Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Real World Evidence on Hormone Receptor Positive and Human Epidermal Growth Factor Receptor 2 Negative Metastatic Breast Cancer in Italy: Insights From 2017 to 2021 Data
Authors Perrone V, Leogrande M ![]() , Cappuccilli M
, Cappuccilli M ![]() , Saragoni S, Cinti Luciani A, Degli Esposti L
, Saragoni S, Cinti Luciani A, Degli Esposti L ![]()
Received 23 October 2024
Accepted for publication 27 February 2025
Published 6 March 2025 Volume 2025:17 Pages 147—155
DOI https://doi.org/10.2147/CEOR.S496606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Valentina Perrone, Melania Leogrande, Maria Cappuccilli, Stefania Saragoni, Andrea Cinti Luciani, Luca Degli Esposti
CliCon S.r.l., Società Benefit, Health, Economics & Outcomes Research, Bologna, 40137, Italy
Correspondence: Valentina Perrone, CliCon S.r.l. Società Benefit, Health, Economics & Outcomes Research, Via Murri 9, Bologna, 40137, Italy, Tel +39 0544 38393, Fax +39 0544 212699, Email [email protected]
Purpose: To describe patients with hormone receptor positive and human epidermal growth factor receptor 2 negative metastatic breast cancer (HR+/HER2- mBC) in Italy for demographic and clinical variables, comorbidity profile, metastases and therapeutic pathways.
Patients and Methods: From 2017 to 2021, HR+/HER2- mBC patients were extrapolated from administrative databases of healthcare entities covering a catchment area of about 3 million health-assisted women. The study included patients with a hospital discharge diagnosis for mBC; AND with specific prescriptions of therapies for HR+; AND without HER2-targeted therapy; OR with at least one prescription for CDK4/6 inhibitors. The following data were collected: age at inclusion, previous drug prescriptions, causes of hospitalization, site and number of metastases, therapeutic pathways and drug utilization during follow-up.
Results: The study was focused on 6603 women with HR+/HER2- mBC subtype, at least two prior systemic therapies for metastatic status or at least one endocrine-based therapy, at least one taxane prescription and at least one CDK4/6 inhibitor prescription and at least 12-months of data available before and after inclusion. Mean age was 59 years; the most common pre-existing conditions were hypertension (53.7%), distantly followed by chronic obstructive pulmonary disease, diabetes and cardiovascular disease. The analysis of treatment patterns during follow-up, which considered 3-month or 6-month gaps for identification of two different aspecific chemotherapies, showed that 97% (N = 236) had a subsequent line and 86% (N = 211) a further treatment during follow-up. The most common prior anticancer treatments, found in almost all patients, were endocrine therapy and CKD4/6i, with 66% patients receiving an aspecific chemotherapy.
Conclusion: This real-world analysis provides key insights into HR+/HER2- mBC in Italy, highlighting treatment patterns, rising diagnoses in younger women, and challenges in managing heavily pretreated patients. It emphasizes the need for further research on treatment sequencing, emerging therapies, and prior treatment duration to enhance clinical decision-making and patient care.
Keywords: administrative databases, cancer therapies, endocrine therapy, metastatic status
Introduction
According to the World Health Organization (WHO), 2.3 million women were diagnosed with breast cancer (BC) in 2022 with 670,000 deaths globally.1 The Globocan 2022 report by the International Agency for Research on Cancer (IARC) has estimated 2,296,840 new cases of BC worldwide in 2022, accounting for 11.5% of all new cancer cases globally. This makes BC the second most commonly diagnosed malignancy after lung cancer.2
Among all BC molecular subtypes, hormone receptor positive and human epidermal growth factor receptor 2 negative (HR+ HER2-) BC is by far the most frequent with an age-adjusted rate of 87.2 new cases per 100,000 women (data referred to 2016–2020 period).3 However, updated information on the epidemiology of metastatic BC (mBC) is scanty.4 Data from the real clinical practice in Italy reported an incidence of de novo HR+/HER2− mBC of 6.9 per 100,000 adult women in 2013.5
For several years, these patients with HR+/HER2− mBC have been conventionally treated with sequential single-agent chemotherapy, but with poor outcomes in many cases.6
However, recently updated WHO data revealed that age-standardized BC mortality in high-income countries dropped by 40% between the 1980s and 2020, suggesting that countries that have succeeded in improving BC with fundamental health policy interventions to deliver the more effective innovative treatments.1 Evidence has shown that combining endocrine therapy with cyclin-dependent kinase 4/6 inhibitors (CDK4/6i) can enhance treatment efficacy in HR+/HER2- mBC.7,8 Although first-line and second-line treatment with endocrine therapy combined with CDK4/6i has improved 5-year overall survival (OS) of patients with HR+/HER2- mBC,7,8 endocrine therapy resistance can still develop.9
A further therapeutic option for women with mBC coming from one to two prior lines of therapy is represented by the recent development of antibody-drug conjugates (ADCs), an innovative class of cancer therapies designed for targeted delivery of chemotherapy directly to cancer cells, thereby minimizing damage to healthy tissues. These agents appear to be a novel promising strategy to overwhelm resistance to chemotherapy or to receptor-based therapy.10 ADCs have shown promise in addressing treatment resistance in metastatic breast cancer through several mechanism. First, by delivering cytotoxic agents directly to cancer cells expressing specific antigens, ADCs can effectively kill cells that have become resistant to standard therapies. Second, some ADCs can release their cytotoxic payload to trigger effects on neighbouring tumor cells, including those lacking the target antigen, thereby overcoming heterogeneous antigen expression within tumors, a mechanism known as bystander effect. Moreover, ADCs can act by targeting resistant cells through novel cytotoxic agents that have unique mechanisms of action, potentially circumventing existing resistance pathways.10
The safety and effectiveness of cancer therapies are primarily investigated in randomized clinical trials (RCTs) which provide high-quality, controlled data from highly selected patient populations with strict inclusion and exclusion criteria. Thus, RCTs may not fully reflect the normal clinical practice, highlighting the need to integrate the results trials with real-world data from unselected patient populations, including those with comorbidities, older age, or other factors that might exclude them from RCTs.9,11,12
This analysis was primarily aimed at describing the population of women affected by HR+/HER2- mBC in the Italian real clinical practice, with a special focus on those highly pretreated (at least two prior systemic therapies for metastatic status and, in any setting, at least one endocrine-based therapy, at least one taxane and at least one CDK4/6i). This cohort of patients was specifically investigated for demographic and clinical variables, comorbidity profile, type and site of metastases and therapeutic pathways.
