Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Real-World Treatment of Patients Newly Diagnosed with Chronic Obstructive Pulmonary Disease: A Retrospective German Claims Data Analysis
Authors Buhl R, Wilke T ![]() , Picker N, Schmidt O, Hechtner M, Kondla A
, Picker N, Schmidt O, Hechtner M, Kondla A ![]() , Maywald U, Vogelmeier CF
, Maywald U, Vogelmeier CF
Received 18 May 2022
Accepted for publication 21 August 2022
Published 22 September 2022 Volume 2022:17 Pages 2355—2367
DOI https://doi.org/10.2147/COPD.S375190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Roland Buhl,1 Thomas Wilke,2 Nils Picker,3 Olaf Schmidt,4 Marlene Hechtner,5 Anke Kondla,5 Ulf Maywald,6 Claus F Vogelmeier7
1Pulmonary Department, Mainz University Hospital, Mainz, Germany; 2IPAM e.V, Wismar, Germany; 3Cytel Inc - Ingress-Health HWM GmbH, Wismar, Germany; 4Pulmonary Group Practice, Koblenz, Germany; 5Boehringer Ingelheim Pharma GmbH & Co. KG, Ingelheim, Germany; 6AOK PLUS, Dresden, Germany; 7Department of Medicine, Pulmonary and Critical Care Medicine, Philipps University of Marburg (UMR), Member of the German Center for Lung Research (DZL), Marburg, Germany
Correspondence: Roland Buhl, Medizinische Klinik und Poliklinik - Universitätsmedizin der Johannes Gutenberg-Universität Mainz, Langenbeckstraße 1, Mainz, 55131, Germany, Tel +49 6131 17 7271, Email [email protected]
Purpose: This study aimed to describe the real-world treatment of German incident COPD patients, compare that treatment with clinical guidelines, and provide insight into disease development after incident diagnosis. In addition, the economic burden of the disease by assessing COPD-related healthcare costs was described.
Patients and Methods: Based on a German claims dataset, continuously insured individuals (04/2014-03/2019) aged 40 years or older with at least two incident pulmonologist’s diagnoses or one inpatient diagnosis of COPD (ICD-10-GM code J44.-; no respective diagnosis in a 12-month baseline period) were selected. Treatment patterns after incident diagnosis considering inhaled maintenance therapies identified by ATC codes (outpatient prescriptions) were analyzed. Prescription patterns were compared with recommendations of German COPD treatment guidelines. Severe exacerbations were assessed as hospitalizations with main diagnosis ICD-10-GM code J44.1. COPD-associated costs from the perspective of the health insurance fund AOK PLUS were calculated per patient-year (PY).
Results: The sample comprised 17,464 incident COPD patients with a mean age of 71.5 years. 58.9% were male and the mean Charlson-Comorbidity-Index was 5.3. During follow-up (median: 2.0 years), 57.1% of the patients received at least one prescription of an inhaled maintenance therapy, whereas 42.9% did not. Among treated patients, 35.2% started their treatment with LABA/LAMA, 25.3% with LAMA monotherapy, 16.2% with LABA/ICS, and 7.8% with LABA/LAMA/ICS therapy. Within four weeks after initial diagnosis, ICS-containing therapies were prescribed in 14.1% of patients. Of all patients with a prescribed triple therapy, 68.9% had no corresponding exacerbation history documented. On average, 0.16 severe exacerbations and 0.19 COPD-related hospitalizations were observed per PY during available follow-up. Direct COPD-related costs were 3,693 €/PY, with COPD-related hospitalizations being responsible for about 79.2% of these costs.
Conclusion: Long-acting bronchodilators are the mainstay of pharmacological treatment of incident COPD patients in Germany, in line with guideline recommendations. Yet, a considerable proportion of incident COPD patients did not receive any inhaled maintenance therapy.
Keywords: COPD, real-world treatment, exacerbation frequency, healthcare costs
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality throughout the world.1,2 COPD is characterized by persistent airflow limitation and chronic respiratory symptoms and is often associated with high rates of hospital admission due to risk of exacerbation.3–5 Severe exacerbations are significantly associated with an overall deterioration in disease-specific health-related quality of life.6–9 Furthermore, severe COPD may lead to chronic respiratory failure requiring patients to receive supplemental oxygen therapy and/or ventilation support in addition to medical treatment.10,11
Pharmacological treatment of COPD aims to relieve respiratory symptoms and prevent future risk, in particular acute exacerbation.12 Guidelines recommend as maintenance treatment option for patients with moderate and stable COPD therapy with long-acting muscarinic antagonists (LAMAs), either as monotherapy or in combination with a long-acting beta-agonist (LABA).13 In moderate to severe disease, treatment with a combination of different classes of COPD medications is recommended over increasing the dosage of a single agent, avoiding side effects due to dose-related toxicity.13,14 For patients with severe COPD and a high risk of acute exacerbations, triple therapy including a LAMA, a LABA, and an inhaled corticosteroid (ICS) may be beneficial.13 However, there are concerns about the long-term side-effects of ICS use in COPD as it might be associated with, in particular, pneumonia but also osteoporosis, diabetes, tuberculosis, and non-tuberculous mycobacterial infection.15,16 Thus, the German COPD guidelines recommend combination treatments including ICS mainly as escalation therapy in well-defined subpopulations.17
Generally, a patient-specific approach that integrates all relevant clinical, genetic, and biological information for each individual aims at optimizing the pharmacological treatment to maximize the therapeutic benefit and reduce the risk of side effects.18 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) proposed an ABCD grouping approach in 2017, enabling a risk assessment based on symptoms and exacerbation risk.13,18,19 The ABCD grouping should be performed after the initial diagnosis of COPD to facilitate a more individualized approach to pharmacological management.
