Back to Journals » ImmunoTargets and Therapy » Volume 14
Recent Advances in Immune Checkpoint Inhibitors for Triple-Negative Breast Cancer
Authors Corti C ![]() , Koca B
, Koca B ![]() , Rahman T
, Rahman T ![]() , Mittendorf EA
, Mittendorf EA ![]() , Tolaney SM
, Tolaney SM ![]()
Received 8 January 2025
Accepted for publication 13 March 2025
Published 3 April 2025 Volume 2025:14 Pages 339—357
DOI https://doi.org/10.2147/ITT.S495751
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah Wheeler
Chiara Corti,1– 4 Beyza Koca,1,2 Tasnim Rahman,1,2 Elizabeth A Mittendorf,1,2,5 Sara M Tolaney1,2,6
1Breast Oncology Program, Dana-Farber Brigham Cancer Center, Boston, MA, USA; 2Harvard Medical School, Boston, MA, USA; 3Division of New Drugs and Early Drug Development for Innovative Therapies, European Institute of Oncology IRCCS, Milan, Italy; 4Department of Oncology and Hematology-Oncology (DIPO), University of Milan, Milan, Italy; 5Division of Breast Surgery, Brigham and Women’s Hospital, Boston, MA, USA; 6Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, USA
Correspondence: Sara M Tolaney, Dana-Farber Cancer Institute, 450 Brookline Ave, Boston, MA, 02215, USA, Tel +1 617-632-3800, Fax +1 617-632-1930, Email [email protected]
Abstract: While immunotherapy has transformed treatment across various cancers, its impact on breast cancer is relatively limited. Recent advances have established immunotherapy as an effective approach for triple-negative breast cancer (TNBC), an aggressive subtype with limited therapeutic targets and poor prognosis. Specifically, pembrolizumab, an immune checkpoint inhibitor (ICI), is now approved for both first-line metastatic and early-stage TNBC. In metastatic TNBC, combining ICIs with chemotherapy, particularly pembrolizumab, has demonstrated survival benefits in patients with PD-L1–positive disease. However, extending these benefits to broader populations has proven challenging, highlighting the need for better patient selection and novel strategies. Emerging approaches include combining ICIs with antibody-drug conjugates, PARP inhibitors, dual ICIs, and bispecific antibodies targeting angiogenesis and immune checkpoints. These strategies aim to overcome resistance and expand immunotherapy’s efficacy beyond the PD-1/PD-L1 pathway. In early-stage disease, pembrolizumab combined with chemotherapy in the neoadjuvant setting has significantly improved pathologic complete response, event-free survival, and overall survival, establishing a new standard of care. Ongoing research aims to determine the optimal timing for ICI administration, explore less toxic chemotherapy backbones, utilize biomarkers for personalized treatment, and assess whether adding complementary treatments, such as radiation therapy for high-risk cases, can improve outcomes. This review examines the successes and setbacks of ICI use in TNBC, offering a comprehensive overview of current practices and future directions. It emphasizes optimizing ICI timing, leveraging biomarkers, and integrating novel agents to refine treatment approaches for both metastatic and early-stage TNBC. As immunotherapy continues to evolve, future research must address the unmet needs of this challenging breast cancer subtype, offering hope for improved outcomes.
Keywords: immunotherapy, precision medicine, biomarker, drug development, breast cancer
Introduction
Immunotherapy with immune checkpoint inhibitors (ICIs) has transformed treatment strategies for several cancer types but has historically lagged in breast cancer (BC).1 Advances in this field have primarily been seen in triple-negative breast cancer (TNBC), a challenging-to-treat subtype due to its lack of the actionable targets found in hormone receptor-positive and human epidermal growth factor receptor 2 (HER2)-positive BCs.2 Accounting for 10–15% of all BCs, TNBC is biologically and clinically aggressive, carrying approximately three times the risk of distant recurrence within five years of diagnosis compared to non-TNBC.3,4 The prognosis of metastatic TNBC remains poor, with a median overall survival (OS) of less than 18 months, and little improvement in outcomes over the past decade.5,6
These unmet needs, along with preclinical evidence of immune cell activation involved in antitumor surveillance and chemotherapy response, prompted immunotherapy-focused clinical trials in the early 2010s.1
Despite significant research investment in immune-oncology, pembrolizumab, an anti-programmed cell death protein 1 (PD-1) inhibitor, is the only US Food and Drug Administration (FDA)-approved immunotherapy-based treatment for TNBC in both advanced and early (stages II–III) settings.7,8
This review provides a concise overview of the current use of ICIs in TNBC clinical practice, highlighting their success as the tip of an iceberg amid numerous failed trials exploring various ICIs and combinations in different settings. We also discuss how these failures, along with emerging signals of activity from early-phase trials, are shaping ongoing efforts to harness the anti-cancer immune response in TNBC.
ICIs in TNBC Clinical Practice
Advanced Setting
In November 2020, the FDA granted accelerated approval of pembrolizumab combined with chemotherapy as the first-line treatment of patients with locally recurrent, unresectable, or metastatic TNBC with programmed cell death ligand 1 (PD-L1) expression (Combined Positive Score [CPS] ≥10, Dako 22C3) and a disease-free interval (DFI) ≥ 6 months. This approval was based on the findings of Phase 3 KEYNOTE-355 trial, a multicenter, double-blind, randomized, placebo-controlled study. The trial demonstrated a median progression-free survival (PFS) of 9.7 months (95% confidence interval [CI]: 7.6–11.3) in the pembrolizumab-chemotherapy arm versus 5.6 months (95% CI: 5.3–7.5) in the placebo arm (hazard ratio [HR]: 0.65; 95% CI: 0.49–0.86; P = 0.0012).8 It also showed a significant OS benefit of 23.0 months versus 16.1 months (HR: 0.73; 95% CI: 0.55–0.95; P = 0.0185) in the PD-L1 CPS ≥10 population.8
Two phase 3 randomized trials evaluated atezolizumab, an anti-PD-L1 agent, as first-line treatment in advanced TNBC. The IMpassion130 trial compared nab-paclitaxel with or without atezolizumab; the anti-PD-L1 agent improved PFS to 7.2 months versus 5.5 months in the intention-to-treat (ITT) population (HR: 0.80; 95% CI: 0.69–0.92; P = 0.002) but did not show a significant OS benefit. The trial’s hierarchical design only allowed formal OS evaluation in the PD-L1-positive population if OS in the overall population was significant.9 Consequently, the OS improvement of 25 months versus 18 months in patients with PD-L1-positive disease remains exploratory. Atezolizumab with nab-paclitaxel is approved by the European Medicines Agency (EMA) for PD-L1-positive tumors (≥1%, Ventana SP142) with a DFI ≥12 months but was withdrawn from FDA accelerated approval by the manufacturer in 2021. The IMpassion131 trial, which investigated atezolizumab with paclitaxel versus paclitaxel alone in patients with PD-L1-positive disease, failed to demonstrate PFS or OS benefits.10 The different results of IMpassion130 and IMpassion131 may be due to overlapping CIs, suboptimal biomarkers for patient selection (PD-L1), variations in premedication and chemotherapy’s immune effects, and the strong performance of the paclitaxel-alone arm.
