Back to Journals » Medical Devices: Evidence and Research » Volume 14
Real-World Outcomes of Patients Undergoing Open Colorectal Surgery with Wound Closure Incorporating Triclosan-Coated Barbed Sutures: A Multi-Institution, Retrospective Database Study
Authors Johnson BH ![]() , Rai P
, Rai P ![]() , Jang SR, Johnston SS, Chen BPH
, Jang SR, Johnston SS, Chen BPH
Received 16 December 2020
Accepted for publication 10 February 2021
Published 24 February 2021 Volume 2021:14 Pages 65—75
DOI https://doi.org/10.2147/MDER.S297671
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Barbara H Johnson,1 Pragya Rai,1 Se Ryeong Jang,2 Stephen S Johnston,1 Brian Po-Han Chen3
1Real World Data Analytics and Research, Epidemiology, Medical Devices, Johnson & Johnson, New Brunswick, NJ, USA; 2College of Population Health, Thomas Jefferson University, Philadelphia, PA, USA; 3Health Economics and Market Access, Ethicon Inc., Somerville, NJ, USA
Correspondence: Stephen S Johnston
Medical Device Epidemiology and Real-World Data Analytics and Research, Johnson & Johnson, New Brunswick, NJ, 08901, USA
Email [email protected]
Purpose: Open colorectal surgery is associated with a high rate of postoperative wound complications. This is a single-arm study of real-world outcomes of triclosan-coated barbed suture (Ethicon’s STRATAFIXTM Symmetric PDSTM Plus Knotless Tissue Control Device [SSPP]) used in open colorectal surgery.
Methods: Retrospective cohort study using the Premier Healthcare Database. The study included patients who underwent an inpatient open colorectal surgery with wound closure using SSPP (size 0 or 1 to increase the likelihood the suture was used in fascia) between October 2015–September 2019 (N=593). Wound complications, hospital length of stay, total hospital costs (2019 US$), and all-cause readmissions post-discharge were measured. Post-hoc multivariable analyses compared wound complications between non-elective admissions and elective.
Results: The overall incidence of wound complications within 30-days post-procedure was 7.1%, with the majority of those being surgical site infections (SSI) (6.0%). Mean operation time was 190 (standard deviation [SD]=64.4) mins, postoperative length of stay was 8.1 (SD=11.9) days, 30-day readmission rate was 11.8%, and total hospital costs were $31,693 (SD=$40,076). As compared with published literature on the rate of SSI in colorectal surgery, the 30-day rate of SSI in the present study (6.0%) fell within the range of 5.4% to 18.2% for open colorectal surgery and from 4.3% to 21.5% for combined open and minimally invasive procedures. Multivariable-adjusted incidence proportions of wound complications were slightly lower for non-elective admissions and did not differ significantly from those of elective admissions.
Conclusion: The rate of wound complications observed in the present study falls within the range of rates previously reported in the literature, suggesting a safe and effective role for SSPP in open colorectal surgery. In post hoc analyses, the adjusted rate of wound complications was similar between non-elective and elective admissions. Head-to-head studies are required to determine comparative advantages or disadvantages for SSPP versus other sutures.
Keywords: open colorectal surgery, barbed sutures, sigmoidectomy, surgical site infections, wound dehiscence
Introduction
Open colorectal surgery is classified as clean-contaminated surgery, where endogenous flora may be involved, and may also involve contaminated or dirty-infected wounds.1 This can result in a high rate of postoperative wound complications, such as surgical site infection (SSI), wound dehiscence, and organ system infection.2,3 Indeed, the incidences of SSI and wound dehiscence after open colorectal surgery have been estimated to vary from 16.4% to 25.2%4,5 and 2% to 3%,6,7 respectively. Wound complications further contribute to perioperative morbidity, extended length of stay in the hospital, and hospital-borne financial burden.8,9
A key factor that influences the incidence of wound complications is the quality of wound closure.10,11 As compared with conventional sutures, barbed sutures have been shown to significantly reduce incision closure time, yield higher cyclical tension, and provide better waterproofing.11–13 Such advantages have led to increasing adoption in arthroplasty,12–16 gastrointestinal,11,17–20 gynecological,21–25 urological,26 and plastic surgery.27 Some barbed sutures are also coated with triclosan, an antiseptic agent, which is intended to inhibit the development of infection.1,10 A recent randomized clinical trial in Spain reported that the use of triclosan-coated barbed sutures (Ethicon STRATAFIXTM Symmetric PDSTM Plus Knotless Tissue Control Device [SSPP]) in emergent abdominal surgery resulted in a statistically significant lower rate of incisional SSI as compared with triclosan-coated and non-coated conventional sutures.10 However, more data are needed to understand the potential role of SSPP in open colorectal surgery in routine clinical practice.
Therefore, we conducted a retrospective, single-arm study of the real-world outcomes of patients undergoing open colorectal surgery with wound closure incorporating SSPP sizes 0 and 1 using a large database collected from multiple institutions throughout the US. Sizes 0 and 1 were included to increase the likelihood that SSPP was used in the fascia closure layer.
Methods
Study Design
This was a single-arm, multi-institution, retrospective cohort study of patients who underwent open colorectal surgery in an inpatient setting with wound closure using SSPP between October 1, 2015 and September 30, 2019.
Data Source
Data were extracted from Premier Healthcare Database, a US hospital-based, all-payer database that contains administrative, healthcare utilization, and financial information. This database contains over 231 million unique deidentified patients and data from over 900 geographically diverse community of teaching hospitals and hospital systems. The database contains information on admissions and discharge diagnosis, patient characteristics, hospital characteristics, physician specialties, and costs from the hospital perspective, among other features. This study was exempt from Institutional Review Board oversight because it contains only deidentified patient records, as dictated by Title 45 Code of Federal Regulations (45 CFR 46, 101(b)(4)). Data were collected from the Premier Healthcare Database using International Classification of Diseases, 10th Revision, Clinical Modification/Procedure Coding System (ICD-10-CM/PCS) codes and other structured fields native to the database.
