Back to Journals » International Journal of Women's Health » Volume 18
Rebozo Technique on Labor Pain Intensity: A Systematic Review
Authors Ermiati E ![]() , Widiasih R
, Widiasih R ![]() , Srimurni NA, Sari NDA, Aini FHQ
, Srimurni NA, Sari NDA, Aini FHQ
Received 13 April 2026
Accepted for publication 30 June 2026
Published 10 July 2026 Volume 2026:18 616559
DOI https://doi.org/10.2147/IJWH.S616559
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Ermiati Ermiati,1 Restuning Widiasih,1 Nita Ayu Srimurni,2 Nadia Dwi Aslama Sari,2 Farah Huwaida Qurrota Aini2
1Department of Maternity, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Ermiati Ermiati, Department of Maternity, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Bandung-Sumedang KM 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +628122109363, Fax +6222-7795596, Email [email protected]
Abstract: Labor pain remains a significant challenge in childbirth due to its impact on maternal comfort and overall birth experience. The Rebozo technique is a traditional non-pharmacological intervention that uses a woven cotton shawl to perform gentle rhythmic movements of the pelvis, aiming to promote relaxation and support labor progression. Despite increasing attention, evidence regarding its effect on labor pain intensity remains fragmented and incomprehensive. This systematic review aimed to synthesize the Rebozo technique in reducing labor pain intensity. A comprehensive search was conducted across PubMed, Scopus, ScienceDirect, and Garuda databases for studies published between 2020 and 2025. The review followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Quantitative studies, including randomized controlled trials (RCT) and quasi-experimental designs involving intrapartum women, were included, with pain intensity as the primary outcome. Study quality was appraised using the Joanna Briggs Institute (JBI) Critical Appraisal Tools. A meta-analysis was not conducted due to heterogeneity in study design, intervention protocols, outcome measures, and sample characteristics, and instead a narrative synthesis was applied. Ten studies comprising 537 participants met inclusion criteria. Results indicate that overall Rebozo technique significantly reduced labor pain intensity (p-values 0.000– 0.016), particularly during the active phase compared with standard care or other non-pharmacological methods. In conclusion, the Rebozo technique appears to be an effective, safe, and adaptable non-pharmacological approach for labor pain management. Limitations include heterogeneity among studies and restricted generalizability due to the predominance of studies from Indonesia and Türkiye. Further studies with standardized protocols and expanded outcome measure are warranted.
Keywords: childbirth, labor pain, Rebozo technique, non-pharmacological intervention
Introduction
Labor pain is a nearly universal experience during childbirth reporting moderate to severe pain throughout labor.1 Unmanaged pain not only reduces the quality of the birth experience but also increases the risk of postpartum psychological complications such as anxiety, depression, and post-traumatic stress disorder, which may disrupt early bonding and breastfeeding success.2 In low- and middle-income countries, access to pharmacological pain relief is limited by cost, infrastructure, workforce shortages, and cultural factors.3 These constraints drive a growing interest in non-pharmacological pain-management approaches that are safer, more affordable, and compatible with women’s preferences for minimal medical intervention.
Growing evidence underscores the importance of non-pharmacological approaches as essential strategies for effective and woman-centered labor pain management. A robust body of research confirms that non-pharmacological methods such as massage, breathing techniques, birthing ball exercises, aromatherapy, acupressure, and freedom of movement are effective in reducing labor pain and enhancing maternal satisfaction.4 Systematic reviews and meta-analyses show that acupressure, aromatherapy, and massage therapy are particularly effective, with aromatherapy and acupressure ranking highest for pain relief and shortening labor duration.5 These interventions are also associated with fewer side effects, greater maternal empowerment, and reduced need for medical interventions.4 Within this context, there is growing interest in integrating traditional and complementary techniques into modern maternity care to further optimize maternal comfort and labor process.
