Back to Journals » Journal of Blood Medicine » Volume 15
Real-World Evidence of Relapsed/Refractory Mantle Cell Lymphoma Patients and Treatments: A Systematic Review
Authors Sancho JM ![]() , Sorigué M, Rubio-Azpeitia E
, Sorigué M, Rubio-Azpeitia E ![]()
Received 13 February 2024
Accepted for publication 18 May 2024
Published 25 May 2024 Volume 2024:15 Pages 239—254
DOI https://doi.org/10.2147/JBM.S463946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Juan-Manuel Sancho,1 Marc Sorigué,1 Eva Rubio-Azpeitia2
1Clinical Hematology Department, ICO-IJC-Hospital Germans Trias I Pujol. Badalona, Universitat Autònoma de Barcelona, Barcelona, Spain; 2Medical Department-Hematology, Janssen-Cilag, S.A, Madrid, Spain
Correspondence: Eva Rubio-Azpeitia, Johnson and Johnson SA, Medical Affairs Hematology, Paseo de las Doce Estrellas, 5-7, Madrid, Spain, Email [email protected]
Introduction: Mantle cell lymphoma (MCL) is an incurable disease with an aggressive clinical course, and most patients eventually relapse after chemotherapy. Targeted therapies developed for relapsed/refractory MCL have been approved based on clinical trial data. However, real-world setting data are scarce and scattered.
Areas Covered: This systematic review aimed to collect, synthesize, and describe the characteristics and treatment outcomes of patients with relapsed/refractory MCL after receiving a second or subsequent line of therapy in the real-world setting.
Expert Opinion: R/R MCL is clinically and biologically heterogeneous and still represents a therapeutic challenge, with high-risk and early relapsed patients remaining an unmet medical need. This systematic review is limited by the quality of the available data and the difficulty of comparing outcomes in R/R MCL due to the heterogeneity of the disease, but the results suggest that covalent BTKis should be positioned as second-line therapy, followed by CAR T-cells in BTK-i-relapsed patients. Chemo-free and combination therapies with established chemoimmunotherapy backbones in the relapsed and front-line settings have been recently developed, and front-line options are being improved to move targeted and cellular therapies to earlier lines, including front-line therapy, in elderly and younger fit patients. In the upcoming years, many new targeted agents will play an important role and will be incorporated to the routine practice as their sequence, and outcomes in unselected patients are determined.
Keywords: CAR-T cells, ibrutinib, mantle cell lymphoma, real-world evidence, relapsed/refractory mantle cell lymphoma (R/R MCL), treatment efficacy
Introduction
Mantle cell lymphoma (MCL) is an infrequent subtype of non-Hodgkin lymphoma (NHL) that accounts for approximately 5 to 7% of lymphoid malignancies in Western Europe,1 but its incidence seems to be increasing over time.2 It is an incurable disease with a median age at diagnosis of 68 years,3 more common in men than in women (ratio around 3:1).1,2
Although two types of clinically indolent MCL variants have been recognized —leukemic non-nodal MCL and in situ mantle cell neoplasia— most patients with MCL present with an aggressive clinical course.1,4 Moreover, MCL patients usually experience multiple relapses, and survival outcomes worsen with increasing lines of therapy.5 Some clinical and pathological features have been identified as prognostic factors of MCL, such as the MCL International Prognostic Index (MIPI), the Ki-67 index, aberrations in the TP53 tumor suppression gene (eg, TP53 mutations and del17p), presence of blastoid or pleomorphic histologic variants, and an early progression of disease after first-line therapy, especially within the first one or two years.6
Historically, several chemotherapy-based strategies have been used for MCL depending on the patient’s age, functional status, and number of previous lines of therapy, but most patients eventually relapse.1 In the last few years, several targeted treatment approaches have been developed for relapsed/refractory MCL (R/R MCL), including Bruton’s tyrosine kinase (BTK) inhibitors, B-cell lymphoma 2 (BCL-2) inhibitors, lenalidomide and bortezomib-based approaches, m-TOR inhibitors, and chimeric antigen receptor (CAR) T-cell therapy.6 Of those, the first–in–class BTK inhibitor ibrutinib has been positioned as the standard of care in the second line of therapy for MCL, based on the data from a pooled analysis of three clinical trials of R/R MCL patients treated with ibrutinib.7
The recommendations of treatment guidelines for R/R MCL are usually based on clinical trial data.1 Nevertheless, it is considered useful to validate the efficacy and safety of treatments in real-world studies to adopt them in routine clinical practice. In this regard, the real-world evidence currently available on R/R MCL treatments is scarce and scattered,8–14 and it is often difficult to compare due to the diversity of the approaches and the patients’ characteristics. Therefore, this systematic review aimed to collect, synthesize, and describe the characteristics and treatment outcomes of patients with R/R MCL after receiving a second or subsequent line of therapy in the real-world setting.
Materials and Methods
A systematic literature search was performed and reported in compliance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement, a guideline for standard reporting of systematic literature reviews.15
Eligibility Criteria
Real-world studies including patients with confirmed R/R MCL, written in English, published between 2010 and 2022, and indexed in PubMed or corresponding to 2021 congress publications of the American Society of Clinical Oncology (ASCO), the American Society of Hematology (ASH), the European Hematology Association (EHA), or the International Conference on Malignant Lymphoma (ICML) were eligible for inclusion. Conversely, clinical trials, case studies, or case series of <10 patients (excepting those considered relevant to mention in this review due to their uniqueness), and publications not reporting original data (eg, letters, editorials, comments, or systematic reviews) were excluded from the study. Other exclusion criteria were patients naïve to MCL treatment, outdated treatment regimens, and studies not reporting outcomes regarding survival or treatment response. Moreover, we excluded studies assessing transplantation strategies, given that they are mostly consolidation therapies with outcomes depending on previous rescue treatments, precluding direct comparisons.
Information Sources and Search Strategy
The literature search was performed on 15 May 2022 using the MEDLINE database through PubMed and websites with relevant conference materials on the subject —ie, the proceedings of the biennial International Conference on Malignant Lymphoma (ICML)16 and the annual meetings of the American Society of Hematology (ASH),17 the American Society of Clinical Oncology (ASCO),18 and the European Hematology Association (EHA).19
The search strategy in MEDLINE was as follows: (“relapsed” AND/OR “refractory”) AND “mantle cell lymphoma” AND (“retrospective” OR “real life” OR “real world” OR “case report”). In addition, for the manual search of ICML, ASH, ASCO, and EHA conference proceedings, the keywords “relapsed”, “refractory”, mantle cell lymphoma, “real world”, “retrospective”, “real life”, and “case series” were used.
In order to cover the most relevant pharmacological strategies for R/R MCL in current daily clinical practice, the search was limited to articles written in English, with full text available, published between 2010 and 2022. Furthermore, if the most relevant results presented to international congresses before 2021 would have already been published as journal articles, the abstracts of the proceedings were manually searched only for studies published since 2021.
Study Selection, Data Collection, and Data Items
Two reviewers independently screened all titles/abstracts and the full text of the retrieved publications potentially relevant for inclusion. Any disagreements were resolved by consulting with a third author. Similarly, the data were independently collected by two reviewers in predefined table disagreements, if any, were resolved by discussion with a third author.
The data collected related to the study included the first author, the year of publication, the treatment, and the sample size. Data regarding the baseline characteristics of study patients included age, gender, Eastern Cooperative Oncology Group (ECOG) score, stage of the disease according to the Ann-Arbor classification, number of previous lines of therapy, previous autologous or allogeneic stem cell transplantation (auto-SCT or allo-SCT, respectively), refractoriness to previous lines of therapy, progression of disease within 24 months (POD24), MIPI or simplified MIPI (sMIPI), Ki-67 index, TP53 aberrations, and presence of aggressive histologic variants (ie, blastoid or pleomorphic MCL). Clinical outcomes related to treatment efficacy were as follows: progression-free survival (PFS), overall survival (OS), overall response rate (ORR), complete response (CR), and follow-up.
Risk of Bias Assessment
The risk of bias of the included studies was assessed by two reviewers using the Joanna Briggs Institute (JBI) critical appraisal tool for case series.20 Any discrepancies were resolved by discussion with a third author.
Data Synthesis and Analyses
Data were presented as a narrative synthesis of the available data reported for each retrieved treatment regimen.
Results
A total of 300 publications were identified using the described search strategies. After removing all duplicates and excluding studies that did not meet the inclusion criteria, a total of 25 journal articles —18 original articles,8–11,14,21–33 3 letters to the editor,34–36 3 short reports,13,37,38 and 1 case report39 and 5 conference publications40–44 were included in the systematic review. All the 30 studies allowed the data collection of 37 treatment regimens for R/R MCL patients. Of them, 15 were based on BTK inhibitors, 14 on chemotherapy or immunochemotherapy, and 8 on other strategies. Table 1 summarizes the general characteristics of the treatment regimens and patients included in the systematic review.