Materials and Methods
Data Source
This observational retrospective analysis was carried out using data collected from the administrative databases (namely beneficiaries, pharmaceuticals, hospitalizations, and outpatient specialist services databases) from a pool of Italian healthcare entities, geographically distributed throughout the country, corresponding to about 3 million health-assisted women. As previously reported by our research group,13 the administrative databases contain a large number of data on healthcare resources covered by the Italian National Health System (INHS). Specifically, data were extracted from the following databases: beneficiaries’ database for patients’ demographics; pharmaceutical database for reimbursed drug prescriptions, including the Anatomical-Therapeutic Chemical (ATC) code, and prescription date; hospitalization database for information on discharge diagnoses at any level classified according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) and date of diagnosis; outpatient diagnostic tests and specialist visits database, for data on the type and date of provisions of diagnostic tests, procedures and specialist visits.
The dataset used consists solely of anonymized data. Approval was obtained from the ethics committees of the involved LHUs: authorization of the Ethics Committee “Brindisi Comitato Indipendente di Etica Medica” (protocol number 48148, approval date 28/05/2021); authorization of the Ethics Committee “Berica Comitato Etico per le Sperimentazioni Cliniche (CESC) della Provincia di Vicenza” (protocol number 1627, approval date 28/10/2020); authorization of the Ethics Committee “Foggia Comitato etico interprovinciale Area I” (protocol number 63/CE/20, approval date 3/12/2020); authorization of the Ethics Committee “Comitato Etico delle Province di Chieti e Pescara” (protocol number 07, approval date 18/03/2021); authorization of the Ethics Committee “Roma 4 Comitato Etico Lazio 1” (protocol number 1079/CE Lazio 1, approval date 23/09/2020); authorization of the Ethics Committee “Roma 5 Comitato Etico Lazio 1” (protocol number 1166/CE Lazio 1, approval date 12/10/2020); authorization of the Ethics Committee “Roma 6 Comitato Etico Lazio 2” (protocol number 0216084/2020, approval date 16/12/2020); authorization of the Ethics Committee “Serenissima Comitato Etico per la Sperimentazione Clinica della provincia di Venezia e IRCCS S. Camillo” (28/07/2020); authorization of the Ethics Committee “Taranto Comitato Indipendente di Etica Medica” (protocol number 48144, approval date 28/05/2021); authorization of the Ethics Committee “Comitato Etico per le province di L’Aquila e Teramo” (protocol number 11, approval date 24/03/2021); authorization of the Ethics Committee “Umbria 2 Comitato Etico Regionale Umbria” (protocol number 19414/20/ON, approval date 16/09/2020); authorization of the Ethics Committee “Vercelli Comitato Etico Interaziendale A.O. SS. Antonio e Biagio e Cesare Arrigo – Alessandria” (protocol number 0008668, approval date 20/04/2021); authorization of the Ethics Committee Roma 3 “Lazio 2” (protocol number 0003146, approval date 09/01/2019); authorization of the Ethics Committee “Taranto Comitato Indipendente di Etica Medica” (protocol number 80673, approval date 24/10/2019).
Study Population
From 2017 to 2021, all the patients with HR+/HER2- mBC were identified by: (i) presence of a diagnosis for mBC AND presence of specific therapies for HR+ AND absence of HER2-targeted therapy (as previously described5,14,15); OR (ii) at least one prescription for CDK4/6i.
Table 1 details the criteria used to select the included population and to search within the databases diagnosis of BC, presence of metastases, and HR/HER2 status through the Anatomical Therapeutic Chemical (ATC) classification system for drugs and the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for hospital discharge diagnoses.
