Back to Journals » ImmunoTargets and Therapy » Volume 15
Recent Advances in Vitiligo Treatment
Authors Qiu Y ![]() , Su X, Chen J, Jiang S, Tang X, He Y
, Su X, Chen J, Jiang S, Tang X, He Y ![]() , Liu F
, Liu F ![]()
Received 29 October 2025
Accepted for publication 1 February 2026
Published 11 February 2026 Volume 2026:15 577653
DOI https://doi.org/10.2147/ITT.S577653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah Wheeler
Ye Qiu, Xiangxi Su, Jingru Chen, Shaojing Jiang, Xinrui Tang, Yurong He, Fang Liu
Department of Dermatology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Fang Liu, Department of Dermatology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Purpose: This review systematically summarizes breakthrough advances in vitiligo treatment from 2020 to 2025 to provide the latest evidence-based insights for clinical practice.
Patients and Methods: We searched ClinicalTrials.gov and PubMed for literature and clinical trials published within this period. Inclusion criteria encompassed randomized controlled trials (RCTs), Phase II and above clinical trial results, and fundamental research with clear clinical translational value.
Results: Our analysis identified that JAK inhibitors achieved significant repigmentation by blocking the IFN-γ/JAK-STAT signaling pathway, while novel agents such as IL-15 inhibitors selectively eliminated pathogenic CD8⁺ T cells, suppressing immune-mediated damage at its source. The combination of 308 nm excimer laser with JAK inhibitors or platelet-rich plasma (PRP) increased repigmentation rates in acral lesions to 56.1%, and vitamin D adjunct therapy demonstrated synergistic effects. For stable disease, ReCell technology combined with narrowband UVB (NB-UVB) emerged as an effective option, whereas miniature punch grafting further optimized surgical outcomes. Additionally, repurposed traditional drugs and antioxidant strategies expanded the available clinical arsenal.
Conclusion: Vitiligo treatment has entered an era of precision immune modulation, with JAK inhibitors establishing themselves as first-line therapy and novel biologics showing significant promise. Combined phototherapy and cellular therapy innovations markedly enhance repigmentation efficiency, and drug repurposing continues to enrich the therapeutic landscape.
Keywords: vitiligo, targeted therapy, JAK inhibitors, IL-15 inhibitors, combined phototherapy
Introduction
Vitiligo is a chronic autoimmune disorder characterized by the destruction and loss of skin melanocytes, with a global prevalence of approximately 0.5%-2%.1 Conventional treatment modalities,2 including phototherapy, topical calcineurin inhibitors, corticosteroids, systemic hormone therapy, and surgical transplantation techniques—exhibit significant limitations: long-term corticosteroid use frequently leads to skin atrophy, telangiectasia, and steroid dependence; phototherapy requires frequent interventions (2–3 sessions per week) and demonstrates suboptimal efficacy in acral regions; while surgical approaches carry the risk of donor-site scarring. There exists an urgent clinical need for safer and more effective innovative treatments.
Recent years have witnessed transformative advances in our understanding of vitiligo’s immunopathogenesis, particularly through elucidation of core mechanisms such as aberrant activation of the JAK/STAT pathway and CD8⁺ T cell-mediated melanocyte damage. These breakthroughs have catalyzed the development of targeted immunomodulatory therapies, innovative phototherapy technologies, and novel cellular treatment strategies, collectively providing unprecedented directions for clinical translation.
Current Research on Vitiligo Treatment
Pathogenesis
The pathogenesis of vitiligo results from the interplay between autoimmune dysregulation and oxidative stress, with the central pathogenic mechanism being the melanocyte-specific destruction mediated by autoreactive CD8⁺ T cells.3 This process initiates with danger-signal-triggered immune system activation: CD8⁺ T cells recognize melanocyte surface antigens and launch cytotoxic attacks, while simultaneously secreting interferon-gamma (IFN-γ). IFN-γ activates the JAK/STAT signaling pathway, inducing keratinocytes and melanocytes to overexpress chemokines CXCL9/10. These chemokines further recruit CXCR3⁺ CD8⁺ T cells to infiltrate lesional skin, establishing a self-perpetuating cycle of amplified immune attack.4
Oxidative stress plays a central initiating role in the pathogenesis of vitiligo: the high metabolic activity of melanocytes leads to excessive generation of reactive oxygen species (ROS), while functional defects in the skin’s antioxidant system result in ROS accumulation, directly triggering mitochondrial dysfunction, endoplasmic reticulum stress, and apoptosis. Simultaneously, ROS promote the release of inflammatory cytokines by activating the NF-κB pathway and stimulate melanocytes to release exosomes enriched with HSP70i, which activate dermal dendritic cells (cDC1) via the JAK1/TYK2-STAT signaling axis, initiating antigen presentation. The oxidative stress environment also upregulates interferon-stimulated genes such as ISG15, promoting sustained secretion of IFN-γ by CD8⁺ T cells; IFN-γ, in turn, induces keratinocytes to highly express CXCL9/CXCL10 through the JAK-STAT pathway, recruiting more autoreactive CD8⁺ T cells and forming a vicious cycle of “oxidative stress-immune attack” (Figure 1).
