Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Real-World Treatment Patterns in Patients with Atopic Dermatitis Initiating Ruxolitinib Cream: A 12-Month Follow-Up Analysis of a US Payer Claims Database
Authors Liu J, Desai K, Chen HYP, Teng CC, Sturm D ![]() , Stockbower GE, Willey VJ
, Stockbower GE, Willey VJ
Received 24 September 2025
Accepted for publication 13 February 2026
Published 11 April 2026 Volume 2026:18 569871
DOI https://doi.org/10.2147/CEOR.S569871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Jinan Liu,1 Karishma Desai,2 Hung-Yuan P Chen,2 Chia-Chen Teng,2 Daniel Sturm,3 Grace E Stockbower,2 Vincent J Willey2
1US Health Economics and Outcomes Research, Incyte Corporation, Wilmington, DE, USA; 2Health Economics and Outcomes Research, Carelon Research, Inc., Wilmington, DE, USA; 3US Medical Affairs, Incyte Corporation, Wilmington, DE, USA
Correspondence: Jinan Liu, US Health Economics and Outcomes Research, Incyte Corporation, 1801 Augustine Cut-Off, Wilmington, DE, 19803, USA, Tel +1 504 810 7282, Email [email protected]
Purpose: This study describes a cohort of US commercially insured and Medicare Advantage patients with atopic dermatitis (AD) using ruxolitinib cream therapy and characterizes their treatment patterns before ruxolitinib cream initiation and during a 12-month follow-up.
Patients and Methods: This retrospective, observational cohort study analyzed longitudinal administrative claims and social drivers of health data for patients diagnosed with AD and treated with ruxolitinib cream. Patient characteristics, treatment patterns, and healthcare resource utilization were described for the 6 months before and 12 months after ruxolitinib cream initiation.
Results: The overall population (N=556) had a mean (SD) age of 40.3 (17.3) years and was 60.8% female, with 71.9% of patients being in the upper 2 socioeconomic status index score quartiles. Baseline predominant treatment patterns (overall cohort) included no treatment (26.6%), topical corticosteroids (53.4%), biologics (22.5%), systemic corticosteroids (20.9%), topical calcineurin inhibitors (14.9%), and topical phosphodiesterase-4 inhibitors (6.7%). Post-index treatment patterns showed a decreasing trend in corticosteroid use, with topical corticosteroid use dropping from 31.3% in months 1– 6 to 26.6% in months 7– 12, and systemic corticosteroid use stabilizing after an initial decrease (16.0% to 16.6%). However, the mean cumulative prednisone-equivalent dose among patients using systemic corticosteroids decreased overall by 28.9%, from 402.1 mg at baseline to 362.3 mg during months 1– 6 and to 285.7 mg during months 7– 12 of follow-up. Among the biologic-naïve cohort (n=431), 90.0% remained biologic-free during follow-up, and among the biologic-experienced cohort (n=125), 14.4% discontinued biologics during follow-up. The percentage of patients with healthcare encounters for AD decreased from 85.3% at baseline to 70.0% during follow-up.
Conclusion: The reduced use of other AD treatments, including corticosteroids, and the high proportion of patients remaining biologic-free during the 12-month follow-up support the durability of the effectiveness of ruxolitinib as a therapeutic option for adults and adolescents with AD.
Plain Language Summary: This study was conducted to see if using ruxolitinib cream was effective in treating eczema, also known as atopic dermatitis, over a full year of observing patients being treated with ruxolitinib cream. Insurance claims of patients with atopic dermatitis were evaluated for 6 months before and 12 months after starting ruxolitinib cream. Medication orders and healthcare provider visits to manage atopic dermatitis were observed to look for patterns. Before starting ruxolitinib cream, 27% of patients were untreated, 53% were treated with steroid creams, 23% were treated with advanced therapies, and 21% were treated with steroid tablets. After starting ruxolitinib cream, about half of the patients were able to stop using steroid creams, and one-fifth were able to stop taking steroid tablets. The patients who were taking steroid tablets before using ruxolitinib cream were able to decrease their dose by about 30%. Overall, most patients did not need to start more complex injectable therapies, and patients needed fewer doctor visits to manage their atopic dermatitis after starting ruxolitinib cream. This study suggests that ruxolitinib cream may be an effective treatment for adults and adolescents with atopic dermatitis.
Keywords: medication trends, dermatological treatments, therapeutic outcomes, eczema, Janus kinase, topical
Introduction
Atopic dermatitis (AD), a chronic, inflammatory skin disease, affects 10% of children and approximately 5–10% of adults in the US.1–3 Itching, sleep disturbance, and skin pain lead to reduced quality of life (QoL) in patients with AD across severity levels.4 Because AD follows a heterogeneous course, multiple strategies based on symptom severity, location of lesions, and treatment history are needed for flare management.5–7
Current guidelines recommend that the management of AD treatment begin with the foundation of emollients and prescription topical therapies due to their effectiveness and tolerability.5,7,8 Recent additions to the topical armamentarium for AD include crisaborole (approved in 2016) and ruxolitinib cream (approved in 2021), both approved for mild to moderate AD.9–11 For those with widespread or more severe AD, QoL impairment, or refractory AD, phototherapy or systemic therapies may be considered.5 Recently introduced novel prescription-based systemic treatment options that are strongly recommended for moderate to severe AD include biologic treatments (dupilumab and tralokinumab) and Janus kinase inhibitors (upadacitinib, abrocitinib, and baricitinib).5,8 Systemic therapies with conditional or mixed recommendations include the immunosuppressants methotrexate, azathioprine, cyclosporine, and mycophenolate mofetil.5,8 Due to its short-lived effectiveness, the possibility of rebound AD flares after discontinuation, and its adverse reaction profile—which includes weight gain, insomnia, adrenal insufficiency, infection risk, bone density loss, and growth impairment—systemic use of corticosteroids is discouraged for chronic mild, moderate, and severe AD.5,8
Although ruxolitinib cream has demonstrated safety and efficacy in clinical trials, its role among other treatment options in real-world practice remains under-researched.12–28 As a potential alternative to steroidal and systemic therapies, it is important to continuously assess the effects of ruxolitinib cream on the use of other treatments to provide insights to care providers, patients, and payers. Owing to the episodic nature of AD symptom intensity, it is especially important to evaluate the impact of ruxolitinib cream over a longer duration of treatment use. A prior study by the same team investigated the short-term effects of ruxolitinib cream on the utilization of other therapies, yet no research has explored the durability of its impact on utilization patterns over a longer time period.29 Follow-up over a full year can also more effectively account for the episodic nature of AD flares, including but not limited to the seasonal variation in symptom severity.30 Therefore, the purpose of this subsequent study was to describe a cohort of US commercially insured and Medicare Advantage patients with AD using ruxolitinib cream therapy and to characterize their treatment patterns before the initiation of ruxolitinib cream and during a 12-month follow-up period.