The knowledge on real-world treatment patterns in incident COPD patients as well as on the degree of guideline adherence is limited. Therefore, this study investigated the real-world treatment of a cohort of German incident COPD patients. Furthermore, the analysis compared initial maintenance therapies for COPD with clinical guideline recommendations to provide new insight into disease development after incident diagnosis, focusing on exacerbation and COPD-related hospitalization frequency. Finally, this study describes the economic disease burden by assessing the direct COPD-related healthcare costs.
Materials and Methods
Data Source
This study is based on a retrospective claims data analysis using an anonymized dataset covering the period 01/04/2014 to 31/03/2019 that was provided by the sixth largest German statutory health insurance fund (AOK PLUS). The claims database included about 3.1 million insured persons in Germany (Saxonia, Thuringia), which reflects 4.3% of the German population insured by statutory health insurance funds. German claims data provide information on patients’ demographics (age, gender, date of death) and detailed reimbursement claims on outpatient care, inpatient care, pharmaceuticals, therapeutic devices, rehabilitation, and sick leaves. For outpatient medication prescriptions, the following information is available: drug class (according to the Anatomical Therapeutic Chemical [ATC] classification system), date of prescription/filling in the pharmacy, prescribed package size, and related Defined Daily Dose (DDD) as published by the German Institute of Medical Documentation and Information (DIMDI).20
The study was coordinated and led by a Scientific Steering Committee consisting of the authors of this manuscript. As the study addressed a retrospective anonymized dataset, ethical approval and informed consent of patients were not required.
Sample Selection and Analysis Periods
The selection of the analysis sample was based on data of all individuals who were continuously insured by the AOK PLUS in the period from 01/04/2014 to 31/03/2019 or until the date of death, whatever came first.
An individual was considered to be an incident COPD case if at least two confirmed outpatient COPD diagnoses documented by a pulmonologist in two separate quarters or one inpatient COPD diagnosis (International statistical Classification of Diseases and related health problems, 10th revision, German Modification - ICD-10-GM code: J44.-) could be identified between 01/04/2015-31/03/2018, without observing any respective COPD diagnosis or COPD-related drug prescription (Table S1) in the baseline period of at least 12 months. The date of the first documented COPD diagnosis was defined as the index date. Patients aged below 40 years at index were excluded from the analysis sample. Furthermore, patients receiving any concomitant diagnosis of asthma (ICD-10-GM code: J45.-) after the index date were not considered in the final analysis sample to exclude subjects for whom an existing COPD could not be clearly confirmed.
A baseline period of 12 months prior to the index date was defined, enabling the description of patient characteristics, including comorbidity and treatment history, at the time of the incident COPD diagnosis. The observational period started at the index date and ended on 31/03/2019 or the date of death, whatever came first. The overall sample included all incident COPD patients with their respective patient-individual follow-up time. For a comparison of initiated maintenance therapies in real-world practice with clinical guideline recommendations, a subsample of patients who could be observed for a period of 12 months was considered (sufficient follow-up period in terms of data availability and no death within 12 months after incident COPD diagnosis). For a specific analysis on long-term treatment patterns and observable switches, a subsample of patients who could be observed for a period of 36 months was considered (sufficient follow-up period in terms of data availability and no death within 36 months after incident COPD diagnosis).
Study Endpoints and Statistical Analysis
Patient characteristics were descriptively analyzed for all patient samples (overall incident sample and subsamples observable for 12, and 36 months). In addition to age, gender, and comorbidities based on the Charlson Comorbidity Index21,22 (CCI without age factor; described in Table S2), the ten most frequently observed comorbidities and the top five prescribed agents at baseline (at least one prescription in the 12 months before the incident COPD diagnosis) were reported. Furthermore, the forced expiratory volume in one second (FEV1), available as ICD-10-GM subcodes (J44.-) of the incident diagnosis, was described. Frequency analysis was applied for all categorical variables, reporting the number and percentage of patients for each category (FEV1<35%, FEV1 35–50%, FEV1 50–70%, and FEV1 >70%). For continuous variables, summary statistics, including mean and standard deviation (SD), were reported.
Description of Treatment of Incident COPD Patients
Maintenance treatments for COPD, including long-acting bronchodilators and ICS, identified by ATC codes on outpatient prescriptions (see Table S1 for specific codes per medication class), were considered within the treatment pattern analysis. Patients were analyzed regarding observed prescriptions of the relevant agent (Table S1) longitudinally, starting the observation at the index date (incident diagnosis) until the end of follow-up. Combined usage of prescribed therapies was assumed if the respective agents were filled within a 21-day window and a similar prescription behavior was repeated at least once. In all other cases, a switch to a new treatment regimen was assumed. Treatment discontinuation was considered if a supply gap of at least 60 additional days after the end of the available medication stock for the respective agent (as approximated based on DDDs) was observed. Kaplan-Meier analysis was applied to evaluate the time to treatment initiations for any long-acting therapy and separately for dual-therapy (LABA/LAMA) and triple-therapy (LABA/LAMA/ICS). Main Kaplan-Meier statistics were reported, and respective Kaplan-Meier curves were depicted. Furthermore, the frequency of different agents/combinations per observable therapy line was described. Finally, based on a subsample of patients with a 36-month follow-up, treatment patterns by means of a Sankey diagram were reported.
Comparison with National Guideline Recommendations
Based on a subsample of patients with a 12-month follow-up, adherence with German treatment guidelines from 201223 and 201817 was determined by the percentage of patients with any ICS therapy within four weeks after initial diagnosis as well as the percentage of patients with LABA/LAMA/ICS prescription but ≤1 outpatient diagnosis and no inpatient diagnosis of an exacerbation (ICD-10 J44.1) at the first date of the LABA/LAMA/ICS prescription.
