Back to Journals » OncoTargets and Therapy » Volume 12
Recent advances and application of PD-1 blockade in sarcoma
Received 19 June 2019
Accepted for publication 31 July 2019
Published 23 August 2019 Volume 2019:12 Pages 6887—6896
DOI https://doi.org/10.2147/OTT.S220045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Wenli Zuo, Lingdi Zhao
Hematology Department, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, Zhengzhou City 450008, People’s Republic of China
Correspondence: Lingdi Zhao
Hematology Department, The Affiliated Cancer Hospital of Zhengzhou University & Henan Cancer Hospital, No. 127 Dongming Road, Jinshui District, Zhengzhou City 450008, People’s Republic of China
Email [email protected]
Abstract: The role of the programmed death-1 (PD-1) signaling pathway in tumor immunotherapy is becoming increasingly important, and several PD-1-blocking agents have been approved by the US Food and Drug Administration. PD-1-blocking therapy alone or in combination with other therapeutic modalities has become a standard treatment for several kinds of solid tumors. However, sarcomas are not indications for anti-PD-1 therapy. Sarcomas are a group of heterogeneous diseases that can currently only be cured by surgery at the early stage. No effective treatments exist for sarcoma patients in advanced stages. Owning to the diversity of sarcomas, it is very difficult to conduct randomized controlled clinical studies on specific subtypes of sarcomas. Although clinical studies of sarcomas continue, few breakthroughs in the treatment of sarcomas have been achieved over the past decades. This review summarizes recent progress in anti-PD-1 therapy for sarcomas. Based on the published data, PD-1 blockade may be more effective in combination with other modalities for the treatment of sarcomas. In addition, biomarkers may be used to ascertain sensitivity to PD-1 blockade in sarcoma patients.
Keywords: PD-1 blockade, immunotherapy, sarcoma
Introduction
Sarcomas are a heterogeneous group of malignancies derived from mesenchymal tissue and also can arise anywhere of the body with considerably different clinical and pathological features. These malignancies are broadly classified as soft tissue sarcomas (STS) or bone sarcomas and account for about 1% of all malignancies in adults and 15% in children; sarcoma is the third leading cause of cancer-related death among children and adolescents.1 Surgical resection en bloc is the mainstay treatment for primary-localized diseases, and the 5-year recurrence-free survival rate is about 60%.2 In patients with distant metastasis, the 5-year survival rate is below 20%.3 Therefore, new treatment options for recurrent/metastatic sarcoma are urgently needed.
Immunological checkpoint inhibitors represented by anti-programmed death-1 (PD-1)/programmed death ligand-1 (PD-L1) monoclonal antibodies (MoAb) have shown promising clinical efficacy for various malignancies and predicted the age of cancer immunotherapy. However, the rarity of sarcomas and variances in the disease, with over 50 histological subtypes, limit the performance of randomized controlled clinical studies. Therefore, data related to PD-1 blockade for the treatment of sarcomas are lacking. Herein, we summarized the latest advancements in the treatment of sarcomas with PD-1 blockade and the possible biomarkers that might predict the efficacy of anti-PD-1 therapy for sarcomas.
PD-1 blockade in recurrent/metastatic sarcoma
Nivolumab is an anti-PD-1 fully human immunoglobulin (Ig)G4 MoAb that has shown broad antitumor activity by binding with PD-1 specifically.4–7 A retrospective study of 10 patients with advanced sarcoma who were treated with nivolumab alone showed that partial remission was achieved in one patient, and stable disease was achieved in four patients; however, progressive disease was observed in five patients.7 Thereafter, studies on PD-1 blockade and sarcomas were reported sporadically.8–11 Alliance A091401 is a prospective study comparing the clinical efficacy of nivolumab alone or in combination with ipilimumab in patients with metastatic sarcomas. Of the 76 eligible patients (38 patients in each group), a confirmed response was achieved in two patients in the nivolumab group and six in the nivolumab plus ipilimumab group. In the nivolumab group, 29 patients had progressive disease at the first evaluation, of whom 18 were eligible for continuing nivolumab treatment. Eleven of these 18 patients were confirmed to have progressive disease after 1 month of treatment, and 7 continued nivolumab therapy for 2–8.5 months. In the nivolumab plus ipilimumab group, 18 patients had progressive disease at the first evaluation, of whom 8 were eligible for continuing combination therapy. Three of the eight patients had progressive disease at the time of confirmation, and the other five patients had a stable disease at the time of confirmation and continued to receive combined therapy for another 3–12 months. Interestingly, one patient receiving combined therapy exhibited a partial response within 3 months of initial progressive disease, which is in accordance with so-called pseudo-progression.12 The median progression-free survival (PFS) was 4.1 months and the median OS was 14.3 months, as to the patients received combination therapy, the 12-month OS rate was 54.6%. Of course, the occurrence of grade 3–4 treatment-related adverse events was higher in patients received combination therapy (14% vs 7%).12 This study indicated that the efficacy of nivolumab alone in patients with unselected sarcomas is limited but might be improved by other immunomodulatory agents. The Phase 2 study of nivolumab in patients with uterine leiomyosarcoma likewise demonstrated the limited efficacy of nivolumab monotherapy; no confirmed response was observed in the 12 patients enrolled in this study.4 However, this study indicated that the histopathological type might be a factor influencing the efficacy of PD-1 blockade, and therefore it is necessary to verify the efficacy of PD-1 blockade in different histopathological subgroups.
