")
Back to Journals » Clinical Ophthalmology » Volume 18
Real-World Study of the Effectiveness and Safety of Intracameral Bimatoprost Implant in a Clinical Setting in the United States
Authors Teymoorian S, Craven ER , Nguyen L, Werts E
Received 16 October 2023
Accepted for publication 3 January 2024
Published 19 January 2024 Volume 2024:18 Pages 187—199
DOI https://doi.org/10.2147/OPTH.S445005
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Savak Teymoorian,1 E Randy Craven,2 Lannhi Nguyen,1 Erica Werts2
1Harvard Eye Associates, Laguna Hills, CA, USA; 2Allergan, an AbbVie company, Irvine, CA, USA
Correspondence: Savak Teymoorian, Harvard Eye Associates, 23961 Calle de la Magdalena, Suite 300, Laguna Hills, CA, 92653, USA, Tel +1 (949) 951-2020, Email [email protected]
Purpose: A sustained-release, biodegradable, intracameral 10-μg bimatoprost implant (Durysta) is approved for single administration per eye to lower intraocular pressure (IOP) in open-angle glaucoma (OAG) and ocular hypertension (OHT). The purpose of this study was to evaluate the IOP-lowering effectiveness and safety of a single implant administration per eye in patients with OAG or OHT in a real-world clinical setting.
Methods: This was a retrospective, single-site study involving 105 consecutive adult patients with OAG or OHT treated with the bimatoprost implant in 1 or both eyes in routine clinical practice. Available medical records of the patients for 12 months or longer after the initial implant administration were reviewed, and data including IOP, IOP-lowering medication and procedure use, and safety outcomes were collected and analyzed. The analysis used ranges of follow-up because of the real-world setting.
Results: The study included 197 eyes (85.3% diagnosed with OAG, 94.9% pseudophakic, and 83.8% with angle grade 4). IOP reduction was observed through 1 year after the bimatoprost implant administration. Mean IOP was 16.6 mmHg at baseline and 13.3 mmHg at 11– 13 months, with the mean number of topical IOP-lowering medications used reduced from 1.4 at baseline to 0.2 at 11– 13 months. IOP and IOP-lowering medication use were similarly reduced in eyes treated with both selective laser trabeculoplasty (SLT) and bimatoprost implant (including 66 eyes with their last SLT before implant administration and 28 eyes with their last SLT after implant administration). There were no cases of treatment-emergent corneal edema after bimatoprost implant administration, and no eye required implant removal.
Conclusion: A single bimatoprost implant administration safely and effectively reduced IOP for up to 1 year and decreased the need for topical IOP-lowering medications in eyes with OAG or OHT with or without previous or subsequent SLT.
Keywords: biodegradable implant, drug delivery system, intraocular injection, prostaglandin analog
Introduction
Bimatoprost implant (Durysta; Allergan, an AbbVie company, North Chicago, IL, USA) is a biodegradable intracameral implant used to lower intraocular pressure (IOP) in patients with open-angle glaucoma (OAG) or ocular hypertension (OHT).1 The small, cylindrical implant is composed of a polymer matrix containing 10 µg of bimatoprost, an IOP-lowering medication of the prostaglandin analog/prostamide (PGA) class.2 A prefilled applicator is used to administer the implant via the corneal limbus into the anterior chamber, where it provides continuous, sustained release of bimatoprost as the polymers are hydrolyzed and metabolized to carbon dioxide and water.3,4 The bimatoprost implant was designed to release bimatoprost for approximately 3–4 months,5 but longer-lasting effects of the implant on IOP have been reported.3,5,6 It has been proposed that with bimatoprost implant administration, patients can achieve IOP lowering that persists beyond the duration of intraocular drug bioavailability, because high bimatoprost concentrations achieved in target tissues by the implant produce enhanced matrix metalloproteinase activation that leads to durable remodeling of aqueous outflow pathways and sustained IOP lowering.3,6–9
The efficacy and safety of intracameral bimatoprost implant treatment were evaluated in the phase 3 ARTEMIS studies.3,5 In these identically designed, 20-month, randomized, clinical trials, the study eye of patients with OAG or OHT received either three administrations of a 10- or 15-µg dose strength of the bimatoprost implant at fixed 16-week dosing intervals or twice-daily topical timolol maleate 0.5%. In each trial, both dose strengths of the bimatoprost implant met the primary endpoint and demonstrated noninferiority to topical timolol in lowering IOP through week 12.3,5 Furthermore, most of the bimatoprost implant–treated eyes required no additional (rescue) IOP-lowering medication for up to 1 year after the third implant administration.3,5 Long-term IOP data (beyond 15 weeks) after single administration were not available from the phase 3 trials, and the present study addresses this information gap.
