Back to Journals » Journal of Inflammation Research » Volume 19
Real World Evidence in Alopecia Areata: Current Management, Emerging Therapies and Future Challenges – A Narrative Review
Authors Khoda F, Chandidzura A ![]() , Sinclair R, Wall D, Meah N, Harries M
, Sinclair R, Wall D, Meah N, Harries M ![]()
Received 18 February 2026
Accepted for publication 6 May 2026
Published 9 June 2026 Volume 2026:19 540843
DOI https://doi.org/10.2147/JIR.S540843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anish R. Maskey
Fatimah Khoda,1 Anne Chandidzura,2 Rodney Sinclair,3 Dmitri Wall,4– 7 Nekma Meah,2,8 Matthew Harries1,2
1Salford Royal Hospital, Northern Care Alliance NHS Foundation Trust, Manchester Academic Health Science Centre, Manchester, M6 8HD, UK; 2Centre for Dermatology Research, Faculty of Biology, Medicine and Health, University of Manchester & NIHR Biomedical Research Centre, Manchester, UK; 3University of Melbourne and Sinclair Dermatology, Melbourne, Australia; 4National and International Skin Registry Solutions (NISR), Dublin, Ireland; 5Charles Institute of Dermatology, UCD School of Medicine, University College Dublin, Dublin, Ireland; 6Hair Restoration Blackrock (HRBR), Dublin, Ireland; 7Department of Dermatology, Mater Misericordiae University Hospital, Dublin, Ireland; 8Mersey & West Lancashire NHS Trust, Marshalls Cross Road, St Helens, WA9 3DA, UK
Correspondence: Matthew Harries, Clinical Senior Lecturer and Honorary Consultant Dermatologist The University of Manchester Salford Royal Hospital Northern Care Alliance NHS Foundation Trust Stott Lane, Salford, Greater Manchester, UK, Tel +44 0 161 2069880, Email [email protected]
Abstract: New targeted therapeutic approaches (eg. biologics, small molecules) have significantly changed the management of inflammatory dermatology conditions in recent years. Alopecia areata (AA), a non-scarring autoimmune hair loss condition, is one of the latest diseases to benefit from these developments. Here we review traditional, new and evolving therapies for AA and highlight the benefits, challenges and uncertainties that come with these new options. We present various real-world data collection approaches currently available and introduce GRASS-UK/GRASS-International as a global collaborative network of prospective AA disease registers designed to study the longer-term safety and effectiveness of new AA therapies as they are introduced.
Keywords: alopecia areata, randomised clinical trials, real-world evidence, research pipeline, disease registers, pharmacovigilance
Introduction
The rapid expansion of novel biologic and small molecule therapies is changing modern healthcare. This therapeutic revolution is driven by the expanding understanding of disease pathogenesis and commonality of mechanisms across distinct conditions, allowing drugs to be re-positioned and regimens refined for different therapeutic indications. This approach has revolutionised the care of several inflammatory dermatology conditions. A striking example of this is the treatment of psoriasis: here the introduction of biologic treatments over 20 years ago has, in effect, ended the previous common practice of recurrent hospital admission for topical (ie., tar or dithranol) therapy that achieved short-term clearance but with high levels of relapse. Importantly, with these modern therapeutic regimens, people with psoriasis can now expect longer term disease control without the uncertainty of disease flares.
In this paper, we will focus on alopecia areata (AA), a common hair loss condition that presents with patchy to complete scalp, face or body hair loss (Figure 1), which is now undergoing a similar paradigm shift in therapeutics to that experienced by psoriasis in the early noughties.1–3 We will review treatment options in AA, with a focus on Janus-kinase (JAK) inhibitors that have rapidly become the standard of care in this condition; but also highlight the research pipeline and diversity of molecular targets being developed, and explore the role of real-world data to inform longer-term safety and effectiveness as newer therapies come to market.
 |
Figure 1 Alopecia areata (The patient featured has provided consent for image publication). |
Alopecia Areata
Alopecia areata is characterised by a non-scarring hair loss affecting any area on the body where terminal hairs are present. Retention of visible follicular ostia within the area of hair loss is used to confirm the alopecia is non-scarring. Additional trichoscopic features that support the diagnosis when present include exclamation-mark hairs, black and yellow dots.4 Exclamation mark hairs are short broken hairs that are easily extracted from the skin and black dots are hairs broken off at the skin surface; both are usually seen at the edge of an expanding patch of alopecia and suggest disease activity. Yellow dots, in contrast, are empty sebum-filled follicular openings typically seen in chronic disease.
Alopecia areata has a lifetime point prevalence (in 2018) of 0.58%5 and overall lifetime incidence of 2.11% in the UK, suggesting that around 1 in 50 people are affected by AA to some degree over their lifetime.6 Interestingly, the incidence of AA is higher in females, people from Asian and other darker skin ethnicities (compared with white ethnicities), those of lower socioeconomic class, and those living in urban areas.5–7
Histologically, AA initially displays a transient dense lymphocytic infiltrate, often likened to a “swarm of bees” around the anagen hair bulb. Later in the disease course there is hair follicle miniaturisation, an increased proportion of catagen/telogen hairs and reduced levels of inflammation that can make diagnosis of chronic AA more challenging, especially when the lymphocytic infiltrate has resolved. The cause of AA is an autoimmune attack of cytotoxic NKG2D+ T-cells against the growing anagen hair bulb,8,9 impacting the hair growth cycle by triggering hair fibre breakage. This results in a localized anagen effluvium, premature catagen induction and termination of hair growth, with subsequent failure of anagen initiation, or truncated anagen growth, leading to persistence of the hair loss.10 Co-expression of a cryptogenic hair follicle antigen with type 1 HLA antigens attracts and activates cytotoxic NKG2D+ T-cells.
In anagen hair follicles, reduced outer root sheath expression of classical HLA type 1 antigens and increased expression of non-classical HLA type 1 anagens simultaneously prevent antigen presentation to cytotoxic T cells and natural killer cells, respectively. This mechanism restricting antigen presentation from certain tissues is termed “immune privilege” and is thought to be an evolutionarily conserved process to prevent excessive inflammation-induced damage to vulnerable essential organs.11 In AA, interferon gamma mediated up-regulation of classical HLA-antigen expression in the hair follicle outer root sheath causes collapse of immune privilege. Thus, hair follicle immune privilege collapse, interferon-gamma dominant lymphocytic inflammation and dystrophic hair cycle growth are key processes that are always present in active disease.12–14
Alopecia areata commonly occurs in association with other autoimmune and atopic conditions, with risk of co-morbid disease development varying with age of AA onset and disease severity (eg., atopy is more common with childhood onset and thyroid dysfunction with older age and extensive hair loss).15,16 A genome-wide association study supports the designation of AA as an autoimmune disease, with several susceptibility genes (eg., CTLA4, BTNL2 and IL-2) present in AA also seen across other autoimmune processes, including Type 1 Diabetes Mellitus, inflammatory bowel disease and rheumatoid arthritis. Further, MHC class 2 genes controlling antigen presentation, as well as hair follicle danger signals (MICA and ULBP3/6) that act as NKG2D activating ligands are prominent in AA and explain, in part, a genetic predisposition to hair follicle immune privilege collapse in those affected.8,9
Alopecia in general has unfairly been labelled as a cosmetic issue; however, in contrast to cosmetic problems, AA has a distinct histopathology, hair has functional importance and hair loss can cause functional impairment. For example, AA is associated with poor quality of life, increased rates of anxiety and depression and higher rates of unemployment.17,18 Strikingly, the impact on mental health and work outcomes is highest in non-white ethnic groups.6 In 2010, the Global Burden of Disease estimated 19.4 DALYs (mean age-adjusted disability-adjusted life years) lost globally reflecting the years lost to disability attributed to AA (where 1 DALY is equivalent to 1 year of healthy life lost). Further, out of 176 diseases in terms of disability burden, AA was ranked 137th and ranked higher than melanoma (138th) and psoriasis (144th).19–21 Alopecia areata can also result in significant financial burden to those affected.22
With this condition predominantly affecting younger people,5 and particularly when experienced during adolescence (a critical time of emotional development), it can have a profound impact on long-term attainment through loss of identity and cumulative life course impairments23 with increased risk of suicide a real concern.24 The lack of developmentally appropriate care25 and few high-quality paediatric clinical trials further compound this issue. Interestingly, priority of hair regrowth can differ between men and women, with men in general prioritizing eyebrow over scalp hair growth compared to women, potentially reflecting cultural norms of baldness in older men and greater utility and acceptance of make-up, microblading, tattooing or transfers to camouflage eyebrow loss in women.26 Further, facial hair loss and nail dystrophy can have functional impacts (eg., eyelash loss resulting in eye irritation) and these extra-scalp manifestations may also disproportionately impact certain religious groups (eg., beard hair loss in the Seikh religion).
The Changing AA Treatment Landscape
Until recently, the treatment options for AA had remained unchanged for years, with many therapies unsatisfactory, of limited benefit or of limited availability, and based on poor quality evidence with no clear standard of care.27–29 This resulted in many people disengaging from medical care when they realised their needs could not be met. Importantly, this position is changing; recognition of this unmet need and a growing understanding of the disease pathogenesis has resulted in greater interest in this condition, enhancing a significance change in the treatment landscape in AA that is only now filtering into dermatology clinics globally;30 specifically, the pharmaceutical industry-driven progression of Janus kinase (JAK) inhibitors.
Therapeutic options in AA are dictated by the severity of disease, patient age and the disease subtype, with disease severity being the main factor influencing treatment selection. Disease severity is usually determined using the Severity of Alopecia Tool (SALT),31,32 which is an assessment based on percentage scalp surface area affected by hair loss; with mild disease representing <20% scalp hair loss, moderate disease 21–49% hair loss, and severe disease >50% hair loss.33 Importantly, there is a clear recognition that disease severity in AA is more than just scalp involvement, with growing consensus that severity grades may be “up-graded” in certain situation, such as significant facial hair involvement, marked psychological impact from AA, rapid progression or chronic unresponsive disease,34 with this approach advocated in various national guidance documents.30,35–37
Traditional AA Therapies
Traditionally, the mainstay of treatment for AA were topical, intra-lesional or systemic corticosteroids, contact immunotherapy or traditional immunosuppressive medications, depending on disease severity and previous treatment responses.30 Treatment was continued until regrowth was achieved and then stopped. However, relapse with this approach was common and treatment side effects (particularly for corticosteroids) limited longer term usage.