One such non-pharmacological approach that has potential role supporting labor comfort and progression is the Rebozo technique. The Rebozo is a 100% cotton shawl made from soft fabric that does not irritate the skin, measuring at least 200×70 cm and capable of supporting up to 225 kg, traditionally used in Mexican and Spanish cultures.6 Rebozo technique is a traditional manual therapy that uses a shawl to perform rhythmic pelvic movement, including gentle shaking, sifting, and rocking motions.7 Several papers state that rebozo relaxes pelvic muscles and uterine ligaments, creating more pelvic space and helping the fetus descend more easily, which may reduce contraction pain.8–10 Another finding support the integration of the rebozo technique into clinical practice, as it can be considered a non-invasive and safe alternative to maternal positioning strategies for promoting anterior rotation of an occiput posterior fetus.11 These characteristics highlight the Rebozo technique as a promising, low-cost intervention with the potential to enhance both maternal comfort and labor outcomes.
The Rebozo technique has gained increasing attention as a non-pharmacological intervention for labor pain management; however, the current evidence remains fragmented and not yet comprehensive. Therefore, this systematic review aims to synthesize available studies on the Rebozo technique in relation to labor pain, with a focus on pain intensity across different stages of labor and related maternal outcomes, including anxiety, labor progression, and childbirth experience.
Materials and Methods
Study Design
This study employed a systematic review design guided by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) framework.12 The PRISMA approach ensured a transparent, structured, and replicable process for identifying, screening, and selecting relevant studies. All procedures, from literature searching to data extraction and appraisal, followed standardized systematic review protocols to maintain methodological rigor throughout the process. This systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420261426112.
Search Strategy
The literature search was conducted in PubMed, Scopus, ScienceDirect, and Garuda for studies published between 2020–2025. The search strategy used general keywords related to the population, intervention, and outcomes of interest. These keywords included terms such as “rebozo”, “rebozo technique”, “labor”, “childbirth”, “intrapartum”, “labor pain”, and “pain intensity”. Boolean operators (AND/OR) were applied to combine these keywords, ensuring a broad yet focused retrieval of studies relevant to the topic. The search was adapted to each database’s indexing system to maximize sensitivity and specificity.
Eligibility Criteria
Studies were included if they met the following criteria: (1) quantitative design, (2) involved intrapartum women experiencing labor, (3) evaluated the Rebozo technique as the primary intervention, and (4) reported labor pain outcomes using validated measurement tools. Studies were excluded if they combined Rebozo with other interventions, were qualitative or review designs, did not measure labor pain, or were published in languages other than English or Indonesia. These criteria were chosen to focus the review on high-quality, comparable evidence that directly addresses the isolated effects of Rebozo on labor pain.
Article Selection Process
The study selection process was guided by the PRISMA framework to ensure a systematic and transparent approach. All identified records were imported into reference management software and duplicates were removed. The five authors independently screened titles and abstracts for relevance to the inclusion criteria, followed by a detailed full-text assessment of potentially eligible studies. Discrepancies were resolved through discussion among the authors.
Quality Appraisal and Data Extraction
The methodological quality of the included studies was appraised using the Joanna Briggs Institute (JBI) Critical Appraisal Tools for RCT and quasi-experimental studies.13,14 Each study was evaluated based on JBI criteria relevant to its design. Detailed item-by-item appraisal results are presented in (Supplementary Table 1) and were used to interpret the review findings.
Data extraction was performed using a structured format to ensure consistency and clarity across the included studies. The extracted information included author and year, country, study design, sample size, intervention, outcome measures, findings, and JBI scores. The intervention column captures detailed information on the type of Rebozo technique and phase of labor, while also indicating the comparator or control conditions when present, such as standard care, warm compress, or pre-post control. The findings column provides numerical results, including p-values, and summarizes the effect of the intervention relative to the comparator, allowing readers to assess the magnitude and significance of outcomes. JBI scores indicate the methodological quality of each study to inform interpretation. This approach ensures that all essential information regarding interventions, comparators, and outcomes is transparently reported.
