Back to Journals » Drug Design, Development and Therapy » Volume 20
Real-World Pharmacokinetic and Exposure–Response Characterization of Venetoclax in Chinese Patients with Hematological Malignancies
Authors Liu Z, Liu X ![]() , Gong Q, Qin S, Zhu X, Kuan IHS, Mak WY
, Gong Q, Qin S, Zhu X, Kuan IHS, Mak WY ![]() , Xiang X
, Xiang X ![]() , Jia C, Wang Q, Cheng L, Li L
, Jia C, Wang Q, Cheng L, Li L
Received 27 August 2025
Accepted for publication 14 January 2026
Published 29 January 2026 Volume 2026:20 563629
DOI https://doi.org/10.2147/DDDT.S563629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mariana Carmen Chifiriuc
Zhirui Liu,1,* Xin Liu,2,* Qiang Gong,3,* Shiwei Qin,1 Xiao Zhu,2,4 Isabelle Hui-San Kuan,5 Wen Yao Mak,2 Xiaoqiang Xiang,2 Changsheng Jia,1 Qian Wang,1 Lin Cheng,1 Ling Li6,7
1Department of Pharmacy, the First Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China; 2Department of Clinical Pharmacy and Pharmacy Administration, School of Pharmaceutical Science, Fudan University, Shanghai, People’s Republic of China; 3Department of Hematology, the First Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China; 4State Key Laboratory of Advanced Drug Formulations for Overcoming Delivery Barriers, Fudan University, Shanghai, People’s Republic of China; 5Momentum Metrix, San Francisco, CA, USA; 6Institute of Hepatobiliary Diseases of Zhongnan Hospital, Transplant Center of Wuhan University, Wuhan, People’s Republic of China; 7National Quality Control Center for Donated Organ Procurement, Hubei Key Laboratory of Medical Technology on Transplantation, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Li, Zhongnan Hospital of Wuhan University, Institute of Hepatobiliary Diseases of Wuhan University, Wuhan, People’s Republic of China, Email [email protected] Lin Cheng, Department of Pharmacy, the First Affiliated Hospital of Army Medical University, Gaotanyan Street, Shapingba, Chongqing, People’s Republic of China, Email [email protected]
Introduction: Post-marketing evaluation of lower-dose regimens is critical for optimizing individualized oncology therapy. Venetoclax (VNX) is approved for the treatment of hematological malignancies at doses of ≥ 400 mg once daily following a ramp-up schedule. However, favorable clinical responses have been observed in Chinese patients receiving lower doses (≤ 200 mg/day), prompting further investigation.
Methods: A prospective, non-interventional, real-world study was conducted in 76 Chinese patients, yielding 121 plasma samples. Published population pharmacokinetic (PopPK) models, primarily developed in Caucasian populations, were applied for external model-based comparisons of VNX exposure between Chinese patients and previously reported Caucasian populations. A new PopPK model was developed for the Chinese population, followed by exposure-response analysis to assess the relationship between VNX dose and therapeutic efficacy.
Results: External model evaluation demonstrated higher VNX exposure in Chinese patients compared with Caucasian populations. The newly developed Chinese PopPK model estimated apparent clearance at 7.33 L/h, substantially lower than previously reported values in Caucasian patients (15– 19.54 L/h). Exposure–response analysis indicated that VNX at 200 mg/day achieved optimal therapeutic efficacy in combination therapy, with minimal incremental benefit observed at higher doses.
Conclusion: Significant ethnic differences in VNX pharmacokinetics were identified. These findings support the clinical effectiveness of lower-dose (200 mg/day) VNX-based regimens in Chinese patients and highlight the importance of population-specific dose optimization.
Keywords: venetoclax, hematological malignancy, exposure-response, therapeutic drug monitoring
Introduction
Optimizing drug dosing is now a central goal in oncology practice and regulatory approval.1,2 This approach seeks to balance efficacy, safety, and cost to improve accessibility, particularly in settings with limited resources.3,4 Although many new oncology medicines have demonstrated significant efficacy in randomized controlled trials (RCT), their widespread clinical application is often restricted due to high cost5 and suboptimal real-world effectiveness.6 Dose regimens tested in RCT often represent maximal tolerated or recommended doses. These doses may not be optimized for clinical efficiency or patient affordability, thus leading to discrepancies between trial outcomes and real-world clinical observations. Increasing evidence from drugs such as lenalidomide,7 ibrutinib,8 and bortezomib9 suggests that lower-dose schedules might maintain comparable clinical efficacy while reducing toxicity and economic burden. These findings underscore the critical role of real-world studies in guiding dose adjustments and informing clinical decision-making.
Venetoclax (VNX) is a first-in-class orally selective inhibitor of the B-cell leukemia/lymphoma-2 (BCL-2) protein, revolutionizing the therapeutic landscape for hematological malignancies such as chronic lymphocytic leukemia (CLL),10,11 small lymphocytic lymphoma (SLL),12 acute myeloid leukemia (AML),13 multiple myeloma (MM).14 Through its targeted mechanism of action, VNX has significantly improved remission rates and survival outcomes, particularly when used in combination with hypomethylating agents (HMAs) or low-dose cytarabine (LDAC).15,16 Based on pivotal clinical trials, a fixed daily dose of 400 mg and 600 mg QD is currently recommended in clinical guidelines.17
Although RCT have demonstrated a clear exposure-response (E-R) relationship for VNX,14,18–20 most were conducted predominantly in non-Asian populations. Therefore, the applicability of these findings to Asian patients, particularly Chinese individuals, remains uncertain. Real-world clinical observations further highlight significant discrepancies from RCT outcomes, manifesting as notably lower median overall survival and slightly reduced remission rate.21 These differences may be attributed to several factors, including less stringent protocol adherence, variations in treatment regimens, and patient heterogeneity, and notably, pharmacokinetic (PK) variability.22,23 Significant interindividual PK differences, especially influenced by dietary factors given VNX’s classification as a Biopharmaceutics Classification System Class IV compound,24–27 hepatic function,28,29 and interactions with CYP3A inhibitors,30 pose substantial challenges for dose standardization in clinical practice. Considering these factors, there is a pressing need for region-specific PK data in Chinese patients to better guide individualized dosing strategies. Therefore, investigating the efficacy and feasibility of lower-dose regimens in China could address these PK variations, mitigate the financial burden, and improve patient access to effective treatments.
The primary objective of this study is to investigate whether lower-dose VNX regimens can achieve near-equivalent clinical outcomes, providing preliminary evidence to support potential dosage optimization. Such optimization could help improve the accessibility and affordability of effective treatments for hematological malignancies in China. Specifically, we aim to (1) conduct prospective, observational real-world cohort study to obtain the PK and efficacy data, (2) characterize the real-world plasma PK profiles of VNX through the development of a Chinese-specific PopPK model, and (3) investigate the E-R relationship.
Methods
Patients and Study Design
This study was a prospective, non-interventional clinical study conducted at Southwest Hospital, Chongqing, from July 2021 to March 2024. The study was approved by the local Institutional Review Board Statement (IRB) (Ethics No. KY202218). Written informed consent was obtained from patients or their legal representatives. All procedures were conducted in accordance with the Declaration of Helsinki. Patients hospitalized and receiving VNX therapy were included according to the following criteria: (a) were diagnosed with AML, or other hematological malignancy receiving VNX; (b) were aged ≥18 years, (c) had blood count, liver function, and renal function results measured within 3 days at the time of VNX concentration measurement, (d) signed informed consent forms. The exclusion criteria were patients who (a) coadministration of moderate and strong CYP3A inhibitors, (b) coadministration of rituximab, (c) with severe hepatic impairment, and (d) currently pregnant.
