Back to Journals » Risk Management and Healthcare Policy » Volume 16
Real-World Prescribing Patterns for Hypertensive Children in China from 2018 to 2021: A Cross-Sectional Multicenter Study
Authors Qian Q, Wang YZ, Kan LD ![]() , Chen J, Wang C, Han G, Li LC
, Chen J, Wang C, Han G, Li LC ![]() , Lou WJ
, Lou WJ
Received 11 October 2022
Accepted for publication 18 February 2023
Published 27 February 2023 Volume 2023:16 Pages 287—299
DOI https://doi.org/10.2147/RMHP.S392224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Qin Qian,* Yu-Zhen Wang,* Lian-Di Kan,* Jie Chen, Chen Wang, Gang Han, Liu-Cheng Li, Wei-Jian Lou
Department of Pharmacy, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, 310016, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liu-Cheng Li; Wei-Jian Lou, Department of Pharmacy, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, 310016, People’s Republic of China, Tel/Fax +86-571-8600-6803, Email [email protected]; [email protected]
Background: Pediatric hypertension become an early marker of cardiovascular diseases, but their antihypertensive drug use patterns are rarely known.
Purpose: To investigate the epidemiological characteristics of pediatric hypertension and the use of antihypertensive drugs in the real world in China.
Methods: In this study, the demographic, diagnosis, and medication prescription data including the antihypertensive drug types and comorbidities, were analyzed. The antihypertensive drugs use were evaluated according to the Chinese guidelines for hypertension.
Results: 1301 prescriptions (number of visits) containing 1880 antihypertensive medical orders were collected. The average number of antihypertensive drugs per prescription was 1.45 (± 0.75). The patients aged 16 to 18 (70.18%) accounted for the highest proportion. Kidney diseases (33.28%) were the most common comorbidities. Calcium channel blocker (CCB), angiotensin II receptor blocker (ARB), and β receptor blocker (BB) were the most used antihypertensive drugs. The most frequent monotherapy was CCB, while that of two and three drugs combination were ARB+CCB and ARB+BB+CCB, respectively. Metoprolol (11.44%), nifedipine (10.64%), amlodipine (10.59%), valsartan (6.12%) were the most commonly used antihypertensive drugs. The utilization rate of fixed compound preparations was 7.34%. However, the percentage of recommended antihypertensive drugs was just 14.20%, while the recommended drug combination was 84.93% according to the guidelines.
Conclusion: For the first time ever we reported the antihypertensive prescription analysis in children in a large area of China. Our data provided new insights into the epidemiological characteristics and drug use in hypertensive children. We found that the guidelines for medication management in hypertensive children were not routinely followed. The wide use of antihypertensive drugs in children and those with weak clinical evidence raised concerns regarding its rational use. The findings could lead to more effective management of hypertension in children.
Keywords: hypertensive children, antihypertensive drugs, drug combination, prescription
Introduction
Hypertension is a major threat to global health affecting millions of families.1–3 It has become a major influencing factor in the risk of cardiovascular disease, therapeutic effect of complications, and a leading cause of serious adverse events including death worldwide.4–7 Hypertension has been recently reported to have a prevalence of 2.5% among children in Ghana.8 In a Chinese national survey, the hypertension prevalence of pediatric population aged 7 to 17 years was reported to be 4.4% to 6.4% from 1995 to 2014.9 In recent Chinese guidelines for hypertension, the prevalence of hypertension in children under the age of 18 ranged from 4% to 5%.10 However, the incidence may be underrated due to the lack of diagnosis in clinical practice, which prevents the guideline-based treatment management including lifestyle changes and medication.11 About 40% of hypertensive children developed adult hypertension without intervention, which had a significantly increased risk of cardiovascular diseases in their adulthood.10 A comprehensive strategic approach for controlling hypertension, including pivotal antihypertensive treatment management is urgently needed.12
Antihypertensive treatment was clearly recommended for symptomatic stage 1 hypertensive children or continuously abnormal blood pressure after 3–6 months without drug treatment, and for all stage 2 hypertensive children.10 Although studies on the treatment of adult hypertension in recent years are increasing, the scope of medication for hypertensive children is narrow, and its clinical medication management is rarely reported. In China, there are limited real-world prescribing studies on antihypertensive use.13 How to use antihypertensive drugs safely, effectively and reasonably in hypertensive patients, especially in children, has attracted widespread attention. There are many epidemiological studies on childhood hypertension in different regions, but few studies are devoted to exploring the optimized treatment options for children diagnosed with hypertension. Besides, the evidence of the treatment strategies is insufficient, and the treatment drugs are limited.
In order to understand the epidemiological characteristics of pediatric hypertension and how pharmacologic treatment with antihypertensive drugs are used, for the first time ever we reported a cross-sectional study on the antihypertensive prescriptions in a large area of China. The demographic, diagnosis, and medication prescription data, including the proportion of different antihypertensive drug classes and comorbidities were retrospectively analyzed. To determine the extent to which the national guidelines for the management of childhood hypertension were followed, the rationality of antihypertensive drugs use and drug combination were evaluated according to recent Chinese guidelines for hypertension.10
Methods
Study Design
This multicenter and cross-sectional study was in line with the guidelines of World Medical Association and Declaration of Helsinki. The Ethics Committee of Sir Run Run Shaw Hospital had reviewed the study protocol and confirmed that the formal ethic approval was not required because this study only involved prescription data from the database of Hospital Prescription Cooperation Project which was widely used as described from previous studies.14,15 Informed consent was also waived by the ethic committee (Approval number, 20220131). Permission was obtained to access the database and all the data used was de-identified upon data collection.
Data Collection
Antihypertensive prescription details were extracted and standardized according to the database of Hospital Prescription Cooperation Project, which was widely used.14–16 The project is an extensive medical record procurement database covering public hospitals in nine cities in China. More than 100 hospitals provided prescription data to the project for each sampling day, and 40 randomized sampling days each year (10 days/quarter) were included and standardized by engineers for research and decision-making. Our hospital is a member of the Hospital Prescription Cooperation Project which allows us to have open access to the prescription data in evaluating the use of drugs. In this study, prescription data from 127 hospitals in Beijing, Tianjin, Haerbin, Shenyang, Guangzhou, Zhengzhou, Hangzhou, Shanghai, and Chengdu were selected. These cities are the most economically developed areas in the local area. These hospitals were located in the east, west, south, and north of China, and thus covered a wide geographic area in China. The guidelines defined the age of a child as under 18.10,17 We started with a preliminary collection of hypertension prescriptions for all ages, then we extracted the pediatric prescriptions for final analysis, which should meet the following criteria: 1) prescriptions with a diagnosis of hypertension, but with no restrictions on diagnostic criteria or levels of hypertension; 2) outpatient prescriptions; 3) aged ≤18 years old; 4) prescription date from the first quarter of 2018 to the second quarter of 2021; and 5) prescribed at least one antihypertensive drug class. The Emergency/Inpatient prescription records, adult prescriptions (aged >18 years old), and prescriptions without antihypertensive drug use were excluded. The included prescription information in this study contained city name, date, hospital grade, patients’ code, sex, age, prescription code, clinical department, insurance, generic name, drug specification, usage, as well as the diagnosis.