Pembrolizumab, another anti-PD-1 humanized IgG4 MoAb, displays antitumor activity in many kinds of solid tumors, including sarcomas.9,10,13–15 SARC028 is a multicenter Phase 2 study designed to estimate the clinical efficacy of pembrolizumab in patients with advanced sarcomas. During the 80 patients eligible for efficacy evaluation, 18% (7/40) of 40 patients with STS displayed an objective response, including 4 of 10 patients with undifferentiated pleomorphic sarcoma (UPS), 2 of 10 patients with liposarcoma, and 1 of 10 patients with synovial sarcoma. No patients with leiomyosarcoma had an objective response. Five percent (2/40) of patients with bone sarcoma had an objective response, including 1 of 22 patients with osteosarcoma and 1 of 5 patients with chondrosarcoma; none of the 13 patients with Ewing’s sarcoma had an objective response. The median PFS was 18 weeks in patients with STS and 8 weeks in patients with bone sarcomas, and severe adverse events occurred in 11% of the patients.13 The results of SARC028 demonstrated promising activity in UPS, suggesting that patients with this subtype of sarcoma might benefit more from pembrolizumab. For patients with other subtypes of sarcomas, the better choice might be PD-1 blockade-combined regimen.
PD-1 blockade in adjuvant or neoadjuvant therapy for sarcoma
Localized sarcomas are primarily managed with surgical resection. For patients with large and/or high-grade sarcomas, neoadjuvant and/or adjuvant therapies are often used to improve local control rates. As the results of PD-1 blockade monotherapy for patients with metastatic sarcomas are unsatisfactory, the combination of PD-1 blockade and other treatment modes has been explored. Radiotherapy is an effective local treatment and can upregulate PD-L1 expression in primary tumors.16–18 Patel et al, examined the expression of PD-L1 in tumor tissue from 46 patients with stage Ⅱ–Ⅲ STS before and after radiotherapy. No PD-L1 expression on tumor cells was observed in any patients before radiotherapy; however, PD-L1 expression on tumor cells was observed in five patients after radiotherapy.18 Moreover, the expression of PD-L1 on tumor-associated macrophages (TAMs) is also increased after radiotherapy, suggesting an increased risk of distant metastasis after surgery.18 This provides a rationale for perioperative PD-L1 blockade plus radiotherapy.
NCT03474094 is a multicenter, randomized Phase 2 study evaluating the sequence of radiotherapy and PD-L1 blockade in the perioperative period in patients with operable localized STS. The patients enrolled in this study will be allocated into three groups: the treatment sequence in group A includes radiotherapy followed by atezolizumab (an anti-PD-L1 antibody) therapy and operation; the treatment sequence in group B includes atezolizumab therapy followed by operation and radiotherapy; the treatment sequence in group C includes operation followed by atezolizumab therapy and radiotherapy. The primary endpoint is the influence of atezolizumab with or without radiotherapy on the pathological response in patients with STS, and the study is anticipated to be completed in 2021. Furthermore, CT03338959 is a Phase 1/2 study performed in patients with intermediate- or high-grade STS. The patients enrolled in this study will receive pembrolizumab plus radiation followed by surgery. The primary endpoint of this study is pathological response.
Based on the results of SARC028, MD Anderson Cancer Center sponsored a Phase 2 study (NCT03307616), which is an investigational study to determine whether nivolumab alone or in combination with ipilimumab before operation is effective for patients with surgically resectable UPS and dedifferentiated liposarcoma. Similar to NCT03307616, NCT03116529 is a Phase 1/2 study conducted in patients with high-risk STS and the purpose is to estimate the efficacy of radiotherapy plus duvalumab and tremelimumab before operation. The primary endpoints of NCT03116529 are safety and pathological responses. In addition, NCT03463408 is an early Phase 1 study in patients with resectable STS, the patients will be allocated to either of the two arms: the patients in arm 1 receive nivolumab and ipilimumab plus radiation before surgery, whereas the patients in arm 2 receive surgery without neoadjuvant or adjuvant therapy. The primary endpoint is safety. These clinical trials are currently recruiting patients.
PD-1 blockade combined with other agents for the treatment of sarcoma
It was reported that the expression of PD-L1 is high and associated with poor prognosis in sarcoma patients.19–21 The expression of PD-L1 provides a potential therapeutic target for anti-PD-1 treatment of sarcomas. However, the expression of PD-L1 is dynamic and could be induced by many factors in the tumor microenvironment.22–24 PD-1 blockade alone is not effective enough in unselected sarcoma patients; thus, PD-1 blockade may be combined with other therapeutic agents.4,12
PD-1 blockade combined with radiotherapy
Preclinical animal studies have shown that immunological checkpoint inhibitor therapy combined with fractionated radiotherapy could induce the abscopal effect.25 Fractionated radiotherapy could enhance T cell trafficking into locally treated tumor sites and augment preexisting antitumor T cell responses, with the capacity to mediate regression of out-of-field tumor lesions when performed in combination with PD-1 blockade agents.26 PD-L1 expression in tumor tissue could be upregulated after radiotherapy.16–18 In UPS of the extremity and trunk (ET-UPS), infiltrating immune cells increase in the tumor microenvironment, and PD-L1 expression on tumor cells is upregulated after radiotherapy.18,27 This evidence provides a theoretical basis for PD-1 blockade plus radiotherapy. A case report showed remarkable tumor regression after combined nivolumab and radiation therapy in a patient with metastatic mediastinal leiomyosarcoma.28 PD-1 blockade combined with radiotherapy for localized sarcoma is discussed above in the “PD-1 blockade in adjuvant or neoadjuvant therapy for sarcoma” section. The NCT03548428 study was initiated to evaluate the efficacy of atezolizumab plus stereotactic body radiation therapy in sarcoma patients with oligometastases; the primary endpoint of this study is the PFS rate at 6 months. At present, the study has not begun to recruit patients.