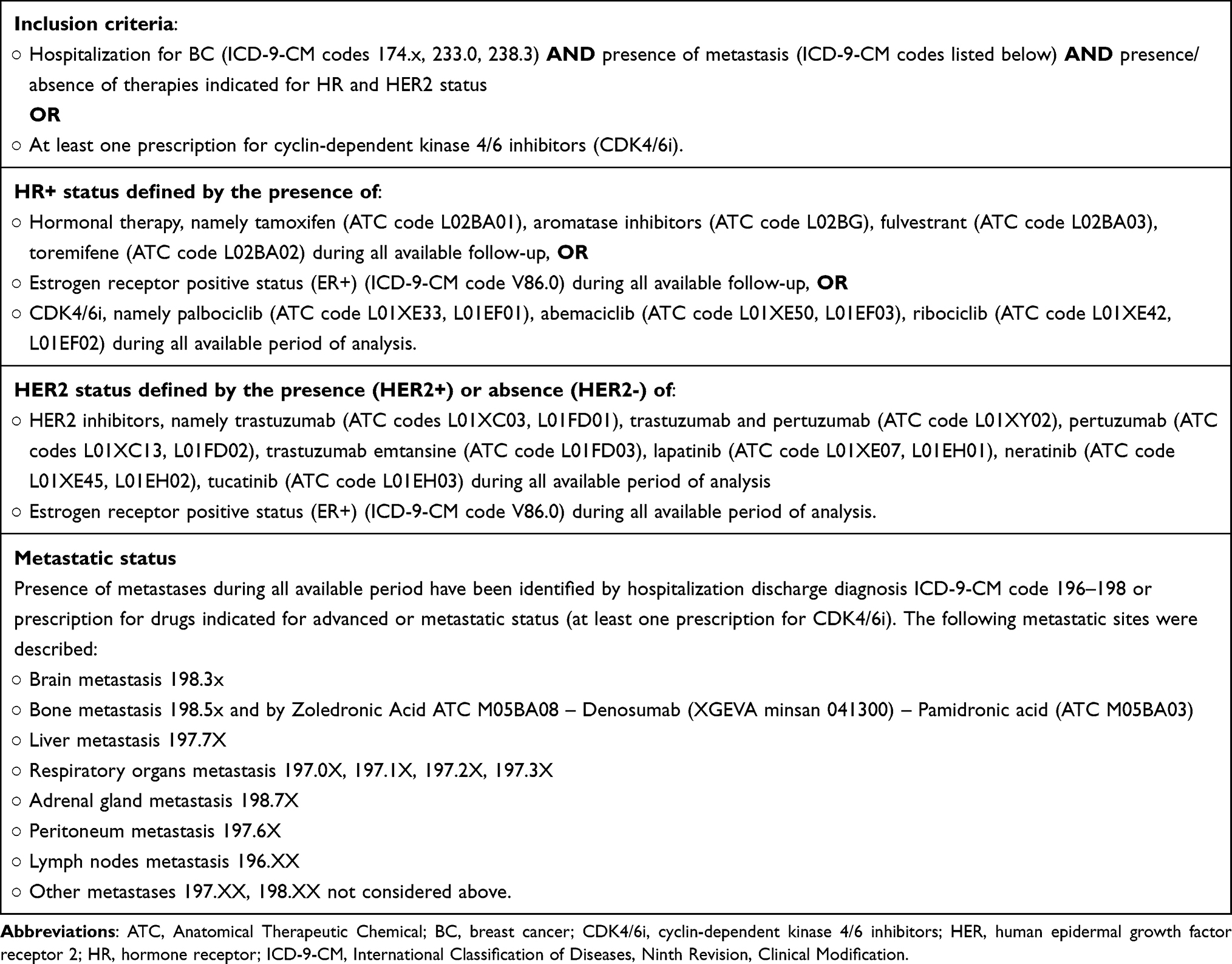 |
Table 1 Criteria and Codes Used to Identify the Included Population |
Patients with no continuous inclusion during the analysis period, patients aged <18 years, those with previous or concomitant other malignancies or synchronous and male subjects were excluded.
The analysis was then focused on women who complied one of the two following conditions: (A) at least two prior systemic therapies for metastatic status AND (B) considering any setting, at least one endocrine-based therapy AND at least one taxane AND at least one CDK4/6i.
The observational period was from January 2010 to December 2022. The time of the recognition of the condition A or B was considered as index-date. The included patients were investigated for all the available period before the index-date (characterization period, at least one year), and followed-up for all the available period after the index-date (follow-up period, at least one year).
For all the patients with at least one year of data availability before and after the index-date, age at index-date and distribution by age ranges (<65 years, 65–75 years, 76–80 years, and >80 years) were recorded. In the year preceding the index-date, patients’ general clinical status was assessed using the Charlson Comorbidity Index (CCI), a tool designed to predict long-term mortality summing the score of 19 weighted comorbidities.16 In this analysis, an adaptation of the CCI, not accounting for cancer, was applied. Patients’ history was also evaluated by collecting data on the most frequent drug prescriptions and causes of hospitalization in the 12-months prior to index-date. Finally, the site and the number of metastases were also investigated.
In the selected patients, therapeutic pathways and drug utilization (in terms of subsequent lines of therapy after index-date, duration of treatment, discontinuation) were analysed during all the available follow-up. Since within administrative databases aspecific chemotherapies is frequently detected in inpatients/outpatient settings, a gap of 3–6 months between consecutive aspecific chemotherapies records was used as a proxy for line identification, based on aspecific chemotherapies regimen duration.17,18 Lastly, the most common prior anticancer treatment class was also investigated.