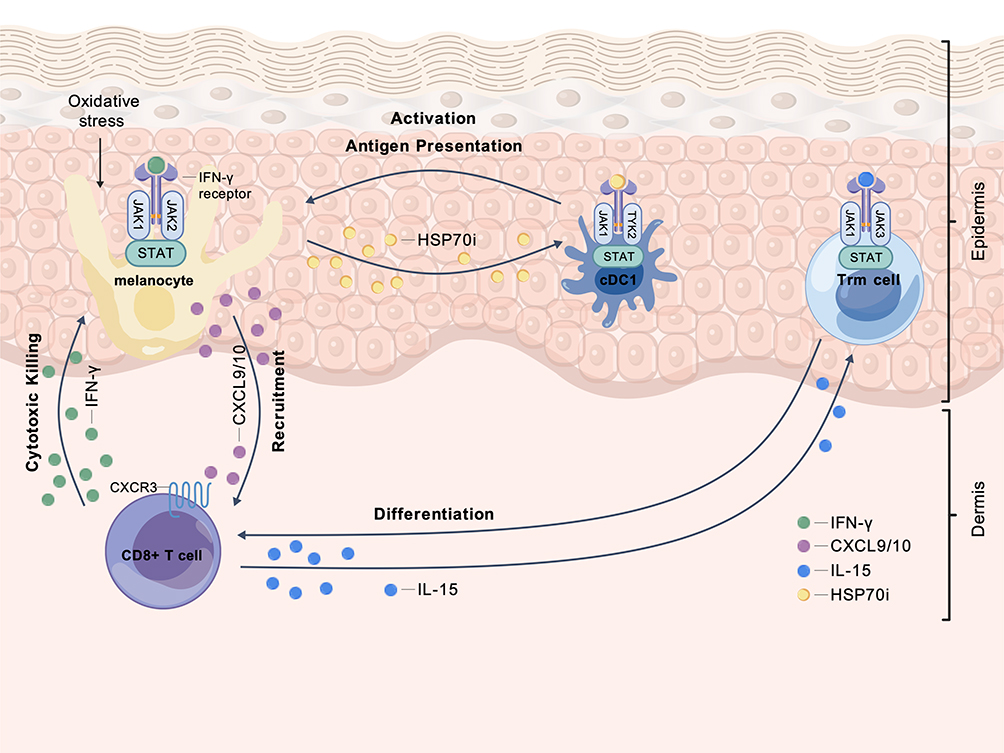 |
Figure 1 Pathogenesis of vitiligo. The schematic illustrates the core autoimmune mechanisms driving melanocyte destruction. Key processes include: CD8⁺ T cell activation following antigen presentation by cDC1; cytotoxic killing of melanocytes and IFN-γ secretion; JAK-STAT pathway activation by IFN-γ in melanocytes, inducing chemokine (CXCL9/10) production and recruiting additional T cells; and persistence of Trm cells maintained by IL-15 signaling via JAK-STAT, enabling disease recurrence. Abbreviations: cDC1, conventional type 1 dendritic cell; Trm, tissue-resident memory T cell. |
Furthermore, tissue-resident memory T cells (Trm) persist long-term with the support of IL-15 (signaling dependent on the JAK-STAT pathway), leading to disease recurrence and stubborn relapse; matrix metalloproteinase (MMP)-mediated degradation of E-cadherin disrupts melanocyte anchoring, while the local inflammatory microenvironment suppresses Treg function and weakens immune tolerance. These mechanisms, together with the JAK-STAT pathway, form a network that drives disease progression.5,6
Current Therapies2
Phototherapy remains the cornerstone of vitiligo management. Narrowband UVB (NB-UVB) is widely recommended as a first-line treatment for non-segmental vitiligo, typically administered 2–3 times per week. While effective for truncal and facial lesions, its efficacy is notably lower in acral areas (repigmentation rates <30%) and treatment often requires 6–12 months or longer. The 308nm excimer laser/light offers targeted phototherapy with potentially faster onset of repigmentation, but its accessibility and cost can be limiting factors.
Topical immunomodulators are first-line for facial and intertriginous areas. Calcineurin inhibitors (tacrolimus, pimecrolimus) are preferred over corticosteroids for sensitive areas to avoid skin atrophy. Topical corticosteroids are effective but their long-term use is restricted by risks of atrophy, telangiectasia, and steroid dependence.
Systemic immunomodulators are utilized for active or rapidly progressive disease. Oral corticosteroid minipulse therapy (eg, betamethasone/dexamethasone on 2 consecutive days per week) can halt disease progression. Conventional immunosuppressants like methotrexate, azathioprine, cyclosporine, and mycophenolate mofetil are also employed, albeit with varying levels of evidence and requiring monitoring for potential adverse effects.
Surgical interventions, including autologous skin grafting, suction blister epidermal grafting, and non-cultured epidermal cell suspensions, are reserved for stable, refractory vitiligo. Success depends on careful patient selection, as variable repigmentation and donor-site scarring remain challenges.