Corneal endothelial cell loss and corneal edema were reported in some bimatoprost implant–treated eyes in the ARTEMIS studies.3,5 However, these adverse effects generally occurred after repeated administrations and were less frequent with the smaller, 10-µg dose strength of implant.3,5 On the basis of these findings, bimatoprost implant 10 µg (measures 1.1 mm long by 0.2 mm diameter) was approved by the US Food and Drug Administration for single administration per eye to lower IOP in patients with OAG or OHT.
Only limited data are available on the long-term effectiveness and safety of a single administration of the bimatoprost implant.1,6,10,11 Thus, the objective of this study was to evaluate the long-term effectiveness and safety of a single bimatoprost implant administration in patients with OAG or OHT in a real-world clinical setting.
Methods
This retrospective cohort study included patients treated with the bimatoprost intracameral implant by one author (ST) at Harvard Eye Associates offices and Alicia Surgical Center, an ambulatory surgery center. The decision to treat was made by the physician and patient and reflected standard medical care. The study used de-identified patient data from an electronic database and was conducted in accordance with the principles of the Declaration of Helsinki and the Health Information Portability and Accountability Act. The study protocol was approved by the Alpha IRB institutional review board. Informed consent was waived because of the use of retrospective, anonymized data.
Patients at least 18 years of age, diagnosed with OAG or OHT, who received an initial bimatoprost implant treatment between July 23, 2020, and March 18, 2021, were potentially eligible for the study. Patients could be treated with the bimatoprost implant in one or both eyes. Patients with a contraindication to bimatoprost implant treatment (active or chronic ocular or periocular infection, corneal endothelial cell dystrophy, prior corneal transplantation, absent or ruptured posterior lens capsule, or hypersensitivity) were excluded. Patients who participated in a clinical trial involving an investigational medicinal product or medical device during the study period were also excluded.
Consecutive patients who met the eligibility criteria were included in the study. The bimatoprost implant was administered intracamerally using a prefilled, single-use, 28-gauge sterile applicator and aseptic technique.3 The patients were followed and managed clinically per standard clinical practice. Slit-lamp biomicroscopy was used routinely to examine the health of the corneal endothelium, and endothelial cell counts were performed if there was a suspected effect on corneal endothelial health.
Electronic health records of the patients’ office and surgical center visits through January 28, 2022, were reviewed. The data collection included all available data regarding baseline patient characteristics, details of the implant administration, the presence or absence of visible implant, IOP, concomitant medications and procedures for IOP control, biomicroscopy and ophthalmoscopy findings, any glaucoma-related test results (eg, visual fields, retinal nerve fiber layer thickness, optic disc cupping), visual acuity, and adverse events. Optical coherence tomography (OCT) evaluations were performed in eyes with vision problems potentially associated with the retina.
Outcomes and Analysis
The primary outcome evaluated in the total study population was the change in IOP from baseline up to 12 months after the bimatoprost implant administration. Use of topical IOP-lowering medications after the bimatoprost implant administration was also evaluated. Preplanned subgroup analysis evaluated these outcomes in eyes treated with both bimatoprost implant and selective laser trabeculoplasty (SLT), as well as eyes previously treated with microincisional glaucoma surgery (MIGS). Safety was evaluated by the occurrence of ocular adverse events (including corneal and ocular inflammatory adverse events and any other clinically relevant adverse events) and the need for implant removals.
The planned analyses used observed data and summarized the results using descriptive statistics. Data from the visit on the day of the implant administration or the most recent previous visit were used as baseline data. Because of the variability of timing of follow-up that occurs in the real-world setting, IOP and IOP-lowering medication usage were analyzed using nominal follow-up visit windows defined by the number of days post bimatoprost implant administration, as follows: 1–7 days, 8–60 days, 61–120 days (“3 months”), 121–150 days (“4.5 months”), 151–210 days (“6 months”), 211–319 days (“7–10 months”), and 320–409 days (“11–13 months”). If an eye had IOP measurements available from multiple visits within a visit window, the average of the measurements was used for analysis. All eyes with available IOP data within these visit windows were included in the main analysis, regardless of whether SLT or a MIGS procedure was used in the follow-up period after the bimatoprost implant administration. Post hoc analyses evaluated IOP and use of IOP-lowering medications in the subgroup of eyes that had not undergone SLT within the 6 months prior to baseline, as well as in the subgroup of eyes that had neither a history of SLT at baseline nor received SLT after the bimatoprost implant administration. Safety analyses used all available data.
Results
The study included a total of 197 eyes in 105 patients that received a 10-µg bimatoprost implant in the period from July 23, 2020, to January 28, 2022. One patient was excluded from the study because the patient had multiple retinal detachments and underwent vitrectomies and endolaser, with use of gas and silicone oil, both prior to and subsequent to the bimatoprost implant administration.