Early Setting
In July 2021, pembrolizumab added to neoadjuvant chemotherapy became the standard of care for early high-risk TNBC, based on results from the phase 3 KEYNOTE-522 trial.7,11–13 This randomized trial investigated the use of neoadjuvant therapy combining paclitaxel-carboplatin and doxorubicin/epirubicin-cyclophosphamide with pembrolizumab/placebo, followed by surgery and subsequent adjuvant pembrolizumab/placebo for 9 cycles in patients with stage II–III TNBC. An interim analysis showed that adding pembrolizumab raised the overall pathologic complete response (pCR) rate from 51% to 65%.11 After a median follow-up of 63.1 months, pembrolizumab demonstrated an improvement in event-free survival (EFS), with rates of 81.3% versus 72.3% in the placebo group, reflecting a 37% reduction in events (HR: 0.63; 95% CI: 0.49–0.81).14 Additionally, at a median follow-up of 75.1 months, pembrolizumab provided a statistically significant and clinically meaningful OS benefit at 60 months, with rates of 86.6% (95% CI: 84.0–88.8) versus 81.7% (95% CI: 77.5–85.2) in the placebo group (p = 0.002).7 The subgroup analysis presented at the 2024 San Antonio Breast Cancer Symposium (SABCS) showed that, consistent with the ITT population, pembrolizumab demonstrated a positive trend in OS across subgroups, including those defined by PD-L1 expression, nodal status, overall stage, and baseline T2N0 status. The greatest OS benefit was observed in the residual cancer burden (RCB)-2 category.15
Other attempts to integrate ICIs in this setting lacked the statistical power to demonstrate EFS and OS benefits, as seen in the IMpassion031 trial.16 Adding atezolizumab to chemotherapy significantly improved the primary endpoint of pCR from 41% in the placebo arm to 58% in the atezolizumab arm (p = 0.004) in the ITT population.16 In the PD-L1-positive group (co-primary), pCR increased from 49% to 69% (p = 0.02).16 After a median follow-up of 39 months, EFS, disease-free survival (DFS), and OS favored the atezolizumab arm, but the differences were not statistically significant (Table 1).17 Recent data from GeparDouze, a phase 3 randomized controlled trial evaluating neoadjuvant chemotherapy with or without atezolizumab, followed by adjuvant atezolizumab or placebo in stage II–III TNBC, were presented at the 2024 SABCS. While adding atezolizumab to neoadjuvant chemotherapy increased pCR from 57% to 63%, it did not significantly improve EFS, the primary endpoint, after a median follow-up of 46.9 months (HR: 0.8; 95% CI: 0.62–1.03). The 4-year EFS was 85.2% in the atezolizumab arm and 81.9% in the control arm.18
 |
Table 1 Overview of Selected Phase 2–3 Clinical Trials Evaluating Immune Checkpoint Inhibitors in Early Triple-Negative Breast Cancer |
The NeoTRIP and GeparNuevo trials, which evaluated atezolizumab and durvalumab (anti-PD-L1) in the neoadjuvant-only setting, failed to meet their primary endpoints of EFS and pCR rate improvement, respectively (Table 1).20–22 Notably, NeoTRIP included the highest-risk population among immunotherapy-based early-stage TNBC trials, with approximately 50% of patients having locally advanced disease and 88% being node-positive;31 GeparNuevo demonstrated significant improvements in invasive DFS, distant DFS, and OS for patients treated with durvalumab.23
Advances and Challenges in the Metastatic Setting
Learning From Immunotherapy’s Failures
Despite promising preclinical and early-phase studies driving numerous trials involving ICIs for BC in the 2010s, as of December 2024, only one ICI, pembrolizumab, has received FDA approval for BC in both early and advanced settings.7,8,11,13 A recent cross-sectional study examined the landscape of BC immunotherapy-based trials conducted between 2004 and 2023.1 Of the 331 trials initiated, 120 had primary completion dates by November 30, 2022, and 30 (25%) failed to report outcomes. Among the 90 trials that reported results, 47 (52.2%) were positive, while 43 (47.8%) were negative. These findings highlight a surprisingly low return on the investment in immunotherapy trials over the past 15 years.1 Beyond ICIs - the focus of this review - other immunotherapy-based strategies, such as cytokines and cancer vaccines, have historically yielded disappointing results.32,33
Negative results from immunotherapy-based regimens - which may guide future ICI trial design - may stem from various factors, including an immunologically challenging clinical setting, such as metastatic disease in patients with heavily pretreated BC, characterized by high tumor burden and resistance mechanisms. Additional contributors include delivery platforms and target selection, particularly for cancer vaccines, the type and presence of concurrent therapies, and poorly understood or uncontrolled mechanisms of immune escape.32,33 These mechanisms may include alterations in antigen processing, loss of human leukocyte antigen expression, downregulation of tumor antigen expression, and factors promoting a cold tumor-immune microenvironment.33
An urgent need in advanced TNBC lies in addressing early relapses, a group for which data on epidemiology, clinical features, and biology remain limited. This subset of TNBC patients typically experiences relapse within 12 to 24 months following curative treatment, depending on the study definition. Early relapsing TNBC is associated with poor outcomes, with a median OS of 10.1 months (95% CI: 9.3–10.9).5 A U.S.-based study also highlighted the role of socioeconomic factors in poor outcomes.34 In a French cohort of patients diagnosed in 2008–2020 and treated with neo-/adjuvant taxane and/or anthracycline-based chemotherapy, 46% of TNBC recurrences (n = 881) occurred within 12 months of curative treatment, affecting younger patients with lower rates of breast cancer susceptibility gene (BRCA)1–2 mutations and higher primary tumor burden compared to those with later relapses.5
Treatment selection in this setting is particularly challenging, as patients relapsing within 12 months are often excluded from clinical trials of first-line ICIs. Specifically, IMpassion130 included patients who had completed neoadjuvant or adjuvant chemotherapy at least 12 months before randomization. Similarly, KEYNOTE-355 allowed patients with stage I–III BC to enroll if at least 6 months had passed since completing curative treatment. However, if a patient had received taxanes, gemcitabine, or platinum agents during curative treatment, the same class of chemotherapy could only be used if at least 12 months had elapsed since the completion of treatment and the first documented local or distant recurrence.
Given this framework, IMpassion132 was an ambitious phase 3 trial targeting a high-risk population of 595 patients with TNBC who relapsed within 12 months of curative treatment.35 Participants were randomized to receive first-line chemotherapy (carboplatin/gemcitabine or capecitabine) with or without atezolizumab. Initially, patients were not biomarker-selected, but a 2019 amendment restricted enrollment to those with PD-L1–positive TNBC (tumor immune cells ≥1%), as these patients had shown the most benefit from atezolizumab in IMpassion130. Among the 354 patients with PD-L1–positive disease, 68% had a DFI of less than 6 months, over 60% had visceral disease, and all had prior anthracycline and taxane-based treatments.35 After a median follow-up of 9.8 months, adding atezolizumab to chemotherapy did not improve OS, the primary endpoint, in the PD-L1–positive population. OS was 12.1 months with atezolizumab versus 11.2 months with placebo (HR 0.93; 95% CI: 0.73–1.20; P = 0.59). Since the primary endpoint was not met, secondary endpoints were not tested. Similarly, OS was not formally evaluated in the modified ITT population (all patients who were randomized before the amendment), but no OS benefit was observed for atezolizumab in this group either.35
Enhancing Immunotherapy Efficacy Through Combination Therapy
Antibody-Drug Conjugates (ADCs)
Following the positive results of the ASCENT trial, which led to FDA approval of sacituzumab govitecan (SG), a trophoblast cell surface protein 2 (TROP2)-targeted ADC with a topoisomerase 1 inhibitor payload, for pretreated metastatic TNBC, several studies are examining its use in combination with ICIs.36–38 The phase 2 Saci-IO TNBC trial (NCT04468061) is investigating whether adding pembrolizumab to SG can improve PFS in patients with PD-L1–negative metastatic TNBC as a first-line treatment. Meanwhile, ASCENT-04 (NCT05382286) is a randomized phase 3 trial comparing SG plus pembrolizumab to physician’s choice of therapy with pembrolizumab in patients with PD-L1–positive metastatic TNBC.
What is known about the potential synergy between ICIs and ADCs comes from the BEGONIA Phase 1b/2 trial (NCT03742102), which evaluates durvalumab combined with chemotherapy and novel targeted therapies as first-line treatment for metastatic TNBC. One arm, studying durvalumab with the HER2-targeted trastuzumab deruxtecan (T-DXd), enrolled 46 patients with advanced hormone receptor-negative, HER2-low BC.39,40 The objective response rate (ORR) was 57% (95% CI: 41–74), slightly improving with PD-L1 expression enrichment (71% for PD-L1-high and 62% for PD-L1-low). Median PFS was 12.6 months (95% CI: 8–not reached), and median duration of treatment (DOR) was not reached. Another arm of the BEGONIA trial evaluated the combination of datopotamab deruxtecan (Dato-DXd), a TROP2-targeted to poisomerase 1 inhibitor-based ADC, with durvalumab in 33 patients. The ORR was 79% (95% CI: 61–91), with responses observed regardless of PD-L1 expression. Median DOR was not reached, and all patients experienced either partial or complete response at 6 months.41 The phase 3 TROPION-Breast05 trial is currently evaluating Dato-DXd with or without durvalumab versus chemotherapy plus pembrolizumab in patients with PD-L1-positive, locally recurrent inoperable, or metastatic TNBC.42 In the early-stage setting, ADC-immunotherapy combinations are being investigated for adjuvant treatment escalation in patients with TNBC who have residual disease after surgical resection following neoadjuvant therapy. Specifically, the phase 3 TROPION-Breast03 trial is evaluating Dato-DXd with or without durvalumab, while the OptimICE-RD trial is assessing SG plus pembrolizumab versus pembrolizumab alone, with both arms optionally including capecitabine.43,44
PARP Inhibitors