Mild to moderate disease is usually treated with potent or very potent topical corticosteroids, administered for 3–6 months, with novel treatment regimens sometimes employed for specific population to reduce side effects (eg., children).38 Efficacy rates range between 20% and 61% and recurrence has been reported in 38–63% of cases suggesting poor long-term control.39 Intralesional corticosteroid injections (usually as triamcinolone acetonide) are advocated as first line therapy in adults with limited AA on the scalp, eyebrows and beard,30 with tolerance of the procedure improved with pain-reducing methods, such as vibration distraction.40 In a UK-based survey conducted prior to the licensing of JAK inhibitors, 83% of clinicians reported intralesional corticosteroids as the most effective treatment for limited AA,41 with this position mirrored across hair-specialist globally.42 Injections are typically administered at a concentration of 2.5–10 mg/mL, with starting concentration and dose adjustment determined by response or side effects (eg., skin atrophy or depigmentation risk).43 For both topical and intralesional steroid, efficacy is greater in patients with milder disease and shorter episode duration.44
In patients with rapidly progressive or moderate to severe disease, a tapering course of oral prednisolone or pulsed intravenous corticosteroid therapy may be used.30,45,46 There are currently no randomised controlled trials comparing differing dosing regimens and treatment duration; however, a dose of 0.5 mg/kg over a period of 6–12 weeks is independently recommended by expert consensus.30,42
Systemic immunosuppressants, including ciclosporin, methotrexate and azathioprine, may be considered as monotherapy, or as a steroid sparing agent. However, most patients continue to require low dose prednisolone to maintain response,47 suggesting that the steroid sparing effect of these agents is limited. Except perhaps for methotrexate in very severe AA,48 the evidence supporting immunosuppressant therapies in AA is limited and generally based on small observational studies with methodological limitations.49–53 None of the systemic treatments described are licensed specifically for AA.
Contact sensitisation, using diphenylcyclopropenone (DPCP) or squaric acid dibutyl ester, can also be considered in moderate-severe AA in both adults and children. A systematic review reported any regrowth rates in 65.5% and complete regrowth in 32.3%; both figures were lower for patients with AU/AT.54 The treatment often requires repeated clinic visits over several months, which may be burdensome for patients. Further, this treatment is often not widely available and typically only offered in a limited number of specialist centres.55 Phototherapy, with psoralen and ultraviolet A (PUVA), is now rarely used but may still be considered in select cases, particularly in patients with Fitzpatrick skin type V and VI, who may be at higher risk of dyspigmentation with contact sensitisation. High quality evidence for both these therapies is limited. Dithranol is an alternative topical therapy used as short-contact irritant therapy that is particularly useful in children and young people with AA, where DPCP is unavailable.30 While poor availability of dithranol in the UK is now limiting its usage, a novel dithranol formulation has recently completed Phase 2 trial in mild-moderate AA, although the data have not been reported to data.56
Adjunctive treatments such as topical or oral minoxidil, and topical prostaglandin analogues are often used to support hair regrowth and reduce the risk of relapse, although the evidence supporting these approaches is weak.57 Advice on cosmetic support options, including wigs, camouflage make-up products, cosmetic tattooing and false eyebrow/eyelashes can help improved quality of life.58 Further, with the significant impact on quality of life, social stigma and increased rates of depression and anxiety seen in AA, referral to psychological support may be appropriate where indicated to provide holistic care.
Janus Kinase (JAK) Inhibitors
There are three JAK inhibitors (JAKi) currently licensed for treating alopecia areata: Baricitinib (Olumiant®; Eli-Lilly), Ritlecitinib (Litfulo®; Pfizer), and Deuruxolitinib (Leqselvi®; Sun Pharma), although these products are not licensed in all jurisdictions, and funding/reimbursement arrangements vary from country to country. For example, in the UK ritlecitinib, baricitinib and deuruxolitinib are licenced, but only ritlecitinib is currently funded on the NHS (https://www.nice.org.uk/guidance/ta958).
Baricitinib
Baricitinib is a selective inhibitor of JAK1 and JAK2. Two parallel RCTs (BRAVE-AA1 and BRAVE-AA2) enrolling approximately 1,200 participants were conducted to investigate baricitinib in patients with severe AA (SALT ≥ 50)59 (Table 1). BRAVE-AA1 was an adaptive phase 2/3 trial that initially explored several dosing regimens, proceeding with 2 mg and 4 mg once daily options. The primary outcome was achievement of absolute SALT score ≤20 at week 36. Several secondary outcomes were also reported, including patient reported outcomes, and clinician reported eyebrow and eyelash response. In BRAVE-AA1, 38.8%, 22.8%, and 6.2% of patients achieved the primary outcome in 4 mg, 2 mg and placebo groups, respectively, which was statistically significant; with comparable results seen in BRAVE-AA2. Most adverse events were mild-to-moderate (Table 2) with serious adverse events being rare. Abnormal laboratory tests were similar to other JAK inhibitors studies for other indications, including decrease in haemoglobin and neutrophil count, and elevated platelet count, creatinine kinase (CPK) and lipids. Lipid levels were raised in 25–40% of patients across the baricitinib-treated participants. One patient discontinued treatment due to anaemia.
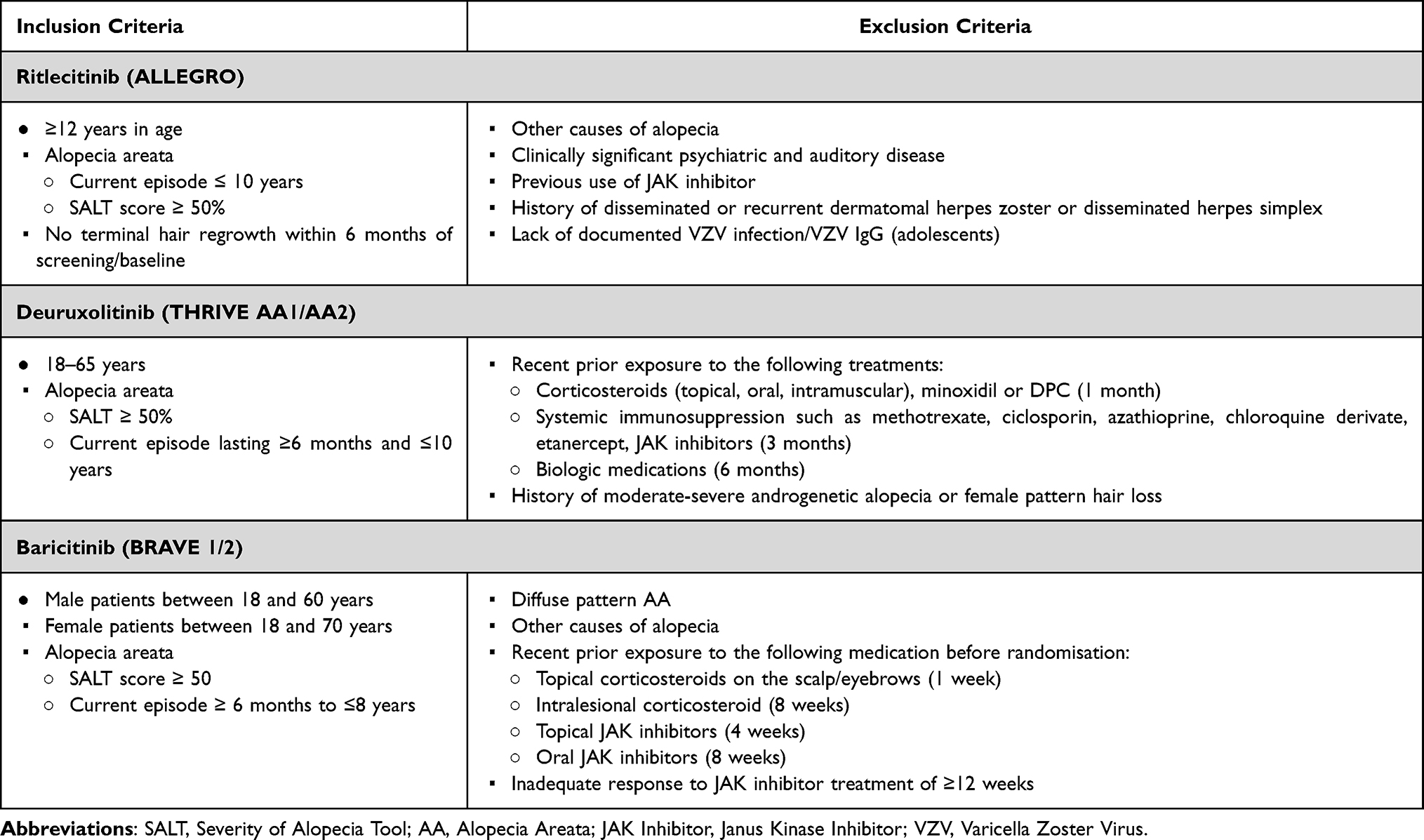 |
Table 1 Key Eligibility Criteria from Phase 3 Clinical Trials of Licensed AA Treatments |
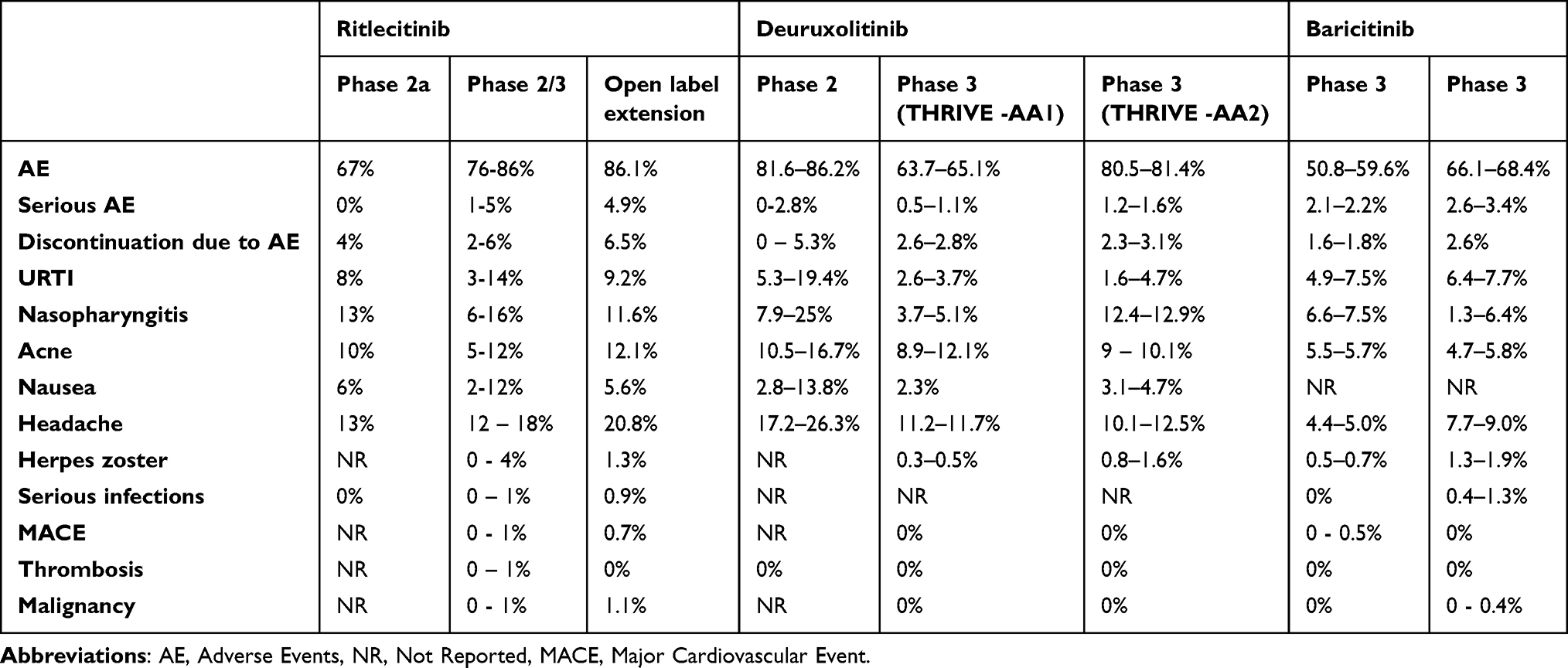 |
Table 2 Summary of Adverse Effects in RCTs Investigating JAKi (Ritlecitinib, Deuruxolitinib and Baricitinib) for the Treatment of Alopecia Areata. Ranges Reflect Dose Variations Across a Study |
More recently, open label extension study data has been reported providing insights through trajectory analysis into treatment response rates, speed to response and prognostic factors. King et al identified different response patterns, dividing participants into early responders (33% of participants), gradual responders (28%), late responders (8%) and non-responders (31%) when followed up for 52 weeks.60 More extensive disease and longer hair loss episode durations were associated with lower response rates and slower time to achieve regrowth. Further, sudden dose reduction or treatment cessation frequently resulted in disease relapse, suggesting (at least in extensive disease) that ongoing therapy is required to maintain control.61
Ritlecitinib
Ritlecitinib selectively inhibits JAK 3 and the tyrosine kinase expressed in hepatocellular carcinoma (TEC). A proof-of-concept phase 2a study investigating ritlecitinib in AA was conducted in 2021, comparing efficacy to placebo and another JAK inhibitor brepocitinib.62 This was followed by a phase 2b-3 study recruiting both adults and adolescents ≥12 years63 (Table 1). Several doses were explored, including loading-based and maintenance only regimens (10–50 mg). The primary endpoint was achievement of an absolute SALT ≤20 at week 24 and was observed in 14–31% of patients receiving ritlecitinib compared with 2% of those receiving placebo; this difference was statistically significant. A dose-response relationship was observed, and the treatment effect was maintained across disease severity and age subgroup analyses. Patient reported outcomes were consistent with primary outcome results. The most common adverse events are reported in Table 2.