Baseline characteristics of the included patients treated with the bimatoprost implant are shown in Table 1. The study population was predominately White and elderly; the mean age was 80.4 years. Most of the patients (87.6%) received the bimatoprost implant bilaterally at separate visits (at least a week apart) for the implant administrations in the right and left eyes. Most eyes (85.3%) treated with the bimatoprost implant were diagnosed with OAG, almost all (94.9%) were pseudophakic, all (100%) had been previously treated with a topical PGA, and 41.6% had previously been treated with SLT to lower IOP (Table 2). At the time of the bimatoprost implant administration, 94.9% of the eyes were being treated with topical IOP-lowering medication; this topical treatment usually included a PGA (Table 2).
 |
Table 1 Patient Demographics (Full Analysis Set) |
 |
Table 2 Baseline Characteristics of Eyes Treated with Bimatoprost Implant (Full Analysis Set) |
Most of the study eyes (83.8%, 165/197) had data available from at least 11 months of follow-up after the implant administration. Eyes with less than 11 months of follow-up data were either lost to follow-up (26 eyes) or were the second eye of the patient to receive an implant, and the second implant administration was less than 11 months before the stop date for data collection (6 eyes).
Effect on IOP
Treated eyes showed a decrease in IOP that was sustained through 1 year after the administration of the bimatoprost implant (Figure 1A). The mean IOP was 16.6 mmHg at baseline and ranged from 11.9 to 14.1 mmHg during the follow-up visit windows. At 11–13 months, the mean IOP was 13.3 mmHg (n = 148). Mean changes in IOP from baseline during follow-up ranged from −2.1 to −4.7 mmHg; mean percentage reductions in IOP from baseline ranged from 12.3% to 27.9%. To reduce a possible confounding effect of SLT performed prior to the bimatoprost implant administration, the analysis was repeated in the subgroup of eyes that had no SLT procedure within 6 months before baseline, with similar results (Figure 1B).
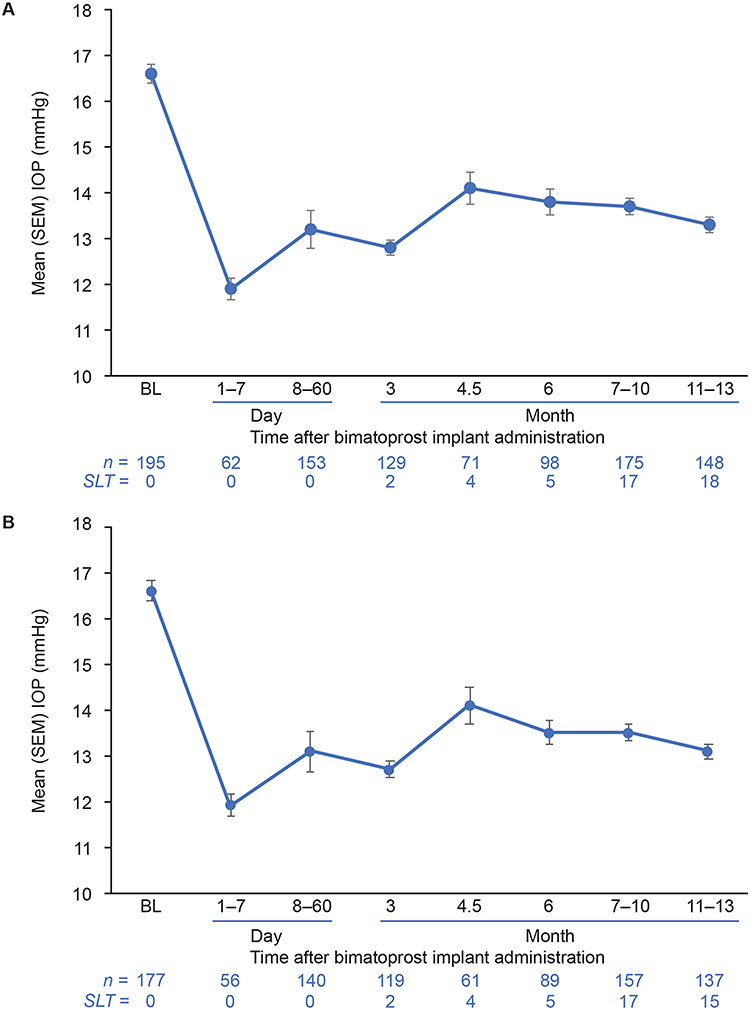 |
Figure 1 Mean IOP at baseline and after bimatoprost implant administration. (A) All eyes. (B) Eyes with no SLT procedure within 6 months prior to baseline. Error bars indicate the standard error of the mean (SEM). The number of eyes with data available within each visit window is indicated by n. The number of eyes that received SLT after the bimatoprost implant administration is indicated by SLT. Abbreviations: BL, baseline; IOP, intraocular pressure; SLT, selective laser trabeculoplasty. |
Use of topical IOP-lowering medications also decreased after administration of the bimatoprost implant (Figure 2A). Topical PGAs used at baseline were discontinued in all eyes. The mean number of IOP-lowering medications used was 1.4 at baseline before the implant administration and 0.2 at 11–13 months post administration; the median number of IOP-lowering medications used was 1 at baseline and 0 throughout follow-up. Mean change from baseline in the number of IOP-lowering medications used ranged from −1.0 to −1.6 medications during follow-up visit windows through 1 year after the bimatoprost implant administration. At 11–13 months, among all 148 eyes with data available, 133 (89.9%) were receiving no topical IOP-lowering medication, and 123 (83.1%) had undergone no additional IOP-lowering procedure after the bimatoprost implant administration. Twenty-five (16.9%) eyes had undergone an IOP-lowering procedure (mainly SLT) after the implant administration, and 7 eyes had received SLT within 4 months before the bimatoprost implant administration. A similar reduction in topical IOP-lowering medication use was observed in the subgroup of eyes that did not undergo SLT within the 6 months prior to the bimatoprost implant administration (Figure 2B).