Statistical Analysis
Given the diversity of study designs, intervention protocols, outcome measures, and sample characteristics among the included studies, a meta-analysis was not appropriate. Instead, a descriptive and narrative synthesis was applied, which is well-suited for systematically comparing heterogeneous studies. This approach enabled clear identification of trends, consistent findings, and methodological strengths across studies, providing a comprehensive overview of the Rebozo technique’s effects on labor pain and related outcomes. The results are presented in tabular and textual formats to facilitate comparison across studies and to highlight methodological variations, overall trends, and sources of heterogeneity among studies.
Results
Overview of Study Selections
A PRISMA flow diagram summarizing the study selection process is presented in (Figure 1). A total of 47 records were identified through database searching, consisting of PubMed (n = 5), Scopus (n = 8), ScienceDirect (n = 19), and Garuda (n = 15). After removing 6 duplicate records, 41 studies proceeded to the screening stage. During title and abstract screening, 19 records were excluded due to inappropriate titles (n = 18) and unsuitable abstracts (n = 1). This left 22 reports for full-text retrieval, of which 4 reports could not be retrieved, resulting in 18 full-text articles assessed for eligibility. Following detailed evaluation, 8 articles were excluded for the following reasons: combined interventions (n = 3), protocol study (n = 1), review articles (n = 3), and qualitative design (n = 1). Ultimately, 10 studies met all inclusion criteria and were included in the final systematic review.
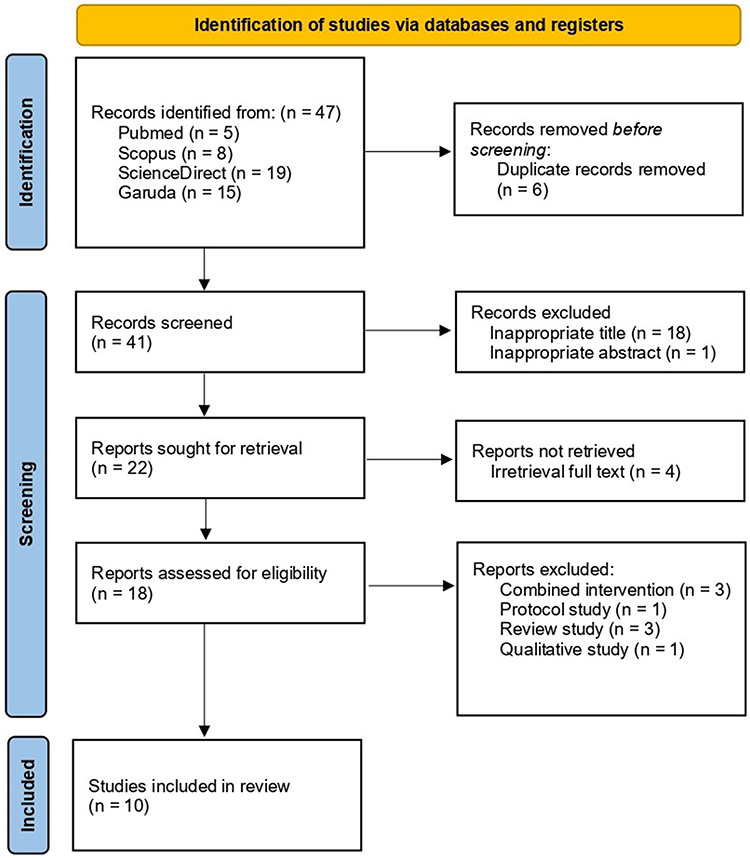 |
Figure 1 Study selection process (PRISMA). |
Characteristics of Included Studies
Based on the search results on (Table 1), the 10 included studies were conducted in Indonesia (n = 7) and Türkiye (n = 3). The studies consisted of quasi-experimental designs (n = 7) and randomized controlled trials (n = 3). The sample sizes ranged from 20 to 146 participants, involving both primiparous and multiparous women. Interventions generally involved the application of the Rebozo technique during the active phase of labor, with variations such as RSTA, RSWLD, or multi-phase protocols. Intervention timing varied across studies, with most applied during the active phase of labor, while some studies included latent and transition phases. Comparison groups included standard care, warm compresses, or relaxation massage. Outcome measurements were primarily focused on pain intensity using validated tools such as the VAS, Wong-Baker Pain Scale, and observational sheets.