PD-1 blockade combined with chemotherapy
Chemotherapy has immunomodulatory functions, which in turn enhance antitumor effects by several mechanisms. Firstly, cancer cell death caused by chemotherapy leads to the release of tumor-specific antigens, which are taken up by antigen-presenting cells. These cells present the antigens to T cells to allow for priming and activating of T cells.29 Secondly, chemotherapy might play several immune-potentiating roles including reduction of regulatory T cell (Treg) activity, selective depletion of myeloid-derived suppressor cells (MDSCs), induction of PD-L1 expression, and maturation of antigen-presenting cells.30,31 These findings form the rationale for the combination of PD-1 blockade and chemotherapy, which has demonstrated synergistic effects on advanced non-small cell lung cancer and nasopharyngeal cancer.14,32 Moreover, both immunological checkpoint inhibitors and metronomic chemotherapy have the potentiation to activate immune cells, and a preclinical study confirmed their synergy.33
NCT02406781 is a multicenter Phase 2 trial conducted to estimate the efficacy of pembrolizumab plus metronomic cyclophosphamide. Fifty-seven patients with advanced sarcomas enrolled in this study, 50 of which the efficacy could be evaluated. The four subtypes of sarcomas included in this study were leiomyosarcoma, UPS, other types of sarcoma, and gastrointestinal stromal tumor (GIST). Partial remission was achieved in three of the 50 patients. The PFS rates at 6 months in the four subtype groups were 0%, 0%, 14.3%, and 11.1%, respectively. The researchers of this study considered that the tumor microenvironment characterized by infiltration of macrophages might restrict the efficacy of treatment, based on analysis of biomarker expression in the tumor tissue.34 Although the clinical efficacy of this study was not remarkable, the analysis of molecular biomarkers revealed that the infiltrating macrophages expressing inhibitory enzyme indoleamine 2, 3-dioxygenase 1 (IDO1) may be related to poor clinical efficacy; thus, combination therapy with IDO inhibitors might improve the clinical efficacy.34 Clinical studies of PD-1 blockade combined with chemotherapy for the treatment of sarcomas registered on clinicaltrials.gov are listed in Table 1.
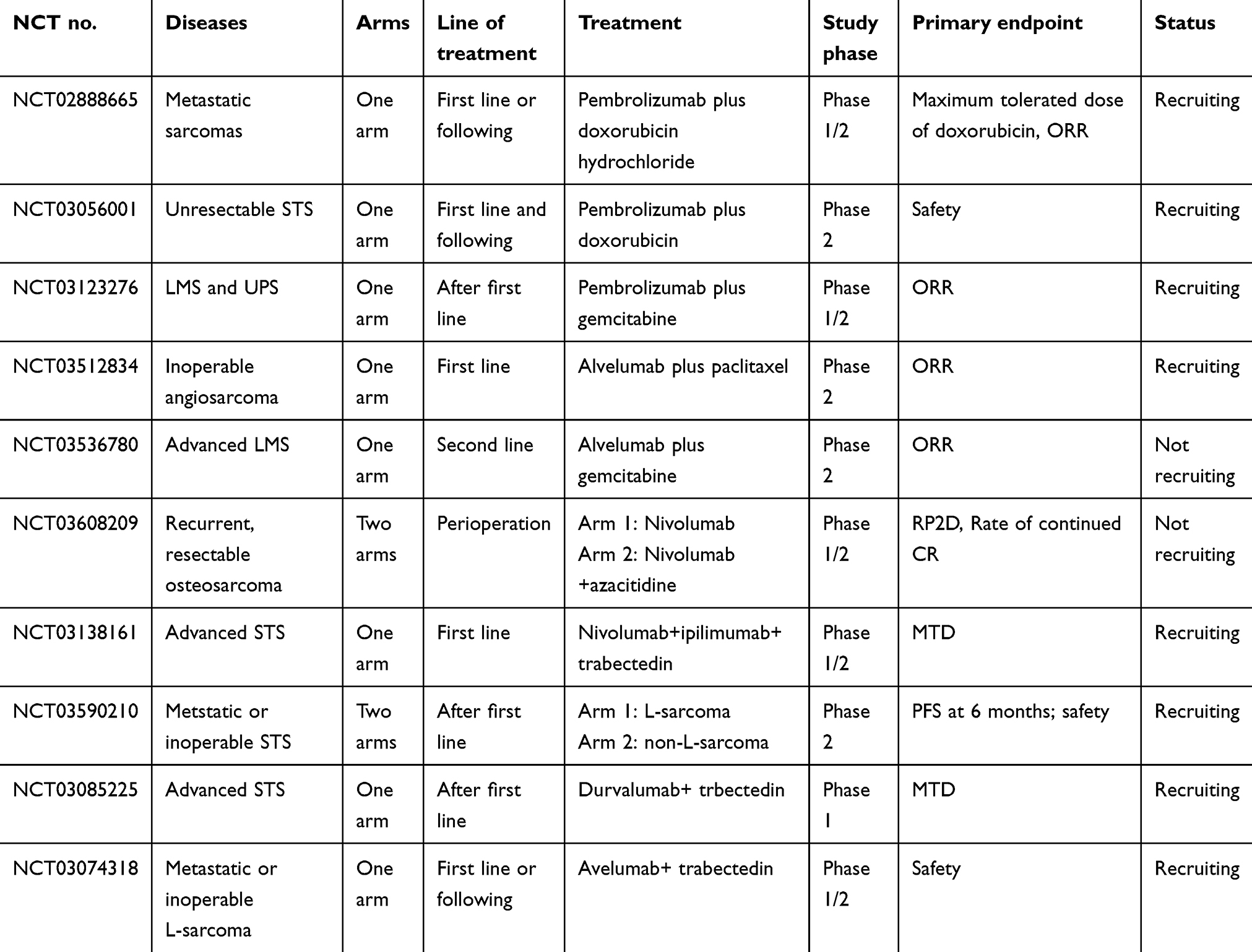 |
Table 1 Clinical studies registered on clinical trials of PD-1 blockade combined with chemotherapy in sarcomas |
PD-1 blockade combined with targeted agents
Angiogenesis plays a central role in tumor growth and metastasis. Vascular endothelial growth factor (VEGF), an endothelial cell-specific mitogen found both in normal and tumor tissues, promotes new blood vessels formation by regulating (or dysregulating) angiogenesis.35 VEGF regulates the tumor microenvironment by several ways, such as activation of the hypoxia-mediated signal pathway; direct impairment of the antigen presentation mechanism; and binding with VEGF receptor (VEGFR) on MDSCs, Tregs, TAMs, and cytotoxic T lymphocytes, all of which support the formation of the immunosuppressive tumor microenvironment.22,36 Blocking the VEGF/VEGFR signaling pathway could interrupt neovascularization and exert antitumor effects. The synergistic effect of PD-1 blockade and anti-angiogenesis has been demonstrated in lung cancer, hepatocellular carcinoma, and renal cancer.15,37,38
Pazopanib is an oral multi-target tyrosine kinase inhibitor targeting VEGFR1–3 and platelet-derived growth factor receptor (PDGFR)1–3. In a retrospective study of pazopanib combined with nivolumab in 14 patients with advanced sarcomas, partial response was achieved in two patients, stable disease was observed in five patients, and seven patients were diagnosed with progressive disease. Grade 3/4 adverse events occurred in five patients, including one case of diarrhea, one case of pneumonitis, and three cases of liver function tests. Nonetheless, this combined regimen was tolerated well, with no treatment-related death.7
