Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 13
Reasons for Extraction of Permanent Teeth in a University Dental Clinic Setting
Authors Ali D
Received 30 November 2020
Accepted for publication 12 February 2021
Published 24 February 2021 Volume 2021:13 Pages 51—57
DOI https://doi.org/10.2147/CCIDE.S294796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Dena Ali
Department of General Dental Practice, Faculty of Dentistry, Kuwait University, Jabriya, Kuwait
Correspondence: Dena Ali
Department of General Dental Practice, Faculty of Dentistry, Kuwait University, PO Box 24923, Safat, 13110, Kuwait
Tel +965-24633433
Fax +965-25326049
Email [email protected]
Purpose: This study aimed to explore the reasons for tooth extraction and investigated the potential correlations between tooth loss and several variables including age, gender, education level, and other risk factors, such as diabetes and smoking habit.
Patients and Methods: The study retrospectively analyzed 1811 dental records of patients who underwent extraction procedure of at least one tooth. Patients’ variables included: age, gender, level of education, diabetes, and smoking habit. Reasons for extraction were recorded as follows: caries, periodontal disease, endodontic treatment complications, orthodontic treatment, impactions, trauma, pre-prosthetic, and others (esthetic reasons, tooth malposition, or unspecified reasons).
Statistical analysis: The significance of variables was analyzed by Chi square test, P < 0.05. The variances in the mean number of extracted teeth per patient were investigated using ANOVA. Pearson correlation test was used to test the strength of the association among the tested variables, P < 0.01.
Results: Out of 1811 reviewed patients’ records, 2654 extracted teeth were identified. Males had a higher number of extracted teeth, 1447 (54.5%), than females, 1207 (45.5%). Males had more extractions due to periodontal disease, while females had more extractions for orthodontic and pre-prosthetic reasons. The highest mean of extracted teeth was identified among the 51-year-old and above age groups (3.73 ± 0.53 teeth) where periodontal disease was shown to have a significant association (P < 0.05). Diabetic patients showed a significant association with periodontal diseases, while smokers showed a significant association with caries. Both diabetics and smokers had moderate correlation (0.055 and 0.04, respectively).
Conclusion: Caries, periodontal disease, and endodontic complications were the most common causes of tooth extraction. In addition, this study indicated that age, diabetes, and smoking habits were found to be suitable forecasters for permanent tooth loss as these variables displayed significant statistical association.
Keywords: tooth extraction, dental caries, periodontal disease
Introduction
Tooth loss remains the foremost universal problematic dental issue.1 Previous studies of the reasons for tooth extractions have been conducted in multiple regions and concluded that caries, periodontal diseases, trauma, orthodontic and prosthodontic treatments, endodontic treatment complications, root fracture, and malpositioned teeth are the main reasons for tooth loss.2–7 In order to implement good measures for oral disease prevention and oral health awareness policies, it is important to understand the reasons for tooth loss.
Multiple studies revealed that dental carious lesions and periodontal disease were the most common reasons for tooth extraction.7–11 In general, most of the studies showed that dental caries was the primary reason for tooth loss among 20 to 60 years old patients. Besides, periodontal disease was the principal reason for tooth loss among patients in their late 40s and older as there was an association between age and periodontal disease. On the other hand, endodontic treatment complications and orthodontic treatment was observed as the main reason for tooth extraction among adolescent patients.12–14
Some studies concluded that there was an association between tooth loss and gender, where females had more tooth loss due to dental caries while males lose their teeth mostly due to periodontal disease.12–14 Other reasons such as root fracture, pre-prosthetic, esthetic reasons, and tooth malposition were found to have less influence on tooth loss.2–6
Few studies explored the association between socio-demographic and medical factors with tooth loss.8,10,17 Therefore, the aims of this study were to explore the reasons for tooth extraction and investigate the potential correlations between tooth loss and several variables including age, gender, education level, and other risk factors, such as diabetes and smoking habit.