Exacerbation Frequency
Hospitalizations with a main diagnosis ICD-10-GM J44.- were considered as COPD-related exacerbations. Hospitalizations with the specific code ICD-10-GM J44.1 were counted as severe exacerbations.
COPD-related healthcare costs were reported per observed PY. COPD-related costs as a percentage of total all-cause costs were determined by considering outpatient care, inpatient care, pharmacy sales of COPD medications (any prescription of an agent listed in Table S1), therapeutic devices related to long-term oxygen therapy (ICD-10-GM codes J96.1, Z99.0, Z99.1, Z99.8, Z99.9, Z46.8, Z46.9; or OPS codes 8–712.1, 8–713.0, 8–716), and inpatient COPD-related rehabilitation.
All statistical analyses were performed using STATA (Version 14.1) and Microsoft Office Excel 16.
Results
Incident COPD Patients
Out of 2,327,309 patients with continuous insurance status in our AOK PLUS database, 100,055 prevalent COPD patients were identified. Among them, 17,464 were classified as incident COPD cases with a new diagnosis of COPD from 01/04/2014 to 31/03/2019 (Figure 1). These patients represented the main analysis sample (all incident COPD patients) and provided an observation of 34,648 patient-years, with a median patient-individual follow-up of 2.01 years (interquartile range: 1.18–2.89).
 |
Figure 1 Attrition chart of patient selection. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Sociodemographic characteristics, most common preexisting comorbidities, and frequently prescribed non-COPD medications at baseline are described in Table 1. The baseline characteristics of patients in the subsamples with a 12- and 36-month follow-up period were similar to the ones of the primary sample, with a tendency towards younger age and lower CCI. Within the observed study period, 5,238 patients died, corresponding to an overall mortality rate of 0.15 cases per patient-year.
 |
Table 1 Characteristics of the Identified Incident COPD Patients |
Treatment of Incident COPD Patients
The median time to initiation of any inhaled maintenance therapy after incident diagnosis of COPD was 4.4 months (95% CI: 3.9–4.9). The proportion of patients who did not receive any maintenance COPD treatment after 12, 24, and 36 months was 43.8% (95% CI: 43.0–44.6), 39.2% (95% CI: 38.4–40.0), and 36.0% (95% CI: 35.2–36.9), respectively (Figure 2). Among patients who started maintenance therapy in the first year, it took a median of 15 days to initiate that treatment. Patients first diagnosed in the hospital were found to have a lower rate of COPD treatment (45.3%) than patients initially diagnosed by outpatient pulmonologists (80.3%). Of the former, 82.3% of inpatient diagnosed cases had a hospital main diagnosis other than COPD. Considering the first twelve months of follow-up, patients who did not initiate any maintenance therapy were older than treated patients (mean 73.6 years versus 69.7 years), more female (58.3% versus 41.7%), and had less severe FEV1 restrictions (FEV1<50%, 10.7% versus 19.3%) with a higher percentage diagnosed with unspecified FEV1 (63.6% versus 52.0%). Furthermore, these patients were more comorbid as measured by the CCI (mean of 5.90 versus 4.73), and their mortality in the first twelve months was higher than in the treated sample (27.3% versus 10.8%). However, even among patients with severe airflow limitation (FEV1<50%), about one-third did not receive at least one prescription for inhaled maintenance therapies (Figure S1). Of the 8,225 patients without any maintenance treatment for COPD in the first twelve months after initial diagnosis, 81.5% also received no prescription of any short-acting bronchodilator (SABA/SAMA).
 |
Figure 2 Kaplan-Meier curves depicting the time to treatment initiation after incident COPD diagnosis. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; ICS, Inhaled glucocorticosteroids; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist. Note: Censoring events: death or end of follow-up (31/03/2019). |
The median time to initiation of dual-therapy with LABA/LAMA and initiation of triple-therapy with LABA/LAMA/ICS was not reached (Figure 2). The estimated mean time to treatment initiation restricted to the observational period was 35.8 months (95% CI: 35.5–36.1) for dual-therapy and 43.7 months for triple-therapy (95% CI: 43.5–43.9).
During the available observation period, the combined usage of LABA/LAMA was the most frequent initial regimen among the treated patients (35.2% in 1st line treatment group), followed by a LAMA monotherapy (25.3% in 1st line treatment group) and use of LABA combined with ICS (16.2% in 1st line treatment group; Figure 3). Almost 8.1% of the treated patients initiated their COPD treatment with a triple therapy consisting of LABA/LAMA/ICS.
 |
Figure 3 Frequency of inhaled maintenance therapies per line of treatment. Abbreviations: ICS, inhaled glucocorticosteroids; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist. Notes: Only based on patients receiving either long-acting bronchodilators or ICS; a combination treatment was assumed if the respective agents were prescribed within a 60-days window and a similar prescription behavior was repeated at least once. |
A subsample of 3,804 patients with a follow-up of 36 months was analyzed to observe not only the frequency of different agents in the initial treatment but the treatment cascade over time (Figure 4). About 10.9% of observed patients received respective maintenance treatment with a prescription exactly on the day of the incident diagnosis. After 12 months, the most frequently prescribed treatment regimens were LABA/LAMA (19.4% of all patients), LAMA mono (12.9%), LABA/ICS (9.4%), and triple therapy LABA/LAMA/ICS (5.7%). Treatment patterns remained relatively stable after 24 and 36 months, with a slight increase of LABA/LAMA to 22.5% after 36 months, LABA/ICS to 11.6%, and triple therapy to 7.3%. The most frequent treatment changes were observed in the 10.8% of patients treated with LAMA at 12 months after the initial diagnosis switching to LABA/LAMA after 24 months, and in the 4.6% of patients on LABA/LAMA after 12 months switching to LABA/LAMA/ICS after 24 months (Figure 4).
