Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Recent Advances in Multimodal Non-Pharmacological Interventions for Late-Life Depression
Authors Xu T, Mao Y, Wang Y, Gong Y, Yu E
Received 22 August 2025
Accepted for publication 11 November 2025
Published 20 November 2025 Volume 2025:21 Pages 2525—2544
DOI https://doi.org/10.2147/NDT.S558969
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Tianmei Xu,1,2 Yanping Mao,2 Ye Wang,3 Yi Gong,1 Enyan Yu2
1The Second Clinical Medical College of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Psychiatry, The Cancer Hospital of the University of Chinese Academy of Sciences (Zhejiang Cancer Hospital), Hangzhou, Zhejiang, People’s Republic of China; 3Tongde Hospital of Zhejiang Province, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Enyan Yu, Department of Psychiatry, The Cancer Hospital of the University of Chinese Academy of Sciences (Zhejiang Cancer Hospital), 1 Banshandong Road, Hangzhou, Zhejiang, 310022, People’s Republic of China, Tel +86 0571-88122222, Email [email protected]
Abstract: Late-life depression (LLD) is a common mental disorder that significantly accelerates cognitive decline, increases the risk of somatic comorbidities, and increases all-cause mortality. Traditional pharmacotherapy for this population faces significant limitations, including increased pharmacokinetic sensitivity, anticholinergic burden, and adverse events associated with multiple medications. These factors collectively lead to poor adherence and limited long-term efficacy. This narrative literature review was conducted using studies retrieved from PubMed, ScienceDirect, and Google Scholar, with general search phrases on LLD and non-pharmacological interventions. The inclusion criteria were clinical trials, meta-analyses, and systematic reviews published between 2020 and 2025. Studies that were finally selected were comprehensively evaluated, with non-English literature and case reports excluded. Non-pharmacological interventions have become a core strategy for the management of LLD due to the advantages of high safety, fewer side effects, and a multi-target nature. Psychotherapy, physical intervention, digital technology, and lifestyle modification can effectively improve patients’ depressive symptoms, improve quality of life, reduce the risk of relapse, and serve as possible alternatives and supplementary treatment options for older patients. There is a need for more in-depth research on non-pharmacological interventions for LLD. Future studies should explore the combined application of different non-pharmacological treatments to optimize treatment plans. Developing individualized non-pharmacological treatment plans to improve the accuracy of treatment and reduce the burden of disease should be considered.
Keywords: older adults, psychiatric disorder, therapy
Introduction
Late-life depression (LLD) is a major depressive disorder occurring in adults aged 65 years and older, with symptoms that often interact with cognitive decline, chronic pain, and social isolation.1 LLD is among the most common psychiatric disorders of old age in later life, with a global prevalence rate of approximately 28.4%.2 The increasing global burden of LLD varies by socioeconomic, gender, regional, and national differences.3 Compared with adult depression, LLD symptoms are often masked by physical illness and cognitive decline, leading to its untimely diagnosis and treatment.4 Although antidepressants can be effective in ameliorating some LLD symptoms, multiple medical comorbidities and drug interactions, in cases of polypharmacy, often pose a more serious adverse events risk.5 Studies have shown that less than half of older adults with major depressive disorder achieve remission when receiving medication alone.6 Notably, many patients with LLD achieve remission of mood symptoms but still have persistent neuropsychological deficits.7,8 The mechanism may be closely related to abnormal functional connectivity of the default mode network (DMN)9 (excessive activation of the DMN promotes ruminative thinking and cognitive rigidity, driving a vicious cycle of depression and cognitive deterioration), which may form the neurobiological basis of LLD relapse. Given that single-modal interventions cannot fully reverse the multi-dimensional pathological mechanisms of LLD, there is an urgent need to achieve complementary and synergistic effects through multi-modal non-pharmacological intervention strategies that integrate neuromodulation, psychobehavioral, and lifestyle components. Such integrated strategies can act on the remodeling of neuroplasticity, regulation of metabolism during inflammation, and repair of social neural circuits, thereby optimizing clinical outcomes and reducing the risk of recurrence. Although previous studies on non-pharmacological interventions for LLD have mostly focused on single therapies10 or followed adult intervention models, such as standard cognitive behavioral therapy, they have generally overlooked the unique clinical complexity of LLD. Consequently, these studies have failed to fully reflect the adaptive adjustments that are tailored to the older adult population, and the intervention settings have mostly been limited to hospitals. This article transcends the traditional single-therapy perspective by integrating psychological, physical, nutritional, and community interventions for treating LLD. It emphasizes the exploration of multi-modal collaborative strategies and personalized treatment planning based on cutting-edge technologies. The article further focuses on bridging the gap between hospital-oriented treatment models and community-based practices, offering a novel perspective for establishing a comprehensive management model for LLD.
Non-Pharmacological Interventions for Late-Life Depression Treatment
Psychotherapy
Psychotherapy for LLD is a non-pharmacological intervention during which professional therapists use structured techniques aimed at modifying patients’ maladaptive cognitive, emotional, and behavioral patterns to improve symptoms, functioning, and quality of life. Current guidelines recommend psychotherapy as the first choice for initial treatment in patients with mild-to-moderate LLD and a combined treatment of antidepressants and psychotherapy for patients with moderate-to-severe depression11 to improve clinical efficacy and treatment adherence. A meta-analysis further confirmed that psychotherapy is significantly advantageous in moderating depression in older patients, with effect sizes of moderate or higher (standardized mean effect size d = 0.72).12 Notably, all psychological interventions compared to conventional treatment were at least moderately effective in improving depressive symptoms in adults, while all 21 antidepressant medications had small-to-moderate effects on symptom improvement.13 Current psychological interventions for LLD include behavioral therapy (BT), cognitive behavioral therapy (CBT), cognitive bibliotherapy, problem-solving therapy (PST), brief psychodynamic therapy (BPD), and reminiscence therapy (RT).14
Cognitive Behavioral Therapy
CBT is a structured, problem-oriented psychotherapeutic model whose core goal is to alleviate emotional symptoms and promote adaptive behavior and cognitive remodeling.15 CBT can partially normalize neural patterns by modulating neural activity in brain regions related to affective and reward processing (eg, amygdala-hippocampus complex, anterior cingulate gyrus, and prefrontal cortex), thereby improving mood and cognitive flexibility.16 Meta-analysis results have shown that CBT is significantly more effective than conventional treatment and wait-list control groups in alleviating depressive symptoms, and this advantage persists at the 6-month follow-up.17 Adaptations have been proposed to better accommodate the changes in sensory deficits, frailty, and mild cognitive impairment associated with aging and may facilitate the effectiveness of CBT for this older population,18 such as enhanced group CBT for older adults (CBT-OA), internet-based CBT (iCBT), and virtual reality (VR)-enhanced CBT (VR-CBT).
Enhanced Group Cognitive Behaviour Therapy for Older Adults (CBT-OA) modifies standard CBT to better meet the needs of older adults. Skosireva et al19 recruited 49 older adults aged >65 years between 2015 and 2019 who presented with symptoms of depression and/or anxiety and underwent five CBT-OA therapy sessions. They demonstrated a significant decrease in Beck Depression Inventory-II scores, with participants aged <78 years showing the greatest gains.
iCBT can effectively address the treatment gap in LLD caused by limited mobility, stigma, or geographical barriers. Meta-analyses have confirmed that iCBT has a positive impact on improving depression and mental health in older adults.20 Moreover, it demonstrates sustained long-term efficacy across all age groups, with observed consistent reductions in depression severity.21
VR-CBT, an innovative intervention, promotes emotional regulation and cognitive flexibility of older patients through multi-sensory stimulation by integrating traditional CBT with VR technology, making up for the limitations of traditional talk therapy. In the treatment of severe depression, VR-CBT has shown potential efficacy, which is comparable to standard pharmacological treatment, effectively alleviating depressive symptoms, suicidal tendencies, and associated anxiety and perceived stress.22
CBT-OA and iCBT can serve as non-pharmacological intervention options for most older adults with depression. VR-CBT is particularly suitable for those seeking an immersive therapeutic experience or for individuals who have not responded adequately to conventional antidepressant medications or standard psychological interventions. Although CBT and its technology-assisted forms represent effective approaches for treating LLD, offering diverse implementation pathways and good adaptability, research within the geriatric population remains limited. In the future, more clinical practice and technological iterations are needed to develop safe, effective, and humanized intervention programs.
Mindfulness-Based Cognitive Therapy
Mindfulness-based cognitive therapy (MBCT) is a novel treatment for depression that combines mindfulness meditation with elements of CBT to reduce negative emotions and anxiety, thereby helping to alleviate depressive symptoms.23 MBCT may improve rumination in this population by modulating the over-activation of the DMN,24 making them more capable of negative emotion regulation to become more competent. MBCT is increasingly being used in the older population, with age-related modifications, such as more sedentary meditation and shorter session durations. Age-modified MBCT is more helpful in controlling depressive symptoms in older patients.25 Further studies have shown that older populations receiving web-based mindfulness intervention do not only exhibit cognitive and emotional improvements but also demonstrate adaptive modulation of neural oscillatory rhythms in specific brain regions.26 MBCT is effective for treating LLD and preventing its recurrence, but individualized program adjustments are needed for groups with low cognitive reserve and acute severe illness.
Problem-Solving Therapy
PST, often considered a form of CBT, is a practical approach focusing on problem solving and action taking and aims to promote problem solving by instilling an optimistic and assertive attitude toward the problem.27 At present, the neural mechanism underlying the effect of this therapy remains unclear. One possibility is that PST improves depressive symptoms by enhancing the activity of the amygdala.28 PST is an effective treatment for LLD, and in a significant number of older adults with major depression and executive dysfunction, it results in significant therapeutic response and remission.29 For patients with LLD who have cognitive decline, a modified PST can significantly reduce depressive symptoms and improve response and remission rates within a 12-week intervention cycle through structured adjustments in therapist-led problem simplification and action planning.30 Modified PST (MPST) directs more focus on the relevance of knowledge transfer, empowering effect of group interaction, and establishment of early trusting relationships, which are more relevant to the cognitive characteristics and psychological needs of older adults.31 PST is efficient for addressing the real-life dilemmas of patients with LLD, especially suitable for patients with mild cognitive impairment. Its structured problem-solving process can significantly enhance functional independence; however, for those who have severe executive impairment and lack social support, it should be applied with caution. MPST can be used to enhance the feasibility of PST through family collaboration and simplification techniques.
