Back to Journals » Journal of Pain Research » Volume 18
Real-World Effectiveness and Tolerability of Low Dose Naltrexone to Treat Chronic Pain: A Retrospective Cohort Study of One Pain Physician’s Practice
Authors Aalto H ![]() , Paul S
, Paul S ![]() , McEwen V
, McEwen V ![]()
Received 19 September 2025
Accepted for publication 4 December 2025
Published 10 December 2025 Volume 2025:18 Pages 6637—6649
DOI https://doi.org/10.2147/JPR.S561662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert B. Raffa
Hannah Aalto,1 Sara Paul,1 Virginia McEwen2– 4
1Department of Undergraduate Medical Education, Northern Ontario School of Medicine (NOSM) University, Thunder Bay, Ontario, Canada; 2Chronic Pain Management Program, St. Joseph’s Care Group, Thunder Bay, ON, Canada; 3Interventional Pain Service, Thunder Bay Regional Health Sciences Centre, Thunder Bay, ON, Canada; 4Clinical Sciences Division, Northern Ontario School of Medicine (NOSM) University, Thunder Bay, ON, Canada
Correspondence: Hannah Aalto, Undergraduate Medical Education, Northern Ontario School of Medicine (NOSM) University, Thunder Bay, ON, Canada, Tel +1 807 632 2948, Email [email protected]
Purpose: Low-dose naltrexone (LDN) is an off-label treatment for chronic pain, with evidence supporting its use mainly consisting of small-scale studies. This retrospective cohort review aimed to contribute to this growing body of literature and evaluate the real-world effectiveness of LDN across a range of chronic pain conditions in a single physician’s practice.
Patients and Methods: A total of 128 patients prescribed LDN between September 2021 and June 2024 were reviewed independently by two investigators, with 93 meeting inclusion criteria. Patients were categorized into 12 groups based on diagnosis, with fibromyalgia representing the largest subgroup (27 patients). Retrospective cohort data was collected and included patient demographics, adverse effects, dosage, duration of therapy, and reported symptom relief. Descriptive statistics were used to analyze findings.
Results: Subjective symptom relief was reported by 53.8% of patients, most commonly improvements in pain (49 patients) and fatigue (25 patients), when taking LDN. The highest response rates were seen in patients with mast cell activation syndromes and arthritis-related conditions (71.4%). Adverse effects occurred in 49.5% of patients, most frequently nausea and fatigue. No serious adverse effects were reported.
Conclusion: These findings suggest that LDN may be an effective and well-tolerated treatment option for a range of chronic pain conditions. Further studies, such as randomized controlled trials, are warranted to confirm these results and optimize dosing strategies.
Keywords: chronic pain, low dose naltrexone, LDN, pain
Introduction
Chronic pain is a prevalent health issue, affecting 1 in 5 Canadians,1 with negative physical, emotional, and financial impacts on those experiencing it.2 Despite a wide array of available analgesics, response to pharmaceuticals for chronic pain is variable between individuals and often suboptimal. Pharmacological treatments for chronic pain have often been discovered by chance and repurposed off-label for chronic pain, but still with limited efficacy or intolerable side effects. Novel analgesics, particularly for chronic pain syndromes with nociplastic features, have been lacking. Low-dose naltrexone (LDN) has been increasingly used off-label in the treatment of chronic pain and inflammatory conditions. At low doses, it has immunomodulatory effects and decreases inflammation.3 Through modulation of glial cells and promotion of endorphin release, LDN may alleviate pain and improve quality of life.3 LDN is a promising treatment option for many patients living with chronic pain, including those who have not responded to other treatments.
Naltrexone was initially created in 1963 for treatment of opioid and alcohol addiction.4 It works through competitive mu, kappa, and delta opioid receptor antagonism, and is prescribed in doses of 50–100 mg per day.5 At these higher doses, it competitively blocks the binding of both beta-endorphins and exogenous opioids.6 It is theorized that naltrexone may exhibit a biphasic dose response phenomenon known as hormesis, characterized by low dose weak agonist effects, and high dose receptor inhibition.7,8 At low doses, opioid receptors are transiently blocked when naltrexone binds to them, causing both receptors and beta-endorphins to be upregulated.9,10 This was first explored clinically in 1985 by Dr Bernard Bihari for the treatment of human immunodeficiency virus (HIV).11 Naltrexone has immunomodulatory, anti-inflammatory, and antinociceptive properties when given at low doses.3,12 And since initial use in 1985, LDN has seen increasing popularity due to these effects. Several preliminary studies have found promising results for pain reduction.10,13–32
LDN is a Toll-like receptor 4 (TLR4) antagonist, which is one mechanism through which anti-inflammatory effects are thought to arise.3 TLR4s are found on microglia, the most prevalent immune cells of the nervous system.33 TLR4s on microglia can be activated by a variety of stimuli such as trauma, infection, and degeneration, and while controlled responses confer immunity, uncontrolled responses result in the release of proinflammatory factors that are recognized contributors to the experience of pain and fatigue.33,34 Known TLR4 mediated cytokines include interleukin-6, tumor necrosis factor alpha, and inflammatory nitric oxide.7,12 TLR4 is upregulated during inflammation, which increases nociception.35 It is hypothesized that both naltrexone and another opioid antagonist, naloxone, may inhibit pain and inflammation by preventing glial cells from releasing proinflammatory cytokines, as well as increasing the production of endorphins.3,21 TLR4 receptors are also present on mast cells and type 1 macrophages, both cells of the immune system that release a host of inflammatory mediators known to play roles in pain physiology.36–39 Evidence therefore suggests that LDN may have a role in minimizing the harmful effects of neuroinflammatory diseases by dampening glial cell activity, as well as immune cells such as type 1 macrophages and mast cells and their amplification of nociception.3,40
Dose variability is an important factor when considering effectiveness and the maximally effective dose of LDN for chronic pain is suggested to be idiosyncratic. The dosing range for LDN in chronic pain is generally considered to be 1–5 mg,6,41 with some studies suggesting that ultra-low doses have shown effect.18 A common test dose in patients with fibromyalgia and other types of chronic pain is 4.5mg.14,18,32,42 Bruun-Plesner et al estimated the dose effective in 50% to be 3.88mg, and the dose effective in 95% to be 5.40mg for patients with fibromyalgia.43 Marcus et al determined the maximally effective dose of LDN to be case dependent and titration necessary for each patient to ensure individualized efficacy of treatment.18 Case studies of chronic fatigue syndrome have used doses as high as 12 mg.44 The available literature reporting on the off-label use of LDN covers a diversity of treated conditions with variation in dosing highlighting only a preliminary understanding of what optimal dosing may be.