Statistical Analysis
A descriptive statistical analysis was carried out for continuous variables, presented as mean with standard deviation (SD), and categorical variables, presented as frequencies and percentages. The results from subgroups including less than 4 patients were not disclosed for data privacy and reported as NI (not issuable). All the analyses were performed using STATA SE version 17.0.
Results
From a catchment area of 3,084,609 health-assisted women, 9754 with a diagnosis of mBC were selected from 2017 to 2021, of whom 6603 (67.7%) were identified with the HR+/HER2- mBC subtype. Among them, the women who had at least two prior systemic therapies for metastatic status or, in any setting, at least one endocrine-based therapy, at least one taxane and at least one CDK4/6i were 353 (5.3%).
Data projected on a national scale estimated 48,616 alive patients with HR+/HER2- mBC at 31/12/2021, of whom 1742 (3.6%) with the above mentioned treatment history of at least two prior systemic therapies for metastatic status or, in any setting, at least one endocrine-based therapy, at least one taxane and at least one CDK4/6i.
Finally, 244 with at least one year of data availability before and after the index-date (hereinafter referred as “selected cohort”) were investigated for demographics, clinical variables and therapeutic patterns.
The demographic and clinical characteristics of the selected cohort of HR+/HER2- mBC patients are reported in Table 2. The patients were aged on average 59 years, and the most of them (69.3%) below 65 years. The adapted CCI with the exclusion of cancer indicated a mild comorbidity profile, as most of the women analysed (151 out of 244, corresponding to 61.9%) had a CCI equal to 0. Hypertension was found in more than half of the patients (53.7%) and chronic obstructive pulmonary disease, diabetes and cardiovascular disease in 17.6%, 11.1%, and 4.5%, respectively.
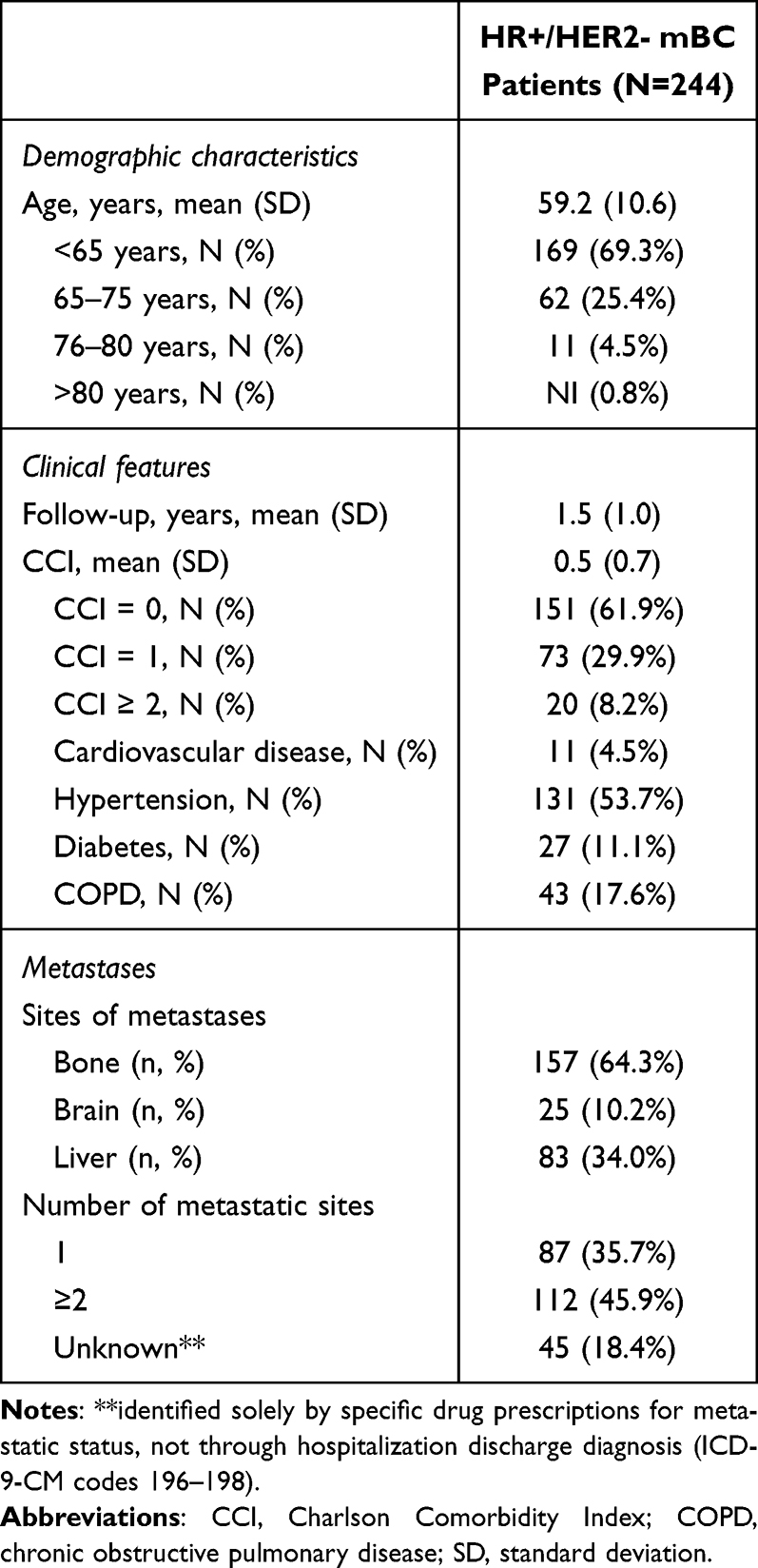 |
Table 2 Demographic and Clinical Characteristics of HR+/HER2- mBC Patients With at Least Two Prior Systemic Therapies for Metastatic Status or, in Any Setting, at Least One Endocrine-Based Therapy, at Least One Taxane and at Least One CDK4/6i |
Table 3 shows the most frequent treatments (second-level ATC code) during the year before the index-date. Endocrine and anticancer therapies were prescribed in most of the patients (91.4% and 83.2%, respectively), followed by drugs for acid-related disorders (78.7%), antibiotics (66.0%), vitamins (61.9%), and systemic corticosteroids (54.9%).