Materials and Methods
Study Design and Data Source
This retrospective observational cohort study was conducted utilizing longitudinal administrative claims data derived from the Healthcare Integrated Research Database (HIRD®), which uses a combination of fully adjudicated medical and pharmacy claims as well as health plan enrollment data for over 90 million lives from 14 Blue Cross and/or Blue Shield licensed plans.31 In addition, the HIRD was linked to community-level social drivers of health (SDOH) data from the American Community Survey (ACS) using 9-digit zip codes.32 The ACS is administered by the US Census Bureau and collects information from approximately 2.0 to 2.5 million randomly sampled households per year. The ACS data report on several neighborhood-level characteristics relevant to SDOH, including demographics (age and race), education, income, living condition (home value, ownership type, and crowding), employment, and family composition (single parent and number of children per household). These indicators represent 5-year averages; specifically, the 2019 ACS data are averages of the 2015 to 2019 annual estimates.
This study was conducted in accordance with the principles of the Declaration of Helsinki. All protected health information data were accessed as a limited data set under an approved data use agreement with a covered entity in a Health Insurance Portability and Accountability Act–compliant manner. As the analysis dataset was fully de-identified, institutional board review was not required.
Time Periods
The study period included data collected between April 1, 2021, and March 31, 2023. The patient identification period extended from October 1, 2021, to March 31, 2022. The index date was the date of the first observed claim of ruxolitinib cream within the patient identification period. The baseline period included the 6-month period prior to but not including the index date. The follow-up period began with the patient’s index date and continued to the end of the planned observation period of 12 months after the index date (Supplemental Figure 1).
Study Population
To be included in the analysis of individuals using ruxolitinib cream for AD, patients 12 years of age and older were required to have ≥1 claim for ruxolitinib cream during the patient identification period, ≥6 months of continuous pre-index health plan enrollment, ≥12 months of continuous post-index health plan enrollment, and ≥1 claim with a diagnosis of AD during the baseline period or on the index date. Patients were excluded from the analysis if they had received a vitiligo diagnosis during the baseline period. Subgroups were defined based on baseline utilization of biologics (monoclonal antibodies) indicated for the treatment of AD (biologic-experienced cohort and biologic-naïve cohort).
Outcomes
Outcomes of interest included baseline patient demographics, SDOH, and clinical characteristics for the overall and subgroup cohorts. SDOH data were obtained from the 2019 ACS and were combined into a composite socioeconomic status (SES) index score based on 7 variables (unemployment rate, poverty rate, median household income, median home value, rate of no high school diploma, rate of college degree, and crowding).32 The SES index score was reported in quartiles, with “4” indicating the top quartile (most advantaged) and “1” indicating the bottom quartile (least advantaged).33 Additionally, patient-level race and ethnicity were captured through a combination of clinical/electronic health records, enrollment records, and imputation through Bayesian Improved Surname and Geocoding (RAND International, Santa Monica, CA, USA; AmeriLINK Consumer Database and Ethnic Technologies, South Hackensack, NJ, USA).34,35 Diagnoses and procedures for both outpatient and inpatient visits/stays were identified by International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM diagnostic), ICD-10 Procedure Coding System, Current Procedural Terminology, and Healthcare Financing Administration Common Procedure Coding System codes. The Elixhauser Comorbidity Index (ECI) is a validated summary measure that quantifies overall comorbidity burden and predicts outcomes, such as in-hospital mortality, by aggregating 30 predefined comorbid conditions derived from ICD-10-CM codes. We used the ICD-10-CM–based summary score developed and validated by Mehta et al (2022), which provides a single, weighted comorbidity score for the baseline period optimized for use in contemporary administrative data.36 Outpatient pharmacy claims were captured by National Drug Codes. Baseline and follow-up treatment patterns and healthcare resource utilization (HCRU) and costs were also described. All healthcare expenditures were a sum of plan- and patient-paid expenses and were adjusted to 2022 United States dollars.37
Analyses
Descriptive statistics, including means and standard deviations for continuous variables and frequencies for categorical variables, were computed for all variables for the overall sample population and the subgroups. No hypothesis testing was conducted (over time or across subgroups). Analyses were conducted using a combination of the Instant Health Data platform (Panalgo, Boston, MA, USA), R version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria), and Statistical Analysis Software (SAS) Enterprise Guide version 9.3 (SAS Institute Inc., Cary, NC, USA).
Results
Baseline Sociodemographic Characteristics
From the overall sample of 1563 patients with ≥1 prescription claims for ruxolitinib cream during the intake period, 556 met all inclusion and exclusion criteria and were included in the final sample. This population was divided into a cohort of patients with baseline use of biologics (biologic-experienced; n=125) and without baseline use of biologics (biologic-naïve; n=431) (Table 1). Baseline sociodemographic characteristics for the overall population as well as the 2 cohorts are presented in Table 1. The biologic-experienced cohort had a mean (SD) age of 41.9 (17.63) years, with 57.6% of patients being female and 60.8% identifying as non-Hispanic White; this cohort was economically diverse. The biologic-naïve cohort had a mean (SD) age of 39.9 (17.22) years, with 61.7% of patients being female and 65.2% identifying as non-Hispanic White; this cohort had fewer patients living in neighborhoods with the lowest SES index score quartile (9.1%) (Table 1).