Most studies report minimal to no adverse effects with LDN, and side effects experienced commonly include nausea, insomnia, vivid dreams, dizziness, and/or headache.3,14,15,32,45,46 A limited side effect profile could make LDN a promising choice for chronic pain due to its safety, particularly in patient populations that may be more sensitive to medications such as the elderly. Through oral ingestion, 90% of naltrexone is absorbed from the gastrointestinal tract, however bioavailability is poor with estimates of 5–40% due to the first pass effect.6,12,41,47,48 Naltrexone undergoes renal clearance and thus may be contraindicated in some patients with severe renal disease, however mild impairment does not require dose adjustments.6,12 At higher doses, naltrexone is an opioid receptor antagonist.4 Due to the mechanism of action of LDN it may be used concurrently with opioids, although with potentially reduced efficacy. LDN has also shown some benefits in enhancing opioid sensitivity. Perioperative considerations may require temporary cessation of LDN just prior to surgery and in the immediate post-operative period. This is to ensure that patients requiring post-surgical opioids will have adequate analgesic effect. However, the implications of LDN use in perioperative pain have not been well studied.49 Some anecdotal evidence notes that patients with thyroid dysfunction may experience changing requirements of thyroid medication when on LDN due to it increasing thyroid function, however this correlation has not been found significant.50
Current literature surrounding LDN and chronic pain has focused on small scale case studies, retrospective cohort studies, and case reports. Chronic pain encompasses a variety of diagnoses, or simply the presence of idiopathic persistent pain. Arthritis,24,51 fibromyalgia,21,31,32,52–54 chronic fatigue syndrome and myalgic encephalomyelitis,44,55 multiple sclerosis,15,17,56,57 and complex regional pain syndrome35,58,59 are some of the many chronic pain conditions reported in the literature, through small studies and reports, for which LDN has been used to relieve pain. LDN has also been found to have effect in dermatological conditions60,61 and gastrointestinal disorders.16,23,26–28,62,63 The small-scale trials conducted have varying success rates and results, often attributed to low power.51,52,64 One randomized control trial (RCT) has been conducted using LDN, specifically looking at pain mechanisms in fibromyalgia.65,66 This RCT found there was no difference from placebo in reducing pain intensity or pressure pain threshold. However, conditioned pain modulation was found significantly different with LDN compared to placebo.66 Fibromyalgia is the only diagnosis for which LDN has been studied in an RCT. Given the limited number of large, controlled studies, expanding the real-world evidence base for LDN across diverse chronic pain conditions is essential to deepening our understanding of its therapeutic potential. Due to the common off-label use of LDN, small studies such as this one provide valuable insights into how it performs in everyday clinical contexts, thereby supporting clinicians in making informed decisions regarding its appropriateness as a treatment option. This retrospective cohort study of one pain physician’s practice contributes to the expansion of research into LDN for the treatment of chronic pain. This study was conducted to explore the real-world clinical utility and efficacy of LDN in various pain diagnoses as well as reported adverse effects to further the understanding of safety and tolerability of LDN.
Material and Methods
Study Design
This was a single center, retrospective cohort study evaluating subjective patient-reported efficacy of LDN on pain symptoms in the practice of a single pain physician in Thunder Bay, Ontario. All prescriptions written for LDN by the principal investigator between September 2021 and June 2024 were reviewed. Patients were eligible if they initiated LDN within this period. Exclusion criteria included failure to initiate LDN or loss to follow up. Patient data was retrieved by manual chart review from the electronic medical records (EMR) of both St. Joseph’s Care Group and Thunder Bay Regional Health Sciences Centre. Data from patients who met exclusion criteria were removed from the dataset prior to analysis. Data was anonymized and transcribed onto the online encrypted data platform Sync by two independent reviewers who were not members of the primary physician’s practice. Both reviewers were provided with a coding manual for protocols and guidelines on data collection, decision making in ambiguous situations, management of missing data, and limits to chart access. Each patient was given a unique identifier, so discrepancies between the two reviewers could be resolved by the physician. Patient sex at birth, age, and diagnoses were recorded. LDN dose was recorded in milligrams, and if LDN was taken more than once daily. Dosages were based clinically on balancing side effects and benefits, as per each patient’s subjective experience. Patients were started on 1.5 mg once daily, titrating up as high as 4.5 mg twice a day. The most common dose achieved was 4.5 mg once daily. Patients’ results were recorded regardless of dose achieved or duration of treatment (if patients discontinued it). The minimum number of weeks of treatment duration with LDN at time of review were recorded, and longer than 6 months recorded as >24. Adverse effects were recorded when reported in the patient chart. Efficacy for pain symptom reduction was recorded as either a yes or no, based on the patient’s subjective report. Pain scores were not available due to the retrospective, time-delayed nature of this study. If additional symptom improvements were found as per a patient’s report, these were also recorded. Any missing or insufficient data was noted, as were patients lost to follow up. Potential confounding variables such as other medications could not be accounted for due to the nature of a retrospective study; however, if the positive response could not specifically be attributed to LDN due to concurrent trials of other medications, the result was reported as negative. No control or comparator group was used. The reporting of this retrospective cohort review followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist. As this was a single-center, retrospective study, potential sources of bias may exist, including selection and reporting bias inherent to the design.
Ethical Approval and Consent
Ethical approval was obtained from the Research Ethics Board (REB) of both St. Joseph’s Care Group (REB #2024001) and Thunder Bay Regional Health Research Institute (REB #100282), in Thunder Bay, Ontario, Canada. Data from both institutions were anonymized and used retrospectively. Anonymization has not distorted scholarly meaning. This project meets the criteria of Article 5.5A of the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans. This study adheres to the Helsinki Declaration and abides by principal 32. A Waiver of Consent was received from both institutions, as both were satisfied there was no risk to individual patients, and appropriate measures were taken to safeguard the individual patient’s personal health information. No identifiable data was reported, and all results were presented in aggregate form.
Statistical Analysis
Data is stratified based on differing pain diagnoses to compare diagnoses and response to LDN exposure. Stratification provides an overall and adjusted effect estimate of a given exposure to LDN. Twelve different groupings were made by diagnosis. Fibromyalgia, widespread pain, and central sensitization are grouped together due to similar pain presentation. Arthralgia, arthritis, and osteoarthritis were grouped as one for the same reason. The other individual categories are low back pain, neuropathic pain, myofascial pain, complex regional pain syndrome (CRPS), pelvic pain, abdominal pain, headache, myalgic encephalitis/chronic fatigue syndrome, hypermobility spectrum disorder/Ehlers-Danlos Syndrome, and mast cell activation syndrome (MCAS). Descriptive statistics were calculated in Microsoft Excel. Percentages were calculated for patient characteristics and efficacy for each group.