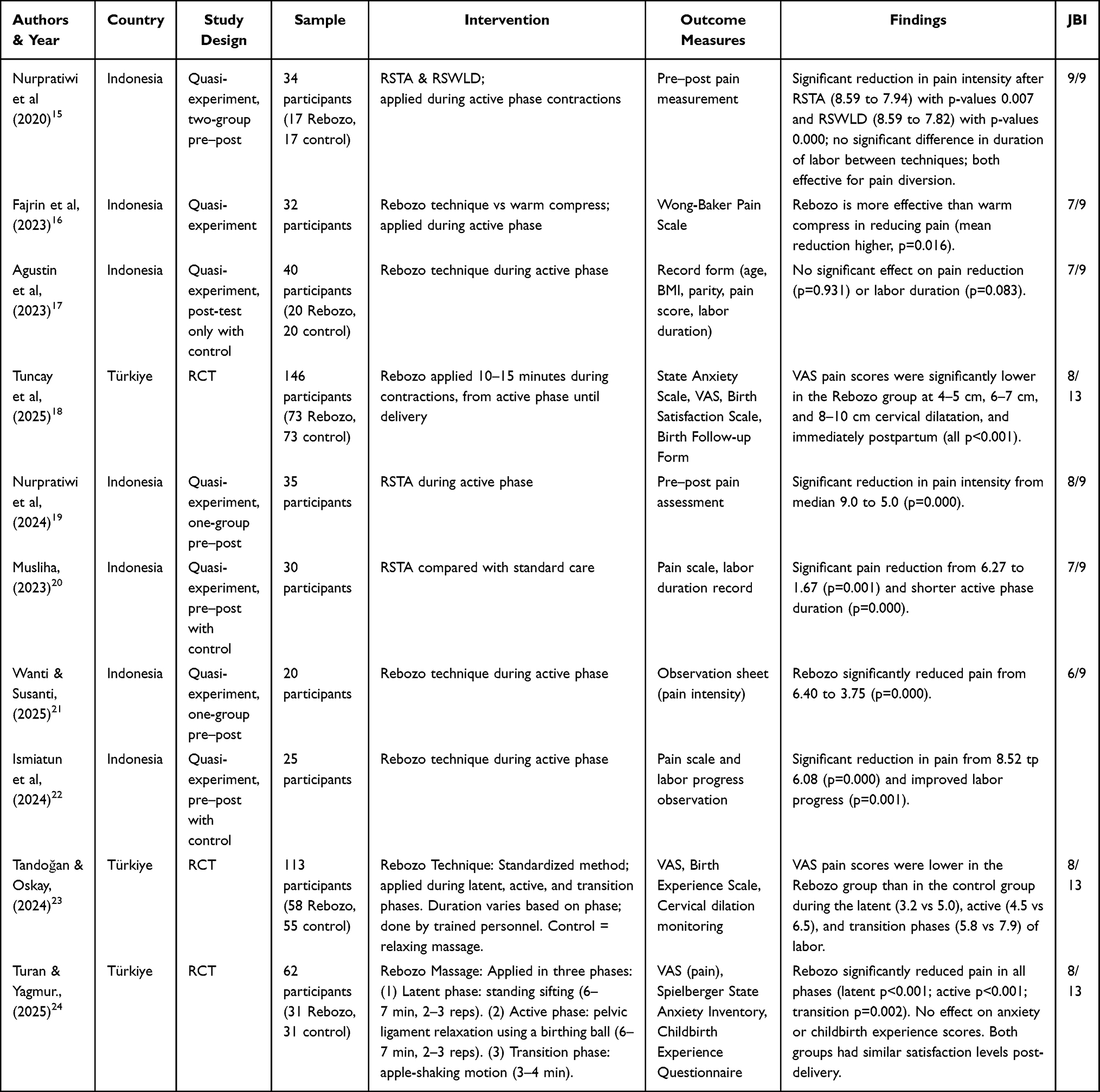 |
Table 1 Results of the Article Review |
Rebozo Technique on Labor Pain Intensity
Across the included studies, 9 out of 10 studies reported a statistically significant reduction in labor pain intensity following the Rebozo intervention compared with control or alternative non-pharmacological methods. Reported p-values across studies ranged from 0.000 to 0.931. Most studies demonstrating significant effects reported p-values below 0.05, particularly during the active phase of labor, while one study reported no statistically significant difference in pain outcomes (p = 0.931).17 Pain reduction was observed across different intervention formats, including RSTA, RSWLD, and multi-phase applications. However, the magnitude of reported pain reduction varied due to differences in measurement tools, intervention duration, and timing of application, and because the studies differed in design, outcomes, and reporting formats, a meta-analysis was not feasible, so the results are summarized using a narrative synthesis.
Discussion
Across the included studies, the majority reported a significant reduction in labor pain intensity among women who received the Rebozo technique compared with standard care or alternative non-pharmacological methods. This effect was observed in both primiparous and multiparous women and across different phases of labor, although evidence was strongest for the active phase. Several studies also reported secondary benefits, such as a shorter duration of the active or second stage of labor and improved maternal satisfaction with the childbirth experience.
Rebozo Technique in Reducing Labor Pain
The findings of this review indicate that the rebozo technique is generally effective in reducing labor pain, although some inconsistencies remain across studies. Most included studies reported a significant decrease in pain intensity following the application of rebozo techniques, particularly when implemented during the active phase of labor, suggesting its role as a beneficial non-pharmacological pain management strategy. For instance, several quasi-experimental studies demonstrated statistically significant reductions in pain scores