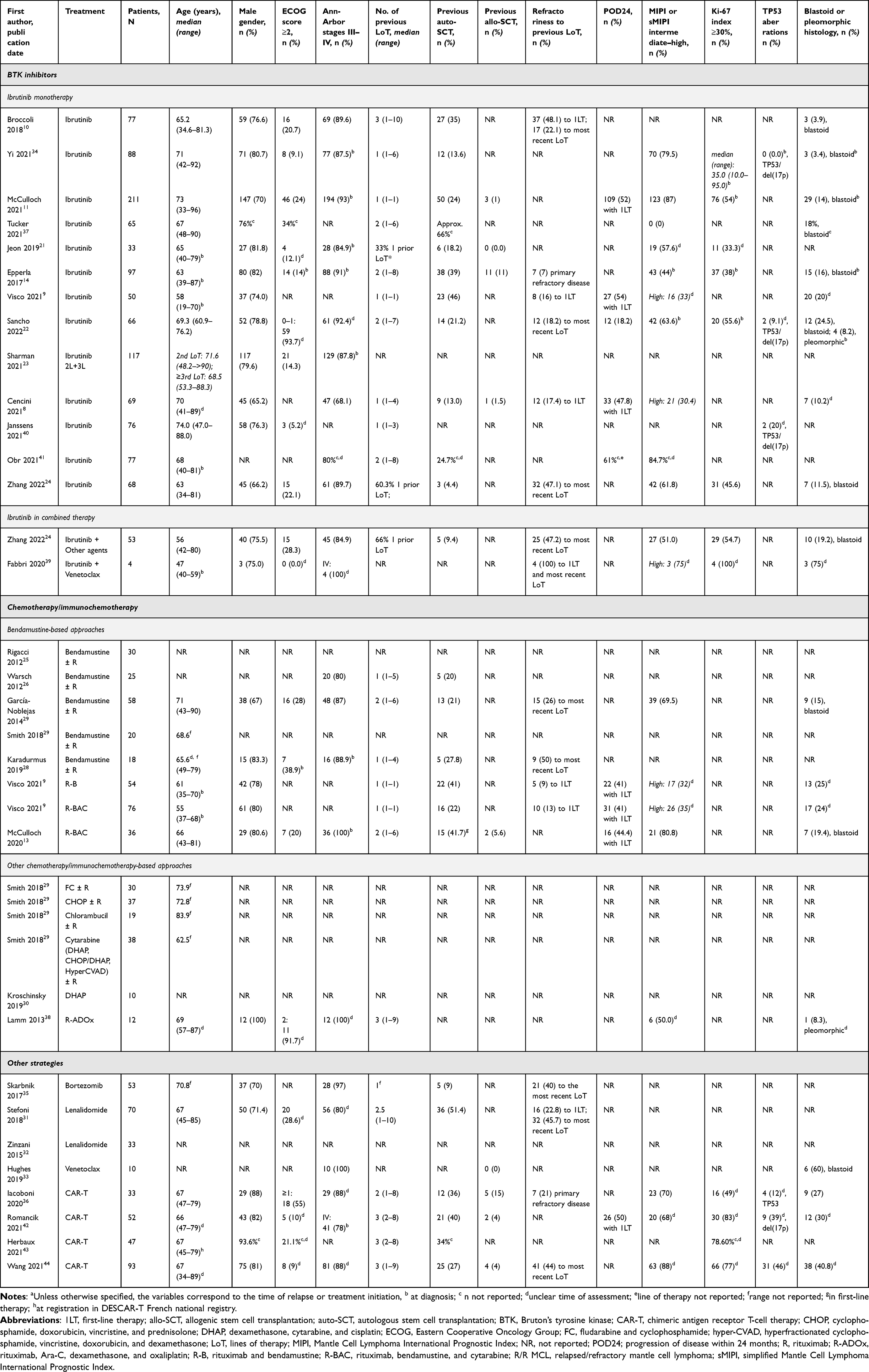 |
Table 1 General Characteristics of the Assessments and Patients Included in the Systematic Review According to the Type of R/R MCL Treatmenta |
BTK Inhibitor Regimens
All studies on BTK inhibitors analyzed the use of ibrutinib, either as monotherapy (n = 13 treatment regimens)8–11,14,21–24,34,37,40,41 or combined (n = 2).24,39
Ibrutinib Monotherapy
The treatment regimens based on ibrutinib monotherapy included from 33 to 211 patients (n = 12), mostly males (65% to 82%, n = 12), with a median age at treatment between 65 and 74 years (n = 8) (Table 1). The percentages of patients with an ECOG score ≥2 and a III–IV stage R/R-MCL according to the Ann-Arbor classification ranged from 5.2% to 34% (n = 9) and from 68.1% to 93% (n = 10), respectively. The median number of previous lines of therapy varied from 1 to 3 (n = 10), and the proportion of patients with a previous auto-SCT was between 13% and 66% (n = 11), and between 0% and 11% (n = 4), for allo-SCTs. Regarding response to previous treatments, between 16% and 48.1% of the patients were refractory to first-line therapy (n = 3) and between 18.2% and 47.1% were refractory to the most recent treatment line (n = 3); 47.8% to 54% of the patients were POD24 regarding their front-line therapy (n = 3). Additionally, the percentage of patients with an intermediate-high MIPI/sMIPI and a Ki-67 index ≥30% ranged between 44% and 87% (n = 7), and between 33.3% and 55.6% (n = 5), respectively. The proportion of patients presenting with high-risk blastoid or pleomorphic histology differed considerably among studies (from 3.4% to 32.6%, n = 9), with only three studies reporting TP53 aberrations, which ranged from 0 to 20%.
The efficacy outcomes of patients treated with ibrutinib alone were also quite variable and included a median PFS ranging from 7.9 to 30.8 months (n = 13), a median OS from 12.4 to 38 months (n = 12), an ORR from 36.4% to 95.9% (n = 10), and a CR from 15% to 39.5% (n = 9), with median follow-ups ranging from 12.6 to 60 months (Table 2).
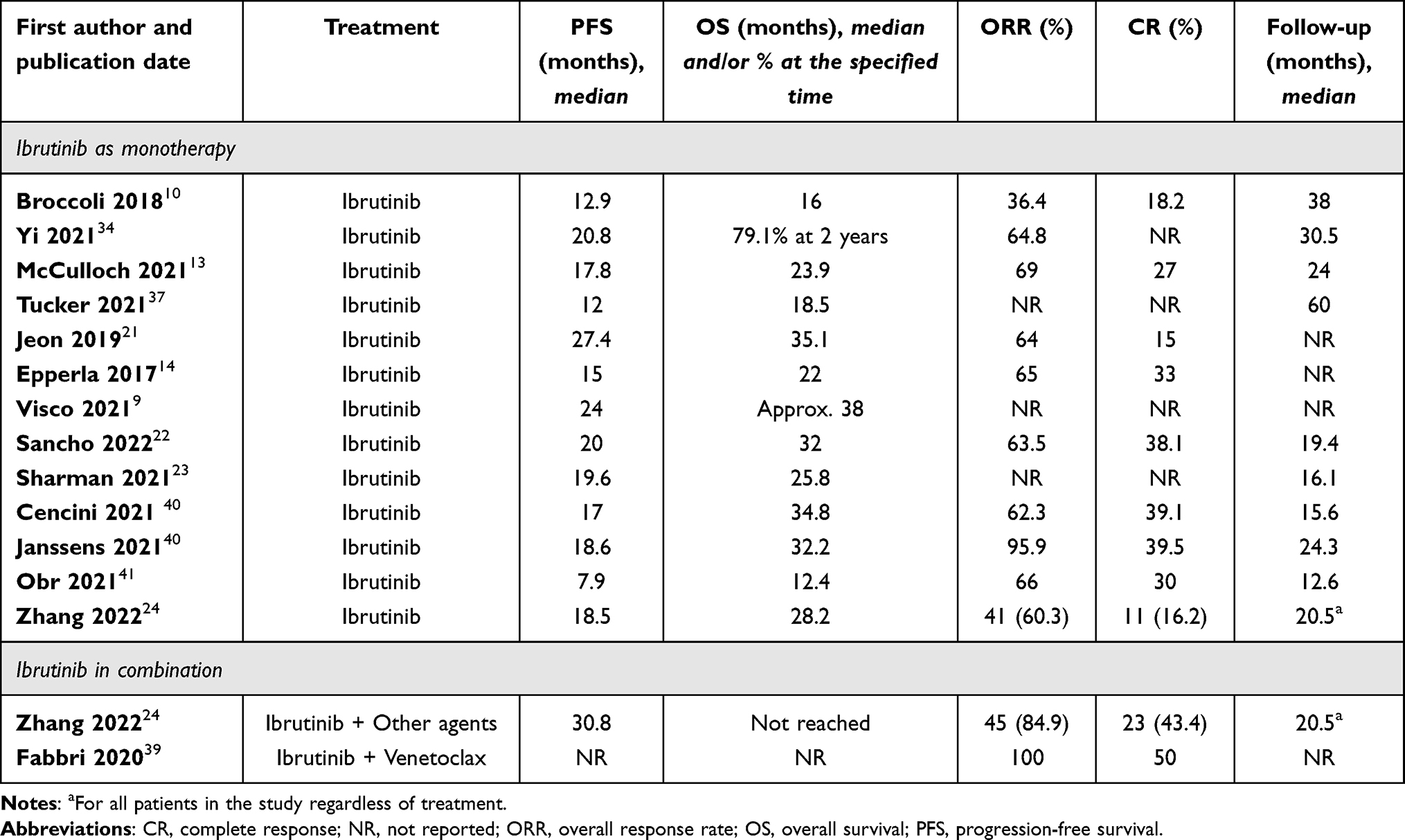 |
Table 2 Effectiveness Outcomes of Patients Treated with Bruton’s Tyrosine Kinase (BTK) Inhibitors |
Ibrutinib in Combination
Two studies analyzed the efficacy of ibrutinib in combination with other agents. The first one reported the outcomes of ibrutinib combined with several other agents (rituximab, lenalidomide, bortezomib, and/or bendamustine) in 53 patients (75.5% males, median age of 56 years),24 of which 28.3%, 84.9%, 51.0%, and 54.7% had an ECOG score ≥2, a III–IV stage R/R-MCL, an intermediate-high sMIPI, and a Ki-67 index ≥30%, respectively. In addition, the percentages of patients with a previous auto-SCT, refractoriness to the most recent line of therapy, and blastoid histology were 9.4%, 47.2%, and 19.2%. The second study described the cases of four patients treated with ibrutinib and venetoclax, who were mostly males with a median age of 47 years at diagnosis.39 All of them had previously been treated with rituximab, high dose cytarabine, and anthracycline and presented an ECOG score between 0 and 1, as well as an IV stage MCL. Three patients out of four presented with three high risk features: high MIPI value, Ki-67 index >30%, and blastoid or pleomorphic histology (Table 1).