Patient Selection
Patients selected for study were aged 18 years and older who had an inpatient admission for open colorectal surgery for which SSPP size 0 or size 1 was used during wound closure (first admission = index admission). Individuals for whom the colorectal surgery was identified as having robotic assistance or converted from a minimally invasive approach were excluded. Patients were stratified by elective vs non-elective (emergency or urgent) admission.
Patient, Procedure, and Hospital/Provider Characteristics
Patient, procedure, and hospital/provider characteristics were measured from the study database using information recorded during the index admission. Variables were selected based on availability within the study database and their role as potential confounding factors in the post hoc analysis comparing between elective and non-elective surgery (described in greater detail below).
Patient demographics included age in years, sex, race, marital status, and payer type. Patient clinical characteristics were measured using ICD-10-CM diagnosis codes designated as being present on admission and included the Charlson comorbidity index score, a widely used and validated sored measure of health status, as well as all individual comorbidities from the Elixhauser comorbidity index, another widely used and validated set of 31 prognostic comorbidities; comorbidities with 0 patients were omitted from the analysis.28 Procedure characteristics included year of procedure, number of days between admission to the hospital and undergoing surgery, whether the primary-coded surgery was in the colon vs the rectum, and whether the surgery involved bypass, excision, or resection. Finally, hospital/provider characteristics included urban or rural hospital, hospital teaching status, hospital geographic region, hospital bed size, hospital surgical volume for colorectal surgery, and procedural physician specialty.
Outcomes
Wound complication outcomes were measured using ICD-10-CM diagnosis codes listed in Appendix 1, including surgical site infection, wound dehiscence, abscess/cellulitis/granuloma, and a composite measure of each of the aforementioned endpoints. These diagnoses were searched for during the index admission, and separately during return visits to a hospital’s network, including inpatient readmission, emergency room visits, urgent outpatient visits, and non-urgent outpatient visits, all over a 30-day follow-up period. To ensure completeness of data capture, patients for whom 30-day wound complication rates were measured and reported were required to have an index admission to a hospital that continued to contribute data for at least that duration of time; 97.6% of patients met this criterion.
Economic and healthcare resource utilization outcomes measured during the index admission included hospital length of stay (LOS), total hospital costs, and all-cause readmissions within 30, 60, and 90 days post-discharge from the index admission. All costs were inflation-adjusted to 2019 US dollars using the Medical Care component of the US Bureau of Labor Statistics Consumer Price Index. All-cause readmissions were measured only among patients for whom we could discern the hospital had discharge records extending throughout the observation period of interest (30, 60, or 90 days). In addition, to further characterize these readmissions, information on the primary diagnoses and procedures for readmissions at 30 days were recorded.
Statistical Analyses
Univariate analysis was performed to report appropriate summary statistics for each study variable of interest: eg count, incidence proportion. Analyses were stratified by elective and non-elective admission type. Sub-analyses of the predominant primary procedure type (sigmoidectomy) were also conducted.
After completion of the analyses addressing the primary objective, post hoc analyses were conducted to compare the incidence of wound complications between patients in the elective vs non-elective admission type groups. Numerous studies have implicated non-elective colorectal surgery as an independent risk factor for SSI, other forms of morbidity, and mortality, perhaps due to contamination of wounds, longer operative time and post-operative hospital length of stay, and less opportunity for preoperative preparations intended to reduce the incidence of SSI.5,29–33
We hypothesized that the historically observed substantial differences in the rate of SSI between those undergoing elective vs non-elective colorectal surgery may appear to be attenuated in the present cohort of patients in whom SSPP was used, after accounting for all patient, procedure, and provider/hospital characteristics. Thus, multivariable generalized linear models (GLM) with a logit link and binomial error distribution were used to compare the incidence proportion of SSI and wound complications at index and over the 30-day follow-up period (including index), adjusting for all variables listed in Tables 1 and 2. These models accounted for hospital-level clustering through robust standard errors. Multivariable-adjusted outcome estimates were generated for each group using marginal standardization. A p-value <0.05 was considered statistically significant. Data management was performed using R version 3.5.3 and statistical analyses were performed using STATA (StataCorp 2015).
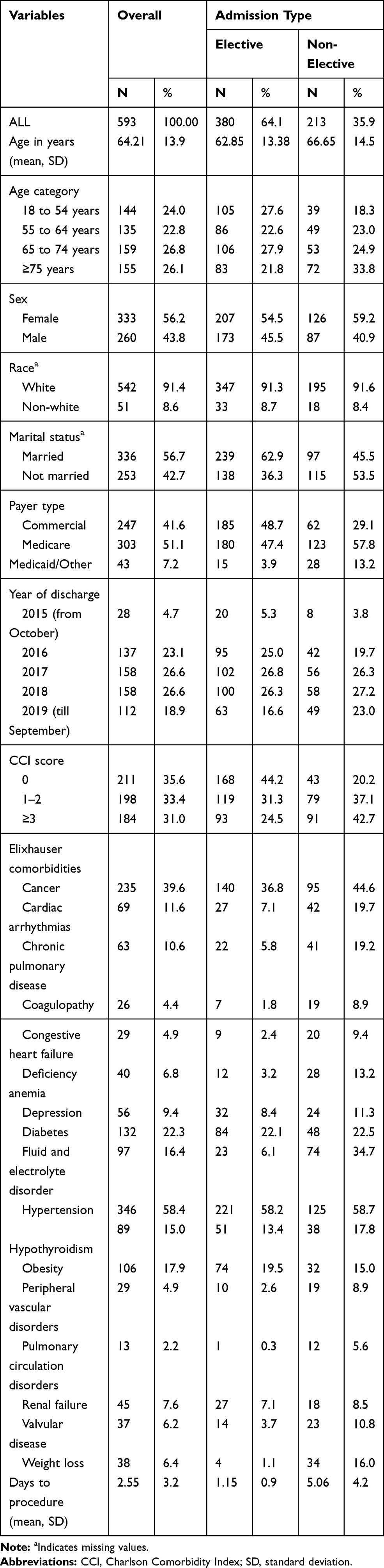 |
Table 1 Patient Demographics and Clinical Characteristics |
 |
Table 2 Hospital/Provider Characteristics |
Comparison with Published Literature
To contextualize the study findings, a literature review was conducted to compare the findings regarding the incidence of wound complications in the present study with those of previously published studies. A literature search was performed for published full-text articles using PubMed. The keywords used in the search were “open colorectal surgery” “colorectal surgery” “wound complications” “surgical site infection” “wound dehiscence” “barbed suture” and “triclosan coated suture” Articles published from January 2015 to September 2020 were included.The initial selection was based on the article title and abstract, where articles on laparoscopic colorectal surgery only, missing information on wound complications, or presenting case reports were excluded. Following this, duplicates were removed and key comparative findings from the remaining 15 articles were summarized.