 |
Figure 2 Mean number of topical IOP-lowering medications used at baseline and after bimatoprost implant administration. (A) All eyes. (B) Eyes with no SLT procedure within 6 months prior to baseline. Fixed combinations of two medication classes are counted as two medications. Error bars indicate the standard error of the mean (SEM). The number of eyes with data available within each visit window is indicated by n. The number of eyes that received SLT after the bimatoprost implant administration is indicated by SLT. Abbreviations: BL, baseline; IOP, intraocular pressure; SLT, selective laser trabeculoplasty. |
IOP reductions in eyes receiving no topical IOP-lowering treatment were observed up to 1 year after the bimatoprost implant administration (Figure 3). Most of these eyes had been treated with one topical IOP-lowering medication at the time of the implant treatment, and the bimatoprost implant treatment replaced the eye drop use and provided additional IOP lowering. At 11–13 months, 15.8% of the drop-free eyes had received SLT treatment after the bimatoprost implant administration, and 84.2% had not (Figure 3).
 |
Figure 3 Mean change in IOP from baseline after bimatoprost implant administration in eyes receiving no topical IOP-lowering medication. Error bars indicate the standard error of the mean (SEM). The number of eyes not being treated with topical IOP-lowering medication that had data available within each visit window is indicated by n. The number of those eyes that had received SLT within 4 months prior to or at any time after the bimatoprost implant administration is indicated by SLT. Abbreviations: IOP, intraocular pressure; SLT, selective laser trabeculoplasty. |
Subgroup of Eyes That Did Not Receive SLT
As in the total study population, IOP and the number of topical IOP-lowering medications used were reduced after bimatoprost implant administration in the subgroup of 103 eyes that had no history of SLT and did not receive SLT after the bimatoprost implant administration (Table 3).
 |
Table 3 IOP and Number of Topical IOP-Lowering Medications Used in the Subgroup of Eyes That Did Not Receive SLT Before or After the Bimatoprost Implant |
Subgroups Treated with Both SLT and Bimatoprost Implant
Reductions in IOP and topical IOP-lowering medication use after implant administration also occurred in eyes that received both the bimatoprost implant and SLT. Among the 197 eyes treated with bimatoprost implant, 94 (47.7%) also were treated with SLT, either both before and after the bimatoprost implant administration (16 eyes, 8.1%), before the bimatoprost implant administration only (66 eyes, 33.5%), or after the bimatoprost implant administration only (12 eyes, 6.1%). Some eyes had repeat SLT before or after the bimatoprost implant administration. When used before the bimatoprost implant, the SLT was weeks to years before the implant administration, and when used after the bimatoprost implant, the SLT was weeks to months after the implant administration. For the 82 eyes with a history of SLT, the mean (SD) (range) time from the most recent SLT procedure to the implant administration was 1055 (836) (14–2516) days. For the 28 eyes that received SLT after the bimatoprost implant, the mean (SD) (range) time from the bimatoprost implant administration to the first post-implant SLT procedure was 200 (84, 33–380) days.