Patients and Methods
This study retrospectively analyzed 1811 dental records of patients who underwent extraction procedure of at least one tooth at the department of Oral and Maxillofacial Surgery at Kuwait University Faculty of Dentistry. The extraction procedures were performed under either local anesthesia alone or combined with nitrous oxide inhalation sedation from the period of January 2015 until December 2019. This study was conducted in full accordance with the World Medical Association Declaration of Helsinki and was approved by the Ethics Committee of the Health Sciences Center at Kuwait University. All previously enrolled patients at Kuwait University dental clinic have signed consent forms that stated the possibility of using patient’s information for scientific projects with assurance of anonymity and privacy. Therefore, the research approval did not require a waiver of informed consent or documentation of informed consent. Patients’ dental records were retrieved using Titanium dental software (Titanium Software, Inc. USA).
One examiner assessed all patients’ dental records where patients’ variables included: age (categorized into six age groups starting with age group <20 years and ending with >60 years of age), gender, level of education, diabetes, and smoking habit. Tooth extraction variables consisted of the reason for extraction which was recorded as follows: caries (including fractured teeth and remaining roots primarily due to caries), periodontal disease (including breakdown of the periodontal apparatus and weakening of the periodontal attachments), endodontic treatment complications (including persistent symptoms, resistant periapical healing as well as fractures), orthodontic treatment, impactions, trauma, pre-prosthetic, and other reasons (esthetic reasons, tooth malposition, or unspecified reasons). In addition, tooth type, number of extracted teeth per patient were recorded. Patients who underwent extraction of supernumerary and deciduous teeth plus dental records with incomplete data entry were excluded from the study.
The data were entered and analyzed using Statistical package for Social Sciences software (SPSS), version 26.0. The significance of the patients’ variables, such as age, gender, education level, diabetes, and smoking habit with reasons of tooth extraction were analyzed by Chi square test, where a p-value <0.05 was considered significant. The variances in the mean number of extracted teeth per patient were investigated using ANOVA test. Pearson correlation test was used to test the strength of the association among the tested variables. Correlation was considered significant at p < 0.01 level (two-tailed; http://dx.doi.org/10.17504/protocols.io.bp7nmrme).
Results
The total number of patients involved in this study was 1811 with a total of 2654 extracted teeth. The mean age of patients was 43.4 ± 11.4, ranging from 16 to 86 years. The mean number of extracted teeth per patient was 1.46 ± 0.67. The distribution of extracted teeth by gender, age groups, level of education, diabetes, and smoking habits is illustrated in Table 1. Male patients count was higher, 990 (54.7%), than female patients, 821 (45.3%). Male patients had a higher number of extracted teeth, 1447 (54.5%), than females, 1207 (45.5%). However, there was no significant differences among the two genders. The age group of 31–40 years included 455 patients (25.1%), and the age group of 41–50 years counted for 429 patients (23.7%). These groups were the highest in count as well as in number of extracted teeth, which was 665 (25.1%) and 632 (23.8%) respectively. The highest mean for the number of extracted teeth per patient was identified among 51 years old and above age groups (3.73 ± 0.53 teeth), with a p-value of 0.03. On the other hand, the lowest mean for the number of extracted teeth per patient was identified among ≤20 years of age (1.43 ± 0.46 teeth), with a p-value of 0.006.
 |
Table 1 Distribution of Extracted Teeth by Patient Variables |
With regards to education level, patients who held a high school diploma were the highest in count, 879 (48.5%), followed by middle school, 427 (23.6%). College & higher education level included 364 patients (20.1%). Subsequently, the total number of extracted teeth, which is shown in Table 1, followed the same arrangement, where 1334 extracted teeth (50.3%) for high school diploma holders vs 603 (22.7%) for middle school education level vs 529 (19.9%) college and higher education level. A total of 165 patients (9.1%) had diabetes and 244 patients (13.5%) had smoking habits. Forty-one patients (2.3%) had both diabetes and smoking habits.
Table 2 illustrates the results from stratifying the entire patients’ population by gender, age groups, level of education, diabetes, and smoking habits with multiple reasons for tooth extractions. The results suggested that dental caries was the major reason for tooth extraction as 1796 (67.7%) teeth were extracted due to caries, followed by periodontal disease, 543 (20.5%), and endodontic treatment complications, 225 (8.5%). Other reasons for tooth extractions such as dental trauma, pre-prosthetic treatment, and esthetics plus malpositioned teeth and unspecified reasons were considered minor.
 |
Table 2 Reasons for Tooth Extraction by Patient Variables |
Dental caries was the chief cause for extraction in both genders, with a slightly higher number among male patients 971 (67.1%) as shown in Table 2. Males reported to have more extractions due to periodontal diseases 315 (21.8%) and endodontic treatment complications 128 (8.8%) than females. On the contrary, females showed more extracted teeth due to orthodontic treatment 35 (2.9%) and pre-prosthetic treatment 4 (0.3%).