The following data were collected from the medical records: (a) Subject demographics and clinical characteristics, including age, sex, weight, and underlying diseases; (b) medication data, including VNX dose, the number of days of VNX treatment at the measurement of concentration, and combined use of chemotherapy drugs; (c) clinical outcome and the corresponding number of days of the outcome obtained after VNX administration; and (d) laboratory results detected within 3 days of VNX concentration determination: liver functions, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), glutamyl transferase (GGT), alkaline phosphatase (ALP), total bilirubin (TBIL), and albumin; renal functions, including blood urea nitrogen (BUN), creatinine, and estimated glomerular filtration rate (eGFR); blood count, including white blood cells (WBC), red blood cells (RBC), hemoglobin (Hb), platelet counts (PLT), hematocrit (HCT), mean corpuscular volume, mean hemoglobin content, neutrophils, lymphocyte number, and lymphocyte percentage; and the percentage of primitive cells in peripheral blood.
Efficacy outcomes were assessed by a bone marrow biopsy performed after completion of one treatment cycle (28 days), typically between Day 28 and Day 45 after the initiation of VNX. This schedule reflects routine clinical practice. The treating physician evaluated treatment effectiveness in accordance with the following criteria.31,32 CR (complete remission): 1) Bone marrow: Three lines of normal hyperplasia without pathological hematopoiesis. Minor megaloblastosis may occur, but pseudo Pelger-Huet, ring sideroblasts, and megakaryocyte pathological hematopoiesis should not occur. The classified primitive cells in the bone marrow do not exceed 5%. If the proportion of erythroid cells is less than 0.5, the proportion of original cells is calculated as all nucleated cells; if the proportion of erythroid cells exceeds 0.5, the proportion of original cells is calculated as non-erythroid cells. 2) Peripheral blood: Hb ≥ 110 g/L, without blood transfusions and without the use of erythropoietin. 3) Neutrophil absolute value ≥ 1.5×109/L, without the use of myeloid colony stimulating factor. 4) PLT ≥ 100×109/L, without the use of thrombopoietin. 5) Absence of primitive cells. 6) Absence of pathological hematopoiesis. PR (partial remission): Apart from a decrease of at least 50% in the proportion of bone marrow original cells compared to pre-treatment or a decrease of at least 1 grade in the FAB classification (regardless of cell morphological changes), the other indicators met the criteria for CR. NR/Relapse: Failure to achieve PR, but the disease did not progress further and persisted for at least 2 months. The proportion of bone marrow original cells increased to the pre-treatment level; neutrophils or PLT decreased by more than 50% from their highest post-treatment levels; Hb was reduced by at least 20 g/L or there was transfusion dependence.
Analytical Methods
All the samples were detected by liquid chromatography-tandem mass spectrometry (LC-MS/MS) method. Venous blood was drawn before the next dose of VNX administration. Plasma VNX was determined using an in-house developed and validated LC-MS/MS.33 Briefly, 20 μL plasma was spiked with 980 μL methanol to precipitate the proteins. Following 2-min vertexing and a 5-min centrifugation at 15,000 rpm, 2 μL of the supernatant was injected into AB SCIEX6500 QTRAP mass system for analysis. The ion transition for VNX was 868.4 > 636.4. The lower limit of quantitation was 20 ng/mL. The intra-day and inter-day precision values for the quality control samples were ≤8.05% and ≤9.49%, respectively.
Assessment of Ethnic Difference in Drug Exposure
To assess the exposure difference between the Asian and non-Asian population, an external evaluation of PopPK models was used. Briefly, the PopPK model search and screen was according to the previously published systematic review34 and the strategy in Supplemental 1. Model predictive performance was assessed according to standard procedures using maximum a posteriori Bayesian estimation. Utilizing the recorded dosing regimens, sampling times, and relevant covariates from the validation dataset, individual and population-predicted VNX concentrations were calculated at corresponding sampling points. In cases where the covariates specified in the PopPK model were not available in the evaluation dataset, the mean or median values of the covariates described in the original publication were utilized. In addition, VNX was administered according to label recommendations with meals in this study, hence bioavailability was fixed under fed conditions.
The predictive accuracy of each published model was evaluated through graphical assessments and statistical metrics. The predictive performance of the model was assessed using both visual and quantitative methods. Visual predictive performance was assessed using goodness-of-fit (GOF) plots, comparing the observed concentrations (Cobs) against both the population-predicted (CPRED) and individual predicted concentrations (CIPRED). Quantitative predictive performance was analyzed by calculating the prediction error (PE%) for each individual (Equation 1), the mean prediction error (MPE%, Equation 2), and the relative root mean squared error (RMSE%, Equation 3). Additionally, normalized prediction distribution error (NPDE) was conducted to assess the model predictive performance. NPDE was computed for the validation set based on 1000 simulations from the final model using the NPDE package (version 2.2). In order to compare the distribution of NPDE values with the reference distribution, graphical methods and appropriate statistical tests were employed. Three statistical tests were utilized, namely the Wilcoxon signed-rank test (H0: mean = 0), the Fisher variance test (H0: variance = 1), and the Shapiro–Wilks test (H0: normal distribution). When previously published models contained substantial prediction biases or poor predictive performance, a new PopPK model would be developed using the observed data from the Chinese patients.

Pharmacokinetic Characterization of Venetoclax in Chinese Patients
To further figure out the PK characteristic of VNX in the Chinese patients, a PopPK model based on the Chinese patient’s data was developed. Non-linear mixed-effects modeling was conducted using NONMEM (version 7.5, ICON Development Solutions, MD, USA) with the first-order conditional estimation with interaction (FOCE-I) algorithm. Based on a review of existing literature, we evaluated the structural models in terms of one-, two-compartment, first-order absorption and linear elimination. IIV was modeled using an exponential approach, while residual variability was tested using proportional, additive, and combined error models, and select the best performance one. Covariate analysis included demographic data (eg, age, weight, sex), lab test results (eg, blood routine test results, liver function test, renal function test listed in Table 1). A stepwise covariate modeling strategy was used (forward selection: p < 0.05; backward elimination: p < 0.01). Covariates were selected based on statistical significance and clinical relevance. Model evaluation was performed using successful convergence, objective function value (OFV), akaike information criterion (AIC), parameter precision, GOF plots, NPDE, and non-parametric bootstrap analysis to confirm model robustness.
Exposure–Efficacy Relationship Evaluation
To evaluate the exposure–efficacy relationship while accounting for approved clinical indications, exposure-response analysis was primarily conducted in patients with AML. The dual primary efficacy endpoints were categorized as NR/Relapse and PR/CR. Exposure indices evaluated included minimum steady-state concentration (Cmin) and average steady-state concentration (Cave) were evaluated. Since the majority of the sampling data were trough concentrations, a post-Bayesian method was applied to generate the PK parameters using the PopPK model derived above. The relationship between VNX exposure and clinical outcomes was explored using Logistic regression analysis, with exposure metrics (Cmin and Cave) as independent predictors. The AIC and p-value were used as statistical indices, with a p-value < 0.05 considered significant. In addition, a sensitivity analysis including the full study population was performed to assess the robustness of the exposure–response relationship.