Reminiscence Therapy
RT aims to promote patients’ sense of wholeness and adaptability, which emphasizes the review of life and recognition of life’s meaning and purpose. Neuroimaging studies have confirmed that it alleviates negative emotions by modulating the thalamocortical pathway and suppressing activity in pain-related brain regions, including the lingual and parahippocampal gyri.32 Liu et al33 found that RT does not only significantly improve depressive symptoms in older patients with chronic diseases but also positively affects LLD groups treated with antidepressant drugs. More notably, group-based RT was superior to individual interventions in terms of efficacy and cost-effectiveness. VR-RT, an innovative intervention, can significantly improve depressive mood and cognitive functioning in older groups without significant adverse effects and has the potential to be useful in more varied settings.34 Trauma history should be screened prior to RT implementation to avoid triggering agitated behaviors or worsening mood.35 RT may likely play a more important role in aging societies, but further research is needed to investigate its long-term effects on depression alleviation. The application of RT is varied in different cultural settings, and in the future, nostalgia intervention protocols should be further developed and standardized to promote its global use.
Cognitive Reading Therapy
Cognitive reading therapy guides patients to self-adjust their cognition through self-help books or materials, which can be understood as a process of reading, reflection, and discussion. In recent years, mental health scientists have studied reading therapy separately from traditional interventions to improve the lives of readers.36 Cognitive reading therapy works by guiding patients to engage in emotional projection and cognitive universalization, thereby effectively alleviating their negative emotions and enhancing their self-efficacy.36 It appears effective in reducing depressive symptoms in adults, and its use as an accessible, cost-effective, and timely intervention can reduce the need for antidepressant medication use.37 Floyd et al’s study38 involving 31 community-dwelling patients aged ≥60 years demonstrated that individual psychotherapy and reading therapy significantly outperformed the delayed-treatment control group. Notably, the reading therapy group exhibited sustained improvement trajectories, with therapeutic effects converging between the two interventions at the 3-month follow-up. This confirms both approaches as viable therapeutic alternatives for LLD. However, cognitive reading therapy lacks interpersonal interaction, has limited effect on those with strong feelings of loneliness, has independent efficacy in the older population, and still needs to be verified in randomized controlled trials (RCTs). Studies related to cognitive reading therapy for LLD treatment are few, and further explorations are still needed in the future.
As summarized in Table 1, the comparative analysis of psychological treatment methods for LLD shows that each method has unique advantages and disadvantages in terms of core mechanisms, target populations, accessibility, and other aspects. For patients with LLD who are frail or bedridden, BT or PST can be implemented using video conferencing to reduce the burden of travel. Caregiver assistance can be incorporated into this process to reinforce the intervention by recording daily activities or providing problem-solving support. For patients with severe somatic debilitation, any BT regimen requiring physical activity should be avoided in favor of supportive talk or RT. For those with severe cognitive impairment, CBT or cognitive reading therapy should be used with caution. Instead, simplified BT approaches—for instance, sensory stimulation activities—or fragmented recall during RT may be more appropriate. The use of tactile object aids (including old photographs and mementos) rather than only verbal recall can also help to reduce cognitive load in RT interventions. During a psychological intervention, the intensity and form of intervention should be dynamically adjusted according to the patient’s functional status. Moreover, physical exertion and emotional response should be continuously monitored. In the future, researchers can further explore joint models, such as “PST+RT”, to enhance the self-efficacy of patients in coping with current challenges by recalling their previous successful problem-solving experiences.
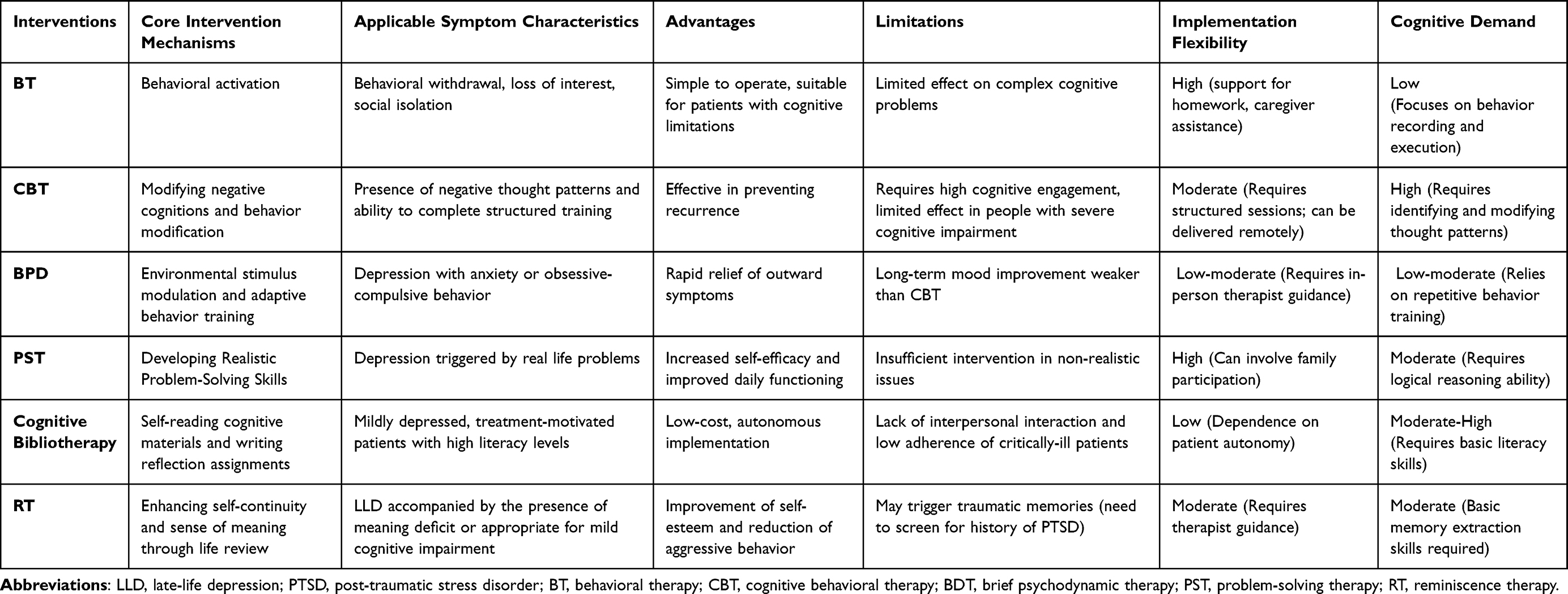 |
Table 1 Comparative Analysis of Psychotherapy Methods for Late-Life Depression |
Physical Therapy
Physical therapy for LLD is a non-pharmacological biological intervention based on neuroplasticity. It involves the precise modulation of physical energy (such as electricity, magnetism, or light) on specific brain regions to directly modify abnormal activity in emotion-processing neural circuits, thereby alleviating depressive symptoms and reducing suicide risk. Neuromodulation techniques currently applied to treat LLD include electroconvulsive therapy (ECT), repetitive transcranial magnetic stimulation (rTMS), vagus nerve stimulation (VNS), deep brain simulation (DBS) and transcranial direct current stimulation (tDCS).39 Furthermore, physical therapy for LLD includes exercise therapy and bright light therapy (BLT). Physical therapy does not only have a faster onset of effectiveness than that observed with single drug therapy but is also more suitable for the older population with coexisting multi-morbidities, as it does not impose systemic drug metabolism burden. The defining features of these neuromodulation and physical therapies for LLD are presented comparatively in Table 2.
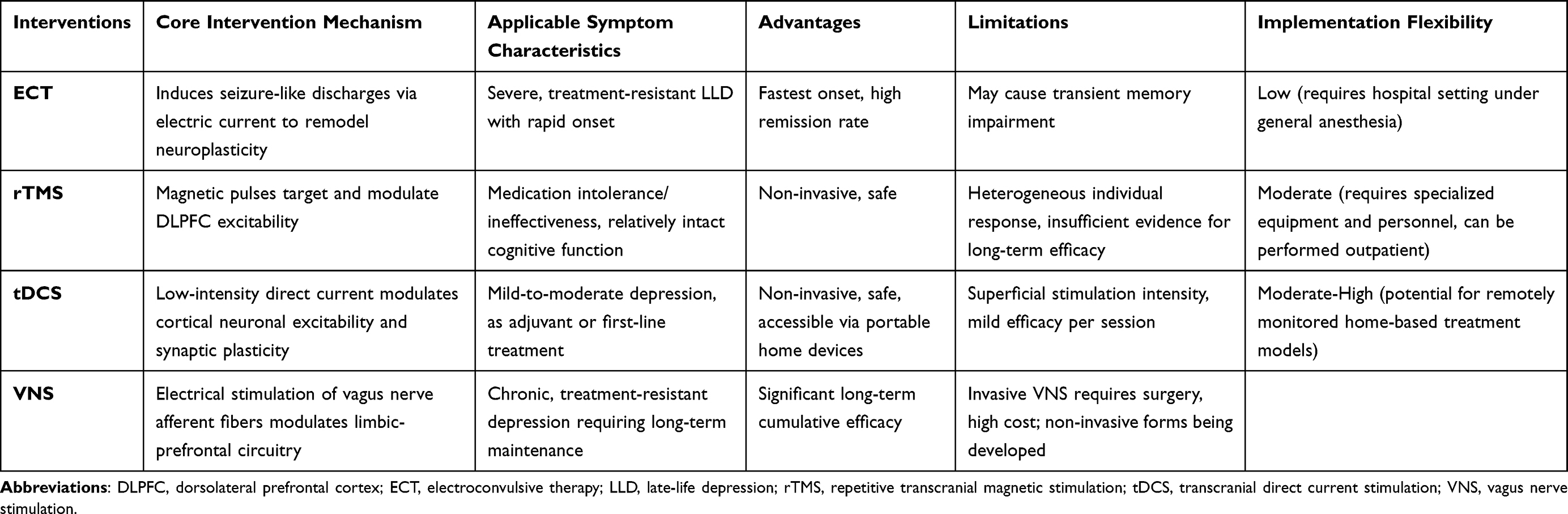 |
Table 2 Comparative Analysis of Physical Interventions for Late-Life Depression |
Electroconvulsive Therapy
ECT is a therapeutic method of stimulating the patient’s head with electric current to cause a grand mal seizure, which results in clinical symptom relief. The therapeutic mechanism of ECT stems from its ability to induce structural neuroplasticity in the brain, particularly, increased hippocampal volume and neurogenesis. This process is accompanied by the upregulation of neurotrophic factors at the molecular level and the reorganization of brain network function.40 Studies have demonstrated that ECT is most effective for severe LLD treatment, and the older the patient, the quicker the response to ECT and subsequent remission (remission rate, up to 80.1%).41 Novel and more tolerable forms of ECT are currently being investigated for LLD treatment, and preliminary results have suggested that right unilateral ultrashort ECT (RUL-UB ECT) is a promising intervention with antidepressant efficacy comparable with that of conventional short-pulse ECT, with less cognitive impact.42 RUL-UB ECT in combination with antidepressants significantly improves acute-phase remission rates and reduces relapse risk compared with that of single-agent therapy.43 Notably, the clinical efficacy of ECT was consistently superior to antidepressants in patients of all ages.44
Modified ECT (MECT) is also known as convulsion-free ECT due to the use of muscle relaxants prior to treatment. For refractory LLD, MECT is an effective, well-tolerated, and safe method.45 MECT is preferred in older patients; it reduces discomfort and anxiety during treatment. It can be used in combination with antidepressant medications, which can improve therapeutic efficacy, especially in the acute treatment phase.46
The specific mechanisms of ECT in the aging brain remain inadequately studied. It is currently unclear how to optimize key parameters such as electrode placement and stimulation dosage based on individual patient characteristics including brain structure and comorbidities. Although ECT is highly effective for acute symptom control, predicting and preventing post-ECT depressive relapse remains a critical research priority. Further exploration is needed to optimize treatment parameters for achieving the optimal balance between therapeutic efficacy and cognitive side effects.