Additionally, Caries as a reason for extraction, scored high in age groups of 50 years and younger. Conversely, periodontal diseases scored higher percentages of extractions among age groups 51–60 and 60 years and higher, 25.3% and 29.3%, respectively. In addition, the number of extracted teeth was significantly higher among middle and high school diploma holders when stratified against caries, periodontal reasons, and endodontic treatment complications. With respect to diabetes and smoking habits, diabetic patients and smokers had high percentages of their teeth extracted due to caries (58.1% and 27.4%) and periodontal reasons (71.0% and 21.0%) respectively, as shown in Table 2.
Correlation and strength of association among variables were tested and revealed that age groups, in general, showed a significant association with caries, periodontal reasons, and endodontic treatment complications; however, only caries and periodontal reasons presented strong correlation associations with age (0.001 and 0.03, respectively). Interestingly, age groups of 41 years and higher have particularly showed a significant association and strong correlation with periodontal reasons (0.042) as a cause of tooth extraction. When gender was tested for association, only males have shown a significant association and moderate correlation with periodontal disease (0.05) as a reason for extraction. With regards to level of education in general, there was a significant association with caries and orthodontic treatment as causes for extraction among high school and college education levels. However, the correlation was weak (−0.016). Concerning diabetic patients, there was a significant association with periodontal diseases as a reason for extraction. On the other hand, smoking habits showed a significant association with caries. Both groups had moderate correlation association (0.055 and 0.04, respectively), shown in Table 2.
Table 3 presents the frequency of extraction of different teeth types with respect to various reasons for tooth extraction. The most commonly extracted teeth were mandibular and maxillary second and third molars, 743 (28%) and 678 (25.4%) sequentially. Dental caries, periodontal diseases, and endodontic treatment complications were among the most frequent reasons for extraction in molar teeth. The least common tooth extracted among all sampled population were mandibular canines, 30 (1.1%), which were mostly extracted due to caries. Nonetheless, mandibular central incisors were commonly extracted due to periodontal diseases while maxillary central incisors were commonly extracted due to caries. Premolars were noticed to be extracted due to orthodontic treatment and endodontic complications besides caries and periodontal reasons. Figure 1 demonstrates the frequency of extracted teeth by tooth type.
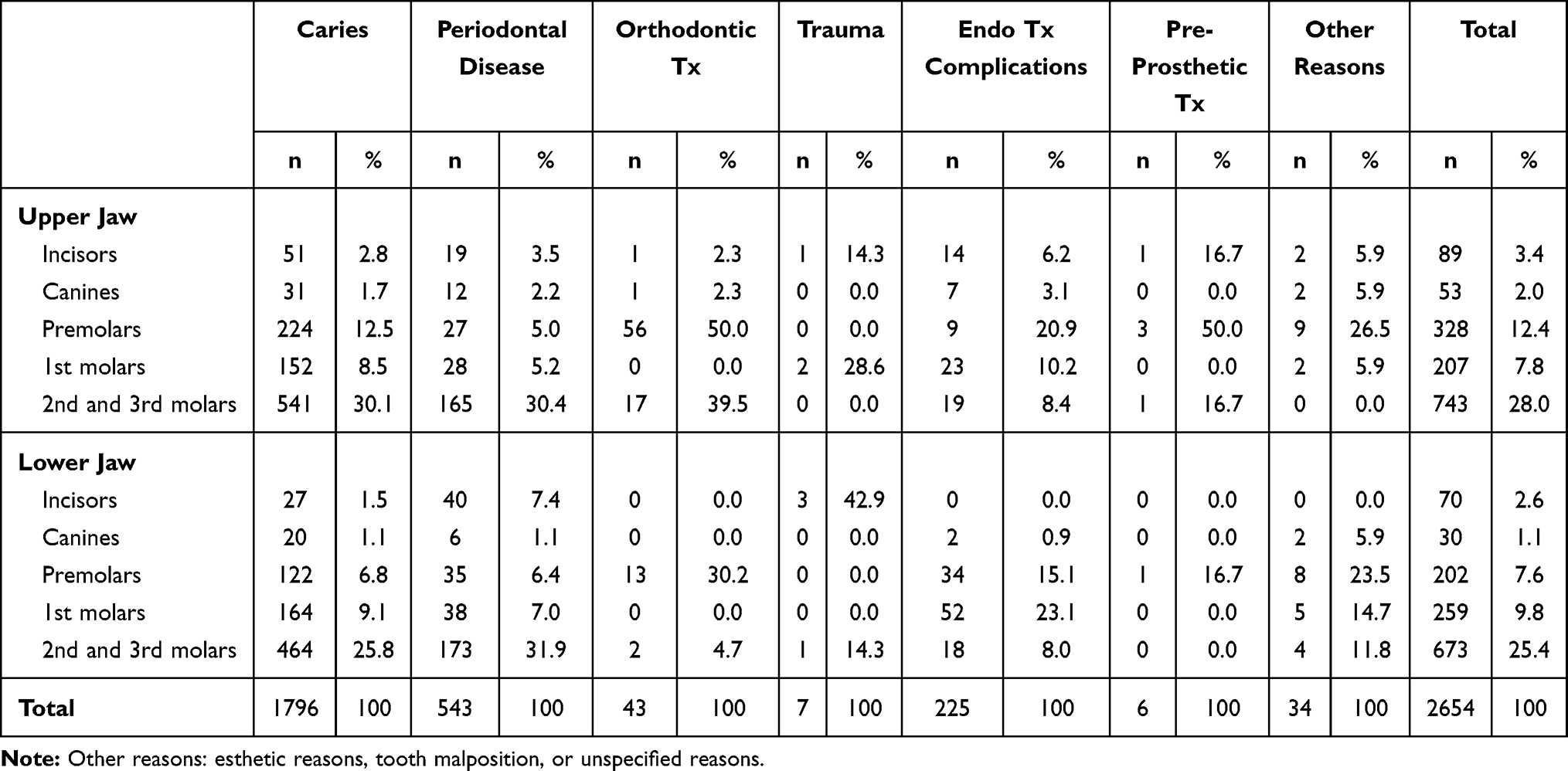 |
Table 3 Distribution of Tooth Type by Reasons for Extraction |
 |
Figure 1 Frequency of extracted teeth by tooth type. |
Discussion