Results
Patient and Hospital/Provider Characteristics
Patient demographic and clinical characteristics are shown in Table 1. A total of 593 patients undergoing open colorectal surgery incorporating wound closure with SSPP were identified from among 21 institutions. Of the 593 patients, 64% underwent elective surgery and 36% underwent non-elective surgery. The majority of patients were aged ≥65 years (53%), female (56%), and just over half (51%) had Medicare insurance. The mean number of days from admission to procedure was 2.6 days (standard deviation [SD] = 3.2). Sigmoidectomy was the most common procedure, performed in 333 patients.
Hospital/provider characteristics are shown in Table 2. Most patients presented in urban hospitals (95%), and/or those located in the Southern US (94%). The majority (61%) of procedures were in large hospitals (≥500 beds) and 44% of hospitals performed over 150 open colorectal surgeries per year. Physicians with a specialty of colon/rectal surgery performed 85% of surgeries.
Wound Complications
Incidence proportions of wound complications during the index admission alone and during the index admission through 30-day follow-up are shown in Table 3. Overall, 3.2% of patients developed any wound complication during their index admission, with SSIs accounting for the majority (3.0%). When analyzing by admission type (elective vs non-elective), the proportion of non-elective patients experiencing any wound complication (SSI, wound dehiscence, abscess/cellulitis/granuloma) was slightly higher than those with an elective admission (3.3% and 3.2%, respectively); SSIs again accounted for the majority of wound complications (3.3% and 2.9%, respectively).
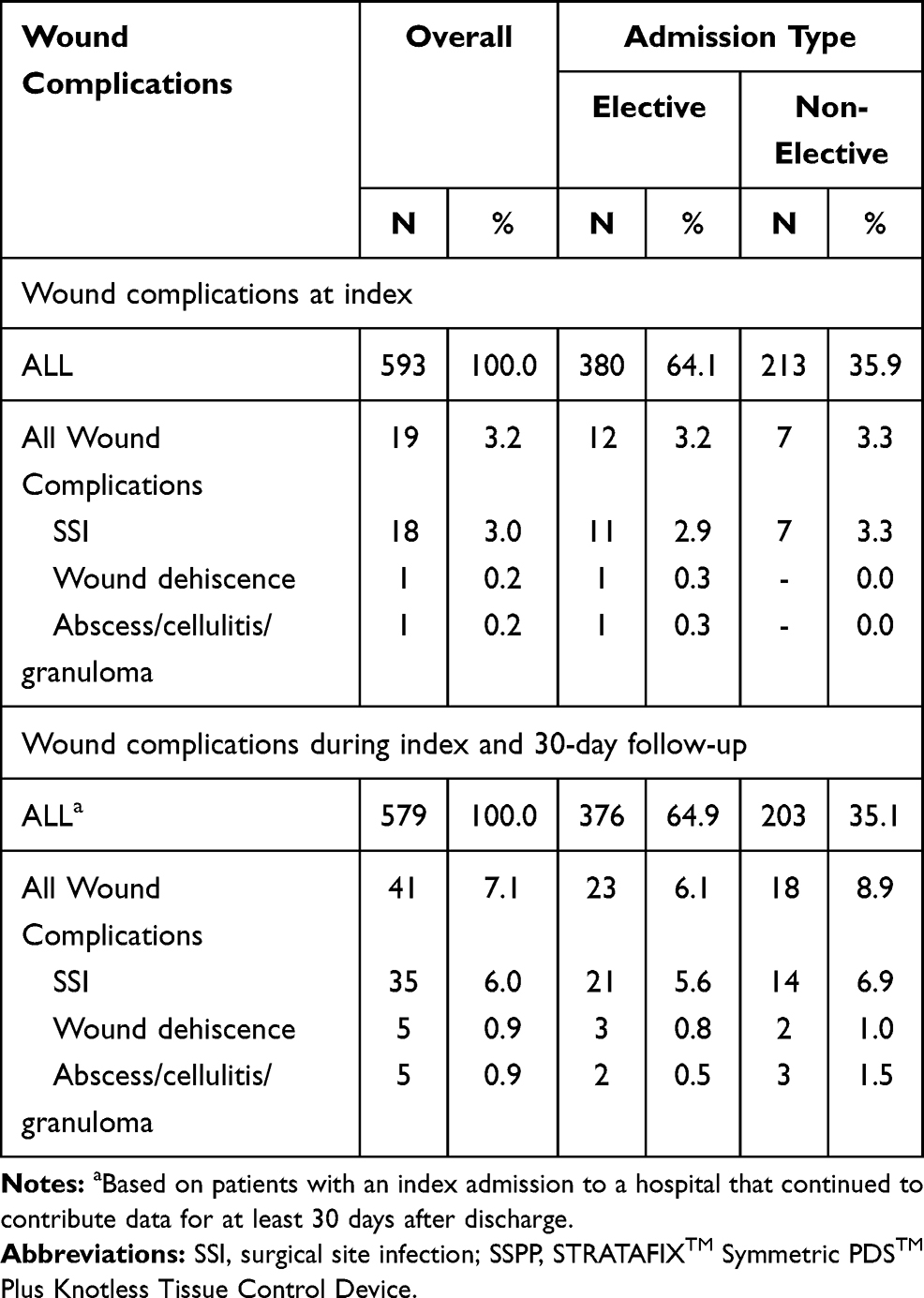 |
Table 3 All Wound Complication, Surgical Site Infections, and Wound Dehiscence During Index and Follow-Up Time Periods After Open Colorectal Surgery Using SSPP |
During the index admission through 30-day follow-up period, among patients for whom we could discern the hospital had discharge records extending at least 30 days (579 patients), 7.1% developed any wound complication, with SSIs accounting for the majority (6.0%). When analyzing by admission type (elective vs non-elective), the proportion of non-elective patients experiencing any wound complication was again higher than those with an elective admission (8.9% and 6.1%, respectively), and SSIs still accounted for the majority of wound complications (6.9% and 5.6%, respectively). The subgroup analysis of sigmoidectomy (Appendix 2) revealed similar findings to the primary analyses.