Assessment of Prescription Data
The demographic, diagnosis, and medication in the prescriptions, including the proportion of different antihypertensive drug classes and comorbidities were summarized and analyzed retrospectively. The pharmacological mechanisms of antihypertensive drugs were classified as angiotensin converting enzyme inhibitors (ACEI), angiotensin II receptor blocker (ARB), β receptor blocker (BB), calcium channel blocker (CCB), diuretics, α1 receptor blocker, α1, β blocker, central α2 receptor agonist, and/or their fixed compound preparations.
The demographic data and drug usage were estimated by prescription number (number of visits) and the proportions. The antihypertensive treatment regimens were divided into monotherapy, two drugs combination, three drugs combination, or more. The rationality of antihypertensive drugs use and drug combination were evaluated by following the 2018 Chinese Guidelines for Prevention and Treatment of Hypertension.10
Statistical Analyses
The antihypertensive prescription data were collected and stored in Microsoft Access software (Microsoft Corp., Redmond, WA, USA) and then transferred to Microsoft Office Excel® 2007 (Microsoft Corp., Redmond, WA, USA) for final statistical analysis. The categorical results were presented as number (n) and percentage (%). The average number of drugs per prescription and the average age were reported as mean (±standard deviations).
Results
Characteristics of Prescription Data
In this survey, hypertension prescriptions for children accounted for 0.027% (1301/4745 062) of all age groups. Finally, a total of 1301 antihypertensive prescriptions (number of visits) that met the inclusion criteria were finally enrolled in our study; 127 hospitals located at 9 major areas of China were included. Among them, Beijing, Chengdu, Tianjin, and Shanghai accounted for the top four in percentage. The average number of antihypertensive drugs per prescription was 1.45 (±0.75). From the prescription data (Table 1), we could disclosure that the highest prevalence of hypertension in children was male (68.18%; 887/1301). The patient sample had an average age of 15.16 (±4.38) years, with 86.32% (1123/1301) aged 13 to 18, and 13.68% (178/1301) under 12. In terms of hospital grade, one case (0.08%) was from community hospital, 42 cases (3.23%) were prescribed in local hospitals, and 1258 cases (96.69%) were prescribed in general hospitals. As for the insurance, 720 patients (55.34%) had reimbursement payments, while 581 patients (44.66%) were self-paid for medical treatment. From the eligible population, 541 children (41.58%) were diagnosed with hypertension without comorbidities. Surprisingly, 58.42% (760/1301) of them had comorbidities. Besides, 42 children (3.23%) were diagnosed with essential hypertension. The characteristics for hypertensive children are presented in Table 1.
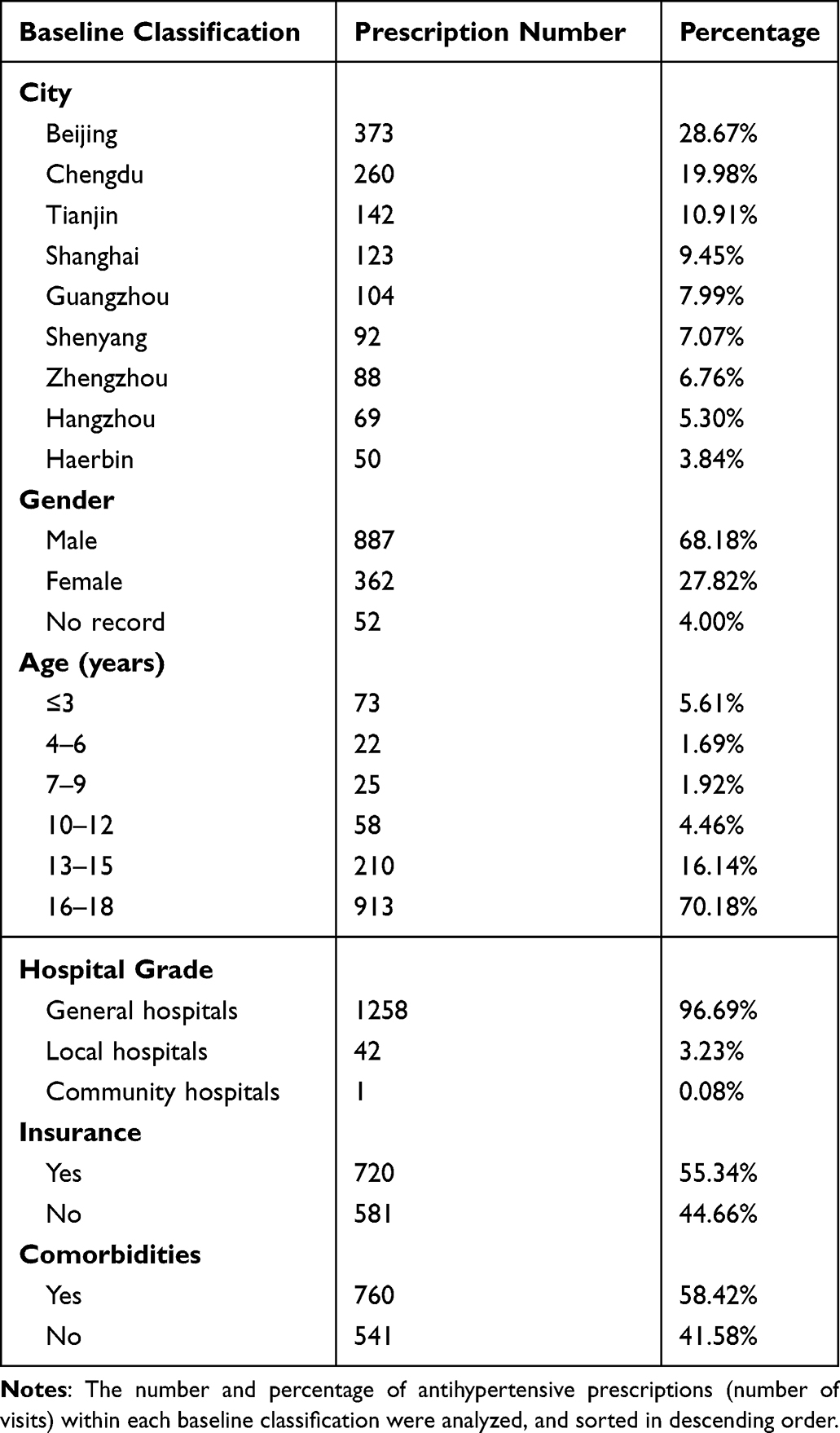 |
Table 1 Baseline Data for Hypertensive Children |
In this study, we found 48 clinical departments were prescribing antihypertensive drugs for children. Among them, the Cardiology Department (463/1301) accounted for the highest constituent ratio with 35.59%. The higher prescription rate was also found in Nephrology Department (300/1301), Pediatrics Department (54/1301), Rheumatology and Immunology Department (53/1301), General Medicine Department (53/1301), and Organ Transplantation Department (52/1301), with 23.06%, 4.15%, 4.07%, 4.07% and 4.00%, respectively, as shown in Figure 1A. Among the antihypertensive prescriptions, which were not found in Cardiology Department, 75.66% (634/838) of the patients were accompanied by comorbidities.