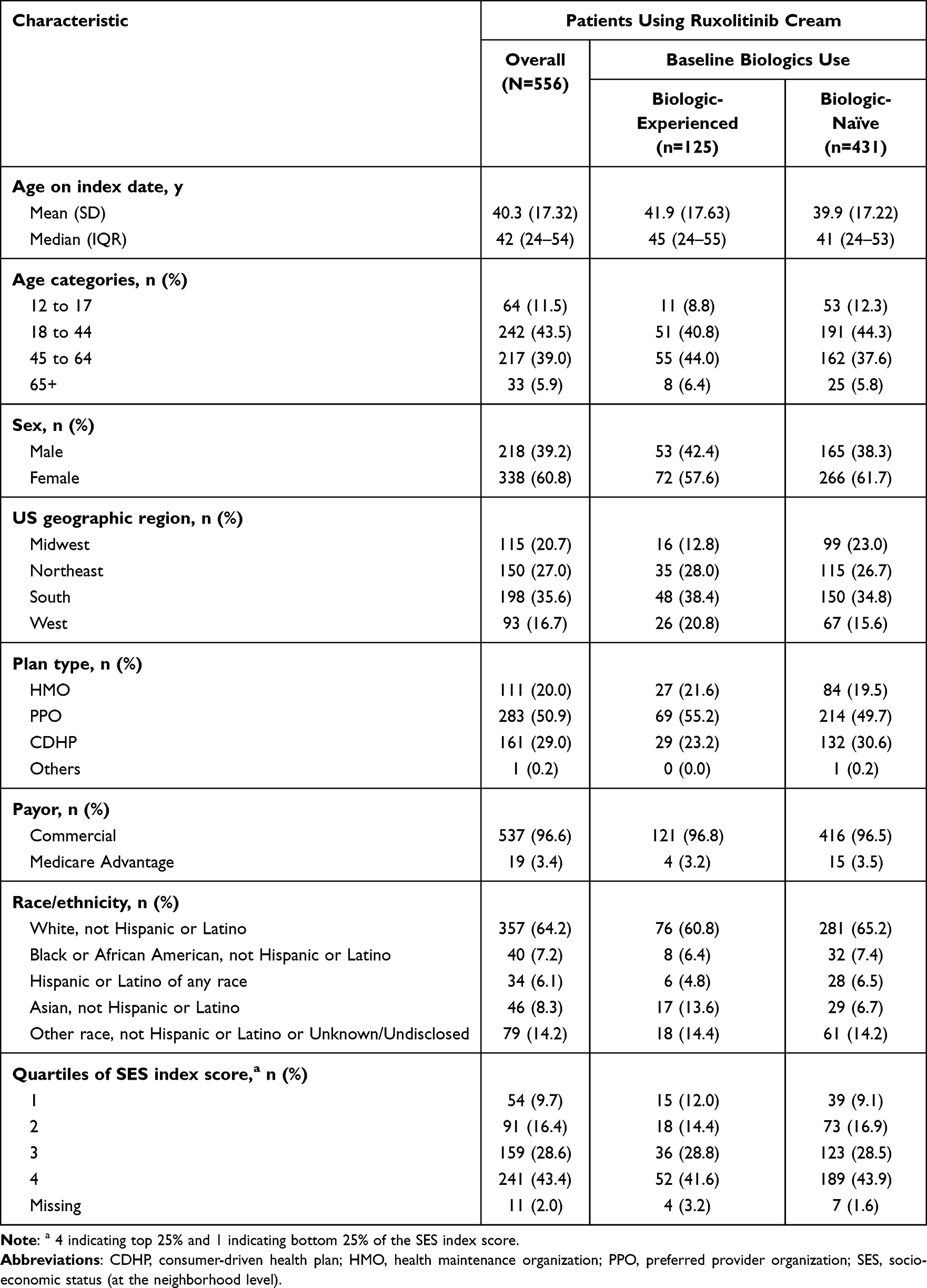 |
Table 1 Baseline Sociodemographic Characteristics |
Baseline Clinical Characteristics
Among patients using ruxolitinib cream, the mean (SD) ECI score was 0.96 (1.48), suggesting a relatively low burden of comorbid conditions. The top 3 ECI comorbidities in the overall population included hypertension (14.9%), chronic pulmonary disease (13.9%), and depression (13.1%), which were also the top 3 most prevalent ECI comorbidities among the biologic-experienced cohort (19.2%, 18.4%, and 16.0%, respectively; Table 2) and the biologic-naïve cohort (13.7%, 12.5%, and 12.3%, respectively; Table 2). Other comorbidities of interest that were most prevalent in the overall population included allergic rhinitis (16.7%), anxiety (12.9%), and asthma (12.6%); these were prevalent in the biologic-experienced cohort (20.0%, 16.0%, and 17.6%, respectively) and in the biologic-naïve cohort (15.8%, 12.1%, and 11.1%, respectively).
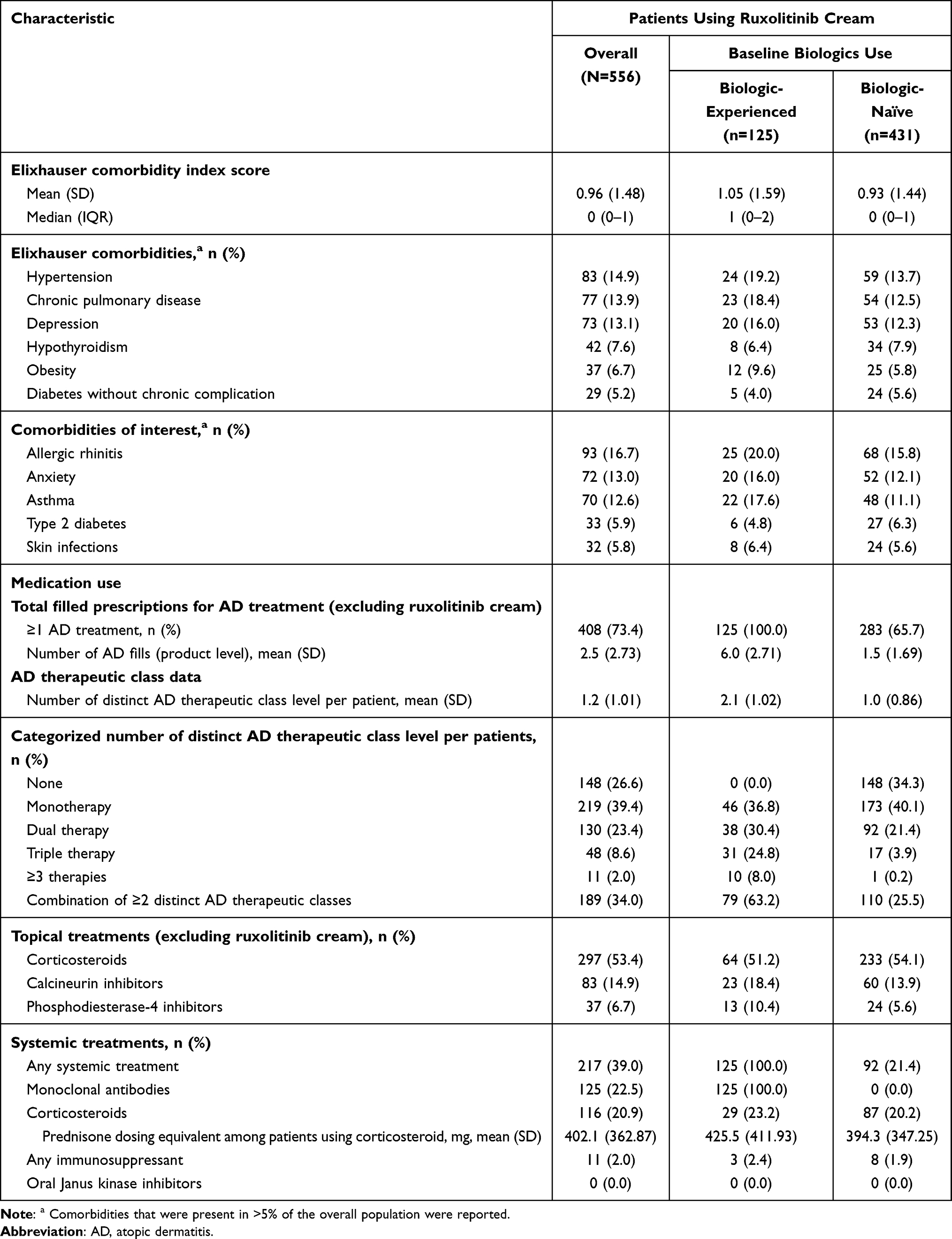 |
Table 2 Baseline Clinical Characteristics |
The baseline AD treatment regimen in the overall cohort was managed for most patients with no AD treatment (26.6%), monotherapy (39.4%), or dual therapy (23.4%). Topical corticosteroids (TCS) were used by 53.4%, biologics by 22.5%, and systemic corticosteroids by 20.9%.