Economic and Healthcare Resource Utilization Outcomes
Economic and healthcare resource utilization outcomes are shown in Table 4. Overall, mean operating room time was 191 minutes (SD = 64) with a mean hospital LOS of 8.1 days (SD = 11.9 days). Mean total hospital costs for open colorectal surgery were $31,693 (SD = $40,076). The predominant drivers of total hospital costs were mean room and board costs of $9956 (SD = $18,714) and mean operating room costs of $9644 (SD = $3531). All-cause readmission rates were 11.8% at 30 days, 16.9% at 60 days and 21.1% at 90 days.
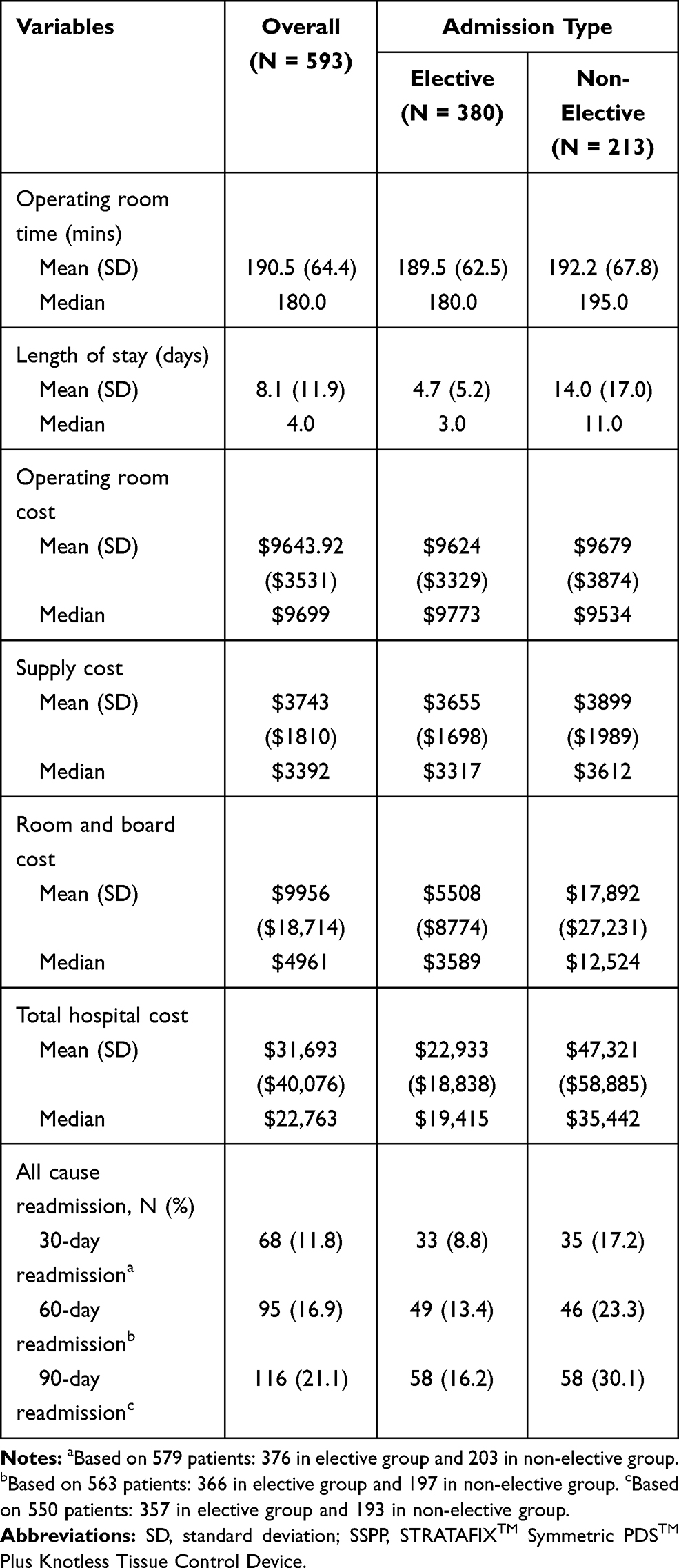 |
Table 4 Economics and Healthcare Resource Utilization Outcomes of Open Colorectal Surgery Using SSPP |
In elective surgery, the mean operating room time was 190 minutes (SD = 63) with a mean hospital LOS of 4.7 days (SD = 5.2). Mean total hospital costs were $22,933 (SD = $18,838). Mean all-cause 30-, 60- and 90-day readmission rates were 8.8%, 13.4%, and 16.2%, respectively. In non-elective surgery, the mean operating room time was 192.2 mins (SD = 67.8) with a mean hospital LOS of 14.0 days (SD = 17). Mean total hospital costs were commiserate with the long hospital LOS at $47,321 (SD = $58,885). Mean all-cause 30-, 60- and 90-day readmission rates were 17.2%, 23.3%30.1%, respectively. The subgroup analysis of sigmoidectomy (Appendix 3) revealed similar findings to the primary analyses.