While single-agent poly-ADP ribose polymerase inhibitors (PARPis) showed limited efficacy in non-BRCA-mutated TNBC, evidence of synergy between PARPis and ICIs, regardless of BRCA status, has led to combination treatment trials.45,46 The open-label TOPACIO trial evaluated niraparib and pembrolizumab in metastatic TNBC.46 Among 47 patients assessed for efficacy, the ORR was 21%, with a disease control rate (DCR) of 49%. Responses were primarily driven by BRCA-mutated tumors, which had an ORR of 47% and a DCR of 80%. Median PFS was 8.3 months for BRCA-mutated tumors and 2.1 months for BRCA wild-type.38,46 The MEDIOLA trial evaluated the combination of durvalumab and olaparib in BRCA mutation carriers.45 Among 30 patients, the ORR was 63%, the DCR was 80%, and median PFS was 8.2 months. These results are not better compared to those from PARPi monotherapy trials like OlympiAD and EMBRACA, suggesting that adding ICI to PARPi did not improve outcomes over monotherapy.38 However, a similar combination strategy added to paclitaxel has been evaluated in the early setting with promising results.27 The phase 2 I-SPY2 trial investigated the neoadjuvant durvalumab-olaparib-paclitaxel combination in stage II–III HER2-negative BC. The regimen increased pCR rates from 20% (299 patients in the paclitaxel control arm) to 37% (73 patients in the experimental arm).27 In TNBC, pCR rates rose from 27% to 47%.27
The phase 2 KEYLYNK-009 trial found that maintenance with pembrolizumab and olaparib after induction with pembrolizumab and carboplatin-gemcitabine did not improve outcomes compared to continued pembrolizumab and chemotherapy in metastatic TNBC.47 The HR for PFS was 0.98 (95% CI: 0.72–1.33; P = 0.4556), and for OS was 0.95 (95% CI: 0.64–1.40) in the ITT population.47 Despite the negative results, pembrolizumab and olaparib maintenance demonstrated similar efficacy to continued chemotherapy with pembrolizumab, along with a lower incidence of treatment-related adverse events (AEs). In BRCA mutation carriers, a positive numerical trend for PFS and OS was observed.47 Finally, a phase 2 randomized trial evaluated olaparib with or without atezolizumab in BRCA-mutated patients with advanced HER2-negative BC. Among 78 enrolled patients, there was no statistically significant difference in PFS, the primary endpoint, between the two arms. PFS was 7.0 months (95% CI, 5.5–11.5) in the olaparib monotherapy arm and 7.67 months (95% CI, 5.6–10) in the combination arm. Median OS was 26.5 months (95% CI, 19.2–NR) for monotherapy versus 22.4 months (95% CI, 16.6–31.3) for the combination.48
Dual Checkpoint Targeting
To broaden the therapeutic use of ICIs in BC, various agents are being explored beyond the PD-1/PD-L1 pathway, targeting Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), Lymphocyte Activation Gene 3 (LAG-3), T cell immunoreceptor with immunoglobulin and ITIM domain (TIGIT), and immunoglobulin-like transcript 3 (ILT3), among others.32,49
CTLA-4, a transmembrane protein on regulatory and anergic T cells, is critical to immune regulation and priming.32 Dual blockade of PD-L1 and CTLA-4, which targets distinct phases of the immune response, is a first-line strategy in several cancers and has shown potential in BC, particularly with high PD-L1 expression. A single-arm pilot study evaluated the overall response rate to durvalumab and tremelimumab (anti-CTLA-4) in BC, but was terminated for futility, as only 3 of 18 patients (17%) responded. Notably, all responses occurred in patients with TNBC, achieving an ORR of 43%.50 The randomized phase 2 KEYNOTE-046 trial evaluated an anti–PD-L1/CTLA-4 bispecific protein combined with nab-paclitaxel, demonstrating promising efficacy.51 Among 25 evaluable patients, the ORR was 44.0% (95% CI, 24.4–65.1), with a not yet mature median duration of response (primary endpoints). Median PFS was 7.33 months (95% CI, 3.68–11.07), and median OS reached 30.9 months (95% CI, 14.75–not evaluable).51 In patients with PD-L1–positive disease, PFS was 8.61 months compared to 4.73 months in patients with PD-L1–negative disease, with a 2-year OS rate of 62.5% versus 57.1%, respectively.51 The NIMBUS trial assessed dual blockade with ipilimumab and nivolumab in patients with metastatic BC with high tumor mutation burden (TMB >9 mutations/Mb).52 Among 30 patients, the ORR was 17% after a median follow-up of 9.7 months, with 3 of the 5 responders being hormone receptor positive. Stable disease was observed as the best response in 20% of patients. Notably, those with TMB >14 mutations/Mb had a significantly higher response rate of 60%, compared to 4% for patients with TMB between 9 and 14.38,52 The DART/SWOG-S1609 study included a cohort of patients with the aggressive metaplastic subtype of TNBC to evaluate the combination of ipilimumab and nivolumab. Preliminary results showed an ORR of 18% (95% CI: 6–40), with responses in 3 of 17 patients, a median PFS of 2 months, and a median OS of 12 months. No association was observed between response and stromal tumor infiltrating lymphocytes (sTILs), PD-L1 expression, or TMB.38,53 Novel technologies, such as bispecific antibodies, have enabled the simultaneous targeting of multiple checkpoint inhibitors with a single drug. This approach was initially developed based on the hypothesis that the targets bound by the bispecific antibody could enhance each other’s binding affinity to the antibody.54 In this regard, a phase 2 study evaluated the anti-PD-L1/CTLA-4 bispecific antibody KN046 as a first-line treatment for metastatic TNBC.51 Among 27 patients receiving KN046 at two dose levels (3 mg/kg and 5 mg/kg), 25 were evaluable for ORR and duration of response, the primary endpoints. The ORR was 44% (95% CI, 24.4–65.1), with a median treatment duration not yet reached. Median PFS was 7.33 months (95% CI, 3.68–11.07), and median OS was 30.92 months (95% CI, 14.75–NE). In patients with PD-L1-positive disease, PFS was 8.61 months versus 4.73 months in patients with PD-L1-negative disease, and the 2-year OS rate was 62.5% versus 57.1%.51
LAG-3 inhibits T-cell proliferation and sustains T-cell exhaustion by binding to major histocompatibility complex (MHC) class II.55 In the metastatic setting, ieramilimab, a humanized anti-LAG-3 monoclonal antibody, showed good tolerability in combination with the anti-PD-1 antibody spartalizumab in a phase 1 study.56 In a phase 2 trial evaluating ieramilimab followed by spartalizumab, TNBC patients who were anti-PD-1/L1–naive reported an ORR of 14.3% (90% CI: 4.0–32.9%) with treatment every three weeks and 4.8% (90% CI: 0.2–20.7%) with treatment every four weeks. No clinical responses were observed in TNBC patients pretreated with anti-PD-1/L1.55
TIGIT, a co-inhibitor receptor expressed on natural killer and T cells, has shown promise in preclinical studies when inhibited alongside PD-L1 blockade.32 Currently, two TIGIT-targeting agents, tiragolumab and SEA-TGT, are under clinical investigation for metastatic TNBC, either alone or in combination with anti-PD-L1 therapies and/or chemotherapy, with results pending (NCT04584112, NCT06175390, NCT04254107).32 Bispecific antibody technologies have also been applied to this immune checkpoint, such as the PD-1/TIGIT bispecific rilvegostomig. This agent is currently being evaluated in a phase 1/2a trial in combination with a B7-H4-directed ADC in patients with advanced solid malignancies, including BC (NCT05123482). Additionally, it is being studied in the early-stage setting in combination with T-DXd as part of the I-SPY platform trial (NCT01042379).
Finally, the inhibitory receptor ILT3, linked to T-cell suppression and immune tolerance, is an adverse prognostic biomarker in TNBC.49 Preclinical studies in BC suggest that targeting ILT3 may mitigate its negative prognostic impact and enhance anti–PD-1–driven T-cell responses.32,57 Early-phase clinical trials evaluating anti-ILT3 monotherapy and its combination with pembrolizumab have demonstrated modest antitumor activity and good tolerability.49
Targeting PD-1/-L1 and VEGF
Combining anti-angiogenic drugs with immunotherapy is another promising approach.58 Historically, pooled analyses of vascular endothelial growth factor (VEGF) inhibitors plus chemotherapy in metastatic TNBC showed a PFS HR of 0.63 (95% CI: 0.52–0.76) and an OS HR of 0.96 (95% CI: 0.79–1.16).58 Bevacizumab improved median PFS to 8.1 months compared to 5.4 months with chemotherapy alone, while median OS was 18.9 versus 17.5 months.58 More recent studies suggest these drugs enhance immunotherapy by modulating the tumor microenvironment, promoting dendritic cell maturation, and reducing suppressive immune cells.54,59 Phase 2 trials FUTURE-C Plus and ATRACTIB tested combinations such as camrelizumab, famitinib, and nab-paclitaxel, as well as atezolizumab, bevacizumab, and paclitaxel, achieving ORRs of 81.3% and 63.0%, respectively.60,61 The FUTURE-C Plus trial reported an OS of 29.4 months (95% CI: 23.3–35.5), the longest in first-line metastatic TNBC at the time, with no significant safety concerns.60 Innovative bispecific antibodies targeting immune checkpoints and angiogenesis are also emerging.54 Ivonescimab, a humanized bispecific antibody targeting PD-1 and VEGF-A, has been approved in China for advanced non-small cell lung cancer in combination with pemetrexed and carboplatin.62,63 A phase 2 trial of ivonescimab with a taxane as first-line therapy for metastatic TNBC (n = 36) recently showed an ORR of 72.4%, with 69.6% in PD-L1 CPS <10 and 86.7% in PD-L1 CPS <1%, outperforming the 40% ORR observed in the KEYNOTE-355 ITT population.64 The SABCS 2024 update reported an ORR of 80.0%, with 79.3% in patients with PD-L1 CPS < 10, 88.2% in those with PD-L1 CPS < 1%, and 83.3% in those with PD-L1 CPS ≥ 10. Median PFS was 9.36 months (95% CI, 6.24–NE).65 In the same first-line setting, the PD-L1/VEGF-A bispecific antibody PM8002/BNT327 combined with nab-paclitaxel demonstrated promising results in a phase 1b/2 study (n = 42). At SABCS 2024, an ORR of 73.8% was reported, with 56.3% in patients with PD-L1 CPS < 10, 76.9% in PD-L1 CPS < 1, and 100.0% in PD-L1 CPS ≥ 10.66,67 Median PFS was 13.5 months (95% CI: 9.4–19.3). Interim OS analysis reported 12-month, 15-month, and 18-month OS rates of 80.8%, 78.1%, and 69.7%, respectively, with median OS not yet reached.67 Similarly, the combination of the anti-PD-1 inhibitor AK105 and the multitargeting antiangiogenic tyrosine kinase inhibitor (TKI) anlotinib as first-line treatment for metastatic TNBC demonstrated an ORR of 75.0%, a median PFS of 10.6 months (95% CI: 7.59–10.69), and a median OS not yet reached (13.3–NR).68 These three strategies demonstrated significant antitumor activity and low primary resistance, with ORR and PFS appearing independent of PD-L1 status. The safety profile was manageable across all studies, primarily involving hematologic and liver toxicity. However, one death from hepatitis was reported in the trial evaluating AK105 and anlotinib.