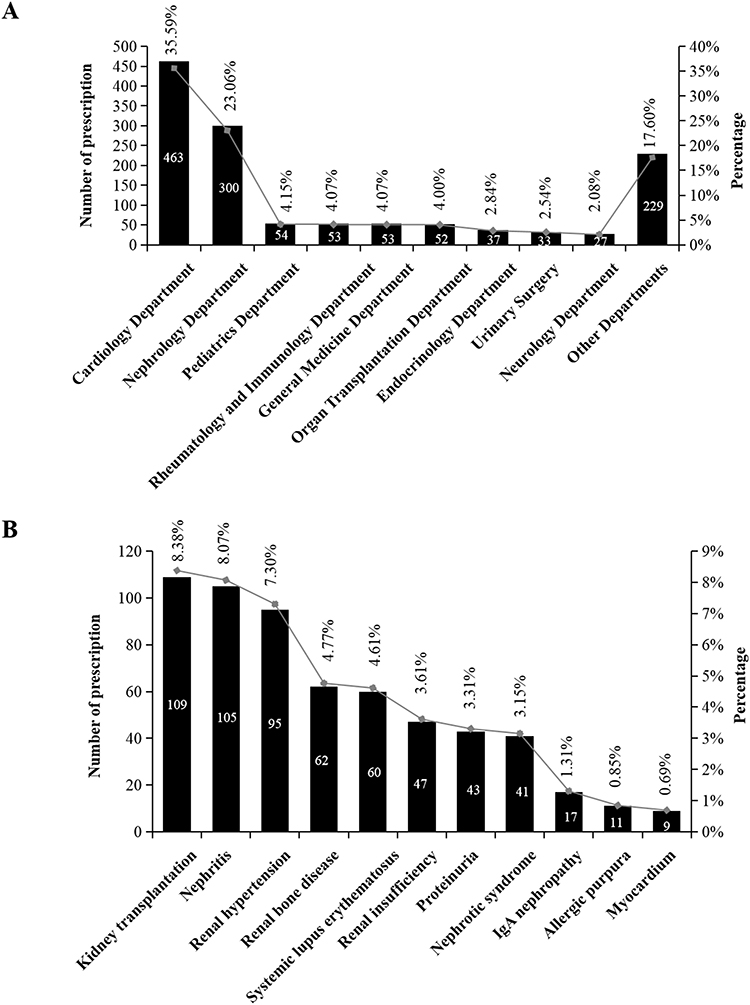 |
Figure 1 Antihypertensive prescriptions in different clinical departments (A) and comorbidities for hypertensive children (B). |
Comorbidities and Medication Frequency of Antihypertensive Drugs for Hypertensive Children
Comorbidities are major obstacles to the management of hypertensive patients in the real world. Therefore, it is of paramount importance to elucidate the comorbidities among the hypertensive children to further understand the epidemiological characteristics of hypertension and facilitate the management of hypertension. In this study, we found that 33.28% of kidney diseases (433/1301) and 5.15% of systemic lupus erythematosus (67/1301) were the top two most common comorbidities among the hypertensive children, and then were myocardial injury, allergic purpura, and hemodialysis. Kidney transplantation, nephritis, renal hypertension, nephrotic syndrome, and renal bone disease were the most recorded kidney diseases in hypertensive children (Figure 1B).
According to the guidelines for hypertension treatment, the use of long-acting preparations once a day was recommended when choosing antihypertensive drugs.10 Multiple daily medications may indicate uncontrolled adherence, leading to substandard treatment outcomes. Thus, the use of short-acting preparations several times a day was not recommended as long-term treatment regimens for patients with hypertension. In this study, 1301 prescriptions (number of visits) containing 1880 antihypertensive medical orders (one prescription might contain several antihypertensive medical orders) were collected and analyzed. Among the medical orders, the most commonly used medication frequency was once daily (74.64%; 1421/1880), followed by twice daily (20.29%; 410/1880) and more frequently (5.07%; 49/1880).
Drugs for Treating Hypertension in Children
As shown in Table 2, the most frequent single component of antihypertensive drug classes were CCB, ARB, BB, and ACEI. Beyond that, 7.34% (138/1880) of antihypertensive drugs were fixed compound preparations. Among them, metoprolol, nifedipine, amlodipine, valsartan were the most frequently used antihypertensive drugs.