Repetitive Transcranial Magnetic Stimulation
rTMS is a neuromodulation technique that non-invasively regulates the excitability of the cerebral cortex using a time-varying magnetic field. TMS modulates whole-brain network function by remodeling signal transmission among the dorsolateral prefrontal cortex (DLPFC), subgenual and dorsal anterior cingulate cortex, and salience-network regions. Additionally, it can promote the transition of behavioral states to positive patterns to exert an antidepressant effect. Its long-lasting therapeutic effect relies on synaptic plasticity, mediated by dopamine and NMDA receptors.47 The application of rTMS in LLD has yielded clinically significant and sustained improvements in quality of life. This is similar to the outcomes observed in younger patients and is comparable to or superior to the benefits of antidepressant medications.48 Remission rates for LLD treated with rTMS range from 20% to 63%, with bilateral stimulation modalities or high-frequency regimens generally showing superior efficacy.49 In addition, the new theta burst stimulation (TBS) patterns, especially bilateral intermittent TBS, have also proven to effectively improve depressive symptoms and executive functions with excellent tolerability.50 Compared with unilateral stimulation, sequential bilateral rTMS can regulate a broader range of neural networks, and higher remission rates and better tolerability have been observed.51 Notably, a bilaterally-combined stimulation regimen (left iTBS + right sustained TBS) for LLD may further optimize efficacy,52 and its short-session characteristics significantly enhance treatment accessibility. In addition, an accelerated rTMS regimen (twice-daily high-frequency stimulation [20 Hz]) of the left DLPFC can significantly shorten the treatment cycle in older patients with refractory depression, with strong evidence of safety.53 Currently, rTMS application is still limited by the heterogeneity of individual responses and the lack of evidence supporting its long-term efficacy. By optimizing target localization and individualized therapeutic parameters while considering age-related brain changes, the precision and effectiveness of this intervention can be enhanced. With further research, rTMS is expected to become a more universal non-pharmacological alternative for LLD treatment.
Transcranial Direct Current Stimulation
tDCS is a safe, noninvasive neuromodulation technique that modulates cortical neuronal excitability and synaptic plasticity through low-intensity direct current (0.5–2 mA).54 tDCS can induce neuroplasticity and ultimately trigger structural changes in brain gray matter by functionally regulating the DLPFC and its network.55 The effects were comparable to those of antidepressant medication and rTMS.56 In most studies, the left DLPFC was stimulated. However, a study reported that in patients with first-episode unmedicated major depression, stimulation targeting the frontal cortex and both papillae significantly improved symptoms.57 In addition, high-definition tDCS (HD-tDCS) precisely focuses the current on the target brain area by adjusting the electrode layout, which greatly improves spatial resolution. HD-tDCS can significantly alleviate depression and effectively improve cognitive function in patients with LLD.58 Notably, a remotely-monitored home-based tDCS program has been shown to be effective and well-tolerated in patients with major depression after a 10-week intervention.59 The continued development of home-based portable tDCS devices is expected to provide a new pathway for long-term maintenance therapy with greater accessibility for LLD treatment. The specific mechanisms by which tDCS induces neuroplasticity in the aging brain remain inadequately studied, and large-scale RCTs confirming its long-term efficacy and value in relapse prevention are lacking. Future advancements should focus on parameter optimization, mechanism elucidation, and integration into multimodal treatment frameworks.
Vagus Nerve Stimulation
VNS is a neuromodulation technique that utilizes an implanted device to deliver electrical pulses to stimulate the vagus nerve. VNS activates vagal afferent fibers through electrical impulses, transmits signals to the nucleus tractus solitarius, and subsequently affects the amygdala, prefrontal cortex, and other brain areas related to emotion regulation, achieving antidepressant and neuromodulatory effects.60 An observational study of an older subgroup confirmed that the long-term efficacy of the adjunct VNS group was significantly better than that of the conventional treatment group, with a significantly higher 5-year cumulative remission (67.6% vs 40.9%) and first remission (43.3% vs 25.7%) rates.61 Transcutaneous auricular VNS, a non-invasive alternative, can prevent the invasive risk and high cost of VNS by modifying the topology of brain networks, which can effectively alleviate the symptoms of depression. It is easy to operate and is more suitable for the elderly.62 Currently, studies on VNS in LLD are insufficient, and the sample size is limited. In the future, expanding the scale of clinical trials, exploring the optimal stimulation target and dosage parameters of VNS treatment, providing more effective individualized targeting means for patients, and continuously optimizing the treatment protocol are needed.
Exercise Therapy
Exercise therapy is a non-pharmacological therapy that uses regular physical activity as a core intervention method, combining safety, effectiveness, and cost-effectiveness. Physical activity and exercise are potential therapeutic interventions for depression and are incorporated into guidelines as adjunctive treatment for mild-to-moderate depression.63 Exercise stimulates endorphin release and promotes neurotransmitter secretion, such as serotonin and dopamine secretion, thereby directly improving mood. Furthermore, exercise induces irisin secretion via the muscular PGC-1α/FNDC5 pathway. The induced irisin enters the brain via circulation, thereby enhancing the expression of brain-derived neurotrophic factor (BDNF) in the hippocampus and promoting neural plasticity.64 Simultaneously, exercise can reverse the atrophy of brain regions associated with depression such as the hippocampus, prefrontal cortex, and anterior cingulate cortex, contributing to symptom improvement.65 Clinical research has confirmed that implementing structured exercise interventions in older adults with significant depressive symptoms significantly reduces depression severity.66
The National Institute for Health and Clinical Excellence recommends incorporating group exercise, especially aerobic exercise, into depression treatment, and they recommend structured and supervised moderate-intensity exercise more than once a week for 10 weeks.67 Aerobic exercise involves sustained, rhythmic activity that engages large muscle groups, during which the body consumes oxygen to generate energy. Previous meta-analyses have robustly confirmed its efficacy in treating LLD.68 Resistance training interventions also hold substantial therapeutic value in LLD, with core objectives centered on augmenting muscular strength, endurance, and power. Meta-analytic evidence has confirmed that resistance training significantly reduces depressive symptom severity and improves self-perception and quality of life among affected individuals.69 Notably, resistance training combined with aerobic exercise is an effective strategy for alleviating depression-related symptoms and is particularly effective in middle-aged and older patients with moderate depression.70
Mind-body exercise can improve quality of life by increasing perceived social support and psychological resilience in older adults.71 A meta-analysis showed that mind-body exercise showed the greatest improvement in depressive symptoms, followed by aerobic and resistance exercise.68 Various forms of mind-body exercise are applicable to the older population, with Tai Chi and Qigong showing the most significant benefits in terms of improvement in general health indicators.72 A review suggested that Tai Chi may be superior to non-orthogonal exercise in alleviating anxiety and depression and improving overall mental health73 and can be practiced safely by those with cardiovascular disease or risk factors.74 Given that physiological changes due to aging generally reduce motor skills and movement precision in older adults, affecting the safety and effectiveness of their fitness activities, artificial intelligence (AI) interventions are practical. Studies have shown that AI precision intervention by wearing a smart armband equipped with an inertial measurement unit (IMU) can effectively enhance the understanding and execution precision of complex taijiquan movements and significantly improve balance in older adults.75 The key to this technology lies in its adoption of the temporal convolutional neural network, an emerging neural network architecture capable of processing IMU data in near real-time. This capability enables the system to concurrently analyze movement standardization during practice, establishing the technical foundation for instant corrective feedback and guidance, thereby endowing the training regimen with a “digital coaching” function.76 Existing studies have mostly focused on the overall efficacy of exercises, such as mind-body exercise, and lack in-depth exploration of their neural mechanisms that affect LLD (specificity, specific mechanisms, optimal solutions, and universality are unclear). Future research should involve designing longitudinal studies, harmonizing data collection, and integrating insights from traditional methodologies with the strength of data-driven techniques.
Bright Light Therapy
BLT is a physical intervention that treats mood disorders by exposing individuals to light of a specific intensity. BLT is an effective option for seasonal major depression; its prevention of relapse requires a combination of antidepressant medications and other strategies.63 In patients with LLD, BLT has been shown to improve depressive symptoms, as well as improve sleep efficiency through supraoptic nucleus stimulation to correct circadian rhythm disturbances and modulate the hypothalamic-pituitary axis.77 As a convenient and accessible treatment modality, meta-analyses have affirmed its positive effects in alleviating depressive symptoms, and it can enhance the effects of psychotherapy and pharmacotherapy.78 In addition, BLT, an adjunct treatment to antidepressants, can significantly enhance the remission and response rates of non-seasonal depression and accelerate the process of treatment response.79 BLT has a favorable safety profile and accessibility for patients with LLD who are resistant or intolerant to conventional antidepressant therapies. However, ocular diseases, such as macular degeneration, are common in older people,80 and BLT is contraindicated in people at high risk of retinopathy.