Results
This retrospective review contained 128 patients that were prescribed LDN within this single center practice. Of the 128 patients, 35 were excluded from this analysis due to the patient not initiating the medication, being lost to follow-up, or transfer of care to other physicians, leaving 93 patients for this analysis. Ages ranged from 18 to 89, with an average age of 47. Three male patients and 32 female patients were excluded, leaving 17 males and 76 females in the study.
Indications for LDN included 12 different diagnostic categories. Multiple diagnoses were grouped into the same categories if the pain presentation was similar. Fibromyalgia, widespread pain, and central sensitization was the largest category with 27 patients, making up 29.0% of patients (Table 1). The next largest category was low back pain, with 11 patients, or 11.8%. CRPS, abdominal pain, and myofascial pain were the categories with the smallest cohorts with three, two, and one patient, respectively.
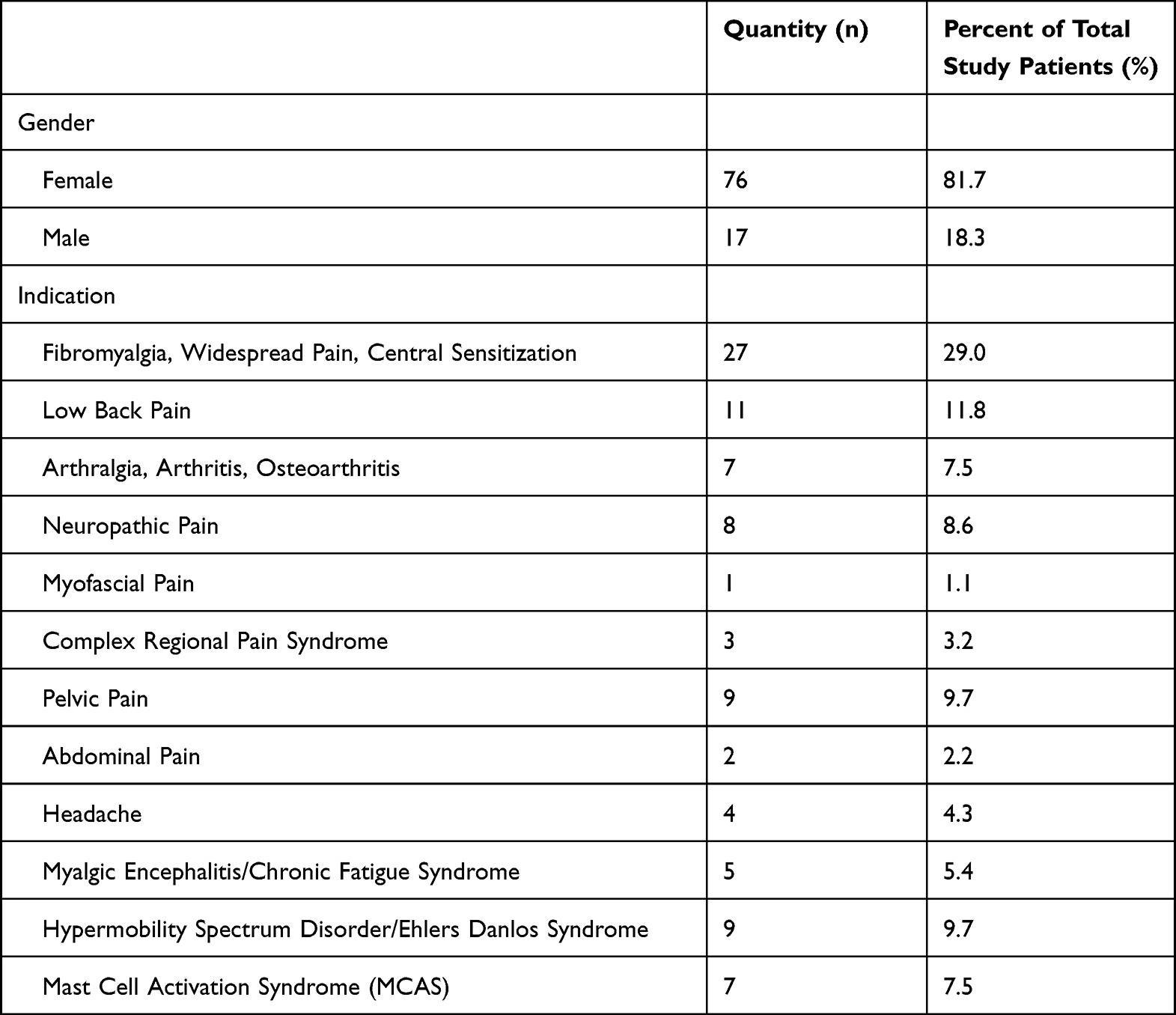 |
Table 1 Patient Characteristics |
Adverse effects were reported in 49.5% of patients. Of the 46 patients reporting adverse effects, 22 stated they were transient. Some patients only experienced one undesirable effect, while others experienced multiple. The most common adverse effect was nausea, with 18 patients reporting this symptom (Table 2). Fatigue was the next most common, with seven patients, followed by vivid dreams, and insomnia, each with six patients reporting. Of the 43 patients who stopped taking LDN or did not report efficacy, 25 reported at least one adverse effect. There were 21 patients who experienced an adverse effect while on LDN who opted to continue to take it due to its benefits. There were 44 patients in the study who reported having at least one adverse effect but also did not benefit from LDN, as indicated in the fourth column of Tables 2 and 3.
 |
Table 2 Reported Adverse Effects Experienced by Multiple Patients |
 |
Table 3 Reported Adverse Effects Experienced by Only One Patients |
Table 4 demonstrates subjective patient-reported efficacy of LDN across the various diagnostic strata. Fifty of 93 total patients found subjective pain relief or benefit for other symptoms with the use of LDN. Of the 27 patients with fibromyalgia, widespread pain, or central sensitization, a mean of 55.6% reported symptom relief. The groups with highest efficacy were arthralgia, arthritis, osteoarthritis, and mast cell activation syndrome. Both groups found 71.4% of patients reporting benefit, with seven patients in each group. Across all chronic diagnoses in the study, a mean of 53.8% of patients had some benefit for pain while using LDN.