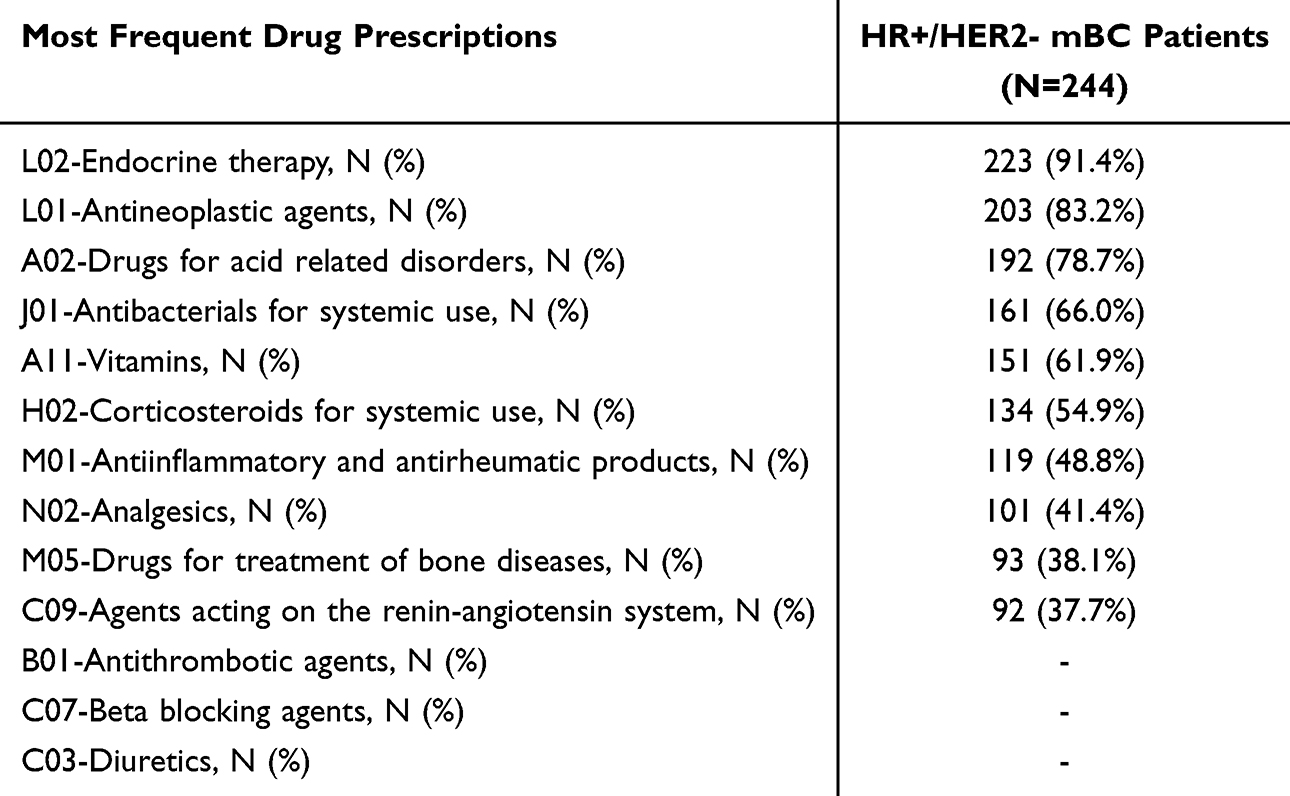 |
Table 3 Most Frequent Treatments in the year Prior Index-Date Among HR+/HER2- mBC Patients With at Least Two Prior Systemic Therapies for Metastatic Status or, in Any Setting, at Least One Endocrine-Based Therapy, at Least One Taxane and at Least One CDK4/6i |
The most frequent hospitalizations grouped by Major Diagnostic Category (MDC) in the selected cohort during the one-year period before the index-date are reported in Figure 1. The most common hospitalizations regard skin, subcutaneous tissue and breast cancer, found in 15.6% of the patients, followed by myeloproliferative diseases and disorders (poorly differentiated neoplasms) found in 13.1%.