Appendix 4 reports the distribution of primary diagnoses and procedures for readmissions at 30 days. The most common primary diagnoses for readmissions were related to infection and gastrointestinal complications. The most common primary procedures performed during readmissions were drainage procedures.
Post Hoc Analyses
Results of the post hoc multivariable analyses comparing the incidence proportions of SSI and overall wound complications between patients in the elective vs non-elective admission type groups are presented in Appendix 5. After adjusting for all variables in Tables 1 and 2, non-elective admissions were associated with statistically insignificant and slightly lower incidence proportions of SSIs and overall wound complications as compared with elective admissions, during both index and the index through 30-day follow-up period.
Comparison with Published Literature
Key results from prior published studies (incidence of SSI and other economic and healthcare resource utilization outcomes) examining colorectal surgery are summarized in Table 5. Information on the incidence of SSI, 30-day readmissions, operating room time and hospital LOS were extracted from four studies34–37 on open colorectal surgery and nine studies38–46 on a combination of both open and minimally invasive surgery (MIS). Of these 13 studies, seven studies utilized information from multiple hospitals while six studies were single-institution studies. Use of non-barbed PDS Plus suture, a triclosan-coated conventional suture, was mentioned in two studies.44,45 Incidence proportions of SSI within 30 days post operation in the present study is 6.0% which falls within the range of 5.4% to 18.2% for open colorectal surgery and from 4.3% to 21.5% for combined open and MIS procedures, as reported in published literature. Overall, 30-day readmission, mean operating room time, and mean hospital LOS ranged from 3% to 12.5%, 145 mins to 213 mins, and 6.8 days to 18.5 days, respectively, all ranges of which include the point estimates from the present study.
 |
Table 5 Comparison of Clinical Outcomes Among Published Studies on Open Colorectal Surgery |
Discussion
To our knowledge, this is the first study to explore clinical and healthcare resource utilization outcomes among patients undergoing open colorectal surgery with wound closure incorporating the use of SSPP. In a randomized multicenter study conducted by Ruiz-Tovar and colleagues, the use of SSPP in emergent abdominal surgery – including clean-contaminated, contaminated, and dirty wounds– had shown significantly lower incisional SSI rates than traditional sutures with and without triclosan-coating (6.4%, 8.9% and 23.4%, respectively).10 Our study in open colorectal surgery similarly found the 30-day SSI rate with wound closure incorporating the use of SSPP to be 6.0%.
Although the present observational study’s results are in line with those of the randomized study conducted by Ruiz-Tovar and colleagues, it adds uniquely to the understanding of the use of SSPP in open colorectal surgery. First, whereas the prior study was conducted within hospitals in Spain, the present study reports the first evidence on wound complications in open colorectal surgery with the use of SSPP within hospitals in the US. Second, whereas the prior study included a relatively small number of patients with SSPP (N=47), the present study was larger, including 593 patients. Finally, whereas the prior study enrolled only patients undergoing emergent surgery, the present study included both elective and non-elective surgery, reflecting a broader population to which the results may apply.
Notably, patients in the non-elective group experienced longer operating room time (median 195 minutes vs 180 minutes), hospital length of stay (median 11 days versus 3 days), greater total hospital costs (median $35,442 vs $19,415), and higher rates of inpatient readmission at 30 days (17.2% vs 8.8%) and beyond, as compared with those in the elective admission group. In the descriptive analysis, patients in the non-elective group also experienced slightly higher incidence proportions of SSI (6.8% vs 5.6%) and overall wound complications (8.9% vs 6.1%) as compared with those in the elective admission group. Consistent with the worse unadjusted outcomes of patients in the non-elective admission group, these patients were also older and had higher prevalence rates of several important comorbidities (Table 1).
However, despite such substantial baseline and outcome differences, multivariable analyses yielded adjusted incidence proportion of SSI and overall wound complications that were slightly lower in the non-elective admission group as compared with the elective admission group, with the difference being statistically insignificant between the groups. These findings are consistent with the hypothesis that SSPP may have attenuated the increased risk of wound complications that is typically associated with non-elective surgery. Because it would be infeasible and unethical to conduct a randomized controlled trial with the assignment of patients to elective versus non-elective colorectal surgery, additional observational studies would be useful to corroborate this aspect of the present study’s findings. If conducted prospectively, such studies could also further explore the role of additional considerations of the wound closure with respect to the layer at which different sutures and other closure technologies (eg, staples, topical skin adhesives) are used.
Since the primary aim of this single-arm study involved no comparators, findings for select clinical and healthcare resource utilization outcomes were compared with published studies on open and MIS colorectal surgery. The incidence of SSIs in the present study (6.0%) fell within the range of published studies (4.3–21.5%). Cross-study differences in the study periods, patient populations, and methods of SSI ascertainment likely accounted for the wide range of estimates. For example, the study published by Maruyama et al (2020) consisted of high-risk patients with benign diseases34 while 62% of the patients in Esemuede study (2015) had an American Society of Anesthesiologists (ASA) physical score of 3 or greater,37 both of which are associated with poorer outcomes and higher incidences of SSI. In addition, the incidence of SSI in this study (6.0%) was similar or lower than those reported with the use of PDS Plus sutures (6.0–12.9%).44,45 Although both SSPP and PDS Plus sutures are coated with triclosan, the barbed nature of SSPP may provide a more watertight closure and thus reduce the risk of contaminants. In addition, SSPP eliminates the need for tying knots along the wound closure compared to non-barbed sutures which can either be knotted loose or tightened too much, leading to insufficient wound healing.10 The knotless feature of SSPP allows for faster procedures, thereby minimizing wound exposure to infectious agents, and homogenous healing of the wounds.10
This is also the first study to report economic outcomes associated with SSPP use in open colorectal surgery. Mean total hospital cost was $31,693, with mean room and board cost and mean operating room cost accounting for approximately 31% and 30% of total cost, respectively. However, there is a lack of data to which the present study’s findings can be compared in terms of economic outcomes during the study’s more recent timeframe extending into September 2019.