Treatment Patterns
For nearly a third of AD patients (29.1%), ruxolitinib cream was the only AD therapy used in the 12-month follow-up period. Patients had a mean (SD) of 2.1 (1.77) fills for ruxolitinib cream over the 12-month follow-up period. A reduction in the use of other types of AD treatment was seen, with 41.9% of patients not receiving a new class of AD treatment added to their baseline therapy during the follow-up period. When assessing the 12-month period divided into 2 consecutive 6-month intervals, the proportions of patients not receiving a new class of AD treatment were 72.5% and 73.9% for the first and last 6 months, respectively. The mean (SD) number of distinct AD therapeutic classes per patient, excluding ruxolitinib cream, decreased from 1.2 (1.01) during baseline to 0.8 (0.86) during the first 6 months of follow-up and 0.8 (0.87) during the 7–12-month follow-up period.
The use of topical agents decreased during the follow-up period. The use of TCS decreased from 53.4% at baseline to 26.6% during the 7–12-month follow-up period (50.2% reduction). The use of topical calcineurin inhibitors (TCI) decreased from 14.9% at baseline to 5.0% during the 7–12-month follow-up period (66.4% reduction), and the use of topical phosphodiesterase-4 (PDE-4) inhibitors decreased from 6.7% at baseline to 1.6% during the 7–12-month follow-up period (76% reduction; Figure 1). In the overall population, among patients using TCS, high potency TCS and ultra-high potency TCS use decreased from 11.7% (n=65) and 19.4% (n=108) at baseline to 6.7% (n=37) and 12.8% (n=71) during the first 6 months of follow-up and to 4.7% (n=26) and 11.0% (n=61) during the 7–12-month follow-up period, respectively.
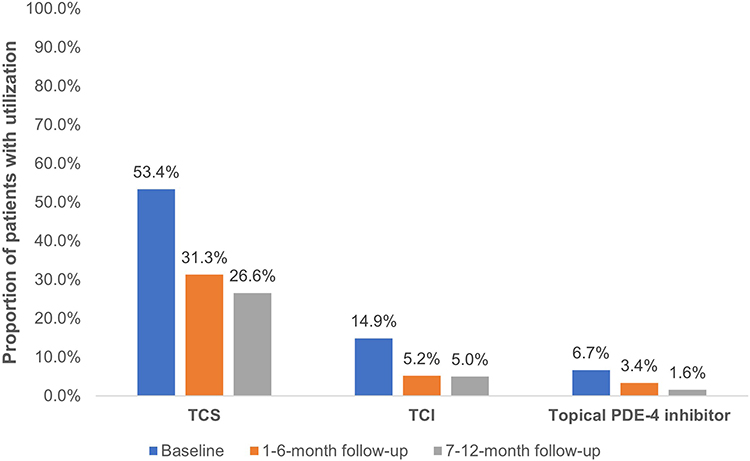 |
Figure 1 Topical Treatment Use for AD Before and After Initiation of Ruxolitinib Cream.a This graph illustrates the proportion of patients using TCS, TCI, and topical PDE-4 inhibitors across 3 distinct time periods: at baseline, 1–6-month follow-up, and 7–12-month follow-up. For example, 53.4% of patients received TCS during baseline, which decreased to 31.3% during the 1–6-month period and 26.6% during the 7–12-month period. Similar decreases were noted for the number of patients on TCI and topical PDE-4 inhibitors. Abbreviations: AD, atopic dermatitis; PDE-4, phosphodiesterase-4; TCI, topical calcineurin inhibitors; TCS, topical corticosteroids. Note: aThe follow-up period is shown in intervals of 1–6 months and 7–12 months. |
When evaluated among the overall population, systemic corticosteroids were used by 20.9% at baseline, by 16.0% of patients in the 1–6-month follow-up period, and by 16.6% of patients during the 7–12-month follow-up period (Figure 2). Within the biologic-experienced cohort, systemic corticosteroid use decreased from 23.2% at baseline to 14.4% during the 1–6-month follow-up period and 19.2% during the 7–12-month follow-up period; within the biologic-naïve cohort, it decreased from 20.2% at baseline to 16.5% during the 1–6-month follow-up period and 15.8% during the 7–12-month follow-up period. In the overall cohort, the mean cumulative prednisone-equivalent dose among all patients (Figure 2A) was reduced by 43.6% between baseline and the 7–12-month follow-up period. The cumulative prednisone-equivalent dose specifically among patients using corticosteroids (Figure 2B) decreased from a mean (SD) of 402.1 (362.87) mg during baseline (approximating 2.2 mg/day on average) to 285.7 (259.56) mg during the 7–12-month follow-up period (approximating 1.4 mg/day on average), representing a 28.9% reduction.