Combination therapy has long been a cornerstone of vitiligo management to enhance efficacy. Established regimens include the combination of phototherapy (NB-UVB) with topical calcineurin inhibitors or corticosteroids, and oral corticosteroid minipulse therapy combined with NB-UVB to concurrently suppress disease activity and stimulate repigmentation.7
Recent Advances (2020-2025)
Targeted Immunomodulation
JAK Inhibitors
Mechanism: The JAK family (JAK1-3, TYK2) are key molecules in cytokine signal transduction.8 In vitiligo, IFN-γ binds to receptors associated with JAK1/JAK2 to initiate signaling. Under oxidative stress, melanocyte-derived exosomes release HSP70, which activates plasmacytoid dendritic cells via JAK1/TYK2 to produce type I IFNs, inducing keratinocytes to express CXCL9/10. Dermal fibroblasts’ sensitivity to IFN-γ also contributes to the recruitment of CD8⁺ T cells. JAK inhibitors block the JAK1/2/3 pathway, suppressing immune responses mediated by proinflammatory cytokines such as IFN-γ and IL-15.9
Advances
Ruxolitinib
A JAK1/JAK2 inhibitor. Phase II trials of its cream formulation have demonstrated significant repigmentation in adults with vitiligo.10 The pivotal Phase III trials (TRuE-V1/V2) confirmed the efficacy and safety of ruxolitinib cream, leading to its regulatory approval.11 A separate Phase II study (NCT05247489) had explored its combination with phototherapy.12 Studies on its application in genital areas (NCT05750823) are ongoing.13
Baricitinib
A selective JAK1/JAK2 inhibitor.14,15 Its Phase II trial combined with phototherapy (NCT04822584) first confirmed efficacy in generalized vitiligo,16 providing evidence for combination therapies.17
Tofacitinib
Inhibits JAK1/JAK3 and partially JAK2/TYK2 activity. Oral administration of 510 mg twice daily achieves satisfactory repigmentation, with enhanced effects when combined with sunlight or NB-UVB therapy.18
Upadacitinib
A highly selective JAK1 inhibitor. Phase II studies showed that the 22 mg group had a significantly higher rate of vitiligo improvement (11.6%) compared to placebo (0%), along with a notable reduction in dermatology life quality index scores.19 Phase III trials (NCT06118411) are ongoing.20
Ritlecitinib
An irreversible JAK3/TEC kinase inhibitor21 that suppresses IL-2/IL-15induced cytotoxicity in Trm cells.22 In Phase IIb trials, the 50 mg daily group (with a loading dose of 200 mg/day for 4 weeks) achieved a 21.2% reduction in F-VASI at 24 weeks, significantly outperforming placebo. Phase III trials (NCT05583526) are ongoing.23
SHR0302 Gel
A highly selective JAK1 inhibitor with excellent Phase III data for atopic dermatitis.24 It is currently in early-stage clinical trials for vitiligo (NCT04774809)25 and is expected to become China’s first topical JAK inhibitor.
Additionally, novel JAK pathway-targeting drugs such as ICP-332 (with prior efficacy in AD)26 and VC005 have advanced to Phase II trials for vitiligo,27 indicating a forthcoming expansion of the therapeutic landscape.
IL-15 inhibitor
The novel drug AMG714 suppresses T cell activation by blocking IL-15 signaling, thereby reducing immune attacks on melanocytes at the source.28 Its phase IIa randomized controlled trial (NCT04338581) is currently evaluating the achievement rate of Facial-Vitiligo Area Scoring Index ≥35 (F-VASI35) after 24 weeks of treatment.29
PDE4 Inhibitors
Roflumilast and crisaborole inhibit inflammation and promote melanocyte proliferation via the cAMP pathway. Crisaborole development has been paused due to corporate strategy adjustments, while 0.3% roflumilast cream applied once daily has shown efficacy in repigmenting refractory facial vitiligo in children with good tolerability.30
Other Targeted Agents
Abatacept (CTLA4 fusion protein): Suppresses T cell activation. Phase I trials (NCT02281058) are ongoing.31
Afamelanotide (α-MSH analog): Activates MC1R to promote melanogenesis. Phase III trials (NCT06109649) are comparing its efficacy in combination with NB-UVB versus NB-UVB monotherapy.32
Rapamycin (mTOR inhibitor): Modulates Treg function. Phase II trials (NCT05342519) are evaluating topical rapamycin cream (0.1%/0.001%).33
Metformin: Regulates immunometabolism via the AMPK pathway. Phase II trials (NCT05607316) are exploring its clinical value.34
Optimization of Phototherapy (308nm Excimer Laser)
Combination with JAK Inhibitors
Baricitinib combined with phototherapy significantly improves both the speed and extent of repigmentation.17
Combination with Platelet-Rich Plasma (PRP)
Increased repigmentation rates in acral lesions from 26.8% with phototherapy alone to 56.1%,35 likely due to growth factors in PRP promoting melanocyte survival.
Combination with Vitamin D Supplementation
Oral vitamin D enhances the repigmentation effect of excimer laser, possibly through immunomodulatory synergy.36
Cellular Therapy and Surgical Innovations
Non-Cultured Cellular Grafting
Autologous cellular grafting has revolutionized the surgical repigmentation of stable vitiligo by transplanting melanocyte-rich suspensions. The most established technique is the non-cultured epidermal cell suspension (NCES, often referred to as “ReCell” technology), which involves applying a suspension of melanocytes and keratinocytes onto dermabraded depigmented skin. A prospective multicenter study is evaluating the repigmentation efficacy of transplanting autologous skin cell suspensions combined with home-based NB-UVB phototherapy for stable depigmented lesions,37 highlighting the trend of combining surgical and light-based modalities. Beyond standard NCES, evolving strategies aim to harness additional melanocyte reservoirs to enhance outcomes, particularly in challenging cases.
Combined Epidermal and Follicular Cell Suspension
For patients with stable yet refractory vitiligo, particularly in difficult-to-treat areas such as acral sites, bony prominences, and regions with leukotrichia, a significant surgical advance is the combined transplantation of non-cultured epidermal cell suspension (NCES) and follicular cell suspension (FCS). This integrated strategy synergistically utilizes the two primary reservoirs of melanocytes and their precursors: the interfollicular epidermis and the melanocyte stem cell (MelSC)-rich outer root sheath of hair follicles.
The clinical superiority of this combined approach over NCES alone has been established by randomized controlled trials. In a seminal study, the NCES + FCS combination demonstrated significantly better outcomes in extent of repigmentation (76% vs 57%), repigmentation rapidity, color match, and patient satisfaction. The enhanced efficacy is attributed to the combined suspension containing a higher proportion of MelSCs and exhibiting upregulated expression of key growth factors (eg, basic fibroblast growth factor and stem cell factor), which are crucial for melanocyte proliferation and survival.38
Recent comparative studies have further validated this strategy. One study reported that 65% of patients in the combined (NCES+FCS) group achieved >75% repigmentation at 4 months, compared to 30% in the NCES-only group, with significantly higher patient satisfaction in the combined group.39 Another study demonstrated that after 6 months, the combination of FCS with mini-punch grafting (a tissue-cellular hybrid approach) yielded significantly better repigmentation than either technique alone, highlighting the additive benefit of incorporating follicular-derived cells.40
This integrated technique, which merges cellular sources from both the epidermis and hair follicles, is now recognized in surgical consensus as a first-line or valuable option for stable, refractory vitiligo. It represents a strategic evolution in cellular therapy, moving beyond single-source grafts towards a combinatorial, physiology-driven approach aimed at achieving more robust, uniform, and durable repigmentation, especially in challenging cases that are resistant to conventional therapies.