Results
Patient Baseline Characteristics
A total of 121 VNX concentration samples from 76 Chinese patients diagnosed with hematologic malignancies were included in this analysis. Among these patients, 46 were males and 30 were females, with age range from 36 to 63 years. The distribution of disease diagnoses was as follows: AML in 63 cases, ALL in 3 cases, APL in 1 case, CMML in 1 case, MDS in 7 cases, and MPAL in 1 case. In addition, all patients received combination chemotherapy involving one or two co-administered agents, including azacitidine, aclarubicin, cytarabine, vincristine, daunorubicin, homoharringtonine, and cladribine (Table S1). Laboratory results indicated that most patients had albumin levels below normal ranges, with substantial deviations in blood count indices compared to healthy populations range (Figures S1 and S2). Detailed demographic and clinical characteristics of the study population are summarized in Table 1.
Differences in Drug Exposure by Ethnicity
Six previously published PopPK models (designated M1–M6)35–40 were included for external evaluation. The key model information for each was summarized in Table S2. All of these models using a classic two-compartment PK model structure to describe the disposition of VNX and typical estimates for the clearance rate (CL) of VNX ranged from 15 to 19.54 L/h without considering the covariates effects on the CL. CYP3A4 inhibitors and rituximab were found to significantly affect the clearance. Sex influenced the distribution volume of the central compartment, and food intake impacted bioavailability. Notably, the Asian populations exhibited approximately 30% lower clearance compared to other regions.40 However, each study included some Asian patients, ranging from 0.4% to 9.3%, and none of these models were exclusively developed using Chinese populations.
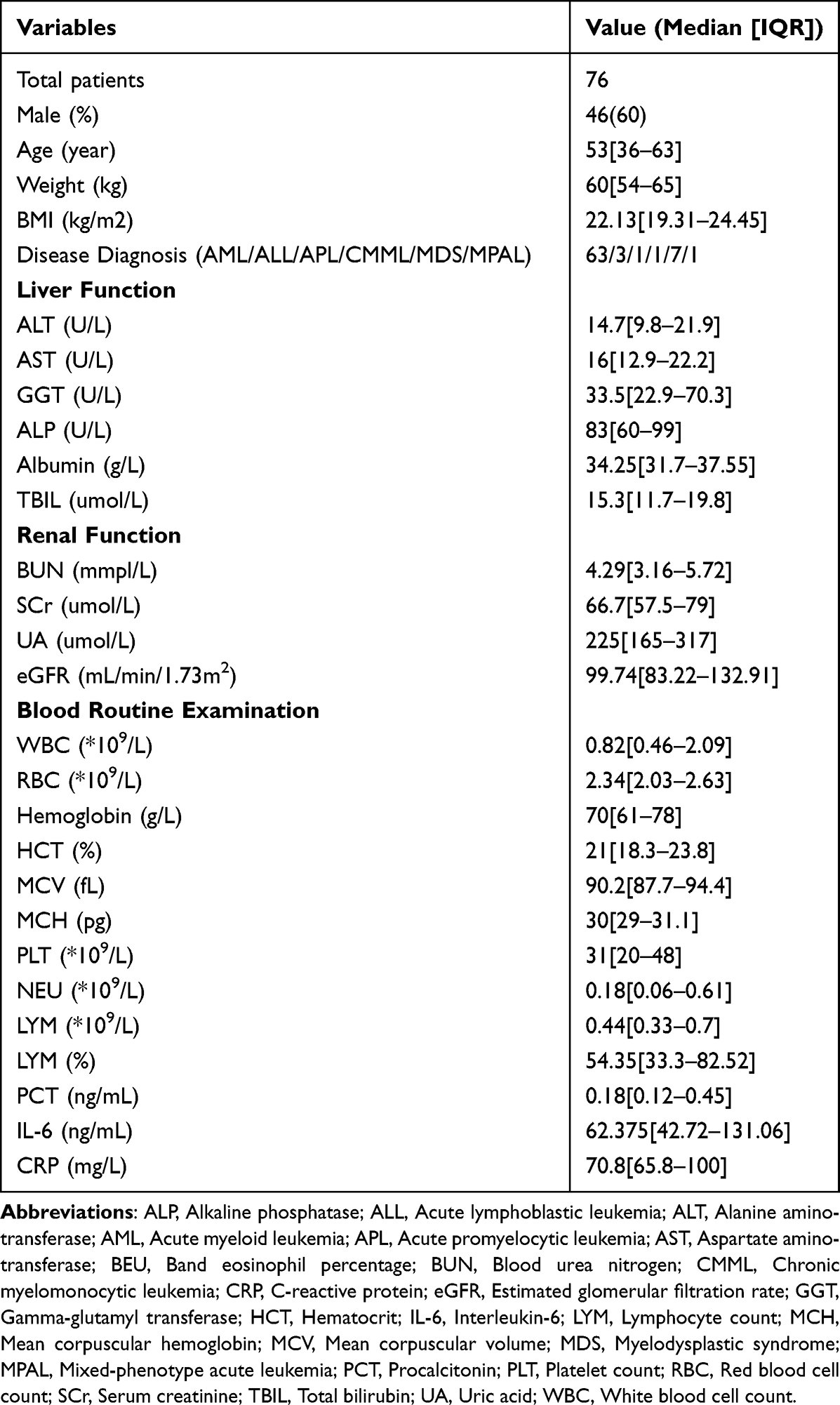 |
Table 1 The Demographic Characteristics of Included Patients |
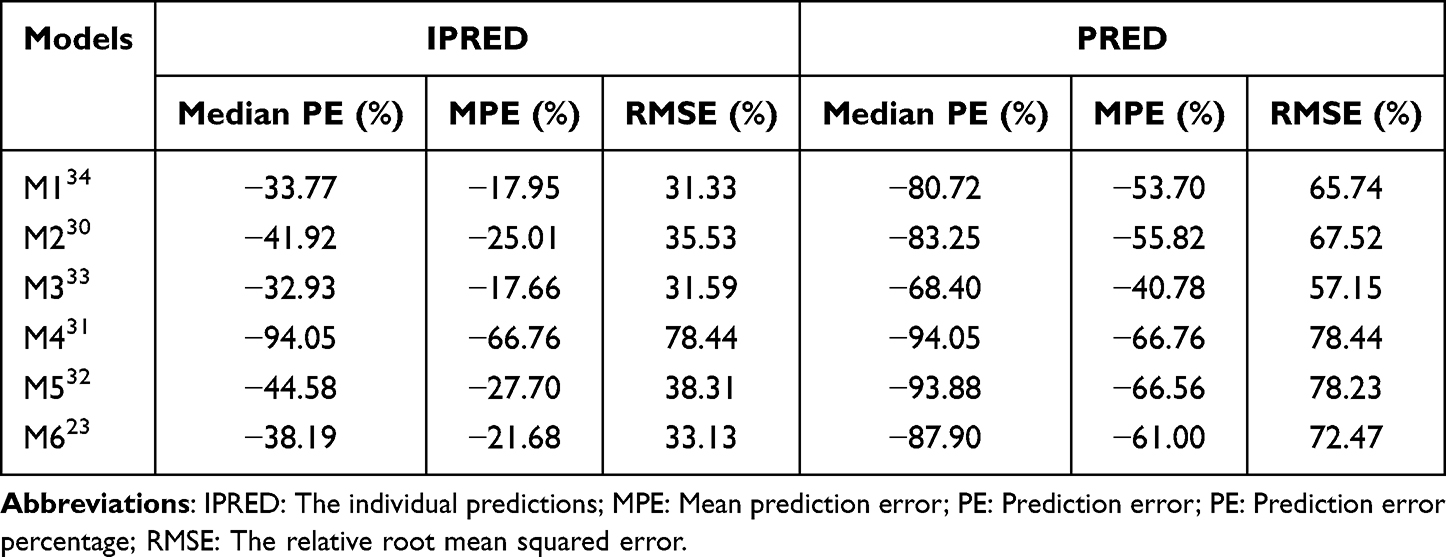 |
Table 2 Prediction Error (PE) of the Individual Predictions (IPRED) and Population Predictions (PRED) to Observations for the Evaluated Models |
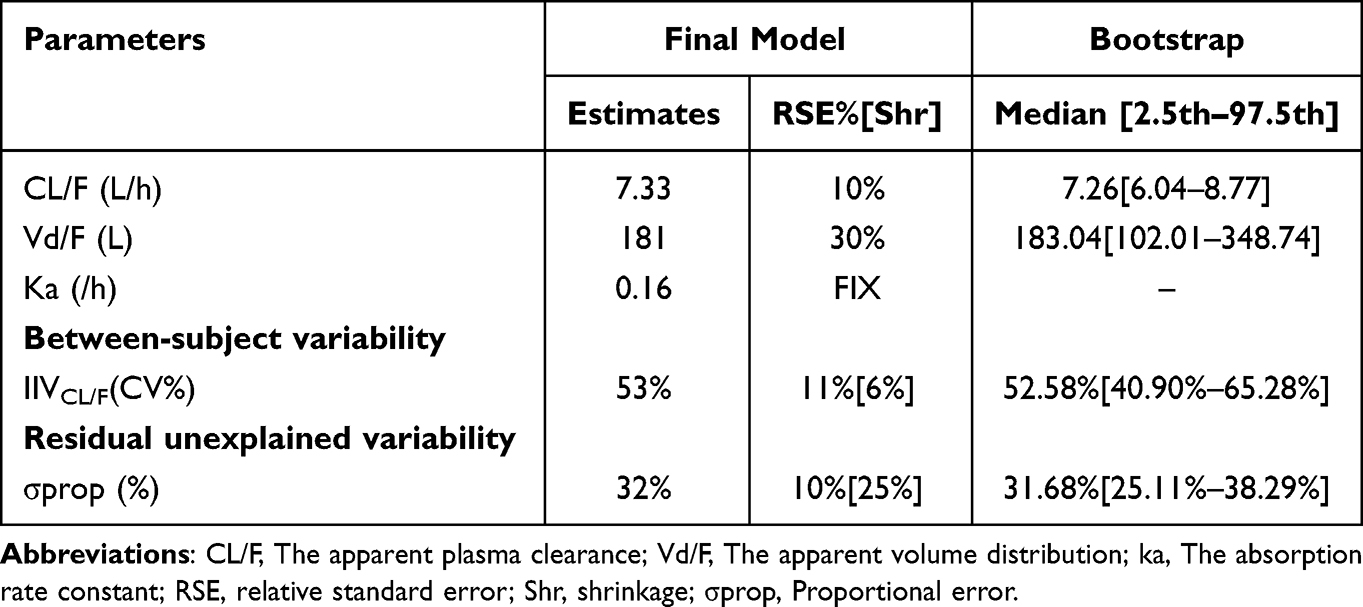 |
Table 3 Final Population Pharmacokinetic Model Parameters and Bootstrap Results |