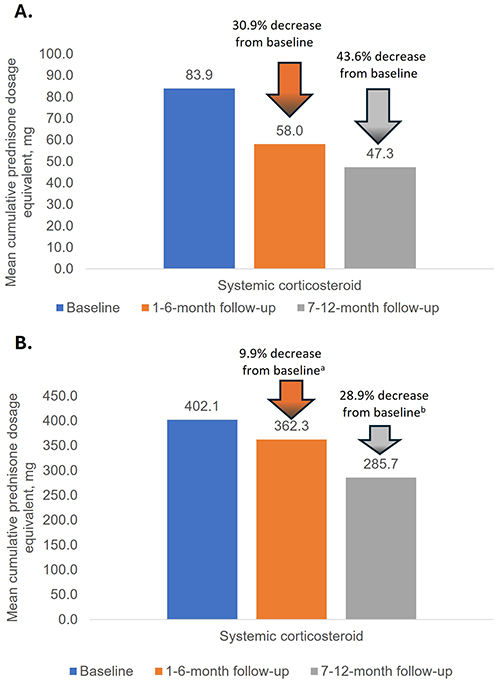 |
Figure 2 Systemic Corticosteroid Use Before and After Initiation of Ruxolitinib Cream. (A) Prednisone-Equivalent Dose Among the Overall Population (N=556). This graph illustrates the prednisone-equivalent dose across 3 distinct time periods: at baseline, 1–6-month follow-up, and 7–12-month follow-up. The cumulative prednisone dose equivalent decreased by 30.9% during months 1–6 and by 43.6% during months 7–12 for the overall population. (B) Prednisone-Equivalent Dose Among Patients Using Corticosteroids. This graph illustrates the prednisone-equivalent dose across 3 distinct periods: at baseline, 1–6-month follow-up, and 7–12-month follow-up. Among patients using corticosteroids, there was a 9.9% reduction in cumulative prednisone dose equivalent during the 1–6-month follow-up period and a 28.9% reduction during the 7–12-month follow-up period. Notes: a10% decrease in mean cumulative dosage and 23% fewer patients using systemic corticosteroids. b30% decrease in mean cumulative dosage and 21% fewer patients using systemic corticosteroids. |
Among the biologic-naïve cohort (Figure 3), 90% did not initiate biologic therapy during the follow-up period. Also, approximately 14% of patients who received AD biologic therapy during the baseline period discontinued biologic use in the 12-month follow-up period after ruxolitinib cream initiation (Figure 4). The total use of biologics remained relatively constant for the duration of the study (22.5% at baseline, 24.8% during the 1–6-month follow-up period, and 23.2% during the 7–12-month follow-up period in the overall cohort). Use of immunosuppressants was low at baseline (2.0% of patients in the overall population) and remained low throughout the follow-up periods (2.0% during the 1–6-month follow-up period and 1.4% during the 7–12-month follow-up period).
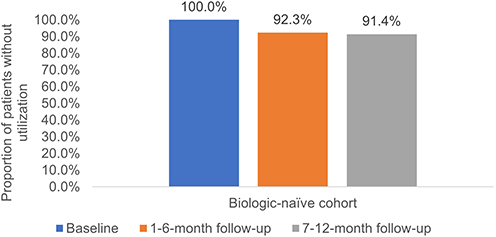 |
Figure 3 Biologics Use for AD Before and After Initiation of Ruxolitinib Cream Among the Biologic-Naïve Cohort (n=431). This graph depicts the proportion of patients who maintained biologic-naïve status across 3 time periods: at baseline, 1–6-month follow-up, and 7–12-month follow-up. Among the cohort that was biologic-naïve at baseline, a consistently high proportion did not initiate biologics during the follow-up periods. Abbreviation: AD, atopic dermatitis. |
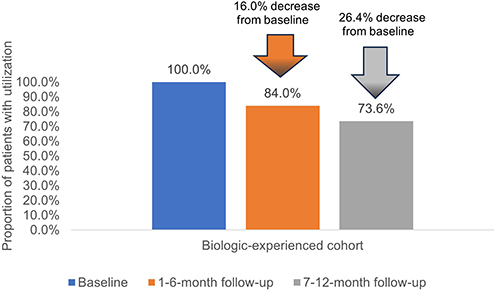 |
Figure 4 Biologics Use for AD Before and After Initiation of Ruxolitinib Cream Among Biologic-Experienced Cohort (n=125). This graph depicts the follow-up utilization of biologics among the cohort of patients who initiated biologic therapy during the baseline period. The proportion of patients continuing biologic use declined, showing a 16.4% decrease during months 1–6 and a 26.4% decrease during months 7–12 across the overall population. Abbreviation: AD, atopic dermatitis. |
Healthcare Resource Utilization and Cost
Healthcare resource utilization at baseline was prevalent among the overall population and remained high during the 12-month follow-up period (Figure 5). AD-related outpatient encounters were lower during follow-up (70.0%) compared with baseline (85.3%; Figure 5). Reductions in utilization were noted in the biologic-experienced cohort, decreasing from 92.8% of patients with utilization at baseline to 83.2% during the 12-month follow-up, whereas the biologic-naïve cohort decreased utilization from 83.1% at baseline to 66.1% during the 12-month follow-up.
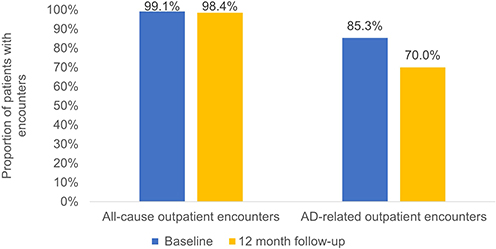 |
Figure 5 Healthcare Resource Utilization at Baseline* and Follow-up Among Patients With ≥1 Visit (N=556). This graph depicts the proportion of patients who had all-cause and AD-related outpatient claims across 2 time periods: at the 6-month baseline and the 12-month follow-up. *Baseline time period was 6 months, whereas the follow-up time period was 12 months. Abbreviation: AD, atopic dermatitis. |
All-cause medical healthcare costs were a mean (SD) of $5888.30 ($12,668.73) over the 6-month baseline period and $12,791.75 ($29,581.77) over the 12-month follow-up, with AD-related outpatient medical costs contributing $244.25 ($360.17) during baseline and $330.92 ($838.58) during follow-up. AD-related pharmacy costs were $3678.86 ($7332.07) for the 6-month baseline period and $13,181.21 ($16,752.41) over the 12-month follow-up, with ruxolitinib cream contributing $4011.71 ($3418.76) of the cost during this period. The biologic-experienced cohort had AD-related pharmacy costs of $15,759.20 ($7085.26) over the 6-month baseline period and $34,220.82 ($17,868.31) over the 12-month follow-up, whereas the biologic-naïve cohort costs were $175.28 ($428.95) and $7079.24 ($10,205.53), respectively.
