Back to Journals » Infection and Drug Resistance » Volume 19
Real-World Evidence and Multidrug Resistant Infections: How Can We Leverage RWE to Improve Patient Outcome with the Novel Beta-Lactam and Beta-Lactam/Beta-Lactamase Inhibitor Combinations
Received 15 November 2025
Accepted for publication 14 January 2026
Published 20 January 2026 Volume 2026:19 541584
DOI https://doi.org/10.2147/IDR.S541584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Milo Gatti,1,2 Federico Pea1,2
1Department of Medical and Surgical Sciences, Alma Mater Studiorum University of Bologna, Bologna, Italy; 2Clinical Pharmacology Unit, IRCCS Azienda Ospedaliero-Universitaria Di Bologna, Bologna, Italy
Correspondence: Federico Pea, Department of Medical and Surgical Sciences, Alma Mater Studiorum University of Bologna, Via Massarenti 9, Bologna, 40138, Italy, Tel +39 051 214 3627, Email [email protected]
Abstract: Translating findings emerged from pivotal trials of novel beta-lactams into real-world clinical practice represents a major concern. Real-world evidence assessing the efficacy of novel beta-lactams in different clinical scenarios may provide some benefits in selecting proper place in therapy. This review aims to perform a critical reappraisal of the issues emerged from pivotal trials of novel beta-lactams and leveraging real-world evidence supporting proper place in therapy in the treatment of multidrug-resistant Gram-negative infections. A comprehensive literature search was performed on PubMed-MEDLINE from January 2015 to September 2025 for identifying pivotal trials and real-world evidence concerning the use of cefiderocol and of novel beta-lactam/beta-lactamase inhibitor combination (BL/BLIc) including those of tomorrow (ie, ceftolozane-tazobactam, ceftazidime-avibactam, meropenem-vaborbactam, imipenem-relebactam, cefepime-enmetazobactam, cefepime-taniborbactam, cefepime-zidebactam, sulbactam-durlobactam, aztreonam-avibactam). Critical issues emerged from pivotal trials in terms of potential appropriate place in therapy of each included agent were summarized. Four different therapeutic algorithms were proposed according to the pattern of antibiotic susceptibility of the pathogens, the genotype of resistance, and pharmacokinetic/pharmacodynamic (PK/PD) features of selected agents: a) extended-spectrum beta-lactamase (ESBL)-producing Enterobacterales; b) carbapenem-producing Enterobacterales (CPE); c) metallo-beta-lactamase (MBL)-producing Pseudomonas aeruginosa; d) carbapenem-resistant Acinetobacter baumannii (CRAB). Real-world evidence suggested that cefepime-enmetazobactam may represent an effective carbapenem-sparing strategy in the management of infections caused by ESBL-producing Enterobacterales and a potential alternative to ceftazidime-avibactam for treating OXA-48-producing infections. Cefepime-taniborbactam, cefepime-zidebactam, and aztreonam-avibactam could finally represent a definitive answer in the challenging scenario of infections caused by MBL-producing Enterobacterales and Pseudomonas aeruginosa. Lastly, the valuable role of sulbactam-durlobactam in CRAB infections was already recognized by international guidelines. Real-world evidence concerning both well-designed observational studies and PK/PD models may represent a mandatory tool for overcoming issues associated with pivotal trials evaluating novel BL/BLIc. The implementation of dedicated well-designed real-world studies would be warranted for ensuring a constant update of proposed therapeutic algorithms.
Keywords: novel beta-lactam/beta-lactamase inhibitor combinations, real-world evidence, multidrug-resistant gram-negative infections, PK/PD optimization, place in therapy, therapeutic algorithms
Introduction
The worldwide diffusion of multidrug-resistant (MDR) Gram-negative pathogens and the ever-growing resistance spread against the currently available beta-lactams (BL) and/or beta-lactam/beta-lactamase inhibitor combinations (BL/BLIc) represent a major health concern nowadays.1–5 Some novel BL/BLIc are currently under way (ie, cefepime-enmetazobactam, cefepime-taniborbactam, cefepime-zidebactam, sulbactam-durlobactam, aztreonam-avibactam) and could represent a valuable enrichment of the therapeutic armamentarium. They could concur either in counteracting the ever-growing spread of resistance against the currently licensed BL/BLIc or in offering a solution to some unmeet clinical needs in covering peculiar pathogen-specific mechanisms of resistance (namely metallo-beta-lactamase [MBL]-producing Enterobacterales/Pseudomonas aeruginosa or carbapenem-resistant Acinetobacter baumannii [CRAB]).6–10
Figure 1A and B summarize the activity that novel BL and BL/BLIc recently licensed and under clinical development, respectively, exhibit against different types of MDR Gram-negatives.
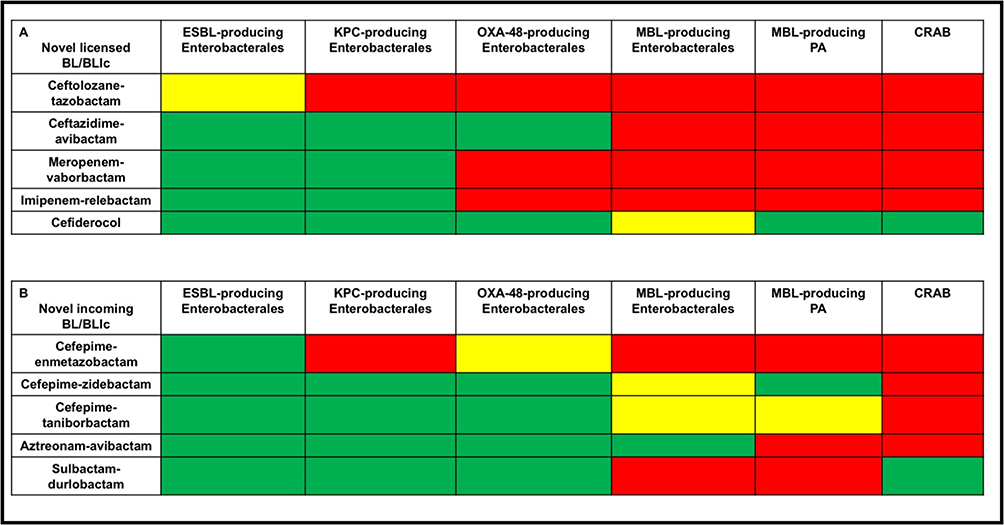 |
Figure 1 Spectrum of activity against MDR Gram-negative pathogens of novel BL and BL/BLIc both recently licensed (A) and under clinical development (B). Green box: agent with documented in vitro and/or in vivo activity and recommended in clinical practice; yellow box: agent with documented in vitro activity but some concerns may occur during clinical practice or more in vitro/in vivo data are required for clinical use; red box: lack of in vitro and/or in vivo activity and not recommended in clinical practice. Abbreviations: BL/BLIc, beta-lactam/beta-lactamase inhibitor combinations; CRAB, carbapenem-resistant Acinetobacter baumannii; ESBL, extended-spectrum beta-lactamase; MBL, metallo-beta-lactamase; PA, Pseudomonas aeruginosa. |
Unfortunately, only a minority of the pivotal trials concerning the currently licensed novel BL and/or BL/BLIc were designed as pathogen-driven study.11–14 This makes often difficult translating the emerged findings into something adding value for properly placing them in daily clinical practice. The case of ceftazidime-avibactam may be mentioned as a paradigmatic example. In the four pivotal trials of this agent, no case of infection due to carbapenem-producing Enterobacterales was included.15–18 Nevertheless, this agent has become first-line therapy for managing KPC- and OXA-48-producing Enterobacterales based on real-world evidence (RWE), as issued by both the Infectious Disease Society of America (IDSA) guidance and the European Society of Clinical Microbiology and Infectious Disease (ESCMID) guidelines.19,20 To be honest, it should be recognized that the way for implementing specific pathogen-driven randomized controlled trials (RCTs) may be burdened by a major issue. In fact, the epidemiological prevalence of some types of MDR Gram-negatives may be quite low (ie, MBL-producing Enterobacterales and/or Pseudomonas aeruginosa), so that the duration of RCTs for enrolling an high enough representative number of patients could be unacceptably too long, and the study may be stopped prematurely, as recently occurred for that of aztreonam-avibactam.21
A valuable complementary way for attributing a proper place in therapy to the incoming BL/BLIc of tomorrow could be that of planning prospective real-world specific well-design pathogen-driven observational studies.14 This approach coupled with population pharmacokinetic/pharmacodynamic (PK/PD) studies focused on selecting the most appropriate dosing regimens in each clinical scenario could represent a helpful way for overcoming this issue, as recently proposed by the IDSA guidance.19
The aim of this review was to perform a critical reappraisal of the issues emerged from pivotal trials of novel beta-lactams and leveraging RWE supporting an appropriate place in for treating MDR Gram-negative infections.
Materials and Methods
A literature search was performed on PubMed-MEDLINE (from January 2015 until October 2025) for retrieving both RCTs and available real-world observational studies concerning novel BL and BL/BLIc, namely ceftazidime-avibactam, ceftolozane-tazobactam, meropenem-vaborbactam, imipenem-relebactam, cefiderocol, cefepime-enmetazobactam, sulbactam-durlobactam, cefepime-taniborbactam, cefepime-zidebactam, and aztreonam-avibactam. The rationale for selecting these agents was based on the in vitro activity against one or more difficult-to-treat resistant (DTR) Gram-negative pathogens, namely extended-spectrum beta-lactamase (ESBL)-producing Enterobacterales, carbapenemase-producing Enterobacterales (CPE) [including KPC, OXA-48 and MBL], MBL-producing Pseudomonas aeruginosa or CRAB. Regarding Pseudomonas aeruginosa, the susceptibility profile to be reviewed concerned only MBL-producing and not DTR-producing genotype as the former has much more limited treatment options than the latter.22,23
Overall, clinical trials and RWE of these agents coming from observational clinical studies and/or case report/series together with studies concerning in vitro susceptibility, PK/PD target attainment, and dosing optimization strategies against specific MDR Gram-negatives were retrieved. Specifically, regarding the novel BL/BLIc just recently licensed, given their availability in the therapeutic armamentarium for some years, the retrieved data concerned, over that RCTs, RWE based on large real-world observational studies, systematic reviews, and real-world PK/PD studies.19,24–26 Considering that two reviews on this topic were published in 2021,24,26 these were searched, and only data published since then were updated.. For previous RWE on this topic, the readers are referred to those reviews.24,26 Conversely, regarding the BL/BLIc incoming tomorrow, due to the recent or under way approval by the regulatory agencies (cefepime-enmetazobactam and aztreonam-avibactam were recently approved by both the Food and Drug Administration [FDA] and the European Medicine Agency [EMA], only sulbactam-durlobactam was recently approved by the FDA only, and cefepime-taniborbactam, cefepime-zidebactam are currently under development), strong RWE is currently lacking, so that it was retrieved, other than RCTs, only RWE based on case series/reports and/or supported by in vitro studies suggesting theoretical benefits in different DTR scenarios. The following terms, alone and/or in combination, were searched: “ceftazidime-avibactam, ceftolozane-tazobactam, meropenem-vaborbactam, imipenem-relebactam, cefiderocol, cefepime-enmetazobactam, sulbactam-durlobactam, cefepime-taniborbactam, cefepime-zidebactam, aztreonam-avibactam, PK/PD target, dosing optimization, MIC, ESBL-producing Enterobacterales, CPE, DTR Pseudomonas aeruginosa, CRAB”. Only articles in English published in the last ten years were included.
Four different clinical scenarios of MDR-related infections were investigated namely, ESBL-producing Enterobacterales, CPE, MBL-producing Pseudomonas aeruginosa and CRAB.24–26 Overall, data were organized in two different sections, namely the first one analyzing the potential critical issues emerged from the pivotal trials and the second one analyzing RWE supporting potential algorithms for proper place in therapy of novel BL/BLIc.