Critical gaps persist regarding the neurobiological mechanisms of BLT in the aging brain and the establishment of standardized, effective treatment protocols for LLD. Current evidence supports its role in alleviating depressive symptoms and improving sleep efficiency. Future studies are needed to clarify the optimal treatment protocols, long-term efficacy, and underlying mechanisms of BLT in LLD management.
Dietary and Nutritional Interventions
Dietary and nutritional interventions are non-pharmacological strategies that improve depressive symptoms by adjusting overall dietary patterns or supplementing specific nutrients. Their core principle involves harnessing the neuroprotective and anti-inflammatory properties of food to support LLD management. Studies have shown that diets high in glycemic index or saturated fat increase depressive symptoms and inflammatory markers in healthy populations.81 In contrast, the Mediterranean Diet has been shown to increase plasma BDNF levels, which can help alleviate depressive symptoms.82 The Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet, which integrates the core concepts of the Mediterranean and antihypertensive diets, is an exemplary balanced pattern. The MIND diet, which is rich in antioxidants, Omega-3 fatty acids, and polyphenols, enhances BDNF levels and cognitive performance, thereby supporting neuroprotection and mood regulation.83 The health value of this model has been validated in the older Chinese population, following the Chinese version of the MIND diet, and it significantly reduced the risk of depression and anxiety symptoms.84 In addition, those who adhered to a high-scoring DASH or MIND diet over a long period had a lower incidence of depressive symptoms.85 The core characteristics of these diets are summarized and compared in Table 3.
 |
Table 3 Nutritional Interventions for Late-Life Depression |
Omega-3 Polyunsaturated Fatty Acids
Omega-3 polyunsaturated fatty acids (n-3 PUFA), a core component of the MIND diet, have neuroprotective and mood-regulatory functions attributed to eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). n-3 PUFA have been recommended as a comprehensive treatment for major depressive disorder,86 and their antidepressant mechanisms may involve the modulation of neuroinflammation, including competitive replacement of pro-inflammatory fatty acids, inhibition of NLRP3 inflammatory vesicles, and facilitation of anti-inflammatory mediator production.87 Clinical evidence has suggested that EPA-based preparations have significant clinical benefits compared to that of a placebo in patients with depression. However, DHA-based preparations did not show equivalent effects, and further RCTs using EPA-based omega-3 highly unsaturated fatty acids are recommended in patients with established or sufficient clinical severity and duration of depression.88 Despite the existence of supportive studies in dietary supplementation in LLD populations,89 current evidence is still insufficient to recommend their systematic clinical use.
Vitamin D
Vitamin D, a fat-soluble vitamin obtained mainly through limited dietary intake and sunlight exposure, plays a key role in physiological processes, such as the maintenance of calcium homeostasis, bone health, and immune regulation.90 Vitamin D targets key pathways in depression pathogenesis through multiple mechanisms: regulating monoamine neurotransmitter synthesis, inhibiting neuroinflammation, promoting BDNF-mediated neuroplasticity, and stabilizing hypothalamic-pituitary-adrenal axis function,91 with particular neuroprotective value. Previous studies have confirmed that specific nutrients—vitamin B-complex, by regulating homocysteine metabolism, and vitamin C via scavenging free radicals—jointly constitute a mood-regulatory network together with vitamin D.92 A large body of research evidence has suggested that low vitamin D levels are associated with an increased risk of depression. Previous meta-analyses have further indicated that vitamin D supplementation in individuals who are deficient demonstrates antidepressant efficacy comparable to conventional antidepressant medications, whereas it provides no significant benefit to those with normal vitamin D levels.93 Notably, vitamin D and omega-3 fatty acids are synergistic in inhibiting neuroinflammation and regulating mood, and the combination of the two is expected to be an adjunctive therapeutic strategy for depression.94 Current evidence relies on observational studies, lacking large-scale RCT validation. Future research must verify efficacy through robust trials and establish precision strategies, integrating deficiency status and nutrigenomics to realize vitamin D’s potential in comprehensive LLD treatment.
Probiotic Metabolites
Probiotic metabolites (short-chain fatty acids [SCFAs] and γ-aminobutyric acid) transmit signals to the nucleus tractus solitarius by activating receptors on the afferent fibers of the vagus nerve, thereby inhibiting the overactivation of the hypothalamic-pituitary-adrenal axis and reducing the overproduction of cortisol and its disruption of neurotransmitter homeostasis.95,96 SCFAs elevate the intestinal tryptophan utilization rate and promote 5-HT synthesis;97 their metabolic derivatives also down-regulate pro-inflammatory cytokine expression and inhibit the progression of mood disorders through anti-inflammatory effects.98 Therefore, intervention strategies targeting the gut microbiota (eg, probiotic supplementation with dietary modification) are valuable in alleviating depressive moods in LLD. In the future, precise nutritional intervention programs including specific probiotic or prebiotic combinations and anti-inflammatory nutrient packages can be designed based on individualized metabolomic profiling of gut microbiota to achieve the synergistic efficacy of neuroinflammation modulation and reconstruction of brain metabolic homeostasis.
Social Support and Community Interventions
Social support and community interventions are non-pharmacological strategies that alleviate social isolation and improve mental health through the building of social networks, provision of community resources, and organization of group activities. Social isolation, a cumulative risk factor for LLD, has negative effects that increase over time. Studies have further demonstrated that social network structure and functioning are strongly correlated with depressive symptoms in older adults, and that subjective loneliness can be reduced by promoting social network integration and community involvement, thereby preventing the development of depressive mood.99 Being socially active significantly inhibits the expression of pro-inflammatory factors, such as interleukin-6, and mediates anti-inflammatory, anti-stress, and immune homeostatic effects by activating the paraventricular nucleus of the hypothalamus oxytocinergic neuron release pathway.100 LLD treatment requires the integration of high-quality social contact as a non-pharmacological intervention and targeted improvement of social determinants at an early stage to enhance efficacy.101 As indicated previously, the landscape of social support and community interventions for LLD is diverse. Their key attributes are succinctly summarized in Table 4 to facilitate comparison.
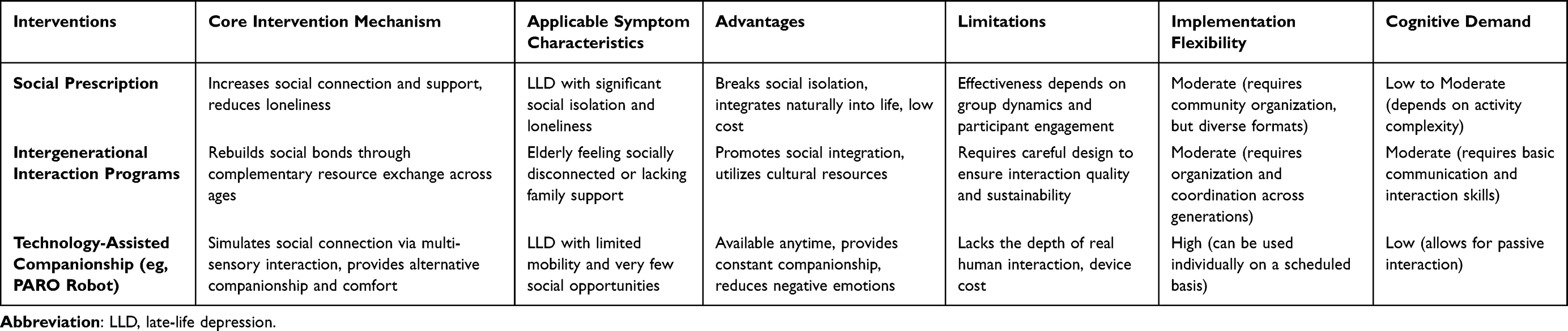 |
Table 4 Community and Social Interventions for Late-Life Depression |
Social prescription activities, such as soccer, gardening, and art are accessible with associated low cost. These interventions do not only provide direct health benefits but also effectively promote the establishment of social connections among emotionally-disturbed older adults by enhancing social support and reducing loneliness,102,103 which has been shown to be positively effective in multiple scenarios. In the future, it will be necessary to combine precision medicine and community ecology to construct a scalable, low-cost, and high-compliance intervention model.
Intergenerational interaction programs rebuild social bonds through age-complementary resource exchange to enhance self-efficacy and social motivation. Intergenerational relationships, serving as social bonds across age groups, encompass not only intra-family interactions and support but also non-family intergenerational interactions such as community mutual aid and communication across ages.104 For example, in the Chinese culture of filial piety, a negative correlation exists between intergenerational relationships and depressive symptoms, which can alleviate depression by improving older adults’ self-assessed health and well-being.105 The sustainability of intergenerational relationships in LLD should be enhanced through standardized designs in the future. In addition, the use of some new technologies has been welcomed by older adults. For example, the long-term care companion robot PARO (Social Seal Robot),106 which simulates vital body responses through multi-sensor interactions and provides alternative social connections for older adults, has a significant positive impact on reducing depression and loneliness in older adults.107,108 Current evidence has suggested that technological-based interventions, such as PARO, can alleviate negative emotions, including feelings of emotional numbness, social disconnection, and worthlessness by alleviating LLD. Research has demonstrated significant synergistic effects between intergenerational support, community services, and smart health devices, indicating the substantial value of integrating a “family-community-technology” model in alleviating depressive symptoms in older adults.109 Current evidence on social and community interventions for LLD remains constrained by fragmented implementation and inadequate cultural adaptation, necessitating the future development of more ecologically-valid models that integrate digital tools.