The survival outcomes of both studies are also shown in Table 2. The treatment strategies reported in the first study resulted in a median PFS of 30.8 months, an ORR of 84.9%, and a CR of 43.4%, with a median follow-up of 20.5 months (for the overall study population).24 Moreover, the efficacy of ibrutinib plus venetoclax in the second study was reported in terms of ORR and CR, which were 100% and 50%, respectively.39
Chemotherapy/Immunochemotherapy-Based Strategies
The strategies based on chemotherapy/immunochemotherapy included eight assessments of bendamustine regimens reported in seven studies;9,13,25–29 one of fludarabine and cyclophosphamide (FC) regimens alone or combined with rituximab;29 one of cyclophosphamide, doxorubicin, vincristine, and prednisolone (CHOP) regimens alone or combined with rituximab;29 one of chlorambucil regimens alone or combined with rituximab,29 two of cytarabine-based regimens;29,30 and one of rituximab, Ara-C, dexamethasone, and oxaliplatin (R-ADOx) regimens38 (Table 1).
Bendamustine-Based Strategies
Seven studies assessed eight bendamustine-based approaches, five with bendamustine either with or without rituximab (bendamustine ± R);25–29 one with bendamustine and rituximab (B–R);9 and two with rituximab, bendamustine, and cytarabine (R-BAC).9,13 These treatment regimens included between 18 and 76 patients (n = 8), predominantly males (between 67% and 83.3%, n = 5), with median ages at treatment initiation varying from 66 to 71 years (n = 3). The percentages of patients with an ECOG score ≥2 and a III–IV Ann-Arbor stage ranged from 20% to 38.9% (n = 3), and from 80% to 100% (n = 4), respectively. The patients had received a median of one to three previous lines of therapy (n = 6), and 20% to 41.7% of them, a previous auto-SCT (n = 6). As for response to previous lines of therapy, between 9% and 13% of the patients were refractory to first-line therapy (n = 2), whereas 26% to 50% of them were refractory to the most recent therapy/chemotherapy (n = 2). In addition, 41% to 44.4% of the individuals were POD24 to their first-line therapy (n = 3). The proportion of patients presenting with an intermediate-high MIPI/sMIPI and a blastoid or pleomorphic MCL ranged from 69.5% to 80.8% (n = 2), and from 15% to 25% (n = 4), respectively (Table 1).
Patients treated with bendamustine-based approaches presented considerably variable survival outcomes, with a median PFS ranging from 10.1 to 25.9 months (n = 5) and a median OS from 12.5 to 43 months (n = 4). The ORR and CR ranged from 70% to 86% (n = 6), and from 40% to 61.1% (n = 5), respectively (Table 3). Median follow-ups ranged from 10 to 22 months.
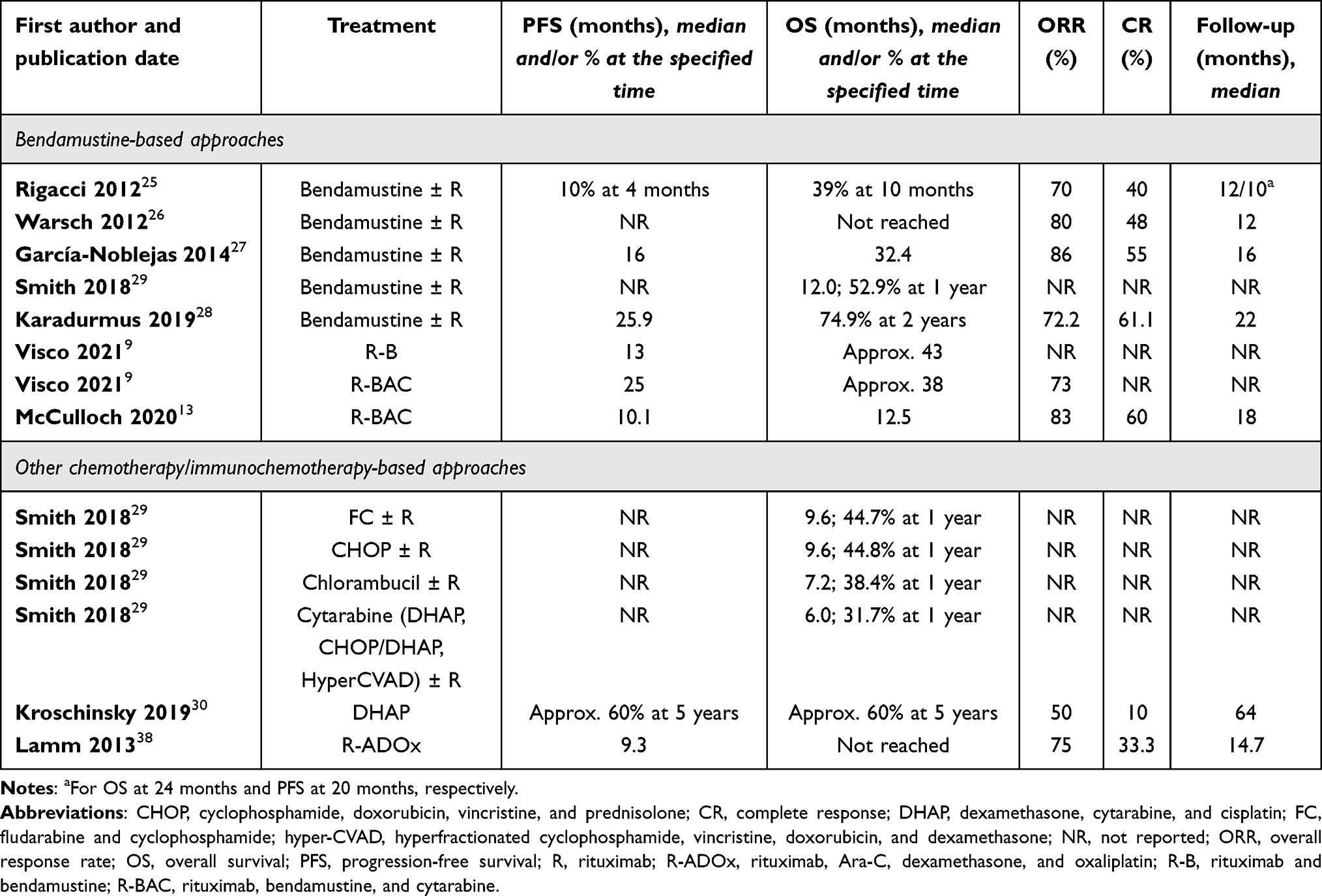 |
Table 3 Effectiveness Outcomes of Patients Treated with Chemotherapy or Immunochemotherapy |
Other Chemotherapy/Immunochemotherapy-Based Approaches
The general characteristics of the remaining chemotherapy/immunotherapy-based treatment regimens can also be seen in Table 1, whereas their corresponding outcomes are summarized in Table 3. The study of Smith et al included the assessments of FC, CHOP, chlorambucil, and cytarabine-based regimens.29 The analysis of FC was performed on 30 patients with a median age at treatment onset of 73.9 years, resulting in a median OS of 9.6 months. Similarly, the assessment of CHOP included 37 patients with a median age at treatment initiation of 72.8 years; their median OS was 9.6 months as well. In contrast, the assessment on chlorambucil included a lower number of patients (n = 19), who were older than those described before (median of 83.9 years) and reported a shorter survival (median OS of 7.2 months). Moreover, the analysis of cytarabine-based regimens —DHAP, CHOP/DHAP, and HyperCVAD, alone or combined with rituximab— was performed among 38 younger patients (median age of 62.5 years) and yielded a median OS of 6.0 months. The other analysis of a cytarabine regimen (specifically, a modified DHAP regimen) included 10 patients and reported a 5-year PFS and OS of approximately 60%, along with an ORR of 50%, and a CR of 10%, with a median follow-up of 64 months.30 As for the assessment of R-ADOx regimens, it included 12 male patients with a median age of 69 years and a median of 3 previous lines of therapy. Most patients (91.7%) had an ECOG=2 and, all of them, an III–IV stage MCL, whereas only one (8.3%) presented with an aggressive MCL histology (pleomorphic). The efficacy outcomes of this approach included a median PFS of 9.3 months, an ORR of 75%, and a CR of 33.3%, with a median follow-up of 14.7 months.38
Other MCL Treatments