Apatinib is an oral small-molecule VEGFR2 inhibitor that has shown antitumor activity in many kinds of tumors including gastric cancer, melanoma, lung cancer, breast cancer, and STS.39–41 PD-1 blockade plus apatinib has demonstrated promising activity in hepatocellular carcinoma and gastric or esophagogastric junction cancer.42 Two Phase 2 clinical studies to assess the activity of PD-1 blockade plus apatinib in sarcomas are underway. NCT03359018 is a trial designed to estimate the efficacy of SHR-1210 (an anti-PD-1 antibody) plus apatinib in 43 enrolled patients with advanced osteosarcoma. The primary endpoint is PFS and overall survival. The recruitment ended and results are pending. NCT03711279 is a multicenter, randomized, open Phase 2 study that is designed to compare the clinical efficacy of SHR-1210 plus apatinib with chemotherapy (doxorubicin combined with ifosfamide or doxorubicin alone) in advanced STS. This study is currently recruiting patients.
Axitinib is an orally administered potent and selective inhibitor of VEGFR1–3 that has been demonstrated to have good clinical efficacy alone or in combination with pembrolizumab in advanced renal cell cancer.15,43 NCT02636725 is an open-label Phase 2 study of pembrolizumab plus axitinib in patients with advanced alveolar STS and other STS. The primary endpoint of this study is the PFS rate at 3 months. The midterm results of this study were reported at the 2018 American Society of Clinical Oncology meeting. Thirty-three patients received at least one dose of study drugs, with 30 patients eligible for evaluation at the primary endpoint. The median PFS was 5.4 months, and the best objective response rate was 21.9%. In patients with alveolar soft part sarcoma, the PFS rate at 3 months was 90.9%, and the best objective response rate was 45.5%. This combination treatment is tolerated well with promising activity in alveolar STS.44 One study revealed the deletion mutation of a mismatch repair (MMR) gene that might be one cause of the good clinical efficacy of PD-1 blockade in alveolar soft part sarcoma.45
Sunitinib is a highly potent selective inhibitor of certain protein tyrosine kinases, including VEGFR1–3, PDGFRα, and PDGFRβ. Clinical data demonstrated the antitumor activity of sunitinib in renal cell cancer, hepatocellular carcinoma, and GIST.46–48 NCT03277924 is a Phase 1/2 study in which the antitumor activity of nivolumab plus sunitinib in patients with advanced sarcomas after the failure of first-line therapy will be estimated; the primary endpoint of this study is the PFS rate at 6 months. Olaratumab is a recombinant human IgG1 MoAb that specifically binds with PDGFRα and has demonstrated antitumor activity in STS.49 NCT03126591 is a Phase 1 study that aims to evaluate the safety of olaratumab plus pembrolizumab in patients with previously treated advanced STS. This study is now recruiting participants.
PD-1 blockade combined with other immunomodulatory agents
PD-1 blockade has shown substantial clinical antitumor activity.7,32,37,38,42,45 As immunological checkpoints are non-redundant and could inhibit T cell activation, proliferation, and effector function within lymph nodes and/or the tumor microenvironment, PD-1 signal pathway blockade combined with other immunomodulatory agents might produce greater antitumor activity than PD-1 blockade alone.50 PD-1 blockade combined with CTLA-4 blockade has shown better clinical efficacy than when used alone in melanoma, lung cancer, renal cell cancer, and sarcoma.5,6,12,51 Clinical studies of PD-1 blockade combined with other immunomodulatory agents registered on the clinicaltrials.gov are listed in Table 2.