Multimodal Integration
Combining non-pharmacological interventions is a therapeutic strategy that employs two or more modalities to enhance overall efficacy through multi-target synergistic effects. Considering the heterogeneous pathological mechanisms of LLD, the multimodal intervention strategy can achieve synergistic effects by simultaneously targeting neuroplasticity remodeling, metabolism regulation during inflammation, and social neural circuit repair. In neuroplasticity, the combination of physical therapies, such as neuromodulation and psychotherapy, can simultaneously enhance prefrontal neuroplasticity, as well as promote hippocampal BDNF expression and synaptic regeneration, accelerating cognitive pattern consolidation. Moreover, clinical studies have demonstrated that light therapy combined with rTMS is significantly more effective than rTMS alone in refractory LLD.110 The combination of psychological and exercise interventions has also demonstrated the advantages of CBT and exercise interventions in reducing suicidal ideation and improving daily functioning compared with that observed using CBT alone.111
Regarding metabolism during inflammation, inhibition of NLRP3 inflammatory vesicle-mediated neuroinflammation using probiotics and anti-inflammatory diets and activation of the iris pathway through individualized exercise effectively blocks the primary inflammatory cascade. This integrated dietary and exercise intervention showed prominent protective effects in Chinese older adults, implying that a combination of various diets and regular exercise resulted in psychological benefits that exceed those of a single intervention.112
Multimodal interventions are also effective for psychological aspects. The integration of CBT and social skills training significantly improved the self-esteem and quality of life of older adults in nursing homes.113 Moreover, the efficacy of an integrated program that combined psychotherapy, positive thinking training, and family education was significantly better than that of a single treatment.114 Evidence has indicated that integrating comprehensive interventions, comprising physical, psychological, social, and lifestyle dimensions, into routine care plans for LLD may not only alleviate individual clinical symptoms and enhance quality of life but also contribute to the optimization of the healthcare system.115 These findings collectively highlight the need for future comprehensive treatments for LLD to transition from single-target interventions to an integrated model aimed at restoring brain homeostasis and overall bodily health.
Current relevant studies have several limitations. First, sample sizes are generally small, and long-term follow-up data are relatively scarce. Second, for studies on combined non-pharmacological interventions targeting the older adult population, the empirical evidence accumulated so far remains insufficient. Furthermore, existing studies have not yet provided clear answers regarding the optimal combination of different intervention models, appropriate treatment courses, and the specific neurobiological mechanisms underlying the synergistic effects of these models. Therefore, future studies should rely on large-scale, rigorously-designed RCTs to further verify and optimize personalized multimodal intervention protocols.
A major challenge in managing multimodal non-pharmacological interventions for LLD is the effective integration of scattered therapies into routine medical practice. Consequently, the Prevention of Suicide in Primary Care Elderly: Collaborative Trial (PROSPECT) model provides an excellent operational framework for the systematic coordination and implementation of non-pharmacological interventions. Through clear role division for the interdisciplinary team, this model ensures the feasibility and continuity of non-pharmacological interventions: primary care physicians are responsible for initial identification and referral of such patients; psychiatrists focus on formulating and reviewing personalized non-pharmacological plans; and care managers, as the core of execution, control patient education, guide treatment, coordinate resources, and provide continuous monitoring.116 Studies have shown that this model, which focuses on collaboration and emphasizes integrated care, can significantly improve the management outcomes of LLD.117 Health administration departments should prioritize the adoption and funding of evidence-based collaborative care models such as the PROSPECT, promote their popularity by establishing standardized procedures and compensation mechanisms, and encourage clinicians to actively participate in flexibly selecting intervention measures based on patients’ specific conditions—for example, providing a simplified problem-solving therapy for those with impaired executive function and introducing VR-based intervention programs for those with limited mobility.
Discussion
This article systematically integrates the latest evidence across multiple dimensions, including psychological, physical, nutritional, and social support interventions. It connects neurobiology with non-pharmacological interventions and explicitly proposes a core framework of “multimodal synergistic intervention”. Multimodal interventions involving combinations of non-pharmacological approaches may have unique advantages in the treatment of LLD. Existing evidence has indicated that strategies such as psychotherapy, physical therapy, nutritional interventions, and community support can alleviate LLD symptoms through specific mechanisms, such as regulating DMN function, enhancing neuroplasticity, reducing neuroinflammation, and repairing social neural circuits. However, due to LLD’s etiological heterogeneity and multidimensional pathophysiology, no single intervention can fully reverse the disease. Multimodal interventions effectively generate synergies, simultaneously acting on multiple pathophysiological links to potentially yield more significant and lasting clinical benefits, especially in patients with LLD.118 For example, neuromodulation may “reset” the brain into a learning-conducive neural environment, boosting the subsequent cognitive remodeling effects of psychotherapy.119 Similarly, combining anti-inflammatory diets with regular exercise may have additive or complementary effects in inhibiting systemic inflammation by acting on the gut microbiota-brain axis and muscle-brain axis, respectively.120 Notably, studies on multimodal interventions for LLD—exclusively non-pharmacological—remain scarce.121 However, most of these synergistic mechanisms are still hypothetical, with limited research among older adults.
Negative Outcomes and Risk Management of Non-Pharmacological Interventions
In psychotherapy, some approaches such as CBT and cognitive reading therapy require patients to have certain cognitive function and educational levels, potentially causing frustration in older adults with cognitive impairment or low education. RT risks reactivating traumatic memories, while poor therapeutic relationships may also have negative effects.35 Digital therapies, lacking real interpersonal interaction, have limited effect on alleviating loneliness.122
Neuromodulation techniques, as physical therapies, have side effects: ECT may cause memory impairment and anesthesia risks;123 rTMS often induces headaches and scalp discomfort;124 and the efficacy of tDCS remains uncertain. Exercise therapy poses injury risks to frail older adults, and patients often struggle with adherence due to insufficient motivation. BLT may cause eye discomfort and is contraindicated for certain groups.80
Nutritional interventions have slow and uncertain efficacy, may trigger gastrointestinal discomfort and drug interactions, and pose financial and adherence challenges during its long-term use. Social support and community interventions depend on activity quality for efficacy, while technology-assisted companionship may fail due to the digital divide.
Most importantly, integrated multimodal interventions may create an “intervention burden”. Simultaneous participation in multiple therapies can excessively drain older patients’ energy, time, and cognitive resources, leading to increased stress, reduced adherence, and even premature treatment discontinuation. Therefore, clinicians must carefully weigh these potential risks and optimize therapeutic benefits through individualized plans and tailored pacing.
Key Limitations in the Field
Despite the promising prospects, this field faces several important limitations. Methodologically, most cited RCTs are constrained by small sample sizes and short follow-up periods, limiting the reliable assessment of long-term efficacy and safety. As a narrative review, this article lacks the methodological rigor of a systematic review, potentially introducing selection and publication biases. Furthermore, the exclusive inclusion of English articles may omit significant findings from other cultural contexts.
Regarding implementation, the generalizability and accessibility of interventions present challenges. Many psychological interventions require relatively intact cognitive function, while digital therapies pose barriers in older adults with low technology adoption rates or in resource-limited settings. The sustainability of community interventions significantly depends on external resources and policy support, with a notable absence of mature, scalable business or public policy models.
Finally, significant gaps remain in mechanistic research and clinical translation. The understanding of how multimodal interventions produce synergistic effects at the cerebral, immune, and metabolic levels remains superficial, lacking robust evidence in the field of systems biology.
Future Research Directions and Practical Recommendations
To address these gaps, future research must conduct large-scale, long-term multicenter RCTs to establish high-level evidence for multimodal interventions. Studies should include cross-cultural comparisons to develop culturally-adapted protocols and integrate precision medicine approaches to identify treatment-guiding biomarkers. Technological developments must incorporate age-friendly designs to enhance usability and adherence. The ultimate goal is to create an integrated hospital-community-home care model, supported by innovative policies and funding, to translate these technological advancements into accessible, effective, and humane care for older adults with depression.
Conclusion
Non-pharmacological interventions have been emphasized in LLD treatment due to advantages, such as fewer side effects and higher patient compliance. The use of such interventions has shifted from monotherapy to comprehensive multidimensional interventions. To facilitate the translation of these interventions from evidence to practice, clinicians should define their roles within collaborative care models, such as the PROSPECT, to systematically integrate multimodal interventions. Concurrently, public health policy makers must establish a robust support framework by institutionalizing these collaborative structures and reforming payment systems. In the future, research in this field should advance along two critical pathways: first, for clinical practice, precision medicine, digital technologies, and community ecology should be integrated to establish an accessible and integrated personalized biopsychosocial care model and second, for research, multicenter, large-sample longitudinal, and cross-cultural comparative studies should be conducted to evaluate the long-term efficacy and feasibility of multimodal interventions, ultimately establishing an efficient, accessible, and humanized mental health care system for older adults with LLD.
Data Sharing Statement
No dataset was used for this study.
Author Contributions
Tianmei Xu: Writing – review & editing, Writing – original draft, Validation, Supervision, Methodology, Formal analysis, Conceptualization. Yanping Mao: Validation, Methodology. Ye Wang: Validation, Supervision. Yi Gong: Project administration, Methodology. Enyan Yu: Investigation, Formal analysis, Conceptualization. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that financial support was received for the research and/or publication of this article. This work was supported by the Science and Technology Plan Project of Zhejiang Province (Project number: 2021C03106).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sekhon S, Patel J, Sapra A. Late-Life Depression. Treasure Island, FL: StatPearls Publishing; 2025.