The subgroup of eyes that received their last SLT procedure before the implant administration demonstrated consistent reductions in IOP from baseline throughout follow-up (Figure 4A). The mean change in IOP from baseline in these eyes at 11–13 months was −3.2 mmHg (n = 46) (Figure 4A). In contrast, the subgroup of eyes that received their last SLT procedure after the implant administration showed similar reductions in IOP from baseline at early visits after the implant administration but a reduced effect after several months (Figure 4A), consistent with the clinical decision to perform SLT. Eyes that underwent SLT after the bimatoprost implant administration also demonstrated a −3.2 mmHg mean change in IOP from baseline at 11–13 months (n = 20) (Figure 4A). The mean number of topical IOP-lowering medications used at baseline before bimatoprost implant administration was 1.4 and 1.5 in the subgroups with last SLT procedure before and after the implant administration, respectively, and was reduced throughout follow-up in both subgroups (Figure 4B).
 |
Figure 4 Outcomes in eyes that received both the bimatoprost implant and SLT in subgroups by timing of the last SLT procedure (before or after the bimatoprost implant administration). (A) Mean change in IOP from baseline. (B) Mean number of topical IOP-lowering medications used. Error bars indicate the standard error of the mean (SEM). The number of eyes in each subgroup with data available within each visit window is indicated by n. Abbreviations: BL, baseline; IOP, intraocular pressure; SLT, selective laser trabeculoplasty. |
Subgroup with Previous MIGS
Favorable effects of the bimatoprost implant on IOP and the need for topical IOP-lowering medications were also seen in the subgroup of eyes that had previously undergone ab interno trabeculotomy with the Trabectome (NeoMedix; Tustin, CA) device. Among the 39 eyes with a history of ab interno trabeculotomy, 32 had data available at 11–13 months after the bimatoprost implant administration. For these 32 eyes, at 11–13 months the mean (SD) IOP change from baseline was −3.2 (2.27) mmHg and the mean (SD) change from baseline in number of topical IOP-lowering medications used was −1.4 (0.83). All 32 eyes required no topical IOP-lowering medications at 11–13 months. Ten of these eyes had received SLT only before the bimatoprost implant, and 3 of these eyes had received SLT after the implant.
Safety Findings
The overall safety profile of the bimatoprost implant was favorable. No eye required implant removal, and there were no observations of impaired corneal endothelial health on slit-lamp examination after implant administration. Because there were no cases of concern, no endothelial cell counts were performed for any eye. One eye had corneal edema associated with preexisting disease. Conjunctival injection in the implant-treated eye was reported at the first follow-up visit in 22 of the patients. There were two cases of iritis, but in each case, the iritis occurred in the fellow eye, not the eye treated with the bimatoprost implant. There were no findings of anterior chamber cells in eyes treated with the bimatoprost implant. During the study, OCT evaluation of the macula was performed in 22 eyes with vision problems. Epiretinal membranes, macular pucker, or macular hole were identified in 9 eyes. Diabetic macular edema was identified in 1 eye and confirmed by a retina specialist. Age-related macular degeneration was identified in 12 eyes. No patient had macular edema associated with the bimatoprost implant.
Three eyes (in three patients) had uncontrolled IOP with the bimatoprost implant, SLT, and topical medications and underwent XEN 45 gel stent (Allergan, an AbbVie company) MIGS. One of these eyes had a high baseline IOP of 38 mmHg that did not respond to the implant. Another of these eyes had an increase in IOP from baseline to 32 mmHg within 2 months after the implant administration. No other implant-treated eye had an IOP increase of ≥10 mmHg from baseline within 2 months after the implant administration, although three eyes had IOP increase to 28 mmHg or higher during the 12 months after the implant administration (one eye with IOP of 28 mmHg at 8 months postadministration, one eye with IOP of 30 mmHg at 8 months postadministration, and one eye with IOP of 28 mmHg at 12 months postadministration).
Discussion
The bimatoprost implant demonstrated effectiveness and safety in this large case series of patients with OAG or OHT treated with a single implant in one or both eyes in routine clinical practice. Mean decreases in IOP were consistently observed through 1 year after the bimatoprost implant administration, while use of topical IOP-lowering medications in the implant-treated eyes decreased by an average of one medication. SLT was commonly part of the treatment algorithm. The study results suggest that a single administration of the bimatoprost implant can be used in untreated eyes or in replacement of topical medication to provide additional, sustained IOP lowering.
Intracameral injection is a safe and effective method to deliver medications intraocularly.12 The procedure requires aseptic technique and can be done in an examination or procedure room in the clinic or in an ambulatory surgical center.12 The patients in our study were usually administered the bimatoprost implant at an ambulatory surgical center. The procedure was well tolerated, and there were no serious complications. The only adverse effect associated with the administration procedure was conjunctival injection, which was observed in 21% of the patients treated with the bimatoprost implant.