Discussion
Few studies have been conducted to demonstrate the effectiveness of the recently approved topical formulation of ruxolitinib in the treatment of AD.11 In this retrospective analysis of patients who initiated ruxolitinib cream for the treatment of AD, treatment patterns were observed after initiation for a full 12 months. As summarized in Table 1, 556 patients initiated ruxolitinib cream (biologic-experienced, n=125; biologic-naïve, n=431). The population consisted primarily of insured adults (mean age, ~41 years; ~60% female; ~62% non-Hispanic White) with a low comorbidity burden (mean ECI, ~1), informing generalizability to comparable populations. Outcomes were reported separately for months 1–6 and 7–12 to distinguish early from later follow-up, examine temporal patterns (including potential seasonality), and assess whether observed treatment and utilization patterns persisted over time.
Overall, a reduction in the use of other AD treatments was observed in the first 6 months, and this was a durable response, continuing for the remaining 7–12-month follow-up period. During follow-up, use of other topical agents was lower than during baseline across observed classes. At the present time, other published studies regarding the effectiveness of ruxolitinib cream for AD treatment over a longer duration are limited to two Phase 3 studies: TRuE-AD1 and TRuE-AD2, with a total population of 1249 individuals.14,18,20 In these analyses, many patients achieved clinically meaningful responses within 8 weeks, and over the additional 44 weeks of follow-up, disease control was maintained.14,18,20 Among patients who did not achieve therapeutic success at 8 weeks, by the end of the 44-week additional follow-up, many patients (55.2% of those treated with 0.75% cream and 56.3% of those treated with 1.5% cream) did achieve therapeutic success.20 The results of the present study add to the evidence beyond randomized controlled trials of the durable response of AD symptoms to treatment with ruxolitinib cream. In addition, this study contributes to the real-world body of literature by extending follow-up to a full year for each patient, so any effect of seasonality on AD flares and subsequent treatment is consistent across the study population.
In the analysis of the use of systemic AD treatments, some important trends were noted. The use of biologic AD treatments was discontinued in a substantial portion of patients using biologics at baseline, and most patients who were not receiving biologics at baseline did not initiate biologics throughout the follow-up period. Perhaps the largest change observed was in systemic corticosteroid use. According to current guidelines, the use of systemic corticosteroids is not advised for chronic mild, moderate, or severe AD, with conditional use reserved exclusively for acute, severe exacerbations and as a short-term bridge to other systemic treatments; despite this, utilization was present in more than 20% of patients at baseline.5,8 This may be attributable to implementation lag, practice patterns predating recent guidance, and limited access to targeted alternatives.38 In the treatment pattern analysis, those who were treated with systemic corticosteroids received 402.1 mg of prednisone-equivalent cumulative dosing over 6 months. For perspective, this is roughly equivalent to 4 prednisone 6-day dose packs over the 6-month period. This prednisone-equivalent dose may be a sufficient dosing level and duration of treatment to cause serious and possibly life-threatening adverse consequences associated with high-dose or long-term use of corticosteroids, including glucocorticoid-induced bone quality and density loss, adrenal insufficiency, and serious bacterial and opportunistic infections.39–41 Prednisone utilization and equivalent dosage decreased substantially in the 1–6-month follow-up and even more deeply in the 7–12-month follow-up, which is an encouraging trend. It is interesting to note that on average, patients with AD filled only 2 prescriptions for ruxolitinib cream over the 12-month period and that even with this low frequency of use, there were meaningful reductions in the use of other AD therapies. Longer-term follow-up is warranted to assess the cost implications over time.
Individuals with AD bear a significant burden of illness from the symptoms of AD and from the iatrogenic burden of AD treatment.4,42 In a study by Silverberg et al, surveyed individuals with AD reported a lower level of satisfaction with life and a lower overall patient-reported health rating than those without AD.4 Overall, 54.4% of survey participants reported that the most burdensome AD symptom was itch, followed by excessive dryness/scaling (19.6%) and red or inflamed skin (7.2%).4 The burden of illness for patients with AD also includes comorbid mental health diseases of interest, namely anxiety and depression; both were present in more than 10% of the current study population, which falls within the published range of prevalence.43 Beyond the clinical burden of AD symptoms, the complex lifestyle modifications, including moisturizing, modified bathing practices, itch-trigger avoidance, humidifiers, loose-fitting clothing, avoiding vigorous physical activity and stress, and utilization of multiple AD treatment agents, can lead to an added iatrogenic burden.42 Individuals in the current study experienced high utilization of AD-related outpatient visits, with most patients having more than 1 visit during the 6-month baseline period. After the initiation of ruxolitinib cream, fewer patients had an AD-related outpatient visit, with a lower mean number of visits per month over the follow-up period. Coupled with the decreased utilization of AD topical treatment regimens and decreased use of systemic corticosteroids during the follow-up period, this may indicate an overall decrease in iatrogenic burden. These results, which show discontinuation of biologic AD treatment in those who were biologic-experienced at baseline, along with the majority of the biologic-naïve cohort remaining biologic-free during follow-up, demonstrate that ruxolitinib cream may offer a more economical pathway to AD management, with lower overall AD-related total pharmacy expenditures during follow-up in the biologic-naïve cohort.
Although claims data are extremely valuable for the efficient and effective examination of healthcare outcomes, treatment patterns, healthcare resource utilization, and healthcare costs, they are collected for the purpose of payment and not for research. Therefore, there are limitations associated with the use of claims data; for example, claims data do not capture the use of product samples distributed at clinician offices. Accuracy can be affected by coding errors and incomplete data. AD severity and response to therapy based on clinician physical exams and assessments are not available from claims data. The study population was limited to commercially insured and Medicare Advantage patients and may not be generalizable to the broader population. The requirement of continuous enrollment 6 months before and 12 months after the index date for the study objectives may limit the generalizability of outcomes.
Conclusion
This study evaluated 12-month real-world treatment patterns, healthcare utilization, and costs following initiation of ruxolitinib cream, a topical Janus kinase (JAK) 1/JAK2 inhibitor approved in the US in 2021 for the treatment of mild to moderate AD. The findings from this study underscore the significant impact of ruxolitinib cream on the management of AD, providing evidence for the durability of its effectiveness as a therapeutic option for both adults and adolescents. The observed reductions in other AD treatments illustrate a shift in treatment patterns, reflecting a substantial decrease in treatment regimen complexity and a lower treatment burden on patients. Over the 12-month follow-up period, there was a clear “step down” from systemic therapy use, marked by reduced reliance on systemic corticosteroids and a reduction in the mean cumulative prednisone-equivalent dose. Additionally, among the biologic-naïve cohort, 90% remained biologic-free, whereas 14% of patients who initially used biologics discontinued their use after starting ruxolitinib cream, further highlighting the role of ruxolitinib cream in potentially minimizing the need for more intensive therapies while maintaining effective management of AD. This simplification in management may enhance patient adherence and outcomes, ultimately leading to improved patient experiences. For clinicians, these trends allow for more personalized and streamlined care. This real-world evidence could benefit payers by lowering costs through a more efficient and cost-effective care pathway for managing AD while also offering data to refine budget forecasting.
