Back to Journals » Clinical Ophthalmology » Volume 16
Real-World Data on Intravitreal Aflibercept for Macular Edema Secondary to Central Retinal Vein Occlusion: 24-Month Outcomes
Authors Shimura M ![]() , Fukumatsu M, Tsujimura J, Hirano K, Sunaya T
, Fukumatsu M, Tsujimura J, Hirano K, Sunaya T
Received 20 October 2021
Accepted for publication 2 February 2022
Published 1 March 2022 Volume 2022:16 Pages 579—592
DOI https://doi.org/10.2147/OPTH.S344194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Masahiko Shimura,1 Makoto Fukumatsu,2 Jun Tsujimura,2 Kazufumi Hirano,2 Toshiyuki Sunaya3 On behalf of the Participating Investigators
1Department of Ophthalmology, Tokyo Medical University Hachioji Medical Center, Tokyo, Japan; 2Medical Affairs & Pharmacovigilance, Bayer Yakuhin, Ltd., Osaka, Japan; 3Research & Development Japan, Bayer Yakuhin, Ltd., Osaka, Japan
Correspondence: Masahiko Shimura, Department of Ophthalmology, Tokyo Medical University Hachioji Medical Center, 1163 Tate-machi, Hachioji, Tokyo, 193-0998, Japan, Tel +81 42 665 5611, Fax +81 42 665 1976, Email [email protected]
Purpose: To report on the safety and effectiveness of intravitreal aflibercept (IVT-AFL) for macular edema secondary to central retinal vein occlusion (CRVO) in clinical practice in Japan.
Patients and Methods: This prospective, noninterventional, multicenter post-authorization safety study enrolled patients who were treated with IVT-AFL for macular edema secondary to CRVO and followed up for 24 months. The primary outcome was the occurrence of safety events. Other pre-specified outcomes were indicators of effectiveness, including best corrected visual acuity (BCVA), central retinal thickness (CRT), and frequency of injections.
Results: The safety analysis included 377 patients who received at least one IVT-AFL. Adverse events (AEs) occurred in 22 patients (5.84%) and adverse drug reactions occurred in 5 (1.33%) over 24 months. Of the 22 patients with AEs, 72.7% experienced their first AEs by the third injection. The effectiveness analysis set comprised 360 patients for whom data on each outcome could be collected. The number of injections over 24 months was 3.4 ± 2.4 (mean ± standard deviation [SD]). BCVA (logarithm of the minimum angle of resolution) was 0.709 ± 0.535 (mean ± SD) (n = 357) at baseline and 0.543 ± 0.559 (n = 97) after 24 months of treatment with IVT-AFL. CRT was 552.6 ± 211.3 μm (mean ± SD) (n = 214) at baseline and 331.5 ± 144.0 μm (n = 54) at 24 months.
Conclusion: There were no new safety issues concerning routine administration of IVT-AFL for macular edema secondary to CRVO. BCVA recovered during 24 months of IVT-AFL treatment in the real-world setting. However, there was a trend toward less improvement compared with the results of randomized controlled trials, likely due in part to undertreatment.