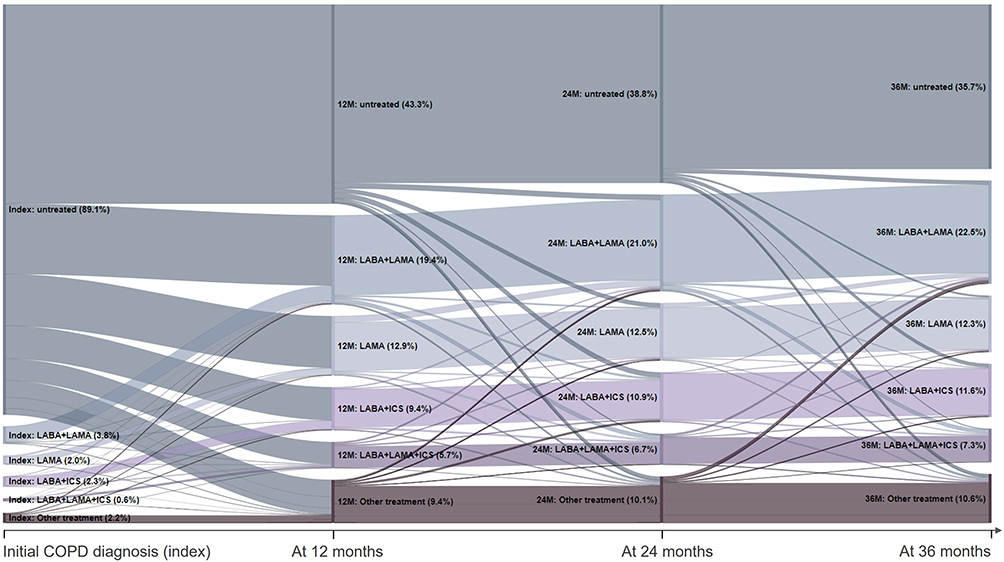 |
Figure 4 Treatment cascades observed after incident COPD diagnosis in a sample of patients with a follow-up of 36 months (n=3,804). Abbreviations: ICS, inhaled glucocorticosteroids; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist. Notes: Other treatments include use of LABA alone, ICS alone, roflumilast and methylxanthines (alone or in combination with other therapies). |
Comparison with Treatment Guideline Recommendations
Of the patients with a 12-months follow-up, 2008 (14.1%) received an ICS-containing therapy within four weeks after the initial diagnosis, which was not in line with 2012 and 2018 guideline recommendations. The same is true for 1019 incident patients who have been prescribed a LABA/LAMA/ICS therapy within 12 months after diagnosis. Of these, 702 patients (68.9%) had fewer than two outpatient diagnoses and no inpatient diagnosis of a prior exacerbation.
Exacerbations and COPD-Related Hospitalizations
Of all incident COPD patients, 2,619 (15.0%) were initially diagnosed with an acute exacerbation (incident diagnosis was ICD-10-GM code J44.1). Figure 5 shows the Kaplan-Meier curve evaluating the time to the first acute exacerbation (hospitalization with the main diagnosis of ICD-10-GM code J44.1) after the index date (incident diagnosis). During the available follow-up (median: 24.1 months), hospitalizations due to exacerbations were seen in less than half of the sample. After 12.2 months (95% CI: 10.0–14.4), a severe exacerbation requiring hospitalization occurred in one-tenth of patients, and the mean event-free time restricted to the available follow-up period was 42.2 months (95% CI: 42.0–42.5).
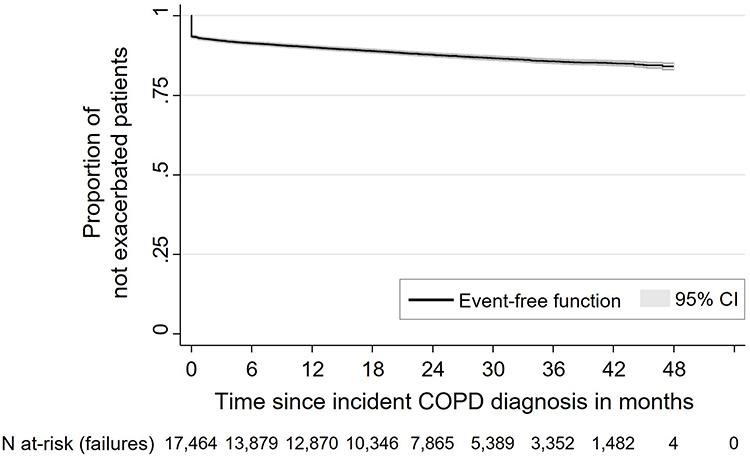 |
Figure 5 Kaplan-Meier curve depicting the time to first severe exacerbation (hospitalization with main diagnosis ICD-10GM code J44.1) after incident COPD diagnosis. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease. Note: Censoring events: death or end of follow-up (31/03/2019). |
The overall number of observed severe exacerbations requiring a hospitalization per patient-year was 0.16. This number decreased to 0.08 when exacerbations observed as index events (incident diagnosis) were not taken into account.
Considering any COPD diagnosis (ICD-10-GM code J44.-), the COPD-related hospitalization rate was 0.19 per patient-year, with 2,513 patients (14.4%) having at least one COPD-related hospitalization during the first 12 months after the incident COPD diagnosis.