A 24-month open label uncontrolled unblinded extension was conducted, assessing longer term safety and durability of response demonstrating ongoing improvement over time.64 Severe disease took longer to respond to treatment, with the proportion of patients achieving SALT score ≤20 being lowest among those with a baseline SALT score of 100. Over 60% of patients had a ≥2 grade improvement in eyebrow and eyelash growth from baseline or a normal score at month 24. The most common AEs were comparable to previous studies, though they reported a higher number of positive SARS-CoV-2 test results likely due to study being conducted during the pandemic. A higher number of serious adverse events were observed as expected with longer follow up (Table 2). Additionally, the attrition rate was 28% over the 24-month follow-up. As with baricitinib, extensive disease, longer episode durations and male sex were associated with poorer and slower responses.65
Deuruxolitinib
Efficacy data for deuruxolitinib, a selective JAK1 and JAK2 inhibitor, in the treatment of AA was published in a phase 2 RCT.66 Following this, THRIVE-AA167 and THRIVE-AA268 were two parallel Phase 3 RCTs conducted over a 24-week period followed by an open-label extension. Here, 8 mg and 12 mg BD dosing regimens were investigated. Patients had severe disease at study entry (mean SALT score 85) (Table 1). The primary efficacy endpoint in both studies was the proportion of patients achieving a SALT score ≤20 at week 24 and key secondary endpoints evaluated patient-reported treatment satisfaction at week 24 and SALT scores of ≤20 at different time intervals throughout the study period. Across the two studies, 29.6–33% of patients receiving 8 mg BD, 38.3–41.5% receiving 12 mg BD, and 0.8% receiving placebo achieved the primary endpoint. All key secondary outcomes also favoured the active treatment cohorts over placebo, with statistically significant results in both trials. In THRIVE-AA1, pyrexia and meningitis were reported in a single patient, which resolved. Laboratory abnormalities were consistent with other JAK inhibitor studies. In THRIVE-AA1, one patient discontinued deuruxolitinib due to anaemia, three because of an increased platelet count and one due to elevated lipase. In THRIVE-AA2, 3 patients discontinued treatment due to neutropenia and 2 patients due to anaemia.
Although no thromboembolic events occurred in the double-blind phase, five thromboembolic events were reported in the long-term open label extension phase of the study, including pulmonary embolism (PE) in three patients. As the majority (including all 3 episodes of PE) occurred in the 12 mg twice daily dose cohort, these patients were switched to the 8 mg twice daily dose,67 and only the 8 mg BD dose was taken forward for market authorisation in the US. Interestingly, deuruxolitinib is metabolised via the CYP2C9 pathway, with poor metabolisers at higher risk of adverse event. Pre-treatment genetic testing for CYP2C9 metabolism status is now mandated by the FDA as part of their market authorisation.
Which JAKi is Best for Treating AA?
It is currently challenging to answer this question as there are no published studies directly comparing each JAKi head-to-head. Further, due to funding and licensing restrictions, many countries will not have developed, as yet, clinical experience across all the different licenced options. Therefore, the best evidence we have is indirect comparison of published RCTs using network meta-analysis approaches. From these, we see a clear dose-response pattern across each JAKi tested, with higher doses of a particular JAKi providing better efficacy. However, these higher doses also appear associated with higher risk of adverse events. For example, deuruxolitinib 12 mg BD dose performed best for efficacy in these analyses,69,70 yet, for commercial reasons, the deuroxetitinib 8 mg BD dose was chosen for FDA submission, reflecting the complex balance between dose-dependent efficacy and safety on this treatment class.
Interestingly, it is possible that several of the available JAKi may still not have found their optimal dose for this indication, as suggested by the current RCT underway for ritlecitinib comparing the licensed 50 mg daily dose vs. 100 mg daily dose.71 Further, with the development of personalised medicine, it is likely that targeting different components of the JAK pathway with different agents may favour certain patients over others, based on the specific disrupted pathways seen at an individual level (eg., JAK1 vs. JAK3, etc).
Future Therapies
Review of the NIH clinical trials database (https://clinicaltrials.gov/; last accessed 26th January 2026) highlights several novel (ie., non-JAKi) molecular targets for AA currently being progressed by different pharmaceutical companies, at different stages of development. This is important as to address the ongoing unmet need for people unresponsive, intolerant or contra-indicated to JAKi therapy. Although some treatments will ultimately be unsuccessful (eg., esterimod did not achieve its primary outcome measure in a recent phase 2 RCT in AA),72 it is encouraging the range and diversity of molecular targets under development, giving hope that new options will be available in the foreseeable future.
See Table 3 that provides an overview of the research pipeline of registered AA trials.
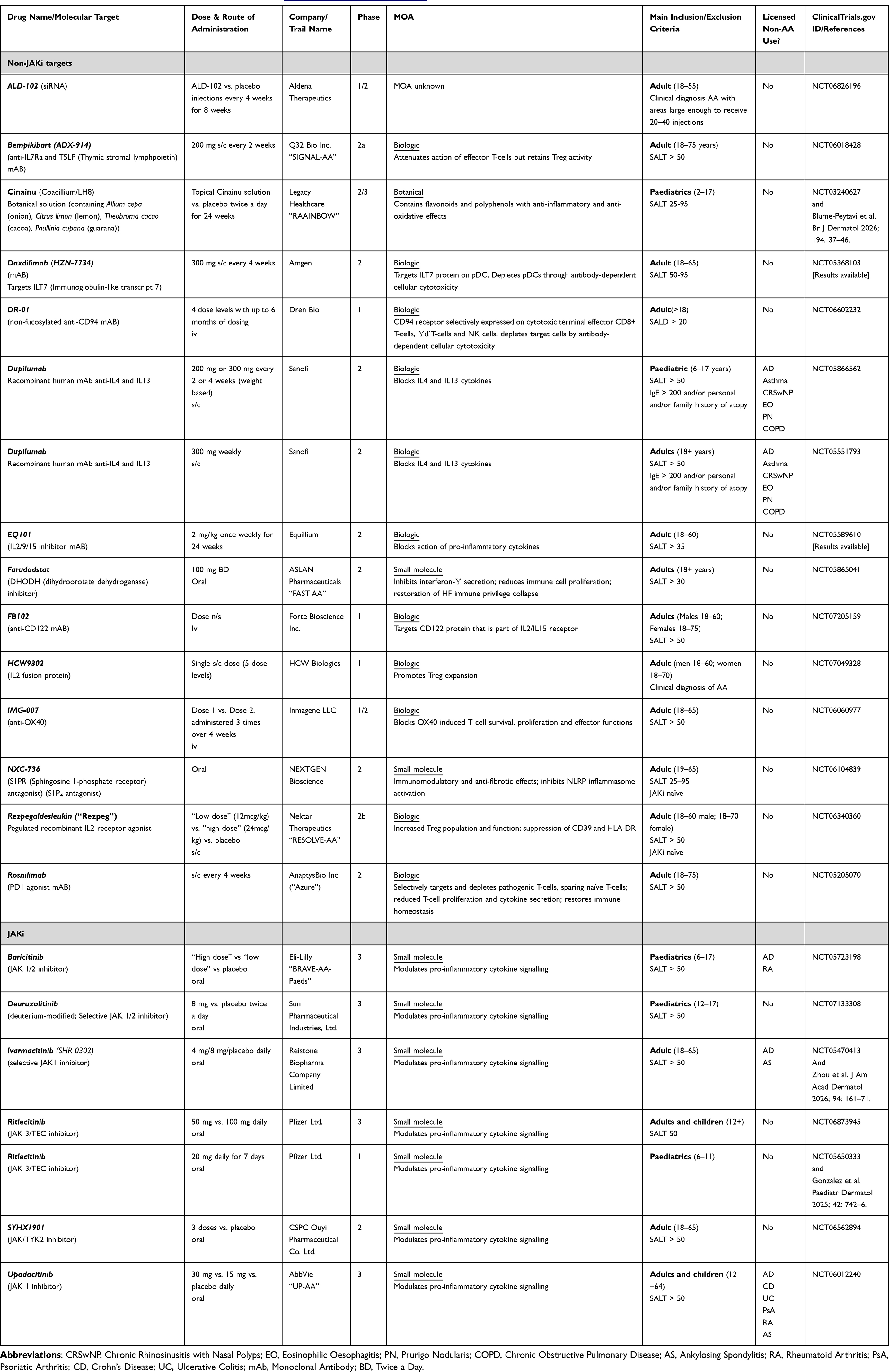 |
Table 3 The Alopecia Areata Clinical Trial Pipeline from https://www.ClinicalTrials.gov – Last Accessed 26th January 2026 |
Importance of Real-World Data
Getting a new therapy market authorisation (“licensing”) is an important, expensive and time-consuming process; however, appraisal of the therapy does not stop when market approval is achieved. Post-marketing pharmacovigilance is a component of real-world data (RWD) collection that is vital in understanding the longer-term risks of a treatment and is a common period in a therapy’s lifecycle where serious side effects are identified. A striking example in dermatology was the withdrawal of the humanized anti-CD11a monoclonal antibody Efalizumab (Raptiva®; Genotech/Merck Serono) for psoriasis following post-marketing identification of several cases of multifocal leukoencephalopathy that had not been identified throughout the Phase 1–3 trial programme. Thus, highlighting the need for continued vigilance with newer therapies with RWD is an important data source for clinicians, patients and regulators in appraising ongoing treatment choices as new data becomes available – the definition of informed consent.