2. Hu T, Zhao X, Wu M, et al. Prevalence of depression in older adults: a systematic review and meta-analysis. Psychiatry Res. 2022;311:114511. doi:10.1016/j.psychres.2022.114511
3. Sun Q, Wei Y, Xie H, et al. The global, regional, and national late-life depression burden and trends from 1990 to 2021: a systematic analysis for the global burden of disease study 2021. Arch Gerontol Geriatr. 2025;131:105758. doi:10.1016/j.archger.2025.105758
4. Paun O. Older adults and late-life depression. J Psychosoc Nurs Ment Health Serv. 2023;61(4):8–9. doi:10.3928/02793695-20230307-02
5. Kok RM. Reynolds CF, III. Management of depression in older adults: a review. JAMA. 2017;317(20):2114–2122. doi:10.1001/jama.2017.5706
6. Blazer DG, Hybels CF, Fillenbaum GG, Pieper CF. Predictors of antidepressant use among older adults: have they changed over time? Am J Psychiatry. 2005;162(4):705–710. doi:10.1176/appi.ajp.162.4.705
7. Reynolds CF III, Butters MA, Lopez O, et al. Maintenance treatment of depression in old age: a randomized, double-blind, placebo-controlled evaluation of the efficacy and safety of donepezil combined with antidepressant pharmacotherapy. Arch Gen Psychiatry. 2011;68(1):51–60. doi:10.1001/archgenpsychiatry.2010.184
8. Alexopoulos GS, Kiosses DN, Klimstra S, Kalayam B, Bruce ML. Clinical presentation of the “depression-executive dysfunction syndrome” of late life. Am J Geriatr Psychiatry. 2002;10(1):98–106. doi:10.1097/00019442-200201000-00012
9. Wang SM, Kim NY, Um YH, et al. Default mode network dissociation linking cerebral beta amyloid retention and depression in cognitively normal older adults. Neuropsychopharmacology. 2021;46(12):2180–2187. doi:10.1038/s41386-021-01072-9
10. Chen Y-J, Li -X-X, Pan B, et al. Non-pharmacological interventions for older adults with depressive symptoms: a network meta-analysis of 35 randomized controlled trials. Aging & Mental Health. 2021;25(5):773–786. doi:10.1080/13607863.2019.1704219
11. Malhi GS, Bell E, Bassett D, et al. An evidence-based perspective on the 2020 Royal Australian and New Zealand College of Psychiatrists Clinical Practice Guidelines. Australas Psychiatry. 2022;30(4):447–451. doi:10.1177/10398562221100703
12. Cuijpers P, Van Straten A, Smit F. Psychological treatment of late-life depression: a meta-analysis of randomized controlled trials. Int J Geriatr Psychiatry. 2006;21(12):1139–1149. doi:10.1002/gps.1620
13. Simon GE, Moise N, Mohr DC. Management of depression in adults: a review. JAMA. 2024;332(2):141–152. doi:10.1001/jama.2024.5756
14. Wilkins VM, Kiosses D, Ravdin LD. Late-life depression with comorbid cognitive impairment and disability: nonpharmacological interventions. Clin Interv Aging. 2010;5:323–331. doi:10.2147/CIA.S9088
15. Beck AT, Haigh EAP. Advances in cognitive theory and therapy: the generic cognitive model. Annu Rev Clin Psychol. 2014;10:1–24. doi:10.1146/annurev-clinpsy-032813-153734
16. König P, Zwiky E, Küttner A, Uhlig M, Redlich R. Brain functional effects of cognitive behavioral therapy for depression: a systematic review of task-based fMRI studies. J Affect Disord. 2025;368:872–887. doi:10.1016/j.jad.2024.09.084
17. Gould RL, Coulson MC, Howard RJ. Cognitive behavioral therapy for depression in older people: a meta-analysis and meta-regression of randomized controlled trials. J Am Geriatr Soc. 2012;60(10):1817–1830. doi:10.1111/j.1532-5415.2012.04166
18. Gallagher-Thompson D, Steffen A, Thompson LW. Handbook of Behavioral and Cognitive Therapies with Older Adults. Springer; 2008. https://link.springer.com/book/10.1007/978-0-387-72007-4.
19. Skosireva A, Gobessi L, Eskes G, Cassidy KL. Effectiveness of enhanced group cognitive behaviour therapy for older adults (CBT-OA) with depression and anxiety: a replication study. Int Psychogeriatr. 2025;37(2):100013. doi:10.1016/j.inpsyc.2024.100013
20. Qiu Y, Wu M, Liu J, et al. Effectiveness of information technology-based cognitive behavioral therapy on depression and anxiety symptoms among older adults: systematic review and meta-analysis. Gen Hosp Psychiatry. 2025;93:9–19. doi:10.1016/j.genhosppsych.2024.12.022
21. Pabst A, Löbner M, Stein J, et al. Internet-based cognitive behavior therapy only for the young? A secondary analysis of a randomized controlled trial of depression treatment. Front Psychiatry. 2020;11:735. doi:10.3389/fpsyt.2020.00735
22. Lee M, Jang S, Shin HK, et al. Virtual reality-based cognitive behavior therapy for major depressive disorder: an alternative to pharmacotherapy for reducing suicidality. Yonsei Med J. 2025;66(1):25–36. doi:10.3349/ymj.2024.0002
23. Torres-Platas SG, Escobar S, Belliveau C, et al. Mindfulness-based cognitive therapy intervention for the treatment of late-life depression and anxiety symptoms in primary care: a randomized controlled trial. Psychother Psychosom. 2019;88(4):254–256. doi:10.1159/000501214
24. Prakash RS, De Leon AA, Patterson B, Schirda BL, Janssen AL. Mindfulness and the aging brain: a proposed paradigm shift. Front Aging Neurosci. 2014;6:120. doi:10.3389/fnagi.2014.00120
25. Wang YH, Wang YL, Leung DKY, et al. Effectiveness of an age-modified mindfulness-based cognitive therapy (MBCT) in improving mental health in older people with depressive symptoms: a non-randomised controlled trial. BMC Complement Med Ther. 2025;25(1):81. doi:10.1186/s12906-025-04781-6
26. Galluzzi S, Lanfredi M, Moretti DV, et al. Cognitive, psychological, and physiological effects of a web-based mindfulness intervention in older adults during the COVID-19 pandemic: an open study. BMC Geriatr. 2024;24(1):151. doi:10.1186/s12877-024-04766-z
27. Cuijpers P, De Wit L, Kleiboer A, Karyotaki E, Ebert DD. Problem-solving therapy for adult depression: an updated meta-analysis. Eur Psychiatry. 2018;48:27–37. doi:10.1016/j.eurpsy.2017.11.006
28. Hadidi NN, Jappe L, Cullen K, Savik K. Impact of problem solving therapy on brain networks associated with depressive symptoms in poststroke older adults. In: Jensen W, Andersen O, Akay M, editors. Replace, Repair, Restore, Relieve – Bridging Clinical and Engineering Solutions in Neurorehabilitation. Biosystems & Biorobotics, Vol 7. Cham: Springer, Cham; 2014. doi:10.1007/978-3-319-08072-7_62.
29. Huang C, Fang Y, Yan F, et al. Efficacy of problem-solving therapy in treating late-life depression with potential cognitive impairment: a systematic review and meta-analysis. BMJ Open. 2024;14(10):e084130. doi:10.1136/bmjopen-2024-084130
30. Areán PA, Raue P, Mackin RS, Kanellopoulos D, McCulloch C, Alexopoulos GS. Problem-solving therapy and supportive therapy in older adults with major depression and executive dysfunction. Am J Psychiatry. 2010;167(11):1391–1398. doi:10.1176/appi.ajp.2010.09091327
31. Wu X, Li J, Zhang C, et al. The effects of modified problem-solving therapy on depression, coping, and self-efficacy in elderly nursing home residents. Front Psychol. 2022;13:1030104. doi:10.3389/fpsyg.2022.1030104
32. Zhang M, Yang Z, Zhong J, et al. Thalamocortical mechanisms for nostalgia-induced analgesia. J Neurosci. 2022;42(14):2963–2972. doi:10.1523/JNEUROSCI.2123-21.2022
33. Liu Z, Yang F, Lou Y, Zhou W, Tong F. The effectiveness of reminiscence therapy on alleviating depressive symptoms in older adults: a systematic review. Front Psychol. 2021;12:709853. doi:10.3389/fpsyg.2021.709853
34. Ng WHD, Ang WHD, Fukahori H, et al. Virtual reality-based reminiscence therapy for older adults to improve psychological well-being and cognition: a systematic review. J Clin Nurs. 2024. doi:10.1111/jocn.17375
35. Woods B, O’Philbin L, Farrell EM, Spector AE, Orrell M. Reminiscence therapy for dementia. Cochrane Database Syst Rev. 2018;3(3):CD001120. doi:10.1002/14651858.CD001120.pub3
36. Monroy-Fraustro D, Maldonado-Castellanos I, Aboites-Molina M, et al. Bibliotherapy as a non-pharmaceutical intervention to enhance mental health in response to the COVID-19 pandemic: a mixed-methods systematic review and bioethical meta-analysis. Front Public Health. 2021;9:629872. doi:10.3389/fpubh.2021.629872
37. Gualano MR, Bert F, Martorana M, et al. The long-term effects of bibliotherapy in depression treatment: systematic review of randomized clinical trials. Clin Psychol Rev. 2017;58:49–58. doi:10.1016/j.cpr.2017.09.006
38. Floyd M, Scogin F, McKendree-Smith NL, Floyd DL, Rokke PD. Cognitive therapy for depression: a comparison of individual psychotherapy and bibliotherapy for depressed older adults. Behav Modif. 2004;28(2):297–318. doi:10.1177/0145445503259284
39. Van Rooij SJH, Riva-Posse P, McDonald WM. The efficacy and safety of neuromodulation treatments in late-life depression. Curr Treat Options Psychiatry. 2020;7(3):337–348. doi:10.1007/s40501-020-00216-w
40. Ruiz AC, Haseeb A, Baumgartner W, Leung E, Scaini G, Quevedo J. New insights into the mechanisms of electroconvulsive therapy in treatment-resistant depression. Front Psychiatry. 2025;16:1614076. doi:10.3389/fpsyt.2025.1614076 Erratum in: Front Psychiatry. 2025;16:1700480. doi: 10.3389/fpsyt.2025.1700480.
41. Rhebergen D, Huisman A, Bouckaert F, et al. Older age is associated with rapid remission of depression after electroconvulsive therapy: a latent class growth analysis. Am J Geriatr Psychiatry. 2015;23(3):274–282. doi:10.1016/j.jagp.2014.05.002
42. Gálvez V, Ho KA, Alonzo A, Martin D, George D, Loo CK. Neuromodulation therapies for geriatric depression. Curr Psychiatry Rep. 2015;17(7):59. doi:10.1007/s11920-015-0592-y
43. Kellner CH, Husain MM, Knapp RG, et al. A novel strategy for continuation ECT in geriatric depression: Phase 2 of the PRIDE study. Am J Psychiatry. 2016;173(11):1110–1118. doi:10.1176/appi.ajp.2016.16010118
44. UK ECT Review Group Review Group. Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. Lancet. 2003;361(9360):799–808. doi:10.1016/S0140-6736(03)12705-5.