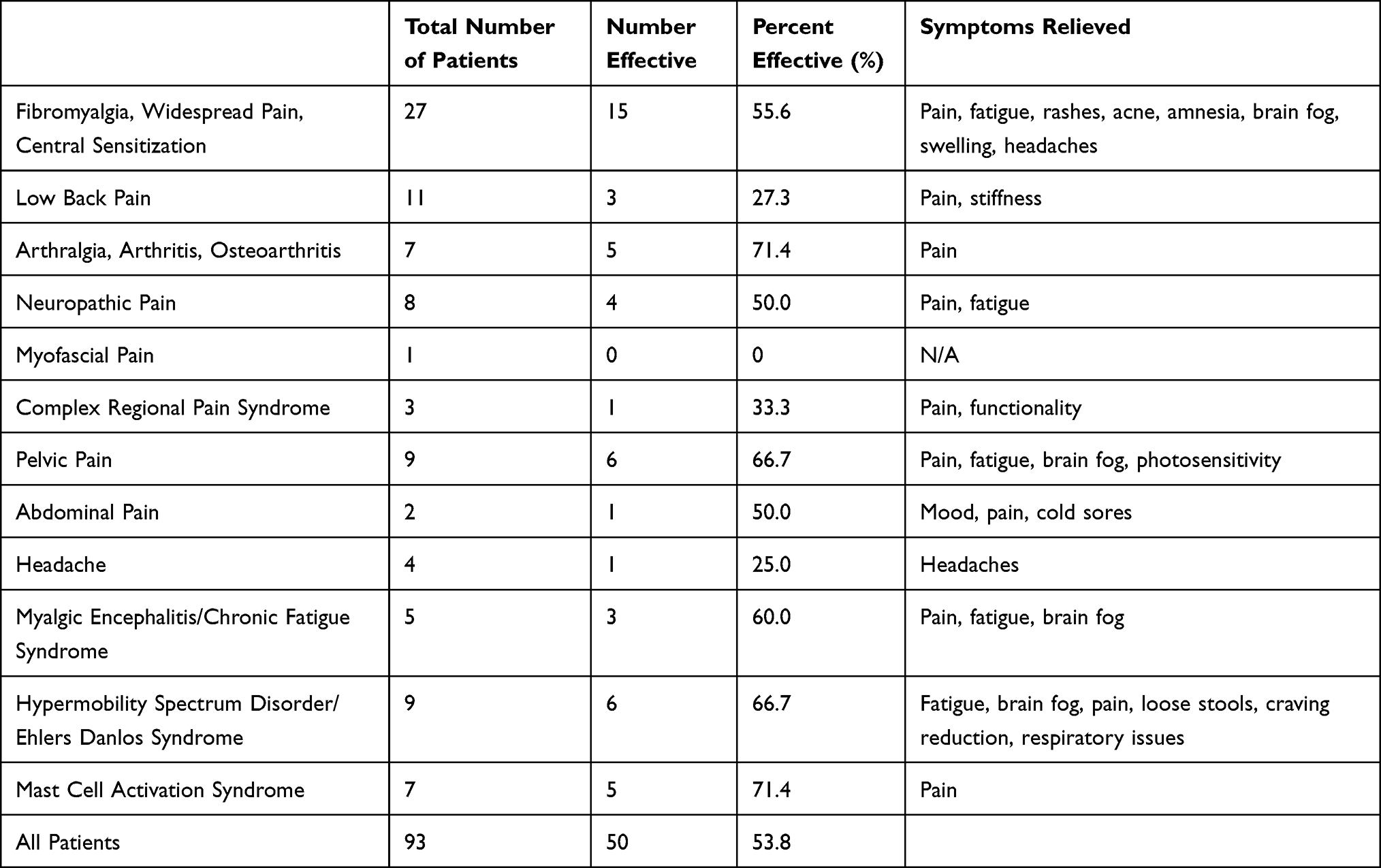 |
Table 4 Subjective Efficacy of LDN |
Patients who responded favourably to LDN reported relief in one or more symptoms (Table 5). The most common symptom relieved was pain with 49 patients reporting this as a benefit, followed by 25 patients with less fatigue, and six patients with a reduction in brain fog. Two patients found headache relief, and several patients experienced improvement of other symptoms following LDN initiation.
 |
Table 5 Relief of Symptoms |
Discussion
Reported Benefits
This retrospective cohort review adds to the evolving body of evidence that LDN may provide meaningful benefit across a range of chronic pain conditions, particularly those with inflammatory or nociplastic mechanisms due to its immunomodulatory, anti-inflammatory, and antinociceptive properties. Of the 93 patients who initiated LDN, 53.8% reported some benefit. Pain relief was the most frequently improved symptom with LDN, followed by improvements in fatigue and brain fog.
These findings are consistent with much of the existing literature, particularly for the treatment of fibromyalgia. LDN use in fibromyalgia has been reported in small scale trials reporting symptom improvement ranging from 30% to 60%, as well as an RCT.31,32,66 Two separate single-blind crossover studies have found symptom relief and decreased pro-inflammatory cytokines when using LDN for fibromyalgia.21,31 A randomized, double-blind, placebo-controlled, crossover study with 31 women also found LDN offered analgesic effect with 57% of patients reporting benefit,32 while another study with 15 fibromyalgia patients found LDN improved pain.53 There have been two trials with under 100 participants focused on fibromyalgia that found no analgesic benefit with LDN over placebo, one being an RCT.52,66 Although the RCT did not find statistically significant pain reduction when using LDN versus placebo, more patients quantitatively responded to LDN than they did placebo.66 This study is congruent with the current body of literature, in which most of LDN’s success is related to anecdotal evidence and smaller studies.10,13–32 Although statistical significance has been inconsistent in small samples, clinical response may be meaningful for a subset of patients.
ME/CFS treatment by LDN was reported effective in 60.0% of our patients with ME/CFS, mirroring a retrospective study where 74% of 218 participants benefitted from LDN.55 LDN for ME/CFS has also been shown effective through case reports.44 Evidence for pelvic pain and MCAS is limited to case reports of success,67–69 congruent with our response rates of 66.7% and 71.4% of patients, respectively. The subset of seven patients with arthritis, arthralgia, or osteoarthritis reported analgesic benefit, with a mean response of 71.4%. However, a double blind, randomized, placebo controlled, crossover clinical trial for 23 patients with arthritis did not find significant difference in analgesic effect between LDN and placebo.51
About 66.7% of the reported patients with Hypermobility Spectrum Disorder (HSD) or Ehlers–Danlos Syndrome (EDS) found benefit using LDN, particularly with reduction of fatigue. Only half of those who improved reported reduced pain. This diagnosis category consisted of nine total patients. A 2024 study exploring dosing of LDN for chronic pain had HSD/EDS as the most common diagnosis within the study, showing LDN being used to treat this diagnosis with some success.18 A case report on 56-year-old woman with both EDS and CRPS reported relief for her gastrointestinal issues, chronic pain, and fatigue.59
Our findings contribute to emerging evidence that LDN may aid in the treatment of CRPS. A prior case report demonstrated improvement in patients with CRPS and EDS,35,58 while a 2023 retrospective study found high response rates in CRPS and neuropathic pain.20 Nine out of 12 of their CRPS patients responded to LDN.20 Our study had a smaller CRPS sample but adds support LDN may be effective for some patients with CRPS.