Double-blind (placebo-controlled) RCTs are the gold-standard for initial assessment of a treatment to support licensing. However, it is important to appreciate that RCTs are designed and powered to show efficacy of the therapy. With relatively short trial durations, limited total numbers of participants, and participant restrictions (with strict inclusion/exclusion criteria), they have a lower ability to identify rare or longer-term adverse events. The use of these inclusion and exclusion criteria allows study of a homogeneous population, but also commonly excludes potential participants with co-morbidities and polypharmacy who are inherently at higher risk of developing treatment side effects.73 For example, patients with psoriasis who are deemed ineligible for RCTs have been found to experience lower biologic effectiveness and higher frequency of adverse events.74 Further, RCTs often struggle to recruit a cohort representative of the population served, with minority ethnic groups and women of child-bearing potential frequently underrepresented.
Unfortunately, established pharmacovigilance approaches, mainly through enhanced reporting (eg., the MHRA “Yellow card” system that has been running since 1964 (https://yellowcard.mhra.gov.uk/), risks under-reporting of significant adverse events. They rely on spontaneous submissions from clinicians, which can be negatively impacted by clinical time pressures, indifference, litigation concerns or lack of appreciation of the findings, with off-label drug use and combination therapy affecting interpretation of these results.
Another approach to post-marketing pharmacovigilance is routinely collected healthcare data through primary-care database resources; examples in the UK are the Clinical Practice Research Datalink (CPRD; (https://www.cprd.com/)) and Royal College of General Practitioners – Research Surveillance Centre (RCGP-RSC; (https://www.rcgp.org.uk/representing-you/research-at-rcgp/research-surveillance-centre)). These resources allow analysis of pseudo-anonymised primary care data from several thousand GP practices, representing several million patients, whose demographic spread is broadly representative of the UK population. However, analysis of these data is challenging due to various factors, including “raw” data (limited to what is recorded in the consultation) and reliant on accurate documentation and coding. Accurate diagnosis, treatment response and adverse event recording are particularly challenging in conditions like AA where training and experience are limited, and, superficially, other hair loss diseases may appear similar. Further, data analysis from these databases is project specific, retrospective, expensive and time consuming, and requires significant skill and expertise to analyse appropriately.75
With the above issues, development of specific disease registers has become more popular, providing an important additional post-marketing level of pharmacovigilance.76 Disease registers (also termed disease registries) are defined as
An organized system that uses observational study methods to collect uniform data (clinical and other) to evaluate specified outcomes for a population defined by a particular disease, condition, or exposure, and that serves one or more predetermined scientific, clinical, or policy purposes.76
They allow collection of high-quality prospective real-world data that are designed to answer clinically relevant questions that cannot be answered with traditional spontaneous reporting approaches, including longer-term safety and effectiveness. Registries are inherently more representative of real-world practice than RCTs as the population of interest is studied directly, incorporating real-life variations in dose, exposure time, combination treatments and patient characteristics to provide a clearer impact of the treatment on response and safety. Further, linkage data to key national data collections (eg., cancer and mortality registers), harmonisation of data to allow pooling and analysis of data through international collaborative networks, and linked bioresources (eg., for biomarker identification) can further enhance these approaches.
However, disease registers are not without their limitations. Treatments are allocated prior to register entry introducing channelling bias, as therapies are selected based on disease severity, age, comorbidities and treatment failure rather than at random. Additionally, missing data remain a challenge, although this may be partially mitigated through linkage data and statistical methods such as multiple imputation. Further, registration is voluntary and does not capture all patients prescribed systemic therapy in a particular population. Also, registers are expensive to run, time consuming, require specialist knowledge to establish and maintain, and demand long follow-up periods with large participant numbers to provide legitimate results. However, notwithstanding these concerns, disease registers hold a specific place in informing clinical decision making, health technology assessments and shaping guidelines going forward.73
The British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR) as an Exemplar
The British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR) is a prospective pharmacovigilance register based in the UK and Republic of Ireland (ROI) (https://www.badbir.org/). This register was established in 2007 as a prospective observational study with the primary aim to collect long-term safety data on patients receiving biologic therapy for psoriasis, and secondary aims to assess treatment effectiveness in this patient group.77
BADBIR has been particularly successful in engaging the UK dermatology community with 168 centres across the UK and ROI actively participating, so that together over 20,000 people with psoriasis have now been recruited, representing more than 110,000 patient episodes,78 collecting data on all current and novel systemic therapies for psoriasis, amounting to at least 38 different agents.77 National research infrastructure support for BADBIR from the NIHR has allowed smaller and traditionally less research-active dermatology departments to take part, and national guideline recommendations that all patients commencing biologic therapy should be considered for inclusion in this project has further supported engagement.79
The impact BADBIR has had on research and clinical practice is significant. For example, the register has enabled comparison of novel treatments to more conventional systemic psoriasis treatments, providing a pragmatic alternative to large head-to-head comparator studies.80,81 Additionally, BADBIR provides opportunities for collaboration with other international registries, as highlighted by a study by Phan et al who compared adalimumab originator to its biosimilar using BADBIR, French national health data and the Spanish BIOBADADERM register82 producing real world data to support biosimilar switch policies.
BADBIR has been particularly important in informing clinical practice. Analysis of biologic drug survival with age stratification has allowed clinicians to better understand patient behaviour and response. For example, BADBIR has shown that: 1) younger patients were more likely to stop biologic therapy due to ineffectiveness, whereas older patients were more likely to cease treatment due to adverse effects;81 2) similar drug survival rates are observed between secukinumab and ustekinumab with lower rates for adalimumab, with differences associated with previous biologic exposure and a concomitant diagnosis of psoriatic arthritis;83 and 3) no significant difference in incident malignancy risk was identified between psoriasis patients using biologic therapy compared conventional therapies.84,85 All these examples have had a material impact on how clinicians manage their patients and inform guideline recommendations.86
Safety, Effectiveness and Real-World Data in AA
The examples outlined above illustrate the importance of ongoing RWD collection. This is now a priority to the dermatology community as new AA therapies are introduced to inform our clinical management decisions. Experience of treatment use for other indications is helpful in identifying safety signals; however, the relevance of a particular finding in a different patient group that may have strikingly different demographics, co-morbidities or risk profiles is still unclear. An example of this are the reports of increased thromboembolic and cardiovascular risk and higher rates of nonmelanoma skin cancers in rheumatoid arthritis patients treated with the JAK-inhibitor tofacitinib. These data prompted regulators in the US, Europe and UK to issue a “black box” warning for all JAK inhibitors across all indications.87 However, without long-term real-world comparative data, it is unclear whether AA patients carry the same or similar risks with these agents.
Undoubtedly, the introduction of new therapies presents new uncertainties. This was reflected in a survey of dermatology clinician attendees at the British Association of Dermatologists (BAD) annual meeting in 2024, where a sizable proportion of dermatologists felt they lacked experience in managing severe AA and using JAK-inhibitors, and specific concerns about short- and longer-term safety of these agents were commonly cited.27
Published RWD in AA
Published RWD in AA currently utilises three main investigational approaches: 1) cross-sectional clinician/patient surveys, 2) database searches and 3) cohort studies.
Cross-Sectional Surveys
Several cross-sectional surveys have been published centred on the Adelphi AA Disease Specific Programme® (DSP), where the same methodology has been used to generate data from different countries, including US, Japan and several European countries and at different timepoints.88–94 Each study provides a cross-sectional “point in time” assessment of real-world practice through linked clinician and patient surveys exploring current management practices, treatment preferences, disease burden, economic burden and patient satisfaction, using standardised patient record data collection and patient reported outcomes. The limitations of this approach are the retrospective nature and single timepoint of the assessment (requiring repeat assessment to identify changes in practice), the potential for selection bias (as only patients attending appointments on treatment are assessed) and that severity rating was allocated based on clinician-determined assessment as opposed to defined standardised severity criterion. The latter point may impact severity and health utility data confidence with this approach particularly as these sources have been used in health technology assessment appraisals submissions (eg., NICE; https://www.nice.org.uk).
Database Studies
Using insurance claims databases is a methodological approach that has been employed to interrogate larger US, UAE and Japanese databases for insurance claims related to AA.95–98 Here AA-cohorts can be compared with matched non-AA cohorts to explore disease incidence, disease severity, associated co-morbidities, and treatment-related adverse events, as well as health resource utilisation and financial burden. The strength of this approach is the large numbers of patient episodes captured, with several thousand affected patients often identified. However, these studies are limited by their descriptive retrospective nature where the quality of data is reliant on accurate coding. Also, only insured patients are captured in the data collection, with different insurance policy criteria potentially excluding certain groups (eg., low income; certain comorbidities, etc)., thereby limiting generalizability of these data.
Using a slightly different approach, Huang et al assessed safety of ritlecitinib using the FDA adverse event reporting system database, a post-marketing repository populated predominantly from the US, but also Puerto Rico and Japan. Safety signals were identified where ritlecitinib increased the likelihood of triggering specific adverse event. Known adverse events identified included headache, raised CPK, urticaria, acne, infections and drug hypersensitivity; however, new adverse events, including diabetes mellitus, hair colour change (ie., white hair growth), thyroid disorders and lipid abnormalities were identified, although several of these signals are likely related to the disease process (white hair growth) or known autoimmune associations.99
Patient Cohorts
The medical literature is littered with case reports, case series and cohort studies in AA. These studies have helped inform therapy, particularly with off-label treatment option being used before robust clinical trial data was available; off-label data for tofacitinib use in AA is a good recent example.100 However, here we focus on treatments with market authorisation for AA. Most studies are single centre retrospective descriptive studies of early experiences of using these agents. They help to confirm effectiveness of this treatment when used in real-world populations that may differ from cohorts included in RCTs. Specifically for AA, longer disease episode durations, no age, sex or co-morbidity restrictions, variability in disease severity, and use of combination therapies alongside the JAKi treatment will differ in these cohorts compared with RCT data (Table 1).