COPD-Related Direct Healthcare Costs
Based on the overall sample of incident patients and addressing the whole available patient-individual follow-up time, Figure 6 outlines the identified direct COPD-related healthcare cost. The total of COPD-related direct costs per observed patient-year was 3,693 €. The inpatient costs were the main driver, with 2,922 € per patient-year (79.1% of total costs). The observed COPD-related medication costs accounted for 7.7% of the total costs (285 € per patient-year), the outpatient cost for 6.7% (246 € per patient-year), and the costs of long-term oxygen therapy for 6.5% (240 € per patient-year). The costs incurred by COPD-related rehabilitation were negligible, with 0.37€ per patient-year. Moreover, COPD-related costs as a whole accounted for one-tenth of total health care costs from the statutory health insurance (SHI) perspective (Figure S2). Other common diagnoses included heart failure, pneumonia, and lung cancer.
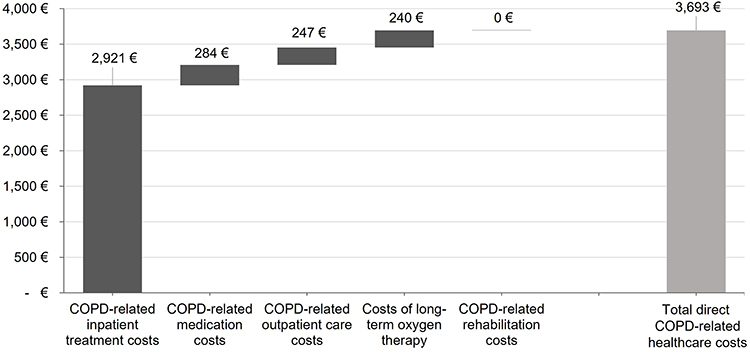 |
Figure 6 COPD-related direct healthcare cost per patient-year. Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease. |
Discussion
Our analyses show that German real-world COPD patients are rather old (mean age of 71.5 years) and suffer from a high number of comorbidities (mean CCI [without age factor] of 5.3). This is in marked contrast to the typical COPD patient included in clinical trials and raises the question of whether clinical trial results in highly selected and much younger patients can simply be extrapolated to this population. This question is even more relevant as the proportion of patients receiving oxygen therapy is quite high (>20%), and almost 20% of German COPD patients died within the first year after their initial COPD diagnosis. This fact may in part explain why a significant proportion of these patients, almost 40%, did not receive COPD medication. However, as the cause of death is not recorded in claims data, we could not assess the influence of COPD in this dataset. However, because the overall annual mortality of persons in the age cohort ≥65 years in Germany was 5.3% in 2019, the mortality observed in this study indicates a considerable COPD-associated excess mortality.
In the analyzed sample, the median time to the initiation of any inhaled maintenance therapy after incident diagnosis of COPD was estimated to be 4.4 months, with a proportion of patients who did not receive any maintenance regimen, including ICS, after 12, 24, and 36 months of 43.8%, 39.2%, and 36.0%. Most of these patients were initially diagnosed during hospitalization. However, in the vast majority of them, COPD was not the main diagnosis, so many patients did not subsequently receive outpatient pharmacological treatment. Therefore, we recommend further investigation of the interface between inpatient and outpatient sectors to improve intersectoral care of patients with newly diagnosed COPD, for example, by implementing more proactive therapeutic approaches to prevent COPD progression to exacerbation as previously described.24,25
Some of the untreated patients suffered from a very low FEV1, indicating a high probability that immediate treatment with maintenance therapies might have been needed and helpful. However, the majority of these patients already needed regular care, demonstrated by a documented level of need for care according to statutory long-term care insurance, and it is probable that a substantial percentage of these patients live in a nursing home or receive regular domestic care. Whether this explains the presumed undertreatment with inhaled maintenance therapies is unknown, but we recommend that the quality of care of these patients should be investigated more in detail. Since previous studies have shown that early use of long-acting bronchodilators as maintenance therapy is beneficial, more emphasis should be placed on early treatment in patients with suspected COPD diagnosis to slow disease progression.26
Among treated patients, about one-third of the patients started their treatment with a LABA/LAMA combination, one-fourth received a LAMA monotherapy, whereas around one-sixth received LABA/ICS, and only eight percent started a triple-therapy (LABA/LAMA/ICS). So, the majority of initial prescriptions for newly diagnosed COPD patients was in line with current COPD guideline recommendations. However, treatment of triple-therapy patients is not in line with current treatment guidelines as these do not recommend the initial use of triple-therapy.17 In addition, the use of triple therapy was not consistent with previously documented exacerbations, which were missing in almost 70% of all triple therapy prescriptions within the first year after diagnosis. One factor that may have contributed to the prescription of triple therapy in patients without exacerbation in clinical practice is that some physicians perceive LABA/LAMA/ICS to be more effective than LABA/LAMA in relieving symptoms and improving lung function (“3 must be better than 2”) which has been observed in the UK,27 Japan,28 and elsewhere.29–31 Recent randomized trials have demonstrated a reduction in mortality and exacerbations among patients with symptomatic COPD treated with inhaled triple therapy (LABA/LAMA/ICS) compared with patients treated with dual therapy32,33 (LABA/LAMA). However, real-world data from the UK showed that in patients with COPD who were newly prescribed LABA/LAMA/ICS, all-cause mortality and the number of severe exacerbations increased slightly in the first year of use, as compared with those initiating treatment with LAMA and LABA.34 In addition, a recent pooled analysis of patients with mild-to-very-severe COPD and predominantly low exacerbation risk showed no differences in mortality with LAMA/LABA vs LAMA/LABA/ICS.35 As there has been no increase in mortality in patients with a history of exacerbations or asthma, escalation of treatment to triple therapy should occur only when recommended.