Innovations in Tissue Grafting Tools and Techniques
Parallel to advances in cellular grafting, significant refinements have been made in traditional tissue grafting methods to improve cosmetic outcomes and reduce morbidity. Instrument innovation is key; for instance, customized, small-diameter electric micro-punches enable mini-punch grafting (MPG) with minimal donor-site trauma, making it particularly suitable for exposed areas like the face and forearms while reducing scarring risk.41 Furthermore, technical modifications such as the transverse incision technique in MPG have been reported to further reduce scar formation and accelerate repigmentation,42 showing particular efficacy in anatomically nuanced areas like the hairline.43 These continuous improvements in precision tools and surgical methods enhance the versatility and patient acceptance of tissue-based grafts for stable vitiligo.
Novel Applications of Traditional Drugs
Total Glucosides of Paeony (TGP)
Combined with NB-UVB and corticosteroid pulse therapy, significantly improves lesion area and disease activity in non-segmental vitiligo.44
Oral Compound Glycyrrhizin (OCG)
When combined with phototherapy in pediatric progressive vitiligo, effectively controls disease progression and accelerates repigmentation.45
Emerging Targets and Technologies
Biomarkers
Serum S100B levels significantly correlate with disease activity and may serve as objective indicators for monitoring and treatment evaluation.46
Psychological Intervention
Vitiligo patients often experience depression and anxiety, leading to low self-esteem and social isolation.47 Psychotherapy can improve emotional state and treatment compliance, with ongoing efficacy evaluation trials (NCT05991596).48
Novel Strategies for Promoting Melanocyte Repigmentation
Antioxidant Therapy
Vitamin E/C and α-lipoic acid protect melanocytes by neutralizing ROS, enhancing repigmentation efficiency when combined with phototherapy.49,50