For baricitinib, most studies are retrospective, single centre cohort studies of limited patient numbers and treatment duration. There is significant heterogeneity between cohorts and variability in outcome measure collected. Most provide effectiveness and safety data in comparison with published RCT data, validating the RCT findings, but only providing limited new insights into therapy.101–118 For example, by far the largest study with the longest follow-up period was a retrospective multicentre Italian study of 253 patients with severe AA (mean SALT 93.7) treated with baricitinib 4 mg daily over 48 months. Here, 63.2% achieved an absolute SALT <20 at 48 months, with adverse events reported in 9.4%.106 Although Caldarola et al did explore treatment responses in those patients with longer disease episodes that would have excluded them from the BRAVE clinical trial programme.117 Longer-term cohorts have identified “slow” and “very slow” responders where clinically meaningful hair regrowth may only occur between 52 and 104 weeks, suggesting longer treatment durations may be required before judging response in some patient groups.108 Further, the role of combination therapy alongside JAKi treatment is starting to be reported, with one study highlighting the use of concomitant systemic steroids to improve regrowth rates.101
Real-world data for Ritlecitinib follows a similar pattern to baricitinib, with publications dominated by small, single-centre retrospective studies that overall reaffirm RCT findings, highlighting efficacy in both adult and adolescent populations.119–127 Interestingly, cohorts describing responses in moderate severity AA (SALT 21–49)124 children <12 years old128 and AA refractory to previous JAKi treatment (baricitinib or tofacitinib)129 offer some unique insights outside of RCT data for ritlecitinib; yet still these represent small studies with the largest cohort comprising 139 consecutive patients at a single tertiary centre.130
Real world safety data is broadly in keeping with RCT results,131 with common side effects such as acne, raised CPK, infections and lipid abnormalities frequently observed. Interestingly, weight gain has been observed in both observational and clinical trial data investigating JAK inhibitors across several drugs and indications, potentially relating to JAK2 inhibition and effects on leptin metabolism, although the evidence in AA is currently limited.132,133
None of the current published real-world cohort studies has a control group, can provide longer term safety or efficacy data or can comment on dose reduction or treatment cessation effects, due to their small sample sizes, heterogeneity of data and limited follow up periods.
Global Register of Alopecia Areata Disease Severity and Treatment Safety (GRASS)-UK
GRASS-UK is a prospective multi-centre pharmacovigilance register that has emerged from consensus involving multistakeholder groups recognising the need for high-quality prospective RWD in AA.134 The register is hosted at the University of Manchester and managed by the British Association of Dermatologists (BAD), with the set-up and pilot phase funded by the UK charities British Skin Foundation and Alopecia UK. GRASS-UK is supported by the National Institute of Health and Care Research (NIHR) infrastructure, and ongoing funding support is through relevant pharmaceutical and other external funded sources through contracts with the BAD.
GRASS-UK is designed primarily to identify uncertainties around longer-term safety and effectiveness of new therapies in moderate-severe AA, supplemented by nationally held linkage data for mortality, malignancy and hospital admissions. Secondary benefits include health economic data and clinical trial recruitment, with a planned expansion to include a linked bioresource collection to improve knowledge of disease mechanisms, responses to treatment, drug survival and to identify biomarkers to inform treatment stratification.
The pilot phase is currently underway at two sites (Salford Royal Hospital and Mersey & West Lancs Hospital) and will shortly be moving into Phase 1, which will involve expansion to approximately 15 centres with specialist hair services, before further expansion in Phase 2 to any department across the UK. Encouragingly, there appears to be an ongoing appetite for BAD members to support GRASS-UK. When BAD members were asked “How important is an alopecia areata disease register in the current climate?”, over 85% responders answered either “absolutely essential” or “very important”.27 Without engagement from clinicians and patients nationally, these large-scale projects will not be successful. For further information please contact [email protected].
GRASS-UK and GRASS-International
Importantly, GRASS-UK is part of a larger collaborative international network (GRASS-International), established to collect harmonised, real-world data in a coordinated manner across countries and healthcare systems globally. The network aims to enable comparable assessment of disease characteristics, outcomes, and treatment safety, while empowering individual national registry members to retain autonomy over local governance.
GRASS-International originated from a global collaborative network that undertook an expert eDelphi consensus process, addressing key aspects of AA diagnosis, investigation and management.42,135 Building on this network and drawing on a framework derived from methodological approaches used to develop the registry dataset of the Treatment of Atopic Eczema (TREAT) Registry Taskforce,136–139 a multistakeholder eDelphi consensus derived a high-level, AA-specific dataset. This dataset was designed to support international data harmonisation and facilitate collaboration both within AA and across dermatological disease registries.134
With investment from the Australasian Hair and Wool Research Society and the National and International Skin Registry solutions (NISR), a platform was developed that has since been implemented across 3 countries (Australia, Italy and Ireland), recruiting over 1000 patients during its pilot phase, with additional support from Pfizer Ltd. Following review, and to simplify and optimise consistent data collection, the registry is being extended to additional countries using a common data platform. Harmonisation measures will also facilitate ongoing collaboration with network members, such as GRASS-UK, who will manage data collection through self-developed platforms.
While GRASS network members will operate sovereign national registries, GRASS-International provides a shared governance and collaboration structure, enabling participating members to benefit from common standards, infrastructure, and collective expertise in registry science and data protection. This approach is intended to maximise the efficient use of limited resources, support methodological consistency, adhere to evolving research and privacy standards, and facilitate future innovation, including the integration of emerging digital technologies, such as artificial intelligence. Through this model, GRASS-International aims to support a broad and inclusive community of physicians, researchers and patients, fostering collaborative research and generating insights that reflect the diversity of real-world patient experience.
Conclusions
We are at the beginning of a treatment revolution in AA, reminiscent of the changes seen previously in other inflammatory-mediated diseases (eg., psoriasis/rheumatoid arthritis). Yet, despite the many similarities between AA and these conditions, AA is a unique disease process requiring bespoke data collection to inform clinical management going forward. Future developments, with “multi-omics” biomarker development for personalised treatment stratification and, ultimately, disease modification, are achievable but still some way off. To get to this point we need better understanding of pathogenic mechanisms, treatment responses and care infrastructure, with early treatment likely being a key target for all newly diagnosed AA patients in future care.
Ultimately, to achieve the impact and insight for AA as achieved by other inflammatory dermatology conditions (cf. BADBIR for psoriasis) we need to act now as new therapies are being established. Importantly, a global consensus is emerging that appreciated the need for prospective high-quality RWD designed to achieve a truly comprehensive assessment of treatment safety and effectiveness in AA.76,134
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
Fatimah Khoda (Data curation, methodology, visualisation, Writing – original draft, Writing – review and editing); Anne Chandidzura (methodology, Writing – original draft, Writing – review and editing), Rodney Sinclair (methodology, Writing – original draft, Writing – review and editing), Dmitri Wall (methodology, Writing – original draft, Writing – review and editing), Nekma Meah (methodology, Writing – original draft, Writing – review and editing), Matthew Harries (Conceptualization, Data curation, methodology, visualisation, Writing – original draft, Writing – review and editing). All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
MJH and AC are supported by the NIHR Manchester Biomedical Research Centre (NIHR203308). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Disclosure
FK and AC = None
RS has acted as consultant or paid speaker for, or participated in clinical trials sponsored by, Leo Pharma, Amgen, Novartis, Merck & Co., Celgene, Coherus Biosciences, Janssen, Regeneron, MedImmune, GlaxoSmithKline, Cutanea, Samson Clinical, Boehringer Ingelheim, Pfizer, MSD, Oncobiologics, Roche, Eli Lilly and Bayer. He is the current President of the Australasian Hair and Wool Research Society.
DW has received personal fees (honoraria) from Janssen, (consultancy fees) Eli-Lilly and non-financial support (travel fees/grant) from Pfizer. He has received personal fees for consultancy from the not-for-profit company, National and International Skin Registry Solutions (NISR).
NM has received consultancy fees/Honoraria from Eli‐Lilly, Dermal, Pfizer and Sun Pharma.
MH has received speaker/consultancy fees (paid to his institution) from Abbvie, Pfizer, Eli Lilly, Legacy Healthcare and Sun Pharma; has received research grants from UCB and Pfizer; he is the CI/PI on clinical trials for Manentia, Abbvie, and Sanofi.
References
1. Han G. The changing landscape of alopecia areata: an introduction. Adv Ther. 2017;34(7):1584–20. doi:10.1007/s12325-017-0544-5
2. Wang ECE, Christiano AM. The changing landscape of alopecia areata: the translational landscape. Adv Ther. 2017;34(7):1586–1593. doi:10.1007/s12325-017-0540-9
3. Renert-Yuval Y, Guttman-Yassky E. The changing landscape of alopecia areata: the therapeutic paradigm. Adv Ther. 2017;34(7):1594–1609. doi:10.1007/s12325-017-0542-7
4. Starace M, Pampaloni F, Quadrelli F, et al. STRIAA (Severity trichoscopy index alopecia areata): validation of a novel trichoscopic tool for evaluation of alopecia areata. Dermatol Ther. 2025;15(1):223–226. doi:10.1007/s13555-024-01313-x