Critical Issues Emerged from the Pivotal Trials of the Licensed and the Incoming Novel BL and BL/BLIc
Table 1 summarizes the Phase III pivotal trials of cefiderocol and of the novel BL/BLIc, either recently licensed or still under way.15–18,21,27–39 Among the 17 identified RCTs, selecting a “weak” comparator and lacking inclusion of patients affected by infections caused by DTR Gram-negative pathogens were the most frequent critical issues emerging for most of them. Consequently, the added value of these RCTs for properly placing these new agents in therapy was very limited, if any.
A well-established pathogen-driven design addressing, specifically, one or more DTR Gram-negative pathogens was adopted in only 5 of these 17 RCTs.21,30,33,34,37 However, also in these trials the emerging findings were affected by some issues that limited their generalizability.
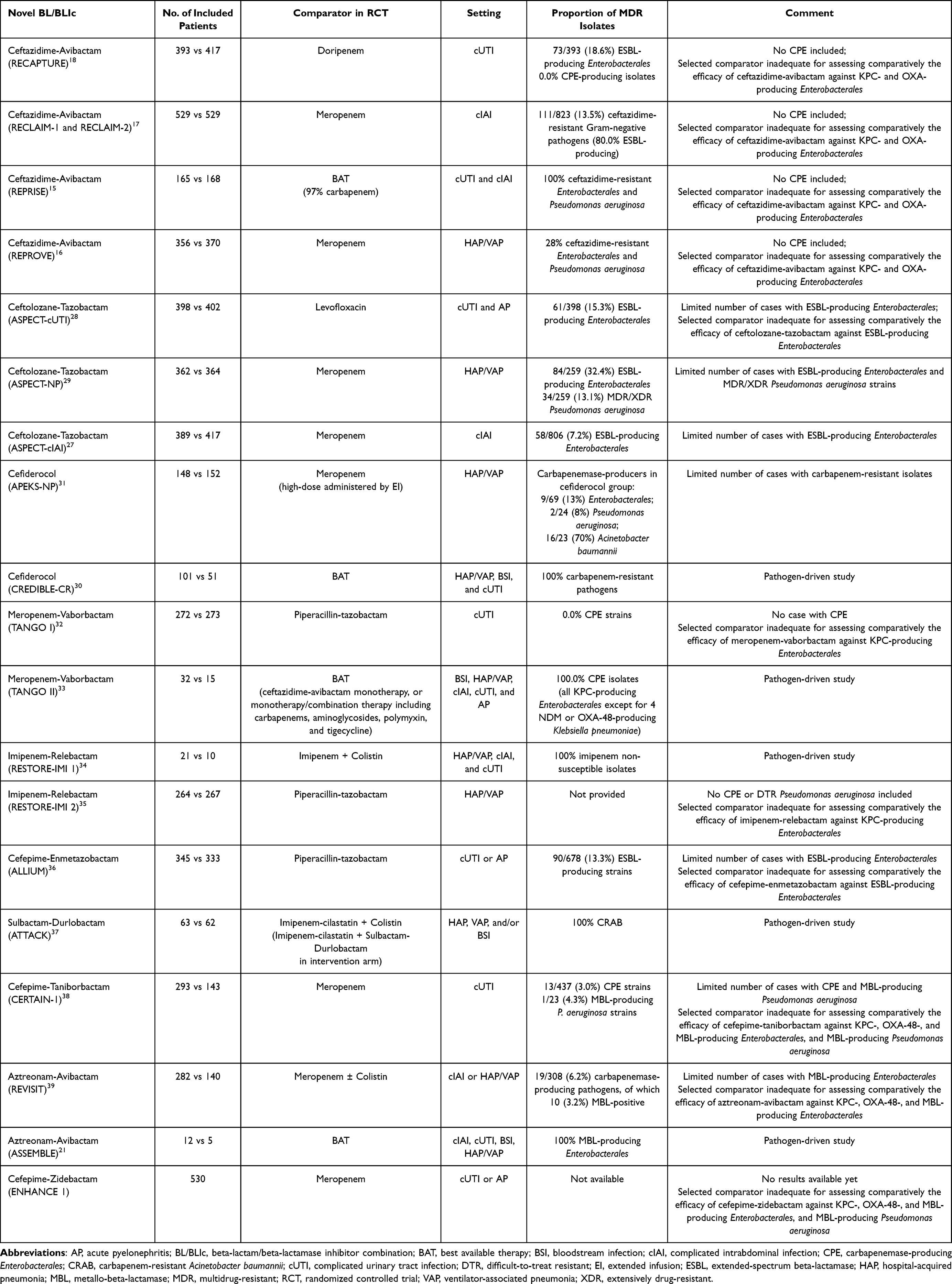 |
Table 1 Summary of Clinical Characteristics and Critical Issues of Available Pivotal Trials for Novel BL/BLIc |
Specifically, the Phase 3 RCT CREDIBLE-CR assessed the efficacy and safety of cefiderocol vs best available therapy (BAT) in 150 patients affected by life-threatening carbapenem-resistant Gram-negative related infections.30 No significant difference in terms of clinical cure and microbiological eradication was documented between the two arms.30 Unfortunately, the imbalance in terms of clinical severity among patients affected by CRAB infections resulted in an overall excess of mortality in the cefiderocol arm.30 Consequently, the guidelines issued by the ESCMID recommended against the use of cefiderocol for the management of CRAB infections.20
The RCT TANGO II assessed the efficacy and safety of meropenem-vaborbactam vs best available therapy (BAT) (including monotherapy/combination therapy with carbapenems, aminoglycosides, polymyxin, and tigecycline) in 47 patients affected by severe CPE-related infections.33 In the meropenem-vaborbactam arm, the clinical cure rate was higher both at the end of treatment (65.6% vs 33.3%; p=0.03) and at the test of cure (59.4% vs 26.7%; p=0.02), and the risk of nephrotoxicity was lower compared to BAT (4.0% vs 24.0%; p<0.001).33 Unfortunately, the limited number of included patients and the lack of a strong comparator (ie, ceftazidime-avibactam) could have limited the generalizability of the findings to real-world clinical scenarios.
The RCT RESTORE-IMI 1 assessed the efficacy and safety of imipenem-relebactam vs combination therapy of imipenem plus colistin in 31 patients affected by imipenem non-susceptible Gram-negative isolates (mainly DTR Pseudomonas aeruginosa).34 No significant difference between the two arms was shown in terms of clinical cure (71.4% vs 70.0%) and of 28-day mortality rate (9.5% vs 30.0%), even if treatment-emergent nephrotoxicity in the imipenem-relebactam arm was lower than in the imipenem plus colistin arm (10.3% vs 56.3%; p=0.002).34 Unfortunately, likewise the aforementioned TANGO II trial, also in this RCT the limited number of included patients, the heterogeneity of clinical isolates other than DTR Pseudomonas aeruginosa, and the lack of a strong comparator could have limited the generalizability of the findings to real-world scenarios.
The ATTACK trial evaluated the efficacy and safety of sulbactam-durlobactam (plus imipenem-cilastatin compared to colistin (plus imipenem-cilastatin) in 125 patients affected by CRAB infections.37 In the sulbactam-durlobactam arm, both the 28-day mortality rate (19% vs 32%; difference −13.2% [95% confidence interval (CI) −30.0–3.5%]) and the nephrotoxicity occurrence (13% vs 38%; p<0.001) were lower compared to colistin.37 Unfortunately, the study findings were biased by the presence of combination therapy with imipenem and by infections being polymicrobial in more than 30% of cases.
The ASSEMBLE trial was designed for assessing the efficacy and safety of aztreonam-avibactam vs BAT in the scenario of severe MBL-producing Gram-negative related infections.21 Unfortunately, the study was closed prematurely because of difficulty in recruiting patients (namely only 15). Besides, the findings at interim analysis showed that aztreonam-avibactam had a higher clinical cure rate (41.7% vs 0.0%), a favorable microbiological response (60.0% vs 0.0%), and lower 28-day mortality rate (8% vs 33%).21
The other 12 RCTs involving novel BL/BLIc did not have a pathogen-driven design and were flawed by a very limited number, if any, of enrolled cases due to those types of resistant pathogens representing the main target of each BL/BLIc in daily clinical practice.15–18,27–29,31,32,35,36,38,39
Specifically, none of the 4 phase III RCTs of ceftazidime-avibactam included patients affected by KPC- and/or OXA-48-producing Enterobacterales -related infections.15–18 Likewise, pivotal trials evaluating ceftolozane-tazobactam in different types of infections included only a limited number of patients affected by ESBL-producing Enterobacterales (ranging from 7.2% to 32.4%) or DTR Pseudomonas aeruginosa (less than 15%).27–29 In the ALLIUM trial evaluating the efficacy and safety of cefepime-enmetazobactam in the setting of complicated urinary tract infection (cUTI) or acute pyelonephritis (AP), the proportion of patients having infections caused by ESBL-producing Enterobacterales was very limited (13.3%). Additionally, selecting as comparator for testing efficacy an agent with limited activity against ESBL, namely piperacillin-tazobactam instead of one fully active, namely meropenem, could be arguable.36 In the CERTAIN-1 trial assessing the efficacy and safety of cefepime-taniborbactam in the setting of cUTI, the proportion of patients affected by infections caused by CPE or MBL-producing Pseudomonas aeruginosa was very limited (3.0% and 4.3%, respectively). Again, selecting as comparator for testing efficacy a drug inactive in vitro against these pathogens, namely meropenem, instead of active one may be arguable.38
Overall, summarizing, it could be concluded that, likewise to what occurred for the most of the recently licensed novel BL and BL/BLIc, even for the incoming ones the RCTs did not add significant knowledge for supporting properly the benefit that they could have in specific scenarios of MDR-related infections.
Fortunately, RWE has just played a major role in finding a proper place of the former in the treatment of MDR Gram-negative infections caused by some types of pathogens producing specific mechanisms of resistance.24–26
Conversely, the RWE concerning the incoming novel BL/BLIc is still limited to case series/reports, so that currently the potential theoretical benefits that these agents may offer in these scenarios could only be presumed and supported by some interesting in vitro studies. In the next two sections, we provide an update for both novel licensed and incoming BL/BLIc.