Acknowledgments
The authors would like to acknowledge Elizabeth Marks, an employee of Carelon Research (Wilmington, DE), for providing medical writing support. Editorial support was provided by Citrus Health Group, Inc. (Chicago, IL) and was funded by Incyte Corporation (Wilmington, DE).
Funding
This study was funded by Incyte Corporation. Authors from Incyte Corporation were involved in study design, analysis and interpretation of results, the writing of the report, and the decision to submit the manuscript for publication.
Disclosure
Dr. Liu and Dr. Sturm are employees and shareholders of Incyte Corporation. Dr. Desai, Mr. Chen, Ms. Teng, Ms. Stockbower, and Dr. Willey are employees of Carelon Research, which received funding from Incyte Corporation to perform this research. Dr. Desai, Ms. Teng, and Dr. Willey are shareholders of Elevance Health, the parent company of Carelon Research. The authors report no other conflicts of interest in this work.
References
1. Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy. 2018;73(6):1284–13. doi:10.1111/all.13401
2. Chiesa Fuxench ZC, Block JK, Boguniewicz M, et al. Atopic dermatitis in America study: a cross-sectional study examining the prevalence and disease burden of atopic dermatitis in the US adult population. J Invest Dermatol. 2019;139(3):583–590. doi:10.1016/j.jid.2018.08.028
3. Silverberg JI, Barbarot S, Gadkari A, et al. Atopic dermatitis in the pediatric population: a cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol. 2021;126(4):417–428. doi:10.1016/j.anai.2020.12.020
4. Silverberg JI, Gelfand JM, Margolis DJ, et al. Patient burden and quality of life in atopic dermatitis in US adults: a population-based cross-sectional study. Ann Allergy Asthma Immunol. 2018;121(3):340–347. doi:10.1016/j.anai.2018.07.006
5. Davis DMR, Drucker AM, Alikhan A, et al. Guidelines of care for the management of atopic dermatitis in adults with phototherapy and systemic therapies. J Am Acad Dermatol. 2024;90(2):e43–e56. doi:10.1016/j.jaad.2023.08.102
6. Garmhausen D, Hagemann T, Bieber T, et al. Characterization of different courses of atopic dermatitis in adolescent and adult patients. Allergy. 2013;68(4):498–506. doi:10.1111/all.12112
7. Sidbury R, Alikhan A, Bercovitch L, et al. Guidelines of care for the management of atopic dermatitis in adults with topical therapies. J Am Acad Dermatol. 2023;89(1):e1–e20. doi:10.1016/j.jaad.2022.12.029
8. Chu DK, Schneider L, Asiniwasis RN, et al. Atopic dermatitis (eczema) guidelines: 2023 American Academy of Allergy, Asthma and Immunology/American College of Allergy, Asthma and Immunology Joint Task Force on Practice Parameters GRADE- and Institute of Medicine-based recommendations. Ann Allergy Asthma Immunol. 2024;132(3):274–312. doi:10.1016/j.anai.2023.11.009
9. Incyte Corporation. OPZELURA (ruxolitinib) cream, for topical use. Incyte. 2011. Available from: https://www.opzelura.com/opzelura-prescribing-information.
10. Pfizer Laboratories. EUCRISA-crisabarole ointment. Pfizer Laboratories Div Pfizer Inc. 2016. Available from: https://labeling.pfizer.com/showlabeling.aspx?id=5331.
11. United States Food & Drug Administration. Advancing health through innovation: new drug therapy approvals 2021. United States Food & Drug Administration. 2021. Available from: https://www.fda.gov/media/155227/download.
12. Blauvelt A, Kircik L, Papp KA, et al. Rapid pruritus reduction with ruxolitinib cream treatment in patients with atopic dermatitis. J Eur Acad Dermatol Venereol. 2023;37(1):137–146. doi:10.1111/jdv.18571
13. Bloudek L, Eichenfield LF, Silverberg JI, et al. Impact of ruxolitinib cream on work productivity and activity impairment and associated indirect costs in patients with atopic dermatitis: pooled results from two phase III studies. Am J Clin Dermatol. 2023;24(1):109–117. doi:10.1007/s40257-022-00734-8
14. Eichenfield LF, Simpson EL, Papp K, et al. Efficacy, safety, and long-term disease control of ruxolitinib cream among adolescents with atopic dermatitis: pooled results from two randomized phase 3 studies. Am J Clin Dermatol. 2024;25(4):669–683. doi:10.1007/s40257-024-00855-2
15. Gong X, Chen X, Kuligowski ME, et al. Pharmacokinetics of ruxolitinib in patients with atopic dermatitis treated with ruxolitinib cream: data from phase II and III studies. Am J Clin Dermatol. 2021;22(4):555–566. doi:10.1007/s40257-021-00610-x
16. Kim BS, Howell MD, Sun K, Papp K, Nasir A, Kuligowski ME. Treatment of atopic dermatitis with ruxolitinib cream (JAK1/JAK2 inhibitor) or triamcinolone cream. J Allergy Clin Immunol. 2020;145(2):572–582. doi:10.1016/j.jaci.2019.08.042
17. Kim BS, Sun K, Papp K, Venturanza M, Nasir A, Kuligowski ME. Effects of ruxolitinib cream on pruritus and quality of life in atopic dermatitis: results from a phase 2, randomized, dose-ranging, vehicle- and active-controlled study. J Am Acad Dermatol. 2020;82(6):1305–1313. doi:10.1016/j.jaad.2020.02.009
18. Papp K, Szepietowski JC, Kircik L, et al. Long-term safety and disease control with ruxolitinib cream in atopic dermatitis: results from two phase 3 studies. J Am Acad Dermatol. 2023;88(5):1008–1016. doi:10.1016/j.jaad.2022.09.060
19. Papp K, Szepietowski JC, Kircik L, et al. Efficacy and safety of ruxolitinib cream for the treatment of atopic dermatitis: results from 2 phase 3, randomized, double-blind studies. J Am Acad Dermatol. 2021;85(4):863–872. doi:10.1016/j.jaad.2021.04.085