The GOF plots revealed systematic underprediction of concentrations across all models (Figure S3). Quantitative analyses showed significant prediction biases, with all the individual and population predicted errors and RMSE far beyond the ± 30% range (Figure S4 and Table 2). Of these, the M4 which included the smallest proportion (0.4%) of Asian subjects38 showed the lowest accuracy and precision. Simulation-based diagnostics (Figure S5) further confirmed poor model performance, revealing non-normal NPDE distributions, notable biases in NPDE related to temporal trends and predicted concentrations, and global statistical tests indicating significant model inadequacy (all corrected p-values <0.001).
VNX PK Characteristics in Chinese Patients
To further investigate the PK characteristic of VNX in the Chinese patients, a PopPK model was developed. A one-compartment model with first-order absorption and elimination was selected as the final model. Due to all of the sampling data were trough concentration, ka value was fixed as 0.16/h according to previous publications.36,39 The final model provided precise parameter estimates with the most relative standard errors well below 30% (Table 3), with an apparent clearance (CL/F) of 7.33 L/h, an apparent volume of distribution (Vd/F) of 181 L.
The bootstrap analysis showed the parameter estimates from the final model closely matching the median values and falling within the 95% confidence interval (Table 3). This alignment confirms the robustness of the model. GOF diagnostic plots (Figure 1) demonstrated unbiased model predictions and successful convergence. Additionally, the quantile-quantile plots and NPDE histograms (Figure 2) indicated a satisfactory model fit with no significant bias or distribution issues. The global statistical tests yielded corrected p-values > 0.05, further affirming the predictive performance of the final PopPK model. For covariates screening, there was no statistically covariates included in the final model after the stepwise screening. The effects of covariates on AUC and Cmin were evaluated using forest plots, which demonstrated no significant differences among the various covariate subgroups (Figure 3 and Figure S6).