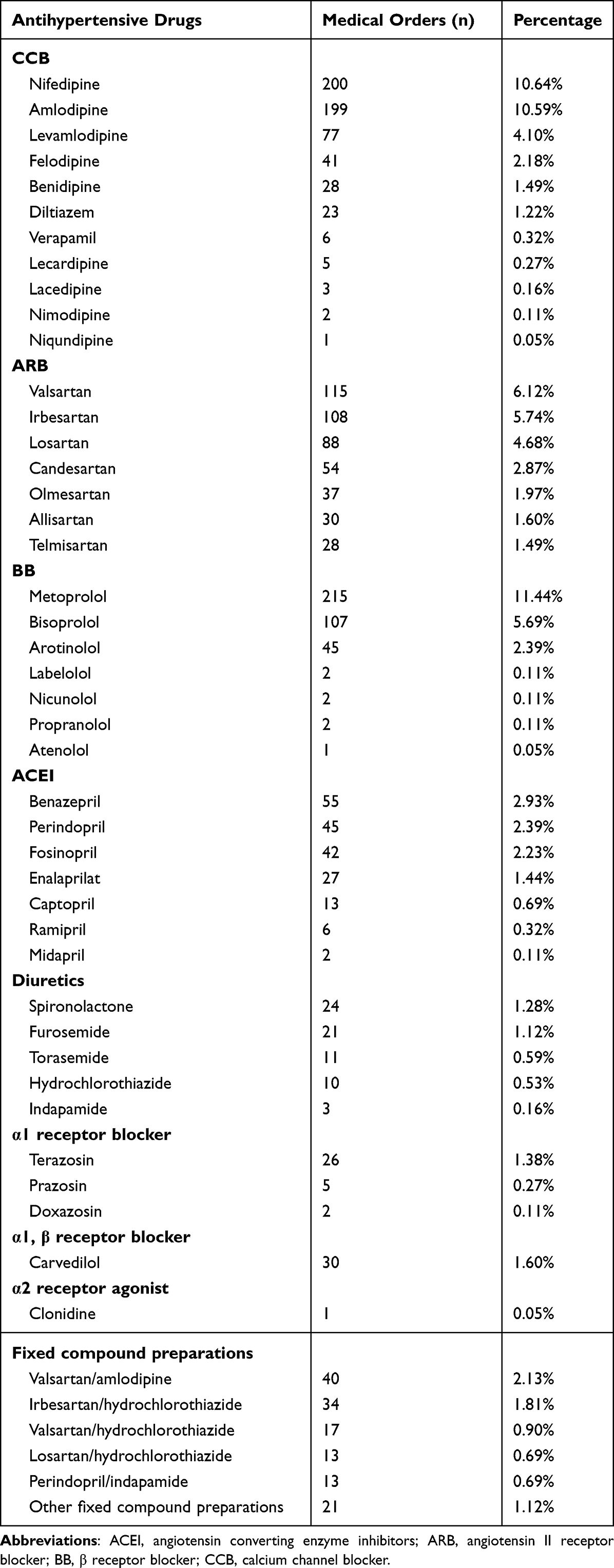 |
Table 2 Drugs for Treating Hypertensive Children |
As for the use of CCB in hypertensive children, the utilization rate of dihydropyridines is as high as 95.04% (556/585). Nifedipine, amlodipine, and levamlodipine were the most used drugs in CCB. Among the use of ARB, valsartan, irbesartan, and losartan were the most frequently prescribed agents. Besides, we found that metoprolol and benazepril were the most used BB and ACEI, respectively. We found that the rate of diuretic use was just 3.67% (69/1880). Spironolactone was the most used diuretics, while terazosin was the most used α1 receptor blocker. Moreover, carvedilol and clonidine were the only used α1, β receptor blocker and α2 receptor agonist, respectively, in this study. Among the fixed compound preparations, valsartan/amlodipine (28.99%; 40/138) and irbesartan/hydrochlorothiazide (24.64%; 34/138) were the most frequently prescribed agents.
According to the guidelines for hypertension treatment, the use of medication for children should based on drug instructions or updated clinical evidence.10 Based on the 2018 Chinese Guidelines for Prevention and Treatment of Hypertension, only amlodipine, captopril, propranolol, atenolol, hydrochlorothiazide, furosemide, and prazosin were recommended to be used for hypertensive children. In this survey, the application rate of above recommended antihypertensive drugs for children was just 14.20% (267/1880). The number of medical orders and proportion of each antihypertensive drug, which were used in the present prescription analysis are listed in Table 2.
Use of Antihypertensive Drug Classes in Different Age Groups
Further analysis was performed to investigate whether there were differences in medication choice of different ages among hypertensive children. Surprisingly, CCB was the most frequently prescribed antihypertensive drug class in all age groups. In addition to the group aged 4–6 years, ARB was second only to CCB in usage, followed by BB. The group aged 16–18 years had the highest use of all antihypertensive drug class. α1 receptor blocker was prescribed for hypertensive children aged over 7 years, especially for the patients over 16 years. Meanwhile, α1, β receptor blocker tended to be used for patients over 13 years and α2 receptor agonist was used for patients over 16 years. ARB/Diuretics was the most commonly used fixed compound preparations in all age groups. The number of medical orders for antihypertensive drugs in different age groups are listed in Table 3.
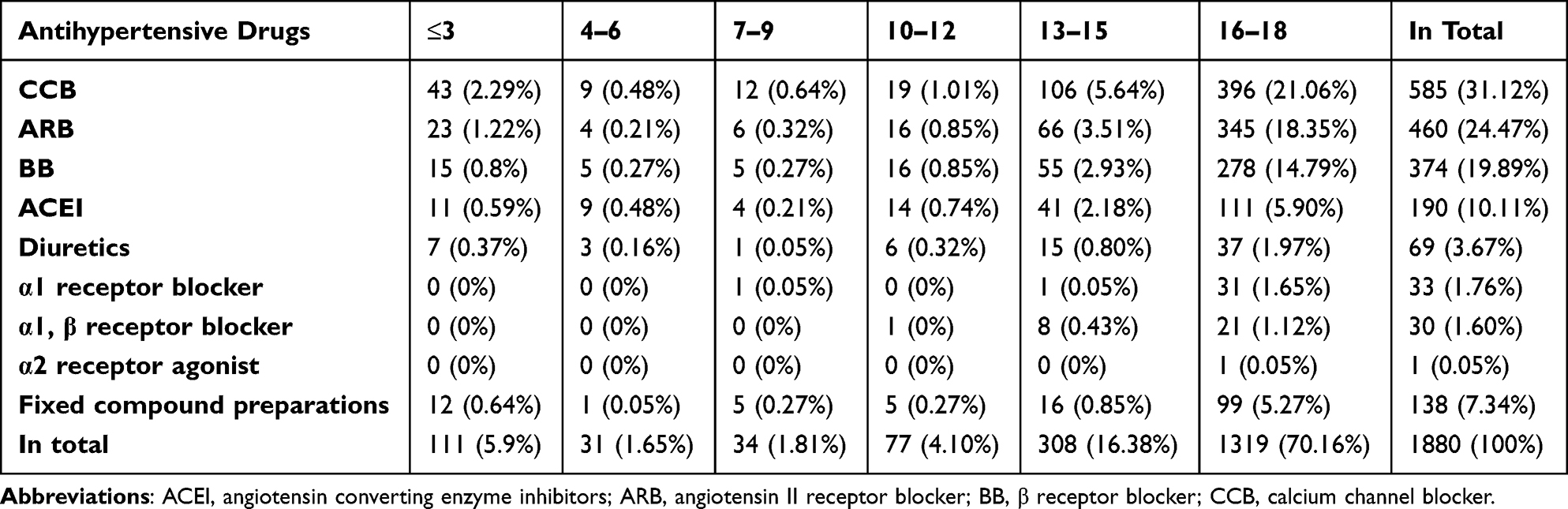 |
Table 3 Number and Percentage of Antihypertensive Medical Orders in Different Age Groups |
Regimens for Treating Hypertension in Children
The principle for treating hypertension in children is to start from single drug (ie monotherapy), and take into account individual treatment, adjust the treatment plan and treatment duration on the basis of the changes of curative effect and blood pressure level, and combine two or more antihypertensive drugs when necessary. The number of prescriptions and number of hypertensive children were the same value, but one prescription could contain 1 or more antihypertensive drugs. In this study, we considered the antihypertensive fixed compound preparations as two drugs combination due to their different pharmacological mechanisms in treating hypertension.