The vast majority (94.9%) of eyes treated with the bimatoprost implant in this study were pseudophakic, and 83.8% had grade 4 angles. In comparison, in the ARTEMIS phase 3 registration trials of the bimatoprost implant, only 23.3% of eyes treated with bimatoprost implant 10 µg were pseudophakic,1 and approximately 66% had grade 4 angles (AbbVie, data on file). These differences in lens status and iridocorneal angle opening of the treated eyes may have contributed to the improved safety profile of the bimatoprost implant observed in this study.
Corneal health was the main safety concern in the ARTEMIS trials.3,5 In those trials, bimatoprost implant 10 or 15 µg was administered on day 1 and weeks 16 and 32. Corneal edema and endothelial cell loss were more frequent with the larger implant (bimatoprost implant 15 µg) and after repeated doses. The observed benefit/risk profile of the study treatments led to the US Food and Drug Administration approval of a single administration of the 10-µg dose strength of bimatoprost implant per eye. It is noteworthy that in the ARTEMIS studies, there were no adverse event reports of corneal edema or corneal endothelial cell loss after administration of bimatoprost implant 10 µg during the 16-week follow-up period before the second implant administration.1 In our study, no treatment-emergent adverse effects on the cornea were observed in the 197 eyes treated with the bimatoprost implant, and most of these eyes were followed for at least 11 months after administration of the implant. These findings are supportive of long-term safety of a single administration of bimatoprost implant 10 µg.
Nonadherence to topical IOP-lowering treatment regimens is endemic in glaucoma and associated with increased risk of vision loss.13–16 A sustained-release implant that lowers IOP and reduces the need for daily treatment with IOP-lowering drops has the potential to improve both treatment adherence and vision outcomes in patients with glaucoma.17 Our study results demonstrate that eyes with OAG or OHT that receive a bimatoprost implant in a clinical setting may be maintained on a reduced number of topical IOP-lowering medications through the following year. The majority of eyes, both in the total study population and in the subgroup of eyes that never underwent SLT, received daily drops of a single IOP-lowering medication before the implant administration and were drop-free at follow-up visits up to 11–13 months postadministration.
SLT is another therapy that can be used to give patients a “drop holiday”. SLT safely and effectively lowers IOP similarly to topical medication and reduces the need for daily eye drops.18,19 Moreover, SLT can be successfully repeated when the IOP-lowering effect of the initial procedure lessens over time.20 Our study results show that the bimatoprost implant can be used with SLT. IOP in treated eyes was reduced and eye drop usage decreased when the bimatoprost implant was administered in eyes that had previous SLT, as well as in eyes that were treated with SLT after the implant administration. A recent retrospective study of bimatoprost implant use in a clinical setting similarly reported that the efficacy of the implant is unaffected by a history of SLT.21 These results, along with the results of our study, suggest that the bimatoprost implant and SLT may be used together to extend patients’ “drop holiday”.
In our study, the IOP-lowering effects of a single bimatoprost implant were long lasting and observed through 1 year postadministration. These findings are consistent with previous results from two prospective clinical studies and a recently reported retrospective case series. In a phase 1/2 prospective study evaluating various dose strengths of the implant in patients with OAG, 23.8% (5/21) of the participants who received bimatoprost implant 10 µg completed the 24-month study without requiring rescue topical IOP-lowering medication or a second implant administration in the study eye.6 At month 24, the mean change in IOP from baseline in the study eye of those 5 participants was −7.4 mmHg.6 The 24-hour and sustained IOP-lowering effects of a single administration of bimatoprost implant 10 µg were subsequently evaluated in a prospective, 12-month, phase 3b study in patients with OAG or OHT.10 In that study, 74.2% (23/31) of study participants required no rescue IOP-lowering treatment in the implant-treated eye for 12 months postadministration, and the mean change in IOP from baseline at month 12 in the non-rescued, implant-treated eyes was −4.3 mmHg.10 Finally, in a retrospective case series of 46 eyes (in 38 patients) with OAG or OHT that were treated with a single bimatoprost implant in an academic clinical setting, 67.4% (31/46) of the eyes did not require restarting topical IOP-lowering medication or undergoing an IOP-lowering procedure over a mean period of 274 days follow-up.11 Together, these study results suggest long-lasting effects of the implant on IOP. These effects are sustained beyond the duration of drug release, as data from drug release assays in vitro, pharmacokinetic studies using animal models, and analysis of aqueous samples taken from human eyes treated with the bimatoprost implant indicate that the entire bimatoprost dose is released from the implant by 3–4 months postadministration.3
Because the polymers in the bimatoprost implant are biodegradable, there is no need to remove the residual implant after drug release is complete. The remnant implant decreases in size over time. In the ARTEMIS studies, at 12 months after the initial implant administration, 82% of the implants were reported to be ≤25% of their initial size or no longer visible. Consistently, in this study, visible implant in the treated eye(s) was noted through 1 year of follow-up in the medical records of the majority of patients. The polymers in the implant demonstrate ocular safety,4 and a small residual implant is not a safety concern.