Other Targeted Therapies
In a phase 1b trial evaluating the pan-AKT inhibitor ipatasertib in combination with atezolizumab and paclitaxel/nab-paclitaxel a 73% ORR among 26 patients was described, with no significant response difference based on PD-L1 expression.69 The Phase II COLET study evaluated the mitogen-activated protein kinase (MEK) inhibitor cobimetinib with chemotherapy, with or without atezolizumab, as first-line therapy for advanced TNBC.70 Although no significant differences in ORR or PFS were observed between treatment arms, patients with a DFI <12 months showed improved PFS (5.4 versus 1.7 months; HR: 0.29; 95% CI; 0.09–0.95). Retrospective analysis indicated better outcomes for PD-L1–positive tumors, with an ORR of 39% versus 19% and median PFS of 7.0 versus 3.7 months (95% CI 2.14–6.14).70
Advances and Challenges in the Early Setting
There is no doubt that ICIs have revolutionized the treatment landscape for TNBC in the curative setting, with recent data from KEYNOTE-522 documenting improvements in pCR, EFS, and, more importantly, OS. However, some questions remain regarding treatment optimization. For example, data suggest that the neoadjuvant phase for administering ICI may be more important than the adjuvant phase, raising the question of whether the adjuvant phase is necessary for all patients. Additionally, the four-drug chemotherapy in KEYNOTE-522, including cardiotoxic anthracyclines, prompts consideration of less toxic preoperative alternatives. Finally, since 35–40% of patients do not experience pCR with this regimen, the potential benefit of escalated regimens to improve outcomes is also under discussion.
Does the Timing of Checkpoint Inhibition—Pre-Operative vs Post-Operative—Matter?
The Alexandra/IMpassion030 trial explored the use of atezolizumab combined with chemotherapy in the adjuvant setting following upfront surgery. The results were disappointing, with futility declared (HR: 1.12; 95% CI: 0.87–1.45; p = 0.370) and no benefits observed across any subgroups, including those defined by PD-L1 status.71 These findings may support the theory that delivering ICIs while the primary tumor remains present may generate a stronger systemic antitumor immune response, likely due to the availability of more neoantigens to activate the immune system.30,72,73
Of note, the A-BRAVE trial randomized early TNBC patients with residual disease (RD) after neoadjuvant chemotherapy or those at high risk following upfront surgery and adjuvant chemotherapy to receive either adjuvant avelumab or observation. While the trial did not achieve its primary endpoint of DFS (HR: 0.81; 95% CI: 0.61–1.09; p = 0.172), it demonstrated significant improvements in OS (secondary endpoint: HR: 0.66; 95% CI: 0.45–0.97; p = 0.035) and distant DFS (exploratory endpoint: HR: 0.70; 95% CI: 0.50–0.96; p = 0.0277).74 The strongest signal for adjuvant immunotherapy benefit was observed in the ~80% of patients with RD after neoadjuvant chemotherapy (Stratum B), while the benefit for those who underwent upfront surgery (Stratum A) remains unclear (events: 11/40 in the avelumab arm vs 12/43 in the control arm), especially in light of Alexandra trial data.75 The phase 3 SWOG1418/NRG-BR006 trial is currently investigating the use of adjuvant pembrolizumab in patients with RD following neoadjuvant chemotherapy.
Pre-Operative Timing of ICI Seems More Important. Is Adjuvant/Post-Operative ICI Necessary?
An indirect comparison of invasive DFS in the GeparNuevo trial, which involved neoadjuvant-only chemoimmunotherapy, and EFS in the KEYNOTE-522 trial, which included both neoadjuvant chemoimmunotherapy and adjuvant immunotherapy, shows similar results.22,23 GeparNuevo reported an 8.4% difference at three years between the experimental (85.6%) and control (77.2%) arms.23 Similarly, KEYNOTE-522 showed a 7.7% difference at three years (EFS: 84.5% experimental arm vs 76.8% control arm), increasing to a 9% difference at 60 months (EFS: 81.3% experimental arm vs 72.3% control arm).7,13 Both trials demonstrated excellent long-term outcomes for patients experiencing pCR, with a 3-year invasive DFS of 95.5% for those receiving durvalumab in GeparNuevo and 94.4% for those receiving pembrolizumab in KEYNOTE-522.13,23
Ongoing trials like A012103/OptimICE-pCR are exploring ICI optimization in TNBC by evaluating the omission of adjuvant pembrolizumab in patients who experience pCR after neoadjuvant chemoimmunotherapy (NCT05812807).25,26
Exploring Alternatives to the Preoperative Chemotherapy Backbone
To address cardiotoxicity concerns related to the presence of anthracyclines in the KEYNOTE-522 regimen, the phase 2 non-randomized NeoPACT study evaluated a shorter treatment regimen. This regimen omits anthracyclines and incorporates docetaxel, carboplatin, and pembrolizumab over 18 weeks. This approach targeted patients with stage I–III TNBC measuring at least 1.0 cm, node-positive disease, or hormone receptor status ≤10%. The study reported a pCR rate of 58% (primary endpoint), with an additional 11% experiencing RCB-1, suggesting a potentially effective and less toxic treatment strategy in the preoperative setting for TNBC.24 The 3-year EFS was 86% overall, with 98% for patients experiencing pCR and 68% for those with RD. The S2212/SCARLET trial is a phase 3 trial that looks to more definitely address this question using a non-inferiority design to compare a shorter chemoimmunotherapy regimen of carboplatin and taxane, excluding anthracyclines, to the KEYNOTE-522 regimen, with EFS as the primary endpoint (NCT05929768).
Ongoing research is investigating whether ADCs could partially or fully replace preoperative chemotherapy. A key hypothesis for anti-topoisomerase 1-based ADCs is that their payloads may induce DNA damage, activating the STING pathway, with potential efficacy enhanced by pembrolizumab.76,77 In the I-SPY2.2 trial, a multicenter phase 2 platform study using a sequential multiple assignment randomized design in the neoadjuvant BC setting, 106 patients were treated with Dato-DXd and durvalumab.28 The overall pCR rate was 50% (53/106), with the highest efficacy observed in the Immune+ subtype (79%), followed by the TNBC subtype (62%). In the Immune+ group, Dato-DXd/durvalumab surpassed the predefined success threshold after block A (experimental therapy), with 54% achieving pCR after Dato-DXd/durvalumab alone and 92% without doxorubicin–cyclophosphamide (after blocks A + B, subtype-specific ‘best in class’ treatment). This treatment strategy progressed through all blocks in the hormone-negative/immune-negative subtype.28 In this context, the TROPION-Breast04 trial is evaluating Dato-DXd with durvalumab in patients with stage II–III TNBC or hormone receptor-low HER2-negative BC. Patients are randomized to receive either Dato-DXd/durvalumab for 8 cycles followed by surgery and 9 additional cycles of durvalumab (with or without treatment escalation with chemotherapy of physician’s choice for residual disease) or the KEYNOTE-522 regimen.78
The NeoSTAR trial is investigating the potential for an ADC to replace part of the chemotherapy backbone used in KEYNOTE-522. It evaluated neoadjuvant SG in patients with TNBC (cT1c–T4, any nodal status). After 4 cycles of SG, patients could either proceed directly to surgery followed by adjuvant treatment at the investigator’s discretion or receive additional neoadjuvant therapy if biopsy-confirmed residual disease was present.79 Among the 50 patients enrolled, 26 proceeded directly to surgery after SG, with an overall pCR rate of 30% (15/50; 95% CI 18–45%). Of the remaining patients, 11 had residual disease, classified as RCB-1 (n = 3), RCB-2 (n = 5), or RCB-3 (n = 3). The trial’s next phase, evaluating SG in combination with pembrolizumab, has completed enrollment and results are awaited.
The combination of T-DXd and durvalumab is currently being studied as a preoperative treatment for patients with inflammatory BC, including HER2-positive disease or HER2-low BC, in the open-label, non-randomized phase 2 TRUDI trial (NCT05795101).
Enhancing the KN522 Regimen: Can Additions Improve Outcomes?
Preliminary findings suggest radiation therapy may enhance the effects of immunotherapy in early BC. For example, the results from the Neo-CheckRay study indicate potential benefits from adding durvalumab (± oleclumab, an anti-CD73 agent that reduces the production of immunosuppressive adenosine) to neoadjuvant chemotherapy and stereotactic body radiation therapy (SBRT) compared to chemotherapy and SBRT alone in patients with early-stage, MammaPrint high-risk (luminal B), hormone receptor-positive/HER2-negative BC. The trial enrolled 135 patients, all of whom received neoadjuvant chemotherapy (paclitaxel followed by dose-dense epirubicin/cyclophosphamide) and SBRT (3 × 8 Gy). Patients were divided into three arms: the standard arm received chemotherapy and SBRT alone, the durvalumab arm added durvalumab to the regimen, and the combination arm included both durvalumab and oleclumab alongside chemotherapy and SBRT. Although the primary endpoint of increasing the RCB 0–1 rate from 15% to 45% was not met, the study showed improvements in pCR rates. The standard arm experienced a pCR rate of 16.7%, while the durvalumab arm reached 33.3%. The combination arm, including both durvalumab and oleclumab, showed a similar pCR improvement at 31.1%.80 Specifically in TNBC, results from a similar strategy combining pembrolizumab and radiation therapy are awaited (P-RAD, NCT04443348, Table 2).