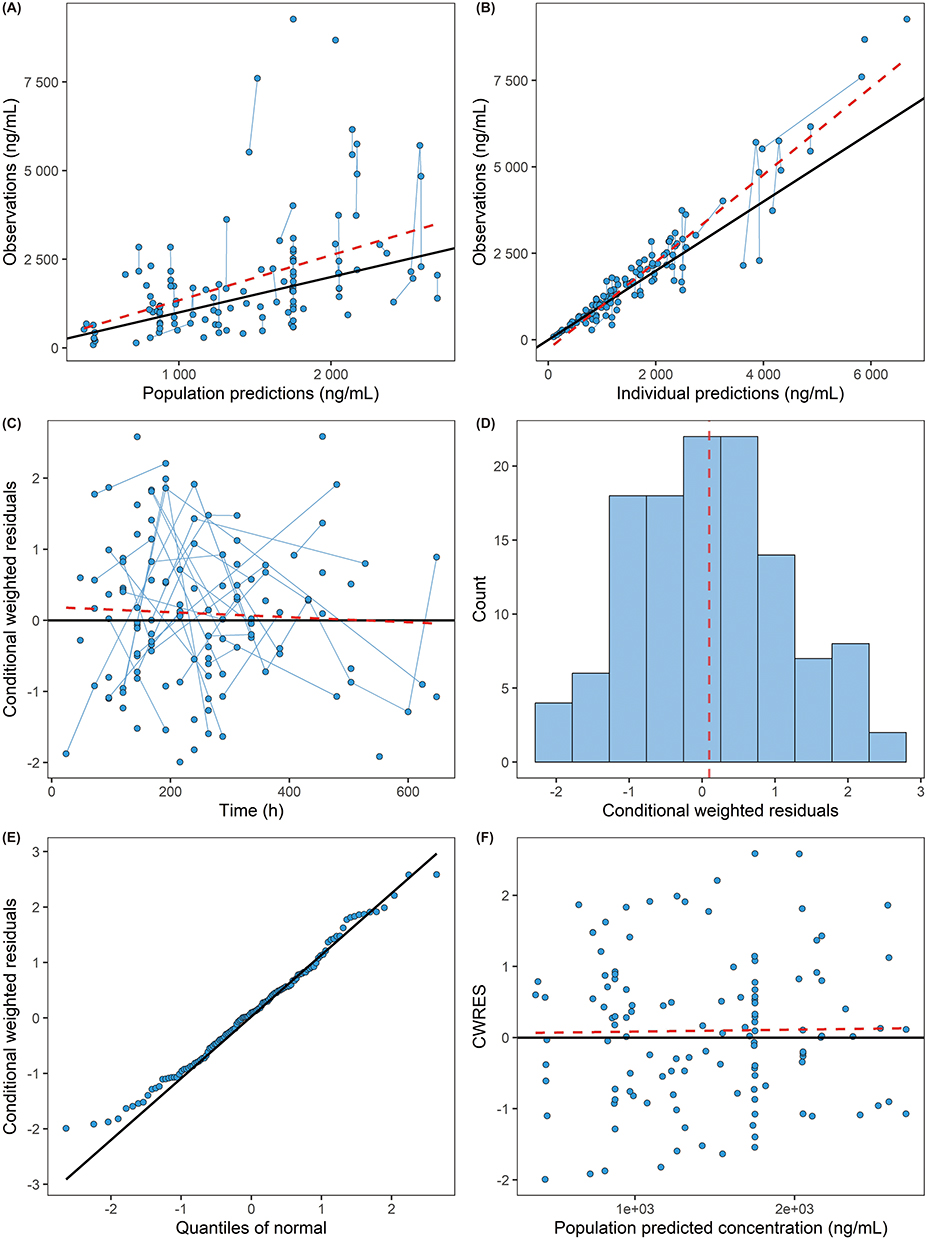 |
Figure 1 Goodness-of-fit plots of the final model. (A) Observations (OBS) versus population predictions (PRED) (B) OBS versus individual predictions (IPRED). (C) Conditional weighted residuals (CWRES) versus time after first dose. (D) Conditional weighted residuals verse count. (E) Quantile-quantile plot. (F) CWRES versus PRED. The line in (A) and (B) represents the line of identity. The solid black line is the line of identity (measured = predicted); the dashed lines are smoothing lines through the data. |
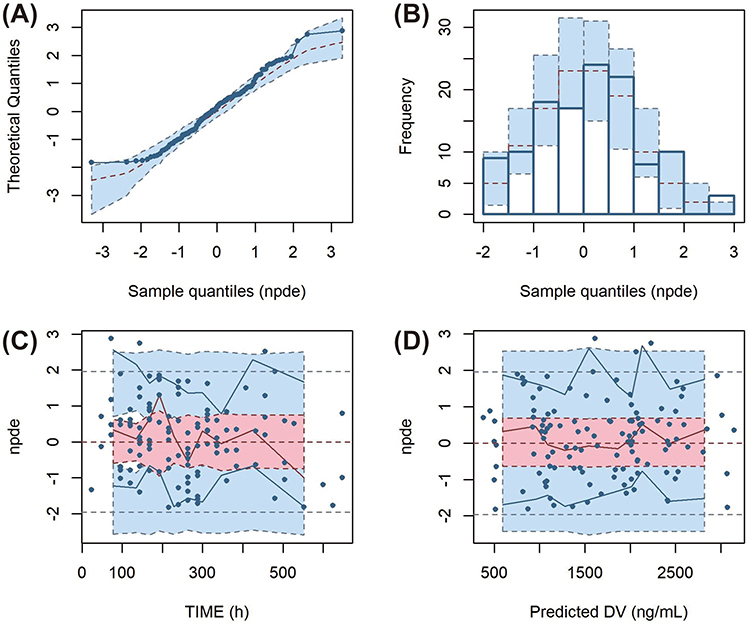 |
Figure 2 Normalized prediction distribution error (NPDE) plots of the models. (A) Quantile–quantile plot of the distribution of the NPDE against theoretical distribution (semitransparent blue fields); (B) Histogram of the distribution of the NPDE against theoretical distribution (semitransparent blue fields); (C) NPDE vs time after dose (h); (D) NPDE vs predicted concentrations. In plots C and D, the solid black lines represent the actual value of the NPDE at the 5th and 95th percentiles, the red solid line represents the 50th percentiles. The semitransparent red field represents a simulation-based 95% confidence interval for the median at 50th percentile, and semitransparent blue fields represent a simulation-based 95% confidence interval for the corresponding model‐predicted 5th and 95th percentiles. The NPDE of the observations are represented by dark blue dots. |
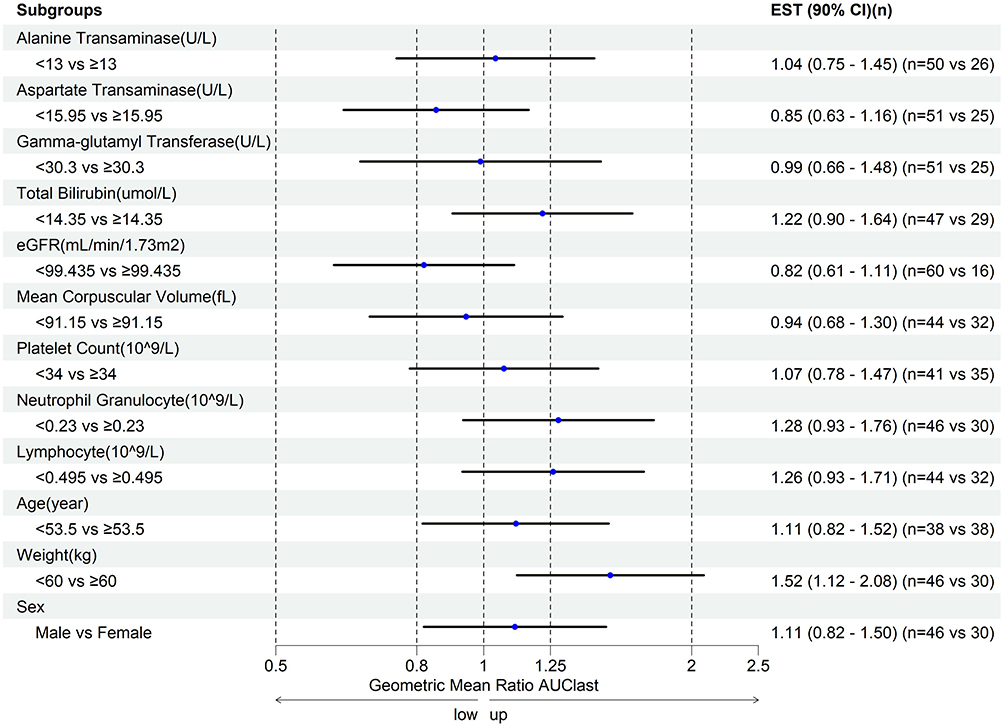 |
Figure 3 The covariates effects on the VNX AUClast. Abbreviations: ALT, Alanine aminotransferase; AST, Aspartate aminotransferase; eGFR, Estimated glomerular filtration rate; GGT, Gamma-glutamyl transferase; LYM, Lymphocyte count; MCV, Mean corpuscular volume; PLT, Platelet count; TBIL, Total bilirubin. |
Exposure–Response Relationship
For oral doses ranging from 100 to 400 mg/day, a positive exposure–response relationship was observed for ORR. Among patients with AML, VNX exposure quantified by Cave was significantly higher in responders (n = 37) compared with non-responders (n = 26). Logistic regression analysis confirmed a statistically significant association between Cave and ORR (p < 0.05). The analysis suggested that doses above 200 mg/day might be required for effective AML treatment in Chinese patients (Figure 4 and Figure S7). Therefore, the correlation between Cave and ORR indicated that therapeutic drug monitoring could potentially optimize drug use. In addition, the full dataset and the AML-only subset exhibited consistent exposure-response trends, supporting the robustness of the primary analysis (Figures S8 and S9). These findings highlight Cave as a potential valuable indicator for response prediction.