after interventions such as RSTA and other rebozo variations, while randomized controlled trials further supported these findings by showing lower pain levels across different labor phases in the intervention groups. However, one study reported no significant effect on pain reduction, highlighting potential variability in the evidence.17 Therefore, despite some heterogeneity, the overall evidence suggests potential of the rebozo technique as a practical and low-risk approach to reducing labor pain. This aligns with the utility of rebozo techniques as a reliable method for mitigating labor pain.6,23
Variations in effect of the Rebozo technique on labor pain intensity across the included studies may be attributed to differences in methodological quality and intervention protocols. Studies employing randomized controlled designs tended to demonstrate more consistent reductions in pain intensity compared to quasi-experimental approaches, indicating stronger internal validity. In addition, the duration, frequency, and type of rebozo application (sifting, shaking, or multi-phase techniques) were not standardized, which may influence outcomes. Participant characteristics such as parity and individual pain perception also likely contributed to the variability in findings. In addition, differences in methodological quality and risk of bias may have influenced the consistency of findings across studies.
Furthermore, when compared with other non-pharmacological methods, the rebozo technique appears to offer comparable or even superior benefits in certain contexts. One study within this review demonstrated greater pain reduction with rebozo compared to warm compresses, indicating its potential added value in clinical practice.16 The rebozo technique not only offers pain relief but also promotes relaxation and can enhance the overall birth experience, making it a valuable adjunct throughout pregnancy and labor.25 Additionally, continuous physical and emotional support during the intervention may lower anxiety and enhance coping, which are known determinants of labor pain experience. Importantly, the rebozo technique is low-cost, non-invasive, and easily adaptable across different care settings.