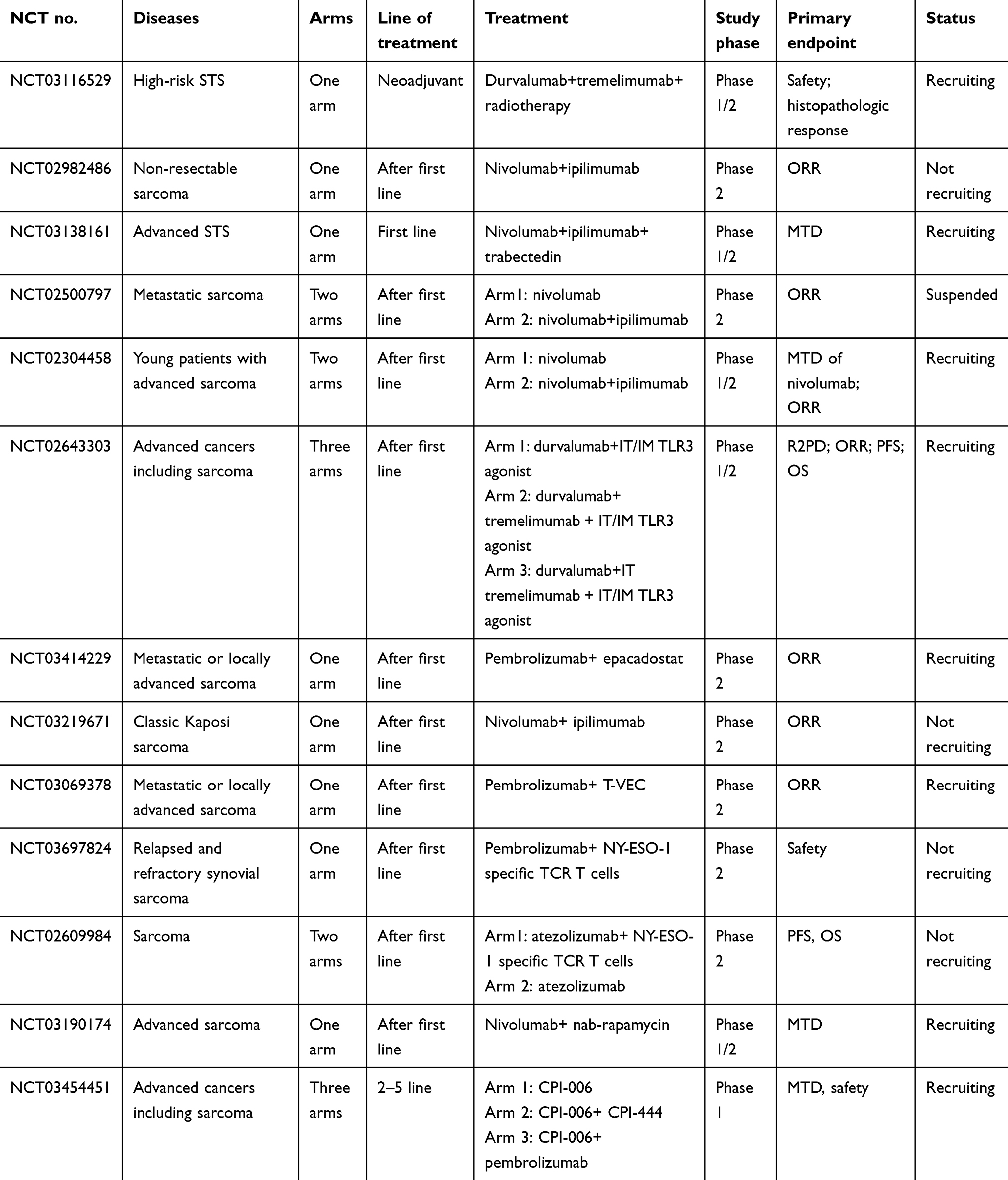 |
Table 2 Clinical studies registered on clinical trials of PD-1 blockade combined with other immunomodulatory agents in sarcomas |
Factors influencing the efficacy of PD-1 blockade in sarcoma
Tumor cells can utilize immunosuppressive factors in the tumor microenvironment, including immune checkpoint molecules, cytokines, and immunosuppressive cells, to escape immune surveillance. The incidences of angiosarcoma and Kaposi sarcoma are high in patients with human immunodeficiency virus infection and those receiving transplantation. Expression of tumor-associated antigens and the initiation of the immune system are also observed in sarcomas. The response to PD-1 blockade depends on the interaction between immune cells and tumor cells in the tumor microenvironment. Currently, the detection of PD-L1 expression by immunohistochemistry is widely used in clinic to predict the efficacy of PD-1 blockade.52 According to PD-L1 expression, the tumor microenvironment is categorized into four distinct types: type I represents tumors without expression of PD-L1 on tumor cells and with tumor-infiltrating lymphocytes (TILs) in the tumor tissue; type II represents tumors with both PD-L1 expression on tumor cells and TILs in the tumor tissue; type III represents tumors with TILs but no expression of PD-L1 on tumor cells; type IV represents tumors with PD-L1 expression on tumor cells and without TILs in the tumor tissue.53 In STS, intratumor infiltration of PD-1-positive lymphocytes and PD-L1 expression was observed in 65% and 58% of the cases, respectively, and multivariate analysis indicated that both PD-1 positivity and PD-L1 positivity were independent prognostic indicators of overall survival and event-free survival.23 Approximately 50% of the sarcomas, notably leiomyosarcomas, chondrosarcomas, liposarcomas, and UPS, expressed PD-L1 based on immunohistochemistry and presented PD-1+ TILs.54 These results suggested that sarcomas may be an indication of PD-1 blockade therapy; however, PD-1 blockade alone did not show promising efficacy clinically.4,12
The expression of PD-L1 is not limited to tumor cells; PD-L1 expression is observed on TAMs, Tregs, and MDSCs in the tumor microenvironment. Noguchi et al, confirmed that PD-L1 expression on tumor cells plays an important role in promoting tumor immune escape.24 Induction of PD-L1 on tumor cells was interferon gamma-dependent and transient, whereas induction of PD-L1 on TAMs was of greater magnitude, only partially interferon gamma-dependent, and stable over time. PD-L1 expression on either tumor cells or host immune cells could lead to tumor escape from the immune system, indicating that total PD-L1 expression in the tumor microenvironment may represent a more accurate biomarker for predicting response to PD-1/PD-L1 blockade therapy, compared with PD-L1 expression on tumor cells alone.24
Tumor mutation burden (TMB) is an emerging biomarker for PD-1 blockade therapy. High TMB predicts a better response to PD-1 blockade55,56 and may induce the formation of tumor-specific neoantigens, which could trigger a more robust immune response driven by TILs.56 One study reported a favorable response to pembrolizumab in one patient with classic Kaposi sarcoma with high TMB.57 More studies on TMB and the efficacy of PD-1 blockade in sarcomas are needed.