Melanocyte Activators
Wnt/β-catenin pathway activators promote melanocyte stem cell differentiation, while PGE2 analogs enhance melanocyte migration.51
Growth Factor Applications
Basic fibroblast growth factor (bFGF) and stem cell-conditioned medium promote melanocyte survival and regeneration via local injection or microneedle delivery.52,53
Physicochemical Adjuvant Techniques
Microneedling enhances drug penetration, while mild chemical peels accelerate epidermal renewal to improve local treatment outcomes.54
Traditional Chinese Medicine and Natural Compounds
Psoralen plus UVA (PUVA) induces repigmentation through photosensitization, while resveratrol exerts adjuvant effects via anti-inflammatory mechanisms.55
Summary of Clinical Evidence
The recent advances discussed above are supported by a robust pipeline of clinical research. Table 1 summarizes key findings from pivotal published trials, while Table 2 provides an overview of the status and scope of notable ongoing studies registered on ClinicalTrials.gov.
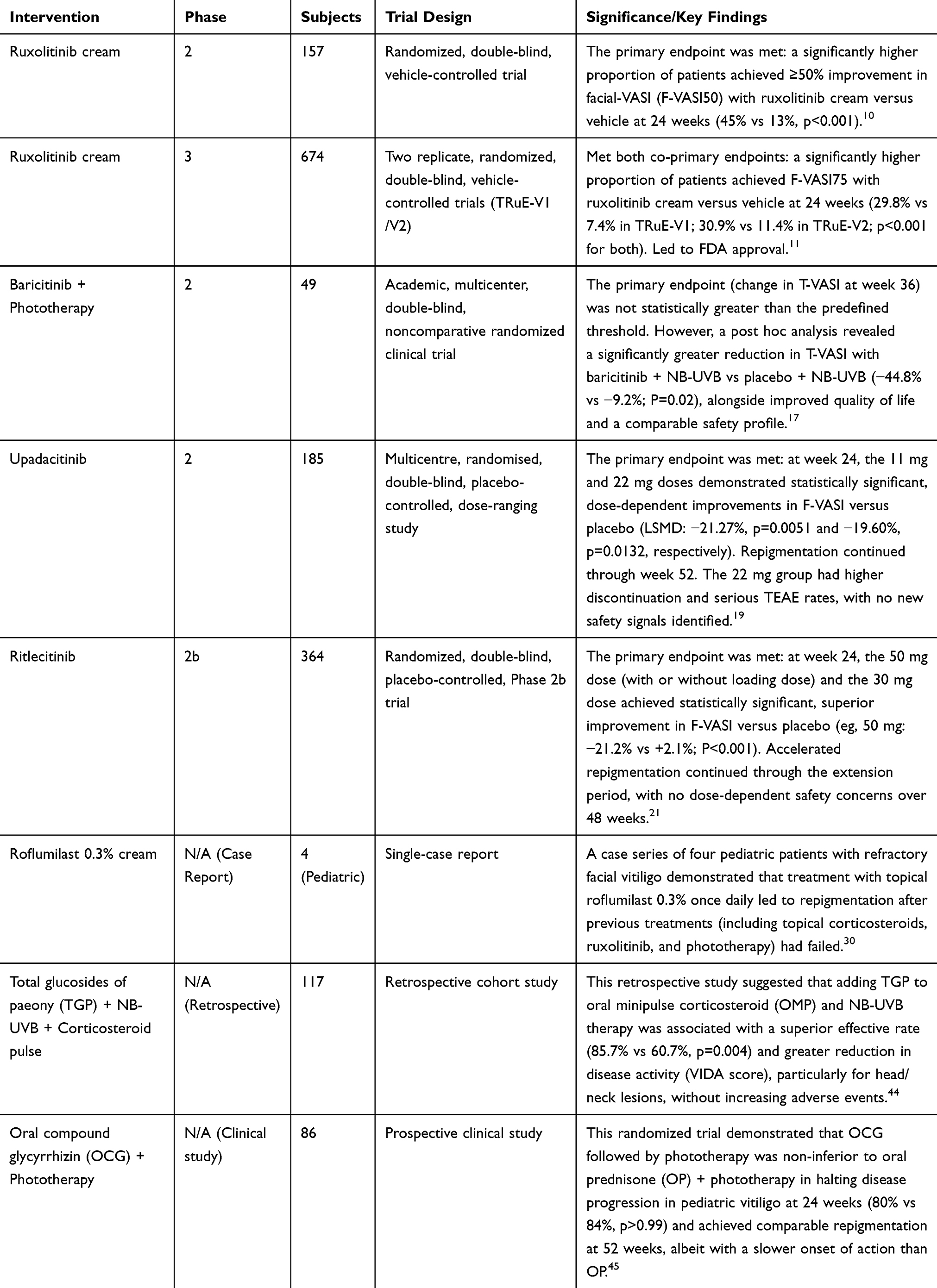 |
Table 1 Key Published Clinical Trials in Vitiligo (2020–2025) |
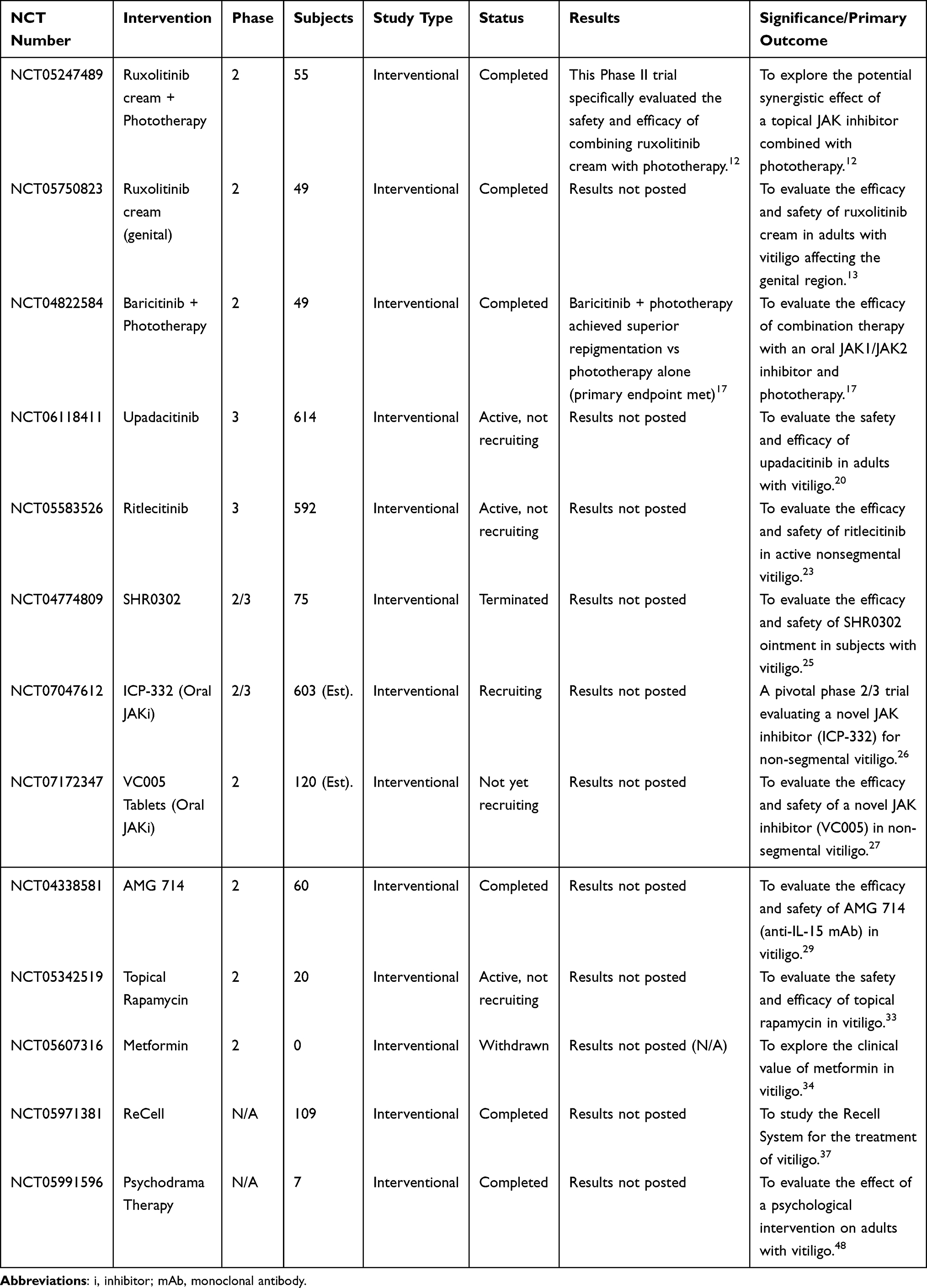 |
Table 2 Key Clinical Trials for Vitiligo (2020–2025) |
Summary and Future Perspectives
Summary
Vitiligo treatment has entered the era of “precision immunomodulation”: JAK inhibitors, with the approval of topical ruxolitinib cream marking a new epoch in targeted therapy, have become important treatment options and are increasingly used in clinical practice; novel therapies like IL-15 inhibitors block the source of immune attacks by eliminating pathogenic T cells; optimized phototherapy combinations and advancements in cellular therapy have significantly enhanced repigmentation efficiency; while the innovative use of traditional medications and antioxidant therapies has further diversified the therapeutic arsenal.