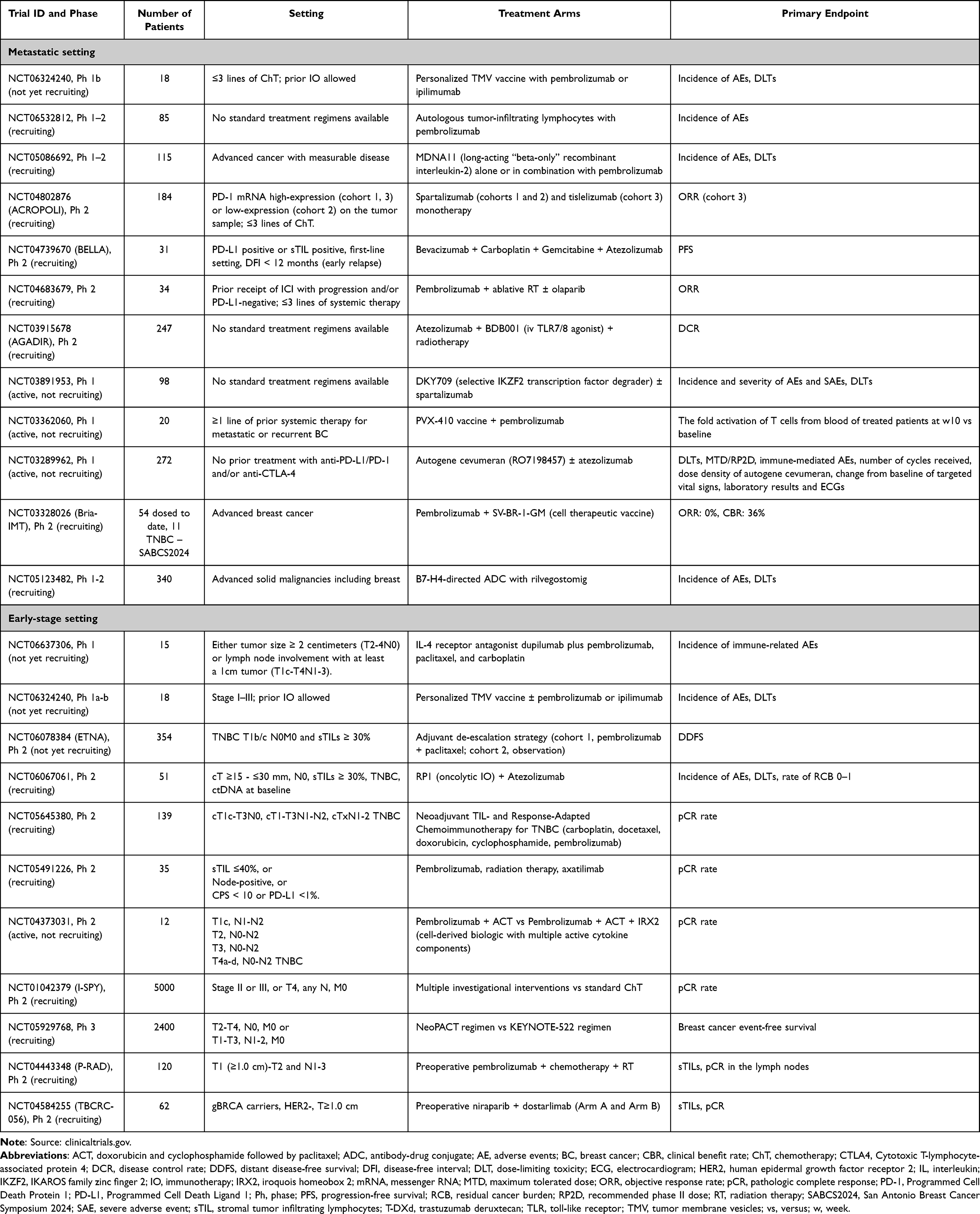 |
Table 2 Ongoing (Recruiting, Active, Not Recruiting or Not yet Recruiting) Clinical Trials Investigating Immune Checkpoints in Triple Negative Breast Cancer, as of October 20th, 2024 |
The addition of a second immune agent in combination with a PD-1/PD-L1 inhibitor has been explored in the early-stage setting following multiple unsuccessful attempts in metastatic disease.1 The I-SPY2 trial, a multicenter, open-label, adaptively randomized phase 2 study, investigated dual immune blockade with the anti-PD-1 agent cemiplimab and fianlimab, an anti-LAG3 agent, in 73 patients with early-stage BC (40 hormone receptor-positive and 33 TNBC).81 The control arm included 357 patients (201 hormone receptor-positive and 156 TNBC). In HER2-negative disease, the estimated pCR rate in the study arm was 44% (95% CI, 34–54%), compared to 21% (95% CI, 17–25%) in the control arm. Among patients with TNBC, the pCR rate was higher at 53% (95% CI, 38–67%) versus 29% (95% CI, 22–36%) in the control arm. Finally, given that an mRNA-based neoantigen vaccine combined with pembrolizumab has demonstrated a 44% reduction in recurrence risk in stage III/IV melanoma, despite significant differences in biology, tumor microenvironment, and immunogenicity between melanoma and BC, similar strategies might warrant exploration in selected BC subtypes.82
Can Biomarkers Help Reduce Therapy or Eliminate Chemotherapy Altogether?
As neoadjuvant chemoimmunotherapy becomes a standard component of treatment for stage II–III TNBC, with potential expansion to other early-stage subtypes, efforts are ongoing to identify predictors of response to ICIs. Notably, the KEYNOTE-522 trial found no evidence supporting PD-L1 as a biomarker for immunotherapy efficacy, as chemoimmunotherapy benefits were observed regardless of PD-L1 status or other clinical and biological factors.30 To date, no predictive biomarkers for chemoimmunotherapy response have been identified.30
Accurately predicting response to chemoimmunotherapy would provide significant clinical value, allowing for tailored treatment to maximize benefits while minimizing toxicity. For example, treatment-related AEs in KEYNOTE-522 led to discontinuation of trial drugs in 23.3% of patients receiving pembrolizumab with chemotherapy and 12.3% in the placebo group.8 In a multicenter real-world study, 39.5% of 228 participants discontinued the KEYNOTE-522 regimen early due to AEs, with 31.9% experiencing immune-related AEs.83 In patients who respond well to neoadjuvant chemotherapy alone, avoiding the risk of immune-related toxicities—which can be severe, irreversible, and potentially impact fertility and quality of life—would be important. Conversely, identifying poor responders to neoadjuvant chemotherapy or chemoimmunotherapy, who are at higher risk of relapse shortly after surgery, would enable treatment escalation, such as enrolling in trials for high-risk patients or exploring alternative therapies or immune combinations.30
In this regard, there is increasing evidence that the effectiveness of neoadjuvant treatments, with or without ICIs, may correlate with pre-treatment tumor characteristics such as mutational profiles, hormone receptor expression, immune cell presence and spatial organization, specific gene signatures, and levels of proliferating versus quiescent cancer and immune cells.30,32,84–86 It may also relate to immune-related changes between baseline and on-treatment samples (tissue or blood-based).86,87 However, challenges persist as studies often focus on specific characteristics in a descriptive manner, making it difficult to synthesize all available knowledge into a comprehensive, holistic framework. Additionally, patient cohorts used to explore predictors or validate signatures often include those who received only chemotherapy or a mix of chemotherapy and chemoimmunotherapy, resulting in a lack of robust data on the specific benefit of adding ICIs to chemotherapy.
Detecting circulating tumor DNA (ctDNA) after surgery may provide another way to identify patients with TNBC at high risk of early relapse. The phase 2 ASPRIA trial (NCT04434040) is currently investigating whether intensified adjuvant therapy with an ADC and ICI combination can eliminate ctDNA and improve survival outcomes in ctDNA-positive patients with RD following surgery. Enhanced assay sensitivity is expected to improve the predictive accuracy of minimal residual disease clearance in relation to pCR.
Furthermore, sTILs are linked to pCR and long-term outcomes in TNBC treated with anthracycline-based chemotherapy. A pooled analysis of two studies involving 474 patients with stage I (T >1 cm)-III TNBC treated with anthracycline-free neoadjuvant regimens recently showed that sTILs, at a 30% threshold, stratified outcomes in stage III disease. Five-year OS was 86% in patients with ≥30% sTILs compared to 57% in those with <30% (HR: 0.29; P = 0.014), with a similar numeric trend in stage II (5-year OS: 93% vs 89%, HR: 0.55; P = 0.179). Among stage II–III patients who experienced pCR, EFS was significantly better in those with ≥30% sTILs (HR: 0.16; P = 0.047).88 Immune enrichment, evaluated by sTILs, PD-L1, and the DetermaIO signature, was observed in nearly 50% of NeoPACT participants and correlated with high pCR rates exceeding 70%.24 Therefore, as sTIL enrichment is strongly associated with pCR in TNBC and may help identify patients suitable for de-escalation of neoadjuvant chemoimmunotherapy, the NeoTRACT trial is investigating tailoring neoadjuvant therapy based on pretreatment sTIL enrichment (NCT05645380). Specifically, for patients with immune-enriched TNBC (sTILs ≥30%), a short, anthracycline-free taxane–platinum chemoimmunotherapy regimen is expected to achieve high pCR rates. Finally, the adaptive phase 2 BELLINI trial investigated whether a short course of combination ICI could induce immune activation, defined as a twofold increase in CD8+ T cells or IFNG (interferon gamma, primary endpoint).29 High levels of sTILs were strongly associated with response. Single-cell RNA sequencing revealed that higher pretreatment levels of tumor-reactive CD8+ T cells and follicular helper T cells, as well as shorter distances between tumor and CD8+ T cells, correlated with response. In contrast, increased regulatory T cells after treatment were linked to nonresponse.29 Based on these findings, Cohort C was opened for patients with high sTILs (≥50%), who received 6 weeks of neoadjuvant anti-PD-1 and anti-CTLA-4 therapy followed by surgery, with pCR as the primary endpoint. Among 15 patients, 53% had a major pathological response (<10% viable tumor), and 33% experienced pCR.29
Conclusion and Future Perspectives
ICIs represent a new era for the treatment of TNBC, offering clinically meaningful improvements in outcomes for selected patient subsets.