Recent RWE Concerning the Role of the Licensed Novel BL/BLIc Against Some Specific Targeted Types of MDR Gram-Negatives
ESBL-Producing Enterobacterales
Previous expert opinion articles suggested ceftolozane-tazobactam and ceftazidime-avibactam as carbapenem-sparing agents in the management of ESBL-producing Enterobacterales.25,26 A large multicenter retrospective study, including 153 patients affected by documented infections caused by ESBL-producing Enterobacterales (mainly pneumonia [30.0%] and complicated urinary tract infection [22.2%]) found an overall clinical success rate of 83.7% with ceftolozane-tazobactam.40 A monocentric retrospective observational study comparing the effectiveness of ceftolozane-tazobactam vs meropenem in 115 patients affected by bloodstream infections (BSIs) due to ESBL-producing Enterobacterales found no significant difference at the inverse probability of treatment weighting analysis in terms of clinical cure (odds ratio [OR] 0.43; 95% CI 0.12–1.53; p=0.19), hospital mortality (OR 1.72; 95% CI 0.54–5.51; p=0.36) and 30-day mortality (OR 1.72; 95% CI 0.54–5.48; p=0.35) between the two agents.41 A meta-analysis including five RCTs comparing ceftazidime-avibactam vs carbapenems reported no significant difference in terms of clinical response at test of cure between the two arms (risk ratio [RR] 1.02; 95% CI 0.97–1.08; p=0.45).42
Indeed, it should be mentioned that some recent findings have raised some concerns about the use of these two agents against ESBL-producers. First, ceftolozane-tazobactam is highly active against ESBL-producing Escherichia coli, but not against ESBL-producing Klebsiella pneumoniae, whose strains may be resistant in 35% of cases.43 Second, a recent population PK study found that the current dosing regimens of ceftolozane-tazobactam, even if delivered by CI, failed to attain an aggressive joint PK/PD target in the majority of cases against ESBL-producing Enterobacterales, with the cumulative fraction of response ranging between 29% and 54%.44 Third, an interesting in vitro study showed that 96% and 34.5% of ESBL-producing Escherichia coli and Klebsiella pneumoniae isolates may exhibit an inoculum effect against ceftolozane-tazobactam and ceftazidime-avibactam, respectively, with a 4- to 64-fold minimum inhibitory concentration (MIC) increase in the presence of high bacterial loads (107 colony forming-unit [CFU]/mL) compared to low bacterial loads (105 CFU/mL)45 thus possibly affecting the role of these agents in severe deep-seated infections with high ESBL-producing bacterial burden such as pneumonia. Besides, it should not be overlooked that these agents should be preferentially reserved for treating CPE or DTR Pseudomonas aeruginosa, as recommended by both the IDSA guidance and the ESCMID guideline.19,20
CPE
KPC-Producing Enterobacterales
Both the IDSA guidance and the ESCMID guideline recommended ceftazidime-avibactam and meropenem-vaborbactam as first-line treatment KPC-producing Enterobacterales related infections.19,20 Unfortunately, the prevalence of KPC-producing isolates resistant to ceftazidime-avibactam has recently challenged the therapeutic approach of this scenario.46,47
Real-world observational studies comparing the clinical efficacy of these two BL/BLIc against KPC-producing Enterobacterales48–50 and PK/PD studies highlighting some potential issues associated with the use of standard-dosing regimens of ceftazidime-avibactam51–53 provided helpful evidence to clinicians for selecting the most appropriate agent in specific situations. Specifically, a retrospective study that included 131 patients affected by CPE infections found no difference in clinical success between patients treated with ceftazidime-avibactam (n=105) or with meropenem-vaborbactam (n=26) (62% vs 69%; p=0.49).48 Likewise, a multicenter retrospective study comparing 131 patients receiving ceftazidime-avibactam with 37 receiving meropenem-vaborbactam found no significant difference in the management of CPE infections between the two agents in terms of clinical success (67.9% vs 64.9%; p=NS), in-hospital mortality (20.6% vs 29.7%; p=NS), and relapse rate (11.5% vs 5.4%; p=0.34).49 Conversely, a retrospective multicenter study comparing 52 patients receiving ceftazidime-avibactam with 36 receiving meropenem-vaborbactam showed in the propensity score analysis that meropenem-vaborbactam granted better clinical improvement at 72 hours (OR 2.19; 95% CI 1.35–3.55), whereas 30-day mortality rate did not differ (OR 0.65; 95% CI 0.55–1.68).50 A recent population PK study conducted among 112 critically ill patients reported that the ceftazidime-to-avibactam ratio was not fixed at 4:1, but it was subjected to wide fluctuations according to renal function.51 Furthermore, the tested permissible ceftazidime-avibactam dosing regimens administered by continuous infusion (CI) did not allow to achieve an optimal probability of target attainment (defined as an aggressive joint PK/PD target) in case of augmented renal clearance or of KPC-producing strains having an MIC equal to the clinical breakpoint of 8 mg/L.51 According to these novel real-world findings, it could be suggested that meropenem-vaborbactam should be preferred over ceftazidime-avibactam in case of KPC-producing isolates having borderline susceptibility to ceftazidime-avibactam, or in patients exhibiting augmented renal clearance or affected by hospital-acquired pneumonia (HAP) and/or ventilator-associated pneumonia (VAP) according to the lower penetration rate of ceftazidime-avibactam in the epithelial lining fluid and its unfavorable BL:BLI ratio.53,54
Overall, the current prevalence of KPC-producing isolates resistant to ceftazidime-avibactam may be around 20% in some centers. These findings suggest that in these centers it may be prudent avoiding empirical treatment with ceftazidime-avibactam for suspected KPC-related infections and reserving it preferably for the targeted therapy of documented infections caused by strains showing phenotypic susceptibility to ceftazidime-avibactam. Interestingly, an innovative population PK/PD study predicted that by administering the licensed dosages of ceftazidime-avibactam by CI rather than by 2-h infusion, it may be possible to attain a cumulative fraction of response against KPC-K. pneumoniae related infections occurring in critically ill patients in as much as 70–90% of cases, OXA-48-K. pneumoniae and OXA-48-Enterobacterales.51
OXA-48-Producing Enterobacterales
Both the IDSA guidance19 and the ESCMID guidelines20 recommend ceftazidime-avibactam as first-line therapy for treating OXA-48-producing Enterobacterales related infections on the basis of RWE.55–58 A recent multicenter retrospective matched cohort study including 180 patients affected by OXA-48-producing Enterobacterales infections found in multivariable logistic regression analyses that ceftazidime-avibactam treatment was protective against mortality (adjusted odds ratio [aOR]=0.37; 95% CI 0.19–0.71; p=0.003) and had better 21-day clinical response (aOR=3.32; 95% CI 1.68–6.53; p<0.001) compared to other best available therapies.58 Likewise, a retrospective monocentric study conducted among 76 patients with OXA-48-producing Klebsiella pneumoniae BSI reported that ceftazidime-avibactam compared to BAT granted better clinical success (OR 6.69; 95% CI 1.68–26.60; p=0.007) and lower 14-day mortality rate (p=0.013).57
Overall, these recent findings may support the use of ceftazidime-avibactam in the management of OXA-48-producing related infections. Interestingly, the aforementioned population PK/PD study predicted that even against OXA-48-K.pneumoniae and OXA-48-Enterobacterales related infections occurring in critically ill patients the cumulative fraction of response may be as high as 70–90% of cases when administering the licensed dosages of ceftazidime-avibactam by CI rather than by 2-h infusion.51
MBL-Producing Enterobacterales
Both the IDSA guidance19 and the ESCMID guidelines20 recommend combining aztreonam with ceftazidime-avibactam or cefiderocol for treating MBL-producing Enterobacterales based on RWE.59,60 A recent meta-analysis, including four observational studies assessing the efficacy of aztreonam combined with ceftazidime-avibactam compared to polymyxin-based regimens, reported a significant lower 30-mortality rate with the former in treating MBL-producing Enterobacterales infections (OR 0.51; 95% CI 0.34–0.76; p<0.001).59 Cefiderocol should be reserved as second-line in this setting, considering the non-negligible resistance rate observed among NDM-producing strains.61 Interestingly, a prospective observational study assessed the efficacy of different therapeutic regimens among 343 patients with documented infections caused by MBL-producing Enterobacterales (328 NDM-producing and 15 VIM-producing, respectively).62 By considering colistin containing regimens as the reference, combination treatment of ceftazidime-avibactam plus aztreonam was independently associated at the sensitivity propensity score analysis with a reduced 30-day mortality rate (adjusted hazard ratio [aHR] 0.39; 95% CI 0.18–0.86; p=0.02), differently from what observed with cefiderocol-containing regimens (aHR 0.83; 95% CI 0.31–2.24; p=0.72).62
Overall, the findings may support the use of ceftazidime-avibactam plus aztreonam as best therapeutic regimen in the challenging scenario of infections caused by MBL-producing Enterobacterales.
MBL-Producing P. Aeruginosa
IDSA guidance19 recommended the use of cefiderocol as first-line therapy for the management of severe infections caused by MBL-producing Pseudomonas aeruginosa, despite the very low number of patients having such an isolate in pivotal trials.63 The real-world multicenter retrospective observational PERSEUS study included 261 patients being treated with cefiderocol because of severe Gram-negative infections other than CRAB.64 In the subgroup analysis of the 174 patients affected by DTR Pseudomonas aeruginosa (42% MBL-producers), clinical cure and 28-day mortality rate were 84.5% and 17.2%, respectively.64 Specifically, in infections caused by Pseudomonas aeruginosa showing resistance to both ceftolozane-tazobactam and ceftazidime-avibactam, clinical cure rate and 28-day mortality rate were 82.8% and 17.2%, respectively.64 Consequently, these promising findings emerged from RWE may support the use of cefiderocol in this challenging scenario.
CRAB
The ESCMID guidelines20 recommended against the use of cefiderocol for treating CRAB infections based on the findings emerged from the CREDIBLE-CR trial.30 Conversely, the IDSA guidance19 recommended the use of cefiderocol provided that in combination with high-dose ampicillin-sulbactam based on different RWE.65–67 Specifically, a meta-analysis including one RCT and seven observational studies providing adjustment for confounders showed that the use of cefiderocol-containing regimens in treating CRAB infections was associated with significantly lower mortality rate compared with other regimens (mainly colistin-based) (OR 0.53; 95% CI 0.41–0.68; p<0.001).65,67 Indeed, caution should be warranted in defining the proper place of cefiderocol in this setting since most of RWE came from retrospective studies using cefiderocol in combination therapy and includes a limited number of patients.68
RWE Supporting the Use of Novel Incoming BL/BLIc in Some Types of MDR Gram-Negative Related Infections
RWE for supporting the use of novel BL/BLIc in specific settings of MDR-Gram negative related infections is summarized in Table 2. Available RWE concerned only cefepime-zidebactam vs MBL-producing P. aeruginosa and sulbactam-durlobactam vs CRAB, namely the only two recently included in the therapeutic armamentarium.
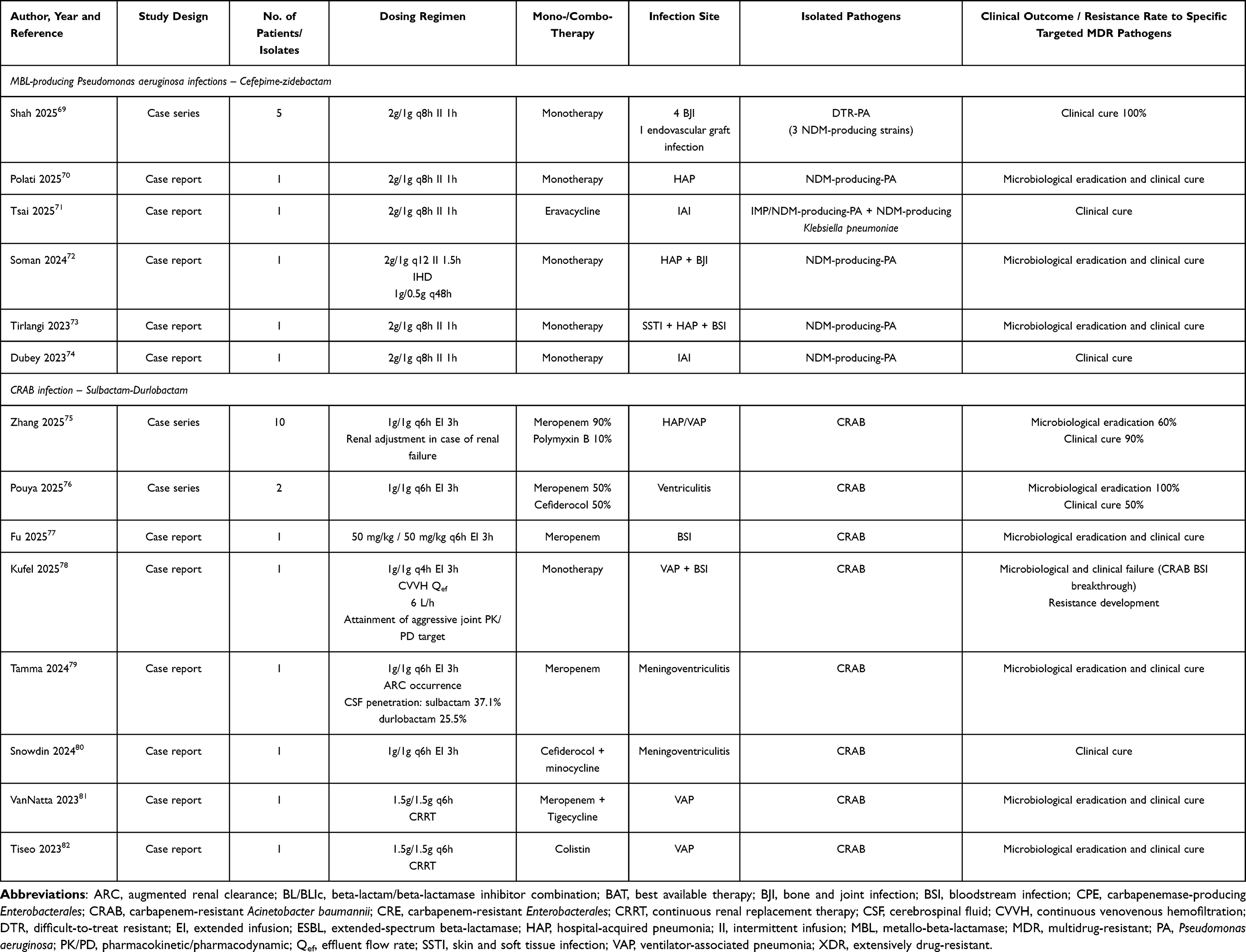 |
Table 2 Real-World Evidence Supporting the Use of Novel Incoming BL/BLIc in Some Types of MDR Gram-Negative Related Infections |
MBL-Producing P. Aeruginosa
One case series69 and five case reports70–74 including a total of 10 patients assessed the efficacy of cefepime-zidebactam in the management of MBL-producing Pseudomonas aeruginosa infections, 80% of which caused by NDM-producing strains. Specifically, bone and joint infections (50.0%) and pneumonia (30.0%) were the most frequent ones. Cefepime-zidebactam was used in monotherapy in all but one case in which combination with eravacycline was implemented.71 Favorable clinical outcome was reported in all of the included cases without any emergence of resistance development.