Keywords: central retinal vein occlusion, macular edema, intravitreal aflibercept, anti-vascular endothelial growth factor treatment, real-world data
Introduction
Retinal vein occlusion (RVO) is an important cause of vision loss, particularly in patients with associated chronic macular edema that extends to the central fovea.1,2 RVO can be divided into two major categories, branch RVO (BRVO) and central RVO (CRVO), depending on the site of occlusion. The estimated prevalence of CRVO worldwide ranges from 0.08% to 0.13% and appears to be fairly constant across countries.3–5
Macular edema is thought to develop and expand in eyes with CRVO when the retina becomes ischemic due to reduced blood flow, excessive amounts of cytokines such as vascular endothelial growth factor (VEGF) are produced, and the permeability of blood vessels is increased.6 Therefore, VEGF is a potential therapeutic target, and the efficacy of intravitreal injection of anti-VEGF inhibitors in patients with macular edema secondary to CRVO has been demonstrated in large-scale randomized controlled trials (RCTs).7,8
Aflibercept (EYLEA®, Regeneron, Tarrytown, NY and Bayer HealthCare, Berlin, Germany) is an anti-VEGF agent that has higher binding affinity to VEGF-A than that of its native receptors and that also binds to VEGF-B and placental growth factor.9 After a report showing that intraocular VEGF and placental growth factor concentrations are high in patients with CRVO,10 it was hypothesized that the binding properties of aflibercept contribute to its efficacy. The clinical efficacy of intravitreal aflibercept (IVT-AFL) in patients with macular edema secondary to CRVO was evaluated as the 6-month primary outcome in two sham injection-controlled studies, COPERNICUS and GALILEO. In these studies, IVT-AFL was shown to be superior to sham injection in terms of visual improvement.7,11 Furthermore, a recent report suggested that fewer injections are needed for IVT-AFL to be effective in the treatment of macular edema secondary to CRVO compared with other anti-VEGF agents.12
Due to the invasive nature of the intraocular injections, a safety protocol must be followed for intravitreal injection of anti-VEGF agents. The main concern is that infectious organisms could potentially be introduced into the vitreous chamber, resulting in intraocular inflammation such as endophthalmitis. Mechanical issues associated with the injection procedure and pharmacodynamics-related local or systemic effects are also important.13 The risk of sterile intraocular inflammation after injection of anti-VEGF agents is a growing concern.14 Major risks, which were selected with reference to Phase III trials of IVT-AFL include arterial thromboembolic events, intraocular inflammatory response, increased intraocular pressure, retinal tear and detachment, and traumatic cataract.7,11,15–19
In the present study, we report 24 months of data on the safety and effectiveness of IVT-AFL treatment in patients with macular edema secondary to CRVO in the real-world clinical practice setting in Japan. To our knowledge, this is the first report of a prospective observational study in a large number of patients with macular edema secondary to CRVO who received IVT-AFL in Japan. Because this study reports local ocular and systemic safety results without limiting the baseline characteristics of patients except for treatment history of IVT-AFL, it is expected to be useful for understanding the actual situation in real-world clinical practice.
Materials and Methods
Study Design
This prospective, noninterventional, multicenter, post-authorization safety study in patients with macular edema secondary to CRVO in Japan was performed from November 2013 to May 2018. The survey component was conducted using the central registration method with electronic data capture (EDC). The maximum survey period was 24 months. Physicians registered patients, confirmed the initial injections, and entered the results at 6 months, 24 months, or the end of treatment. Observation was terminated in the event of 1) discontinuation of IVT-AFL due to adverse events (AEs), insufficient effectiveness or any other reason, or 2) loss to follow-up (no visit/contact on the scheduled visit date or within 4 months of the last visit).
The number of patients in the study was set at 300 to allow detection of at least one adverse drug reaction (ADR; AE considered by the clinician to be undeniably due to IVT-AFL) occurring with an incidence of 1% at a 95% probability.
Patients and Treatment
Patients of either sex with a diagnosis of macular edema secondary to CRVO were followed up after the decision had been made by the investigator to start treatment with IVT-AFL. Patients who had previously received IVT-AFL or were contraindicated based on the approved label were not followed. If both eyes were followed up, both were analyzed for safety and the eye that started IVT-AFL treatment earlier was analyzed for effectiveness. If both eyes started IVT-AFL on the same day, the one with worse visual acuity at baseline was selected.
Prior treatments for macular edema secondary to CRVO were recorded as variables if a patient had received an anti-VEGF treatment other than IVT-AFL, photocoagulation, surgery, or other therapy. After patients received the initial injection, the decision of repeat injections was left to the physician’s discretion. The interval between injections was set to be at least 1 month in accordance with the package insert.
Outcome Measures
The primary outcomes were AEs, ADRs, and ocular or non-ocular AEs. These events were coded based on Medical Dictionary for Regulatory Activities version 22.0 (MedDRA ver. 22.0) using its terminology for each type of event. In accordance with the risk management plan required by the Japanese Pharmaceutical and Medical Devices Agency, safety specifications consisting of important risks to be considered were also investigated. The safety specifications are listed in Supplementary Table 1.
Secondary outcomes were factors considered to affect safety, including the incidence of ADRs stratified by patient characteristics.