Besides the treatment regimens based on BTK inhibitors and chemotherapy/immunotherapy, we found other R/R MCL treatment approaches, including treatment regimens based on bortezomib (n = 1),35 lenalidomide (n = 2),31,32 venetoclax (n = 1),33 and CAR T-cell therapies (n = 4).36,42–44
Bortezomib
The study of the treatment regimen based on bortezomib included 53 patients (70% males) with a median age at treatment initiation of 70.8 years, with almost all of those with available data (97%) being at stages III–IV. Patients had received a median of 1 previous line of therapy, and 9% of them had undergone a previous auto-SCT. In addition, 40% of the patients were refractory to the most recent treatment (Table 1). This study reported a median PFS of 4.7 months and a median OS of 11.3 months, with a median follow-up of 5.3 months35 (Table 4).
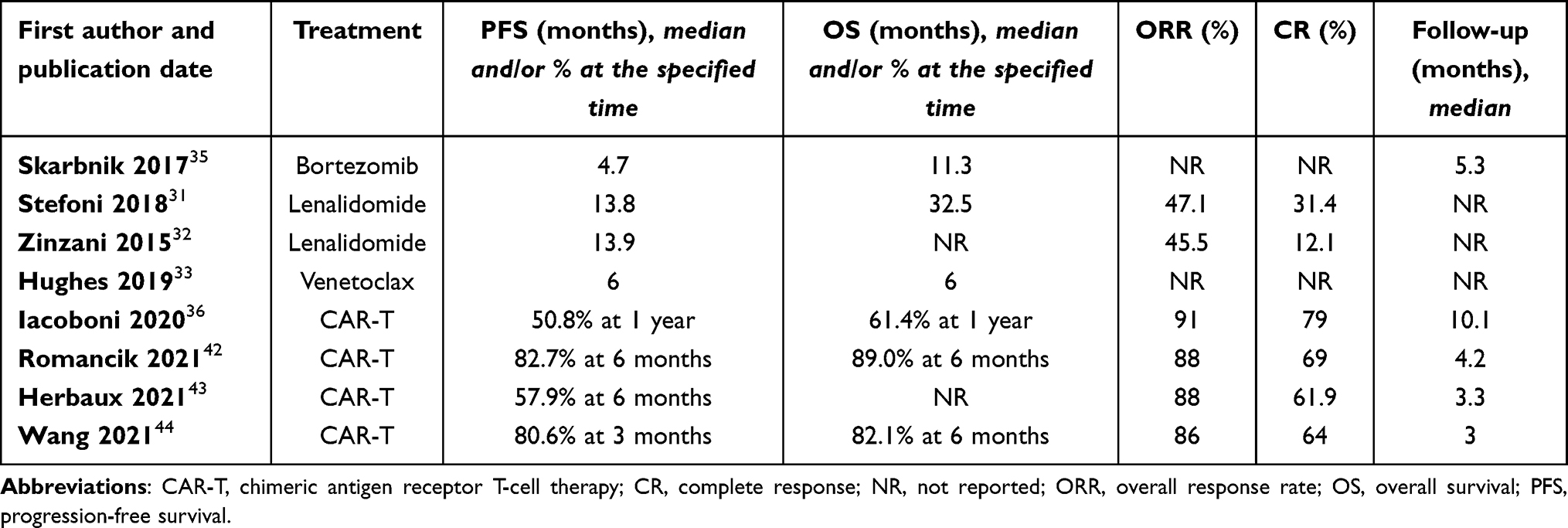 |
Table 4 Effectiveness Outcomes of Patients Treated with Other Strategies |
Lenalidomide
The study by Stefoni et al included 70 patients (71.4% males) with a median age of 67 years. Of them, 28.6% had an ECOG score ≥2, and 80% were at an III–IV stage. Patients had a median of 2.5 lines of therapy, and more than half of them (51.4%) had received an auto-SCT. In this regard, 22.8% and 45.7% of the patients were refractory to the first and the most recent line of therapy, respectively (Table 1). The authors reported a median PFS of 13.8 months, a median OS of 32.5 months, an ORR of 47.1%, and a CR of 31.4%31 (Table 4). Similarly, the study of Zinzani et al, which included 33 patients with R/R MCL treated with lenalidomide, reported a PFS of 13.9 months, an ORR of 45.5% and a lower CR of 12.1%32 (Table 4).
Venetoclax
The study on venetoclax included 10 patients, of which 90% had previously been treated with ibrutinib, 60% presented with blastoid histology, and all of them were at an III–IV stage (Table 1). Venetoclax treatment resulted in a median PFS and OS of 6 months33 (Table 4).
CAR T-Cell Therapies
Four studies evaluated the use of CAR T-cell therapies with brexucabtagene on R/R MCL patients.36,42–44 They included 33 to 93 patients, mostly males (81% to 93.6%, n = 4), with median ages between 66 and 67 years (n = 4). The proportion of patients with an ECOG score ≥2 ranged from 9% to 21.1% (n = 3), whereas the percentage of individuals at III–IV stages was 88% (n = 2). The number of previous lines of therapy varied from 2 to 3 (n = 4), the proportion of patients who had previously received an auto-SCT and an allo-SCT ranged from 27% to 40% (n = 4) and from 4% to 15% (n = 3), respectively, and patients previously treated with BTKis ranged 82% to 100% (n = 2). Regarding prognostic factors, 68% to 88% of the individuals had a MIPI/sMIPI intermediate-high (n = 3), whereas 49% to 83% of them presented with a Ki-67 index ≥30% (n = 4). Moreover, TP53 aberrations and blastoid or pleomorphic variants were found in 12% to 46% (n = 3) and in 27% to 45% (n = 3) of patients, respectively (Table 1).
Regarding efficacy outcomes, two studies reported 6-month PFS, ranging from 57.9% to 82.7%, whereas other studies reported similar rates at different time points (3-month PFS of 80.6%, n = 1, and 1-year PFS of 50.8%, n = 1). However, the 6-month OS was relatively homogeneous among the studies (82.1% to 89.4%, n = 3). The ORR and CR were also very similar, ranging from 86 to 91% (n = 4) and from 61.9 to 79% (n = 4), respectively. Median follow-ups were variable, ranging from 3 to 10.1 months (Table 4).
Risk of Bias Assessment
Table S1 summarizes the analysis of the risk of bias of the studies included in the systematic review. Of them, 26 (86.7%) clearly described eligibility criteria, 25 (83.3%) reported consecutive inclusion of participants, and only 8 (26.7%) stated complete inclusion of participants. In addition, 16 (53.3%) studies measured the lymphoma in a standard and reliable way for all the participants, but only 9 (30.0%) studies reported using valid methods to diagnose it. Demographics and clinical characteristics of R/R MCL patients were clearly reported for each treatment regimen in 23 (76.7%) and 15 (50.0%) of the studies, respectively, although the latter would increase if we considered the whole study population (ie, not only patients with R/R MCL) and/or all the treatment regimens of the studies. All studies (n = 30, 100.0%) clearly reported efficacy outcomes (ie, treatment response and survival) and demographic information of the sites or center where the studies were conducted. Finally, the statistics were clearly reported in 18 (60.0%) studies.