5. Harries M, Macbeth AE, Holmes S, et al. The epidemiology of alopecia areata: a population-based cohort study in UK primary care. Br J Dermatol. 2022;186(2):257–265. doi:10.1111/bjd.20628
6. Thompson AR, Tziotzios C, Nesnas J, Randall R, Czachorowski M, Messenger AG. Lifetime incidence and healthcare disparities in alopecia areata: a UK population-based cohort study. Br J Dermatol. 2024;191(6):924–935. doi:10.1093/bjd/ljae307
7. Harries M, Macbeth AE, Holmes S, et al. Epidemiology, management and the associated burden of mental health illness, atopic and autoimmune conditions, and common infections in alopecia areata: protocol for an observational study series. BMJ Open. 2021;11(11):e045718. doi:10.1136/bmjopen-2020-045718
8. Petukhova L, Duvic M, Hordinsky M, et al. Genome-wide association study in alopecia areata implicates both innate and adaptive immunity. Nature. 2010;466(7302):113–117. doi:10.1038/nature09114
9. Xing L, Dai Z, Jabbari A, et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nat Med. 2014;20(9):1043–1049. doi:10.1038/nm.3645
10. Messenger AG, Slater DN, Bleehen SS. Alopecia areata: alterations in the hair growth cycle and correlation with the follicular pathology. Br J Dermatol. 1986;114(3):337–347. doi:10.1111/j.1365-2133.1986.tb02825.x
11. Paus R, Bertolini M. The role of hair follicle immune privilege collapse in alopecia areata: status and perspectives. J Investig Dermatol Symp Proc. 2013;16(1):S25–7. doi:10.1038/jidsymp.2013.7
12. McElwee KJ, Gilhar A, Tobin DJ, et al. What causes alopecia areata? Exp Dermatol. 2013;22(9):609–626. doi:10.1111/exd.12209
13. Paus R. The evolving pathogenesis of alopecia areata: major open questions. J Investig Dermatol Symp Proc. 2020;20(1):S6–s10. doi:10.1016/j.jisp.2020.04.002
14. Paus R, Bulfone-Paus S, Bertolini M. Hair follicle immune privilege revisited: the key to alopecia areata management. J Investig Dermatol Symp Proc. 2018;19(1):S12–s17. doi:10.1016/j.jisp.2017.10.014
15. Chu SY, Chen YJ, Tseng WC, et al. Comorbidity profiles among patients with alopecia areata: the importance of onset age, a nationwide population-based study. J Am Acad Dermatol. 2011;65(5):949–956. doi:10.1016/j.jaad.2010.08.032
16. Han TY, Lee JH, Noh TK, et al. Alopecia areata and overt thyroid diseases: a nationwide population-based study. J Dermatol. 2018;45(12):1411–1417. doi:10.1111/1346-8138.14648
17. Macbeth AE, Holmes S, Harries M, et al. The associated burden of mental health conditions in alopecia areata: a population-based study in UK primary care. Br J Dermatol. 2022;187(1):73–81. doi:10.1111/bjd.21055
18. Asfour L, Solomon E, Montgomery K, Harries M. The emotional impact of alopecia and role of psychological interventions in supporting patients with hair loss. Clin Exp Dermatol. 2025;51(1):133–134. doi:10.1093/ced/llaf372
19. Hay RJ, Johns NE, Williams HC, et al. The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol. 2014;134(6):1527–1534. doi:10.1038/jid.2013.446
20. Jeon JJ, Lee S, Kim MS, et al. The burden of alopecia areata among United States, 2000-2021: a systematic analysis for the Global Burden of Disease Study 2021. J Am Acad Dermatol. 2025;93(6):1619–1621. doi:10.1016/j.jaad.2025.08.047
21. Karimkhani C, Boyers LN, Naghavi M, et al. The global burden of disease associated with alopecia areata. Br J Dermatol. 2015;172(5):1424–1426. doi:10.1111/bjd.13559
22. Zucchelli F, Harries M, Messenger A, Montgomery K. Establishing the financial burden of alopecia areata and its predictors. Skin Health Dis. 2024;4(1):e301. doi:10.1002/ski2.301
23. Burns LJ, Mesinkovska N, Kranz D, Ellison A, Senna MM. Cumulative life course impairment of alopecia areata. Int J Trichol. 2020;12(5):197–204. doi:10.4103/ijt.ijt_99_20
24. Sinclair RD. Alopecia areata and suicide of children. Med J Aust. 2014;200(3):145. doi:10.5694/mja13.10895
25. De Vere Hunt I, McNiven A, McPherson T, Vere Hunt I. A qualitative exploration of the experiences of adolescents with alopecia areata and their messages for healthcare professionals. Br J Dermatol. 2021;184(3):557–559. doi:10.1111/bjd.19598
26. Coppinger AJ, Wambier CG, Mostaghimi A, et al. Evaluation of eyebrow and eyelash regrowth and patient satisfaction in the phase 3 THRIVE-AA2 trial of deuruxolitinib in adult patients with alopecia areata. J Am Acad Dermatol. 2025;92:(6):e203–e204. doi:10.1016/j.jaad.2024.11.086
27. Harries M, Al-Nuaimi Y, Wall D, Chandidzura A, Ahmed S, Meah N. The global register of alopecia areata disease severity and treatment safety - United Kingdom (GRASS-UK): importance of real-world data in alopecia areata. Clin Exp Dermatol. 2025;50(6):1250–1252. doi:10.1093/ced/llaf055
28. MacDonald Hull SP, Wood ML, Hutchinson PE, Sladden M, Messenger AG. Guidelines for the management of alopecia areata. Br J Dermatol. 2003;149(4):692–699. doi:10.1046/j.1365-2133.2003.05535.x
29. Messenger AG, McKillop J, Farrant P, McDonagh AJ, Sladden M. British Association of Dermatologists’ guidelines for the management of alopecia areata 2012. Br J Dermatol. 2012;166(5):916–926. doi:10.1111/j.1365-2133.2012.10955.x
30. Harries MJ, Ahmed A, Ascott A, et al. British Association of Dermatologists living guideline for managing people with alopecia areata 2025. Br J Dermatol. 2025;192:190–205. doi:10.1093/bjd/ljaf452
31. Olsen E, Hordinsky M, McDonald-Hull S, et al. Alopecia areata investigational assessment guidelines. National Alopecia Areata Foundation. J Am Acad Dermatol. 1999;40(2 Pt 1):242–246. doi:10.1016/s0190-9622(99)70195-7
32. Olsen EA, Hordinsky MK, Price VH, et al. Alopecia areata investigational assessment guidelines--Part II. National Alopecia Areata Foundation. J Am Acad Dermatol. 2004;51(3):440–447. doi:10.1016/j.jaad.2003.09.032
33. Wyrwich KW, Kitchen H, Knight S, et al. The Alopecia Areata Investigator Global Assessment scale: a measure for evaluating clinically meaningful success in clinical trials. Br J Dermatol. 2020;183(4):702–709. doi:10.1111/bjd.18883
34. King BA, Senna MM, Ohyama M, et al. Defining severity in alopecia areata: current perspectives and a multidimensional framework. Dermatol Ther. 2022;12(4):825–834. doi:10.1007/s13555-022-00711-3
35. Kushnir-Grinbaum D, Bokhari L, Frewen J, et al. Systemic treatment of moderate to severe alopecia areata in adults: updated australian expert consensus statement. Australas J Dermatol. 2025;66(7):e444–e460. doi:10.1111/ajd.14597
36. Senna M, Ko J, Glashofer M, et al. Predictors of QOL in patients with alopecia areata. J Invest Dermatol. 2022;142(10):2646–2650.e3. doi:10.1016/j.jid.2022.02.019
37. Wall D, Rees H, Bokhari L, Meah N, York K, Sinclair R. Signposts to the promised land in alopecia areata. J Invest Dermatol. 2023;143(1):9–10. doi:10.1016/j.jid.2022.08.031
38. Lenane P, Macarthur C, Parkin PC, et al. Clobetasol propionate, 0.05%, vs hydrocortisone, 1%, for alopecia areata in children: a randomized clinical trial. JAMA Dermatol. 2014;150(1):47–50. doi:10.1001/jamadermatol.2013.5764
39. Gregoire S, McIntosh B, Sanchez K, Biba U, Mostaghimi A. Local corticosteroids for alopecia areata: a narrative review. Dermatol Ther. 2025;15(7):1607–1631. doi:10.1007/s13555-025-01421-2
40. Wynne MD, Harries T, Hennegan C, O’Donoghue N, Cummins DM, Harries M. Vibration assisted analgesia during intralesional corticosteroid therapy for alopecia. Skin Health Dis. 2024;4(3):e363. doi:10.1002/ski2.363
41. Frewen J, Alsaadi D, Asfour L, et al. Prescribing patterns amongst UK dermatologists for the treatment of alopecia areata, female pattern hair loss, and frontal fibrosing alopecia. JEADV Clinical Practice. 2025;4(1):72–81. doi:10.1002/jvc2.495
42. Meah N, Wall D, York K, et al. The Alopecia Areata Consensus of Experts (ACE) study: results of an international expert opinion on treatments for alopecia areata. J Am Acad Dermatol. 2020;83(1):123–130. doi:10.1016/j.jaad.2020.03.004
43. Yee BE, Tong Y, Goldenberg A, Hata T. Efficacy of different concentrations of intralesional triamcinolone acetonide for alopecia areata: a systematic review and meta-analysis. J Am Acad Dermatol. 2020;82(4):1018–1021. doi:10.1016/j.jaad.2019.11.066
44. Suchonwanit P, Kositkuljorn C, Mahasaksiri T, Leerunyakul K. A comparison of the efficacy and tolerability of three corticosteroid treatment regimens in patients with alopecia areata. J DermatolTreat. 2022;33(2):756–761. doi:10.1080/09546634.2020.1773384
45. Kurosawa M, Nakagawa S, Mizuashi M, et al. A comparison of the efficacy, relapse rate and side effects among three modalities of systemic corticosteroid therapy for alopecia areata. Dermatology. 2006;212(4):361–365. doi:10.1159/000092287
46. Vañó-Galván S, Hermosa-Gelbard Á, Sánchez-Neila N, et al. Pulse corticosteroid therapy with oral dexamethasone for the treatment of adult alopecia totalis and universalis. J Am Acad Dermatol. 2016;74(5):1005–1007. doi:10.1016/j.jaad.2015.12.026
47. Lai VWY, Sinclair R. Utility of azathioprine, methotrexate and cyclosporine as steroid-sparing agents in chronic alopecia areata: a retrospective study of continuation rates in 138 patients. J Eur Acad Dermatol Venereol. 2020;34(11):2606–2612. doi:10.1111/jdv.16858
48. Joly P, Lafon A, Houivet E, et al. Efficacy of methotrexate alone vs methotrexate plus low-dose prednisone in patients with alopecia areata totalis or universalis: a 2-step double-blind randomized clinical trial. JAMA Dermatol. 2023;159(4):403–410. doi:10.1001/jamadermatol.2022.6687
49. Husein-ElAhmed H, Steinhoff M. Efficacy and predictive factors of cyclosporine A in alopecia areata: a systematic review with meta-analysis. J DermatolTreat. 2022;33(3):1643–1651. doi:10.1080/09546634.2021.1886230
50. Phan K, Ramachandran V, Sebaratnam DF. Methotrexate for alopecia areata: a systematic review and meta-analysis. J Am Acad Dermatol. 2019;80(1):120–127.e2. doi:10.1016/j.jaad.2018.06.064
51. Farshi S, Mansouri P. Efficacy and safety of long-term azathioprine therapy for severe alopecia areata: a 10-year cohort study. J Cosmet Dermatol. 2025;24(5):e70187. doi:10.1111/jocd.70187
52. Vañó-Galván S, Hermosa-Gelbard Á, Sánchez-Neila N, et al. Treatment of recalcitrant adult alopecia areata universalis with oral azathioprine. J Am Acad Dermatol. 2016;74(5):1007–1008. doi:10.1016/j.jaad.2015.12.055
53. Gupta P, Verma KK, Khandpur S, Bhari N. Weekly azathioprine pulse versus betamethasone oral mini-pulse in the treatment of moderate-to-severe alopecia areata. Indian J Dermatol. 2019;64(4):292–298. doi:10.4103/ijd.IJD_481_16
54. Lee S, Kim BJ, Lee YB, Lee WS. Hair regrowth outcomes of contact immunotherapy for patients with alopecia areata: a systematic review and meta-analysis. JAMA Dermatol. 2018;154(10):1145–1151. doi:10.1001/jamadermatol.2018.2312
55. Karanovic S, Harries M, Kaur MR. Diphenylcyclopropenone for alopecia areata: a U.K. survey. Br J Dermatol. 2018;179(2):514–515. doi:10.1111/bjd.16489
56. Available from: https://www.hra.nhs.uk/planning-and-improving-research/application-summaries/research-summaries/controlled-release-formulation-of-sts01-to-treat-alopecia-areata/.