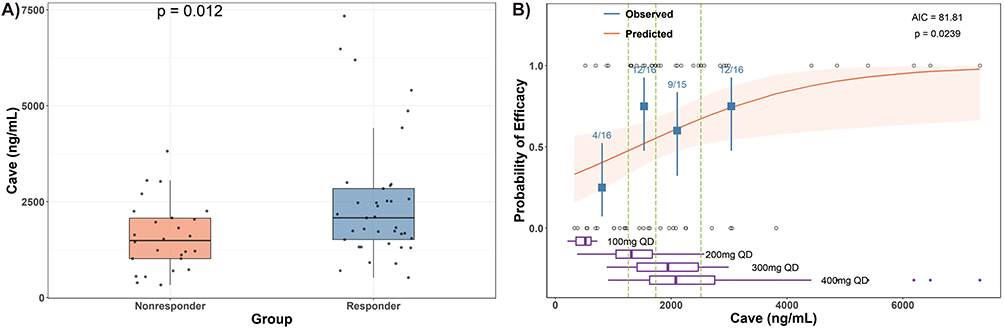 |
Figure 4 The Cave comparison between different group (A) and exposure–response relationship of the overall response in the AML patients who received the VNX versus the predicted Cave (B). Notes: (A) Black dots are the individual exposure metrics predicted based on actual dosing and individual PopPK model parameter estimates. Cave, the average concentration during the steady state. (B): error bars are 95% CI of ORR in the respective exposure quartile groups. Shaded areas of the logistic regression plots represent 95% CI of the predicted ORR. Short vertical lines at the lower and upper part of the plotting area represent the exposure metrics in nonresponders and responders, respectively. The boxplots represent the concentration range in each dosage group. |
Discussion
This study provides important real-world evidence demonstrating the clinical near-equivalence of lower-dose (200 mg) VNX-based therapy compared to the standard recommended dose (400 mg) in Chinese patients with hematological malignancies. We observed a significant difference in VNX exposure between Chinese and non-Asian populations. Moreover, our findings reveal similar clinical efficacy across these doses, strongly supporting the feasibility of adopting lower-dose VNX treatment strategies for Chinese patients. This study thus offers an example of dose optimization, highlighting the potential to enhance drug accessibility and inform individualized dosing strategies tailored specifically to the unique pharmacokinetic and clinical profiles of Chinese patients.
External evaluation of published PopPK models revealed systematic underprediction of VNX exposure in our Chinese cohort. This finding suggests that ethnic and environmental factors,34 such as differences in dietary patterns, baseline physiological parameters, and genetic backgrounds, may significantly influence VNX pharmacokinetics. Previous studies have reported approximately 67% higher VNX bioavailability in Asian patients compared to non-Asians,10 aligning with the observed elevation in drug exposure in Chinese patients at lower doses. Real-world factors such as variable dietary intake and less standardized medication timing likely further increase interindividual PK variability, highlighting the limitations of applying dosing protocols from RCTs directly to routine practice. In particular, food intake with different fats content (low-, moderate-, and high-fat) has been shown to increase VNX bioavailability to different degrees (2.99-, 3.77-, and 4.25-fold) compared to fasting condition.36 Additionally, dose-dependent bioavailability of VNX has been reported,38,39 with doses ≤400 mg, as utilized in our study, potentially associated with higher relative bioavailability than higher doses employed in earlier clinical trials.
Given these observations, the development of a Chinese-specific PopPK model was warranted. Our model estimated a markedly lower apparent clearance (CL/F) of 7.33 L/h compared to 15–19.54 L/h reported in previous studies, reinforcing the need for population-specific dosing regimens. Notably, no significant covariates were identified in our model, which may be attributed to the relatively homogeneous patient population, where all patients were ethnically Chinese and received VNX postprandially without CYP3A or OATP1B3 modulators. This uniformity likely minimized the influence of external variability on drug disposition.
Therapeutic drug monitoring (TDM) and pharmacokinetically guided dosing strategies have been proposed to minimize the variability and improve the efficacy.41 Beyond model validation, TDM results further revealed significant difference between real-world and RCT-derived exposure profiles. Our observed average VNX Cmin of 1470.18 ± 855.63 ng/mL in 200 mg group aligns closely with previously reported 400 mg group, such as the real-world data from Chinese (1018 ± 729 ng/mL, or 1030 ± 400 ng/mL),25,42 Japanese (1020 ng/mL),43 and French populations (1010 ± 470 ng/mL),22 yet significantly exceeds concentrations reported from registered clinical trials (490–840 ng/mL).22 This exposure was approximated to the optimal therapeutic target concentration (1200 ng/mL),44 suggesting that a 200 mg dose could be the minor effective dosage suitable for Chinese patients. Approximately 40% of our patients receiving lower daily doses (100–200 mg) achieved relatively high trough concentrations, further supporting the feasibility of dose individualization based on real-world TDM data rather than relying solely on RCT-derived standards.
Consistent with earlier findings,20,45 a clear exposure–response relationship was also observed in this study. Specifically, the ORR significantly improved from 42% at 100 mg to 68% at 200 mg (Figure 4); however, only a limited improvement was observed from 200 mg to 400 mg. This observation aligns closely with findings reported by Badawi et al46 which indicating that when the average VNX plasma concentration exceeded 1777 ng/mL, the remission rate no longer significantly increased, suggesting minimal clinical benefit from higher doses based on their data. Collectively, these findings reinforce the hypothesis that the optimal therapeutic exposure range may be between 1000 and 2000 ng/mL, highlighting both the clinical and economic advantages of TDM for individualized dosing in Chinese patients with hematological malignancies.
There were several limitations existed in the current study should be acknowledged. First, this was a single-center study with a relatively small sample size, potentially limiting generalizability. Second, the sampling was solely from the trough concentration, which did not sufficiently reflect the absorption and distribution characteristics of VNX. Future multi-center, prospective studies with larger patient cohorts and well-designed sampling schedule are necessary to confirm and extend these findings. Notwithstanding, this study provides the findings for VNX in real-world Chinese patients and provides guidance for making a better therapeutic decision on VNX dosing regimen to maximize the treatment outcomes for Chinese patients.