Discussion
In this systematic review of the characteristics and treatment outcomes of patients with R/R MCL in the clinical practice, we found that most treatment regimens were based on BTKis (specifically, ibrutinib) or chemotherapy/immunochemotherapy strategies (especially those including bendamustine). As expected, most patients were males with a median age ranging from 65 to 75 years at treatment initiation. Of the treatment regimens reporting each variable of interest, approximately two thirds of them included a percentage of patients with an ECOG score ≥2 between 10% and 30%, most of them had ≥80% of the patients with an III–IV stage disease, reflecting the reality of the treatment of the disease in the routine clinical practice. All of them reported a median number of previous lines of therapy of between 1 and 3. The percentage of patients who had previously received an auto-SCT was quite variable, but ranged from 10% to 40% in approximately two-thirds of the treatment regimens, depending on the age and status of the patients included in the study. More than half of the patients presented with an intermediate-high MIPI/sMIPI in treatment regimens reporting it. In addition, the percentages of patients with high-risk features, such as TP53 aberrations, and a Ki67 ≥30% were reported in a small number of studies and ranged from 0% to 46%, and from 33.3% to 100% of the patients, respectively, further reflecting high variability among patients included in these studies. Additionally, the percentage of patients with blastoid or pleomorphic histology was variable, ranging from 3.4% to 27–40% in CAR T-cell studies where, as expected, patients are in later lines and have more high-risk features.
Interestingly, only studies using ibrutinib and CAR T-cells (brexucabtagene autoleucel) reported similar efficacy outcomes in RWE studies7–10,13,28–31,33,35,36,39–43 compared to clinical trials (CTs).6,45 When comparing the values of each outcome of interest, the real-world treatment regimens using ibrutinib monotherapy8–11,14,21–24,34,37,40,41 yielded a wide range of values for all the studied variables where those of the pooled analysis fell.7 As for the treatment response, the lowest values of ORR were reported with the lenalidomide regimens25,26 and the cytarabine regimen.29 Of note, the ibrutinib study by Broccoli et al10 reported an ORR of 36%, but physicians in the study erroneously considered that ibrutinib induced transient lymphocytosis as PD and stopped treatment. The highest ORR values were the ibrutinib-based regimens reported by Janssens and Fabbri et al,38,39 all four CAR T-cell treatment regimens,36,42–44 and one study reporting bendamustine ± rituximab.27 Interestingly, the ORR rates reported in the bendamustine RWE studies (ranging 70% to 86%) were generally lower than those reported in clinical trials.45–50 Regarding CR rates, the highest CR values corresponded to the CAR T-cell treatment regimens,36,42–44 whereas the lowest ones were those reported by the ibrutinib monotherapy regimens of Jeon et al,21 Zhang et al,24 and the already mentioned Broccoli et al,10 the DHAP regimen,30 and the lenalidomide regimen reported by Zinzani et al.32 It is important to note that, among ibrutinib studies, there was a high variability between CR rates, ranging from 39.5% to 15%28,39 which may be due not only to the baseline characteristics of the patients and the line of therapy in which ibrutinib was used, but also to the response criteria used in the study, which may vary significantly in this type of retrospective routine clinical practice studies. Moreover, it has been widely described in the successive follow-ups of ibrutinib clinical trials51 that ORRs and CR rates improve over time, so these differences may also be due to short follow-up periods.
Regarding survival outcomes, the highest median PFS values were found with ibrutinib21,24 and bendamustine (median PFS ranging from 10.1 to 25.9 months)9,28 regimens. The ibrutinib-based treatment regimens resulted in a wide range of median PFS values, from 7.9 to 30.8 months.8–11,14,21–24,34,37,39–41 The PFS reported in the pooled analysis,6 with a median follow-up of 9.7 years, was 12.5 months in all the population (median of 2 prior lines) and 25.4 months in patients with one prior line of therapy. Thus, the number of prior lines of therapy the patient received before ibrutinib treatment should be considered in order to contextualize PFS results of the RWE studies. In the study by Obr et al, recently updated,52 reporting a median PFS of 7.9 months, patients were heavily pretreated, with 72% of the patients with 2 or more previous lines of therapy. On the contrary, in the studies reporting data from patients treated with ibrutinib as second-line therapy,8,9,13,34,40 where the best PFS results are expected, PFS ranged between 17 and 24 months, in line with the results of the pooled analysis, considering unselected RWE populations. Conversely, bortezomib35 and venetoclax33 treatment studies yielded the lowest PFS values, potentially because in these studies they were used as monotherapy in late lines of therapy and in elderly patients.
The highest median OS values were also found among ibrutinib8–11,14,21–24,37,40,41 and bendamustine9,13,27 treatment regimens. All of the other treatment regimens reporting OS yielded lower median OS values, and the lowest ones were those corresponding to cytarabine,29 bortezomib,35 and venetoclax33 regimens, with the last two being lower than those reported in CTs.49–51 CAR-T regimen studies did not report median PFS and OS due to their short follow-up, but the longest follow-up by Iacoboni et al36 reported an estimated 50.8% PFS and 61.4% OS at 12 months, very promising results in this heavily pretreated high-risk patient population. In this context, it is important to note that multivariate analysis have shown several prognostic markers to have a deleterious effect in PFS and OS besides previous lines of therapy in the context of R/R MCL and need to be considered when comparing the efficacy results reported in the different studies:6 ECOG, sMIPI, bulky disease, early progression of disease (POD24 status), and ultra-high-risk features, such as blastoid/pleomorphic histology and TP53 mutation.
When looking at clinical trials assessing the efficacy of the same agents retrieved in this review for treating R/R MCL patients,7,45–50,53–63 we observed some similarities in the efficacy outcomes. Regarding response outcomes, as in the real-world studies, the highest ORRs were reported by clinical trials assessing bendamustine,47,48 CAR T-cell therapy,61 and ibrutinib combined with rituximab.56 Conversely, the lowest ORRs were those found in clinical studies evaluating lenalidomide63 and bortezomib.59 Additionally, studies using CAR T-cell therapy61 and bendamustine47 reported the highest CR rates, whereas the lowest CR values were those reported in clinical trials using bortezomib59 and lenalidomide.63 Conversely, the highest median PFS values corresponded to ibrutinib-based therapies6,53,55 and CAR T-cell therapies, considering that CAR T-cell therapies have been tried mostly in a post iBTK setting, whereas bortezomib,59,60 together with lenalidomide,63 yielded the lowest median PFS values.
It is important to note that bendamustine-based therapy results in higher CR rates than ibrutinib monotherapy in RWE and CTs, which does not translate into improved PFS/OS results, which could suggest that, besides attaining a CR, a well-established endpoint that prolongs PFS,6 continuous treatment may play an important role in delaying progression of the disease in MCL. One proof of that is that rituximab maintenance after front line therapy has been shown to delay progression of the disease and improve PFS/OS64–66 and has thus been established as standard of care. In the retrospective study MANTLE FIRST, Visco et al9 compared second line ibrutinib, R-BAC, R-bendamustine, and a variety of other treatments in young R/R MCL patients. The CR rates obtained with R-BAC and R-Benda were 63% and 43%, respectively, whereas ibrutinib yielded a lower CR rate of 38%, which did not translate into a better PFS for R-BAC (mPFS2: 25 m.) and R-bendamustine (mPFS2: 13 m.) in comparison with ibrutinib (mPFS2: 24 m.); conversely, ibrutinib resulted in a significantly longer PFS in POD24 patients compared to those attained with R-BAC and R-bendamustine (p=0.02) besides CR rates, reflecting that the attainment of deep responses, in the setting of targeted continuous therapies, may not be the only goal of therapy and may be achieved later in time without direct impact on PFS.
This study has some limitations, mainly associated with the quality of the data but also with the difficulty of comparing outcomes in R/R MCL due to the heterogeneity of the disease. First, the methods to assess the treatment outcomes were not always described accurately in the retrieved studies, which may entail a measurement bias and affect results. Secondly, not all the studies reported the same data on the characteristics of patients and the studied outcomes. In this regard, most studies did not report the Ki-67 index or the presence of TP53 aberrations, which are prognostic factors of MCL and, thus, may affect the efficacy of the treatment. Besides, many studies were basket studies and not only involved patients with R/R MCL and one treatment regimen, but also patients with other types of lymphomas, treatment-naïve MCL, and/or different treatment approaches. Given that not all these studies reported the variables by type of lymphoma, naïve or relapsed status, or treatment approach, we could not always retrieve the data corresponding to R/R MCL patients for a given treatment approach. Another limitation relies on the high variability of real-world data, making it difficult to compare the different treatment regimens among them and from those obtained in clinical trials. However, most of these limitations are inherent to real-world data, which are essential to complement those of clinical trials.