However, a critical analysis reveals a clear distinction between theoretical promise and established clinical evidence. JAK inhibitors, particularly topical ruxolitinib, currently possess the most robust data from large-scale Phase 3 trials, solidifying their real-world position. In contrast, the promise of IL-15 inhibitors and several other novel agents remains largely theoretical, pending confirmation from larger and longer-term studies. Furthermore, the current evidence base has notable limitations: many trials have relatively short follow-up periods, obscuring long-term safety and durability of response, especially for systemic immunomodulators. There is also a scarcity of head-to-head trials comparing novel therapies against each other or against optimized conventional combinations, making it difficult to establish a definitive treatment hierarchy. Finally, the high efficacy rates reported in structured clinical trials may not fully translate to routine practice, where patient adherence, comorbidities, and access to advanced therapies like cellular grafting can significantly impact outcomes.
Future Directions
Safety Studies
Long-term monitoring is required to assess the late-onset safety profiles of JAK inhibitors and IL-15 inhibitors, particularly regarding infection risks and potential oncogenic effects.
Combination Therapy Development
Future efforts should focus on investigating multimodal synergistic approaches combining immunomodulators, phototherapy, and cellular therapies, while developing personalized treatment strategies tailored to disease stages and lesion locations.
Technological Innovation
Develop precision treatment decision-making models based on biomarkers such as serum S100B and HLA typing;46 explore the feasibility of using CRISPR-Cas9 gene editing technology to repair melanocyte functional defects, thereby advancing vitiligo treatment from symptom control to targeting root causes.51
Acknowledgments
The figures are created in BioGDP.com.
Funding
Our work was supported by National Natural Science Foundation of China (NSFC) (82273551).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Ezzedine K, Eleftheriadou V, Whitton M, et al. Vitiligo. Lancet. 2015;386(9988):74–11. doi:10.1016/S0140-6736(14)60763-7
2. Seneschal J, Speeckaert R, Taïeb A, et al. Worldwide expert recommendations for the diagnosis and management of vitiligo: position statement from the international Vitiligo Task ForcePart 2: specific treatment recommendations. J Eur Acad Dermatol Venereol. 2023;37(11):21852195. doi:10.1111/jdv.19450
3. Frisoli ML, Essien K, Harris JE. Vitiligo: mechanisms of pathogenesis and treatment. Annu Rev Immunol. 2020;38:621648. doi:10.1146/annurevimmunol100919023531
4. Tulic MK, Cavazza E, Cheli Y, et al. Innate lymphocyte-induced CXCR3B-mediated melanocyte apoptosis is a potential initiator of T-cell autoreactivity in vitiligo. Nat Commun. 2019;10(1):2178. doi:10.1038/s41467-019-09963-8
5. Richmond JM, Strassner JP, Rashighi M, et al. Resident memory and recirculating memory T cells cooperate to maintain disease in a mouse model of vitiligo. J Invest Dermatol. 2019;139(4):769778. doi:10.1016/j.jid.2018.10.032
6. Lee EJ, Kim JY, Yeo JH, et al. ISG15-USP18 dysregulation by oxidative stress promotes IFN-γ secretion from CD8+ T cells in vitiligo. J Invest Dermatol. 2024;144(2):273–283.e11. doi:10.1016/j.jid.2023.08.006
7. Fai D, Cassano N, Vena GA. Narrow-band UVB phototherapy combined with tacrolimus ointment in vitiligo: a review of 110 patients. J Eur Acad Dermatol Venereol. 2007;21(7):916–920.
8. Inoue S, Suzuki T, Sano S, et al. JAK inhibitors for the treatment of vitiligo. J Dermatol Sci. 2024;113(3):8692. doi:10.1016/j.jdermsci.2023.12.008
9. Qi F, Liu F, Gao L. Janus kinase inhibitors in the treatment of vitiligo: a review. Front Immunol. 2021;12:790125. doi:10.3389/fimmu.2021.790125
10. Rosmarin D, Pandya AG, Lebwohl M, et al. Ruxolitinib cream for treatment of vitiligo: a randomised, controlled, phase 2 trial. Lancet. 2020;396(10244):110120. doi:10.1016/S0140-6736(20)30609-7
11. Rosmarin D, Passeron T, Pandya AG, et al. Two phase 3, randomized, controlled trials of ruxolitinib cream for vitiligo. N Engl J Med. 2022;387(16):1445–1455. doi:10.1056/NEJMoa2118828
12. A study to evaluate the efficacy and safety of ruxolitinib cream with phototherapy in participants with vitiligo.ClinicalTrials.gov identifier: NCT05247489. 2025. Available from: https://clinicaltrials.gov/study/NCT05247489.
13. A study to assess the safety and efficacy of ruxolitinib cream in participants with genital vitiligo. ClinicalTrials.gov identifier: NCT05750823.July 11, 2025. Available from: https://clinicaltrials.gov/study/NCT05750823.