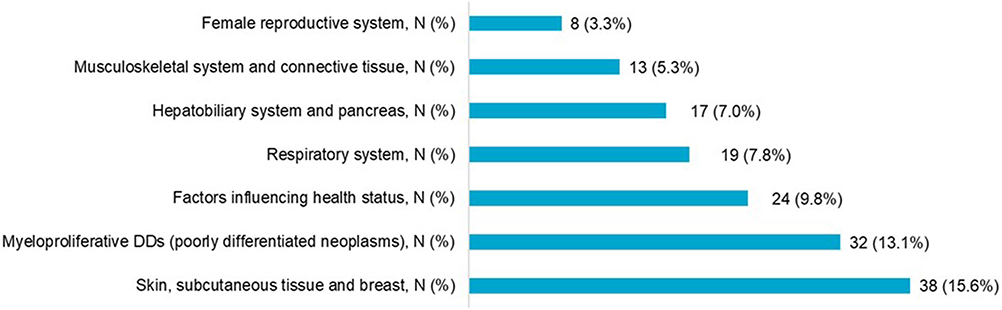 |
Figure 1 Most frequent hospitalizations in the year prior index-date among 244 hR+/HER2- mBC patients with at least two prior systemic therapies for metastatic status or, in any setting, at least one endocrine-based therapy, at least one taxane and at least one CDK4/6i. Abbreviation: DDs, diseases and disorders. |
The possible subsequent treatment patterns were evaluated after the index-date. Any differences due to the used 3-month or 6-month gap for identification of two different aspecific chemotherapy evaluation were considered and mentioned. With gaps of 3 and 6 months, among the 244 patients identified, 97% (N = 236) had a subsequent line and 86% (N = 211) a further treatment during all the available follow-up (Figure 2). Concerning the most common prior anticancer treatment classes, all patients had a previous treatment with endocrine therapy and CKD4/6i, while about 66% had an aspecific chemotherapy.
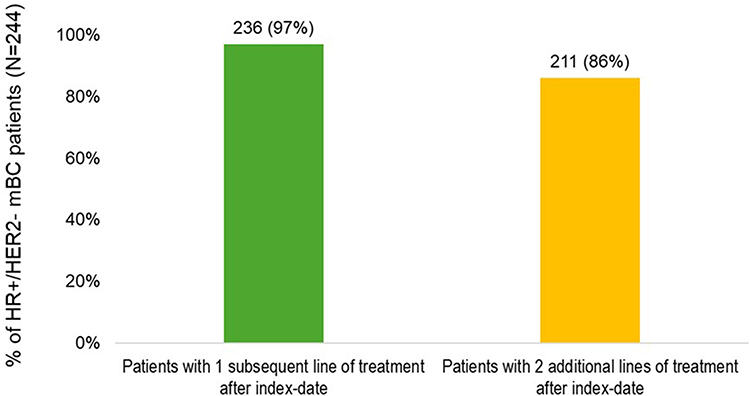 |
Figure 2 Proportion of patients with a subsequent line (green bar) and with a further treatment (yellow bar) during all the available follow-up (considering 3- and 6-month gaps), among 244 hR+/HER2- mBC patients with at least two prior systemic therapies for metastatic status or, in any setting, at least one endocrine-based therapy, at least one taxane and at least one CDK4/6i. |
Discussion and Conclusions
The present analysis was meant to investigate the current scenario of HR+/HER2- mBC in a setting of real clinical practice in Italy, focusing on the cohort of highly pretreated patients, who had received at least two prior systemic therapies for metastatic status or, in any setting, at least one endocrine-based therapy, at least one taxane and at least one CDK4/6i.