Other pre-specified outcomes were effectiveness variables (best corrected visual acuity [BCVA] and central retinal thickness [CRT]), which were summarized over time in the entire study population and subgroups (based on presence or absence of prior treatment and baseline decimal BCVA [≤0.1, >0.1 to ≤0.5, >0.5]), and the number of injections. The change in BCVA (logarithm of the minimum angle of resolution [logMAR]) from baseline was divided in three categories, and the proportion of patients in each category was calculated over time. These categories were as follows: “improved”, change in logMAR BCVA ≤−0.3; “maintained”, change in logMAR BCVA between −0.3 and 0.3; or “worsened”, change in logMAR BCVA ≥0.3. The relationship between number of injections and occurrence of AEs, the percentage of patients with final decimal BCVA >0.5, BCVA stratified by baseline decimal BCVA (<0.0625, ≥0.0625 to ≤0.5, >0.5), the number of injections in patients with both baseline and 24-month data, and changes in intraocular pressure for each subgroup based on the presence or absence (as a comorbidity or history) of glaucoma or ocular hypertension were analyzed as post hoc outcomes.
Statistical Analysis
The statistical analyses were exploratory and descriptive. Categorical variables were summarized as frequencies and proportions. Continuous variables were expressed as descriptive statistics. Patients who received at least one dose of IVT-AFL were included in the safety analysis set (SAS). The number and frequency of patients who developed ADRs or AEs between the first IVT-AFL injection and 24 months were summarized. Based on the classification of patient characteristics, the incidence of ADRs and 95% confidence intervals (CIs) were calculated. The effectiveness analysis set (EAS) included patients who had at least one measurement of BCVA or CRT available. The effectiveness analysis was performed using observed data; that is, the results were summarized over time only in patients for whom data for each outcome at each evaluation point could be collected. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
Patient Population
A total of 396 patients were enrolled, 377 of whom received at least one IVT-AFL injection and had electronic case report forms collected. These 377 patients were included in the SAS. After exclusion of patients whose BCVA and CRT could not be assessed, data for 360 patients were included in the EAS (Figure 1).
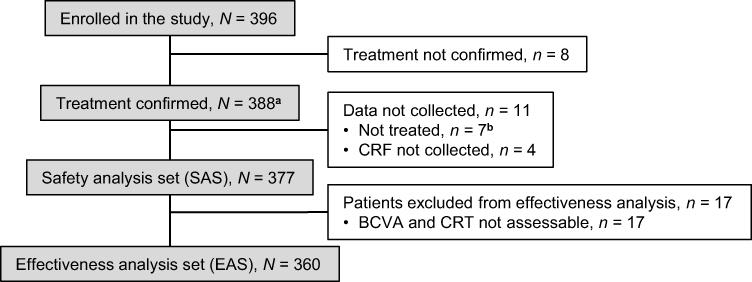 |
Figure 1 Flow of patients through the study. Abbreviations: BCVA, best corrected visual acuity; CRF, case report form; CRT, central retinal thickness. Notes: aEnrolled patients who were confirmed to have been either previously treated with IVT-AFL or not according to the enrollment form. bIncludes one patient for whom no record of use of IVT-AFL was found on the CRF. |
Patient characteristics at baseline in the SAS are shown in Table 1. Mean age was 72.0 years and 51.2% were male. The duration of disease before the start of IVT-AFL was less than 2 months in 95 patients (25.2%). Decimal BCVA at baseline was ≤0.1 in 130 patients (34.5%), >0.1 to ≤0.5 in 151 (40.1%), and >0.5 in 89 (23.6%). CRT was 552.1 ± 210.2 μm in the 217 patients for whom data were available. Two hundred and thirty-six patients (62.6%) had not previously received treatment and 134 (35.5%) had received prior treatment. Details of prior treatment are shown in Supplementary Table 2 and the Medical history is shown in Supplementary Table 3.