57. McMullen E, Gupta S, Pham M, et al. Combined low dose oral minoxidil and immunomodulator efficacy and safety in alopecia areata: a systematic review. Int J Dermatol. Dec 9 2025; doi:10.1111/ijd.70194
58. Montgomery K, White C, Thompson A. A mixed methods survey of social anxiety, anxiety, depression and wig use in alopecia. BMJ Open. 2017;7(4):e015468. doi:10.1136/bmjopen-2016-015468
59. King B, Ohyama M, Kwon O, et al. Two phase 3 trials of baricitinib for alopecia areata. N Engl J Med. 2022;386(18):1687–1699. doi:10.1056/NEJMoa2110343
60. King B, Shapiro J, Ohyama M, et al. When to expect scalp hair regrowth during treatment of severe alopecia areata with baricitinib: insights from trajectories analyses of patients enrolled in two Phase III trials. Br J Dermatol. 2023;189(6):666–673. doi:10.1093/bjd/ljad253
61. King B, Ko J, Kwon O, et al. Baricitinib withdrawal and retreatment in patients with severe alopecia areata: the BRAVE-AA1 randomized clinical trial. JAMA Dermatol. 2024;160(10):1075–1081. doi:10.1001/jamadermatol.2024.2734
62. King B, Guttman-Yassky E, Peeva E, et al. A phase 2a randomized, placebo-controlled study to evaluate the efficacy and safety of the oral Janus kinase inhibitors ritlecitinib and brepocitinib in alopecia areata: 24-week results. J Am Acad Dermatol. 2021;85(2):379–387. doi:10.1016/j.jaad.2021.03.050
63. King B, Zhang X, Harcha WG, et al. Efficacy and safety of ritlecitinib in adults and adolescents with alopecia areata: a randomised, double-blind, multicentre, phase 2b–3 trial. Lancet. 2023;401(10387):1518–1529. doi:10.1016/S0140-6736(23)00222-2
64. Tziotzios C, Sinclair R, Lesiak A, et al. Long-term safety and efficacy of ritlecitinib in adults and adolescents with alopecia areata and at least 25% scalp hair loss: results from the ALLEGRO-LT phase 3, open-label study. J Eur Acad Dermatol Venereol. 2025;39(6):1152–1162.
65. King B, Mirmirani P, Lo Sicco K, et al. Patterns of clinical response in patients with alopecia areata treated with ritlecitinib in the ALLEGRO clinical development programme. J Eur Acad Dermatol Venereol. 2025;39(6):1163–1173. doi:10.1111/jdv.20547
66. King B, Mesinkovska N, Mirmirani P, et al. Phase 2 randomized, dose-ranging trial of CTP-543, a selective Janus Kinase inhibitor, in moderate-to-severe alopecia areata. J Am Acad Dermatol. 2022;87(2):306–313. doi:10.1016/j.jaad.2022.03.045
67. King B, Senna MM, Mesinkovska NA, et al. Efficacy and safety of deuruxolitinib, an oral selective Janus kinase inhibitor, in adults with alopecia areata: results from the phase 3 randomized, controlled trial (THRIVE-AA1). J Am Acad Dermatol. 2024;91(5):880–888. doi:10.1016/j.jaad.2024.06.097
68. Tsianakas A, Passeron T, Magnolo N, et al. Efficacy and safety of deuruxolitinib, an oral selective Janus kinase 1/2 inhibitor, in adults with alopecia areata: results from the THRIVE-AA2 phase 3, randomized, double-blind, controlled trial. J Am Acad Dermatol. 2025. doi:10.1016/j.jaad.2025.11.070
69. Babul A, Mehta D, Soliman Y, Hussain M, Babul N. Comparative efficacy of janus kinase inhibitors indicated for severe alopecia areata: a bayesian network meta-analysis and matching-adjusted indirect comparison. J Dermatol. 2025. doi:10.1111/1346-8138.17959
70. Gupta AK, Bamimore MA, Mirmirani P, Piguet V, Talukder M. The relative efficacy and safety of monotherapies for alopecia areata: a network meta-analysis study. J Cosmet Dermatol. 2025;24(4):e70185. doi:10.1111/jocd.70185
71. King B, McMichael A, Sinclair R, et al. Rationale and design of a novel,phase 3,external and synthetic placebo-controlled clinical trial of ritlecitinib 50 mg and 100 mg for alopecia areata. Dermatol Ther. 2025;15(12):3793–3803. doi:10.1007/s13555-025-01543-7
72. King B, Mesinkovska N, Senna M, Luo X, Minkiewicz J, Selfridge A. Efficacy and safety of etrasimod in alopecia areata: a multicentre, randomized, double-blind, placebo-controlled, phase 2 study. J Eur Acad Dermatol Venereol. 2025;39(6):1174–1184. doi:10.1111/jdv.20605
73. Asfour L, Yiu ZZN, Warren RB. How is safety of dermatology drugs assessed: trials, registries, and spontaneous reporting. Expert Opin Drug Saf. 2020;19(4):449–457. doi:10.1080/14740338.2020.1746267
74. Mason KJ, Barker J, Smith CH, et al. Comparison of drug discontinuation, effectiveness, and safety between clinical trial eligible and ineligible patients in BADBIR. JAMA Dermatol. 2018;154(5):581–588. doi:10.1001/jamadermatol.2018.0183
75. Al-Janabi A, Yiu ZZN. Biologics in psoriasis: updated perspectives on long-term safety and risk management. Psoriasis. 2022;12:1–14. doi:10.2147/ptt.S328575
76. Wall D, Alhusayen R, Arents B, et al. Learning from disease registries during a pandemic: moving toward an international federation of patient registries. Clin Dermatol. 2021;39(3):467–478. doi:10.1016/j.clindermatol.2021.01.018
77. British Association of Dermatologists Biologics and Immunomodulators Register. BADBIR annual update 2025. Internet. University of Manchester. Available from: https://www.badbir.org/wp-content/uploads/sites/372/2025/11/BADBIR_newsletter_20251.pdf.
78. British Association of Dermatologists Biologics and Immunomodulators Register. British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Available from: https://www.badbir.org.
79. Smith CH, Yiu ZZN, Bale T, et al. British Association of Dermatologists guidelines for biologic therapy for psoriasis 2020: a rapid update. Br J Dermatol. 2020;183(4):628–637.
80. Alabas OA, Mason KJ, Yiu ZZN, et al. Effectiveness and survival of methotrexate versus Adalimumab in patients with moderate-to-severe psoriasis: a cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br J Dermatol. 2023;189(3):271–278. doi:10.1093/bjd/ljad179
81. Alabas OA, Mason KJ, Yiu ZZN, et al. Age and biologic survival in patients with moderate-to-severe psoriasis: a cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br J Dermatol. 2025;192(5):907–916. doi:10.1093/bjd/ljaf017
82. Phan DB, Jourdain H, Descalzo-Gallego MA, et al. Drug survival and safety of biosimilars for treating psoriasis compared with originator Adalimumab: a multinational cohort study. Br J Dermatol. 2025;192(4):641–652. doi:10.1093/bjd/ljae454
83. Yiu ZZN, Mason KJ, Hampton PJ, et al. Drug survival of adalimumab, ustekinumab and secukinumab in patients with psoriasis: a prospective cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR). Br J Dermatol. 2020;183(2):294–302. doi:10.1111/bjd.18981
84. Mason KJ. 238 The risk of keratinocyte carcinoma (KC) in psoriasis patients receiving biologic therapy compared to conventional systemic therapy: results from The British Association of Dermatologists Biologic Interventions Register (BADBIR). J Invest Dermatol. 2018;138(5):S41. doi:10.1016/j.jid.2018.03.244
85. Esse S, Alabas O, Mason K, et al. P072 Risk of incident cancer, excluding keratinocyte carcinoma, in patients with psoriasis treated with biologic therapy: a prospective cohort study from the British Association of Dermatologists Biologic and Immunomodulators Register (BADBIR), on behalf of the BADBIR Study Group. Br J Dermatol. 2024;191(Supplement_1):i48–i48. doi:10.1093/bjd/ljae090.099
86. Smith CH, Yiu ZZN, Bale T, et al. British Association of Dermatologists guidelines for biologic therapy for psoriasis 2023: a pragmatic update. Br J Dermatol. 2024;190(2):270–272. doi:10.1093/bjd/ljad347
87. Mease P, Charles-Schoeman C, Cohen S, et al. Incidence of venous and arterial thromboembolic events reported in the tofacitinib rheumatoid arthritis, psoriasis and psoriatic arthritis development programmes and from real-world data. Ann Rheum Dis. 2020;79(11):1400–1413. doi:10.1136/annrheumdis-2019-216761
88. Edson-Heredia E, Aranishi T, Isaka Y, Anderson P, Marwaha S, Piercy J. Patient and physician perspectives on alopecia areata: a real-world assessment of severity and burden in Japan. J Dermatol. 2022;49(6):575–583. doi:10.1111/1346-8138.16360
89. Ohyama M, Kamei K, Yuasa A, Anderson P, Milligan G, Sakaki-Yumoto M. Economic burden of alopecia areata: a study of direct and indirect cost in Japan using real-world data. J Dermatol. 2023;50(10):1246–1254. doi:10.1111/1346-8138.16888
90. Anderson P, Piercy J, Austin J, et al. Alopecia areata treatment patterns and satisfaction: results of a real-world cross-sectional survey in Europe. Dermatol Ther. 2024;14(12):3243–3258. doi:10.1007/s13555-024-01280-3
91. Fridman M, Ray M, Gandhi K, Shy ME, Mostaghimi A. Treatment patterns and treatment satisfaction among adults with alopecia areata in the United States. Adv Ther. 2022;39(12):5504–5513. doi:10.1007/s12325-022-02338-4
92. Nakamura K, Kamei K, Austin J, et al. Degree of alignment between japanese patients and physicians on alopecia areata disease severity and treatment satisfaction: a real-world survey. Dermatol Ther. 2024;14(1):151–167. doi:10.1007/s13555-023-01067-y
93. Vañó-Galván S, Blume-Peytavi U, Farrant P, et al. Physician- and patient-reported severity and quality of life impact of alopecia areata: results from a real-world survey in five european countries. Dermatol Ther. 2023;13(12):3121–3135. doi:10.1007/s13555-023-01057-0
94. Vañó-Galván S, Egeberg A, Piraccini BM, et al. Characteristics and management of patients with alopecia areata and selected comorbid conditions: results from a survey in five European countries. Dermatol Ther. 2024;14(4):1027–1037. doi:10.1007/s13555-024-01133-z
95. Hammadi AA, Parmar NV, Farghaly M, et al. A retrospective analysis of disease epidemiology, comorbidities, treatment patterns, and healthcare resource utilization of alopecia areata in the United Arab Emirates using claims database. J Dermatol. 2024;51(9):1157–1171. doi:10.1111/1346-8138.17381
96. Campos-Alberto E, Hirose T, Napatalung L, Ohyama M. Prevalence, comorbidities, and treatment patterns of Japanese patients with alopecia areata: a descriptive study using Japan medical data center claims database. J Dermatol. 2023;50(1):37–45. doi:10.1111/1346-8138.16615
97. Ray M, Swallow E, Gandhi K, et al. Healthcare utilization and costs among US adolescents with alopecia areata. J Health Econ Outcomes Res. 2022;9(2):11–18. doi:10.36469/001c.36229