Impact on Labor Progression and Maternal Experience
The findings indicate that the rebozo technique may positively influence labor progression, although results remain somewhat mixed. Several studies, particularly randomized controlled trials, reported shorter labor duration, faster cervical dilation, and reduced second-stage length, as well as lower rates of episiotomy and perineal trauma.18,23,24 These effects are likely related to improved fetal positioning and increased pelvic flexibility facilitated by the technique. This aligns with existing evidence showing that maternal movement and upright or dynamic positions during labor can enhance uterine efficiency, facilitate fetal descent, and shorten labor duration.26 However, findings were not consistent across all studies, indicating that effects may vary depending on context and study design.
In terms of maternal experience, the rebozo technique generally contributes to improved satisfaction and reduced anxiety during labor. Women receiving the intervention reported greater comfort and more positive birth experiences, including lower pain perception and higher satisfaction scores. This is consistent with prior evidence that continuous physical support and non-pharmacological comfort measures improve maternal well-being and childbirth satisfaction.27 Nevertheless, study reported no significant differences in anxiety or childbirth experience, indicating that individual and contextual factors may influence perceived benefits.24
Clinical Implications
The Rebozo technique may have potential for integration into clinical practice due to its low cost, non-invasive nature, and adaptability across labor positions and settings. Its applicability in diverse contexts, including Indonesia and Türkiye, highlights its cultural flexibility and relevance for low- and middle-income countries where access to pharmacological analgesia is limited. However, effective implementation requires appropriate training and standardization. Variability in techniques (eg, sifting, pelvic rocking) and application protocols across studies likely contributed to inconsistent outcomes This underscores the need for clear clinical guidelines and competency-based training to ensure consistent practice. The observed heterogeneity and study design limitations should be considered when translating findings into practice.
Despite encouraging findings, the evidence base remains limited by heterogeneity and the predominance of quasi-experimental designs. Future research should prioritize high-quality randomized trials with standardized protocols, as well as comparative studies evaluating Rebozo alongside other non-pharmacological interventions. Additionally, research exploring maternal preferences, implementation feasibility, and long-term outcomes would further strengthen the evidence base.
Limitations
This systematic review has several limitations. The predominance of quasi-experimental designs and variability in methodological quality may have affected the strength of the overall conclusions. There was also significant heterogeneity in rebozo techniques, intervention timing, and outcome measures, making comparisons across studies difficult. Additionally, the studies were largely conducted in Indonesia and Türkiye, which may restrict broader applicability. Potential publication bias and language restrictions may have further limited the completeness of the evidence. Future research should focus on well-designed randomized controlled trials with standardized intervention protocols to strengthen the evidence base, as well as explore long-term maternal and neonatal outcomes, comparative effectiveness with other non-pharmacological methods, and the feasibility of integrating the rebozo technique into routine maternity care across different clinical and cultural settings.
Conclusion
This systematic review indicates that the Rebozo technique is promising, feasible, and potentially beneficial as a non-pharmacological method for reducing labor pain intensity, particularly during the active phase. The majority of studies reported significant pain reduction, with additional benefits for labor progress and maternal comfort. However, the evidence remains limited due to heterogeneity across studies, small sample sizes, and predominance of quasi-experimental designs. Healthcare providers, especially in low-resource settings with limited access to pharmacological analgesia, may consider integrating the Rebozo technique into routine labor support. Training and standardized protocols are recommended to ensure consistent and effective implementation. Future research should focus on larger randomized controlled trials with standardized protocols, secondary outcomes, and applicability across diverse settings to strengthen the evidence base and guide clinical practice.
Abbreviations
BMI, Body Mass Index; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; JBI, Joanna Briggs Institute; SLR, Systematic Literature Review; RCT, Randomized Controlled Trial; VAS, Visual Analogue Scale; RSTA, Rebozo Shake the Apple; RSWLD, Rebozo Sifting While Lying Down; SOP, Standard Operating Procedure; LMICs, Low- and Middle-Income Countries.