In metastatic TNBC, the approval of pembrolizumab for PD-L1–positive disease has marked a pivotal advance, yet outcomes remain suboptimal, particularly for early-relapsing or heavily pretreated patients. The median OS of 18 months in metastatic TNBC is still a major research failure, despite years of effort. Novel strategies, such as combining ICIs with ADCs, PARPis, dual immunotherapies, or bispecific antibodies, are showing promise in overcoming resistance and enhancing efficacy (Figure 1), but it remains to be proven whether these combinations will provide meaningful hope for this patient population.
 |
Figure 1 Successes and Challenges in Incorporating Immune Checkpoint Inhibitors into the Treatment Arsenal for Triple-Negative Breast Cancer. Created in BioRender. Corti, C (2024) https://BioRender.com/u62i348. Abbreviations: ADC, antibody-drug conjugate; ChT, chemotherapy; FDA, Food and Drug Administration; HIF1α, Hypoxia-Inducible Factor 1 alpha; ICI, immune checkpoint inhibitor; IO, immunotherapy; KN, Keynote; Op, operative; PARP, poly-ADP ribose polymerase; pCR, pathologic complete response; PD-1, Programmed Cell Death Protein 1; RD, residual disease; TNBC, triple-negative breast cancer; VEGF, Vascular endothelial growth factor. |
In the early-stage setting, the addition of pembrolizumab to neoadjuvant chemotherapy has significantly enhanced pCR, EFS and – more importantly – OS, establishing a new standard of care for high-risk TNBC. However, the KEYNOTE-522 trial employed a four-drug chemotherapy regimen, which extended the treatment duration and resulted in increased fatigue, treatment interruptions, and short-term side effects. The addition of pembrolizumab also introduced potential immune-related long-term toxicities. While pCR is an easily measurable endpoint linked to favorable survival outcomes in TNBC, it has shown limitations in some ICI-based trials. Finally, unlike chemotherapy, where treatment timing (preoperative or postoperative) historically did not impact survival, the timing of ICI-based treatment appears to be more crucial for outcomes. Future research must refine the use of biomarkers to personalize treatment, reduce toxicity, and identify patients who may benefit from therapy de-escalation or alternative combinations.
Looking ahead, ongoing studies are exploring ways to optimize immunotherapy timing, improve predictive biomarkers, and incorporate innovative therapies. From tailoring neoadjuvant regimens to leveraging adaptive trial designs, the future of immunotherapy in TNBC depends on addressing both biological and clinical challenges. These efforts hold promise to expand the benefits of ICIs and improve outcomes for this aggressive and heterogeneous disease.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, article design, and literature search, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
CCo reports travel/accommodations (to scientific meeting) from Veracyte (2023), and is supported by the Fondazione Gianni Bonadonna (FGB) and Associazione Italiana per la Ricerca contro il Cancro (AIRC) (2024-2026). All the competing interests were outside the submitted work. BK and TR have no potential conflicts of interest to disclose. EAM reports compensated service on scientific advisory boards for AstraZeneca, BioNTech, Merck and Moderna; uncompensated service on steering committees for Bristol Myers Squibb and Roche/Genentech; speakers honoraria and travel support from Merck Sharp & Dohme; and institutional research support from Roche/Genentech (via SU2C grant) and Gilead. EAM also reports research funding from Susan Komen for the Cure for which she serves as a Scientific Advisor, and uncompensated participation as a member of the American Society of Clinical Oncology Board of Directors. All the competing interests were outside the submitted work. SMT reports a consulting or advisory role for Novartis, Pfizer (SeaGen), Merck, Eli Lilly, AstraZeneca, Genentech/Roche, Eisai, Sanofi, Bristol Myers Squibb/Systimmune, Daiichi Sankyo, Gilead, Zymeworks, Zentalis, Blueprint Medicines, Reveal Genomics, Sumitovant Biopharma, Artios Pharma, Menarini/Stemline, Aadi Bio, Bayer, Incyte Corp, Jazz Pharmaceuticals, Natera, Tango Therapeutics, eFFECTOR, Hengrui USA, Cullinan Oncology, Circle Pharma, Arvinas, BioNTech, Johnson&Johnson/Ambrx, Launch Therapeutics, Zuellig Pharma, Bicycle Therapeutics, BeiGene Therapeutics, Mersana, Summit Therapeutics; reports institutional research funding from Genentech/Roche, Merck, Exelixis, Pfizer, Lilly, Novartis, Bristol Myers Squibb, Eisai, AstraZeneca, Gilead, NanoString Technologies, Seattle Genetics, OncoPep, Daiichi Sankyo, Menarini/Stemline, Jazz Pharmaceuticals; and receives travel support from Eli Lilly, Sanofi, Gilead, Jazz Pharmaceuticals, Pfizer, Arvinas. All the competing interests were outside the submitted work.
References
1. Mariani M, Viale G, Galbardi B, et al. Completion rate and positive results reporting among immunotherapy trials in breast cancer, 2004-2023. JAMA Network Open. 2024;7(7):e2423390. doi:10.1001/jamanetworkopen.2024.23390
2. Licata L, Dieci MV, De Angelis C, et al. Navigating practical challenges in immunotherapy for metastatic triple negative breast cancer. Cancer Treat Rev. 2024;128:102762. doi:10.1016/j.ctrv.2024.102762
3. Zagami P, Carey LA. Triple negative breast cancer: pitfalls and progress. NPJ Breast Cancer. 2022;8(1):95. doi:10.1038/s41523-022-00468-0
4. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49. doi:10.3322/caac.21820
5. Grinda T, Antoine A, Jacot W, et al. Real-world clinical and survival outcomes of patients with early relapsed triple-negative breast cancer from the ESME national cohort. Eur J Cancer. 2023;189:112935. doi:10.1016/j.ejca.2023.05.023
6. Grinda T, Antoine A, Jacot W, et al. Evolution of overall survival and receipt of new therapies by subtype among 20 446 metastatic breast cancer patients in the 2008-2017 ESME cohort. ESMO Open. 2021;6(3):100114. doi:10.1016/j.esmoop.2021.100114
7. Schmid P, Cortes J, Dent R, et al. Overall survival with pembrolizumab in early-stage triple-negative breast cancer. N Engl J Med. 2024;391(21):1981–1991. doi:10.1056/NEJMoa2409932
8. Cortes J, Rugo HS, Cescon DW, et al. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N Engl J Med. 2022;387(3):217–226. doi:10.1056/NEJMoa2202809
9. Schmid P, Adams S, Rugo HS, et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379(22):2108–2121. doi:10.1056/NEJMoa1809615
10. Miles D, Gligorov J, André F, et al. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised Phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol. 2021;32(8):994–1004. doi:10.1016/j.annonc.2021.05.801
11. Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382(9):810–821. doi:10.1056/NEJMoa1910549
12. Nanda R, Liu MC, Yau C, et al. Effect of pembrolizumab plus neoadjuvant chemotherapy on pathologic complete response in women with early-stage breast cancer: an analysis of the ongoing phase 2 adaptively randomized I-SPY2 trial. JAMA Oncol. 2020;6(5):676–684. doi:10.1001/jamaoncol.2019.6650
13. Schmid P, Cortes J, Dent R, et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386(6):556–567. doi:10.1056/NEJMoa2112651
14. Schmid P, Cortés J, Dent R, et al. LBO1-01: neoadjuvant pembrolizumab or placebo plus chemotherapy followed by adjuvant pembrolizumab or placebo for early-stage triple-negative breast cancer: updated event-free survival results from the phase 3 KEYNOTE-522 study.
15. Dent R, Schmid P, Cortés J, et al. PS12-09: neoadjuvant pembrolizumab or placebo plus chemotherapy followed by adjuvant pembrolizumab or placebo for high-risk, early-stage triple-negative breast cancer: overall survival and subgroup results from the phase 3 KEYNOTE-522 study.
16. Mittendorf EA, Zhang H, Barrios CH, et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): a randomised, double-blind, phase 3 trial. Lancet. 2020;396(10257):1090–1100. doi:10.1016/S0140-6736(20)31953-X
17. Barrios C, Harbeck N, Zhang HA, et al. LBA1: final analysis of the placebo-controlled randomised phase III IMpassion031 trial evaluating neoadjuvant atezolizumab (atezo) plus chemotherapy (CT) followed by open-label adjuvant atezo in patients (pts) with early-stage triple-negative breast cancer (eTNBC. ESMO Open. 2023;8;1:101571.
18. Geyer CE, Tang G, Nekljudova V, et al. GS3-05: NSABP B-59/GBG-96-GeparDouze. A randomized double-blind phase III clinical trial of neoadjuvant chemotherapy with atezolizumab or placebo followed by adjuvant atezolizumab or placebo in patients with Stage II and III triple-negative breast cancer.
19. Chen L, Li H, Zhang H, et al. Camrelizumab vs placebo in combination with chemotherapy as neoadjuvant treatment in patients with early or locally advanced triple-negative breast cancer: the CamRelief randomized clinical trial. JAMA. 333(8):673–681. doi:10.1001/jama.2024.23560
20. Gianni L, Huang CS, Egle D, et al. Pathologic complete response (pCR) to neoadjuvant treatment with or without atezolizumab in triple-negative, early high-risk and locally advanced breast cancer: neoTRIP Michelangelo randomized study. Ann Oncol. 2022;33(5):534–543. doi:10.1016/j.annonc.2022.02.004
21. Gianni L, Huang C, Egle D, et al. LBA19: event-free survival (EFS) analysis of neoadjuvant taxane/carboplatin with or without atezolizumab followed by an adjuvant anthracycline regimen in high-risk triple negative breast cancer (TNBC): neoTRIP Michelangelo randomized study. Ann Oncol. 2023;34(suppl_2):S1254–S1335. doi:10.1016/annonc/annonc1358
22. Loibl S, Untch M, Burchardi N, et al. A randomised phase II study investigating durvalumab in addition to an anthracycline taxane-based neoadjuvant therapy in early triple-negative breast cancer: clinical results and biomarker analysis of GeparNuevo study. Ann Oncol. 2019;30(8):1279–1288. doi:10.1093/annonc/mdz158
23. Loibl S, Schneeweiss A, Huober J, et al. Neoadjuvant durvalumab improves survival in early triple-negative breast cancer independent of pathological complete response. Ann Oncol. 2022;33(11):1149–1158. doi:10.1016/j.annonc.2022.07.1940
24. Sharma P, Stecklein SR, Yoder R, et al. Clinical and biomarker findings of neoadjuvant pembrolizumab and carboplatin plus docetaxel in triple-negative breast cancer: neoPACT phase 2 clinical trial. JAMA Oncol. 2023;9(8):1083–1089. doi:10.1001/jamaoncol.2023.5033
25. Kolberg H-C, Schumacher J, Erber R. PS16-01: comparison of an Atezolizumab monotherapy window followed by Atezolizumab and chemotherapy vs. Atezolizumab and chemotherapy alone in triple negative breast cancer (TNBC) – final analysis of the neoadjuvant neoMono trial.