Microsatellite instability (MSI) is known as a condition of genetic hypermutability resulting from impaired DNA MMR. The presence of MSI indicates that the MMR function is abnormal. High MSI and deletion mutation of MMR genes are present in a subset of tumors and appear to be biomarkers that predict response to PD-1 blockade therapy.58 In pleomorphic rhabdomyosarcoma and alveolar soft part sarcoma, patients with MSI-high tumors could benefit from PD-1 blockade therapy.45,59 In addition, it was reported that deletion mutation of MMR genes correlates with PD-L1 overexpression.59
Conclusion
Sarcomas are uncommon tumors. Currently, no effective systemic therapeutic modality for patients with advanced sarcomas exists, and the prognosis remains very poor. The advent of PD-1-blocking agents changed the treatment modality for many types of solid tumors, in which they show satisfactory efficacy. However, data corresponding to sarcomas, especially from randomized clinical studies of PD-1 blockade, are rare, and no results of randomized Phase 3 studies of PD-1 blockade in sarcomas are available. Sarcomas represent a large group of heterogeneous diseases including more than 50 subtypes, and the tumor microenvironment is highly complicated. PD-1 blockade monotherapy cannot achieve satisfactory efficacy according to the available data. As research on the sarcomas microenvironment proceeds, it may be possible to identify patients who are sensitive to PD-1 blockade by examination of PD-L1 expression, TMB, and MSI. For unselected sarcoma patients, PD-1 blockade combined with other types of treatment, such as localized radiation, tumor injection with cytokines or oncolytic viruses, and treatment with other types of immunomodulatory agents, may provide better results.
Abbreviations
PD-1, programmed death protein 1; Ig, immunoglobulin; MoAb, onoclonal antibody; STS, soft tissue sarcoma; UPS, undifferentiated pleomorphic sarcoma; PFS, progression-free survival; SAE, severe adverse events; PD-L1, programmed death protein ligand 1; TAM, tumor-associated macrophage; SBRT, stereotactic body radiotherapy; VEGF, vascular endothelial growth factor; VEGFR, vascular endothelial growth factor receptor; MDSCs, myeloid-derived suppressor cells; Tregs, regulatory T cells; CTL, cytotoxic T lymphocyte; PDGFR, platelet-derived growth factor receptor; TMB tumor mutation burden; TIL, tumor-infiltrating lymphocyte; MSI, microsatellite instability; MMR, mismatch repair.
Acknowledgment
We would like to give our thanks to www.editage.cn for the language editing. This study was funded by Industry-University-Research Collaboration of Health Commission of Henan Province (No. 182107000027).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442
2. Brennan MF, Antonescu CR, Moraco N, Singer S. Lessons learned from the study of 10,000 patients with soft tissue sarcoma. Ann Surg. 2014;260(3):416–421. doi:10.1097/SLA.0000000000000869
3. Gelderblom H, Blay JY, Seddon BM, et al. Brostallicin versus doxorubicin as first-line chemotherapy in patients with advanced or metastatic soft tissue sarcoma: an European organisation for research and treatment of cancer soft tissue and bone sarcoma group randomised phase II and pharmacogenetic study. Eur J Cancer. 2014;50(2):388–396. doi:10.1016/j.ejca.2013.10.002
4. Ben-Ami E, Barysauskas CM, Solomon S, et al. Immunotherapy with single agent nivolumab for advanced leiomyosarcoma of the uterus: results of a phase 2 study. Cancer. 2017;123(17):3285–3290. doi:10.1002/cncr.30738
5. Hellmann MD, Rizvi NA, Goldman JW, et al. Nivolumab plus ipilimumab as first-line treatment for advanced non-small-cell lung cancer (CheckMate 012): results of an open-label, phase 1, multicohort study. Lancet Oncol. 2017;18(1):31–41. doi:10.1016/S1470-2045(16)30624-6
6. Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277–1290. doi:10.1056/NEJMoa1712126
7. Paoluzzi L, Cacavio A, Ghesani M, et al. Response to anti-PD1 therapy with nivolumab in metastatic sarcomas. Clin Sarcoma Res. 2016;6:24. doi:10.1186/s13569-016-0064-0
8. Sindhu S, Gimber LH, Cranmer L, et al. Angiosarcoma treated successfully with anti-PD-1 therapy - a case report. J Immunother Cancer. 2017;5(1):58. doi:10.1186/s40425-017-0263-0
9. Marcrom S, De Los Santos JF, Conry RM. Complete response of mediastinal clear cell sarcoma to pembrolizumab with radiotherapy. Clin Sarcoma Res. 2017;7:14. doi:10.1186/s13569-017-0079-1
10. Song HN, Kang MG, Park JR, et al. Pembrolizumab for refractory metastatic myxofibrosarcoma: a case report. Cancer Res Treat. 2018;50(4):1458–1461. doi:10.4143/crt.2017.529
11. Delyon J, Bizot A, Battistella M, Madelaine I, Vercellino L, Lebbé C. PD-1 blockade with nivolumab in endemic kaposi sarcoma. Ann Oncol. 2018;29(4):1067–1069. doi:10.1093/annonc/mdy006
12. D’Angelo SP, Mahoney MR, Van Tine BA, et al. Nivolumab with or without ipilimumab treatment for metastatic sarcoma (Alliance A091401): two open-label, non-comparative, randomised, phase 2 trials. Lancet Oncol. 2018;19(3):416–426. doi:10.1016/S1470-2045(18)30006-8