In contrast to the carefully selected, generally healthy patient populations that typically participate in prospective clinical trials of treatments for OAG and OHT, the patients seen in clinical practice have diverse medical histories and treatment backgrounds. Studies in patients with varying demographic and clinical characteristics and disease severities, who may have concomitant conditions and be receiving ongoing therapies that could influence the effectiveness of the investigated treatment, are necessary to confirm treatment safety and effectiveness in the real world. In the present study, the bimatoprost implant was used in accordance with its prescribing information22 as medically indicated. The eyes treated with the bimatoprost implant were diagnosed with OAG of all stages, or OHT, and were primarily pseudophakic with grade 4 angles. Eyes with prior MIGS and SLT were also included. The study results suggest that the bimatoprost implant is a valuable treatment option for eyes with these characteristics.
One limitation of this study is that it was conducted at a single practice. The proportion of patients who were White is representative of the US population, but quite a large proportion of patients identified as “Hispanic or mixed race”, and other races/ethnicities appeared to be underrepresented in the study population. Other study limitations are that the study was retrospective, and data were not available for all eyes within all visit windows because of the real-world setting. Some patients returned to the practice for scheduled visits regularly over 1 year, but others returned to the referring physician’s practice or for other reasons did not attend regular follow-up visits. Follow-up was not specified and varied by patient and schedule availability. Some fluctuations in the mean IOP between consecutive visit windows may have occurred because of study population sampling and missing data. Nonetheless, the mean IOP was consistently reduced throughout follow-up, with most treated eyes requiring no topical IOP-lowering medications or additional IOP-lowering procedures, indicating that in clinical practice, a single administration of the bimatoprost implant can provide effective IOP lowering for up to 1 year.
Conclusions
This study demonstrated that the intracameral bimatoprost implant can be safe and effective in lowering IOP in pseudophakic eyes with OAG or OHT in the clinical setting. The bimatoprost implant reduces the need for topical IOP-lowering medication and can give patients a reprieve from using eye drops while providing additional IOP lowering. The bimatoprost implant is compatible with SLT.
Abbreviations
IOP, intraocular pressure; MIGS, microincisional glaucoma surgery; OAG, open-angle glaucoma; OHT, ocular hypertension; PGA, prostaglandin analog/prostamide; SD, standard deviation; SLT, selective laser trabeculoplasty.
Data Sharing Statement
AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual, and trial-level data (analysis data sets), as well as other information (eg, protocols, clinical study reports, or analysis plans), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications. These clinical trial data can be requested by any qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan (SAP), and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time after approval in the US and Europe and after acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process or to submit a request, visit the following link: https://www.abbvieclinicaltrials.com/hcp/data-sharing/.
Acknowledgments
A contract research organization, iuvo BioScience, LLC (Rush, NY) performed the data analysis. Medical writing assistance was provided to the authors by Evidence Scientific Solutions, Inc (Philadelphia, PA) and funded by AbbVie. All authors had access to relevant data and participated in the drafting, review, and approval of this publication. No honoraria or payments were made for authorship.
Funding
AbbVie funded this study and participated in the study design; data interpretation; and the preparation, review, and approval of the manuscript.
Disclosure
Savak Teymoorian is a consultant for Aerie, Alcon, Allergan (an AbbVie company), Bausch + Lomb, Ellex, Glaukos, MDBackline.com, and Omeros; has received research funding from Aerie, Allergan (an AbbVie company), and Bausch + Lomb; and receives royalties from Slack. E Randy Craven and Erica Werts are employees of AbbVie and may hold stock. Lannhi Nguyen has no financial relationships to disclose.