26. Zdenkowski N, Loi S, Niman S, et al. LBO-03: randomized phase II STUDY OF NEOADJUVANT NIVolumab (N) 2 week lead-in followed by 12 weeks of concurrent N+carboplatin plus paclitaxel (CbP) vs concurrent N+CbP in triple negative breast cancer (TNBC): (BCT1902/IBCSG 61-20 Neo-N).
27. Pusztai L, Yau C, Wolf DM, et al. Durvalumab with olaparib and paclitaxel for high-risk HER2-negative stage II/III breast cancer: results from the adaptively randomized I-SPY2 trial. Cancer Cell. 2021;39(7):989–998.e5. doi:10.1016/j.ccell.2021.05.009
28. Shatsky RA, Trivedi MS, Yau C, et al. Datopotamab-deruxtecan plus durvalumab in early-stage breast cancer: the sequential multiple assignment randomized I-SPY2.2 phase 2 trial. Nat Med. 2024;30:3737–3747. doi:10.1038/s41591-024-03267-1
29. Nederlof I, Isaeva OI, de Graaf M, et al. Neoadjuvant nivolumab or nivolumab plus ipilimumab in early-stage triple-negative breast cancer: a phase 2 adaptive trial. Nat Med. 2024;30(11):3223–3235. doi:10.1038/s41591-024-03249-3
30. Corti C, Binboğa Kurt B, Koca B, et al. Estrogen signaling in early-stage breast cancer: impact on neoadjuvant chemotherapy and immunotherapy. Cancer Treat Rev. 2024;132:102852. doi:10.1016/j.ctrv.2024.102852
31. Gianni L, Huang CS, Egle D, et al. Pathologic complete response (pCR) to neoadjuvant treatment with or without atezolizumab in triple-negative, early high-risk and locally advanced breast cancer: neoTRIP Michelangelo randomized study. Ann Oncol. 2022;33(5):534–543. doi:10.1016/j.annonc.2022.02.004
32. Corti C, Nicolò E, Curigliano G. Novel immune targets for the treatment of triple-negative breast cancer. Expert Opin Ther Targets. 2021;25(10):815–834. doi:10.1080/14728222.2021.2006187
33. Corti C, Berton Giachetti P, Eggermont A, et al. Therapeutic vaccines for breast cancer: has the time finally come? Eur J Canc. 2021. doi:10.1016/j.ejca.2021.10.027
34. Asad S, Barcenas CH, Bleicher RJ, et al. Sociodemographic factors associated with rapid relapse in triple-negative breast cancer: a multi-institution study. J Natl Compr Canc Netw. 2021;19(7):797–804. doi:10.6004/jnccn.2020.7659
35. Dent R, André F, Gonçalves A, et al. IMpassion132 double-blind randomised phase III trial of chemotherapy with or without atezolizumab for early relapsing unresectable locally advanced or metastatic triple-negative breast cancer. Ann Oncol. 2024;35(7):630–642. doi:10.1016/j.annonc.2024.04.001
36. Bardia A, Hurvitz SA, Tolaney SM, et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021;384(16):1529–1541. doi:10.1056/NEJMoa2028485
37. Bardia A, Rugo HS, Tolaney SM, et al. Final results from the randomized phase III ASCENT clinical trial in metastatic triple-negative breast cancer and association of outcomes by human epidermal growth factor receptor 2 and trophoblast cell surface antigen 2 expression. J Clin Oncol. 2024:JCO2301409. doi:10.1200/JCO.23.01409.
38. Michaels E, Chen N, Nanda R. The role of immunotherapy in triple-negative breast cancer (TNBC). Clin Breast Cancer. 2024;24(4):263–270. doi:10.1016/j.clbc.2024.03.001
39. Schmid P, Wysocki P, Park YH, et al. Abstract PD11-08: trastuzumab deruxtecan (T-DXd) + durvalumab (D) as first-line (1L) treatment for unresectable locally advanced/metastatic hormone receptor-negative (HR−), HER2-low breast cancer: updated results from BEGONIA, a phase 1b/2 study. Cancer Res. 2023;83(5_Supplement):851–65.
40. Corti C, Giugliano F, Nicolò E, et al. HER2-low breast cancer: a new subtype? Curr Treat Options Oncol. 2023;24(5):468–478. doi:10.1007/s11864-023-01068-1
41. Schmid P, Wysocki PJ, Ma CX, et al. 379MO: datopotamab deruxtecan (Dato-DXd) + durvalumab (D) as first-line (1L) treatment for unresectable locally advanced/metastatic triple-negative breast cancer (a/mTNBC): updated results from BEGONIA, a phase Ib/II study. Ann Oncol. 2023;34:S337. doi:10.1016/j.annonc.2023.09.556
42. Schmid P, Oliveira M, O’Shaughnessy J, et al. 261TiP: TROPION-Breast05: phase (Ph) III study of datopotamab deruxtecan (Dato-DXd) ± durvalumab (D) vs chemotherapy (CT) + pembrolizumab (pembro) in patients (pts) with PD-L1+ locally recurrent inoperable or metastatic triple-negative breast cancer (TNBC). ESMO Open. 2024:9. doi:10.1016/j.esmoop.2024.103282.
43. Tolaney SM, DeMichele A, Takano T, et al. OptimICE-RD: sacituzumab govitecan + pembrolizumab vs pembrolizumab (± capecitabine) for residual triple-negative breast cancer. Future Oncol. 2024;20(31):2343–2355. doi:10.1080/14796694.2024.2357534
44. Bardia A, Pusztai L, Albain K, et al. TROPION-Breast03: a randomized phase III global trial of datopotamab deruxtecan ± durvalumab in patients with triple-negative breast cancer and residual invasive disease at surgical resection after neoadjuvant therapy. Ther Adv Med Oncol. 2024;16:17588359241248336. doi:10.1177/17588359241248336
45. Domchek SM, Postel-Vinay S, Im SA, et al. Olaparib and durvalumab in patients with germline BRCA-mutated metastatic breast cancer (MEDIOLA): an open-label, multicentre, phase 1/2, basket study. Lancet Oncol. 2020;21(9):1155–1164. doi:10.1016/S1470-2045(20)30324-7
46. Vinayak S, Tolaney SM, Schwartzberg L, et al. Open-label clinical trial of niraparib combined with pembrolizumab for treatment of advanced or metastatic triple-negative breast cancer. JAMA Oncol. 2019;5(8):1132–1140. doi:10.1001/jamaoncol.2019.1029
47. Rugo H, Robson M, Im S-A, et al. Abstract GS01-05: pembrolizumab + olaparib vs pembrolizumab + chemotherapy after induction with pembrolizumab + chemotherapy for locally recurrent inoperable or metastatic TNBC: randomized open-label phase 2 KEYLYNK-009 study. Cancer Res. 2024;84(9_Supplement):GS01–05. doi:10.1158/1538-7445.sabcs23-gs01-05
48. Fanucci KA, Pilat MJ, Shyr D, et al. Abstract CT145: olaparib ± atezolizumab in patients with BRCA-mutated (BRCAmt) locally advanced unresectable or metastatic (advanced) breast cancer: an open-label, multicenter, randomized phase II trial. Cancer Res. 2023;83(8_Supplement):CT145. doi:10.1158/1538-7445.am2023-ct145
49. Gutierrez M, Spreafico A, Wang D, et al. Phase 1 first-in-human study of anti–ILT3 mAb MK-0482 as monotherapy and in combination with pembrolizumab in advanced solid tumors: dose escalation results. J Clin Oncol. 2022;40(16_suppl):2505. doi:10.1200/JCO.2022.40.16_suppl.2505
50. Santa-Maria CA, Kato T, Park JH, et al. A pilot study of durvalumab and tremelimumab and immunogenomic dynamics in metastatic breast cancer. Oncotarget. 2018;9(27):18985–18996. doi:10.18632/oncotarget.24867
51. Li Q, Liu J, Zhang Q, et al. The anti-PD-L1/CTLA-4 bispecific antibody KN046 in combination with nab-paclitaxel in first-line treatment of metastatic triple-negative breast cancer: a multicenter phase II trial. Nat Commun. 2024;15(1):1015. doi:10.1038/s41467-024-45160-y
52. Barroso-Sousa R, Li T, Reddy S, et al. Abstract GS2-10: nimbus: a phase 2 trial of nivolumab plus ipilimumab for patients with hypermutated her2-negative metastatic breast cancer (MBC). Cancer Res. 2022;82(4_Supplement):GS2–10. doi:10.1158/1538-7445.sabcs21-gs2-10
53. Adams S, Othus M, Patel SP, et al. A multicenter phase II trial of ipilimumab and nivolumab in unresectable or metastatic metaplastic breast cancer: cohort 36 of dual anti-CTLA-4 and anti-PD-1 blockade in rare tumors (DART, SWOG S1609). Clin Cancer Res. 2022;28(2):271–278. doi:10.1158/1078-0432.CCR-21-2182
54. Antonarelli G, Giugliano F, Corti C, et al. Research and clinical landscape of bispecific antibodies for the treatment of solid malignancies. Pharmaceuticals. 2021;14(9):884. doi:10.3390/ph14090884
55. Lin CC, Garralda E, Schöffski P, et al. A phase 2, multicenter, open-label study of anti-LAG-3 ieramilimab in combination with anti-PD-1 spartalizumab in patients with advanced solid malignancies. Oncoimmunology. 2024;13(1):2290787. doi:10.1080/2162402X.2023.2290787