In contrast, benefit for low back pain (27.3%) and neuropathic pain (50%) was more modest. In retrospective analysis, with 18 patients experiencing back pain, 33% found benefit with LDN.20 A 35-year-old man suffering from chronic back pain for two years trialled LDN with great effect, allowing him to return to full-time work.70 Neuropathic pain has shown success in the literature, with 14 of 21 patients experiencing benefit in a chart review.20 Reports of headache improvement are rare, with only one patient in this study adding to a previous case report.71 Headaches are often reported as a side effect of LDN.3,13
One of the two patients in the sample with abdominal pain reported benefit. A previous study of patients with inflammatory bowel disease on LDN found 74.5% found clinical improvement, while 25.5% of patients experienced remission.16 Another study looking at the Norwegian Prescription Database, this time for LDN for inflammatory bowel disease, again found a decrease in the number of dispenses of other medications once a patient initiated LDN, supporting analgesic benefit.23 LDN has also been found to be effective in Crohn’s disease.26–28,63
Between these conditions and fibromyalgia, our findings suggest LDN may be best suited to treat conditions with inflammatory or nociplastic components, consistent with its mechanisms of action involving proinflammatory cytokine blockage, glial cell modulation, and increased endorphin production. The results of this retrospective cohort study also suggest broad applications of LDN across multiple conditions, with the ability to treat or improve a large variety of symptoms, as seen in Table 5.
Expanding Treatments for Chronic Pain
Opioids, although not first line, are still commonly used in the treatment of chronic pain. Finding alternative therapies will help reduce the number of people exposed to the potential harmful effects of opioids, including addiction. Other chronic pain treatments, such as NSAIDs, tricyclic antidepressants, and gabapentinoids often have an undesired side effect profile. Minimal adverse effects while still experiencing symptom relief are uncommon among the current pharmaceutical options for chronic pain, making LDN a promising alternative.
Due to its multiple mechanisms of action, LDN is a promising option for a variety of pain conditions. LDN has been shown to decrease pro-inflammatory cytokines,21 and it has reported immunomodulation, anti-inflammation, TLR4 receptor antagonism, and glial cell modulation as contributing mechanisms of action.3 The broad mechanisms of action make it a viable treatment option for a variety of conditions.
Two studies in Norway examined the Norwegian Prescription Database to determine changes in trends of dispensing other medications for treatment of inflammatory bowel disease and arthritis, respectively, when patients were prescribed LDN.23,24 In the inflammatory bowel disease cohort, there was a reduction in filling of prescriptions for other drugs for disease treatment when patients were taking LDN.23 In the arthritis cohort, the prescription database noted correlating trends in patients prescribed LDN simultaneously reduced their opioid and NSAID use.24 LDN seems to present a potentially safer pharmaceutical option to help manage pain in patients with chronic pain conditions.
Adverse Effects
While LDN has not been found to result in serious adverse effects, this contrasts greatly with opioids, which can result in tolerance, addiction, respiratory depression, and a litany of other adverse effects.72 Use of opioids can also cause hyperalgesia and allodynia.72 NSAIDs likewise are associated with some serious side effects, such as gastrointestinal ulceration and bleeding, or cardiovascular toxicity.73 LDN may present a safer adjunct or alternative to current medications used in treating chronic pain, making it a more feasible option for patient populations with increased risks, and in a wide variety of pain diagnoses. This study also highlighted the management of chronic pain in a real-world setting, where some patients have multiple comorbidities.
The tolerability of LDN in this study was favourable. Adverse effects occurred in 46 patients, representing 49.5% of the population within this study. These were mainly mild, transient, and none were life threatening. Notably, 21 patients discontinued LDN due to lack of efficacy, while 25 stopped due to adverse effects that may have precluded benefit. The most common adverse effect was nausea, with 18 cases reported, 12 of which were transient. Nine patients who reported nausea discontinued LDN. The next most common adverse effects reported were fatigue with seven patients, and vivid dreams and insomnia each with six patients, respectively. A variety of other adverse effects were reported in this study; however, most were experienced by only one patient.
Naltrexone has generally not been found to cause any serious adverse effects.12,45,46,74,75 A 2008 pilot study on LDN for multiple sclerosis reported two patients with serious adverse effects, one being renal failure and the other lung carcinoma.15 The patient with renal failure was found to have polycystic kidney disease, and there are no known correlations between LDN and carcinoma; it is believed neither serious adverse effect can be attributed specifically to LDN.15 Nausea, fatigue, and vivid dreams are reportedly the most common effects.3,32,56,76 Anxiety, headaches, and insomnia are also commonly reported, aligning with the data found in this analysis.14,32,76 The absence of serious complications underscores LDN’s potential safety across diverse pain conditions.
Limitations
A limitation of this study is the constraints of a retrospective review using patient reported satisfaction, as opposed to a prospective approach collecting quantitative pain scores pre- and post-treatment. Results may have been affected by patient recollection of benefits between appointments. Having baseline pain scores and changes to this score using a validated rating as the patient progressed on LDN could have provided a more objective measurement of clinically significant reduction of pain, which is often considered to be 30%. Included data was limited to what was recorded within the charts and may have underreported adverse effects in some patients when the benefit outweighed the adverse effect. Several patients were lost to follow up, and several others declined to initiate a trial of LDN for unknown reasons. This, combined with patients stopping LDN prior to six months due to no perceived benefit or adverse effects, may have resulted in selection bias. Further, it was not possible to select an equal number of males and females due to the retrospective nature of the study.
The sample size within this dataset is modest with only 93 patients, and several strata had very few patients. There were a variety of discrepancies in terms of the percentage of patients who found benefit while using LDN when comparing this study to previous literature, which may be a result of small sample sizes in both this study and the literature. This study was also conducted at a single centre, limiting its generalizability to broader populations. The small number of patients also limited the ability to make population-level generalizations on the utility of LDN.
In some cases, it was unclear if treatment cessation was due to side effects or to lack of efficacy; also, it was not always reported which symptom was most prevalent and bothersome to the patient. Another limitation is the varied nature of the diagnoses within this study and that many patients had more than one chronic pain condition but were evaluated solely based on their primary pain diagnosis. Considering this was a retrospective study, it was not possible to account for any confounding variables. If patients were on other medications or seeking other treatments, these were not stopped while trialing LDN, which may have had unknown effects.
Conclusion
Low-dose naltrexone is a promising option for the treatment of various chronic pain conditions. This retrospective study demonstrated that 53.8% of patients experienced subjective improvement in pain symptoms with minimal side effects, none of which were serious or life-threatening. Its oral administration and favourable risk-benefit profile support the consideration of LDN as a chronic pain treatment for various conditions. This expands the therapeutic options available to patients amid the current real-world limitations of safe and effective chronic pain medications. Further large scale, randomized studies could be done to determine efficacy of LDN for the treatment of chronic pain, with particular focus on different conditions and which symptoms are alleviated.