Among metastatic BC patients identified from 2017 to 2020, the percentage of HR+/HER2- subtype was 67.7% was consistent with published Italian and international evidence, reporting a range between 66.2% and 75%.19–22 These numbers were also in line with US data from the American Cancer Society’s biennial update of statistics on breast cancer, which estimated approximately 217,500 new cases of HR+/HER2- mBC in 2024.23
In the population included in the analysis, the mean age of patients (59 years) was in line with data from RCTs,9 registries24,25 statistics surveys,26 and real-world evidence studies,27 indicating how over the past few years, an increasing number of patients have been diagnosed with mBC at a younger age,25 in general younger than most of the other types of cancers.26 Although age-stratified analyses were beyond the purposes of the current study, it is worthwhile conducting additional investigations on younger patients (<40 years of age) to better clarify the impact of this age shift on mBC disease burden. The most common metastatic sites were bone, brain and liver, and this finding is also in agreement with data from Globocan 2020.2 Consistent with existing evidence, almost all patients in our population had received a previous treatment with endocrine therapy and CKD4/6i, and about two-thirds aspecific chemotherapy. Experience from RCTs has suggested that patients with HR+/HER2- mBC whose treatment options had been limited to sequential single-agent chemotherapy, are prone to develop endocrine resistance.9 Indeed, real-world data have recently suggested how, besides the number of lines of chemotherapy, their duration might also play a role in the therapeutic and clinical journey of patients with mBC.28,29 The duration of prior treatments significantly influences outcomes in subsequent therapies for mBC. A study analyzing 5363 patients found that longer durations of prior treatment were associated with decreased overall survival after initiating CDK4/6i. Specifically, compared to patients with no prior treatments, those with less than one year of prior treatment had a 30% increased hazard of death, those with one to less than three years had a 68% increase, and those with three or more years had a 55% increase. This underscores the importance of considering prior treatment duration in clinical decision-making.30
The main novelty of this study is represented by the intent to investigate the highly demanding clinical management of this specific population of mBC women who proceeded through several lines of therapy with different drug classes on a large population, with a valuable representativeness of the Italian population. Moreover, the support of real-world evidence has gained an increasing interest in oncology: the availability of a large amount of data from thousands of patients makes it possible to extrapolate and apply reliable information on unselected populations that reflect real clinical practice.31
These results should anyhow be interpreted considering some intrinsic limitations of administrative databases. At first, since HR+/HER2- mBC was identified using hospitalization codes or drug prescriptions as proxies, the patients who were never hospitalized, and those who did not receive a treatment specific for that setting or those participating in clinical trials where the drug under investigation is not recorded in the pharmaceutical administrative database were missed. Likewise, the CCI was also assessed using codes of drug prescription and hospitalisations, hence untreated/non-hospitalized comorbidities were not captured. More patients receiving medroxyprogesterone-acetate were missed, feasibly because low cost drugs are not routinely recorded, so they are not traceable in the pharmaceutical database. Another point to mention is that ibandronic acid was not included in proxy bone metastases because it did not have a specific indication for bone metastases. This choice was made to avoid misclassification with osteoporosis, only those agents identified via minsan code as those with the unique specific indication for bone metastases were considered. It should be specified that the treatment scenario has recently changed since the end of inclusion, considering the recent entry into the clinical practice of novel therapies32 which were not included in the present analysis. Besides, it should be specified that the current analysis relies on data from a sample of the Italian population, which may limit the generalizability of our results on a larger scale. Lastly, for some small subgroups of less than 3 patients, results could not be disclosed for privacy reasons, and this might limit the robustness of subgroup analysis. Further studies on a larger catchment area are necessary to overcome this flaw and also to apply inferential rather than descriptive statistics.
In conclusion, these results generated from the real clinical practice provide valuable insights into the clinical characteristics, treatment patterns, and therapeutic trajectories of HR+/HER2- mBC patients in Italy, particularly those who have undergone multiple lines of therapy. Our findings align with existing literature, reinforcing the prevalence of this subtype and highlighting the increasing diagnosis of mBC in younger women. The analysis underscores the complexity of managing heavily pretreated patients and the need for further research on optimizing treatment sequencing, particularly in the post-CDK4/6i setting.
Future research should focus on expanding the study population, integrating emerging therapies, and exploring the impact of prior treatment duration on long-term outcomes. Such investigations will be crucial for refining clinical decision-making and improving patient care in HR+/HER2- mBC management.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Breast cancer. Available at: https://www.who.int/news-room/fact-sheets/detail/breast-cancer?utm.
2. Globocan 2022 Italy Available from: https://gco.iarc.who.int/media/globocan/factsheets/cancers/20-breast-fact-sheet.pdf.
3. Cancer stat facts: female breast cancer subtypes. Available at: https://seer.cancer.gov/statfacts/html/breast-subtypes.html.
4. Mariotto AB, Etzioni R, Hurlbert M, Penberthy L, Mayer M. Estimation of the number of women living with metastatic breast cancer in the United States. Cancer Epidemiol Biomarkers Prev. 2017;26(6):809–815. doi:10.1158/1055-9965.EPI-16-0889
5. Piccinni C, Dondi L, Ronconi G, et al. HR+/HER2- metastatic breast cancer: epidemiology, prescription patterns, healthcare resource utilisation and costs from a large Italian real-world database. Clin Drug Investig. 2019;39(10):945–951. doi:10.1007/s40261-019-00822-4
6. Rugo HS, Rumble RB, Macrae E, et al. Endocrine therapy for hormone receptor-positive metastatic breast cancer: American society of clinical oncology guideline. J Clin Oncol. 2016;34(25):3069–3103. doi:10.1200/JCO.2016.67.1487
7. Finn RS, Boer K, Bondarenko I, et al. Overall survival results from the randomized Phase 2 study of palbociclib in combination with letrozole versus letrozole alone for first-line treatment of ER+/HER2- advanced breast cancer (PALOMA-1, TRIO-18). Breast Cancer Res Treat. 2020;183(2):419–428. doi:10.1007/s10549-020-05755-7
8. Slamon DJ, Neven P, Chia S, et al. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. N Engl J Med. 2020;382(6):514–524. doi:10.1056/NEJMoa1911149
9. Rugo HS, Bardia A, Marmé F, et al. Sacituzumab govitecan in hormone receptor-positive/human epidermal growth factor receptor 2-negative metastatic breast cancer. J Clin Oncol. 2022;40(29):3365–3376. doi:10.1200/JCO.22.01002
10. Santa-Maria CA, Wolff AC. Antibody-drug conjugates in breast cancer: searching for magic bullets. J Clin Oncol. 2023;41(4):732–735. doi:10.1200/JCO.22.02217
11. Azoulay L. Rationale, strengths, and limitations of real-world evidence in oncology: a Canadian review and perspective. Oncologist. 2022;27(9):e731–e738. doi:10.1093/oncolo/oyac114
12. Modi S, Jacot W, Yamashita T, et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
13. Nava FA, Mangia A, Riglietta M, et al. Analysis of patients’ characteristics and treatment profile of people who use drugs (PWUDs) with and without a co-diagnosis of viral hepatitis C: a real-world retrospective Italian analysis. Ther Clin Risk Manag. 2023;19:645–656. doi:10.2147/TCRM.S409134
14. Nordstrom BL, Whyte JL, Stolar M, Mercaldi C, Kallich JD. Identification of metastatic cancer in claims data. Pharmacoepidemiol Drug Saf. 2012;21 Suppl 2(S2):21–28. doi:10.1002/pds.3247
15. Nordstrom BL, Simeone JC, Malley KG, et al. Validation of claims algorithms for progression to metastatic cancer in patients with breast, non-small cell lung, and colorectal cancer. Front Oncol. 2016;6:18. doi:10.3389/fonc.2016.00018
16. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
17. Linee Guida AIOM 2018 Neoplasie della mammella. Available at: https://www.aiom.it/wp-content/uploads/2018/11/2018_LG_AIOM_Mammella.pdf. Italian.