56. Schöffski P, Tan DSW, Martín M, et al. Phase I/II study of the LAG-3 inhibitor ieramilimab (LAG525) ± anti-PD-1 spartalizumab (PDR001) in patients with advanced malignancies. J Immunother Cancer. 2022;10(2). doi:10.1136/jitc-2021-003776
57. Koni M, Castellano I, Venturelli E, et al. Interleukin-3-receptor-α in triple-negative breast cancer (TNBC): an additional novel biomarker of TNBC aggressiveness and a therapeutic target. Cancers. 2022;14(16):3918. doi:10.3390/cancers14163918
58. Miles DW, Diéras V, Cortés J, Duenne AA, Yi J, O’Shaughnessy J. First-line bevacizumab in combination with chemotherapy for HER2-negative metastatic breast cancer: pooled and subgroup analyses of data from 2447 patients. Ann Oncol. 2013;24(11):2773–2780. doi:10.1093/annonc/mdt276
59. Meder L, Schuldt P, Thelen M, et al. Combined VEGF and PD-L1 blockade displays synergistic treatment effects in an autochthonous mouse model of small cell lung cancer. Cancer Res. 2018;78(15):4270–4281. doi:10.1158/0008-5472.CAN-17-2176
60. Chen L, Jiang YZ, Wu SY, et al. Famitinib with camrelizumab and nab-paclitaxel for advanced immunomodulatory triple-negative breast cancer (FUTURE-C-Plus): an open-label, single-arm, phase II trial. Clin Cancer Res. 2022;28(13):2807–2817. doi:10.1158/1078-0432.CCR-21-4313
61. Gion M, Cortez-Castedo P, Blancas I, et al. Abstract PS16-02: efficacy and safety of first-line atezolizumab + bevacizumab + paclitaxel in patients with advanced triple-negative breast cancer: the ATRACTIB phase 2 trial. Cancer Res. 2024;84(9_Supplement):PS16–02. doi:10.1158/1538-7445.sabcs23-ps16-02
62. Fang W, Zhao Y, Luo Y, et al. Ivonescimab plus chemotherapy in non-small cell lung cancer with EGFR variant: a randomized clinical trial. JAMA. 2024;332(7):561–570. doi:10.1001/jama.2024.10613
63. Dhillon S. Ivonescimab: first approval. Drugs. 2024;84(9):1135–1142. doi:10.1007/s40265-024-02073-w
64. Ouyang Q, Wang X, Tian C, et al. The safety and efficacy of ivonescimab in combination with chemotherapy as first-line (1L) treatment for triple-negative breast cancer (TNBC). Ann Oncol. 2024;35:S360–S361. doi:10.1016/j.annonc.2024.08.295
65. Ouyang Q, Wang X, Tian C, et al. PS3-05: evaluation of the safety and efficacy of ivonescimab in Combination with chemotherapy as first-line treatment for TNBC.
66. Wu J, et al. 348MO: a phase Ib/II study to assess the safety and efficacy of PM8002/BNT327 in combination with nab-paclitaxel for first-line treatment of locally advanced or metastatic triple-negative breast cancer.
67. Wu J, Zhang J, Tong Z, et al. PS3-08: interim Overall Survival of Patients with Locally Advanced or Metastatic Triple-Negative Breast Cancer Treated with First-Line PM8002/BNT327 in Combination with Nab-Paclitaxel in a Phase Ib/II Study.
68. Zhang, et al. PS3-06: a prospective phase 2 study on efficacy and safety of AK105 (penpulimab), anlotinib combined with nab-paclitaxel (nab-P) as a first-line therapy in patients (pts) with advanced TNBC.
69. Crompton JG, Sukumar M, Roychoudhuri R, et al. Akt inhibition enhances expansion of potent tumor-specific lymphocytes with memory cell characteristics. Cancer Res. 2015;75(2):296–305. doi:10.1158/0008-5472.CAN-14-2277
70. Brufsky A, Kim SB, Zvirbule Ž, et al. A phase II randomized trial of cobimetinib plus chemotherapy, with or without atezolizumab, as first-line treatment for patients with locally advanced or metastatic triple-negative breast cancer (COLET): primary analysis. Ann Oncol. 2021;32(5):652–660. doi:10.1016/j.annonc.2021.01.065
71. Ignatidis M, Bailey A, McArthur HL, et al. GS01-03: adding atezolizumab to adjuvant chemotherapy for stage II and III triple-negative breast cancer is unlikely to improve efficacy: interim analysis of the ALEXANDRA/IMpassion030 phase 3 trial. Cancer Res. 2024;84(9_Supplement):GS01–03.
72. Litchfield K, Reading JL, Puttick C, et al. Meta-analysis of tumor- and T cell-intrinsic mechanisms of sensitization to checkpoint inhibition. Cell. 2021;184(3):596–614.e14. doi:10.1016/j.cell.2021.01.002
73. Versluis JM, Long GV, Blank CU. Learning from clinical trials of neoadjuvant checkpoint blockade. Nat Med. 2020;26(4):475–484. doi:10.1038/s41591-020-0829-0
74. Conte PF, Dieci MV, Bisagni G, et al. A-BRAVE trial: a phase III randomized trial with avelumab in early triple-negative breast cancer with residual disease after neoadjuvant chemotherapy or at high risk after primary surgery and adjuvant chemotherapy. J Clin Oncol. 2024;42(17_suppl):LBA500. doi:10.1200/JCO.2024.42.17_suppl.LBA500
75. Conte PF, Dieci MV, Bisagni G, et al. Is more better? Customizing systemic therapy for high-risk, nonmetastatic breast cancer.
76. Malli Cetinbas N, Monnell T, Soomer-James J, et al. Tumor cell-directed STING agonist antibody-drug conjugates induce type III interferons and anti-tumor innate immune responses. Nat Commun. 2024;15(1):5842. doi:10.1038/s41467-024-49932-4
77. McKenzie JA, Mbofung RM, Malu S, et al. The effect of topoisomerase I inhibitors on the efficacy of T-cell-based cancer immunotherapy. J Natl Cancer Inst. 2018;110(7):777–786. doi:10.1093/jnci/djx257
78. McArthur H, Tolaney S, Loibl S, et al. PO1-20-13: TROPION-Breast04: a phase 3 study of neoadjuvant datopotamab deruxtecan (Dato-DXd) + durvalumab followed by adjuvant durvalumab vs the standard of care in treatment-naive early-stage triple negative or HR-low/HER2– breast cancer. Cancer Res. 2024;84(9_Supplement):PO1–20–13. doi:10.1158/1538-7445.sabcs23-po1-20-13
79. Spring L, Tolaney SM, Desai NV, et al. Phase 2 study of response-guided neoadjuvant sacituzumab govitecan (IMMU-132) in patients with localized triple-negative breast cancer: results from the NeoSTAR trial. J Clin Oncol. 2022;40(16_suppl):512. doi:10.1200/JCO.2022.40.16_suppl.512
80. Caluwé A D, Desmoulins I, Cao K, et al. LBA10: primary endpoint results of the Neo-CheckRay phase II trial evaluating stereotactic body radiation therapy ± durvalumab ± oleclumab combined with neoadjuvant chemotherapy for early-stage, high risk ER+/HER2– breast cancer.
81. Isaacs C, Nanda R, Yau C, et al. GS5-03: Evaluation of Anti-PD-1 Cemiplimab Plus Anti-LAG-3 REGN3767 in Early-Stage, High-Risk HER2-Negative Breast Cancer: Results From the Neoadjuvant I-SPY 2 Trial. Presented at. SABCS.
82. Weber JS, Carlino MS, Khattak A, et al. Individualised neoantigen therapy mRNA-4157 (V940) plus pembrolizumab versus pembrolizumab monotherapy in resected melanoma (KEYNOTE-942): a randomised, phase 2b study. Lancet. 2024;403(10427):632–644. doi:10.1016/S0140-6736(23)02268-7
83. Hofherr M, Hedgecorth J, Ademuyiwa FO, et al. P3-06-06: real-world analysis of adverse events of patients with triple negative breast cancer receiving therapy per KEYNOTE-522.
84. Kabraji S, Solé X, Huang Y, et al. AKT1(low) quiescent cancer cells persist after neoadjuvant chemotherapy in triple negative breast cancer. Breast Cancer Res.;19(1):88. doi:10.1186/s13058-017-0877-7.
85. Criscitiello C, Corti C, Pravettoni G, Curigliano G. Managing side effects of immune checkpoint inhibitors in breast cancer. Crit Rev Oncol Hematol. 2021;162:103354. doi:10.1016/j.critrevonc.2021.103354
86. Wang XQ, Danenberg E, Huang CS, et al. Spatial predictors of immunotherapy response in triple-negative breast cancer. Nature. 2023;621(7980):868–876. doi:10.1038/s41586-023-06498-3
87. Dyikanov D, Zaitsev A, Vasileva T, et al. Comprehensive peripheral blood immunoprofiling reveals five immunotypes with immunotherapy response characteristics in patients with cancer. Cancer Cell. 2024;42(5):759–779.e12. doi:10.1016/j.ccell.2024.04.008
88. Martín M, Yoder R, Salgado R, et al. Tumor-infiltrating lymphocytes refine outcomes in triple-negative breast cancer treated with anthracycline-free neoadjuvant chemotherapy. Clin Cancer Res. 2024;30(10):2160–2169. doi:10.1158/1078-0432.CCR-24-0106
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.