Conclusion
To our knowledge, this is the first systematic review of the real-world evidence on R/R MCL treatments. Baseline characteristics of patients included in the studies reflect the reality of R/R MCL in a real-world setting and the heterogeneity of the disease. A very important part of the studies retrieved were ibrutinib monotherapy studies, maybe due to the increasing importance in the last few years of real-world evidence and the need to confirm clinical trial results in a routine clinical practice setting with unselected patient populations. Furthermore, ibrutinib was a first-in-class BTK inhibitor and its first publication in 201367 raised interest in the medical community due to the unprecedented efficacy results reported for a targeted agent in monotherapy, its favorable tolerability profile, and its convenience compared to classic chemoimmunotherapy strategies, something that may have boosted interest in confirming those results in the routine clinical practice. Chemoimmunotherapy is still being widely used in the R/R setting, as evidenced by the broad range of studies considered in this review, but the use of other targeted therapies is very limited. Regarding efficacy outcomes, the best results obtained in RWE studies are those of ibrutinib, CAR T-cells and bendamustine-based regimens, the first two similar to those reported in clinical trials. Those results have led to expert/guidelines recommendations prioritizing BTKis at first relapse and CAR T-cells as the best option after BTKi relapse.68–71 However, these results should be interpreted with caution since they are limited by the quality of the real-world data available and the difficulty of comparing outcomes in R/R MCL due to the heterogeneity of the disease.
Expert Opinion
Despite recent advances that have prolonged survival, R/R MCL is clinically and biologically heterogeneous and is still a therapeutic challenge, with high-risk and early relapsed patients remaining an unmet medical need. There is no standard treatment for R/R MCL, but considering patients’ advanced age, tolerability profile, and convenient administration, BTKis should be positioned as second line of therapy,6 and CAR T-cells should be the approach to BTKi-relapsed patients.61 However, access to CAR T is not universal, and more therapies in this setting are still needed.
In this sense, there is a huge development in the MCL field with many chemo-free and combination regimens with established chemoimmunotherapy backbones being studied not only in the relapsed setting, but to improve front-line treatment options and to move forward to earlier lines targeted and cellular therapies. For instance, the randomized Phase 3 SHINE study, where continuous ibrutinib or placebo was combined with rituximab-bendamustine followed by rituximab maintenance in front-line elderly MCL patients, showed a promising 80.6-month median PFS for the ibrutinib + BR arm, which is the longest PFS ever reported for this type of non-candidate to auto-SCT patients. The results of the TRIANGLE trial, evaluating the use of ibrutinib alone or in combination with auto-SCT in the front-line setting in candidates to auto-SCT72 are also worth mentioning. These trial results seem to indicate that auto-SCT, currently the most efficacious standard of care for front-line transplant-eligible patients, is not superior to front-line ibrutinib monotherapy in young fit MCL patients. This is an unprecedented result leading us to hypothesize that auto-SCT may be replaced with the addition of ibrutinib to the induction therapy in these patients as front-line treatment, avoiding auto-SCT-associated morbidities and mortality. These results, along with other promising clinical trials including new targeted agents in combination with other therapies, may bring these therapies to the front-line setting and help improve patient outcomes since diagnosis (MANGROVE, NCT04002297; SYMPATICO, NCT03112174; OAsIs, NCT02558816; ENRICH, BOVEN, NCT03824483). Furthermore, these new therapeutic schemes could decrease toxicity compared to the standard chemotherapy mentioned in this study, being more convenient and tolerable, opening new venues towards improving both efficacy and tolerability in the newly diagnosed MCL population, often enriched in non-transplant eligible, elderly unfit patients.
Additionally, many new targeted agents will play an important role in the upcoming years (the non-covalent BTKis such as pirtobrutinib, anti-ROR1 conjugate zilovertamab, bispecific antiCD20-CD3 antibodies epcoritamab, glofitamab, other CAR T-cells like lisocabtagene and other small molecules) and will eventually evolve to be used in the front-line setting, where therapies have been proved more efficacious. Conversely, it can be hypothesized that chemoimmunotherapy will have a small role, while targeted agents along with CAR-T cells will have a major role in the front-line setting and the first relapse, where the best results will be achieved, and the life of MCL patients will be prolonged. How these therapies will be incorporated to the daily clinical practice will depend on many factors, including access to novel therapies in different geographical regions. Irrespective of access, these agents and their combinations will have to be added to the treatment strategies according to patients’ status and age. Furthermore, optimal sequencing will have to be determined, and those results will have to be confirmed in non-selected MCL populations, which are usually elderly and have comorbidities and use concomitant medications that may affect the outcomes of these treatments. The rise of RWE studies has been very positive to the medical community, expanding knowledge about these therapies, not only in terms of effectiveness, but also of their long-term security profile in real-world populations.
Acknowledgments
The authors would like to thank the i2e3 Procomms team (Barcelona, Spain) and especially, Alba Rebollo, Ph.D., for providing medical writing support during the preparation of this manuscript.
Funding
This study was funded by Janssen-Cilag.
Disclosure
JMS has received honoraria for consultancy or advisory role from AbbVie, Janssen, Roche, Gilead-Kite, Lilly, Beigene, Novartis, Incyte, and BMS-Celgene and received honoraria as speaker in medical education activities organized by Janssen, Roche, Gilead-Kite, Incyte, and BMS-Celgene. ERA is a Janssen employee. MS declares no conflicts of interest in this work.
References
1. Dreyling M, Campo E, Hermine O, et al. Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017:28(suppl_4):iv62–iv71. doi:10.1093/ANNONC/MDX223
2. Monga N, Garside J, Quigley J, et al. Systematic literature review of the global burden of illness of mantle cell lymphoma. Curr Med Res Opin. 2020;36(5):843–852. doi:10.1080/03007995.2020.1742101
3. Zhou Y, Wang H, Fang W, et al. Incidence trends of mantle cell lymphoma in the United States between 1992 and 2004. Cancer. 2008;113(4):791–798. doi:10.1002/CNCR.23608
4. Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375. doi:10.1182/BLOOD-2016-01-643569
5. Kumar A, Sha F, Toure A, et al. Patterns of survival in patients with recurrent mantle cell lymphoma in the modern era: progressive shortening in response duration and survival after each relapse. Blood Cancer J. 2019;9(6):50. doi:10.1038/s41408-019-0209-5
6. Romancik JT, Gerber DG, Zhuang T, Cohen JB. SOHO State of the Art Updates and Next Questions: managing Relapsed Mantle Cell Lymphoma. Clin Lymphoma Myeloma Leuk. 2022;22(8):557–565. doi:10.1016/J.CLML.2022.01.008
7. Dreyling M, Goy A, Hess G, et al. Long-term Outcomes With Ibrutinib Treatment for Patients With Relapsed/Refractory Mantle Cell Lymphoma: a Pooled Analysis of 3 Clinical Trials With Nearly 10 Years of Follow-up. Hemasphere. 2022;6(5):e712. doi:10.1097/HS9.0000000000000712
8. Cencini E, Mecacci B, Morelli F, et al. Ibrutinib in patients with relapsed/refractory mantle cell lymphoma: a real-life, retrospective, multicenter trial on behalf of the “RTL” (regional Tuscan lymphoma network). Am J Blood Res. 2021;11(4):373.
9. Visco C, Di Rocco A, Evangelista A, et al. Outcomes in first relapsed-refractory younger patients with mantle cell lymphoma: results from the MANTLE-FIRST study. Leukemia. 2021;35(3):787–795. doi:10.1038/S41375-020-01013-3
10. Broccoli A, Casadei B, Morigi A, et al. Italian real life experience with ibrutinib: results of a large observational study on 77 relapsed/refractory mantle cell lymphoma. Oncotarget. 2018;9(34):23443–23450. doi:10.18632/ONCOTARGET.25215
11. McCulloch R, Lewis D, Crosbie N, et al. Ibrutinib for mantle cell lymphoma at first relapse: a United Kingdom real-world analysis of outcomes in 211 patients. Br J Haematol. 2021;193(2):290–298. doi:10.1111/BJH.17363
12. Murakami H, Yoshioka T, Moriyama T, Ishikawa T, Makita M, Sunami K. Bendamustine Plus Rituximab as Salvage Treatment for Patients with Relapsed or Refractory Low-grade B-cell Lymphoma and Mantle Cell Lymphoma: a Single-Center Retrospective Study. Acta Med Okayama. 2021;75(4):461–469. doi:10.18926/AMO/62398
13. McCulloch R, Visco C, Eyre TA, et al. Efficacy of R-BAC in relapsed, refractory mantle cell lymphoma post BTK inhibitor therapy. Br J Haematol. 2020;189(4):684–688. doi:10.1111/BJH.16416
14. Epperla N, Hamadani M, Cashen AF, et al. Predictive factors and outcomes for ibrutinib therapy in relapsed/refractory mantle cell lymphoma-a “real world” study. Hematol Oncol. 2017;35(4):528–535. doi:10.1002/HON.2380
15. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. PLoS Med. 2021;18(3):e003583. doi:10.1371/JOURNAL.PMED.1003583
16. International Conference on Malignant Lymphoma. Available from: https://www.icml.ch/icml/home.html.
17. American Society of Hematology. Meetings - Hematology.org. Available from: https://annualmeeting.hematology.org/home.