13. Tawbi HA, Burgess M, Bolejack V, et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): a multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017;18(11):1493–1501. doi:10.1016/S1470-2045(17)30624-1
14. Langer CJ, Gadgeet SM, Borghaei H, et al. Carboplatin and pemetrexed with or without pembrolizumab for advanced, non-squamous non-small-cell lung cancer: a randomised, phase 2 cohort of the open-label KEYNOTE-021 study. Lancet Oncol. 2016;17(11):1497–1508. doi:10.1016/S1470-2045(16)30498-3
15. Atkins MB, Plimack ER, Puzanov I, et al. Axitinib in combination with pembrolizumab in patients with advanced renal cell cancer: a non-randomised, open-label, dose-finding, and dose-expansion phase 1b trial. Lancet Oncol. 2018;19(3):405–415. doi:10.1016/S1470-2045(18)30081-0
16. Deng L, Liang H, Burnette B, et al. Irradiation and anti-PD-L1 treatment synergistically promote antitumor immunity in mice. J Clin Invest. 2014;124(2):687–695. doi:10.1172/JCI67313
17. Song X, Shao Y, Jiang T, et al. Radiotherapy upregulates programmed death ligand-1 through the pathways downstream of epidermal growth factor receptor in glioma. EBioMedicine. 2018;28:105–113. doi:10.1016/j.ebiom.2018.01.027
18. Patel KR, Martinez A, Stahl JM, et al. Increase in PD-L1 expression after pre-operative radiotherapy for soft tissue sarcoma. Oncoimmunology. 2018;7(7):e1442168. doi:10.1080/2162402X.2018.1490854
19. D’Angelo SP, Shoushtari AN, Agaram NP, et al. Prevalence of tumor-infiltrating lymphocytes and PD-L1 expression in the soft tissue sarcoma microenvironment. Hum Pathol. 2015;46(3):357–365. doi:10.1016/j.humpath.2014.11.001
20. Kim C, Kim EK, Jung H, et al. Prognostic implications of PD-L1 expression in patients with soft tissue sarcoma. BMC Cancer. 2016;16:434. doi:10.1186/s12885-016-2451-6
21. Boxberg M, Steiger K, Lenze U, et al. PD-L1 and PD-1 and characterization of tumor-infiltrating lymph.ocytes in high grade sarcomas of soft tissue - prognostic implications and rationale for immunotherapy. Oncoimmunology. 2018;7(3):e1389366. doi:10.1080/2162402X.2018.1490854
22. D’Ignazio L, Batie M, Rocha S. Hypoxia and inflammation in cancer, focus on HIF and NF-kappaB. Biomedicines. 2017;5(2). pii: E21. doi:10.3390/biomedicines5020021.
23. Kim JR, Moon YJ, Kwon KS, et al. Tumor infiltrating PD1-positive lymphocytes and the expression of PD-L1 predict poor prognosis of soft tissue sarcomas. PLoS One. 2013;8(12):e82870. doi:10.1371/journal.pone.0082870
24. Noguchi T, Ward JP, Gubin MM, et al. Temporally distinct PD-L1 expression by tumor and host cells contributes to immune escape. Cancer Immunol Res. 2017;5(2):106–117. doi:10.1158/2326-6066.CIR-16-0391
25. Dewan MZ, Galloway AE, Kawashima N, et al. Fractionated but not single-dose radiotherapy induces an immune-mediated abscopal effect when combined with anti-CTLA-4 antibody. Clin Cancer Res. 2009;15(17):5379–5388. doi:10.1158/1078-0432.CCR-09-0265
26. Dovedi SJ, Cheadle EJ, Popple AL, et al. Fractionated radiation therapy stimulates antitumor immunity mediated by both resident and infiltrating polyclonal T-cell populations when combined with PD-1 blockade. Clin Cancer Res. 2017;23(18):5514–5526. doi:10.1158/1078-0432.CCR-16-1673
27. Keung EZ, Tsai JW, Ali AM, et al. Analysis of the immune infiltrate in undifferentiated pleomorphic sarcoma of the extremity and trunk in response to radiotherapy: rationale for combination neoadjuvant immune checkpoint inhibition and radiotherapy. Oncoimmunology. 2018;7(2):e1385689. doi:10.1080/2162402X.2018.1490854
28. Xi C, Wencheng Z, Dong Q, et al. Tumor regression after combination of radiation and PD-1 antibody nivolumab treatment in a patient with metastatic mediastinal leiomyosarcoma: a case report. Cancer Biol Ther. 2019;20(4):408–412. doi:10.1080/15384047. 2018.1537577.
29. Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39(1):1–10. doi:10.1016/j.immuni.2013.07.012
30. Apetoh L, Ladoire S, Coukos G, Ghiringhelli F. Combining immunotherapy and anticancer agents: the right path to achieve cancer cure? Ann Oncol. 2015;26(9):1813–1823. doi:10.1093/annonc/mdv209
31. Qiao M, Jiang T, Ren S, Zhou C. Combination strategies on the basis of immune checkpoint inhibitors in non-small-cell lung cancer: where do we stand?. Clin Lung Cancer. 2018;19(1):1–11. doi:10.1016/j.cllc.2017.06.005
32. Fang W, Yang Y, Ma Y, et al. Camrelizumab (SHR-1210) alone or in combination with gemcitabine plus cisplatin for nasopharyngeal carcinoma: results from two single-arm, phase 1 trials. Lancet Oncol. 2018;19(10):1338–1350. doi:10.1016/S1470-2045(18)30495-9
33. Mkrtichyan M, Najjar YG, Raulfs EC, et al. Anti-PD-1 synergizes with cyclophosphamide to induce potent anti-tumor vaccine effects through novel mechanisms. Eur J Immunol. 2011;41(10):2977–2986. doi:10.1002/eji.201141639
34. Toulmonde M, Penel N, Adam J, et al. Use of PD-1 targeting, macrophage infiltration, and IDO pathway activation in sarcomas: a phase 2 clinical trial. JAMA Oncol. 2018;4(1):93–97. doi:10.1001/jamaoncol.2017.1617