Surgical site infections after colorectal surgery have been associated with a substantial economic and healthcare resource use burden. For example, Ammann and colleagues reported that among 9738 patients undergoing low anterior resection (LAR) in the US from 2010 to 2015, those who experienced surgical site infection had 7.3–7.7 days longer hospital length of stay for the LAR procedure, 6.2–15.0% higher absolute incremental risk of discharge to institutional post-acute care, 10.6–16.4% higher absolute incremental risk of 90-day inpatient readmission, $20,382 higher costs for the LAR admission from the hospital perspective, and $23,934 higher costs for the LAR admission from the payer perspective.47 Leaper and colleagues reported that among 107,665 patients undergoing colorectal surgery in the US from 2014 to 2018, 12-month costs associated with SSI ranged from $17,551 - $102,280 for Medicare and from $36,429 - $144,809 for commercial payers.48 They also projected that triclosan sutures, such as SSPP, could significantly reduce median payer costs by $807 - $1170 as compared with traditional sutures, based on probabilistic cost analysis. As more data accrue to support comparative analysis of SSPP with other sutures in open colorectal surgery, future studies should compare economic and healthcare resource utilization outcomes between these alternatives in the real-world setting.
The present study is subject to limitations. First, although this study focused on the use of sutures specifically intended for closure in fascia, the tissue layer or anatomy in which the suture was used (eg, anastomosis) cannot be ascertained from the database. To address this limitation, we specifically selected only patients in whom SSPP sizes 0 and 1 were used in order to increase the likelihood that SSPP was used in the fascia closure layer. The tensile strength of the fascial wound is known to be one of the most important aspects of optimal closure, and sutures in this layer may experience significant pressure, leading to abdominal wound dehiscence due to sutures pulling through the fascia.49 Incision through the fascia is also a risk factor for deep incisional SSI and organ/space SSI.50 Second, other barbed and/or conventional sutures and wound closure technologies may have been used during the procedure which may have influenced the study outcomes. Appropriate abdominal superficial skin closure is also important for wound healing and may be achieved through sutures, skin staples, or topical skin adhesives and skin closure systems. Third, large databases that contain real-world administrative healthcare data are currently limited with respect to detailed information on medical devices. As a result of this data source limitation, we may not have captured all open colorectal procedures incorporating the use of SSPP during the study period. The aforementioned three limitations could be overcome in the future through the use of a prospective study design with customized case report forms, although the comparatively higher cost of such a study design would be an important logistical consideration. Finally, the study results are not generalizable to all the hospitals in the US. Despite these limitations, this is the first study to report on SSPP use in open elective and non-elective colorectal surgery in real-world clinical practice, providing a benchmark for the outcomes of SSPP use in elective and non-elective surgery.
Conclusion
In this study of 593 patients undergoing open colorectal surgery with wound closure incorporating SSPP, approximately 7% of patients developed wound complication, irrespective of elective vs non-elective admission. In post hoc analyses, the adjusted rate of wound complications was similar between non-elective and elective admissions. The rate of wound complications observed in the present study falls within the range of rates previously reported in the literature, suggesting a safe and effective role for SSPP in open colorectal surgery. Head-to-head studies are required to determine whether any comparative advantages or disadvantages exist for SSPP versus other sutures.
Ethics Approval Statement
This study was exempt from Institutional Review Board oversight because it contains only deidentified patient records, as dictated by Title 45 Code of Federal Regulations (45 CFR 46, 101(b)(4)).
Acknowledgments
We would like to acknowledge Nivesh Elangovanraaj for his work on analyzing the data for this project.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Sponsorship for this study, the article processing charges, and Open Access fee was funded by Johnson & Johnson (Ethicon, Somerville, NJ).
Disclosure
Barbara Johnson is an employee of Johnson & Johnson. Pragya Rai is an employee under contract with Johnson & Johnson. Stephen Johnston is an employee of Johnson & Johnson and Johnson & Johnson stockholder. Brian Po-Han Chen is an employee of Ethicon. The authors report no other conflicts of interest in this work.
References
1. Baracs J, Huszar O, Sajjadi SG, Horvath OP. Surgical site infections after abdominal closure in colorectal surgery using triclosan-coated absorbable suture (PDS Plus) vs. uncoated sutures (PDS II): a randomized multicenter study. Surg Infect (Larchmt). 2011;12(6):483–489. doi:10.1089/sur.2011.001
2. Alves A, Panis Y, Mathieu P, Mantion G, Kwiatkowski F, Slim K. Postoperative mortality and morbidity in French patients undergoing colorectal surgery: results of a prospective multicenter study. Arch Surg (Chicago, Ill: 1960). 2005;140(3):278–283, discussion 284. doi:10.1001/archsurg.140.3.278
3. Tevis SE, Kennedy GD. Postoperative complications: looking forward to a safer future. Clin Colon Rectal Surg. 2016;29(3):246–252. doi:10.1055/s-0036-1584501