20. Simpson EL, Kircik L, Blauvelt A, et al. Clinically relevant improvements in adults and adolescents with atopic dermatitis who did not achieve Investigator’s Global Assessment treatment success following 8 weeks of ruxolitinib cream monotherapy. J Dermatol. 2023;50(12):1523–1530. doi:10.1111/1346-8138.16975
21. Hu W, Thornton M, Livingston RA. Real-world use of ruxolitinib cream: safety analysis at 1 year. Am J Clin Dermatol. 2024;25(2):327–332. doi:10.1007/s40257-023-00840-1
22. Rosmarin D, Passeron T, Pandya AG, et al. Two phase 3, randomized, controlled trials of ruxolitinib cream for vitiligo. N Engl J Med. 2022;387(16):1445–1455. doi:10.1056/NEJMoa2118828
23. Blauvelt A, Kallender H, Sturm D, Li Q, Ren H, Eichenfield LF. Efficacy and safety of ruxolitinib cream in atopic dermatitis based on previous medication history. Dermatol Ther. 2024;14(11):3161–3174. doi:10.1007/s13555-024-01272-3
24. Eichenfield LF, Liu J, Marwaha S, Piercy J, Sturm D, Anderson P. Satisfaction with control of mild to moderate atopic dermatitis with ruxolitinib cream: US physician and patient perspectives. Dermatol Ther. 2024;14(3):685–696. doi:10.1007/s13555-024-01116-0
25. Simpson EL, Bissonnette R, Chiesa Fuxench ZC, et al. Ruxolitinib cream monotherapy demonstrates rapid improvement in the extent and signs of mild to moderate atopic dermatitis across head and neck and other anatomic regions in adolescents and adults: pooled results from 2 phase 3 studies. J Dermatol Treat. 2024;35(1):2310633. doi:10.1080/09546634.2024.2310633
26. Simpson EL, Kircik L, Blauvelt A, et al. Ruxolitinib cream in adolescents/adults with atopic dermatitis meeting severity thresholds for systemic therapy: exploratory analysis of pooled results from two phase 3 studies. Dermatol Ther. 2024;14(8):2139–2151. doi:10.1007/s13555-024-01219-8
27. Stein Gold L, Bissonnette R, Forman S, et al. A maximum-use trial of ruxolitinib cream in children aged 2-11 years with moderate to severe atopic dermatitis. Am J Clin Dermatol. 2025;26(2):275–289. doi:10.1007/s40257-024-00909-5
28. Zhou S, Lei L, Jiang L, et al. Adverse event of ruxolitinib cream: a real-world analysis based on FDA Adverse Event Reporting System from 2021 to 2024. Expert Opin Drug Saf. 2024:1–6. doi:10.1080/14740338.2024.2446432
29. Liu J, Desai K, Teng CC, et al. Atopic dermatitis treatments before and after initiation of ruxolitinib cream: 6-month follow-up analysis of a US payer claims database. Clinicoecon Outcomes Res. 2025;17:69–77. doi:10.2147/CEOR.S506043
30. Fleischer AB Jr. Atopic dermatitis: the relationship to temperature and seasonality in the United States. Int J Dermatol. 2019;58(4):465–471. doi:10.1111/ijd.14289
31. Carelon Research. Technical white paper. Carelon Research’s healthcare integrated research database (HIRD). Elevance Health. 2024. Available from: https://www.carelonresearch.com/content/dam/digital/carelon/pdf/Carelon_Research_HIRD_technical_white_paper_March_2024_fv.pdf.
32. United States Census Bureau. American community survey 5-year data (2015-2019). U.S. Department of Commerce. 2019. Available from: https://www.census.gov/data/developers/data-sets/acs-5year.html.
33. United States Census Bureau. Understanding and Using American Community Survey Data: What All Data Users Need to Know. Washington, DC: U.S. Government Publishing Office; 2024 November 8.
34. RAND Corporation. RAND Bayesian improved surname geocoding. Advancing equity through data science. 2024. Available from: https://www.rand.org/health-care/tools-methods/bisg.html.
35. Ethnic Technologies. Understand your audience. Ethnic Technologies. 2024. Available from: https://www.ethnictechnologies.com/.
36. Mehta HB, Li S, An H, Goodwin JS, Alexander GC, Segal JB. Development and validation of the summary elixhauser comorbidity score for use with ICD-10-CM-coded data among older adults. Ann Intern Med. 2022;175(10):1423–1430. doi:10.7326/M21-4204
37. United States Bureau of Labor Statistics. Consumer price index. 2022. Available from: https://www.bls.gov/cpi/home.htm.
38. Loiselle AR, Chovatiya R, Thibau IJ, Johnson JK, Guadalupe M, Smith Begolka W. Evaluating access to prescription medications in the atopic dermatitis patient population in the USA. Dermatol Ther. 2024;14(7):1811–1821. doi:10.1007/s13555-024-01205-0
39. Pelewicz K, Miskiewicz P. Glucocorticoid withdrawal-an overview on when and how to diagnose adrenal insufficiency in clinical practice. Diagnostics. 2021;11(4):728. doi:10.3390/diagnostics11040728
40. Schneeweiss MC, Perez-Chada L, Merola JF. Comparative safety of systemic immunomodulatory medications in adults with atopic dermatitis. J Am Acad Dermatol. 2021;85(2):321–329. doi:10.1016/j.jaad.2019.05.073
41. Mazzantini M, Di Munno O. Glucocorticoid-induced osteoporosis: 2013 update. Reumatismo. 2014;66(2):144–152. doi:10.4081/reumatismo.2014.787
42. Chovatiya R, Silverberg JI. Iatrogenic burden of atopic dermatitis. Dermatitis. 2022;33(6s):S17–S23. doi:10.1097/DER.0000000000000799
43. Fasseeh AN, Elezbawy B, Korra N, et al. Burden of atopic dermatitis in adults and adolescents: a systematic literature review. Dermatol Ther. 2022;12(12):2653–2668. doi:10.1007/s13555-022-00819-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Management of Atopic Dermatitis: Clinical Utility of Ruxolitinib
Owji S, Caldas SA, Ungar B
Journal of Asthma and Allergy 2022, 15:1527-1537
Published Date: 25 October 2022
Atopic Dermatitis Treatments Before and After Initiation of Ruxolitinib Cream: 6-Month Follow-Up Analysis of a US Payer Claims Database
Liu J, Desai K, Teng CC, Sturm D, Stockbower G, Patadia H, Willey V
ClinicoEconomics and Outcomes Research 2025, 17:69-77
Published Date: 6 February 2025