While our study demonstrated that the proportion of COPD patients receiving LABA/LAMA/ICS is currently rather low, previous data from a German registry (DACCORD) in 2016 indicated that 36.4% of the patients are on LAMA monotherapy, 16.1% on LABA/LAMA, and 29% on triple-therapy.36 The same study also showed that treatment with LABA/LAMA/ICS did not improve outcomes compared with dual bronchodilation in terms of either exacerbations or health status based on a matched-pairs analysis.37 So, the percentage of treated patients and the percentage of patients on triple-therapy were higher in DACCORD, which might be explained by the fact that all these patients were included in a registry and, in that sense, were pre-selected, whereas in our study, only newly diagnosed COPD cases were observed. In another recent study based on electronic medical records, Quint et al reported that the most common pathway to triple COPD therapy is LABA/ICS therapy or no previous therapy.38 We can confirm that most of our observed triple-therapy patients did not receive any previous maintenance treatment, but the percentage of patients who received a previous mono- or dual-therapy and then switched to triple-therapy was very low. A few years ago, the COSYCONET study showed a very different picture with respect to the use of ICS in COPD patients with low exacerbation rates. Accordingly, two-thirds of these patients had received ICS despite opposite recommendations in clinical guidelines.39 The present study, therefore, clearly shows that a rebalancing of the early use of ICS in clinical practice has taken place. Based on our longitudinal analysis of treatment patterns in the first three years after the incident COPD diagnosis in those patients who could be observed for these three years, 22.5% of the patients were treated with LABA/LAMA within 36 months (compared to 19.4% within the first 12 months), 12.3% of the patients were treated with LAMA only (with a similar proportion observed after 12 months), 11.6% were treated with LABA/ICS (compared to 9.4% after 12 months), and only 7.3% of patients progressed to triple-therapy (compared to 5.7% after 12 months).
In the overall follow-up period, a rate of exacerbation-/COPD-related hospitalizations of 0.16/0.19 per patient-year was observed. In addition, more than one in five patients received oxygen therapy during the observable follow-up period. Our cost analysis demonstrated the respective associated high economic burden of COPD, which is consistent with previous findings from the literature.40,41 The overall direct COPD-related costs were 3,693 € per patient-year, with COPD-related hospitalizations being responsible for about 79.2% of these costs. These numbers are slightly lower with regard to outpatient and medication costs in comparison to an earlier analysis published by Wacker et al.39 This might be related to our large percentage of untreated patients and our observation of incident COPD patients only. In addition, the above previous analysis considered all-cause medication costs, whereas we only considered costs directly related to COPD medications. In our study, however, only about 10% of all-cause costs were directly related to COPD. Because respiratory complications (pneumonia, lung cancer, etc.) or cardiovascular comorbidities (eg, heart failure) may be fundamentally related to COPD, the total COPD-related costs are likely higher than reported here.
There are some limitations of this retrospective claims data analysis that need to be acknowledged. Firstly, we were only able to assess the comorbidity history as well as the treatment history of our patients for a baseline period of 12 months. Secondly, we did not include patients if they had been diagnosed by GPs only, so there is a risk of underestimating the incidence of COPD. However, as there exists a trade-off between the accuracy of COPD diagnoses and the higher generalizability of data, we decided to focus on reliably diagnosed COPD patients. For this reason, we also excluded all patients aged below 40 years and/or who had received a diagnosis of asthma after the incident COPD diagnosis. Treatment patterns and cost of these patients might differ from the included patients, but uncertainty around diagnosis reliability of these patients led us to exclude them. Thirdly, an exact assessment of the severity of disease was not feasible in our study, given the nature of the data. So, even if it is unlikely that all untreated patients did not require any inhaled maintenance therapy, our conclusions are limited in this way. Fourthly, our longitudinal analysis of treatment patterns in the three years after the incident diagnosis addressed patients who survived the first 36 months only. Thus, the respective results can be influenced by an immortal time bias. The same bias applies to the 12-month study cohort, which was analyzed to assess adherence to guideline recommendations. We accepted these limitations as the objective of the respective analyses was to observe long-term treatment patterns in patients who were treated for 12 and 36 months, respectively. Finally, any treatment rationale around the initiation of escalation therapies was not documented in the dataset. So, a final assessment of the level of guideline adherence of the treatment of patients is limited by this lack of data.
However, the main strength of this study is the analysis of a large, unbiased incident COPD patient sample with coverage of all relevant outpatient and inpatient prescriptions (no missing prescriptions due to treatment by more than one physician and/or treatment by both outpatient and inpatient physicians).
Conclusion
Although COPD in Germany is associated with a substantial patient and economic burden, a high proportion of newly diagnosed patients remains untreated after the incident diagnosis. It was found that these patients were often initially diagnosed in the inpatient setting while suffering from other serious comorbidities such as heart failure. Therefore, early prescription of long-acting bronchodilators for these patients according to current COPD guidelines could reduce the likelihood of exacerbations and disease progression, thereby significantly improving survival prognosis while avoiding treatment with ICS whenever possible to keep the medication-related burden low. In addition, interdisciplinary and cross-sectoral care of COPD patients should be improved in order to ensure early treatment initiation.
Acknowledgments
This manuscript was developed in memoriam of Silke Geier, who developed the idea for this study but passed away during the study. The work of IPAM and Ingress-health in this study was sponsored by Boehringer-Ingelheim. The data for this study was provided by AOK PLUS. A summary of the results of this study was presented at the 13th Congress of the German Society for Health Economics (dggö) and the 20th Congress of the German Network on Health Services Research (DKVF) during conference talks, as well as at the 127th and the 128th Congress of the German Society of Internal Medicine (DGIM), and the 31st International Congress of the European Respiratory Society (ERS) as poster presentations.