98. George P, Jagun O, Liu Q, et al. Incidence rates of infections, malignancies, thromboembolism, and cardiovascular events in an alopecia areata cohort from a US claims database. Dermatol Ther. 2023;13(8):1733–1746. doi:10.1007/s13555-023-00937-9
99. Huang Y, Ke C, Chen M. Safety assessment of ritlecitinib based on the FDA Adverse Event Reporting System (FAERS) database: a real-world pharmacovigilance study. J Dermatol. 2025;52(10):1561–1569. doi:10.1111/1346-8138.17886
100. Guo L, Feng S, Sun B, Jiang X, Liu Y. Benefit and risk profile of tofacitinib for the treatment of alopecia areata: a systemic review and meta-analysis. J Eur Acad Dermatol Venereol. 2020;34(1):192–201. doi:10.1111/jdv.15937
101. Mourtada A, Douarec C, Wargny M, et al. Real-life effectiveness and safety of baricitinib in adults with alopecia areata: a multicentre study. J Eur Acad Dermatol Venereol. 2025;39(10):e919–e921. doi:10.1111/jdv.20657
102. Apalla Z, Zafiriou E, Zagkliverinou E, et al. Real-World experience of tofacitinib and baricitinib use in alopecia areata in Greek population: a retrospective analysis with focus on safety. Dermatol Pract Concept. 2024;14(2). doi:10.5826/dpc.1402a73
103. Katoulis AC, Pappa G, Markou E, Kanelleas A, Bozi E, Sgouros D. Baricitinib in alopecia areata: real-world data from a case series in Greece. J Eur Acad Dermatol Venereol. 2024;38(8):e671–e673. doi:10.1111/jdv.19822
104. Lee JW, Shin HT, Lee Y, Kim DY, Park J, Choi GS. Clinical efficacy and safety of baricitinib in patients with alopecia areata in Korea. Ann Dermatol. 2025;37(5):307–313. doi:10.5021/ad.25.059
105. Niki M, Kamata M, Tada Y, Kubo Y. Duration of current alopecia areata episode predicts the effectiveness of baricitinib in Japanese patients with alopecia areata: a single-center retrospective study. J DermatolTreat. 2025;36(1):2555684. doi:10.1080/09546634.2025.2555684
106. Piraccini BM, Cedirian S, Pampaloni F, et al. Effectiveness and safety of baricitinib in severe alopecia areata: 48-week results. J Eur Acad Dermatol Venereol. 2025;39:1143–1151. doi:10.1111/jdv.70067
107. Piraccini BM, Pampaloni F, Cedirian S, et al. Real-life effectiveness and safety of baricitinib in patients with severe alopecia areata: a 24-week Italian study. J Eur Acad Dermatol Venereol. 2024. doi:10.1111/jdv.20312
108. Wada-Irimada M, Takahashi T, Sekine M, et al. Long-Term Real-World outcomes of baricitinib in severe alopecia areata: a 104-week retrospective analysis from a single institute. J Dermatol. 2025. doi:10.1111/1346-8138.17829
109. Van Helmond SC, Willaert M, Nguyen VH, Nijsten T, Waalboer-Spuij R, Hijnen D. Real-world effectiveness and safety of janus kinase inhibitors in alopecia areata: a retrospective cohort study of 72 patients. Acta Derm Venereol. 2025;105:adv42990. doi:10.2340/actadv.v105.42990
110. Garcia-Nunez A, Alcala Ramirez Del Puerto A, Daza-Garcia R, et al. Predictive factors of response and real-world experience of baricitinib on alopecia areata: a single tertiary center study on a 72 patients’ cohort. Int J Dermatol. 2025;65:1040–1043. doi:10.1111/ijd.70138
111. Seneschal J, Figueras Nart L, Sabatino S, Papadimitropoulos M, Dabral S, Lampropoulou A. Real-World evidence for baricitinib in the treatment of atopic dermatitis and alopecia areata: systematic literature review 2020-2023. Dermatol Ther. 2025;15(7):1719–1754. doi:10.1007/s13555-025-01425-y
112. Aleid NM, Alhuwairini SF, Almuhana GA, Al-Aojan SA, Abanomy SA, Almohanna HM. Effectiveness of baricitinib in severe alopecia areata in real life: a retrospective study of 87 patients. Acta Dermatovenerol Alp Pannonica Adriat. 2025;34(4):183–186.
113. Lambiase S, Cavalloro D, Cioni A, et al. A 52-Week real-life study of baricitinib in moderate to severe alopecia areata: clinical, trichoscopic assessment and patient reported outcomes. J Clin Med. 2025;14(22). doi:10.3390/jcm14228170
114. Muñoz-Barba D, García-Moronta C, Haselgruber-de Francisco S, Sánchez-Díaz M, Arias-Santiago S. Effectiveness and safety of baricitinib in alopecia areata: a prospective cohort study. J DermatolTreat. 2025;36(1):2583877. doi:10.1080/09546634.2025.2583877
115. Muñoz-Barba D, García-Moronta C, Soto-Moreno A, Sánchez-Díaz M, Arias-Santiago S. Defining a therapeutic window of opportunity in alopecia areata: predictors of early response to baricitinib. J Clin Med. 2025;14(20). doi:10.3390/jcm14207312
116. Vignoli CA, Gargiulo L, Ibba L, et al. Baricitinib for the treatment of severe alopecia areata: results from a 52-week multicenter retrospective real-world study. J DermatolTreat. 2025;36(1):2444494. doi:10.1080/09546634.2024.2444494
117. Caldarola G, Pinto LM, Acri MC, et al. Effectiveness of baricitinib in alopecia areata patients with a current episode lasting longer than 8 years: an italian multicenter real-life experience in the lazio region. Int J Dermatol. 2025;64(9):1706–1707. doi:10.1111/ijd.17722
118. Gargiulo L, Ibba L, Vignoli CA, et al. Effectiveness and safety of baricitinib in patients with severe alopecia areata: a 36-week multicenter real-world experience. J DermatolTreat. 2023;34(1):2268764. doi:10.1080/09546634.2023.2268764
119. Foggia L, Nappa P, Ocampo-Garza SS, et al. Comparative clinical, trichoscopic, and safety outcomes of baricitinib, ritlecitinib, and upadacitinib in alopecia areata: a real-world experience. Clin Exp Dermatol. 2025;doi:10.1093/ced/llaf509.
120. Huang J, Jian J, Li M, et al. Real-world efficacy of ritlecitinib in treating alopecia areata across various anatomical sites: potential rapid response predictors. J Am Acad Dermatol. 2025;93(5):1236–1242. doi:10.1016/j.jaad.2025.07.008
121. Okazaki T, Takahashi T, Wada-Irimada M, et al. Ritlecitinib in alopecia areata: a 24-week real-world experience contrasting JAK inhibitor-naive and JAK inhibitor-experienced patients. J Dermatol. 2025. doi:10.1111/1346-8138.70123
122. Sheng Y, Wang Q, Tao K, et al. Real-world efficacy and safety of ritlecitinib in alopecia areata: a single-centre experience. J Eur Acad Dermatol Venereol. 2025;39(12):e996–e998. doi:10.1111/jdv.20664
123. Valtellini L, Avallone G, Murgia G, et al. Real-world assessment of ritlecitinib in patients with severe alopecia areata: a 24-week multicentre retrospective study. Clin Exp Dermatol. 2025;50(11):2297–2300. doi:10.1093/ced/llaf312
124. Xu M, Leong H, Zhu Y, et al. Evaluating the early efficacy and safety of ritlecitinib in moderate alopecia areata: a real-world, single-center study. J Am Acad Dermatol. 2025;94:618–620. doi:10.1016/j.jaad.2025.10.008
125. Zhang W, Li X, Zhang Y, Luo Y, Li H, Zhou C. Ritlecitinib in alopecia areata: a multicenter retrospective real-world analysis. J Am Acad Dermatol. 2025;93(4):1136–1137. doi:10.1016/j.jaad.2025.06.041
126. Dai R, Duan L, Li S, Zheng S, Wu X. Ritlecitinib in clinical practice: a real-world study of efficacy, safety and prior Janus kinase inhibitor impact in alopecia areata. Clin Exp Dermatol. 2025;50(9):1866–1867. doi:10.1093/ced/llaf194
127. Franzese P, Balato A, Di Brizzi EV, et al. Ritlecitinib efficacy in adolescents with alopecia areata: a real-world experience. Int J Dermatol. 2026. doi:10.1111/ijd.70330
128. Wang X, Liu Y, Sun Y, Ma L, Xu Z, Zhang B. Ritlecitinib for severe alopecia areata in children under 12 years: a retrospective review of 18 cases. J Am Acad Dermatol. 2026;94(1):280–282. doi:10.1016/j.jaad.2025.09.008
129. Huang J, Jian J, Li M, et al. Use of ritlecitinib in patients with alopecia areata refractory to tofacitinib or baricitinib: a single-center retrospective cohort study. J Am Acad Dermatol. 2026;94(1):351–353. doi:10.1016/j.jaad.2025.09.053
130. Sebastian N, Abraheem A, Chandidzura A, et al. Ritlecitinib for the treatment of severe alopecia areata: real-world experience from a UK tertiary centre. Clin Exp Dermatol. 2026. doi:10.1093/ced/llag067
131. Qi Z, Li Y. Safety of oral JAK inhibitors in treating alopecia areata: a systematic review and network meta-analysis. Front Pharmacol. 2025;16:1576553. doi:10.3389/fphar.2025.1576553
132. Ibba L, Gargiulo L, Bianco M, et al. Potential role of leptin in Janus kinase 2 inhibitor-associated weight gain: a monocentric retrospective study. Clin Exp Dermatol. 2025;50(9):1834–1837. doi:10.1093/ced/llaf144
133. Xiong G, Yu E, Heung M, Yang J, Lowe M, Abu-Hilal M. Weight gain secondary to the use of oral Janus kinase inhibitors: a systematic review and meta-analysis. JAAD Int. 2025;19:1–9. doi:10.1016/j.jdin.2024.11.009
134. Wall D, Meah N, York K, et al. A global eDelphi exercise to identify core domains and domain items for the development of a Global Registry of Alopecia Areata Disease Severity and Treatment Safety (GRASS). JAMA Dermatol. 2021;157(4):1–11. doi:10.1001/jamadermatol.2020.5839
135. Meah N, Wall D, York K, et al. The Alopecia Areata Consensus of Experts (ACE) study part II: results of an international expert opinion on diagnosis and laboratory evaluation for alopecia areata. J Am Acad Dermatol. 2021;84(6):1594–1601. doi:10.1016/j.jaad.2020.09.028
136. Gerbens LA, Boyce AE, Wall D, et al. TREatment of ATopic eczema (TREAT) Registry Taskforce: protocol for an international Delphi exercise to identify a core set of domains and domain items for national atopic eczema registries. Trials. 2017;18(1):87. doi:10.1186/s13063-016-1765-7
137. Gerbens LAA, Apfelbacher CJ, Irvine AD, et al. TREatment of ATopic eczema (TREAT) Registry Taskforce: an international Delphi exercise to identify a core set of domains and domain items for national atopic eczema photo- and systemic therapy registries. Br J Dermatol. 2019;180(4):790–801. doi:10.1111/bjd.16714
138. Spuls PI, Gerbens LAA, Apfelbacher CJ, et al. The International TREatment of ATopic Eczema (TREAT) registry taskforce: an initiative to harmonize data collection across national atopic eczema photo- and systemic therapy registries. J Invest Dermatol. 2017;137(9):2014–2016. doi:10.1016/j.jid.2017.05.014
139. Vermeulen FM, Gerbens LAA, Bosma AL, et al. TREatment of ATopic eczema (TREAT) Registry Taskforce: consensus on how and when to measure the core dataset for atopic eczema treatment research registries. Br J Dermatol. 2019;181(3):492–504. doi:10.1111/bjd.17715
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.