CRAB
Two case series75,76 and six case report77–82 including a total of 18 patients assessed the efficacy of sulbactam-durlobactam in the management of different types of CRAB infections, with HAP/VAP (72.2%) and meningoventriculitis (22.2%) being the two most represented. Sulbactam-durlobactam was used in all but one case in combination therapy (mainly with meropenem).78 Favorable clinical outcome was reported in 83.3% of the included patients, and in one case (5.6%) resistance development to sulbactam-durlobactam was reported. Interestingly, Tamma et al evaluated the penetration rate of sulbactam-durlobactam in cerebrospinal fluid in one patient affected by CRAB meningoventriculitis, reporting a penetration rate of 37.1% and 25.5% for sulbactam and durlobactam, respectively.79
In vitro, Preclinical Studies, and Potential Place in Therapy of Novel Incoming BL/BLIc Against Some Specific Targeted Types of MDR Gram-Negatives Related Infections
In vitro and preclinical studies supporting the potential role of novel incoming BL/BLIc against some specific targeted types of MDR Gram-negatives related infections are summarized in Tables 3 and 4. Figure 2 shows the four different potential positioning algorithms for targeted therapy of infections caused by ESBL-producing Enterobacterales (panel A), CPE (panel B), MBL-producing Pseudomonas aeruginosa (panel C), and CRAB (panel D) according to potential place in therapy of novel incoming BL/BLIc.
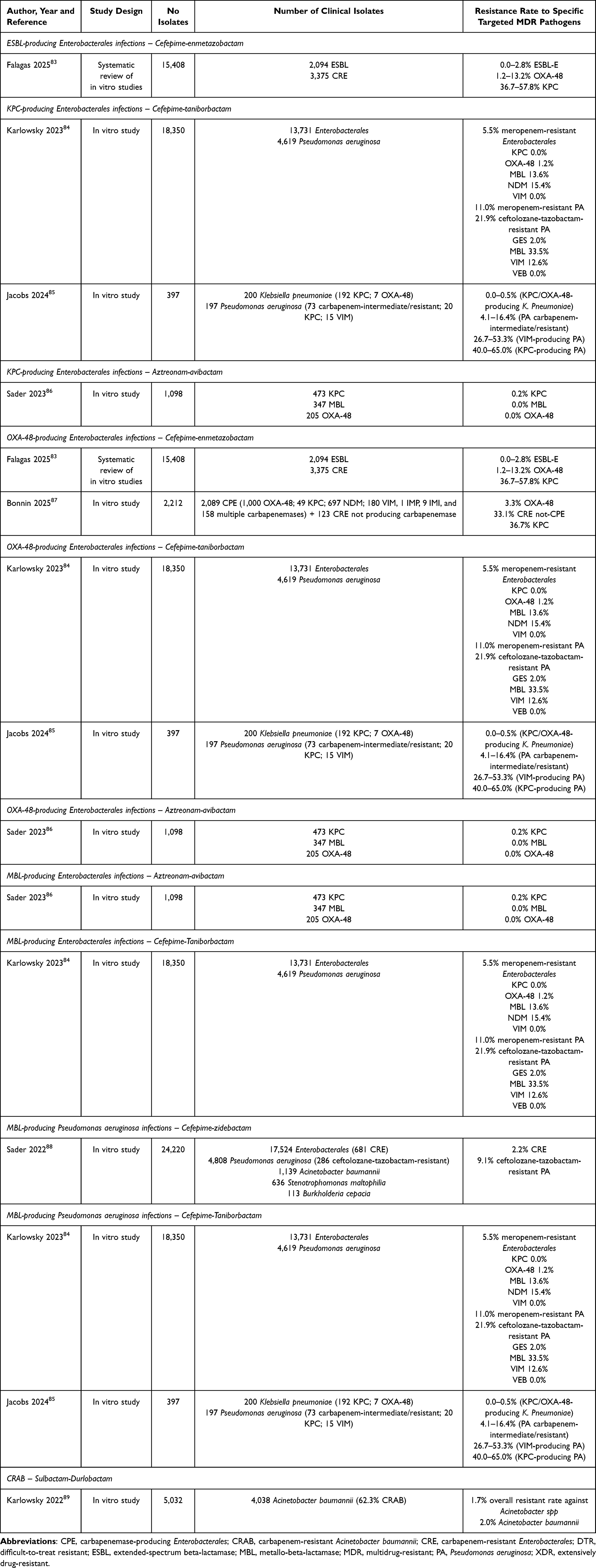 |
Table 3 In Vitro Studies Supporting the Potential Role of the Incoming Novel BL/BLIc in Treating Some Specific Targeted Types of MDR Gram-Negative Related Infections |
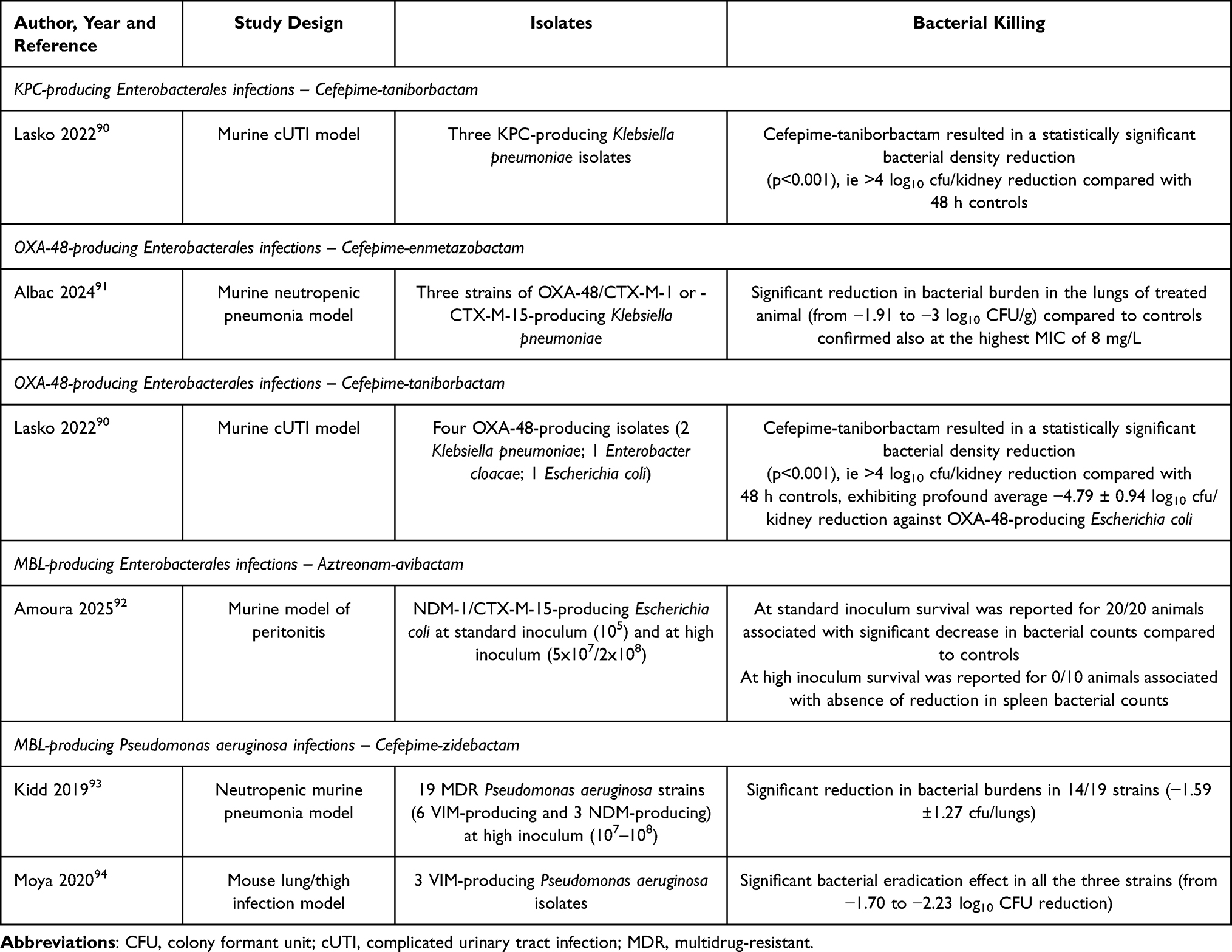 |
Table 4 Preclinical Studies Supporting the Potential Role of the Incoming Novel BL/BLIc in Treating Some Specific Targeted Types of MDR Gram-Negative Related Infections |
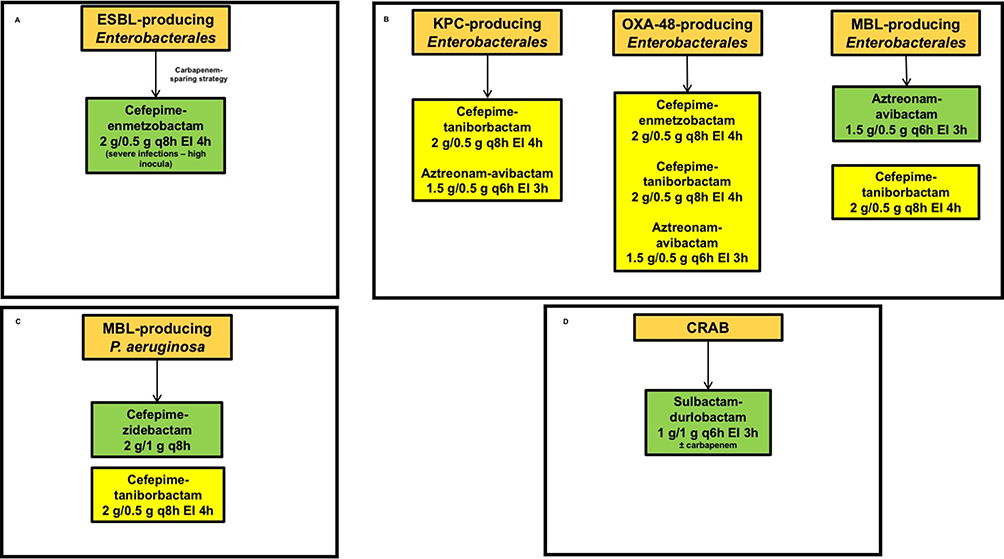 |
Figure 2 Algorithms for targeted treatment of infections caused by Gram-negative pathogens showing different pattern of susceptibility. (A) ESBL-producing Enterobacterales; (B) CPE; (C) MBL-producing Pseudomonas aeruginosa; (D) CRAB. Abbreviations: CRAB, carbapenem-resistant Acinetobacter baumannii; EI, extended infusion; ESBL, extended-spectrum beta-lactamase; MBL, metallo-beta-lactamase. |
Regarding the novel BL/BLIc just recently licensed, we recall here the algorithms of potential place in therapy just previously published in the aforementioned reviews (Table 5).24,26 Most of the recent updating RWE may further support these algorithms.