References
1. Medeiros FA, Sheybani A, Shah MM, et al. Single administration of intracameral bimatoprost implant 10 µg in patients with open-angle glaucoma or ocular hypertension. Ophthalmol Ther. 2022;11(4):1517–1537. doi:10.1007/s40123-022-00527-6
2. Weinreb RN, Bacharach J, Brubaker JW, et al. Bimatoprost implant biodegradation in the phase 3, randomized, 20-month ARTEMIS studies. J Ocul Pharmacol Ther. 2023;39(1):55–62. doi:10.1089/jop.2022.0137
3. Medeiros FA, Walters TR, Kolko M, et al. Phase 3, randomized, 20-month study of bimatoprost implant in open-angle glaucoma and ocular hypertension (ARTEMIS 1). Ophthalmology. 2020;127(12):1627–1641. doi:10.1016/j.ophtha.2020.06.018
4. Lee SS, Hughes P, Ross AD, Robinson MR. Biodegradable implants for sustained drug release in the eye. Pharm Res. 2010;27(10):2043–2053. doi:10.1007/s11095-010-0159-x
5. Bacharach J, Tatham A, Ferguson G, et al. Phase 3, randomized, 20-month study of the efficacy and safety of bimatoprost implant in patients with open-angle glaucoma and ocular hypertension (ARTEMIS 2). Drugs. 2021;81(17):2017–2033. doi:10.1007/s40265-021-01624-9
6. Craven ER, Walters T, Christie WC, et al. 24-Month phase I/II clinical trial of bimatoprost sustained-release implant (Bimatoprost SR) in glaucoma patients. Drugs. 2020;80(2):167–179. doi:10.1007/s40265-019-01248-0
7. Lee SS, Dibas M, Almazan A, Robinson MR. Dose-response of intracameral bimatoprost sustained-release implant and topical bimatoprost in lowering intraocular pressure. J Ocul Pharmacol Ther. 2019;35(3):138–144. doi:10.1089/jop.2018.0095
8. Weinreb RN, Robinson MR, Dibas M, Stamer WD. Matrix metalloproteinases and glaucoma treatment. J Ocul Pharmacol Ther. 2020;36(4):208–228. doi:10.1089/jop.2019.0146
9. Stamer WD, Perkumas KM, Kang MH, Dibas M, Robinson MR, Rhee DJ. Proposed mechanism of long-term intraocular pressure lowering with the bimatoprost implant. Invest Ophthalmol Vis Sci. 2023;64(3):15. doi:10.1167/iovs.64.3.15
10. Weinreb RN, Christie WC, Medeiros FA, et al. Single administration of bimatoprost implant: effects on 24-hour intraocular pressure and 1-year outcomes. Ophthalmol Glaucoma. 2023;6(6):599–608. doi:10.1016/j.ogla.2023.06.007
11. Xu W, Zhou P, Kansara ND, Frankfort BJ, Blieden LS, Chang PT. Intraocular pressure and eyedrop usage reduction with intracameral bimatoprost implant. J Ocul Pharmacol Ther. 2023;39(6):398–403. doi:10.1089/jop.2023.0013
12. Liebmann JM, Barton K, Weinreb RN, et al. Evolving guidelines for intracameral injection. J Glaucoma. 2020;29 Suppl 1:S1–S7. doi:10.1097/IJG.0000000000001451
13. Olthoff CM, Schouten JS, van de Borne BW, Webers CA. Noncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension an evidence-based review. Ophthalmology. 2005;112(6):953–961. doi:10.1016/j.ophtha.2004.12.035
14. Yeaw J, Benner JS, Walt JG, Sian S, Smith DB. Comparing adherence and persistence across 6 chronic medication classes. J Manag Care Pharm. 2009;15(9):728–740. doi:10.18553/jmcp.2009.15.9.728
15. Konstas AG, Maskaleris G, Gratsonidis S, Sardelli C. Compliance and viewpoint of glaucoma patients in Greece. Eye. 2000;14(Pt 5):752–756. doi:10.1038/eye.2000.197
16. Sleath B, Blalock S, Covert D, et al. The relationship between glaucoma medication adherence, eye drop technique, and visual field defect severity. Ophthalmology. 2011;118(12):2398–2402. doi:10.1016/j.ophtha.2011.05.013
17. Lewis RA, Christie WC, Day DG, et al. Bimatoprost sustained-release implants for glaucoma therapy: 6-month results from a phase I/II clinical trial. Am J Ophthalmol. 2017;175:137–147. doi:10.1016/j.ajo.2016.11.020
18. Garg A, Gazzard G. Selective laser trabeculoplasty: past, present, and future. Eye. 2018;32(5):863–876. doi:10.1038/eye.2017.273
19. Chi SC, Kang YN, Hwang DK, Liu CJ. Selective laser trabeculoplasty versus medication for open-angle glaucoma: systematic review and meta-analysis of randomised clinical trials. Br J Ophthalmol. 2020;104(11):1500–1507. doi:10.1136/bjophthalmol-2019-315613
20. Jang HJ, Yu B, Hodge W, Malvankar-Mehta MS. Repeat selective laser trabeculoplasty for glaucoma patients: a systematic review and meta-analysis. J Curr Glaucoma Pract. 2021;15(3):117–124. doi:10.5005/jp-journals-10078-1302
21. Wong MK, Bowers ME, Ventimiglia J, et al. Short-term outcomes of bimatoprost sustained-release intracameral implant in glaucoma. J Glaucoma. 2023;32(9):738–743. doi:10.1097/IJG.0000000000002271
22. Allergan. Durysta (bimatoprost implant) prescribing information. 2020; Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/211911s000lbl.pdf.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.