. J Thorac Cardiovasc Surg. 2016;152(6):1559–1569.e2. doi:10.1016/j.jtcvs.2016.08.014
3. Kamiya H, Hagl C, Kropivnitskaya I, et al. The safety of moderate hypothermic lower body circulatory arrest with selective cerebral perfusion: a propensity score analysis. J Thorac Cardiovasc Surg. 2007;133(2):501–509. doi:10.1016/j.jtcvs.2006.09.045
4. Keeling WB, Tian DH, Leshnower BG, et al. Safety of moderate hypothermia with antegrade cerebral perfusion in total aortic arch replacement. Ann Thorac Surg. 2018;105(1):54–61. doi:10.1016/j.athoracsur.2017.06.072
5. Harrington DK, Lilley JP, Rooney SJ, Bonser RS. Nonneurologic morbidity and profound hypothermia in aortic surgery. Ann Thorac Surg. 2004;78(2):596–601. doi:10.1016/j.athoracsur.2004.01.012
6. Ise H, Kitahara H, Oyama K, et al. Hypothermic circulatory arrest induced coagulopathy: rotational thromboelastometry analysis. Gen Thorac Cardiovasc Surg. 2020;68(8):754–761. doi:10.1007/s11748-020-01399-y
7. Al Douri M, Shafi T, Al Khudairi D, et al. Effect of the administration of recombinant activated factor VII (rFVIIa; NovoSeven) in the management of severe uncontrolled bleeding in patients undergoing heart valve replacement surgery. Blood Coagul Fibrinolysis. 2000;11(Suppl 1):S121–S127. doi:10.1097/00001721-200004001-00023
8. Yank V, Tuohy CV, Logan AC, et al. Comparative Effectiveness of In-Hospital Use of Recombinant Factor VIIa for Off-Label Indications Vs. Usual Care. Rockville (MD): Agency for Healthcare Research and Quality (US); Report No.: 10-ehc030-ef. 2010.
9. Gill R, Herbertson M, Vuylsteke A, et al. Safety and efficacy of recombinant activated factor VII: a randomized placebo-controlled trial in the setting of bleeding after cardiac surgery. Circulation. 2009;120(1):21–27. doi:10.1161/CIRCULATIONAHA.108.834275
10. Hoffmann T, Assmann A, Dierksen A, et al. A role for very low-dose recombinant activated factor VII in refractory bleeding after cardiac surgery: lessons from an observational study. J Thorac Cardiovasc Surg. 2018;156(4):1564–1573.e8. doi:10.1016/j.jtcvs.2018.03.167
11. Goksedef D, Panagopoulos G, Nassiri N, Levine RL, Hountis PG, Plestis KA. Intraoperative use of recombinant activated factor VII during complex aortic surgery. J Thorac Cardiovasc Surg. 2012;143(5):1198–1204. doi:10.1016/j.jtcvs.2012.01.004
12. Takamoto S, Motomura N, Miyata H, Tsukihara H. Current status of cardiovascular surgery in Japan, 2013 and 2014: a report based on the Japan Cardiovascular Surgery Database (JCVSD). 1: mission and history of JCVSD. Gen Thorac Cardiovasc Surg. 2018;66(1):1–3. doi:10.1007/s11748-017-0843-4
13. Levi M, Levy JH, Andersen HF, Truloff D. Safety of recombinant activated factor VII in randomized clinical trials. N Engl J Med. 2010;363(19):1791–1800. doi:10.1056/NEJMoa1006221
14. Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. doi:10.1038/bmt.2012.244
15. Guan X, Li J, Gong M, Lan F, Zhang H. The hemostatic disturbance in patients with acute aortic dissection: a prospective observational study. Medicine. 2016;95(36):e4710. doi:10.1097/MD.0000000000004710
16. Davies RS, Abdelhamid M, Wall ML, Vohra RK, Bradbury AW, Adam DJ. Coagulation, fibrinolysis, and platelet activation in patients undergoing open and endovascular repair of abdominal aortic aneurysm. J Vasc Surg. 2011;54(3):865–878. doi:10.1016/j.jvs.2011.04.010
17. Kurazumi H, Mikamo A, Fukamitsu G, et al. Validation of the JapanSCORE versus the logistic EuroSCORE for predicting operative mortality of cardiovascular surgery in Yamaguchi University Hospital. Gen Thorac Cardiovasc Surg. 2011;59(9):599–604. doi:10.1007/s11748-011-0784-2
18. Haithcock BE, Shepard AD, Raman SB, Conrad MF, Pandurangi K, Fanous NH. Activation of fibrinolytic pathways is associated with duration of supraceliac aortic cross-clamping. J Vasc Surg. 2004;40(2):325–333. doi:10.1016/j.jvs.2004.04.015
19. Zindovic I, Sjögren J, Ahlsson A, et al. Recombinant factor VIIa use in acute type A aortic dissection repair: a multicenter propensity-score-matched report from the Nordic Consortium for Acute Type A Aortic Dissection. J Thorac Cardiovasc Surg. 2017;154(6):1852–1859.e2. doi:10.1016/j.jtcvs.2017.08.020
20. Paparella D, Rotunno C, Guida P, et al. Hemostasis alterations in patients with acute aortic dissection. Ann Thorac Surg. 2011;91(5):1364–1369. doi:10.1016/j.athoracsur.2011.01.058
21. Tanaka M, Kawahito K, Adachi H, Ino T. Platelet dysfunction in acute type A aortic dissection evaluated by the laser light-scattering method. J Thorac Cardiovasc Surg. 2003;126(3):837–841. doi:10.1016/S0022-5223(03)00734-7
22. Alfirevic A, Duncan A, You J, Lober C, Soltesz E. Recombinant factor VII is associated with worse survival in complex cardiac surgical patients. Ann Thorac Surg. 2014;98(2):618–624. doi:10.1016/j.athoracsur.2014.04.126
23. Fitzgerald J, McMonnies R, Sharkey A, Gross PL, Karkouti K. Thrombin generation and bleeding in cardiac surgery: a clinical narrative review. [Génération de thrombine et saignements en chirurgie cardiaque: un compte rendu narratif clinique]. Can J Anaesth. 2020;67(6):746–753. [French]. doi:10.1007/s12630-020-01609-4
24. Hsia CC, Chin-Yee IH, McAlister VC. Use of recombinant activated factor VII in patients without hemophilia: a meta-analysis of randomized control trials. Ann Surg. 2008;248(1):61–68. doi:10.1097/SLA.0b013e318176c4ec
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.