14. Zhang J, Qi F, Dong J, et al. Application of Baricitinib in Dermatology. J Inflamm Res. 2022;15:1935–1941. doi:10.2147/JIR.S356316
15. Dong J, Huang X, Ma LP, et al. Baricitinib is effective in treating progressing vitiligo in vivo and in vitro. Dose Response. 2022;20(2):15593258221105370. doi:10.1177/15593258221105370
16. A study of the effect and tolerance of the association of baricitinib and phototherapy versus phototherapy in adults with progressive vitiligo (BARVIT). ClinicalTrials.gov identifier: NCT04822584. June 13, 2023. Available from: https://clinicaltrials.gov/study/NCT04822584.
17. Seneschal J, Guyon M, Merhi R, et al. Combination of baricitinib and phototherapy in adults with active vitiligo: a randomized clinical trial. JAMA Dermatol. 2025;161(4):375–382. doi:10.1001/jamadermatol.2024.5737
18. Sonthalia S, Aggarwal P. Oral tofacitinib: contemporary appraisal of its role in dermatology. Indian Dermatol Online J. 2019;10(5):503–518. doi:10.4103/idoj.IDOJ_474_18
19. Passeron T, Ezzedine K, Hamzavi I, et al. Once-daily upadacitinib versus placebo in adults with extensive non-segmental vitiligo: a phase 2, multicentre, randomised, double-blind, placebo-controlled, dose-ranging study. EClinicalMedicine. 2024:102655. Erratum in: EClinicalMedicine. 2025; 19;82:103167. doi:10.1016/j.eclinm.2025.103167. doi:10.1016/j.eclinm.2024.102655
20. A study to assess adverse events and effectiveness of upadacitinib oral tablets in adult and adolescent participants with vitiligo (Viti-Up). ClinicalTrials.gov identifier: NCT06118411. 2025. Available from: https://clinicaltrials.gov/study/NCT06118411.
21. Ezzedine K, Peeva E, Yamaguchi Y, et al. Efficacy and safety of oral ritlecitinib for the treatment of active nonsegmental vitiligo: a randomized phase 2b clinical trial. J Am Acad Dermatol. 2023;88(2):395–403. Erratum in: J Am Acad Dermatol. 2023; 89(3):639. doi:10.1016/j.jaad.2023.04.001. doi:10.1016/j.jaad.2022.11.005
22. Cheuk S, Schlums H, Gallais Sérézal I, et al. CD49a expression defines tissueResident CD8+ T cells poised for cytotoxic function in human skin. Immunity. 2017;46(2):287300. doi:10.1016/j.immuni.2017.01.009
23. A 52-week study of ritlecitinib oral capsules in adults and adolescents with nonsegmental vitiligo (Active and Stable) Tranquillo (Tranquillo). ClinicalTrials.gov identifier: NCT05583526. July 11, 2025. Available from: https://clinicaltrials.gov/study/NCT05583526.
24. Zhao Y, Zhang L, Ding Y, et al. Efficacy and safety of SHR0302, a highly selective Janus kinase 1 inhibitor, in patients with moderate to severe atopic dermatitis: a phase ii randomized clinical trial. Am J Clin Dermatol. 2021;22(6):877–889. doi:10.1007/s40257-021-00627-2
25. A study to assess the efficacy and safety of SHR0302 ointment in adult patients with vitiligo. ClinicalTrials.gov identifier: NCT04774809. 2022. Available from: https://clinicaltrials.gov/study/NCT04774809.
26. A study of ICP-332 in subjects with non-segmental vitiligo. ClinicalTrials.gov identifier: NCT07047612. 2025. Available from: https://clinicaltrials.gov/study/NCT07047612.
27. A phase II study of the efficacy and safety of VC005 tablets in subjects with non-segmental vitiligo. ClinicalTrials.gov identifier: NCT07172347. 2025. Available from: https://clinicaltrials.gov/study/NCT07172347.
28. Su X, Liu F. Targeting the IL-15/CD122 signaling pathway: reversing TRM cell-mediated immune memory in vitiligo. Front Immunol. 2025;16:1639732. doi:10.3389/fimmu.2025.1639732
29. A study to evaluate AMG 714 for vitiligo (REVEAL). ClinicalTrials.gov identifier: NCT04338581. 2025. Available from: https://clinicaltrials.gov/study/NCT04338581.
30. Warren K, Sanchez S. Recalcitrant pediatric facial vitiligo successfully treated with roflumilast cream 0.3% once daily. J Clin Aesthet Dermatol. 2025;18(1):52–54.
31. An open-label pilot study of Abatacept for the treatment of vitiligo. ClinicalTrials.gov identifier: NCT02281058. 2017. Available from: https://clinicaltrials.gov/study/NCT02281058.
32. A study to compare the efficacy and safety of SCENESSE and narrow-band ultraviolet (NB-UVB) light versus NB-UVB light alone in patients with vitiligoClinicalTrials.gov identifier: NCT06109649. 2025. Available from: https://clinicaltrials.gov/study/NCT06109649.
33. A study of daily topical rapamycin for vitiligo. ClinicalTrials.gov identifier: NCT05342519. 2025. Available from: https://clinicaltrials.gov/study/NCT05342519.
34. A study to evaluate the efficacy and safety of metformin in vitiligo. ClinicalTrials.gov identifier: NCT05607316. 2024. Available from: https://clinicaltrials.gov/study/NCT05607316.
35. Khalili M, Solhjou S, Amiri R, et al. Triple combination of fractional carbon dioxide laser, 308nm excimer lamp, and plateletrich plasma in refractory vitiligo: a randomized splitbody comparative study. J Cutan Aesthet Surg. 2025;18(1):3441. doi:10.25259/JCAS_16_2024
36. Kim JC, Kim HR, Park JS, et al. Vitamin D supplementation can enhance therapeutic effects of excimer laser in patients with vitiligo. J Cosmet Dermatol. 2024;23(3):839848. doi:10.1111/jocd.16043
37. A study of the repigmentation of stable vitiligo lesions using Spray-On Skin™ cells (TONE). ClinicalTrials.gov identifier: NCT05971381. 2025. Available from: https://clinicaltrials.gov/study/NCT05971381.