There were 67 antihypertensive regimens used for hypertensive children. The commonly used antihypertensive regimens were dominated by monotherapy, followed by two drugs combination, three drugs combination and four drugs combination (Figure 2A). Among the treatment regimens, the use of CCB, ARB, BB, ACEI, and ARB+CCB had the highest prescription rates (Figure 2B).
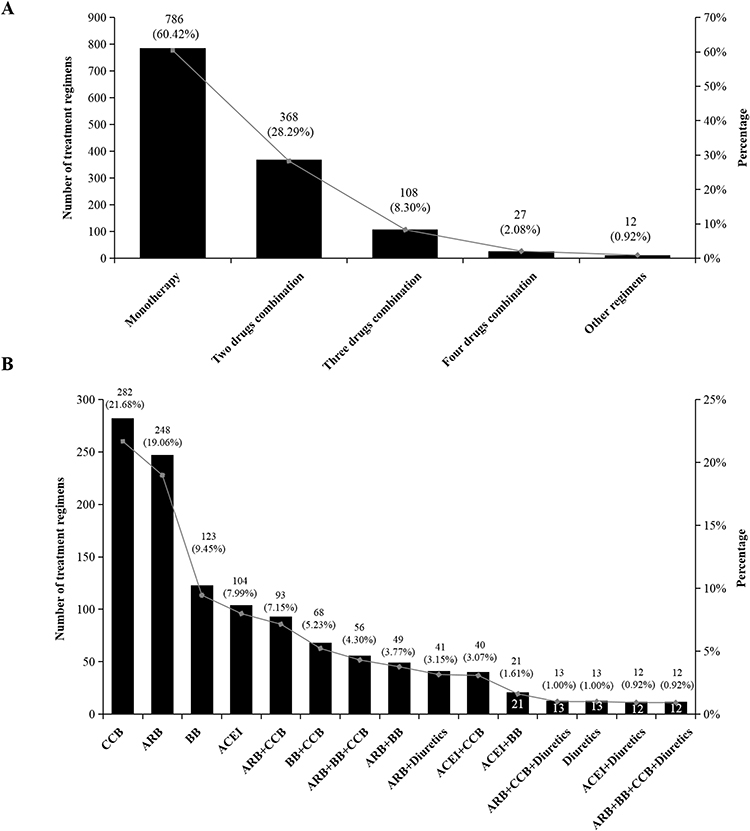 |
Figure 2 Number and percentage of different combination drug regimens (A) and the top 15 most used regimens (B) for treating hypertension in children. Abbreviations: ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin II receptor blocker; BB, β receptor blocker; CCB, calcium channel blocker. |
The most frequent monotherapy were CCB, ARB, and BB, while the most frequent two drugs combination were ARB+CCB, BB+CCB and ARB+BB. Among the three drugs combination, ARB+BB+CCB was the most used, followed by ARB+CCB+Diuretics and ACEI+BB+CCB. Among other drugs combinations, the most used regimen was ARB+BB+CCB+Diuretics, which was accounted for 0.92% (12/1301). The most used monotherapy, two drugs combination, three drugs combination, and four drugs combination were amlodipine, valsartan+amlodipine, valsartan+metoprolol+amlodipine, and irbesartan+metoprolol+levamlodipine+ hydrochlorothiazide, respectively. The number and proportion of different drugs combination as well as the most used drugs among the corresponding regimens are shown in Table 4.
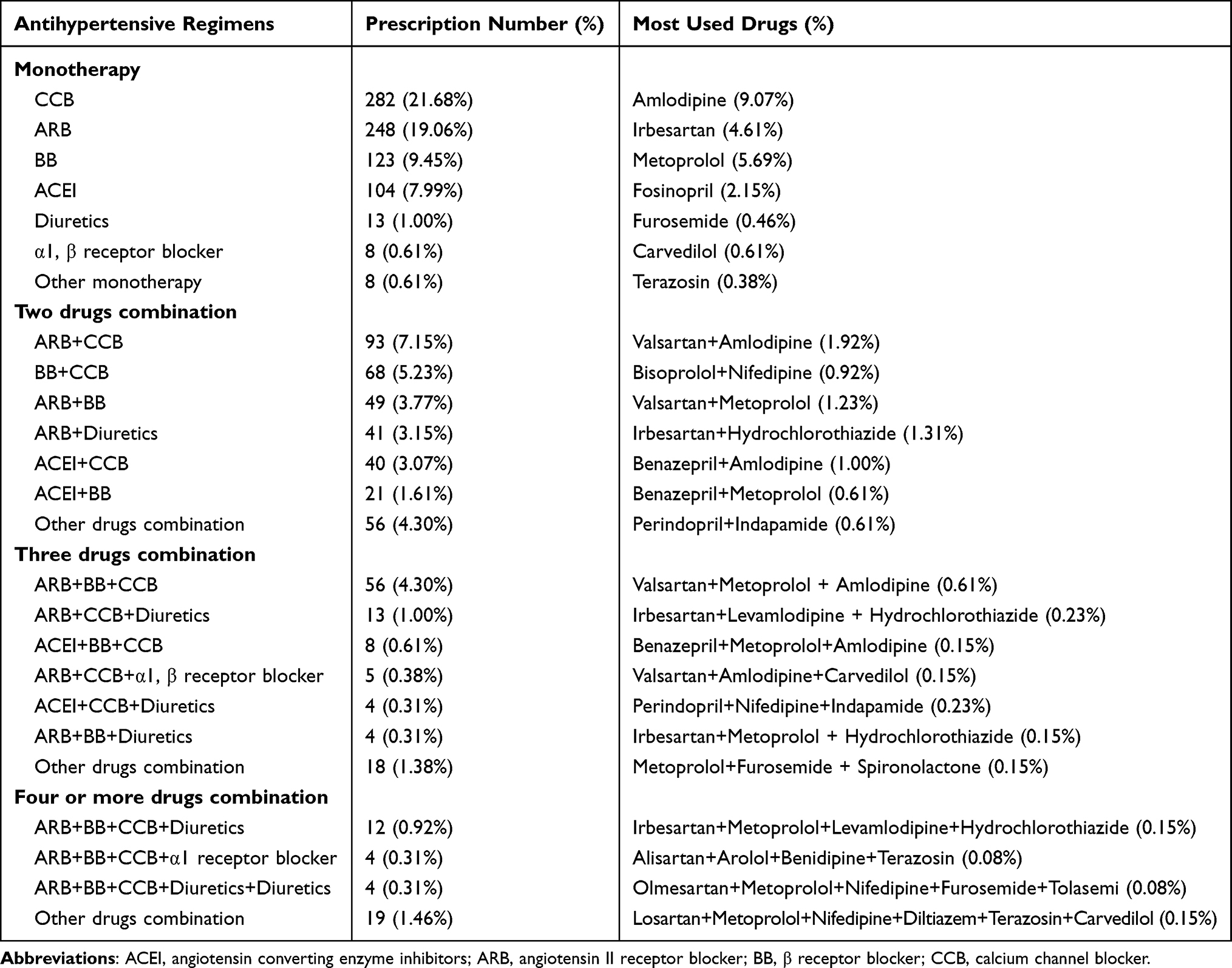 |
Table 4 Number and Percentage of Different Drugs Combination and the Most Used Drugs |