Abbreviations
LDN, low dose naltrexone; HIV, human immunodeficiency virus; TLR4, toll-like receptor 4; RCT. Randomized control trial; EMR, electronic medical record; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; MCAS, mast cell activation syndrome; CRPS, chronic regional pain syndrome; HSD, hypermobility spectrum disorder; EDS, Ehlers–Danlos Syndrome.
Acknowledgments
The undergraduate authors of this study received financial support for time dedicated to the project from the Northern Ontario School of Medicine (NOSM) University’s Summer Medical Student Research Award and by the Northern Ontario Academic Medicine Association’s (NOAMA) Local Education Group.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Government of Canada. Canadian Pain Task Force. 2020. Available from: https://www.canada.ca/en/health-canada/corporate/about-health-canada/public-engagement/external-advisory-bodies/canadian-pain-task-force.html.
2. Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. A Blueprint for Transforming Pain Prevention, Care, Education, and Research. In: Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research. National Academies Press (US); 2011. Available from: https://www.ncbi.nlm.nih.gov/books/NBK92514/.
3. Younger J, Parkitny L, McLain D. The use of low-dose naltrexone (LDN) as a novel anti-inflammatory treatment for chronic pain. Clin Rheumatol. 2014;33(4):451–459. doi:10.1007/s10067-014-2517-2
4. Srivastava AB, Gold MS. Naltrexone: a History and Future Directions. Cerebrum Dana Forum Brain Sci. 2018;2018:13–18.
5. Kim PS, Fishman MA. Low-Dose Naltrexone for Chronic Pain: update and Systemic Review. Curr Pain Headache Rep. 2020;24(10):64. doi:10.1007/s11916-020-00898-0
6. Dara P, Farooqui Z, Mwale F, Choe C, van Wijnen AJ, Im HJ. Opiate Antagonists for Chronic Pain: a Review on the Benefits of Low-Dose Naltrexone in Arthritis versus Non-Arthritic Diseases. Biomedicines. 2023;11(6):1620. doi:10.3390/biomedicines11061620
7. Cant R, Dalgleish AG, Allen RL. Naltrexone Inhibits IL-6 and TNFα Production in Human Immune Cell Subsets following Stimulation with Ligands for Intracellular Toll-Like Receptors. Front Immunol. 2017;8. doi:10.3389/fimmu.2017.00809
8. Kim YHJ, West K. Treating chronic pain with low dose naltrexone and ultralow dose naltrexone: a review paper. J Pain Manag Ther. 2019;3(1):1.
9. Brown N, Panksepp J. Low-dose naltrexone for disease prevention and quality of life. Med Hypotheses. 2009;72(3):333–337. doi:10.1016/j.mehy.2008.06.048
10. Jackson D, Singh S, Zhang-James Y, Faraone S, Johnson B. The Effects of Low Dose Naltrexone on Opioid Induced Hyperalgesia and Fibromyalgia. Front Psychiatry. 2021;12:1. doi:10.3389/fpsyt.2021.593842
11. Bihari B, Strub SO. Efficacy of low dose naltrexone as an immune stabilizing agent for the treatment of HIV/ AIDS. AIDS Patient Care. 1995;9(1):3. doi:10.1089/apc.1995.9.3
12. Patten DK, Schultz BG, Berlau DJ. The Safety and Efficacy of Low‐Dose Naltrexone in the Management of Chronic Pain and Inflammation in Multiple Sclerosis, Fibromyalgia, Crohn’s Disease, and Other Chronic Pain Disorders. Pharmacother J Hum Pharmacol Drug Ther. 2018;38(3):382–389. doi:10.1002/phar.2086
13. Dieckmann G, Ozmen MC, Cox SM, Engert RC, Hamrah P. Low-dose naltrexone is effective and well-tolerated for modulating symptoms in patients with neuropathic corneal pain. Ocul Surf. 2021;20:33–38. doi:10.1016/j.jtos.2020.12.003
14. Driver CN, D’Souza RS. Efficacy of Low-Dose Naltrexone and Predictors of Treatment Success or Discontinuation in Fibromyalgia and Other Chronic Pain Conditions: a Fourteen-Year, Enterprise-Wide Retrospective Analysis. Biomedicines. 2023;11(4):1087. doi:10.3390/biomedicines11041087
15. Gironi M, Martinelli-Boneschi F, Sacerdote P, et al. A pilot trial of low-dose naltrexone in primary progressive multiple sclerosis. Mult Scler Houndmills Basingstoke Engl. 2008;14(8):1076–1083. doi:10.1177/1352458508095828
16. Lie MRKL, van der Giessen J, Fuhler GM, et al. Low dose Naltrexone for induction of remission in inflammatory bowel disease patients. J Transl Med. 2018;16(1):55. doi:10.1186/s12967-018-1427-5
17. Ludwig MD, Turel AP, Zagon IS, McLaughlin PJ. Long-term treatment with low dose naltrexone maintains stable health in patients with multiple sclerosis. Mult Scler J - Exp Transl Clin. 2016;2:2055217316672242. doi:10.1177/2055217316672242
18. Marcus NJ, Robbins L, Araki A, Gracely EJ, Theoharides TC. Effective Doses of Low-Dose Naltrexone for Chronic Pain – an Observational Study. J Pain Res. 2024;17:1273–1284. doi:10.2147/JPR.S451183
19. Martin SJ, McAnally HB, Okediji P, Rogosnitzky M. Low-dose naltrexone, an opioid-receptor antagonist, is a broad-spectrum analgesic: a retrospective cohort study. Pain Manag. 2022;12(6):699–709. doi:10.2217/pmt-2021-0122
20. McKenzie-Brown AM, Boorman DW, Ibanez KR, Agwu E, Singh V. Low-Dose Naltrexone (LDN) for Chronic Pain at a Single Institution: a Case Series. J Pain Res. 2023;16:1993–1998. doi:10.2147/JPR.S389957
21. Parkitny L, Younger J. Reduced Pro-Inflammatory Cytokines after Eight Weeks of Low-Dose Naltrexone for Fibromyalgia. Biomedicines. 2017;5(2):16. doi:10.3390/biomedicines5020016
22. Pogue J, Johnson D, Burch A. A Utilization Review of Patients That Respond to Low-Dose Naltrexone (LDN) for Chronic Pain at a Single Institution. J Pain Palliat Care Pharmacother. 2024;2024:1–8. doi:10.1080/15360288.2024.2358941
23. Raknes G, Simonsen P, Småbrekke L. The Effect of Low-Dose Naltrexone on Medication in Inflammatory Bowel Disease: a Quasi Experimental Before-and-After Prescription Database Study. J Crohns Colitis. 2018;12(6):677–686. doi:10.1093/ecco-jcc/jjy008
24. Raknes G, Småbrekke L. Low dose naltrexone: effects on medication in rheumatoid and seropositive arthritis. A nationwide register-based controlled quasi-experimental before-after study. PLoS One. 2019;14(2):e0212460. doi:10.1371/journal.pone.0212460
25. Roehmer C, Deshpande K, Khan S, Navlani R, Chu A. Low-dose naltrexone for treatment of refractory chronic pain. J Pain Manag. 2022;15(2):119–123.