38. Razmi T, Kumar R, Rani S, Kumaran SM, Tanwar S, Parsad D. Combination of follicular and epidermal cell suspension as a novel surgical approach in difficult-to-treat vitiligo: a randomized clinical trial. JAMA Dermatol. 2018;154(3):301–308. doi:10.1001/jamadermatol.2017.5795
39. Eleslam Shaker ES, Abdelkawy Abdelaal SS, Mostafa WA, Nassar SO. Comparative study between combined follicular and epidermal cell suspension versus epidermal cell suspension in treatment of stable vitiligo. Arch Dermatol Res. 2025;317(1):388. doi:10.1007/s00403-025-03813-y
40. ElGhareeb MI, Kandeel AH, Attia SA. Combination of autologous FCS and MPG versus each technique alone in the treatment of stable vitiligo. Arch Dermatol Res. 2024;316(7):358. doi:10.1007/s00403-024-03045-6
41. Kerure AS, Ghia DH, Sabhandasani SP, et al. Customized short punches for mini punch grafting in vitiligo. J Cutan Aesthet Surg. 2025;18(1):6365. doi:10.25259/JCAS_144_2024
42. Ragab M, El Zagh O, Farid C. Transverse needling after autologous MiniPunch grafts improves repigmentation in stable nonsegmental vitiligo. Clin Cosmet Invest Dermatol. 2021;14:827835. doi:10.2147/CCID.S315407
43. Zhou Q, Wang W, Yu Q, et al. Transversely sectioned minipunch grafting: a novel technique for effective treatment of hairline vitiligo. Clin Cosmet Invest Dermatol. 2023;16:15391543. doi:10.2147/CCID.S412948
44. Gui J, Li Z, Zhou B, et al. Combination of total glucosides of paeony, narrowband ultraviolet B, and oral corticosteroid minipulse therapy for nonsegmental vitiligo: a retrospective study. Skin Res Technol. 2024;30(6):e13769. doi:10.1111/srt.13769
45. Zhang J, Zhang L, Liu S, et al. Effectiveness and safety of oral compound glycyrrhizin followed by phototherapy for the treatment of progressive vitiligo in children. Pigm Cell Melanoma Res. 2025;38(2):e13226. doi:10.1111/pcmr.13226
46. He K, Li S, Li C, et al. Circulatory levels of alarmins in patients with non-segmental vitiligo: potential biomarkers for disease diagnosis and activity/severity assessment. Front Immunol. 2022;13:1069196. doi:10.3389/fimmu.2022.1069196
47. Osinubi O, Grainge MJ, Hong L, et al. The prevalence of psychological comorbidity in people with vitiligo: a systematic review and metaanalysis. Br J Dermatol. 2018;178(4):863878. doi:10.1111/bjd.16049
48. A study of vitiligo and psychodrama therapy. ClinicalTrials.gov identifier: NCT05991596. 2025. Available from: https://clinicaltrials.gov/study/NCT05991596.
49. Chang WL, Ko CH. The role of oxidative stress in vitiligo: an update on its pathogenesis and therapeutic implications. Cells. 2023;12(6):936. doi:10.3390/cells12060936
50. Speeckaert R, Bulat V, Speeckaert MM, van Geel N. The impact of antioxidants on vitiligo and melasma: a scoping review and meta-analysis. Antioxidants. 2023;12(12):2082. doi:10.3390/antiox12122082
51. Huang L, Zuo Y, Li S, Li C. Melanocyte stem cells in the skin: origin, biological characteristics, homeostatic maintenance and therapeutic potential. Clin Transl Med. 2024;14(5):e1720. doi:10.1002/ctm2.1720
52. Salem SAM, Fezeaa TA, El Khazragy N, Soltan MY. Effect of platelet-rich plasma on the outcome of mini-punch grafting procedure in localized stable vitiligo: clinical evaluation and relation to lesional basic fibroblast growth factor. Dermatol Ther. 2021;34(2):e14738. doi:10.1111/dth.14738
53. Wang Q, Guo W, Niu L, et al. 3D-hUMSCs exosomes ameliorate vitiligo by simultaneously potentiating treg cells-mediated immunosuppression and suppressing oxidative stress-induced melanocyte damage. Adv Sci. 2024;11(31):e2404064. doi:10.1002/advs.202404064
54. Salloum A, Bazzi N, Maalouf D, Habre M. Microneedling in vitiligo: a systematic review. Dermatol Ther. 2020;33(6):e14297. doi:10.1111/dth.14297
55. Sahu N, Jain P, Sahu D, Kaur K, Nagori K, Ajazuddin. Recent trends in the treatment of vitiligo using novel drug delivery system. Int J Pharm. 2025;670:125106. doi:10.1016/j.ijpharm.2024.125106
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Case of Vitiligo Combined with Systemic Lupus Erythematosus Treated with Tofacitinib
Lin Q, Zhu J, Gao X
Clinical, Cosmetic and Investigational Dermatology 2024, 17:707-711
Published Date: 20 March 2024
Concurrent Refractory Atopic Dermatitis and Generalized Vitiligo Successfully Treated with Abrocitinib: A Case Report
Shao X, Pan X, Chen Y, Zhu Y, Chen S, Chen J
Journal of Asthma and Allergy 2024, 17:1259-1263
Published Date: 3 December 2024
Treatment of Generalized Granuloma Annulare with JAK Inhibitors: Systematic Review
Jaguan D, Gratz BW, Jaguan SI, Ehrlich A
Clinical, Cosmetic and Investigational Dermatology 2026, 19:524634
Published Date: 20 April 2026