The results of the current study concluded that caries (67.7%) and periodontal disease (20.5%) are the foremost reasons for tooth extractions at Kuwait University Dental Clinic. This finding is in agreement with the majority of previous studies conducted within the same region, such as Saudi Arabia, Yemen, and Kuwait, as well as internationally, in Italy, Greece, and Iran, where caries was the primary reason for tooth extraction followed by periodontal disease.7–10,18,19 However, in other studies, periodontal disease ranked higher than caries as a reason for tooth loss.12–14 These studies were conducted in private practice settings where most of the patients that were periodontally involved aged 40 years and above. Third common reason for tooth extraction was endodontic treatment complications, 225 (8.5%). Previous studies by Pretzl et al and Suzuki et al have explained that root canal treatment had a significant effect on tooth loss. They explained that root canal therapy might cause deterioration of furcation lesions in molars, root fracture, and recurrent carious lesions.20,21
In the current study, there was no significant difference between genders although male patients had more extractions than female patients. It is noteworthy to mention that male patients displayed a significant association with periodontal disease, however, the correlation association was moderate. This finding was also reported in previous studies.15–17 These studies rationalized the higher number of tooth extraction among males due to less interest in adhering to dental maintenance and recall programs plus common smoking habits among males.
The mean number of tooth loss in the present study was higher among older population of age groups of 51 years and higher, 3.73 ± 0.53, compared to the other groups, which is similar to other studies.2,7,10 Remarkably, in this age group, tooth loss due to periodontal disease was more common than in younger population. In addition, the correlation association test indicated a strong correlation among age and dental caries and periodontal disease. This finding has been attributed to multiple factors including the presence of systemic conditions in older population, medications, manual dexterity and oral hygiene maintenance, and genetic proneness to periodontal diseases. Dental caries, however, was the main cause of tooth extraction in patients aged 50 years and younger, a similar finding was reported by several studies and attributed it to irregular dental visits, fail to comply with oral hygiene instructions, and high sugar intake.8,10,17
With respect to education level, the highest tooth extraction frequency was among patients who held high school (50.2%) and middle school (23.0%) degrees. This finding is in agreement with other studies where tooth loss was associated with primary level of education.9,22,23 Further, there was a significant association between education level and dental caries and orthodontic treatment. This finding can be rationalized to the fact that orthodontic treatment is conducted mostly on younger/adolescent population which include extraction of premolars and non-restorable teeth.