Acknowledgments
The authors appreciated the Universitas Padjadjaran for facilitating the database search and funding this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Intrapartum care for a positive childbirth experience. 2018. Available from: http://apps.who.int/iris/bitstream/10665/260178/1/9789241550215-eng.pdf?ua=1%0Ahttp://www.who.int/reproductivehealth/publications/intrapartum-care-guidelines/en/.
2. O’Dea GA, Youssef GJ, Hagg LJ, et al. Associations between maternal psychological distress and mother-infant bonding: a systematic review and meta-analysis. Arch Womens Ment Health. 2023;26(4):441–8. doi:10.1007/s00737-023-01332-1
3. Morriss WW, Roques CJ. Pain management in low- and middle-income countries. BJA Educ. 2018;18(9):265–270. doi:10.1016/j.bjae.2018.05.006
4. AlHabardi NM, Alotaibi RM, Almutairi GS, et al. Nonpharmacological approaches for managing labor pain: systematic review. Int J Med Dev Ctries. 2025;8(12):3808.
5. Larki M, Karimi L, Jahanfar S, Mohammadi S, Makvandi S. Unveiling the latest evidence: an updated systematic review and meta-analysis and GRADE assessment on the effectiveness of acupressure in managing labor pain. BMC Complement Med Ther. 2025;25(1). PubMed PMID: 40349040. doi:10.1186/s12906-025-04908-9
6. Uludağ DS, Kocatürk AA. The effect of using rebozo technique during labor on the sensation of labor pain and labor duration. Razi Int Med J. 2024;4(1):45–54. doi:10.56101/rimj.v4i1.152
7. Damayanti A, Fatimah YU. The effect of rebozo technique to reducing pain and progress maternity. In:
8. Wahyuni Bahrum S, Sri Rejeki I, Fajri F. The effectiveness of acupressur and rebozzo techniques in preparation for delivery in mandiri midwife practices, gowa regency. Int J Heal Pharm. 2022;3(2):259–264. doi:10.51601/ijhp.v3i2.162
9. Sari DY. Rebozo technique on pain intensity in the first stage of the active phase and length. J Anesthesiol Clin Res. 2024;5(1):548–551. doi:10.37275/jacr.v5i1.517
10. Astuti ADW, Intanwati I, Presty MR, Yasinta A. Knowledge overview of thirdtrimester pregnant women and women in labor about the rebozo technique. Indones J Glob Heal Res. 2024;6(1):159–164. doi:10.37287/ijghr.v6i1.2654
11. Fumagalli S, Antolini L, Nespoli A, et al. Rebozo and advanced maternal postures: a promising set of intrapartum interventions to reduce persistent occiput posterior position of the fetal head. Eur J Midwifery. 2024;8:1–11. doi:10.18332/EJM/191511
12. Page MJ, Mckenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews systematic reviews and meta-analyses. BMJ. 2021:n71. doi:10.1136/bmj.n71
13. Barker T, Stone J, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid Synth. 2023;23(3):494–506. doi:10.11124/JBIES-22-00430
14. Barker T, Habibi N, Aromataris E, Stone J, Leonardi-Bee J, Sears K. The revised JBI critical appraisal tool for the assessment of risk of bias quasi-experimental studies. JBI Evid Synth. 2024;22(3):378–388. doi:10.11124/JBIES-23-00268
15. Nurpratiwi Y, Hadi M, Idriani I. Teknik Rebozo terhadap intensitas nyeri kala I fase aktif dan lamanya persalinan pada ibu multigravida [The Rebozo technique on the intensity of pain in the first active phase and the duration of labor in multigravida mothers]. J Keperawatan Silampari. 2020;4(1):293–304. doi:10.31539/jks.v4i1.1627
16. Hidayati Fajrin D, Audina V. Perbedaan Pengaruh Rebozo dan Kompres Hangat terhadap Penurunan Skala Nyeri Persalinan Kala I Fase Aktif [The difference in the effect of rebozo and warm compresses on reducing the pain scale of labor in the active phase]. J Kesehat Poltekes Kemenkes Ri Pangkalpinang. 2023;11(2):1–255.