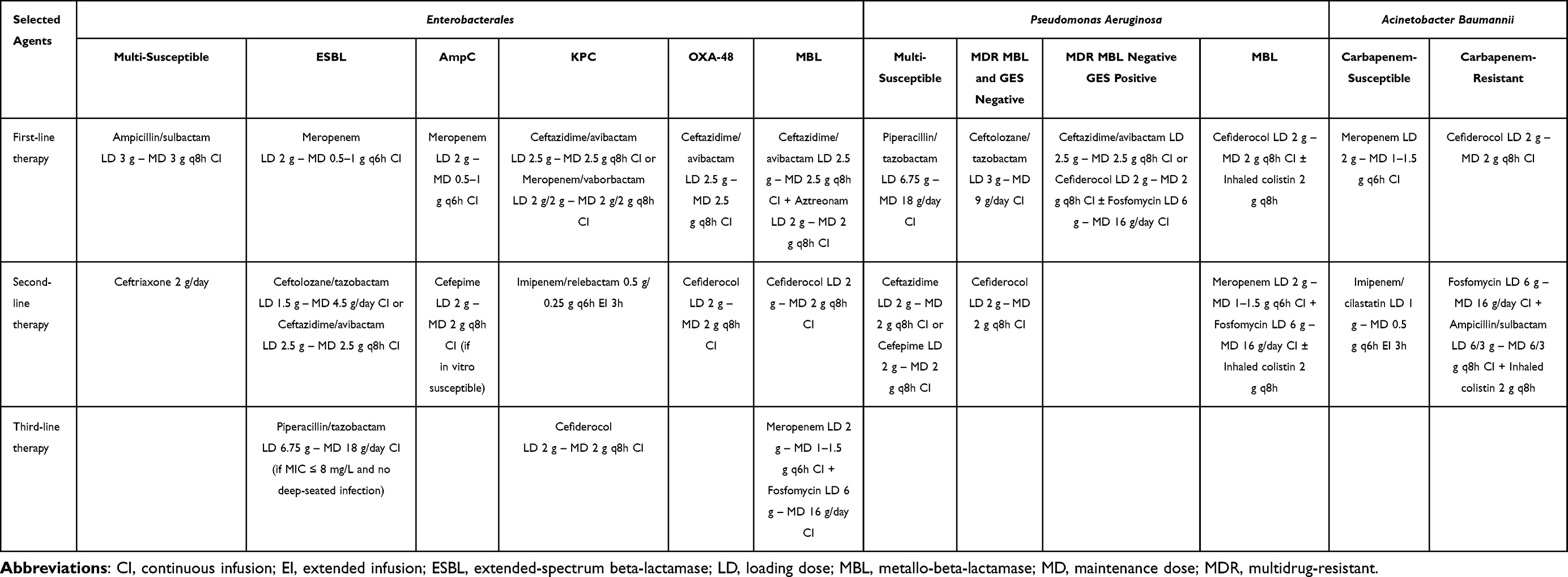 |
Table 5 Proposed Algorithms for the Management of Infections Caused by Enterobacterales, Pseudomonas Aeruginosa, and Acinetobacter Baumannii with Different Pattern of Antibiotic Susceptibility (Adapted with Permission From)24,26 |
ESBL-Producing Enterobacterales
Some in vitro studies assessed the susceptibility of cefepime-enmetazobactam against ESBL-producing Enterobacterales.83,87 Specifically, a recent systematic review including ten in vitro studies assessing the susceptibility of 15,408 Gram-negative isolates to cefepime-enmetazobactam reported a resistance rate ranging from 0.0% to 2.8% among 2,094 ESBL-producing Enterobacterales.83 An in vitro study showed that the proportion of ESBL-producing Escherichia coli and Klebsiella pneumoniae clinical isolates exhibiting an inoculum effect, namely a 4- to 64-fold MIC increase in the presence of high bacterial loads (107 CFU/mL) compared to low bacterial loads (105 CFU/mL), may greatly vary among the different BL/BLIc. Interestingly, it was as low as 10.3% against cefepime-enmetazobactam compared to 34.5% and 96% against ceftazidime-avibactam and ceftolozane-tazobactam, respectively.45
Based on available data,45,83 it may be speculated that cefepime-enmetazobactam could represent a promising and valuable carbapenem-sparing agent in the treatment ESBL-producing Enterobacterales (Figure 2A). Interestingly, the low propensity to the inoculum effect could favor its role in severe infections with high bacterial burden, namely HAP or VAP. However, clinical RWE would be warranted for confirming this hypothesis.
CPE
KPC-Producing Enterobacterales
Both cefepime-taniborbactam and aztreonam-avibactam exhibit excellent in vitro activity against KPC-producing Enterobacterales.84–86 Regarding cefepime-taniborbactam, an in vitro study collecting 13,731 Enterobacterales isolates found that all of the 5.5% KPC producing strains were susceptible to cefepime-taniborbactam.84 Likewise, another in vitro study collecting 192 KPC-producing Klebsiella pneumoniae strains reported that the resistance rate to cefepime-taniborbactam was very low, if any (0.0–0.5%).85 Interestingly, a murine model of complicated urinary tract infection caused by KPC-producing Klebsiella pneumoniae showed that cefepime-taniborbactam resulted in a statistically significant reduction of bacterial density >4 log10 CFU/kidney at 48 hours compared to controls.90
Regarding aztreonam-avibactam, an in vitro study collecting 473 KPC-producing Enterobacterales found that the resistance rate was of 0.2%.86 These data may provide a good basis for considering these two agents as potentially active against KPC-producing Enterobacterales related infections, but obviously clinical RWE should be collected before any definitive conclusion on this.
Based on the available data,84–86 both cefepime-taniborbactam and aztreonam-avibactam could represent valuable alternatives in treating infections caused by KPC-producing Enterobacterales (Figure 2B), especially in settings burdened by high resistance rates to both ceftazidime-avibactam and meropenem-vaborbactam.95 Unfortunately, no clinical RWE is currently available for these novel incoming BL/BLIc, and further studies would be warranted for confirming their place in therapy in this scenario.
OXA-48-Producing Enterobacterales
Cefepime-enmetazobactam, cefepime-taniborbactam, and aztreonam-avibactam could be promising alternatives in the management of OXA-48-producing Enterobacterales related infections.83–87 Specifically, in regard to cefepime-enmetazobactam a systematic review of ten in vitro studies including an overall 3,375 CRE reported a resistance rate among 1,423 strains carrying OXA-48-carbapenemase ranging from 1.2% to 13.2%.83 Likewise, a large in vitro study collecting 2,089 CPE reported a resistance rate to cefepime-enmetazobactam of 3.3% among 1,000 OXA-48-producing strains.87 Interestingly, a murine neutropenic pneumonia model induced by OXA-48-producing Klebsiella pneumoniae showed that cefepime-enmetazobactam significantly reduced the lung bacterial burden of −1.91 to −3 log10 CFU/g compared to controls.91 This effect was also confirmed at the highest MIC of 8 mg/L.91
A large in vitro study including 13,731 Enterobacterales showed that the resistance rate to cefepime-taniborbactam among 168 strains producing OXA-48-carbapenemase was of 1.2%.84 A murine complicated urinary tract infection model induced by OXA-48-producing Enterobacterales showed that cefepime-taniborbactam reduced significantly the bacterial density by >4 log10 CFU/kidney at 48 hours compared to controls, especially against OXA-48-producing Escherichia coli strains (average −4.79 ± 0.94 log10 cfu/kidney).90
An in vitro study collecting 205 OXA-48-producing Enterobacterales reported a resistance rate of 0.0% to aztreonam-avibactam.86 Larger clinical RWE would be warranted for assessing the role of novel BL/BLIc of tomorrow in the management of infections caused by OXA-48-producing Enterobacterales.
Based on available data,83–87 cefepime-enmetazobactam, cefepime-taniborbactam, and aztreonam-avibactam could represent valuable alternatives to ceftazidime-avibactam in treating infections caused by OXA-48-producing Enterobacterales (Figure 2B). Unfortunately, no clinical RWE is currently available for these novel incoming BL/BLIc, and further studies would be warranted for confirming their place in therapy in this scenario.
MBL-Producing Enterobacterales
Aztreonam-avibactam could become the first-line therapy for treating infections caused by MBL-producing Enterobacterales.96 An in vitro study collecting 347 MBL-producing Enterobacterales showed that all were susceptible to aztreonam-avibactam.86 A murine model of assessing the efficacy of aztreonam-avibactam against NDM-1/CTX-M-1 or CTX-M-15-coproducing Escherichia coli causing peritonitis at standard (105) or high inocula (107–108).92 Treatment was always effective in granting both animal survival and significant decrease in the bacterial burden compared to controls in presence of standard inoculum whereas conversely failed in presence of high inocula.92
Cefepime-taniborbactam could represent an alternative in this setting,97 but it should not be overlooked that the overall resistance rate resistance rate to this agent reported by in vitro studies among MBL-producing strains was overall of 13.6%, ranging from 0.0% among VIM-producers to 15.4% among NDM-producers.84 Indeed, different MBL-producing variants showing resistance to cefepime-taniborbactam have been recently characterized, including IMP, VIM-83, NDM-9, and NDM-30.98–100
Based on the limited data of the ASSEMBLE trial21 and on the available in vitro evidence,84,86 aztreonam-avibactam could become, in the future, the first-line choice for treating infections caused by MBL-producing Enterobacterales (Figure 2B). Cefepime-taniborbactam could be a valuable alternative in some cases, taking care of the resistance development to this agent showed by IMP, VIM-83, NDM-9, or NDM-30-producing strains.98–100
MBL-Producing P. Aeruginosa
Several in vitro studies assessed the susceptibility of cefepime-zidebactam and cefepime-taniborbactam against MBL-producing Pseudomonas aeruginosa strains. Specifically, in an in vitro study testing cefepime-zidebactam activity against 4,808 Pseudomonas aeruginosa isolates, 286 of which were ceftolozane-tazobactam-resistant, the susceptibility rate was of 90.9%.88 Interestingly, a neutropenic murine pneumonia model assessing 19 MDR Pseudomonas aeruginosa strains (of which 6 VIM-producing and 3 NDM-producing) at high inoculum reported that cefepime-zidebactam significantly reduced bacterial burdens in 14/19 isolates (mean reduction of −1.59±1.27 cfu/lungs).93 Furthermore, a mouse lung/thigh infection model evaluating three VIM-producing Pseudomonas aeruginosa strains found that cefepime-zidebactam ensured a significant bacterial eradication against all the three isolates (from −1.70 to −2.23 log10 CFU reduction).94
Two large in vitro studies84,85 tested the activity of cefepime-taniborbactam against MBL-producing Pseudomonas aeruginosa. Indeed, a large in vitro study including 4,619 Pseudomonas aeruginosa isolates reported that the resistance rate to cefepime-taniborbactam was 11.0% and 21.9% among meropenem-resistant and ceftolozane-tazobactam-resistant strains, respectively.84 Moving to genotypic characterization of DTR Pseudomonas aeruginosa strains, cefepime-taniborbactam showed a resistance rate of 12.6% and 33.5% against VIM- and MBL-positive strains, respectively.84 Another in vitro study including 197 Pseudomonas aeruginosa isolates, of which 73 showing intermediate susceptibility and/or resistance to carbapenems reported a resistance rate to cefepime-taniborbactam of 4.1–16.4% in this latter group, whereas higher resistance rate was found against VIM- (26.7–53.3%) and KPC-producing strains (40.0–65.0%).85 Overall, based on these preliminary data, both cefepime-zidebactam and cefepime-taniborbactam could represent promising alternatives for the management of MBL-producing Pseudomonas aeruginosa, although clinical RWE would be warranted for supporting this hypothesis.
Based on available evidence,69–74,84,85,88 cefepime-zidebactam could become, in future, a valuable alternative to cefiderocol in treating infections caused by MBL-producing Pseudomonas aeruginosa, whereas cefepime-taniborbactam could be a second-line alternative for targeted therapy, if an in vitro susceptibility of the clinical isolate is confirmed (Figure 2C).