26. Smith JP, Bingaman SI, Ruggiero F, et al. Therapy with the Opioid Antagonist Naltrexone Promotes Mucosal Healing in Active Crohn’s Disease: a Randomized Placebo-Controlled Trial. Dig Dis Sci. 2011;56(7):2088–2097. doi:10.1007/s10620-011-1653-7
27. Smith JP, Field D, Bingaman SI, Evans R, Mauger DT. Safety and Tolerability of Low-dose Naltrexone Therapy in Children With Moderate to Severe Crohn’s Disease: a Pilot Study. J Clin Gastroenterol. 2013;47(4):339. doi:10.1097/MCG.0b013e3182702f2b
28. Smith JP, Stock H, Bingaman S, Mauger D, Rogosnitzky M, Zagon IS. Low-Dose Naltrexone Therapy Improves Active Crohn’s Disease. Off J Am Coll Gastroenterol ACG. 2007;102(4):820. doi:10.1111/j.1572-0241.2007.01045.x
29. Srinivasan A, Dutta P, Bansal D, Chakrabarti A, Bhansali AK, Hota D. Efficacy and safety of low-dose naltrexone in painful diabetic neuropathy: a randomized, double-blind, active-control, crossover clinical trial. J Diabetes. 2021;13(10):770–778. doi:10.1111/1753-0407.13202
30. Tamariz L, Bast E, Klimas N, Palacio A. Low-dose Naltrexone Improves post–COVID-19 condition Symptoms. Clin Ther. 2024;46(3):e101–e106. doi:10.1016/j.clinthera.2023.12.009
31. Younger J, Mackey S. Fibromyalgia Symptoms Are Reduced by Low-Dose Naltrexone: a Pilot Study. Pain Med. 2009;10(4):663–672. doi:10.1111/j.1526-4637.2009.00613.x
32. Younger J, Noor N, McCue R, Mackey S. Low-dose naltrexone for the treatment of fibromyalgia: findings of a small, randomized, double-blind, placebo-controlled, counterbalanced, crossover trial assessing daily pain levels. Arthritis Rheum. 2013;65(2):529–538. doi:10.1002/art.37734
33. Watkins LR, Hutchinson MR, Ledeboer A, Wieseler-Frank J, Milligan ED, Maier SF. Glia as the “bad guys”: implications for improving clinical pain control and the clinical utility of opioids. Brain Behav Immun. 2007;21(2):131–146. doi:10.1016/j.bbi.2006.10.011
34. Kelley KW, Bluthé RM, Dantzer R, et al. Cytokine-induced sickness behavior. Brain Behav Immun. 2003;17(1):112–118. doi:10.1016/S0889-1591(02)00077-6
35. Chopra P, Cooper MS. Treatment of Complex Regional Pain Syndrome (CRPS) Using Low Dose Naltrexone (LDN). J Neuroimmune Pharmacol. 2013;8(3):470–476. doi:10.1007/s11481-013-9451-y
36. Bruno K, Woller SA, Miller YI, et al. Targeting Toll-like receptor-4 (TLR4) – emerging therapeutic target for persistent pain states. Pain. 2018;159(10):1908–1915. doi:10.1097/j.pain.0000000000001306
37. McCurdy JD, Lin TJ, Marshall JS. Toll-like receptor 4-mediated activation of murine mast cells. J Leukoc Biol. 2001;70(6):977–984. doi:10.1189/jlb.70.6.977
38. Ramachandran R, Wang Z, Saavedra C, et al. Role of Toll-like receptor 4 signaling in mast cell-mediated migraine pain pathway. Mol Pain. 2019;15:1744806919867842. doi:10.1177/1744806919867842
39. Theoharides TC, Twahir A, Kempuraj D. Mast cells in the autonomic nervous system and potential role in disorders with dysautonomia and neuroinflammation. Ann Allergy Asthma Immunol. 2024;132(4):440–454. doi:10.1016/j.anai.2023.10.032
40. Milligan ED, Maier SF, Watkins LR. Review: neuronal-glial interactions in central sensitization. Semin Pain Med. 2003;1(3):171–183. doi:10.1016/S1537-5897(03)00044-2
41. Toljan K, Vrooman B. Low-Dose Naltrexone (LDN)—Review of Therapeutic Utilization. Med Sci. 2018;6(4):82. doi:10.3390/medsci6040082
42. Soin A, Soin Y, Dann T, et al. Low-Dose Naltrexone Use for Patients with Chronic Regional Pain Syndrome: a Systematic Literature Review. Pain Physician. 2021;24(4):E393–E406.
43. Bruun-Plesner K, Blichfeldt-Eckhardt MR, Vaegter HB, Lauridsen JT, Amris K, Toft P. Low-Dose Naltrexone for the Treatment of Fibromyalgia: investigation of Dose–Response Relationships. Pain Med. 2020;21(10):2253–2261. doi:10.1093/pm/pnaa001
44. Bolton MJ, Chapman BP, Marwijk HV. Low-dose naltrexone as a treatment for chronic fatigue syndrome. BMJ Case Rep CP. 2020;13(1):e232502. doi:10.1136/bcr-2019-232502
45. Bolton M, Hodkinson A, Boda S, et al. Serious adverse events reported in placebo randomised controlled trials of oral naltrexone: a systematic review and meta-analysis. BMC Med. 2019;17(1):10. doi:10.1186/s12916-018-1242-0
46. Ploesser J, Weinstock LB, Thomas E. Low dose naltrexone: side effects and efficacy in gastrointestinal disorders. Int J Pharm Compd. 2010;14(2):171–173.