We further investigated whether there were differences in antihypertensive regimens in different age groups. In the groups aged ≤3, 7–9, and 13–15, the monotherapy CCB was the most prescribed antihypertensive regimens. The most used CCB were amlodipine for patients aged ≤3 and 13–15, but the most used CCB for patients aged 7–9 was nifedipine. Besides, the monotherapy ACEI was the most prescribed regimens in the groups aged 4–6 and 10–12. The most used ACEI were enalapril for patients aged 4–6, but the most used ACEI for patients aged 10–12 was fosinopril. For patients aged 16–18, the monotherapy ARB was the most used regimens, while losartan was the most used agents. The number and percentage of antihypertensive regimens in different age groups are listed in Table 5.
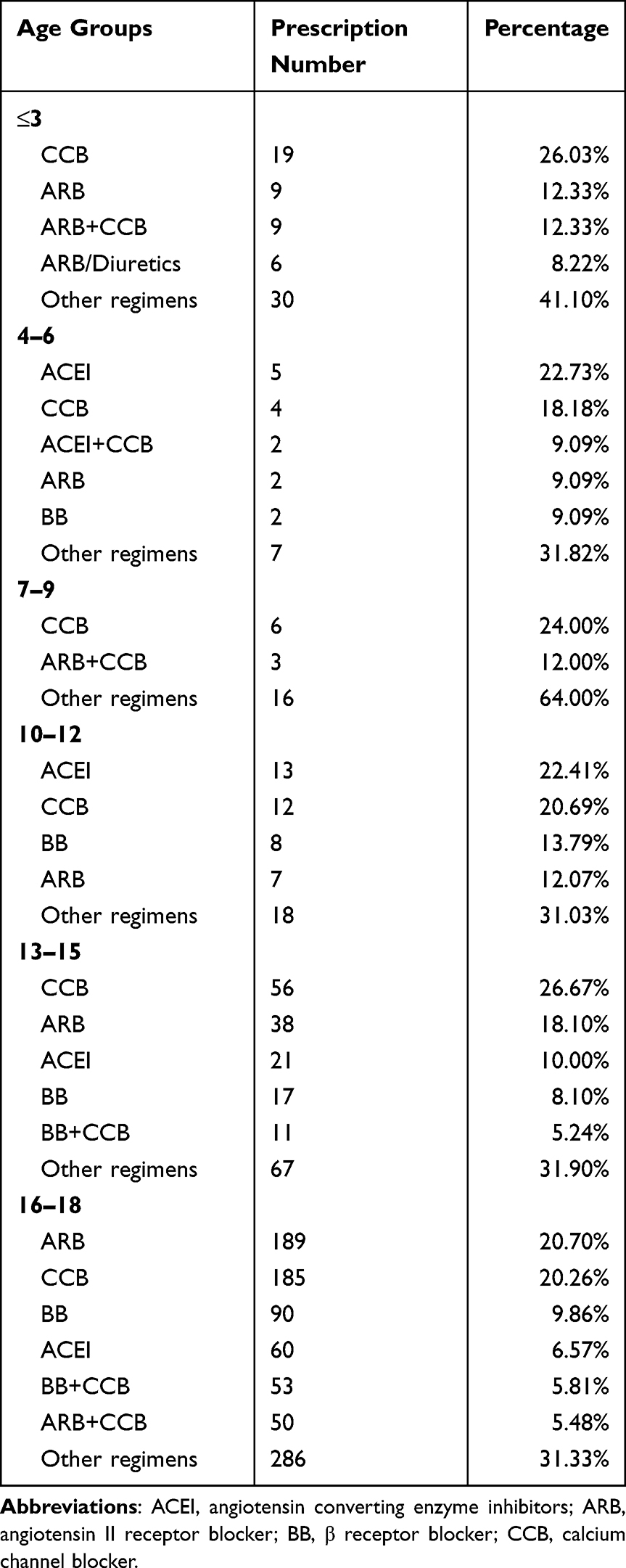 |
Table 5 Number and Percentage of Antihypertensive Regimens in Different Age Groups |
In this study, the application rate of recommended antihypertensive drugs for children from the guideline of China was just 14.20% (267/1880). At the same time, this guidelines also recommended not to use the regimens with ACEI+ACEI, ARB+ARB, ACEI+ARB, ACEI+BB, ARB+BB, CCB+CCB, α1 receptor blocker+α1, β receptor blocker, and BB+α2 receptor agonist. Here, the proportion of the recommended regimens for hypertensive children that followed the guidelines was 84.93% (1105/1301).
Discussion
Hypertension in children increases the risk of cardiovascular events in their adult period.12,18,19 Despite multifactorial factors were proven to influence the development of hypertension in children and several preventive measures were recommended, the incidence of hypertension in children has been on the rise in the past 20 years.19–21 To the best of our knowledge, the present multicenter study was the first report to investigate the epidemiologic characteristics for pediatric hypertension, and clarify how antihypertensive drugs were used among these patients in China through a real-world multicenter prescription analysis.