CRAB
Sulbactam-durlobactam may represent a promising alternative for treating CRAB infections according to in vitro susceptibility studies. Specifically, in a large in vitro study testing sulbactam-durlobactam activity against 4,038 Acinetobacter baumannii isolates, 62.3% of which were CRAB, the resistance rate among CRAB strains was of 2.0%.89
Based on the findings of the ATTACK trial,37 and on RWE,75–82 the IDSA guidance19 recommended combination of sulbactam-durlobactam with a carbapenem as first-line treatment of infections caused by CRAB. RWE should provide in future enough evidence to define whether this agent can be used as monotherapy in this setting. Meanwhile, available evidence37,75–82 may support the role of sulbactam-durlobactam especially for treating pneumonia and/or meningoventriculitis (Figure 2D).
Expert Opinion
Overall, RWE concerning both well-designed observational studies and PK/PD studies, by overcoming the issues deriving from the RCTs, should represent the cornerstones for supporting the role of the incoming novel BL/BLIc in the management of some specific types of MDR Gram-negative related infections. In this setting, conducting population PK/PD studies in real-world could be helpful in providing clinicians the most appropriate dosing regimens for either maximizing clinical outcome or preventing resistance development. In this every-changing scenario, continuous update coming from newly available RWE will be fundamental.
In the last years, RWE was revealed very helpful in better defining the place of the recently licensed novel BL/BLIc in treating specific types of MDR Gram-negative infections, as issued by the IDSA guidance.19 In this context, planning PK/PD studies of novel BL/BLIc in real-world could hopefully provide definitive answers on how relevant maximizing the likelihood of aggressive joint PK/PD target attainment may be in both preventing resistance development54 and enabling personalized treatment of different types of special populations.51,52,101,102 Waiting for this, a potential place in therapy of the novel incoming BL/BLIc could be based on preliminary evidence. Based on this, it may be speculated that cefepime-enmetazobactam could represent a carbapenem-sparing strategy in treating infections caused by ESBL-producing Enterobacterales and a potential alternative to ceftazidime-avibactam in treating OXA-48-producing infections. Cefepime-taniborbactam, cefepime-zidebactam, and aztreonam-avibactam could represent a definitive answer in treating MBL-producing Enterobacterales and MBL-producing Pseudomonas aeruginosa. Lastly, sulbactam-durlobactam has already been recognized by international guidelines as potentially having a valuable role in treating CRAB infections.19 Overall, according to preliminary in vitro data and to RWE, the different incoming novel BL/BLIc seems promising for the management of infections caused by MDR Gram-negative pathogens, including those exhibiting the most challenging susceptibility profile (ie, MBL-producing Enterobacterales or Pseudomonas aeruginosa, CRAB). However, it should not be overlooked that some concerns need to be addressed. Specifically, the limited tissue penetration rate of these agents could potentially result in aggressive PK/PD target non-attainment at the infection site when treating the deep-seated infections (ie, pneumonia) with standard dosing regimens.14 Furthermore, there is a need to assess the cost-effectiveness of using these agents compared to current first-line options in terms of length of hospital stay and/or resistance development. Finally, it should be recognized that the availability of the novel incoming BL/BLIc could be limited to only some parts of the world, as just previously occurred for the currently licensed novel BL/BLIc. This could cause disparities in managing MDR Gram-negative infections with the potential consequence of having significant differences in terms of clinical outcomes.
In conclusions, in an era characterized by the widespread diffusion of Gram-negative pathogens and the ever-growing resistance rates, RWE should represent an essential tool for properly placing novel BL/BLIc in routine clinical practice. The ever-growing number of RWE would offer the opportunity for continuously updating algorithms positioning novel BL/BLIc in the management of MDR Gram-negative pathogens.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
MG received personal fees from Angelini, and participated in advisory board for Advanz Pharma and Viatris. FP participated in speaker bureau for Advanz Pharma, Angelini, Gilead, InfectoPharm, Menarini, Merck Sharp & Dohme, Pfizer and Shionogi, and on the advisory board for Advanz Pharma, Merck Sharp & Dohme, Pfizer and Viatris, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Tacconelli E, Carrara E, Savoldi A. et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–23. doi:10.1016/S1473-3099(17)30753-3
2. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
3. Macesic N, Uhlemann AC, Peleg AY. Multidrug-resistant Gram-negative bacterial infections. Lancet. 2025;405(10474):257–272. doi:10.1016/S0140-6736(24)02081-6
4. Patel TS, Sati H, Lessa FC, et al. Defining access without excess: expanding appropriate use of antibiotics targeting multidrug-resistant organisms. Lancet Microbe. 2024;5(1):e93–e98. doi:10.1016/S2666-5247(23)00256-2
5. Willems RPJ, van Dijk K, Vehreschild MJGT, et al. Incidence of infection with multidrug-resistant Gram-negative bacteria and vancomycin-resistant enterococci in carriers: a systematic review and meta-regression analysis. Lancet Infect Dis. 2023;23(6):719–731. doi:10.1016/S1473-3099(22)00811-8
6. Darlow CA, Hope W, Dubey V. Cefepime/Enmetazobactam: a microbiological, pharmacokinetic, pharmacodynamic, and clinical evaluation. Expert Opin Drug Metab Toxicol. 2024;1–9. doi:10.1080/17425255.2024.2427310
7. Bassetti M, Larosa B, Vena A, Giacobbe DR. Novel agents in development for the treatment of resistant Gram-negative infections. Exp Rev Anti-Infective Ther. 2024;22(11):965–976. doi:10.1080/14787210.2024.2407068
8. Zhanel GG, Mansour C, Mikolayanko S, et al. Cefepime-taniborbactam: a novel Cephalosporin/β-Lactamase inhibitor combination. Drugs. 2024;84(10):1219–1250. doi:10.1007/s40265-024-02082-9
9. McLeod SM, O’Donnell JP, Narayanan N, Mills JP, Kaye KS. Sulbactam-durlobactam: a β-lactam/β-lactamase inhibitor combination targeting Acinetobacter baumannii. Future Microbiol. 2024;19(7):563–576. doi:10.2217/fmb-2023-0248
10. Yahav D, Giske CG, Grāmatniece A, Abodakpi H, Tam VH, Leibovici L. New β-Lactam-β-Lactamase inhibitor combinations. Clin Microbiol Rev. 2020;34(1):e00115–20. doi:10.1128/CMR.00115-20
11. Bassetti M, Giacobbe DR. Cefepime-taniborbactam and CERTAIN-1: can we treat carbapenem-resistant infections? Med. 2024;5(5):380–382. doi:10.1016/j.medj.2024.03.011
12. Bassetti M, Vena A, Giacobbe DR. Clinical trials that could change the management of severe multidrug-resistant Gram-negative infections. Curr Opin Infect Dis. 2025. doi:10.1097/QCO.0000000000001150
13. Paul M, Dishon-Benattar Y, Dickstein Y, Yahav D. Optimizing patient recruitment into clinical trials of antimicrobial-resistant pathogens. JAC-Antimicrob Resist. 2022;5(1):dlad005. doi:10.1093/jacamr/dlad005
14. Gatti M, Pea F. Critical reappraisal of current issues for improving the proper clinical use of the incoming beta-lactam/beta-lactamase inhibitor combinations of tomorrow. Exp Rev Anti-Infective Ther. 2025;23(7):433–443. doi:10.1080/14787210.2025.2493077
15. Carmeli Y, Armstrong J, Laud PJ, et al. Ceftazidime-avibactam or best available therapy in patients with ceftazidime-resistant Enterobacteriaceae and Pseudomonas aeruginosa complicated urinary tract infections or complicated intra-abdominal infections (REPRISE): a randomised, pathogen-directed, phase 3 study. Lancet Infect Dis. 2016;16(6):661–673. doi:10.1016/S1473-3099(16)30004-4
16. Torres A, Zhong N, Pachl J, et al. Ceftazidime-avibactam versus meropenem in nosocomial pneumonia, including ventilator-associated pneumonia (REPROVE): a randomised, double-blind, phase 3 non-inferiority trial. Lancet Infect Dis. 2018;18(3):285–295. doi:10.1016/S1473-3099(17)30747-8
17. Mazuski JE, Gasink LB, Armstrong J, et al. Efficacy and safety of ceftazidime-avibactam plus metronidazole versus meropenem in the treatment of complicated intra-abdominal infection: results from a randomized, controlled, double-blind, phase 3 program. Clin Infect Dis. 2016;62(11):1380–1389. doi:10.1093/cid/ciw133
18. Wagenlehner FM, Sobel JD, Newell P, et al. Ceftazidime-avibactam versus doripenem for the treatment of complicated urinary tract infections, including acute pyelonephritis: RECAPTURE, a phase 3 randomized trial program. Clin Infect Dis. 2016;63(6):754–762. doi:10.1093/cid/ciw378
19. Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious diseases society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clinl Infect Dis. 2024;ciae403. doi:10.1093/cid/ciae403
20. Paul M, Carrara E, Retamar P, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin Microbiol Infect. 2022;28(4):521–547. doi:10.1016/j.cmi.2021.11.025
21. Daikos GL, Cisneros JM, Carmeli Y, et al. Aztreonam-avibactam for the treatment of serious infections caused by metallo-β-lactamase-producing Gram-negative pathogens: a Phase 3 randomized trial (ASSEMBLE). JAC Antimicrob Resist. 2025;7(4):dlaf131. doi:10.1093/jacamr/dlaf131
22. Grabein B, Arhin FF, Daikos GL, Moore LSP, Balaji V, Baillon-Plot N. Navigating the current treatment landscape of Metallo-β-Lactamase-producing gram-negative infections: what are the limitations? Infect Dis Ther. 2024;13(11):2423–2447. doi:10.1007/s40121-024-01044-8
23. Hidalgo-Tenorio C, Bou G, Oliver A, Rodríguez-Aguirregabiria M, Salavert M, Martínez-Martínez L. The challenge of treating infections caused by Metallo-β-Lactamase-producing gram-negative bacteria: a narrative review. Drugs. 2024;84(12):1519–1539. doi:10.1007/s40265-024-02102-8
24. Gatti M, Viaggi B, Rossolini GM, Pea F, Viale P. An evidence-based multidisciplinary approach focused on creating algorithms for targeted therapy of Infection-Related Ventilator-Associated Complications (IVACs) caused by pseudomonas aeruginosa and acinetobacter baumannii in critically ill adult patients. Antibiotics. 2021;11(1):33. doi:10.3390/antibiotics11010033
25. Gatti M, Viaggi B, Rossolini GM, Pea F, Viale P. An evidence-based multidisciplinary approach focused at creating algorithms for targeted therapy of infection-related ventilator associated complications (IVACs) caused by Enterobacterales in critically ill adult patients. Expert Rev Anti Infect Ther. 2022;20(3):331–352. doi:10.1080/14787210.2021.1976145
26. Gatti M, Viaggi B, Rossolini GM, Pea F, Viale P. An evidence-based multidisciplinary approach focused at creating algorithms for targeted therapy of BSIs, cUTIs, and cIAIs caused by enterobacterales in critically ill adult patients. Infect Drug Resist. 2021;14:2461–2498. doi:10.2147/IDR.S314241