17. Agustin AI. Pengaruh Teknik Rebozoterhadap Nyeri Dan Lama Persalinan Kala 1 Fase Aktif [Effect of the rebozo technique on pain and duration of the active phase of the first stage of labor]. WOMB Midwifery J. 2023;2(2):42–49. doi:10.54832/wombmidj.v2i2.125
18. Tuncay Z, Cayir G, Sule H, Yldz A. Effects of the Rebozo technique on labor outcomes in primiparous women: a randomized controlled trial. Explore. 2025;21(6):103282. doi:10.1016/j.explore.2025.103282
19. Nurpratiwi Y, Armi, Setiawan Y, Azizah NN. Pengaruh teknik rebozo shake the apple (RSTA) terhadap intensitas nyeri persalinan kala I fase aktif pada ibu primigravida [The effect of the rebozo shake the apple (rsta) technique on the intensity of first stage pain during the active phase in primigrav. Edu Res Indones Inst Corp Learn Stud. 2024;5(1):70–80.
20. Musliha I. Efektivitas Teknik Rebozo Shake the Apple (RSTA) Terhadap Intensitas Nyeri Dan Lama Kala 1 Fase Aktif Pada Persalinan Ibu Multigravida [(The effectiveness of the rebozo shake the apple (RASTA) technique on pain intensity and duration of the 1st stage of t. Indones Sch J Nurs Midwifery Sci. 2023;2(10):893–901. doi:10.54402/isjnms.v2i10.359
21. Wanti W, Susanti K. Efektivitas teknik rebozo dalam mengurangi nyeri persalinan kala 1 fase aktif pada ibu bersalin di RSUD bangkinang [The effectiveness of the rebozo technique in reducing first stage pain in the active phase in women giving birth at bangkinang hospital]. J Kesehat Tambusai. 2025;6(3):10619–10628.
22. Ismiatun, Nila Q, Inggit Primadevi S. Efektifitas Tehnik Rebozo Mengurangi Rasa Nyeri Dan Kemajuan Persalinan Pada Ibu Bersalin Di PMB Wilayah Kerja Kota Bandar Lampung [Effectiveness of the rebozo technique in reducing pain and improving labor progress among women giving birth at independent. Innov J Soc Sci Res. 2024;4(6):5746–5763.
23. Tandoğan Ö, Oskay Ü, Szabo L. The effect of Rebozo technique on perceived labour pain and childbirth experience: a randomized controlled trial. Medicine. 2024;22(1):1–8. doi:10.1186/s12916-023-03187-w
24. Turan Z, Yağmur Y. The effect of rebozo massage on birth pain, anxiety, and childbirth experience in the intrapartum period: a randomized controlled trial in Türkiye. J Transcult Nurs. 2025;1–11. doi:10.1177/10436596251366932
25. Farag WKA, Ibrahim HI, Alam THM. Effect of rebozo techniques on pain intensity, anxiety and birth experience among primiparous women during the active phase of labor. Menoufia Nurs J. 2024;9(4):281–300. doi:10.21608/menj.2024.414770
26. Gupta J, Sood A, Hofmeyr G, Vogel J. Position in the second stage of labour for women with epidural anaesthesia. Cochrane Database Syst Rev. 2017;5(5). PMID: 23440824. doi:10.1002/14651858.CD008070.pub2
27. Hodnett ED, Gates S, Hofmeyr GJ, Sakala C. Continuous support for women during childbirth. Cochrane Database Syst Rev. 2013;7(7):1–130. PMID: 23076901. doi:10.1002/14651858.CD003766.pub5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.