47. Greig SL, Keating GM. Naltrexone ER/Bupropion ER: a Review in Obesity Management. Drugs. 2015;75(11):1269–1280. doi:10.1007/s40265-015-0427-5
48. Trofimovitch D, Baumrucker SJ. Pharmacology Update: low-Dose Naltrexone as a Possible Nonopioid Modality for Some Chronic, Nonmalignant Pain Syndromes. Am J Hosp Palliat Med. 2019;36(10):907–912. doi:10.1177/1049909119838974
49. Goel A, Kapoor B, Wu M, et al. Perioperative Naltrexone Management: a Scoping Review by the Perioperative Pain and Addiction Interdisciplinary Network. Anesthesiology. 2024;141(2):388–399. doi:10.1097/ALN.0000000000005040
50. Raknes G, Småbrekke L. No change in the consumption of thyroid hormones after starting low dose naltrexone (LDN): a quasi-experimental before-after study. BMC Endocr Disord. 2020;20(1):151. doi:10.1186/s12902-020-00630-4
51. Beaudette-Zlatanova B, Lew RA, Otis JD, et al. Pilot Study of Low-dose Naltrexone for the Treatment of Chronic Pain Due to Arthritis: a Randomized, Double-blind, Placebo-controlled, Crossover Clinical Trial. Clin Ther. 2023;45(5):468–477. doi:10.1016/j.clinthera.2023.03.013
52. Bested K, Jensen LM, Andresen T, et al. Low-dose naltrexone for treatment of pain in patients with fibromyalgia: a randomized, double-blind, placebo-controlled, crossover study. Pain Rep. 2023;8(4):e1080. doi:10.1097/PR9.0000000000001080
53. Oaks Z, Stage A, Middleton B, Faraone SV, Johnson B. Clinical Utility of the Cold Pressor Test: evaluation of Pain Patients and Treatment of Opioid-Induced Hyperalgesia and Fibromyalgia with Low Dose Naltrexone. Discov Med. 2018;26(144):197–206.
54. Ramanathan S, Panksepp J, Johnson B. Is fibromyalgia an endocrine/endorphin deficit disorder? Is low dose naltrexone a new treatment option? Psychosomatics. 2012;53(6):591–594. doi:10.1016/j.psym.2011.11.006
55. Polo O, Pesonen P, Tuominen E. Low-dose naltrexone in the treatment of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Fatigue Biomed Health Behav. 2019;7(4):207–217. doi:10.1080/21641846.2019.1692770
56. Cree BAC, Kornyeyeva E, Goodin DS. Pilot trial of low-dose naltrexone and quality of life in multiple sclerosis. Ann Neurol. 2010;68(2):145–150. doi:10.1002/ana.22006
57. Sharafaddinzadeh N, Moghtaderi A, Kashipazha D, Majdinasab N, Shalbafan B. The effect of low-dose naltrexone on quality of life of patients with multiple sclerosis: a randomized placebo-controlled trial. Mult Scler Houndmills Basingstoke Engl. 2010;16(8):964–969. doi:10.1177/1352458510366857
58. Soin A. Management of pediatric complex regional pain syndrome with low-dose naltrexone. Interv Pain Manag Rep. 2021;5(3):109–113.
59. Weinstock LB, Myers TL, Walters AS, et al. Identification and Treatment of New Inflammatory Triggers for Complex Regional Pain Syndrome: small Intestinal Bacterial Overgrowth and Obstructive Sleep Apnea. AA Pract. 2016;6(9):272. doi:10.1213/XAA.0000000000000292
60. Ibrahim O, Hogan SR, Vij A, Fernandez AP. Low-Dose Naltrexone Treatment of Familial Benign Pemphigus (Hailey-Hailey Disease). JAMA Dermatol. 2017;153(10):1015–1017. doi:10.1001/jamadermatol.2017.2445
61. Jaros J, Lio P. Low Dose Naltrexone in Dermatology. J Drugs Dermatol. 2019;2019:1.
62. Kariv R, Tiomny E, Grenshpon R, et al. Low-Dose Naltreoxone for the Treatment of Irritable Bowel Syndrome: a Pilot Study. Dig Dis Sci. 2006;51(12):2128–2133. doi:10.1007/s10620-006-9289-8
63. Shannon A, Alkhouri N, Mayacy S, Kaplan B, Mahajan L. Low-dose naltrexone for treatment of duodenal Crohn’s disease in a pediatric patient. Inflamm Bowel Dis. 2010;16(9):1457. doi:10.1002/ibd.21185
64. de Carvalho JF, Skare T. Low-Dose Naltrexone in Rheumatological Diseases. Mediterr J Rheumatol. 2023;34(1):1–6. doi:10.31138/mjr.34.1.1
65. Due Bruun K, Christensen R, Amris K, et al. Effect of Naltrexone on Spinal and Supraspinal Pain Mechanisms and Functional Capacity in Women with Fibromyalgia: exploratory Outcomes from the Randomized Placebo-Controlled FINAL Trial. CNS Drugs. 2025;2025:1. doi:10.1007/s40263-025-01183-7
66. Due Bruun K, Christensen R, Amris K, et al. Naltrexone 6 mg once daily versus placebo in women with fibromyalgia: a randomised, double-blind, placebo-controlled trial. Lancet Rheumatol. 2024;6(1):e31–e39. doi:10.1016/S2665-9913(23)00278-3
67. Rivera V, DeCicco J, Espiritu S. Proceedings #47: low Dose Naltrexone: a Viable Alternative for Long Term Chronic Pain? Brain Stimulat. 2019;12(2):e118–e120. doi:10.1016/j.brs.2018.12.216
68. Kurta AO, Weinstock LB, Semchyshyn N. Erythromelalgia in a Patient with Mast Cell Activation Syndrome: response to Low Dose Naltrexone. SKIN J Cutan Med. 2020;4(3):288–291. doi:10.25251/skin.4.3.15
69. Weinstock LB, Brook JB, Myers TL, Goodman B. Successful treatment of postural orthostatic tachycardia and mast cell activation syndromes using naltrexone, immunoglobulin and antibiotic treatment. Case Rep. 2018;2018:1. doi:10.1136/bcr-2017-221405
70. Ghai B, Bansal D, Hota D, Shah CS. Off-Label, Low-Dose Naltrexone for Refractory Chronic Low Back Pain. Pain Med. 2014;15(5):883–884. doi:10.1111/pme.12345
71. Sangalli L, Miller CS. Low-dose naltrexone for treatment of burning mouth syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol. 2023;135(4):e83–e88. doi:10.1016/j.oooo.2022.04.048
72. Chang G, Chen L, Mao J. Opioid Tolerance and Hyperalgesia. Med Clin. 2007;91(2):199–211. doi:10.1016/j.mcna.2006.10.003
73. Ghlichloo I, Gerriets V. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs). In: StatPearls. StatPearls Publishing; 2023. Available from http://www.ncbi.nlm.nih.gov/books/NBK547742/.
74. Aitcheson N, Lin Z, Tynan K. Low-dose naltrexone in the treatment of fibromyalgia: a systematic review and narrative synthesis. Aust J Gen Pract. 2023;52(4):189–195. doi:10.31128/AJGP-09-22-6564
75. Yang J, Shin KM, Do A, et al. The Safety and Efficacy of Low-Dose Naltrexone in Patients with Fibromyalgia: a Systematic Review. J Pain Res. 2023;16:1017–1023. doi:10.2147/JPR.S395457
76. Irwin MN, David AC, Berland D, Marshall VD, Smith MA. Efficacy and Safety of Low Dose Naltrexone for Chronic Pain. J Pain Palliat Care Pharmacother. 2024;38(1):13–19. doi:10.1080/15360288.2024.2302550
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.