45. Jiang X, Xie Q, Liu LZ, Zhong BL, Si L, Fan F. Efficacy and safety of modified electroconvulsive therapy for the refractory depression in older patients. Asia Pac Psychiatry. 2020;12(4):e12411. doi:10.1111/appy.12411
46. Yin BW, Yang L. Comparative efficacy of augmenting escitalopram with modified electroconvulsive therapy or high-frequency repetitive transcranial magnetic stimulation on depressive symptoms, quality of life, and cognitive function in treatment-resistant depression. Tohoku J Exp Med. 2024;262(3):191–199. doi:10.1620/tjem.2023.J103
47. Downar J, Siddiqi SH, Mitra A, et al. Mechanisms of action of TMS in the treatment of depression. Curr Top Behav Neurosci. 2024;66:233–277. doi:10.1007/7854_2024_483
48. Göke K, Downar J, Vila-Rodriguez F, et al. The effects of rTMS on self-reported quality of life in younger and older adults with major depressive disorder. Psychol Med. 2025;55:e303. doi:10.1017/S0033291725102079
49. Băcilă CI, Cornea M, Lomnasan A, et al. Efficacy and safety of transcranial magnetic stimulation for treating late-life depression: a scoping review. J Clin Med. 2025;14(10):3609. doi:10.3390/jcm14103609
50. Cristancho P, Arora J, Nishino T, et al. A pilot randomized sham controlled trial of bilateral iTBS for depression and executive function in older adults. Int J Geriatr Psychiatry. 2023;38(1):e5851. doi:10.1002/gps.5851
51. Trevizol AP, Goldberger KW, Mulsant BH, et al. Unilateral and bilateral repetitive transcranial magnetic stimulation for treatment-resistant late-life depression. Int J Geriatr Psychiatry. 2019;34(6):822–827. doi:10.1002/gps.5091
52. Blumberger DM, Mulsant BH, Thorpe KE, et al. Effectiveness of standard sequential bilateral repetitive transcranial magnetic stimulation vs bilateral theta burst stimulation in older adults with depression: the FOUR-D randomized noninferiority clinical trial. JAMA Psychiatry. 2022;79(11):1065–1073. doi:10.1001/jamapsychiatry.2022.2862
53. Zheng W, Zhang XY, Xu R, et al. Adjunctive accelerated repetitive transcranial magnetic stimulation for older patients with depression: a systematic review. Front Aging Neurosci. 2022;14:1036676. doi:10.3389/fnagi.2022.1036676
54. Woodham R, Rimmer RM, Mutz J, Fu CHY. Is tDCS a potential first line treatment for major depression? Int Rev Psychiatry. 2021;33(3):250–265. doi:10.1080/09540261.2021.1879030
55. Jog MA, Anderson C, Kubicki A, et al. Transcranial direct current stimulation (tDCS) in depression induces structural plasticity. Sci Rep. 2023;13:2841. doi: 10.1038/s41598-023-29792-6.
56. Brunoni AR, Moffa AH, Fregni F, et al. Transcranial direct current stimulation for acute major depressive episodes: meta-analysis of individual patient data. Br J Psychiatry. 2016;208(6):522–531. doi:10.1192/bjp.bp.115.164715
57. Wang H, Wang K, Xue Q, et al. Transcranial alternating current stimulation for treating depression: a randomized controlled trial. Brain. 2022;145(1):83–91. doi:10.1093/brain/awab252
58. Ngan STJ, Chan LK, Chan WC, et al. High-definition transcranial direct current stimulation (HD-tDCS) as augmentation therapy in late-life depression (LLD) with suboptimal response to treatment-a study protocol for a double-blinded randomized sham-controlled trial. Trials. 2022;23(1):914. doi:10.1186/s13063-022-06855-z
59. Woodham RD, Selvaraj S, Lajmi N, et al. Home-based transcranial direct current stimulation treatment for major depressive disorder: a fully remote phase 2 randomized sham-controlled trial. Nat Med. 2025;31(1):87–95. doi:10.1038/s41591-024-03305-y
60. Fang YT, Lin YT, Tseng WL, et al. Neuroimmunomodulation of vagus nerve stimulation and the therapeutic implications. Front Aging Neurosci. 2023;15:1173987. doi:10.3389/fnagi.2023.1173987
61. Aaronson ST, Sears P, Ruvuna F, et al. A 5-year observational study of patients with treatment-resistant depression treated with vagus nerve stimulation or treatment as usual: comparison of response, remission, and suicidality. Am J Psychiatry. 2017;174(7):640–648. doi:10.1176/appi.ajp.2017.16010034
62. Guo ZP, Liao D, Chen L, et al. Transcutaneous auricular vagus nerve stimulation modulating the brain topological architecture of functional network in major depressive disorder: an fMRI study. Brain Sci. 2024;14(9):945. doi:10.3390/brainsci14090945
63. Cleare A, Pariante CM, Young AH, et al. Evidence-based guidelines for treating depressive disorders with antidepressants: a revision of the 2008 British Association for Psychopharmacology guidelines. J Psychopharmacol. 2015;29(5):459–525. doi:10.1177/0269881115581093
64. Wrann CD, White JP, Salogiannnis J, et al. Exercise induces hippocampal BDNF through a PGC-1α/FNDC5 pathway. Cell Metab. 2013;18(5):649–659. doi:10.1016/j.cmet.2013.09.008
65. Gujral S, Aizenstein H, Reynolds CF, Butters MA, Erickson KI. Exercise effects on depression: possible neural mechanisms. Gen Hosp Psychiatry. 2017;49:2–10. doi:10.1016/j.genhosppsych.2017.04.012
66. Bridle C, Spanjers K, Patel S, Atherton NM, Lamb SE. Effect of exercise on depression severity in older people: systematic review and meta-analysis of randomised controlled trials. Br J Psychiatry. 2012;201(3):180–185. doi:10.1192/bjp.bp.111.095174
67. National Institute for Health and Care Excellence. Guidelines-Depression in Adults: Treatment and Management. London: National Institute for Health and Care Excellence (NICE); 2022.
68. Miller KJ, Gonçalves-Bradley DC, Areerob P, Hennessy D, Mesagno C, Grace F. Comparative effectiveness of three exercise types to treat clinical depression in older adults: a systematic review and network meta-analysis of randomised controlled trials. Ageing Res Rev. 2020;58:100999. doi:10.1016/j.arr.2019.100999
69. Gordon BR, McDowell CP, Hallgren M, Meyer JD, Lyons M, Herring MP. Association of efficacy of resistance exercise training with depressive symptoms: meta-analysis and meta-regression analysis of randomized clinical trials. JAMA Psychiatry. 2018;75(6):566–576. doi:10.1001/jamapsychiatry.2018.0572
70. Wang H, Liu Q, Pan Y. Impact of combiner aerobic and resistance training on depression: a systematic review and meta-analysis of randomized controlled trials. BMC Sports Sci Med Rehabil. 2025;17(1):10. doi:10.1186/s13102-025-01058-w
71. Yang Q, Zhang Y, Li S. The impact of mind-body exercise on the quality of life in older adults: the chain mediation effect of perceived social support and psychological resilience. Front Public Health. 2024;(12):1446295. doi:10.3389/fpubh.2024.1446295
72. Alowaydhah S, Weerasekara I, Walmsley S, Marquez J. The effects of various types of physical exercise on health outcomes in older adults with depression: a systematic review and meta-analysis of controlled trials. Depress Anxiety. 2024;2024:9363464. doi:10.1155/2024/9363464
73. Yin J, Yue C, Song Z, Sun X, Wen X. The comparative effects of Tai chi versus non-mindful exercise on measures of anxiety, depression and general mental health: a systematic review and meta-analysis. J Affect Disord. 2023;337:202–214. doi:10.1016/j.jad.2023.05.037
74. Yang G, Li W, Klupp N, et al. Does tai chi improve psychological well-being and quality of life in patients with cardiovascular disease and/or cardiovascular risk factors? A systematic review. BMC Complement Med Ther. 2022;22(1):3. doi:10.1186/s12906-021-03482-0
75. Zhang Y, Li H, Huang R. The effect of Tai Chi (Bafa Wubu) training and artificial intelligence-based movement-precision feedback on the mental and physical outcomes of elderly. Sensors. 2024;24(19):6485. doi:10.3390/s24196485
76. Li X, Zou L, Li H. Tai Chi movement recognition and precise intervention for the elderly based on inertial measurement units and temporal convolutional neural networks. Sensors. 2024;24(13):4208. doi:10.3390/s24134208
77. Lieverse R, Van Someren EJW, Nielen MMA, Uitdehaag BMJ, Smit JH, Hoogendijk WJG. Bright light treatment in elderly patients with nonseasonal major depressive disorder: a randomized placebo-controlled trial. Arch Gen Psychiatry. 2011;68(1):61–70. doi:10.1001/archgenpsychiatry.2010.183
78. Tong H, Dong N, Lam CLM, Lee TMC. The effect of bright light therapy on major depressive disorder: a systematic review and meta-analysis of randomised controlled trials. Asian J Psychiatr. 2024;99:104149. doi:10.1016/j.ajp.2024.104149
79. Menegaz de Almeida A, Aquino De Moraes FC, Cavalcanti Souza ME, et al. Bright light therapy for nonseasonal depressive disorders: a systematic review and meta-analysis. JAMA Psychiatry. 2025;82(1):38–46. doi:10.1001/jamapsychiatry.2024.2871
80. Margrain TH, Boulton M, Marshall J, Sliney DH. Do blue light filters confer protection against age-related macular degeneration? Prog Retin Eye Res. 2004;23(5):523–531. doi:10.1016/j.preteyeres.2004.05.001
81. Firth J, Solmi M, Wootton RE, et al. A meta-review of “lifestyle psychiatry”: the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020;19(3):360–380. doi:10.1002/wps.20773
82. Sánchez-Villegas A, Galbete C, Martinez-González MA, et al. The effect of the Mediterranean diet on plasma brain-derived neurotrophic factor (BDNF) levels: the PREDIMED-Navarra randomized trial. Nutr Neurosci. 2011;14(5):195–201. doi:10.1179/1476830511Y.0000000011
83. Esmaeilzadeh M, Nasrollah M. Nutrition & exercise for brain health: enhancing cognitive function and neuroplasticity. Adv Clin Exp Med. 2025;34(9):1419–1423. doi:10.17219/acem/208533