We identified that hypertension prescriptions for children just accounted for 0.027% of hypertension prescriptions for all ages. It was lower than the incidence of hypertension (1.7%) from a randomized trial,22 which may be due to the natural disadvantage of random sampling, inadequate diagnosis, or less aggressive drug interventions in younger populations. Our results also showed that hypertension was greater in boys than in girls, which was consistent with the guidelines for different regions.10,17 We found that hypertensive children were prescribed with ACEI, ARB, BB, CCB, diuretics, α1 receptor blocker, α1, β blocker, or α2 receptor agonist, from nine geographical regions in China. We disclosed that the most frequent single component of antihypertensive drug classes were CCB, ARB, BB, and ACEI. Of these antihypertensive drugs, metoprolol, nifedipine, and amlodipine were the most commonly used. Here, we found the constituent ratio of hypertensive children treated with monotherapy were 60.42% and the average number of antihypertensive drugs was 1.45 drugs/patient. 40.51% hypertensive children were prescribed more than two antihypertensive drugs. The most frequent two drugs combination was ARB+CCB and that of three drugs combination was ARB+BB+CCB. The utilization rate of fixed compound preparations among antihypertensive drugs was 7.34%. The fixed compound preparations were convenient to take and easy to improve compliance for patients, thus it should be first recognized by doctors if the patients needed more than two antihypertensive drugs.
In Canada’s 2020 guidelines for the treatment of hypertension in children, the recommended treatment included the groups of ACEI, ARB, CCB, and BB without specific drug designation.23 The updated pediatric hypertension guidelines issued by American Academy of Pediatrics showed that 19 kinds of single drugs among ACEI, ARB, thiazide diuretics, and CCB were recommended for the pharmacologic treatment in hypertensive children.17 However, only specific drugs including amlodipine, captopril, propranolol, atenolol, hydrochlorothiazide, furosemide, and prazosin were clearly recommended to be used for hypertensive children in the guidelines from China.10 Though these guidelines had different recommendations for the classification of antihypertensive drugs used for hypertensive children, the agents from ACEI and CCB were universally recommended.10,17,23
Based on the guidelines from China, our data revealed that the application rate of recommended antihypertensive drugs was just 14.20%.10 Diuretics were recommended for first-line treatment for hypertension due to their low side effect profile.10 But only 10.61% of them were prescribed. Folic acid supplementation was beneficial in hypertensive patients who had hyperhomocysteinemia (H-type hypertension) and reduced the risk of stroke.24 The low use of folic acid (2.69%) in this study indicated that clinicians did not pay enough attention to H-type hypertension and its potential risks.
Surprisingly, 58.42% hypertensive children had comorbidities in this study. Kidney disease (33.28%) was the most common comorbidities. We hypothesized that hypertension in these patients may be caused by the comorbidities. As is known that ACEI and ARB are beneficial for patients’ kidney function. But only captopril was approved ACEI for children while no drug was approved in ARB according to the guidelines.10 Here, we found 35.42% hypertensive children with renal impairment were prescribed with ACEI and ARB with the exception of captopril. We also found that 15.07% of the treatment regimens, including the prescription of two identical drugs, ARB+β-blocker, or ACEI+ARB, were not routinely recommended by the guidelines.10 Moreover, this study provided evidence that the reimbursement rate of antihypertensive drugs was just 55.34%, which was seriously inadequate.
This study covered general hospitals, community hospitals, and local hospitals in nine major cities of China. It was a systematic real-world study with large coverage, but there were still some limitations. First of all, though 127 hospitals were selected for this study, these hospitals were all from the database of Hospital Prescription Cooperation Project, and thus might not fully reflect the prescription characteristics in China. Besides, the total number of prescriptions for children was not as large as expected, possibly due to its low morbidity, not all children receiving clinical intervention, or the nature of random sampling. Secondly, it is difficult to evaluate the results of drug dosage because the information management systems in different hospitals differ in the way they write the drug dosage. Thirdly, due to the retrospective nature of this study, there was a lack of follow-up data on therapeutic changes in life style, hypertension grading, blood pressure control level, concomitant diseases, as well as clinical endpoint events. Whether the patients were contraindicated to certain antihypertensive drugs were difficult to determine based on the prescription records. It may affect the rationality of antihypertensive drugs use.
Fourthly, if some diagnosis of hypertension was not written in the prescriptions or some patients were not prescribed antihypertensive drugs by the doctor during the visits, there would be a lack of population data. Besides, some of the underdiagnosis and over-diagnosis may be due to the complexity of identifying children with hypertension in the range of normal blood pressure by gender, height percentile, and age, as well as improper identification of hypertension like abnormal blood pressure due to inaccurate measurements, pain, or white-coat hypertension. Accurate diagnosis and guideline-based treatment management seem to be equally important for effective treatment. Large samples are essential to explore the factors associated with the diagnosis and treatment for children hypertension. Unlike hypertension in adults that recommended the initiation of special antihypertensive agents, limited hypertension guidelines for children generally specified antihypertensive drugs initiation hierarchy.10,25 Thus, we could not judge what stage of hypertension was suitable for what antihypertensive drugs yet.
This study demonstrated the capabilities and limitations of pooling electronic medical record data from multiple different hospitals to create “big data” for researches. However, sharing data across systems is a challenge due to the lack of data standards and inconsistencies in data collection. The effectiveness of aggregating electronic medical record data for researches should increase with the widespread use of electronic medical records, the increasing ease of data extraction, and the affordable cost of supporting these observational researches. It is also recommended that the emerging clinical evidence should be fully evaluated to update future treatment regimens for hypertensive children. Clinical pharmacists should carry out professional pharmaceutical care for outpatient hypertensive children and provide comprehensive advice to prescribers.
Conclusions
We reported the antihypertensive prescription analysis in children in a large area of China and found the guidelines recommendations for selecting antihypertensive drugs for children were not well followed. It not only provided new insights into the epidemiological characteristics and drug use in hypertensive children, but also provided evidence for future antihypertensive prescription management in medical institutions. Future clinical practice involving the efficacy and safety of antihypertensive drugs in different age groups and larger data analysis, including real-world studies are strongly encouraged to improve the management of hypertension in children.
Abbreviations
ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin II receptor blocker; BB, β receptor blocker; CCB, calcium channel blocker; CNY, Chinese Yuan.
Data Sharing Statement
The original contributions are included in this article, further inquiries can be directed to the corresponding authors.
Ethics Statements
This study was approved by the Ethics Committee of our hospital. Written informed consent was not required for this study in line with the national legislation and institutional requirements.