The abstracts on the conference talks were published online (https://dggoe.de/konferenzen/2021/programm/9/sitzung/33; DOI:10.3205/21dkvf206). The posters’ abstracts were published in INTERNIST, Vol. 62, No. SUPPL 2, INTERNIST, vol. 63, no. SUPPL 3, pp. 352-353, and the European Respiratory Journal 2021; 58: Suppl. 65, (DOI:10.1183/13993003.congress-2021.PA2409; DOI:10.1183/13993003.congress-2021.PA2406).
Disclosure
Professor Roland Buhl reports personal fees from AstraZeneca, Berlin-Chemie, Chiesi, Cipla, Sanofi, teva, and grants from Boehringer Ingelheim, GSK, Novartis, and Roche outside the submitted work. Professor Thomas Wilke reports grants from GSK and Cytel during the conduct of the study and grants from Pfizer, Janssen, and Apontis outside the submitted work. Nils Picker and Dr Olaf Schmidt have no conflicts of interest to disclose. Dr Marlene Hechtner and Dr Anke Kondla are employees of Boehringer Ingelheim Pharma GmbH & Co. KG. Professor Claus F Vogelmeier reports personal fees from Aerogen, Insmed, Menarini, and Nuvaira; and grants from AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, GlaxoSmithKline, Grifols, and Novartis outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. França EB, Passos VMDA, Malta DC, et al. Cause-specific mortality for 249 causes in Brazil and states during 1990–2015: a systematic analysis for the global burden of disease study 2015. Popul Health Metr. 2017;15(1):39. doi:10.1186/s12963-017-0156-y
2. Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
3. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi:10.1164/rccm.200703-456SO
4. Søgaard M, Madsen M, Løkke A, Hilberg O, Sørensen HT, Thomsen RW. Incidence and outcomes of patients hospitalized with COPD exacerbation with and without pneumonia. Int J COPD. 2016;11(1):455–465. doi:10.2147/COPD.S96179
5. Lindenauer PK, Dharmarajan K, Qin L, Lin Z, Gershon AS, Krumholz HM. Risk trajectories of readmission and death in the first year after hospitalization for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(8):1009–1017. doi:10.1164/RCCM.201709-1852OC
6. Stöber A, Lutter JI, Schwarzkopf L, et al. Impact of lung function and exacerbations on health-related quality of life in COPD patients within one year: real-world analysis based on claims data. Int J Chron Obstruct Pulmon Dis. 2021;16:2637–2651. doi:10.2147/COPD.S313711
7. Menn P, Weber N, Holle R. Health-related quality of life in patients with severe COPD hospitalized for exacerbations - comparing EQ-5D, SF-12 and SGRQ. Health Qual Life Outcomes. 2010;8(1):39. doi:10.1186/1477-7525-8-39
8. Guo J, Chen Y, Zhang W, Tong S, Dong J. Moderate and severe exacerbations have a significant impact on health-related quality of life, utility, and lung function in patients with chronic obstructive pulmonary disease: a meta-analysis. Int J Surg. 2020;78:28–35. doi:10.1016/J.IJSU.2020.04.010
9. Esteban C, Quintana JM, Moraza J, et al. Impact of hospitalisations for exacerbations of COPD on health-related quality of life. Respir Med. 2009;103(8):1201–1208. doi:10.1016/J.RMED.2009.02.002
10. Lindenauer PK, Stefan MS, Shieh MS, Pekow PS, Rothberg MB, Hill NS. Hospital patterns of mechanical ventilation for patients with exacerbations of COPD. Ann Am Thorac Soc. 2015;12(3):402–409. doi:10.1513/ANNALSATS.201407-293OC
11. Lindenauer PK, Stefan MS, Shieh MS, Pekow PS, Rothberg MB, Hill NS. Outcomes associated with invasive and noninvasive ventilation among patients hospitalized with exacerbations of chronic obstructive pulmonary disease. JAMA Intern Med. 2014;174(12):1982–1993. doi:10.1001/JAMAINTERNMED.2014.5430
12. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
13. Global initiative for chronic obstructive lung disease (GOLD) guidelines; 2017. Available from: https://www.ajmc.com/view/global-initiative-for-chronic-obstructive-lung-disease-gold-guidelines-2017-update.
14. Singh D. New combination bronchodilators for chronic obstructive pulmonary disease: current evidence and future perspectives. Br J Clin Pharmacol. 2015;79(5):695–708. doi:10.1111/bcp.12545
15. Lee CH, Kim K, Hyun MK, Jang EJ, Lee NR, Yim JJ. Use of inhaled corticosteroids and the risk of tuberculosis. Thorax. 2013;68(12):1105–1113. doi:10.1136/thoraxjnl-2012-203175
16. Ernst P, Saad N, Suissa S. Inhaled corticosteroids in COPD: the clinical evidence. Eur Respir J. 2015;45:525–537. doi:10.1183/09031936.00128914
17. Vogelmeier C, Buhl R, Burghuber O, et al. Guideline for the diagnosis and treatment of COPD patients: issued by the German respiratory society and the German atemwegsliga in cooperation with the Austrian society of pneumology. Pneumologie. 2018;72(4):253–308. doi:10.1055/s-0043-125031
18. Leung JM, Obeidat M, Sadatsafavi M, Sin DD. Introduction to precision medicine in COPD. Eur Respir J. 2019;53(4):1802460. doi:10.1183/13993003.02460-2018
19. GOLD 2017. Global initiative for chronic obstructive lung disease: pocket guide to COPD diagnosis, management, and prevention, A guide for health care professionals. Gold. 2017;1–33. doi:10.1097/00008483-200207000-00004
20. Fricke U, Günther J, Nieprasch-von Dollen K, Zawinell A. Anatomisch-Therapeutisch-Chemische-Klassifikation Mit Tagesdosen Amtliche Fassung Des ATC-Index Mit DDD-Angaben Für Deutschland Im Jahre 2019. BMC Ecol. 2019. doi:10.1186/s12898-019-0245-9
21. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
22. Sundararajan V, Henderson T, Perry C, Muggivan A, Quan H, Ghali WA. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004;57(12):1288–1294. doi:10.1016/j.jclinepi.2004.03.012
23. Abholz HH, Gillissen A, Magnussen H, Schultz K, Ukena DWH. Nationale Versorgungsleitlinie COPD; 2012. Available from: http://www.copd.versorgungsleitlinien.de.