Conclusion
This study identified significant pharmacokinetic differences in Venetoclax exposure between Chinese and non-Asian populations. Importantly, it provides real-world evidence that lower-dose Venetoclax-based regimens (200 mg) can achieve favorable clinical outcomes in Chinese patients with hematological malignancies, thus potentially enhancing treatment accessibility and affordability.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Ling Li) upon reasonable request.
Ethics Approval
The protocol of this study was approved by the Ethics Committee of the First Affiliated Hospital of the Army Medical University (No. KY202218). All procedures were conducted in accordance with the Declaration of Helsinki.
Informed Consent
Informed consent was obtained from each patient included.
Acknowledgments
The authors want to thank all the participants in this study and thank Certara for providing free access of Pirana.
Funding
This work was supported by the General Program of Chongqing Health Care Commission (grant no. 2024MSXM028); Health Joint Medical Research of Shapingba District, Chongqing, China (2025SQKWLHMS023); and the Chongqing Clinical Pharmacy Key Specialties Construction Project, China. General Project of Science.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Fourie Zirkelbach J, Shah M, Vallejo J. et al. Improving Dose-Optimization Processes Used in Oncology Drug Development to Minimize Toxicity and Maximize Benefit to Patients. J Clin Oncol. 2022;40(30):3489–13. doi:10.1200/JCO.22.00371
2. Singh H, Vellanki PJ, Pazdur R. The Retrofit: lessons From Sotorasib’s Dosing Conundrum. JCO. 2025;43(3):248–250. doi:10.1200/JCO.24.00310
3. Tannock IF, de Vries EGE, Fojo A, Buyse M, Moja L. Dose optimisation to improve access to effective cancer medicines. Lancet Oncol. 2025;26(3):e171–e180. doi:10.1016/S1470-2045(24)00648-X
4. Tannock IF, Ratain MJ, Goldstein DA, et al. Near-Equivalence: generating Evidence to Support Alternative Cost-Effective Treatments. J Clin Oncol. 2021;39(9):950–955. doi:10.1200/JCO.20.02768
5. Prasad V, De Jesús K, Mailankody S. The high price of anticancer drugs: origins, implications, barriers, solutions. Nat Rev Clin Oncol. 2017;14(6):381–390. doi:10.1038/nrclinonc.2017.31
6. Di Maio M, Perrone F, Conte P. Real-World Evidence in Oncology: opportunities and Limitations. Oncologist. 2020;25(5):e746–e752. doi:10.1634/theoncologist.2019-0647
7. Quach H, Fernyhough L, Henderson R, et al. Upfront lower dose lenalidomide is less toxic and does not compromise efficacy for vulnerable patients with relapsed refractory multiple myeloma: final analysis of the Phase II RevLite study. Br J Haematol. 2017;177(3):441–448. doi:10.1111/bjh.14562
8. Mj R, Jj M, As L. Ibrutinib’s Cardiotoxicity-An Opportunity for Postmarketing Regulation. JAMA Oncol. 2021;7:1.
9. Bringhen S, Larocca A, Rossi D, et al. Efficacy and safety of once-weekly bortezomib in multiple myeloma patients. Blood. 2010;116(23):4745–4753. doi:10.1182/blood-2010-07-294983
10. Roeker LE, Fox CP, Eyre TA, et al. Tumor Lysis, Adverse Events, and Dose Adjustments in 297 Venetoclax-Treated CLL Patients in Routine Clinical Practice. Clin Cancer Res. 2019;25(14):4264–4270. doi:10.1158/1078-0432.CCR-19-0361
11. Davids MS, Hallek M, Wierda W, et al. Comprehensive Safety Analysis of Venetoclax Monotherapy for Patients with Relapsed/Refractory Chronic Lymphocytic Leukemia. Clin Cancer Res. 2018;24(18):4371–4379. doi:10.1158/1078-0432.CCR-17-3761
12. Roberts AW, Davids MS, Pagel JM, et al. Targeting BCL2 with Venetoclax in Relapsed Chronic Lymphocytic Leukemia. N Engl J Med. 2016;374(4):311–322. doi:10.1056/NEJMoa1513257
13. Pollyea DA, Pratz K, Letai A, et al. Venetoclax with azacitidine or decitabine in patients with newly diagnosed acute myeloid leukemia: long term follow-up from a Phase 1b study. Am J Hematol. 2021;96(2):208–217. doi:10.1002/ajh.26039
14. Freise KJ, Jones AK, Verdugo ME, et al. Moving Beyond Maximum Tolerated Dose for Targeted Oncology Drugs: use of Clinical Utility Index to Optimize Venetoclax Dosage in Multiple Myeloma Patients. Clin Pharmacol Ther. 2017;102(6):970–976. doi:10.1002/cpt.712
15. DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia. N Engl J Med. 2020;383(7):617–629. doi:10.1056/NEJMoa2012971
16. Wei AH, Montesinos P, Ivanov V, et al. Venetoclax plus LDAC for newly diagnosed AML ineligible for intensive chemotherapy: a Phase 3 randomized placebo-controlled trial. Blood. 2020;135(24):2137–2145. doi:10.1182/blood.2020004856
17. Brackman D, Eckert D, Menon R, et al. Venetoclax exposure-efficacy and exposure-safety relationships in patients with treatment-naïve acute myeloid leukemia who are ineligible for intensive chemotherapy. Hematol Oncol. 2022;40(2):269–279. doi:10.1002/hon.2964
18. Parikh A, Gopalakrishnan S, Freise KJ, et al. Exposure-response evaluations of venetoclax efficacy and safety in patients with non-Hodgkin lymphoma. Leuk Lymphoma. 2018;59(4):871–879. doi:10.1080/10428194.2017.1361024
19. Freise KJ, Jones AK, Menon RM, et al. Relationship between venetoclax exposure, rituximab coadministration, and progression-free survival in patients with relapsed or refractory chronic lymphocytic leukemia: demonstration of synergy. Hematol Oncol. 2017;35(4):679–684. doi:10.1002/hon.2373
20. Freise KJ, Jones AK, Eckert D, et al. Impact of Venetoclax Exposure on Clinical Efficacy and Safety in Patients with Relapsed or Refractory Chronic Lymphocytic Leukemia. Clin Pharmacokinet. 2017;56(5):515–523. doi:10.1007/s40262-016-0453-9
21. Solana-Altabella A, Rodríguez-Veiga R, Martínez-Cuadrón D, Montesinos P. A systematic review of venetoclax for the treatment of unfit AML patients in real-world: is all that glitters gold? Ann Hematol. 2024;104(2):913–935. doi:10.1007/s00277-024-05891-w
22. Philippe M, Guitton J, Goutelle S, et al. Pharmacokinetic Consideration of Venetoclax in Acute Myeloid Leukemia Patients: a Potential Candidate for TDM? A Short Communication. Ther Drug Monit. 2024;46(1):127–131. doi:10.1097/FTD.0000000000001151