35. Ferrara N, Gerber HP, LeCouter J. The biology of VEGF and its receptors. Nat Med. 2003;9(6):669–676. doi:10.1038/nm0603-669
36. Li Y, Zhao H, Ren XB. Relationship of VEGF/VEGFR with immune and cancer cells: staggering or forward? Cancer Biol Med. 2016;13(2):206–214. doi:10.20892/j.issn.2095-3941.2015.0070
37. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
38. Pishvaian MJ, Lee MS, Ryoo BY, et al. Updated safety and clinical activity results from a phase 1b study of atezolizumab+bevacizumab in hepatocellular carcinoma (HCC). Ann Oncol. 2018;29(suppl_8):LBA26. doi:10.1093/annonc/mdx807
39. Xue JM, Astere M, Zhong MX, Lin H, Shen J, Zhu Y-X. Efficacy and safety of apatinib treatment for gastric cancer, hepatocellular carcinoma and non-small cell lung cancer: a meta-analysis. Onco Targets Ther. 2018;11:6119–6128. doi:10.2147/OTT.S172717
40. Zhao D, Hou H, Zhang X. Progress in the treatment of solid tumors with apatinib: a systematic review. Onco Targets Ther. 2018;11:4137–4147. doi:10.2147/OTT.S172305
41. Xie L, Guo W, Wang Y, et al. Apatinib for advanced sarcoma: results from multiple institutions’ off-label use in China. BMC Cancer. 2018;18(1):396. doi:10.1186/s12885-018-4242-8
42. Xu JM, Zhang Y, Jia R, et al. Anti-PD-1 Antibody SHR-1210 combined with apatinib for advanced hepatocellular carcinoma, gastric or esophagogastric junction cancer: an open-label, dose escalation and expansion study. Clin Cancer Res. 2019;25(2):515–523. doi:10.1158/1078-0432.CCR-18-2484
43. Hutson TE, Lesovoy V, AI-Shukri S, et al. Axitinib versus sorafenib as first-line therapy in patients with metastatic renal-cell carcinoma: a randomised open-label phase 3 trial. Lancet Oncol. 2013;14(13):1287–1294. doi:10.1016/S1470-2045(13)70465-0
44. Wilky BA, Trucco MM, Kolonias D, et al. A phase II trial of axitinib plus pembrolizumab for patients with advanced alveolar soft part sarcoma (ASPS) and other soft tissue sarcomas (STS). J Clin Oncol. 2018;36(15_suppl):11547. doi:10.1200/JCO.2018.36.15_suppl.11547
45. Lewin J, Davidson S, Anderson ND, et al. Response to immune checkpoint inhibition in two patients with alveolar soft-part sarcoma. Cancer Immunol Res. 2018;6(9):1001–1007. doi:10.1158/2326-6066.CIR-18-0037
46. Mejean A, Ravaud A, Thezenas S, et al. Sunitinib alone or after nephrectomy in metastatic renal-cell carcinoma. N Engl J Med. 2018;379(5):417–427. doi:10.1056/NEJMoa1803675
47. Faivre S, Zappa M, Vilgrain V, et al. Changes in tumor density in patients with advanced hepatocellular carcinoma treated with sunitinib. Clin Cancer Res. 2011;17(13):4504–4512. doi:10.1158/1078-0432.CCR-10-1708
48. Reichardt P, Kang YK, Rutkowski P, et al. Clinical outcomes of patients with advanced gastrointestinal stromal tumors: safety and efficacy in a worldwide treatment-use trial of sunitinib. Cancer. 2015;121(9):1405–1413. doi:10.1002/cncr.29220
49. Tap WD, Jones RL, Van Tine BA, et al. Olaratumab and doxorubicin versus doxorubicin alone for treatment of soft-tissue sarcoma: an open-label phase 1b and randomised phase 2 trial. Lancet. 2016;388(10043):488–497. doi:10.1016/S0140-6736(16)30587-6
50. Parry RV, Chemnitz JM, Frauwirth KA, et al. CTLA-4 and PD-1 receptors inhibit T-cell activation by distinct mechanisms. Mol Cell Biol. 2005;25(21):9543–9553. doi:10.1128/MCB.25.21.9543-9553.2005
51. Hodi FS, Chiarion-Sileni V, Gonzalez R, et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018;19(11):1480–1492. doi:10.1016/S1470-2045(18)30700-9
52. Patel SP, Kurzrock R. PD-L1 expression as a predictive biomarker in cancer immunotherapy. Mol Cancer Ther. 2015;14(4):847–856. doi:10.1158/1535-7163.MCT-14-0983
53. Kim TK, Herbst RS, Chen L. Defining and understanding adaptive resistance in cancer immunotherapy. Trends Immunol. 2018;39(8):624–631. doi:10.1016/j.it.2018.05.001
54. Movva S, Wen W, Chen W, et al. Multi-platform profiling of over 2000 sarcomas: identification of biomarkers and novel therapeutic targets. Oncotarget. 2015;6(14):12234–12247. doi:10.18632/oncotarget.3498
55. Rizvi NA, Hellmann MD, Snyder A, et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015;348(6230):124–128. doi:10.1126/science.aaa1348
56. Palmieri G, Colombino M, Cossu A, et al. Genetic instability and increased mutational load: which diagnostic tool best direct patients with cancer to immunotherapy? J Transl Med. 2017;15(1):17. doi:10.1186/s12967-017-1119-6
57. Saller J, Walko CM, Millis SZ, et al. Response to checkpoint inhibitor therapy in advanced classic kaposi sarcoma: a case report and immunogenomic study. J Natl Compr Canc Netw. 2018;16(7):797–800. doi:10.6004/jnccn.2018.7018
58. Dudley JC, Lin MT, Le DT, et al. Microsatellite instability as a biomarker for PD-1 blockade. Clin Cancer Res. 2016;22(4):813–820. doi:10.1158/1078-0432.CCR-15-1678
59. Tlemsani C, Leroy K, Gimenez-Roqueplo AP, et al. Chemoresistant pleomorphic rhabdomyosarcoma: whole exome sequencing reveals underlying cancer predisposition and therapeutic options. J Med Genet. 2018. pii: jmedgenet-2018-105594. doi:10.1136/jmedgenet-2018-105594.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.