18. American Society of Clinical Oncology. Meeting Library | home. Available from: https://conferences.asco.org/am/attend.
19. Library by European Hematology Association (EHA). Available from: https://ehaweb.org/meetings.
20. Munn Z, Barker TH, Moola S, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Evid Synth. 2020;18(10):2127–2133. doi:10.11124/JBISRIR-D-19-00099
21. Jeon YW, Yoon S, Min GJ, et al. Clinical outcomes for ibrutinib in relapsed or refractory mantle cell lymphoma in real-world experience. Cancer Med. 2019;8(16):6860–6870. doi:10.1002/CAM4.2565
22. Sancho JM, Marín A, Fernández S, et al. IBRORS-MCL Study: a Spanish Retrospective and Observational Study of Relapsed/Refractory Mantle-Cell Lymphoma (MCL) Treated with Ibrutinib in Routine Clinical Practice. Int J Hematol. 2022;116(3):381–392. doi:10.1007/s12185-022-03367-z
23. Sharman J, Kabadi SM, Clark J, Andorsky D. Treatment patterns and outcomes among mantle cell lymphoma patients treated with ibrutinib in the United States: a retrospective electronic medical record database and chart review study. Br J Haematol. 2021;192(4):737–746. doi:10.1111/BJH.16922
24. Zhang Y, Liu P, Cai J, et al. Ibrutinib as monotherapy versus combination therapy in Chinese patients with relapsed/refractory mantle cell lymphoma: a multicenter study. Cancer Med. 2022;11(22):4134–4145. doi:10.1002/cam4.4765
25. Rigacci L, Puccini B, Cortelazzo S, et al. Bendamustine with or without rituximab for the treatment of heavily pretreated non-Hodgkin’s lymphoma patients: a multicenter retrospective study on behalf of the Italian Lymphoma Foundation (FIL). Ann Hematol. 2012;91(7):1013–1022. doi:10.1007/S00277-012-1422-5
26. Warsch S, Hosein PJ, Maeda LS, Alizadeh AA, Lossos IS. A retrospective study evaluating the efficacy and safety of bendamustine in the treatment of mantle cell lymphoma. Leuk Lymphoma. 2012;53(7):1299–1305. doi:10.3109/10428194.2011.649476
27. García-Noblejas A, Martínez Chamorro C, Navarro Matilla B, et al. Bendamustine as salvage treatment for patients with relapsed or refractory mantle cell lymphoma patients: a retrospective study of the Spanish experience. Ann Hematol. 2014;93(9):1551–1558. doi:10.1007/S00277-014-2077-1
28. Karadurmus N, Paydas S, Esin E, et al. Effectiveness of bendamustine in relapsed or refractory lymphoma cases: a Turkish Oncology Group study. Arch Med Sci. 2019;17(4):920–927. doi:10.5114/AOMS.2019.83000
29. Smith A, Roman E, Appleton S, et al. Impact of novel therapies for mantle cell lymphoma in the real world setting: a report from the UK’s Haematological Malignancy Research Network (HMRN). Br J Haematol. 2018;181(2):215–228. doi:10.1111/BJH.15170
30. Kroschinsky F, Röllig D, Riemer B, et al. Modified DHAP regimen in the salvage treatment of refractory or relapsed lymphomas. J Cancer Res Clin Oncol. 2019;145(12):3067–3073. doi:10.1007/S00432-019-03027-6
31. Stefoni V, Pellegrini C, Broccoli A, et al. Lenalidomide in Pretreated Mantle Cell Lymphoma Patients: an Italian Observational Multicenter Retrospective Study in Daily Clinical Practice (the Lenamant Study). Oncologist. 2018;23(9):1033–1038. doi:10.1634/THEONCOLOGIST.2017-0597
32. Zinzani PL, Rigacci L, Cox MC, et al. Lenalidomide monotherapy in heavily pretreated patients with non-Hodgkin lymphoma: an Italian observational multicenter retrospective study in daily clinical practice. Leuk Lymphoma. 2015;56(6):1671–1676. doi:10.3109/10428194.2014.964702
33. Hughes ME, Landsburg DJ, Rubin DJ, et al. Treatment of Patients With Relapsed/Refractory Non-Hodgkin Lymphoma With Venetoclax: a Single-Center Evaluation of Off-Label Use. Clin Lymphoma Myeloma Leuk. 2019;19(12):791–798. doi:10.1016/J.CLML.2019.09.612
34. Yi JH, Kim SJ, Yoon DH, et al. Real‐world outcomes of ibrutinib therapy in Korean patients with relapsed or refractory mantle cell lymphoma: a multicenter, retrospective analysis. Cancer Commun. 2021;41(3):275. doi:10.1002/CAC2.12150
35. Skarbnik AP, Ma E, Lafeuille MH, et al. Treatment patterns and outcomes with subcutaneous bortezomib in patients with relapsed mantle cell lymphoma: a retrospective, observational study of patient medical records from US community oncology practices. Leuk Lymphoma. 2017;58(8):1968–1972. doi:10.1080/10428194.2016.1272688
36. Iacoboni G, Rejeski K, Villacampa G, et al. Real-world evidence of brexucabtagene autoleucel for the treatment of relapsed or refractory mantle cell lymphoma. Blood Adv. 2022;6(12):3606–3610. doi:10.1182/BLOODADVANCES.2021006922
37. Tucker D, Morley N, MacLean P, et al. The 5-year follow-up of a real-world observational study of patients in the United Kingdom and Ireland receiving ibrutinib for relapsed/refractory mantle cell lymphoma. Br J Haematol. 2021;192(6):1035–1038. doi:10.1111/BJH.16739
38. Lamm W, Drach J, Kiesewetter B, et al. Rituximab, Ara-C, dexamethasone and oxaliplatin (R-ADOx) is effective for treatment of elderly patients with relapsed mantle cell lymphoma. J Cancer Res Clin Oncol. 2013;139(10):1771–1775. doi:10.1007/S00432-013-1475-4
39. Fabbri A, Cencini E, Congiu AG, Miglino M, Rigacci L, Bocchia M. Ibrutinib in association with venetoclax for the treatment of mantle-cell lymphoma: a multicenter case series. Am J Blood Res. 2020;10(6):355.
40. Janssens A, Snauwaert S, Bron D, et al. Effectiveness and safety of ibrutinib in chronic lymphocytic leukemia (CLL) and mantle cell lymphoma (MCL) in Belgian routine clinical practice with a 3-year follow-up. EHA Library. 2021;325414:EP654.