Diabetic patients reported a significant association with tooth extraction due to periodontal disease while smokers reported a significant association with tooth extraction due to caries, both with moderate correlation. Passarelli et al have reported that diabetes and smoking habits have a direct association with tooth loss.8 On the other hand, Kawahara et al have reported that there was no clear correlation between systemic diseases, such as diabetes, and tooth loss.15
With regards to tooth types, the most commonly extracted tooth type was molars due to dental caries primarily followed by periodontal diseases. This finding is in agreement with Passarelli et al and Jafarian et al where they reasoned it to the anatomical development of molar tooth type that results in the formation of grooves and fissures making them more susceptible to dental caries. Additionally, first and second molars erupt in the oral cavity at a relatively young age making them more prone to dental caries and periodontal attacks.8,9
Lower incisors were extracted mostly due to periodontal reasons. This observation has been reported previously, and a possible explanation was attributed to the fact that lower incisors are less prone to caries as they are protected by the tongue, but are more likely to be retained in older population where they are more prone to periodontal disease.7–9 Premolars were extracted mainly due to orthodontic reasons and endodontic treatment complications, at a lesser extent. This can be attributed to the fact that premolars are extracted either for relieve of crowding or for facial profile change. The least common extracted teeth were the canines; a possible justification is that canines have prominent smooth clinical crowns and large bulbous roots with an extensive periodontal attachment making them resistible to caries and periodontal diseases.
According to the results of the present study, dental caries and periodontal disease continue to be the foremost causes of permanent tooth extraction. This emphasizes the role of the oral healthcare provider in raising oral health awareness among the general population on one side and provide preventative measures for patients with a high risk for caries or periodontal disease.
This study had some limitations that might be beneficial to explore in future projects. For instance, oral hygiene status needs to be explored in association with the number of extracted teeth. In addition, caries risk assessment tests and periodontal screening tests including Streptococcus mutans, Lactobacilli, and Porphyromonas gingivalis species count, in addition to saliva buffering capacity and production tests can be explored in order to test the degree of association with the reasons of tooth extraction.
Conclusion
We found that dental caries, periodontal disease, and endodontic treatment complications were the most common causes of extraction. However, this study has provided that age, diabetes, and smoking habits were found to be suitable forecasters for permanent tooth loss as they displayed strong statistical association. Further studies are needed to provide an overview of the role of the oral healthcare provider in raising awareness of oral health and provide efficient screening strategies for caries and periodontal disease in order to shift the paradigm of dental health from oral disease treatment to disease prevention.
Acknowledgments
The author would like to thank Mrs Daiven Manuel for assisting in data collection and data entry.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Gerritsen AE, Allen PF, Witter DJ, Bronkhorst EM, Creugers NH. Tooth loss and oral health-related quality of life: a systematic review and meta-analysis. Health Qual Life Outcomes. 2010;8:126. doi:10.1186/1477-7525-8-126
2. Passarelli PC, Lajolo C, Pasquantonio G, et al. Influence of mandibular third molar surgical extraction on the periodontal status of adjacent second molars. J Periodontol. 2019;90(8):847–855. doi:10.1002/JPER.18-0415
3. Lee CY, Chang YY, Shieh TY, Chang CS. Reasons for permanent tooth extractions in Taiwan. Asia Pac J Public Health. 2015;27(2):Np2350–Np2357. doi:10.1177/1010539512448814
4. McCaul LK, Jenkins WM, Kay EJ. The reasons for extraction of permanent teeth in Scotland: a 15-year follow-up study. Br Dent J. 2001;190(12):658–662. doi:10.1038/sj.bdj.4801068
5. Richards W, Ameen J, Coll AM, Higgs G. Reasons for tooth extraction in four general dental practices in South Wales. Br Dent J. 2005;198(5):275–278. doi:10.1038/sj.bdj.4812119
6. Jovino-Silveira RC, Caldas Ade F, de Souza EH, Gusmão ES. Primary reason for tooth extraction in a Brazilian adult population. Oral Health Prev Dent. 2005;3(3):151–157.