18. Seah DS, Luis IV, Macrae E, et al. Use and duration of chemotherapy in patients with metastatic breast cancer according to tumor subtype and line of therapy. J Natl Compr Canc Netw. 2014;12(1):71–80. doi:10.6004/jnccn.2014.0008
19. Airtum Working Group. Tagliabue G, Fabiano S, Contiero P, et al. Molecular subtypes, metastatic pattern and patient age in breast cancer: an analysis of Italian Network of Cancer Registries (AIRTUM) data. J Clin Med. 2021;10(24):5873. doi:10.3390/jcm10245873
20. Crocetti E, Ravaioli A, Giuliani O, et al. Female breast cancer subtypes in the Romagna Unit of the Emilia-Romagna cancer registry, and estimated incident cases by subtypes and age in Italy in 2020. J Cancer Res Clin Oncol. 2023;149(10):7299–7304. doi:10.1007/s00432-023-04593-6
21. Simon J, Chaix M, Billa O, et al. Survival in patients with HR+/HER2- metastatic breast cancer treated with initial endocrine therapy versus initial chemotherapy. A French population-based study. Br J Cancer. 2020;123(7):1071–1077. doi:10.1038/s41416-020-0979-3
22. Surveillance, epidemiology, and end results (SEER) program - cancer stat facts: female breast cancer subtypes. Available at: https://seer.cancer.gov/statfacts/html/breast-subtypes.html.
23. Giaquinto AN, Sung H, Newman LA, et al. Breast cancer statistics 2024. CA Cancer J Clin. 2024;74(6):477–495. doi:10.3322/caac.21863
24. Mangone L, Bisceglia I, Michiara M, et al. Breast cancer in Italy: stage and region distribution. Breast Cancer. 2022;14:125–131. doi:10.2147/BCTT.S360244
25. DeSantis CE, Fedewa SA, Goding Sauer A, Kramer JL, Smith RA, Jemal A. Breast cancer statistics, 2015: convergence of incidence rates between black and white women. CA Cancer J Clin. 2016;66(1):31–42. doi:10.3322/caac.21320
26. Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66(4):271–289. doi:10.3322/caac.21349
27. Kaufman PA, Neuberger E, Schwartz NRM, et al. Real-world patient characteristics, treatment patterns, and clinical outcomes associated with tucatinib therapy in HER2-positive metastatic breast cancer. Front Oncol. 2023;13:1264861. doi:10.3389/fonc.2023.1264861
28. Wang R, Zhu Y, Liu X, Liao X, He J, Niu L. The Clinicopathological features and survival outcomes of patients with different metastatic sites in stage IV breast cancer. BMC Cancer. 2019;19(1):1091. doi:10.1186/s12885-019-6311-z
29. Coe F, Misra V, McCabe Y, et al. Average duration of prior treatment lines predicts clinical benefit to eribulin chemotherapy in patients with metastatic breast cancer. Breast Cancer Res Treat. 2022;191(3):535–543. doi:10.1007/s10549-021-06438-7
30. Franks J, Caston NE, Elkhanany A, Gerke T, Azuero A, Rocque GB. Effect of prior treatments on post-CDK 4/6 inhibitor survival in hormone receptor-positive breast cancer. Breast Cancer Res Treat. 2023;197(3):673–681. doi:10.1007/s10549-022-06823-w
31. Mahajan R. Real world data: additional source for making clinical decisions. Int J Appl Basic Med Res. 2015;5(2):82. doi:10.4103/2229-516X.157148
32. AIFA (Italian Medicines Agency). DETERMINA 15 dicembre 2023 Regime di rimborsabilià e prezzo a seguito di nuove indicazioni terapeutiche del medicinale per uso umano «Enhertu». (Determina n. 760/2023). Available at: https://www.aifa.gov.it/documents/20142/847786/Determina_ENHERTU_GU296.pdf. Italian.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.