24. Cardoso J, Ferreira AJ, Guimarães M, Oliveira AS, Simão P, Sucena M. Treatable traits in COPD – a proposed approach. Int J Chron Obstruct Pulmon Dis. 2021;16:3167–3182. doi:10.2147/COPD.S330817
25. Zatloukal J, Brat K, Neumannova K, et al. Chronic obstructive pulmonary disease – diagnosis and management of stable disease; a personalized approach to care, using the treatable traits concept based on clinical phenotypes. Position paper of the Czech pneumological and phthisiological society. Biomed Pap. 2020;164(4):325–356. doi:10.5507/BP.2020.056
26. Welte T, Vogelmeier C, Papi A. COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract. 2015;69(3):336–349. doi:10.1111/IJCP.12522
27. Brusselle G, Price D, Gruffydd-Jones K, et al. The inevitable drift to triple therapy in COPD: an analysis of prescribing pathways in the UK. Int J Chron Obstruct Pulmon Dis. 2015;10(1):2207. doi:10.2147/COPD.S91694
28. Miyazaki M, Nakamura H, Takahashi S, et al. The reasons for triple therapy in stable COPD patients in Japanese clinical practice. Int J Chron Obstruct Pulmon Dis. 2015;10:1053. doi:10.2147/COPD.S79864
29. Papala M, Kerenidi N, Gourgoulianis KI. Everyday clinical practice and its relationship to 2010 and 2011 GOLD guideline recommendations for the management of COPD. Prim Care Respir J J Gen Pract Airways Gr. 2013;22(3):362. doi:10.4104/PCRJ.2013.00073
30. Corrado A, Rossi A. How far is real life from COPD therapy guidelines? An Italian observational study. Respir Med. 2012;106(7):989–997. doi:10.1016/J.RMED.2012.03.008
31. Burgel PR, Deslée G, Jebrak G, et al. Real-life use of inhaled corticosteroids in COPD patients versus the GOLD proposals: a paradigm shift in GOLD 2011? Eur Respir J. 2014;43(4):1201–1203. doi:10.1183/09031936.00162313
32. Lipson DA, Crim C, Criner GJ, et al. Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;201(12):1508–1516. doi:10.1164/RCCM.201911-2207OC/SUPPL_FILE/DISCLOSURES.PDF
33. Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced all-cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease a randomized, double-blind, multicenter, parallel-group study. Am J Respir Crit Care Med. 2021;203(5):553–564. doi:10.1164/RCCM.202006-2618OC/SUPPL_FILE/DISCLOSURES.PDF
34. Suissa S, Dell’aniello S, Ernst P. Triple inhaler versus dual bronchodilator therapy in COPD: real-world effectiveness on mortality. COPD. 2022;19(1):1–9. doi:10.1080/15412555.2021.1977789
35. Miravitlles M, Verhamme K, Calverley PMA, et al. A pooled analysis of mortality in patients with COPD receiving dual bronchodilation with and without additional inhaled corticosteroid. Int J Chron Obstruct Pulmon Dis. 2022;17:545–558. doi:10.2147/COPD.S350167
36. Young D, Buhl R, Criée P, et al. A year in the life of German patients with COPD: the DACCORD observational study. Int J COPD. 2016;11(1):1639–1646. doi:10.2147/COPD.S112110
37. Buhl R, Criée CP, Kardos P, et al. Dual bronchodilation vs triple therapy in the “real-life” COPD DACCORD study. Int J Chron Obstruct Pulmon Dis. 2018;13:2557. doi:10.2147/COPD.S169958
38. Quint JK, O’Leary C, Venerus A, et al. Prescribing pathways to triple therapy: a multi-country, retrospective observational study of adult patients with chronic obstructive pulmonary disease. Pulm Ther. 2020;6(2):333–350. doi:10.1007/s41030-020-00132-7
39. Wacker ME, Jörres RA, Schulz H, et al. Direct and indirect costs of COPD and its comorbidities: results from the German COSYCONET study. Respir Med. 2016;111:39–46. doi:10.1016/j.rmed.2015.12.001
40. Darnell K, Dwivedi AK, Weng Z, Panos RJ. Disproportionate utilization of healthcare resources among veterans with COPD: a retrospective analysis of factors associated with COPD healthcare cost. Cost Eff Resour Alloc. 2013;11(1). doi:10.1186/1478-7547-11-13
41. Wang Y, Stavem K, Dahl FA, Humerfelt S, Haugen T. Factors associated with a prolonged length of stay after acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Int J COPD. 2014;9:99–105. doi:10.2147/COPD.S51467
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characteristics of Users and New Initiators of Single- and Multiple-Inhaler Triple Therapy for Chronic Obstructive Pulmonary Disease in Germany
Beeh KM, Rothnie KJ, Claussen J, Hardtstock F, Knapp RK, Wilke T, Czira A, Compton C, Ismaila AS
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:945-956
Published Date: 17 April 2024