7. Al-Shammari KF, Al-Ansari JM, Al-Melh MA, Al-Khabbaz AK. Reasons for tooth extraction in Kuwait. Med Princ Pract. 2006;15(6):417–422. doi:10.1159/000095486
8. Passarelli PC, Pagnoni S, Piccirillo GB, et al. Reasons for tooth extractions and related risk factors in adult patients: a cohort study. Int J Environ Res Public Health. 2020;17(7):2575. doi:10.3390/ijerph17072575
9. Jafarian M, Etebarian A. Reasons for extraction of permanent teeth in general dental practices in Tehran, Iran. Med Princ Pract. 2013;22(3):239–244. doi:10.1159/000345979
10. Chrysanthakopoulos NA. Reasons for extraction of permanent teeth in Greece: a five-year follow-up study. Int Dent J. 2011;61(1):19–24. doi:10.1111/j.1875-595X.2011.00004.x
11. Aida J, Morita M, Akhter R, Aoyama H, Masui M, Ando Y. Relationships between patient characteristics and reasons for tooth extraction in Japan. Community Dent Health. 2009;26(2):104–109.
12. Ong G. Periodontal reasons for tooth loss in an Asian population. J Clin Periodontol. 1996;23(4):307–309. doi:10.1111/j.1600-051X.1996.tb00550.x
13. Matthews DC, Smith CG, Hanscom SL. Tooth loss in periodontal patients. J Can Dent Assoc. 2001;67(4):207–210.
14. Stadler AF, Mendez M, Oppermann RV, Gomes SC. Tooth loss in patients under periodontal maintenance in a private practice: a retrospective study. Braz Dent J. 2017;28(4):440–446. doi:10.1590/0103-6440201701476
15. Kawahara H, Inoue M, Okura K, Oshima M, Matsuka Y. Risk factors for tooth loss in patients undergoing mid-long-term maintenance: a retrospective study. Int J Environ Res Public Health. 2020;17(17):6258. doi:10.3390/ijerph17176258
16. Costa FO, Lages EJ, Cota LO, Lorentz TC, Soares RV, Cortelli JR. Tooth loss in individuals under periodontal maintenance therapy: 5-year prospective study. J Periodontal Res. 2014;49(1):121–128. doi:10.1111/jre.12087
17. Yoshino K, Ito K, Kuroda M, Sugihara N. Tooth loss in problem-oriented, irregular, and regular attenders at dental offices. Bull Tokyo Dent Coll. 2016;57(1):11–19. doi:10.2209/tdcpublication.57.11
18. Alesia K, Khalil HS. Reasons for and patterns relating to the extraction of permanent teeth in a subset of the Saudi population. Clin Cosmet Investig Dent. 2013;5:51–56. doi:10.2147/CCIDE.S49403
19. Noman NA, Aladimi AA, Alkadasi BA, et al. social habits and other risk factors that cause tooth loss: an associative study conducted in taiz governorate, Yemen. J Contemp Dent Pract. 2019;20(4):428–433. doi:10.5005/jp-journals-10024-2534
20. Pretzl B, Eickholz P, Saure D, Pfefferle T, Zeidler A, Dannewitz B. Endodontic status and retention of molars in periodontally treated patients: results after 10 or more years of supportive periodontal therapy. J Clin Periodontol. 2016;43(12):1116–1123. doi:10.1111/jcpe.12621
21. Suzuki S, Yoshino K, Takayanagi A, et al. Number of non-vital teeth as indicator of tooth loss during 10-year maintenance: a retrospective study. Bull Tokyo Dent Coll. 2017;58(4):223–230. doi:10.2209/tdcpublication.2016-0044
22. Silva-Junior MF, Sousa ACC, Batista MJ, Sousa M. Oral health condition and reasons for tooth extraction among an adult population (20–64 years old). Cien Saude Colet. 2017;22(8):2693–2702. doi:10.1590/1413-81232017228.22212015
23. Hamasha AA, Al Qudah MA, Bataineh AB, Safadi RA. Reasons for third molar teeth extraction in Jordanian adults. J Contemp Dent Pract. 2006;7(5):88–95. doi:10.5005/jcdp-7-5-88
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.