Acknowledgments
The authors would like to give special thanks the Hospital Prescription Cooperation Project of China for collecting and providing the data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Zhejiang Provincial Science Technology Projects of Traditional Chinese Medicine (No. 2021ZB174), and the Zhejiang Provincial Natural Science Foundation of China (No. LYY19H280006).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xie K, Gao X, Bao L, Shan Y, Shi H, Li Y; UPPDATE Investigators. The integrated management of hypertension in general hospitals and community hospitals. Risk Manag Healthc Policy. 2021;14:2537–2545. doi:10.2147/RMHP.S306735
2. Jiang Q, Gong D, Li H, et al. Development and validation of a risk score screening tool to identify people at risk for hypertension in Shanghai, China. Risk Manag Healthc Policy. 2022;15:553–562. doi:10.2147/RMHP.S354057
3. Xu L, Wen X, Yang Y, Cui D. Trends and comparisons of blood pressure and fasting plasma glucose in patients with hypertension, diabetes, and comorbidity: 4-year follow-up data. Risk Manag Healthc Policy. 2022;15:2221–2232. doi:10.2147/RMHP.S385815
4. Lin H, Wu Y, Wu J, Chen Q, Yu J, Lin Y. Prevalence of hypertension and 10-Year cardiovascular disease risk among older adults living in Quanzhou, a coastal region of southeast China. Risk Manag Healthc Policy. 2022;15:1045–1053. doi:10.2147/RMHP.S341148
5. Cohn J, Bygrave H, Roberts T, Khan T, Ojji D, Ordunez P. Addressing failures in achieving hypertension control in low- and middle-income settings through simplified treatment algorithms. Glob Heart. 2022;17(1):28. doi:10.5334/gh.1082
6. Li SS, Li JM, Liu LL, Liu W, Yang H, Feng CG. Analysis of the risk factors related to the success rate of distal transradial artery access in patients with coronary heart disease. Risk Manag Healthc Policy. 2022;15:657–663. doi:10.2147/RMHP.S357780
7. Nie Z, Xu H, Chen C, et al. Population attributable risks of potential modifiable factors for atrial fibrillation in China: a national survey. Risk Manag Healthc Policy. 2022;15:1215–1224. doi:10.2147/RMHP.S360285
8. Afaa TJ, Seneadza H, Ameyaw E, Rodrigues OP. Blood pressure profile, prevalence of hypertension and associated familial factors in school children in Accra, Ghana. Niger J Clin Pract. 2022;25(4):386–390. doi:10.4103/njcp.njcp_1832_21
9. Dong Y, Ma J, Song Y, et al. Secular trends in blood pressure and overweight and obesity in Chinese boys and girls aged 7 to 17 years from 1995 to 2014. Hypertension. 2018;72(2):298–305. doi:10.1161/HYPERTENSIONAHA.118.11291
10. Joint Committee for Guideline Revision. 2018 Chinese guidelines for prevention and treatment of hypertension-A report of the revision committee of Chinese guidelines for prevention and treatment of hypertension. J Geriatr Cardiol. 2019;16(3):182–241. doi:10.11909/j.issn.1671-5411.2019.03.014
11. Fox C. Pediatric hypertension. Prim Care. 2021;48(3):367–378. doi:10.1016/j.pop.2021.04.001
12. Cormick G, Ciapponi A, Cafferata ML, Cormick MS, Belizán JM. Calcium supplementation for prevention of primary hypertension. Cochrane Database Syst Rev. 2022;1(1):CD010037. doi:10.1002/14651858.CD010037.pub4
13. Yang R, Tang J, Zhuo Y, Kuang M, Liu H. Current prescription status of antihypertensive drugs in Chinese patients with hypertension: analysis by type of comorbidities. Clin Exp Hypertens. 2022;44(3):240–248. doi:10.1080/10641963.2021.2022688
14. Li LC, Chen J, Zhu XB, et al. Trends of complications in patients with Parkinson’s disease in seven major cities of China from 2016 to 2019. Int Clin Psychopharmacol. 2021;36(5):274–278. doi:10.1097/YIC.0000000000000370
15. Ying J, Li LC, Wu CY, Yu ZW, Kan LD. The status of proton pump inhibitor use: a prescription survey of 45 hospitals in China. Rev Esp Enferm Dig. 2019;111(10):738–743. doi:10.17235/reed.2019.6155/2019
16. Gong X, He Q, Yan J, et al. A drug utilization study of oral anticoagulants in five representative cities of China between 2015 and 2019. J Clin Pharm Ther. 2022;47(1):38–45. doi:10.1111/jcpt.13538
17. Flynn JT, Kaelber DC, Baker-Smith CM, Subcommittee on Screening and Management of High Blood Pressure in Children. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2017;140(3):e20171904. doi:10.1542/peds.2017-1904
18. Awazu M. Isolated nocturnal hypertension in children. Front Pediatr. 2022;10:823414. doi:10.3389/fped.2022.823414
19. Tran AH, Urbina EM. Hypertension in children. Curr Opin Cardiol. 2020;35(4):376–380. doi:10.1097/HCO.0000000000000744
20. Pérez-Gimeno G, Rupérez AI, Vázquez-Cobela R, et al. Energy dense salty food consumption frequency is associated with diastolic hypertension in Spanish children. Nutrients. 2020;12(4):1027. doi:10.3390/nu12041027
21. Song P, Zhang Y, Yu J, et al. Global prevalence of hypertension in children: a systematic review and meta-analysis. JAMA Pediatr. 2019;173(12):1154–1163. doi:10.1001/jamapediatrics.2019.3310
22. Kharbanda EO, Asche SE, Sinaiko AR, et al. Clinical decision support for recognition and management of hypertension: a randomized trial. Pediatrics. 2018;141(2):e20172954. doi:10.1542/peds.2017-2954
23. Rabi DM, McBrien KA, Sapir-Pichhadze R, et al. Hypertension Canada’s 2020 comprehensive guidelines for the prevention, diagnosis, risk assessment, and treatment of hypertension in adults and children. Can J Cardiol. 2020;36(5):596–624. doi:10.1016/j.cjca.2020.02.086
24. Singh Y, Samuel VP, Dahiya S, et al. Combinational effect of angiotensin receptor blocker and folic acid therapy on uric acid and creatinine level in hyperhomocysteinemia-associated hypertension. Biotechnol Appl Biochem. 2019;66(5):715–719. doi:10.1002/bab.1799
25. Robinson CH, Chanchlani R. High blood pressure in children and adolescents: current perspectives and strategies to improve future kidney and cardiovascular health. Kidney Int Rep. 2022;7(5):954–970. doi:10.1016/j.ekir.2022.02.018
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.