41. Obr A, Klener P, Janíková A, et al. Ibrutinib in Mantle Cell Lymphoma Patients: analysis of the Czech Lymphoma Study Group. Blood. 2021;138(Supplement 1):4526. doi:10.1182/BLOOD-2021-146589
42. Romancik JT, Goyal S, Gerson JN, et al. Analysis of Outcomes and Predictors of Response in Patients with Relapsed Mantle Cell Lymphoma Treated with Brexucabtagene Autoleucel. Blood. 2021;138(Supplement 1):1756. doi:10.1182/BLOOD-2021-153277
43. Herbaux C, Bret C, Di Blasi R, et al. Kte-X19 in Relapsed or Refractory Mantle-Cell Lymphoma, a Real-Life Study from the Descar-T Registry and Lysa Group. Blood. 2021;138(Supplement 1):743. doi:10.1182/BLOOD-2021-148626
44. Wang Y, Jain P, Locke FL, et al. Brexucabtagene Autoleucel for Relapsed/Refractory Mantle Cell Lymphoma: real World Experience from the US Lymphoma CAR T Consortium. Blood. 2021;138(Supplement 1):744. doi:10.1182/BLOOD-2021-147563
45. Friedberg JW, Vose JM, Kelly JL, et al. The combination of bendamustine, bortezomib, and rituximab for patients with relapsed/refractory indolent and mantle cell non-Hodgkin lymphoma. Blood. 2011;117(10):2807–2812. doi:10.1182/BLOOD-2010-11-314708
46. Czuczman MS, Goy A, Lamonica D, Graf DA, Munteanu MC, van der Jagt RH. Phase II study of bendamustine combined with rituximab in relapsed/refractory mantle cell lymphoma: efficacy, tolerability, and safety findings. Ann Hematol. 2015;94(12):2025–2032. doi:10.1007/S00277-015-2478-9
47. Ohmachi K, Ando K, Ogura M, et al. Multicenter phase II study of bendamustine for relapsed or refractory indolent B-cell non-Hodgkin lymphoma and mantle cell lymphoma. Cancer Sci. 2010;101(9):2059–2064. doi:10.1111/J.1349-7006.2010.01635.X
48. Koenigsmann M, Knauf WU, Herold M, et al. Fludarabine and bendamustine in refractory and relapsed indolent lymphoma--a multicenter phase I/II Trial of the east German society of hematology and oncology (OSHO). Leuk Lymphoma. 2004;45(9):1821–1827. doi:10.1080/1042819042000223822
49. Visco C, Finotto S, Zambello R, et al. Combination of rituximab, bendamustine, and cytarabine for patients with mantle-cell non-Hodgkin lymphoma ineligible for intensive regimens or autologous transplantation. J Clin Oncol. 2013;31(11):1442–1449. doi:10.1200/JCO.2012.45.9842
50. Weide R, Hess G, Köppler H, et al. High anti-lymphoma activity of bendamustine/mitoxantrone/rituximab in rituximab pretreated relapsed or refractory indolent lymphomas and mantle cell lymphomas. A multicenter phase II study of the German Low Grade Lymphoma Study Group (GLSG). Leuk Lymphoma. 2007;48(7):1299–1306. doi:10.1080/10428190701361828
51. Rule S, Dreyling M, Goy A, et al. Outcomes in 370 patients with mantle cell lymphoma treated with ibrutinib: a pooled analysis from three open-label studies. British Journal of Haematology. 2017;179(3):430–438. doi:10.1111/bjh.14870
52. Obr A, Benesova K, Janikova A, et al. Ibrutinib in mantle cell lymphoma: a real-world retrospective multi-center analysis of 77 patients treated in the Czech Republic. Ann Hematol. 2023;102(1):107–115. doi:10.1007/S00277-022-05023-2
53. Tam CS, Anderson MA, Pott C, et al. Ibrutinib plus Venetoclax for the Treatment of Mantle-Cell Lymphoma. N Engl J Med. 2018;378(13):1211–1223. doi:10.1056/NEJMOA1715519
54. Wang M, Ramchandren R, Chen R, et al. Concurrent ibrutinib plus venetoclax in relapsed/refractory mantle cell lymphoma: the safety run-in of the phase 3 SYMPATICO study. J Hematol Oncol. 2021;14(1):179. doi:10.1186/S13045-021-01188-X
55. Portell CA, Wages NA, Kahl BS, et al. Dose-finding study of ibrutinib and venetoclax in relapsed or refractory mantle cell lymphoma. Blood Adv. 2022;6(5):1490–1498. doi:10.1182/BLOODADVANCES.2021005357
56. Jain P, Romaguera J, Srour SA, et al. Four-year follow-up of a single arm, phase II clinical trial of ibrutinib with rituximab (IR) in patients with relapsed/refractory mantle cell lymphoma (MCL). Br J Haematol. 2018;182(3):404–411. doi:10.1111/BJH.15411
57. Jerkeman M, Eskelund CW, Hutchings M, et al. Ibrutinib, lenalidomide, and rituximab in relapsed or refractory mantle cell lymphoma (PHILEMON): a multicentre, open-label, single-arm, Phase 2 trial. Lancet Haematol. 2018;5(3):e109–e116. doi:10.1016/S2352-3026(18)30018-8
58. Goy A, Younes A, McLaughlin P, et al. Phase II study of proteasome inhibitor bortezomib in relapsed or refractory B-cell non-Hodgkin’s lymphoma. J Clin Oncol. 2005;23(4):667–675. doi:10.1200/JCO.2005.03.108
59. Goy A, Bernstein SH, Kahl BS, et al. Bortezomib in patients with relapsed or refractory mantle cell lymphoma: updated time-to-event analyses of the multicenter phase 2 PINNACLE study. Ann Oncol. 2009;20(3):520–525. doi:10.1093/ANNONC/MDN656
60. O’Connor OA, Moskowitz C, Portlock C, et al. Patients with chemotherapy-refractory mantle cell lymphoma experience high response rates and identical progression-free survivals compared with patients with relapsed disease following treatment with single agent bortezomib: results of a multicentre Phas. Br J Haematol. 2009;145(1):34–39. doi:10.1111/J.1365-2141.2008.07466.X
61. Wang M, Munoz J, Goy A, et al. Three-Year Follow-Up of KTE-X19 in Patients With Relapsed/Refractory Mantle Cell Lymphoma, Including High-Risk Subgroups, in the ZUMA-2 Study. J Clin Oncol. 2022:JCO2102370. doi:10.1200/JCO.21.02370
62. Davids MS, Roberts AW, Kenkre VP, et al. Long-term Follow-up of Patients with Relapsed or Refractory Non-Hodgkin Lymphoma Treated with Venetoclax in a Phase I, First-in-Human Study. Clin Cancer Res. 2021;27(17):4690–4695. doi:10.1158/1078-0432.CCR-20-4842
63. Witzig TE, Luigi Zinzani P, Habermann TM, et al. Long-term analysis of phase II studies of single-agent lenalidomide in relapsed/refractory mantle cell lymphoma. Am J Hematol. 2017;92(10):E575–E583. doi:10.1002/AJH.24854
64. Le GS, Thieblemont C, Oberic L, et al. Rituximab after Autologous Stem-Cell Transplantation in Mantle-Cell Lymphoma. N Engl J Med. 2017;377(13):1250–1260. doi:10.1056/NEJMOA1701769/SUPPL_FILE/NEJMOA1701769_DISCLOSURES.PDF
65. Kluin-Nelemans HC, Hoster E, Hermine O, et al. Treatment of Older Patients with Mantle-Cell Lymphoma. N Engl J Med. 2012;367(6):520–531. doi:10.1056/NEJMOA1200920/SUPPL_FILE/NEJMOA1200920_DISCLOSURES.PDF
66. Hilal T, Wang Z, Almader-Douglas D, Rosenthal A, Reeder CB, Jain T. Rituximab maintenance therapy for mantle cell lymphoma: a systematic review and meta-analysis. Am J Hematol. 2018;93(10):1220–1226. doi:10.1002/AJH.25226
67. Wang ML, Rule S, Martin P, et al. Targeting BTK with Ibrutinib in Relapsed or Refractory Mantle-Cell Lymphoma. N Engl J Med. 2013;369(6):507–516. doi:10.1056/NEJMOA1306220/SUPPL_FILE/NEJMOA1306220_DISCLOSURES.PDF
68. O’Reilly MA, Sanderson R, Wilson W, et al. Addendum to British Society for Haematology Guideline for the management of mantle cell lymphoma, 2018 (Br. J. Haematol. 2018; 182: 46–62): risk assessment of potential CAR T candidates receiving a covalent Bruton tyrosine kinase inhibitor for relapsed/re. Br J Haematol. 2022;199(1):40–44. doi:10.1111/BJH.18378
69. Munshi PN, Hamadani M, Kumar A, et al. ASTCT, CIBMTR, and EBMT clinical practice recommendations for transplant and cellular therapies in mantle cell lymphoma. Bone Marrow Transplant. 2021;56(12):2911–2921. doi:10.1038/S41409-021-01288-9
70. National Comprehensive Cancer Network. NCCN Guidelines for B-Cell Lymphomas V.1.2022.; 2022. https://www.nccn.org/patients/guidelines/content/PDF/nhl-diffuse-patient.pdf.
71. GELTAMO. Guía de GELTAMO. Guía Clínica Para El Diagnóstico y Tratamiento Del Linfoma de Células Del Manto; 2022. Available from: https://www.geltamo.com/images/Guia_LCM_OK_ACTUALIZADO_08.06.2022_v2.pdf.
72. Dreyling M, Doorduijn JK, Gine E, et al. Efficacy and Safety of Ibrutinib Combined with Standard First-Line Treatment or As Substitute for Autologous Stem Cell Transplantation in Younger Patients with Mantle Cell Lymphoma: results from the Randomized Triangle Trial By the European MCL Network. Blood. 2022;140(Supplement 1):1–3. doi:10.1182/BLOOD-2022-163018
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.