4. Gomila A, Carratalà J, Camprubí D, et al. Risk factors and outcomes of organ-space surgical site infections after elective colon and rectal surgery. Antimicrob Resist Infect Control. 2017;6:40. doi:10.1186/s13756-017-0198-8
5. Hübner M, Diana M, Zanetti G, Eisenring M-C, Demartines N, Troillet N. Surgical site infections in colon surgery: the patient, the procedure, the hospital, and the surgeon. Arch Surg (Chicago, Ill: 1960). 2011;146(11):1240–1245. doi:10.1001/archsurg.2011.176
6. Söderbäck H, Gunnarsson U, Martling A, Hellman P, Sandblom G. Incidence of wound dehiscence after colorectal cancer surgery: results from a national population-based register for colorectal cancer. Int J Colorectal Dis. 2019;34(10):1757–1762. doi:10.1007/s00384-019-03390-3
7. Kenig J, Richter P, Żurawska S, Lasek A, Zbierska K. Risk factors for wound dehiscence after laparotomy-clinical control trial. Pol Przegl Chir. 2012;84(11):565–573. doi:10.2478/v10035-012-0094-0
8. Ishikawa K, Kusumi T, Hosokawa M, Nishida Y, Sumikawa S, Furukawa H. Incisional surgical site infection after elective open surgery for colorectal cancer. Int J Surg Oncol. 2014;2014:419712. doi:10.1155/2014/419712
9. Scarborough JE, Schumacher J, Kent KC, Heise CP, Greenberg CC, Milone M. Associations of specific postoperative complications with outcomes after elective colon resection: a procedure-targeted approach toward surgical quality improvement. JAMA Surg. 2017;152(2):e164681–e164681. doi:10.1001/jamasurg.2016.4681
10. Ruiz-Tovar J, Llavero C, Jimenez-Fuertes M, Duran M, Perez-Lopez M, Garcia-Marin A. Incisional surgical site infection after abdominal fascial closure with triclosan-coated barbed suture vs triclosan-coated polydioxanone loop suture vs polydioxanone loop suture in emergent abdominal surgery: a randomized clinical trial. J Am Coll Surg. 2020;230(5):766–774. doi:10.1016/j.jamcollsurg.2020.02.031
11. Wiggins T, Majid MS, Markar SR, Loy J, Agrawal S, Koak Y. Benefits of barbed suture utilisation in gastrointestinal anastomosis: a systematic review and meta-analysis. Ann R Coll Surg Engl. 2020;102(2):153–159. doi:10.1308/rcsann.2019.0106
12. Li P, Zhang W, Wang Y, et al. Barbed suture versus traditional suture in primary total knee arthroplasty: a systematic review and meta-analysis of randomized controlled studies. Medicine (Baltimore). 2020;99(21):e19945–e19945. doi:10.1097/MD.0000000000019945
13. Sundaram K, Piuzzi NS, Klika AK, et al. Barbed sutures reduce arthrotomy closure duration and suture utilisation compared to interrupted conventional sutures for primary total hip arthroplasty: a randomised controlled trial. HIP Int. 2020;1120700020911891. Doi:10.1177/1120700020911891
14. Ting NT, Moric MM, Della Valle CJ, Levine BR. Use of knotless suture for closure of total hip and knee arthroplasties: a prospective, randomized clinical trial. J Arthroplasty. 2012;27(10):1783–1788. doi:10.1016/j.arth.2012.05.022
15. Han Y, Yang W, Pan J, et al. The efficacy and safety of knotless barbed sutures in total joint arthroplasty: a meta-analysis of randomized-controlled trials. Arch Orthop Trauma Surg. 2018;138(10):1335–1345. doi:10.1007/s00402-018-2979-9
16. Thacher RR, Herndon CL, Jennings EL, Sarpong NO, Geller JA. The impact of running, monofilament barbed suture for subcutaneous tissue closure on infection rates in total hip arthroplasty: a retrospective cohort analysis. J Arthroplasty. 2019;34(9):2006–2010. doi:10.1016/j.arth.2019.05.001
17. Milone M, Di Minno MN, Galloro G, et al. Safety and efficacy of barbed suture for gastrointestinal suture: a prospective and randomized study on obese patients undergoing gastric bypass. J Laparoendosc Adv Surg Tech A. 2013;23(9):756–759. doi:10.1089/lap.2013.0030
18. Zhou H, Wang S, Fan F, Peng J. Primary closure with knotless barbed suture versus traditional T-tube drainage after laparoscopic common bile duct exploration: a single-center medium-term experience. J Int Med Res. 2020;48(1):300060519878087.
19. Pennestri F, Gallucci P, Prioli F, et al. Barbed vs conventional sutures in bariatric surgery: a propensity score analysis from a high-volume center. Updates Surg. 2019;71(1):113–120. doi:10.1007/s13304-018-0589-2
20. Bracale U, Merola G, Cabras F, Andreuccetti J, Corcione F, Pignata G. The use of barbed suture for intracorporeal mechanical anastomosis during a totally laparoscopic right colectomy: is it safe? A retrospective nonrandomized comparative multicenter study. Surg Innov. 2018;25(3):267–273. doi:10.1177/1553350618765871
21. Tulandi T, Einarsson JI. The use of barbed suture for laparoscopic hysterectomy and myomectomy: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2014;21(2):210–216. doi:10.1016/j.jmig.2013.09.014
22. Gardella B, Dominoni M, Iacobone AD, et al. What is the role of barbed suture in laparoscopic myomectomy? A meta-analysis and pregnancy outcome evaluation. Gynecol Obstet Invest. 2018;83(6):521–532. doi:10.1159/000488241
23. López CC, Ríos JFL, González Y, et al. Barbed suture versus conventional suture for vaginal cuff closure in total laparoscopic hysterectomy: randomized controlled clinical trial. J Minim Invasive Gynecol. 2019;26(6):1104–1109. doi:10.1016/j.jmig.2018.08.030
24. Karacan T, Ozyurek E, Usta T, et al. Comparison of barbed unidirectional suture with figure-of-eight standard sutures in vaginal cuff closure in total laparoscopic hysterectomy. J Obstet Gynaecol. 2018;38(6):842–847. doi:10.1080/01443615.2017.1416597
25. Nakayama K, Razia S, Ishikawa M, et al. Comparison between bidirectional Stratafix(®) barbed suture and conventional suture in laparoscopic myomectomy: a retrospective study. BMC Womens Health. 2020;20(1):164. doi:10.1186/s12905-020-01030-5
26. Bertolo R, Campi R, Klatte T, et al. Suture techniques during laparoscopic and robot-assisted partial nephrectomy: a systematic review and quantitative synthesis of peri-operative outcomes. BJU Int. 2019;123(6):923–946. doi:10.1111/bju.14537