84. Niu T, Zhang Y, Zhou X, et al. Associations of cMIND Diet with depressive and anxiety symptoms among old people in China: a nationwide study. Eur J Nutr. 2025;64(3):122. doi:10.1007/s00394-025-03628-7
85. Cherian L, Wang Y, Holland T, Agarwal P, Aggarwal N, Morris MC. DASH and Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) diets are associated with fewer depressive symptoms over time. J Gerontol a Biol Sci Med Sci. 2021;76(1):151–156. doi:10.1093/gerona/glaa044
86. Guu TW, Mischoulon D, Sarris J, et al. A multi-national, multi-disciplinary Delphi consensus study on using omega-3 polyunsaturated fatty acids (n-3 PUFAs) for the treatment of major depressive disorder. J Affect Disord. 2020;265:233–238. doi:10.1016/j.jad.2020.01.050
87. Malau IA, Chang JPC, Lin YW, Chang CC, Chiu WC, Su KP. Omega-3 fatty acids and neuroinflammation in depression: targeting damage-associated molecular patterns and neural biomarkers. Cells. 2024;13(21):1791. doi:10.3390/cells13211791
88. Hallahan B, Ryan T, Hibbeln JR, et al. Efficacy of omega-3 highly unsaturated fatty acids in the treatment of depression. Br J Psychiatry. 2016;209(3):192–201. doi:10.1192/bjp.bp.114.160242
89. Varteresian T, Lavretsky H. Natural products and supplements for geriatric depression and cognitive disorders: an evaluation of the research. Curr Psychiatry Rep. 2014;16(8):456. doi:10.1007/s11920-014-0456-x
90. Rebelos E, Tentolouris N, Jude E. The role of vitamin D in health and disease: a narrative review on the mechanisms linking vitamin D with disease and the effects of supplementation. Drugs. 2023;83(8):665–685. doi:10.1007/s40265-023-01875-8
91. Sailike B, Onzhanova Z, Akbay B, Tokay T, Molnár F. Vitamin D in central nervous system: implications for neurological disorders. Int J Mol Sci. 2024;25(14):7809. doi:10.3390/ijms25147809
92. Gao Y, Song XN, Wen ZP, et al. The association of vitamin deficiency with depression risk in late-life depression: a review. Front Nutr. 2025;12:1551375. doi:10.3389/fnut.2025.1551375
93. Spedding S. Vitamin D and depression: a systematic review and meta-analysis comparing studies with and without biological flaws. Nutrients. 2014;6(4):1501–1518. doi:10.3390/nu6041501
94. Raza ML, Hassan ST, Jamil S, Fatima W, Fatima M. Nutritional interventions in depression: the role of vitamin D and omega-3 fatty acids in neuropsychiatric health. Clin Nutr. 2025;45:270–280. doi:10.1016/j.clnu.2025.01.009
95. Slyepchenko A, Maes M, Jacka FN, et al. Gut microbiota, bacterial translocation, and interactions with diet: pathophysiological links between major depressive disorder and non-communicable medical comorbidities. Psychother Psychosom. 2017;86(1):31–46. doi:10.1159/000448957
96. Işık M, Köse F, Budak Ö, et al. Probiotic Bactolac alleviates depression-like behaviors by modulating BDNF, NLRP3 and MC4R levels, reducing neuroinflammation and promoting neural repair in rat model. Pflugers Arch. 2025;477(6):797–814. doi:10.1007/s00424-025-03084-6
97. Reigstad CS, Salmonson CE, Rainey III JF, et al. Gut microbes promote colonic serotonin production through an effect of short-chain fatty acids on enterochromaffin cells. FASEB J. 2015;29(4):1395–1403. doi:10.1096/fj.14-259598
98. Shah A, Lee YY, Suzuki H, et al. A pathophysiologic framework for the overlap of disorders of gut-brain interaction and the role of the gut microbiome. Gut Microbes. 2024;16(1):2413367. doi:10.1080/19490976.2024.2413367
99. Santini ZI, Jose PE, York Cornwell E, et al. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. Lancet Public Health. 2020;5(1):e62–e70. doi:10.1016/S2468-2667(19)30230-0
100. Trachtenberg E. The beneficial effects of social support and prosocial behavior on immunity and health: a psychoneuroimmunology perspective. Brain Behav Immun Health. 2024;37:100758. doi:10.1016/j.bbih.2024.100758
101. Woods A, Solomonov N, Liles B, Guillod A, Kales HC, Sirey JA. Perceived social Support and Interpersonal Functioning as predictors of treatment response among depressed older adults. Am J Geriatr Psychiatry. 2021;29(8):843–852. doi:10.1016/j.jagp.2020.12.021
102. Paquet C, Whitehead J, Shah R, et al. Social prescription interventions addressing social isolation and loneliness in older adults: meta-review integrating on-the-ground resources. J Med Internet Res. 2023;25:e40213. doi:10.2196/40213
103. Sadio R, Henriques A, Nogueira P, Costa A. Social prescription for the elderly: a community-based scoping review. Prim Health Care Res Dev. 2024;25:e46. doi:10.1017/S1463423624000410
104. Sneed RS, Chan ACY. The implications of intergenerational relationships for minority aging: a review of recent literature. Curr Epidemiol Rep. 2023;10(1):44–50. doi:10.1007/s40471-023-00319-x
105. Feng W, Geng P, Ge H, et al. The influence of intergenerational relationships on depressive symptoms in elderly patients with multiple chronic conditions: the mediating roles of self-rated health and well-being. BMC Public Health. 2025;25(1):1478. doi:10.1186/s12889-025-22759-4
106. Valentí Soler M, Agüera-Ortiz L, Olazarán Rodríguez J, et al. Social robots in advanced dementia. Front Aging Neurosci. 2015;7:133. doi:10.3389/fnagi.2015.00133
107. Yen HY, Huang CW, Chiu HL, Jin G. The effect of social robots on depression and loneliness for older residents in long-term care facilities: a meta-analysis of randomized controlled trials. J Am Med Dir Assoc. 2024;25(6):104979. doi:10.1016/j.jamda.2024.02.017
108. Yen HY, Huang CW, Chiu HL, Jin G. Social companion robots for alleviating depression and loneliness in institutional older adults. Psychiatry Res. 2023;328:115425. doi:10.1016/j.psychres.2023.115425
109. Mu Y, Lu P, Liu Q. Intergenerational support and depressive symptoms: moderating effects of community services and smart health devices. J Affect Disord. 2025;388:119602. doi:10.1016/j.jad.2025.119602
110. Barbini B, Attanasio F, Manfredi E, Cavallini MC, Zanardi R, Colombo C. Bright light therapy accelerates the antidepressant effect of repetitive transcranial magnetic stimulation in treatment resistant depression: a pilot study. Int J Psychiatry Clin Pract. 2021;25(4):375–377. doi:10.1080/13651501.2021.1894579
111. Abdollahi A, Lebouthillier DM, Najafi M, et al. Effect of exercise augmentation of cognitive behavioural therapy for the treatment of suicidal ideation and depression. J Affect Disord. 2017;219:58–63. doi:10.1016/j.jad.2017.05.012
112. Dong Y, Huang J, Liu H. Independent and joint associations of dietary diversity and physical activity on mental health among older adults in China: a cross-sectional study. BMC Public Health. 2025;25(1):599. doi:10.1186/s12889-025-21834-0
113. Gupta R, Omkarappa DB, Andrade RJ. Effectiveness of multimodal intervention for depression, self-esteem, and quality of life among elderly people residing at selected old age homes in Jalandhar, Punjab. J Educ Health Promot. 2023;12:154. doi:10.4103/jehp.jehp_138_23
114. Cabanel N, Kundermann B, Franz M, Müller MJ. Multiprofessional inpatient psychotherapy of depression in old age. Nervenarzt. 2017;88(11):1221–1226. doi:10.1007/s00115-017-0406-z
115. Hussenoeder FS, Jentzsch D, Matschinger H, et al. Depression and quality of life in old age: a closer look. Eur J Ageing. 2020;18(1):75–83. doi:10.1007/s10433-020-00573-8
116. Bruce ML, Ten Have TR, Reynolds CF, et al. Reducing suicidal ideation and depressive symptoms in depressed older primary care patients: a randomized controlled trial. JAMA. 2004;291(9):1081–1091. doi:10.1001/jama.291.9.1081
117. Alexopoulos GS, Reynolds CF, Bruce ML, et al. Reducing suicidal ideation and depression in older primary care patients: 24-month outcomes of the PROSPECT study. Am J Psychiatry. 2009;166(8):882–890. doi:10.1176/appi.ajp.2009.08121779
118. Alexopoulos GS. Mechanisms and treatment of late-life depression. Transl Psychiatry. 2019;9(1):188. doi:10.1038/s41398-019-0514-6
119. Brakowski J, Spinelli S, Dörig N, et al. Resting state brain network function in major depression - Depression symptomatology, antidepressant treatment effects, future research. J Psychiatr Res. 2017;92:147–159. doi:10.1016/j.jpsychires.2017.04.007IF:3.2Q2
120. Marx W, Lane M, Hockey M, et al. Diet and depression: exploring the biological mechanisms of action. Mol Psychiatry. 2021;26(1):134–150. doi:10.1038/s41380-020-00925-xIF:10.1Q1
121. Patrick RE, Dickinson RA, Gentry MT, et al. Treatment resistant late-life depression: a narrative review of psychosocial risk factors, non-pharmacological interventions, and the role of clinical phenotyping. J Affect Disord. 2024;356:145–154.
122. Shah SGS, Nogueras D, van Woerden HC, Kiparoglou V. Evaluation of the effectiveness of digital technology interventions to reduce loneliness in older adults: systematic review and meta-analysis. J Med Internet Res. 2021;23(6):e24712. doi:10.2196/24712
123. Dai X, Zhang R, Deng N, Tang L, Zhao B. Anesthetic influence on electroconvulsive therapy: a comprehensive review. Neuropsychiatr Dis Treat. 2024;20:1491–1502. doi:10.2147/NDT.S467695
124. O’Connell NE, Marston L, Spencer S, DeSouza LH, Wand BM. Non-invasive brain stimulation techniques for chronic pain. Cochrane Database Syst Rev. 2018;4(4):CD008208. doi:10.1002/14651858.CD008208.pub4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.