27. Solomkin J, Hershberger E, Miller B, et al. Ceftolozane/Tazobactam plus metronidazole for complicated intra-abdominal infections in an era of multidrug resistance: results from a randomized, double-blind, phase 3 trial (ASPECT-cIAI). Clin Infect Dis. 2015;60(10):1462–1471. doi:10.1093/cid/civ097
28. Wagenlehner FM, Umeh O, Steenbergen J, Yuan G, Darouiche RO. Ceftolozane-tazobactam compared with levofloxacin in the treatment of complicated urinary-tract infections, including pyelonephritis: a randomised, double-blind, phase 3 trial (ASPECT-cUTI). Lancet. 2015;385(9981):1949–1956. doi:10.1016/S0140-6736(14)62220-0
29. Kollef MH, Nováček M, Kivistik Ü, et al. Ceftolozane-tazobactam versus meropenem for treatment of nosocomial pneumonia (ASPECT-NP): a randomised, controlled, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2019;19(12):1299–1311. doi:10.1016/S1473-3099(19)30403-7
30. Bassetti M, Echols R, Matsunaga Y, et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): a randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect Dis. 2021;21(2):226–240. doi:10.1016/S1473-3099(20)30796-9
31. Wunderink RG, Matsunaga Y, Ariyasu M, et al. Cefiderocol versus high-dose, extended-infusion meropenem for the treatment of Gram-negative nosocomial pneumonia (APEKS-NP): a randomised, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2021;21(2):213–225. doi:10.1016/S1473-3099(20)30731-3
32. Kaye KS, Bhowmick T, Metallidis S, et al. Effect of meropenem-vaborbactam vs piperacillin-tazobactam on clinical cure or improvement and microbial eradication in complicated urinary tract infection: the TANGO I randomized clinical trial. JAMA. 2018;319(8):788. doi:10.1001/jama.2018.0438
33. Wunderink RG, Giamarellos-Bourboulis EJ, Rahav G, et al. Effect and safety of meropenem–vaborbactam versus best-available therapy in patients with carbapenem-resistant enterobacteriaceae infections: the TANGO II randomized clinical trial. Infect Dis Ther. 2018;7(4):439–455. doi:10.1007/s40121-018-0214-1
34. Motsch J, Murta De Oliveira C, Stus V, et al. RESTORE-IMI 1: a multicenter, randomized, double-blind trial comparing efficacy and safety of imipenem/relebactam vs colistin plus imipenem in patients with imipenem-nonsusceptible bacterial infections. Clinl Infect Dis. 2020;70(9):1799–1808. doi:10.1093/cid/ciz530
35. Titov I, Wunderink RG, Roquilly A, et al. A randomized, double-blind, multicenter trial comparing efficacy and safety of imipenem/cilastatin/relebactam versus piperacillin/tazobactam in adults with hospital-acquired or ventilator-associated bacterial pneumonia (RESTORE-IMI 2 Study). Clinl Infect Dis. 2021;73(11):e4539–e4548. doi:10.1093/cid/ciaa803
36. Kaye KS, Belley A, Barth P, et al. Effect of cefepime/enmetazobactam vs piperacillin/tazobactam on clinical cure and microbiological eradication in patients with complicated urinary tract infection or acute pyelonephritis: a randomized clinical trial. JAMA. 2022;328(13):1304. doi:10.1001/jama.2022.17034
37. Kaye KS, Shorr AF, Wunderink RG, et al. Efficacy and safety of sulbactam–durlobactam versus colistin for the treatment of patients with serious infections caused by Acinetobacter baumannii–calcoaceticus complex: a multicentre, randomised, active-controlled, phase 3, non-inferiority clinical trial (ATTACK). Lancet Infect Dis. 2023;23(9):1072–1084. doi:10.1016/S1473-3099(23)00184-6
38. Wagenlehner FM, Gasink LB, McGovern PC, et al. Cefepime-taniborbactam in complicated urinary tract infection. N Engl J Med. 2024;390(7):611–622. doi:10.1056/NEJMoa2304748
39. Carmeli Y, Cisneros JM, Paul M, et al. Aztreonam-avibactam versus meropenem for the treatment of serious infections caused by Gram-negative bacteria (REVISIT): a descriptive, multinational, open-label, phase 3, randomised trial. Lancet Infect Dis. 2025;25(2):218–230. doi:10.1016/S1473-3099(24)00499-7
40. Bassetti M, Vena A, Giacobbe DR, et al. Ceftolozane/tazobactam for treatment of severe ESBL-Producing enterobacterales infections: a multicenter nationwide clinical experience (CEFTABUSE II Study). Open Forum Infect Diseases. 2020;7(5):ofaa139. doi:10.1093/ofid/ofaa139
41. Basoulis D, Gkoufa A, Mastrogianni E, et al. Comparison of ceftolozane/tazobactam and meropenem in treating bloodstream infections caused by extended-spectrum β-lactamase-producing Enterobacterales: a single-centre, retrospective, real-world study. J Antimicrob Chemother. 2025;80(8):2314–2322. doi:10.1093/jac/dkaf229
42. Isler B, Ezure Y, Romero JLGF, Harris P, Stewart AG, Paterson DL. Is ceftazidime/avibactam an option for serious infections due to Extended-Spectrum-β-Lactamase- and AmpC-producing enterobacterales ? A systematic review and meta-analysis. Antimicrob Agents Chemother. 2020;65(1):e01052–20. doi:10.1128/AAC.01052-20
43. Rahim Khorasani M, Rostami S, Bakhshi A, Sheikhi R. Global evaluation of the antibacterial activity of Ceftolozane/tazobactam against ESBLs-producing escherichia coli and klebsiella pneumoniae: a systematic review and meta-analysis. Therapeutic Advances in Infection. 2023;10:20499361231212074. doi:10.1177/20499361231212074
44. Pai MP, Cojutti PG, Gatti M, et al. Keeping the horse with the cart: are we underdosing tazobactam even when using continuous-infusion ceftolozane/tazobactam for effectively preventing resistance development by ESBL-producing Enterobacterales? Antimicrob Agents Chemother. 2025:e01215–25. doi:10.1128/aac.01215-25
45. Wi YM, Choi JY, Lee DE, Jun SH, Kwon KT, Ko KS. Antimicrobial activity of cephamycins and β-lactam/β-lactamase inhibitors against ESBL-producing Escherichia coli and Klebsiella pneumoniae unDer Standard and high bacterial inocula. Sci Rep. 2025;15(1):9785. doi:10.1038/s41598-025-90762-1
46. Hobson CA, Pierrat G, Tenaillon O, et al. Klebsiella pneumoniae carbapenemase variants resistant to ceftazidime-avibactam: an evolutionary overview. Antimicrob Agents Chemother. 2022;66(9):e00447–22. doi:10.1128/aac.00447-22
47. Ding L, Shen S, Chen J, et al. Klebsiella pneumoniae carbapenemase variants: the new threat to global public health. Clin Microbiol Rev. 2023;36(4):e00008–23. doi:10.1128/cmr.00008-23
48. Ackley R, Roshdy D, Meredith J, et al. Meropenem-vaborbactam versus ceftazidime-avibactam for treatment of carbapenem-resistant enterobacteriaceae infections. Antimicrob Agents Chemother. 2020;64(5):e02313–19. doi:10.1128/AAC.02313-19
49. Mezzadri L, Corti N, Ricci E, et al. Comparison of meropenem-vaborbactam with ceftazidime-avibactam in the treatment of carbapenem-resistant Enterobacterales infections. J Global Antimicrob Resist. 2024;39:4. doi:10.1016/j.jgar.2024.10.011
50. Marino A, Maraolo AE, Mazzitelli M, et al. Head-to-head: meropenem/vaborbactam versus ceftazidime/avibactam in ICUs patients with KPC-producing K. pneumoniae infections- results from a retrospective multicentre study. Infection. 2025. doi:10.1007/s15010-025-02608-7
51. Cojutti PG, Pai MP, Gatti M, et al. An innovative population pharmacokinetic/pharmacodynamic strategy for attaining aggressive joint PK/PD target of continuous infusion ceftazidime/avibactam against KPC- and OXA-48- producing Enterobacterales and preventing resistance development in critically ill patients. J Antimicrob Chemother. 2024;79(11):2801–2808. doi:10.1093/jac/dkae290
52. Gatti M, Rinaldi M, Cojutti PG, et al. A pre-post quasi-experimental study of antimicrobial stewardship exploring the impact of a multidisciplinary approach aimed at attaining an aggressive joint pharmacokinetic/pharmacodynamic target with ceftazidime/avibactam on treatment outcome of KPC-producing Klebsiella pneumoniae infections and on ceftazidime/avibactam resistance development. Antimicrob Agents Chemother. 2025:e0048825. doi:10.1128/aac.00488-25
53. Gatti M, Viale P, Pea F. Therapeutic drug monitoring of ceftazidime/avibactam: why one leg is not enough to run. J Antimicrob Chemother. 2024;79(1):195–199. doi:10.1093/jac/dkad367
54. Gatti M, Pea F. Jumping into the future: overcoming pharmacokinetic/pharmacodynamic hurdles to optimize the treatment of severe difficult to treat-Gram-negative infections with novel beta-lactams. Exp Rev Anti-Infective Ther. 2023;21(2):149–166. doi:10.1080/14787210.2023.2169131
55. la Calle C D, Rodríguez O, Morata L, et al. Clinical characteristics and prognosis of infections caused by OXA-48 carbapenemase-producing Enterobacteriaceae in patients treated with ceftazidime-avibactam. Int J Antimicrob Agents. 2019;53(4):520–524. doi:10.1016/j.ijantimicag.2018.11.015
56. Mert A, Derin O, Akalın H, et al. Multicenter evaluation of ceftazidime-avibactam use in carbapenem-resistant Klebsiella pneumoniae bloodstream infections in OXA-48 endemic regions. Sci Rep. 2024;14(1):26337. doi:10.1038/s41598-024-77259-z
57. Lima O, Sousa A, Longueira-Suárez R, et al. Ceftazidime-avibactam treatment in bacteremia caused by OXA-48 carbapenemase-producing Klebsiella pneumoniae. Eur J Clin Microbiol Infect Dis. 2022;41(9):1173–1182. doi:10.1007/s10096-022-04482-9
58. Aslan AT, Tanriverdi ES, Kaya SY, et al. Comparison of ceftazidime-avibactam with other appropriate antimicrobial therapy for the treatment of OXA-48- or KPC-producing enterobacterales infections in Türkiye: a multi-centre retrospective matched-cohort study. Int J Antimicrob Agents. 2025:107650. doi:10.1016/j.ijantimicag.2025.107650
59. Gupta N, Boodman C, Prayag P, Manesh A, Kumar TP. Ceftazidime-avibactam and aztreonam combination for Carbapenem-resistant enterobacterales bloodstream infections with presumed Metallo-β-lactamase production: a systematic review and meta-analysis. Expert Rev Anti Infect Ther. 2024;22(4):203–209. doi:10.1080/14787210.2024.2307912
60. Mauri C, Maraolo AE, Di Bella S, Luzzaro F, Principe L. The revival of aztreonam in combination with avibactam against Metallo-β-Lactamase-Producing Gram-Negatives: a systematic review of in vitro studies and clinical cases. Antibiotics. 2021;10(8):1012. doi:10.3390/antibiotics10081012
61. Warecki BA, Tamma PD, Bonomo RA, Vila AJ. NDM-driven cefiderocol resistance: effect and therapeutic considerations. Lancet Infect Dis. 2025;25(10):1068–1069. doi:10.1016/S1473-3099(25)00477-3
62. Falcone M, Giordano C, Leonildi A, et al. Clinical Features and outcomes of infections caused by Metallo-β-Lactamase–Producing enterobacterales: a 3-year prospective study from an endemic area. Clinl Infect Dis. 2024;78(5):1111–1119. doi:10.1093/cid/ciad725
63. Timsit JF, Paul M, Shields RK, et al. Cefiderocol for the treatment of infections due to Metallo-B-lactamase-Producing pathogens in the CREDIBLE-CR and APEKS-NP phase 3 randomized studies. Clin Infect Dis. 2022;75(6):1081–1084. doi:10.1093/cid/ciac078
64. Torre-Cisneros J, Almirante B, Martos CDLF, et al. Effectiveness and safety of cefiderocol treatment in patients with Gram-negative bacterial infections in Spain in the early access programme: results of the PERSEUS study. Eur J Clin Microbiol Infect Dis. 2025;44(6):1375–1390. doi:10.1007/s10096-025-05108-6