27. Rubin JP, Hunstad JP, Polynice A, et al. A multicenter randomized controlled trial comparing absorbable barbed sutures versus conventional absorbable sutures for dermal closure in open surgical procedures. Aesthetic Surg J. 2014;34(2):272–283. doi:10.1177/1090820X13519264
28. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
29. Mullen MG, Michaels AD, Mehaffey JH, et al. Risk associated with complications and mortality after urgent surgery vs elective and emergency surgery: implications for defining “quality” and reporting outcomes for urgent surgery. JAMA Surg. 2017;152(8):768–774. doi:10.1001/jamasurg.2017.0918
30. Udholm LS, Rasmussen SL, Madsbøll TK, Omairi M, El-Hussuna A. A systemic review and metaanalysis of postoperative outcomes in urgent and elective bowel resection in patients with Crohn’s disease. Int J Colorectal Dis. 2021;36(2):253–263. doi:10.1007/s00384-020-03786-6
31. Hennessey DB, Burke JP, Ni-Dhonochu T, Shields C, Winter DC, Mealy K. Risk factors for surgical site infection following colorectal resection: a multi-institutional study. Int J Colorectal Dis. 2016;31(2):267–271. doi:10.1007/s00384-015-2413-5
32. Hou TY, Gan HQ, Zhou JF, et al. Incidence of and risk factors for surgical site infection after colorectal surgery: a multiple-center prospective study of 3663 consecutive patients in China. Int J Infect Dis. 2020;96:676–681. doi:10.1016/j.ijid.2020.05.124
33. Watanabe M, Suzuki H, Nomura S, et al. Risk factors for surgical site infection in emergency colorectal surgery: a retrospective analysis. Surg Infect (Larchmt). 2014;15(3):256–261. doi:10.1089/sur.2012.154
34. Maruyama H, Kusachi S, Makino H, Kanno H, Yoshida H, Niitsuma T. Current status of postoperative infection after colorectal surgery: subanalysis of data from the 2015 Japan postoperative infectious complications survey. J Nippon Med Sch. 2020;87:204–210. doi:10.1272/jnms.JNMS.2020_87-403
35. Napolitano MA, Skancke M, Walters J, et al. Outcomes and trends in colorectal surgery in U.S. Veterans: a 10-year experience at a tertiary veterans affairs medical center. J Laparoendosc Adv Surg Tech A. 2020;30(4):378–382. doi:10.1089/lap.2019.0739
36. Huh JW, Lee WY, Park YA, et al. Oncological outcome of surgical site infection after colorectal cancer surgery. Int J Colorectal Dis. 2019;34(2):277–283. doi:10.1007/s00384-018-3194-4
37. Esemuede IO, Gabre-Kidan A, Fowler DL, Kiran RP. Risk of readmission after laparoscopic vs. open colorectal surgery. Int J Colorectal Dis. 2015;30(11):1489–1494. doi:10.1007/s00384-015-2349-9
38. Hajirawala LN, Legare TB, Tiu SPT, et al. The impact of a colorectal care bundle for surgical site infections at an academic disproportionate share hospital with a level I trauma center. Am Surg. 2020;3134820940240.
39. de Paula TR, Nemeth S, Kiran RP, Keller DS. Predictors of complications from stoma closure in elective colorectal surgery: an assessment from the American College of Surgeons National Surgical Quality Improvement Program (ACSNSQIP). Tech Coloproctol. 2020;24:1–9. doi:10.1007/s10151-019-02132-5
40. Kethman WC, Shelton EA, Kin C, Morris AM, Shelton AA. Effects of colorectal surgery classification on reported postoperative surgical site infections. J Surg Res. 2019;236:340–344. doi:10.1016/j.jss.2018.12.005
41. Rudder NJ, Borgert AJ, Kallies KJ, Smith TJ, Shapiro SB. Reduction of surgical site infections in colorectal surgery: a 10-year experience from an independent academic medical center. Am J Surg. 2019;217(6):1089–1093. doi:10.1016/j.amjsurg.2018.11.010
42. Martin D, Hübner M, Moulin E, et al. Timing, diagnosis, and treatment of surgical site infections after colonic surgery: prospective surveillance of 1263 patients. J Hosp Infect. 2018;100(4):393–399. doi:10.1016/j.jhin.2018.09.011
43. Kamboj M, Childers T, Sugalski J, et al. Risk of Surgical Site Infection (SSI) following colorectal resection is higher in patients with disseminated cancer: an NCCN member cohort study. Infect Control Hosp Epidemiol. 2018;39(5):555–562. doi:10.1017/ice.2018.40
44. Yamashita K, Takeno S, Hoshino S, et al. Triclosan sutures for surgical site infection in colorectal cancer. J Surg Res. 2016;206(1):16–21. doi:10.1016/j.jss.2016.06.070
45. Mattavelli I, Rebora P, Doglietto G, et al. Multi-center randomized controlled trial on the effect of triclosan-coated sutures on surgical site infection after colorectal surgery. Surg Infect (Larchmt). 2015;16(3):226–235. doi:10.1089/sur.2014.005
46. Kobayashi S, Ito M, Yamamoto S, et al. Randomized clinical trial of skin closure by subcuticular suture or skin stapling after elective colorectal cancer surgery. Br J Surg. 2015;102(5):495–500. doi:10.1002/bjs.9786
47. Ammann EM, Goldstein LJ, Nagle D, Wei D, Johnston SS. A dual-perspective analysis of the hospital and payer-borne burdens of selected in-hospital surgical complications in low anterior resection for colorectal cancer. Hosp Pract (1995). 2019;47(2):80–87. doi:10.1080/21548331.2019.1568718
48. Leaper DJ, Holy CE, Spencer M, et al. Assessment of the risk and economic burden of surgical site infection following colorectal surgery using a US longitudinal database: is there a role for innovative antimicrobial wound closure technology to reduce the risk of infection? Dis Colon Rectum. 2020;63(12):1628–1638. doi:10.1097/DCR.0000000000001799
49. Mizell JS, Rosen M, Chen W Complications of abdominal surgical incisions; 2020; Available from: https://www.uptodate.com/contents/complications-of-abdominal-surgical-incisions?topicRef=4&source=see_link.
50. NHSN. Surgical site infection event. Procedure-associated module; 2021; Available from: https://www.cdc.gov/nhsn/PDFs/pscManual/9pscSSIcurrent.pdf.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.