23. Groenland SL, Mathijssen RHJ, Beijnen JH, Huitema ADR, Steeghs N. Individualized dosing of oral targeted therapies in oncology is crucial in the era of precision medicine. Eur J Clin Pharmacol. 2019;75(9):1309–1318. doi:10.1007/s00228-019-02704-2
24. Freise KJ, Shebley M, Salem AH. Quantitative Prediction of the Effect of CYP3A Inhibitors and Inducers on Venetoclax Pharmacokinetics Using a Physiologically Based Pharmacokinetic Model. J Clin Pharmacol. 2017;57(6):796–804. doi:10.1002/jcph.858
25. Yang X, Mei C, He X, et al. Quantification of Venetoclax for Therapeutic Drug Monitoring in Chinese Acute Myeloid Leukemia Patients by a Validated UPLC-MS/MS Method. Molecules. 2022;27(5):1607. doi:10.3390/molecules27051607
26. Kaufman JL, Gasparetto C, Schjesvold FH, et al. Targeting BCL-2 with venetoclax and dexamethasone in patients with relapsed/refractory t(11;14) multiple myeloma. Am J Hematol. 2021;96(4):418–427. doi:10.1002/ajh.26083
27. Emami Riedmaier A, Lindley DJ, Hall JA, et al. Mechanistic Physiologically Based Pharmacokinetic Modeling of the Dissolution and Food Effect of a Biopharmaceutics Classification System IV Compound-The Venetoclax Story. J Pharm Sci. 2018;107(1):495–502. doi:10.1016/j.xphs.2017.09.027
28. Salem AH, Dave N, Marbury T, et al. Pharmacokinetics of the BCL-2 Inhibitor Venetoclax in Subjects with Hepatic Impairment. Clin Pharmacokinet. 2019;58(8):1091–1100. doi:10.1007/s40262-019-00746-4
29. Salem AH, Agarwal SK, Dunbar M, et al. Effect of Low- and High-Fat Meals on the Pharmacokinetics of Venetoclax, a Selective First-in-Class BCL-2 Inhibitor. J Clin Pharmacol. 2016;56(11):1355–1361. doi:10.1002/jcph.741
30. Liu H, Michmerhuizen MJ, Lao Y, et al. Metabolism and Disposition of a Novel B-Cell Lymphoma-2 Inhibitor Venetoclax in Humans and Characterization of Its Unusual Metabolites. Drug Metab Dispos. 2017;45(3):294–305. doi:10.1124/dmd.116.071613
31. Leukemia & Lymphoma Group, Chinese Society of Hematology, Chinese Medical Association. Chinese guidelines for diagnosis and treatment of adult acute myeloid leukemia (not APL) (2023). Zhonghua Xue Ye Xue Za Zhi. 2023;44(9):705–712. doi:10.3760/cma.j.issn.0253-2727.2023.09.001
32. Döhner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood. 2022;140(12):1345–1377. doi:10.1182/blood.2022016867
33. Eisenmann ED, Jin Y, Weber RH, Sparreboom A, Baker SD. Development and validation of a sensitive UHPLC-MS/MS analytical method for venetoclax in mouse plasma, and its application to pharmacokinetic studies. J Chromatogr B Analyt Technol Biomed Life Sci. 2020;1152:122176. doi:10.1016/j.jchromb.2020.122176
34. Zhao Y, Guo N, Zhu Y, et al. Population Pharmacokinetic Models of Venetoclax in Hematologic Malignancies: a Systematic Review. DDDT. 2024;18:1771–1784. doi:10.2147/DDDT.S458927
35. Gong JQX, Suleiman AA, Menon R, et al. Pooled Population Pharmacokinetic Analyses of Venetoclax in Patients Across Indications and Healthy Subjects from Phase 1, 2, and 3 Clinical Trials. J Clin Pharmacol. 2023;63(8):950–960. doi:10.1002/jcph.2248
36. Jones AK, Freise KJ, Agarwal SK, et al. Clinical Predictors of Venetoclax Pharmacokinetics in Chronic Lymphocytic Leukemia and Non-Hodgkin’s Lymphoma Patients: a Pooled Population Pharmacokinetic Analysis. AAPS J. 2016;18(5):1192–1202. doi:10.1208/s12248-016-9927-9
37. Minocha M, Zeng J, Medema JK, Othman AA. Pharmacokinetics of the B-Cell Lymphoma 2 (Bcl-2) Inhibitor Venetoclax in Female Subjects with Systemic Lupus Erythematosus. Clin Pharmacokinet. 2018;57(9):1185–1198. doi:10.1007/s40262-017-0625-2
38. Samineni D, Gibiansky L, Wang B, et al. Pharmacokinetics and Exposure-Response Analysis of Venetoclax + Obinutuzumab in Chronic Lymphocytic Leukemia: phase 1b Study and Phase 3 CLL14 Trial. Adv Ther. 2022;39(8):3635–3653. doi:10.1007/s12325-022-02170-w
39. Samineni D, Huang W, Gibiansky L, et al. Population Pharmacokinetics and Exposure-Response Analyses for Venetoclax in Combination with R-CHOP in Relapsed/Refractory and Previously Untreated Patients with Diffuse Large B Cell Lymphoma. Adv Ther. 2022;39(1):598–618. doi:10.1007/s12325-021-01919-z
40. Deng R, Gibiansky L, Lu T, et al. Bayesian Population Model of the Pharmacokinetics of Venetoclax in Combination with Rituximab in Patients with Relapsed/Refractory Chronic Lymphocytic Leukemia: results from the Phase III MURANO Study. Clin Pharmacokinet. 2019;58(12):1621–1634. doi:10.1007/s40262-019-00788-8
41. Verheijen RB, Yu H, Schellens JHM, et al. Practical Recommendations for Therapeutic Drug Monitoring of Kinase Inhibitors in Oncology. Clin Pharmacol Ther. 2017;102(5):765–776. doi:10.1002/cpt.787
42. Gao P, Zhang W, Fang X, et al. Simultaneous quantification of venetoclax and voriconazole in human plasma by UHPLC-MS/MS and its application in acute myeloid leukemia patients. J Pharm Biomed Anal. 2023;227:115279. doi:10.1016/j.jpba.2023.115279
43. Kobayashi M, Yasu T, Suzaki K, Kosugi N. Utility of therapeutic drug monitoring of venetoclax in acute myeloid leukemia. Med Oncol. 2022;39(12):259. doi:10.1007/s12032-022-01865-y
44. Matsui M, Yasu T, Makimoto A, Yuza Y. Pharmacokinetic analysis of crushed venetoclax tablets combined with azacitizine for recurrent pediatric acute myeloid leukemia (AML). Cancer Chemother Pharmacol. 2024;95(1). doi:10.1007/s00280-024-04730-z
45. Wille K, Dumke M, Wilsdorf N, et al. Venetoclax Combined With FLAG - IDA in Refractory or Relapsed Acute Myeloid Leukemia. Eur J Haematol. 2025;114(1):17–25. doi:10.1111/ejh.14302
46. Badawi M, Gopalakrishnan S, Engelhardt B, et al. Dosing of Venetoclax in Pediatric Patients with Relapsed Acute Myeloid Leukemia: analysis of Developmental Pharmacokinetics and Exposure-Response Relationships. Clin Ther. 2024;46(10):759–767. doi:10.1016/j.clinthera.2024.09.008
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Population Pharmacokinetic Analyses and Exposure–Efficacy Relationships of Venetoclax in Chinese Pediatric Patients with Hematological Malignancy in a Real‐World Setting
Zhao Y, Song X, Zhang L, Zhu Y, Chen J, Gong Y, Luo X, He H, Zhang X, Huang L
Drug Design, Development and Therapy 2026, 20:583847
Published Date: 20 March 2026