65. Gatti M, Cosentino F, Giannella M, Viale P, Pea F. Clinical efficacy of cefiderocol-based regimens in patients with carbapenem-resistant acinetobacter baumannii infections: a systematic review with meta-analysis. Int J Antimicrob Agents. 2024;63(2):107047. doi:10.1016/j.ijantimicag.2023.107047
66. Onorato L, de Luca I, Monari C, Coppola N. Cefiderocol either in monotherapy or combination versus best available therapy in the treatment of carbapenem-resistant acinetobacter baumannii infections: a systematic review and meta-analysis. J Infect. 2024;88(3):106113. doi:10.1016/j.jinf.2024.01.012
67. Gatti M, Cosentino F, Giannella M, Viale P, Pea F. In reply to the letter to the editor regarding “Clinical efficacy of cefiderocol-based regimens in patients with carbapenem-resistant acinetobacter baumannii infections: a systematic review with meta-analysis. Int J Antimicrob Agents. 2024;63(6):107168. doi:10.1016/j.ijantimicag.2024.107168
68. Shields RK, Paterson DL, Tamma PD. Navigating available treatment options for carbapenem-resistant acinetobacter baumannii-calcoaceticus complex infections. Clinl Infect Dis. 2023;76(Supplement_2):S179–S193. doi:10.1093/cid/ciad094
69. Shah P, Neeravi A, Karthik R, et al. Successful use of cefepime/zidebactam in deep-seated infections due to extensively drug-resistant Pseudomonas aeruginosa: a case series. J Glob Antimicrob Resist. 2025;44:464–469. doi:10.1016/j.jgar.2025.07.009
70. Polati VR, Gattu S, Maturu VN, Prakasham PS, Maqsood M. Investigational antibiotic cefepime/zidebactam as a therapeutic option for the treatment of an unyielding empyema in a paediatric patient caused by extensively drug-resistant pseudomonas aeruginosa: a case report. Eur J Clin Microbiol Infect Dis. 2025;44(6):1349–1355. doi:10.1007/s10096-025-05106-8
71. Tsai S, Nigo M, Kang D, et al. Cefepime-zidebactam therapy for extensively drug-resistant pseudomonas aeruginosa and klebsiella pneumoniae infection as a bridge to liver transplantation. JAC Antimicrob Resist. 2025;7(4):dlaf129. doi:10.1093/jacamr/dlaf129
72. Soman R, Sirsat R, Sunavala A, et al. Successful treatment of sino-pulmonary infection & skull base osteomyelitis caused by New Delhi metallo-β-lactamase-producing pseudomonas aeruginosa in a renal transplant recipient by using an investigational antibiotic cefepime/zidebactam (WCK 5222). Eur J Clin Microbiol Infect Dis. 2024. doi:10.1007/s10096-024-04791-1
73. Tirlangi PK, Wanve BS, Dubbudu RR, et al. Successful use of cefepime-zidebactam (WCK 5222) as a salvage therapy for the treatment of disseminated extensively drug-resistant New Delhi Metallo-β-Lactamase-Producing pseudomonas aeruginosa infection in an adult patient with acute t-cell leukemia. Antimicrob Agents Chemother. 2023;67(8):e0050023. doi:10.1128/aac.00500-23
74. Dubey D, Roy M, Shah TH, et al. Compassionate use of a novel β-lactam enhancer-based investigational antibiotic cefepime/zidebactam (WCK 5222) for the treatment of extensively-drug-resistant NDM-expressing pseudomonas aeruginosa infection in an intra-abdominal infection-induced sepsis patient: a case report. Ann Clin Microbiol Antimicrob. 2023;22(1):55. doi:10.1186/s12941-023-00606-x
75. Zhang P, Wu J, Xu Y, Wan H, Chen J, Huang M. Sulbactam-durlobactam treatment for pulmonary infections caused by carbapenem-resistant Acinetobacter baumannii in lung transplant recipients. J Infect. 2025;91(3):106596. doi:10.1016/j.jinf.2025.106596
76. Pouya N, Finch NA, Granillo A, Bhimraj A, Tam VH, Miller WR. Pharmacokinetics of sulbactam-durlobactam in patients with Acinetobacter baumannii ventriculitis: a report of two cases. Antimicrob Agents Chemother. 2025;e0067425. doi:10.1128/aac.00674-25
77. Fu C, Tang X, Guo X, Huang L, Gao J, Yang R. Sulbactam-durlobactam combination therapy for carbapenem-resistant Acinetobacter baumannii sepsis with cutaneous involvement in an infant with acute monocytic leukemia: a case report. Front Pharmacol. 2025;16:1633982. doi:10.3389/fphar.2025.1633982
78. Kufel WD, Zeineddine N, Fouad A, et al. Pharmacokinetic and pharmacodynamic evaluation of sulbactam-durlobactam in a critically ill patient on continuous venovenous hemofiltration infected with carbapenem-resistant Acinetobacter baumannii-calcoaceticus complex. Pharmacotherapy. 2025;45(7):396–402. doi:10.1002/phar.70027
79. Tamma PD, Immel S, Karaba SM, et al. Successful treatment of Carbapenem-Resistant Acinetobacter baumannii meningitis with sulbactam-durlobactam. Clinl Infect Dis. 2024:ciae210. doi:10.1093/cid/ciae210
80. Snowdin JW, Mercuro NJ, Madaio MP, Rawlings SA. Case report: successful treatment of OXA-23 Acinetobacter baumannii neurosurgical infection and meningitis with sulbactam-durlobactam combination therapy. Front Med. 2024;11:1381123. doi:10.3389/fmed.2024.1381123
81. VanNatta M, Grier L, Khan MH, et al. In vivo emergence of pandrug-resistant acinetobacter baumannii strain: comprehensive resistance characterization and compassionate use of sulbactam-durlobactam. Open Forum Infect Dis. 2023;10(10):ofad504. doi:10.1093/ofid/ofad504
82. Tiseo G, Giordano C, Leonildi A, et al. Salvage therapy with sulbactam/durlobactam against cefiderocol-resistant Acinetobacter baumannii in a critically ill burn patient: clinical challenges and molecular characterization. JAC-Antimicrob Resist. 2023;5(3):dlad078. doi:10.1093/jacamr/dlad078
83. Falagas ME, Romanos LT, Kontogiannis DS, Tsiara K, Kakoullis SA. Resistance of Gram-Negative bacteria to cefepime-enmetazobactam: a systematic review. Pathogens. 2025;14(8):777. doi:10.3390/pathogens14080777
84. Karlowsky JA, Hackel MA, Wise MG, et al. In vitro activity of Cefepime-Taniborbactam and comparators against clinical isolates of Gram-Negative Bacilli from 2018 to 2020: results from the Global Evaluation of Antimicrobial Resistance via Surveillance (GEARS) Program. Antimicrob Agents Chemother. 2023;67(1):e0128122. doi:10.1128/aac.01281-22
85. Jacobs MR, Abdelhamed AM, Good CE, et al. ARGONAUT-III and -V: susceptibility of carbapenem-resistant Klebsiella pneumoniae and multidrug-resistant Pseudomonas aeruginosa to the bicyclic boronate β-lactamase inhibitor taniborbactam combined with cefepime. Antimicrob Agents Chemother. 2024;68(9):e0075124. doi:10.1128/aac.00751-24
86. Sader HS, Castanheira M, Kimbrough JH, Kantro V, Mendes RE. Aztreonam/avibactam activity against a large collection of carbapenem-resistant Enterobacterales (CRE) collected in hospitals from Europe, Asia and Latin America (2019-21). JAC Antimicrob Resist. 2023;5(2):dlad032. doi:10.1093/jacamr/dlad032
87. Bonnin RA, Jeannot K, Santerre Henriksen A, Quevedo J, Dortet L. In vitro activity of cefepime-enmetazobactam on carbapenem-resistant Gram negatives. Clin Microbiol Infect. 2025;31(2):240–249. doi:10.1016/j.cmi.2024.09.031
88. Sader HS, Mendes RE, Duncan LR, Carvalhaes CG, Castanheria M. Antimicrobial activity of cefepime/zidebactam (WCK 5222), a β-lactam/β-lactam enhancer combination, against clinical isolates of Gram-negative bacteria collected worldwide (2018-19). J Antimicrob Chemother. 2022;77(10):2642–2649. doi:10.1093/jac/dkac233
89. Karlowsky JA, Hackel MA, McLeod SM, Miller AA. In vitro activity of sulbactam-durlobactam against global isolates of acinetobacter baumannii-calcoaceticus complex collected from 2016 to 2021. Antimicrob Agents Chemother. 2022;66(9):e0078122. doi:10.1128/aac.00781-22
90. Lasko MJ, Nicolau DP, Asempa TE. Clinical exposure–response relationship of cefepime/taniborbactam against Gram-negative organisms in the murine complicated urinary tract infection model. J Antimicrob Chemother. 2022;77(2):443–447. doi:10.1093/jac/dkab405
91. Albac S, Anzala N, Chavanet P, et al. In vivo efficacy of enmetazobactam combined with cefepime in a murine pneumonia model induced by OXA-48-producing Klebsiella pneumoniae. Microbiol Spectr. 2024;12(12):e0234524. doi:10.1128/spectrum.02345-24
92. Amoura A, Benchetrit L, Magréault S, et al. Impact of the inoculum size on the in vivo activity of the aztreonam-avibactam combination in a murine model of peritonitis due to Escherichia coli expressing CTX-M-15 and NDM-1. Arias CA, ed. Antimicrob Agents Chemother. 2025;69(2):e01288–22. doi:10.1128/aac.01288-22
93. Kidd JM, Abdelraouf K, Nicolau DP. Efficacy of human-simulated bronchopulmonary exposures of cefepime, zidebactam and the combination (WCK 5222) against MDR Pseudomonas aeruginosa in a neutropenic murine pneumonia model. J Antimicrob Chemother. 2019;dkz414. doi:10.1093/jac/dkz414
94. Moya B, Bhagwat S, Cabot G, Bou G, Patel M, Oliver A. Effective inhibition of PBPs by cefepime and zidebactam in the presence of VIM-1 drives potent bactericidal activity against MBL-expressing Pseudomonas aeruginosa. J Antimicrob Chemother. 2020;75(6):1474–1478. doi:10.1093/jac/dkaa036
95. Di Pilato V, Principe L, Andriani L, et al. Deciphering variable resistance to novel carbapenem-based β-lactamase inhibitor combinations in a multi-clonal outbreak caused by Klebsiella pneumoniae carbapenemase (KPC)-producing Klebsiella pneumoniae resistant to ceftazidime/avibactam. Clin Microbiol Infect. 2023;29(4):
96. Sangiorgio G, Calvo M, Stefani S. Aztreonam and avibactam combination therapy for metallo-β-lactamase-producing gram-negative bacteria: a Narrative Review. Clin Microbiol Infect. 2025;31(6):971–978. doi:10.1016/j.cmi.2024.11.006
97. Van Helden SR, Al Musawa M, Bleick CR, Herbin SR, Rybak MJ. Cefepime-taniborbactam: ushering in the era of metallo-β-lactamase inhibition. Pharmacotherapy. 2025;45(7):448–461. doi:10.1002/phar.70036
98. Le Terrier C, Gruenig V, Fournier C, Nordmann P, Poirel L. NDM-9 resistance to taniborbactam. Lancet Infect Dis. 2023;23(4):401–402. doi:10.1016/S1473-3099(23)00069-5
99. Le Terrier C, Viguier C, Nordmann P, Vila AJ, Poirel L. Relative inhibitory activities of the broad-spectrum β-lactamase inhibitor taniborbactam against metallo-β-lactamases. Antimicrob Agents Chemother. 2024;68(2):e0099123. doi:10.1128/aac.00991-23
100. Tamma PD, Munita JM. The metallo-β-lactamases strike back: emergence of taniborbactam escape variants. Antimicrob Agents Chemother. 2024;68(2):e0151023. doi:10.1128/aac.01510-23
101. Gatti M, Rinaldi M, Gaibani P, et al. A descriptive pharmacokinetic/pharmacodynamic analysis of continuous infusion ceftazidime-avibactam for treating DTR gram-negative infections in a case series of critically ill patients undergoing continuous veno-venous haemodiafiltration (CVVHDF). J Crit Care. 2023;76:154301. doi:10.1016/j.jcrc.2023.154301
102. Gatti M, Rinaldi M, Tonetti T, et al. Pharmacokinetics/pharmacodynamics of cefiderocol administered by continuous infusion in a case series of critically ill patients with carbapenem-resistant Acinetobacter baumannii infections undergoing continuous venovenous haemodiafiltration (CVVHDF). Int J Antimicrob Agents. 2023;62(2):106852. doi:10.1016/j.ijantimicag.2023.106852
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.