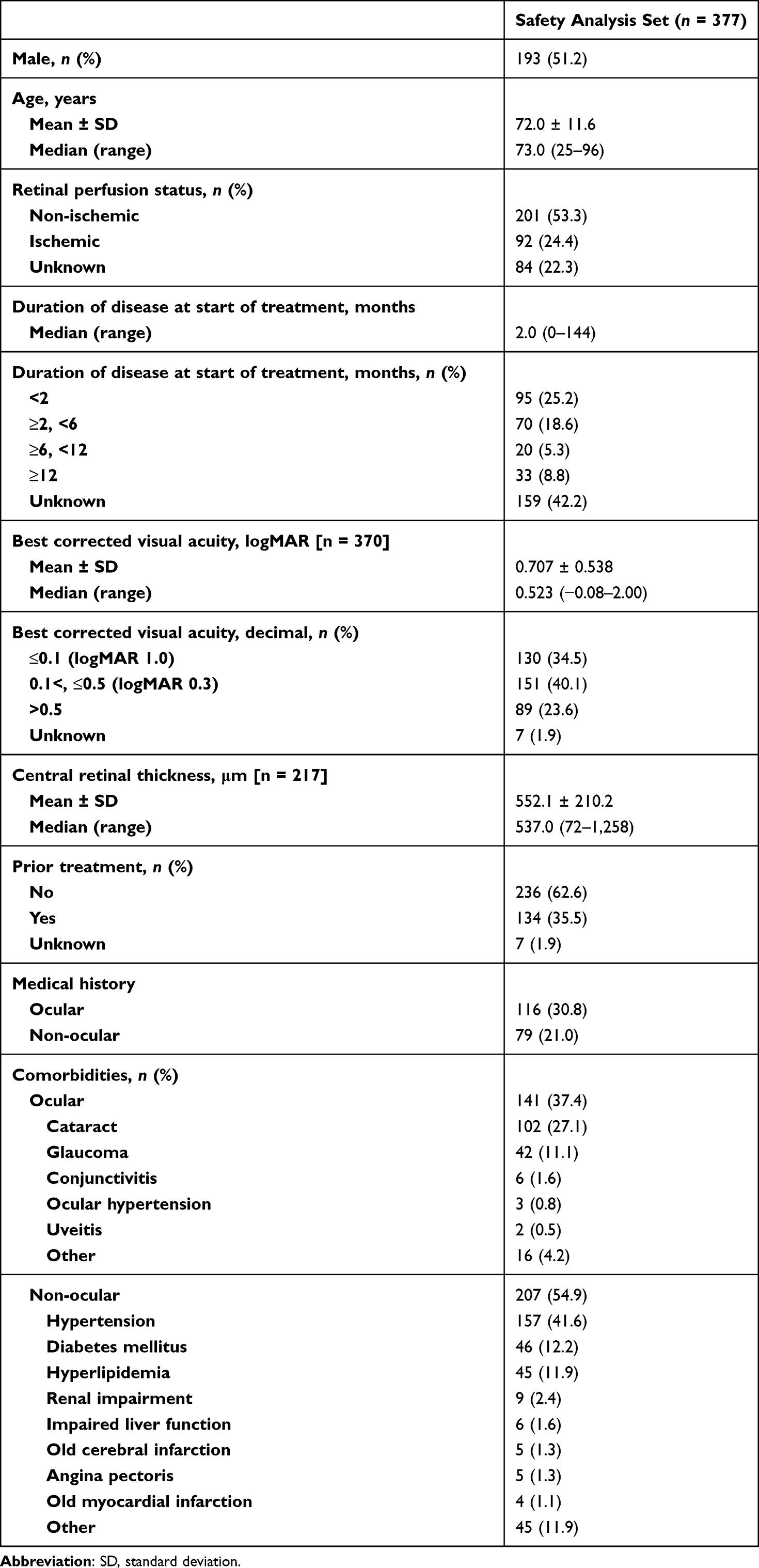 |
Table 1 Patient Characteristics at Baseline |
In the SAS, ocular comorbidities were reported in 141 patients (37.4%), including cataract in 102 (27.1%), glaucoma in 42 (11.1%), and conjunctivitis in 6 (1.6%). Two hundred and seven patients (54.9%) had non-ocular comorbidities, including hypertension (n = 157, 41.6%), diabetes mellitus (n = 46, 12.2%), and hyperlipidemia (n = 45, 11.9%).
Safety Outcomes
In the SAS, the duration of observation was 601.4 ± 286.5 days (median 724.0, range 1–1,204) and the number of injections was 3.3 ± 2.5. The median number of injections was 2 (range 1–15), and 107 patients (28.4%) received only one dose of IVT-AFL.
AEs occurred in 22 (5.84%) of the 377 patients in the SAS. SAEs included 2 patients with RVO (worsened ischemic CRVO in 1 patient and development of CRVO in the fellow eye in 1 patient) and 1 patient each with neovascular glaucoma, cataract, malignant glaucoma, cataract operation, bacterial pneumonia, malignant mesothelioma, facial paralysis, cardiac failure, myocardial infarction, familial amyloidosis, and death (Table 2). In the 22 patients with AEs, the number of injections until the first AE was 2.8; 72.7% had AEs by the third injection and 9.1% had their first AE after the seventh injection.
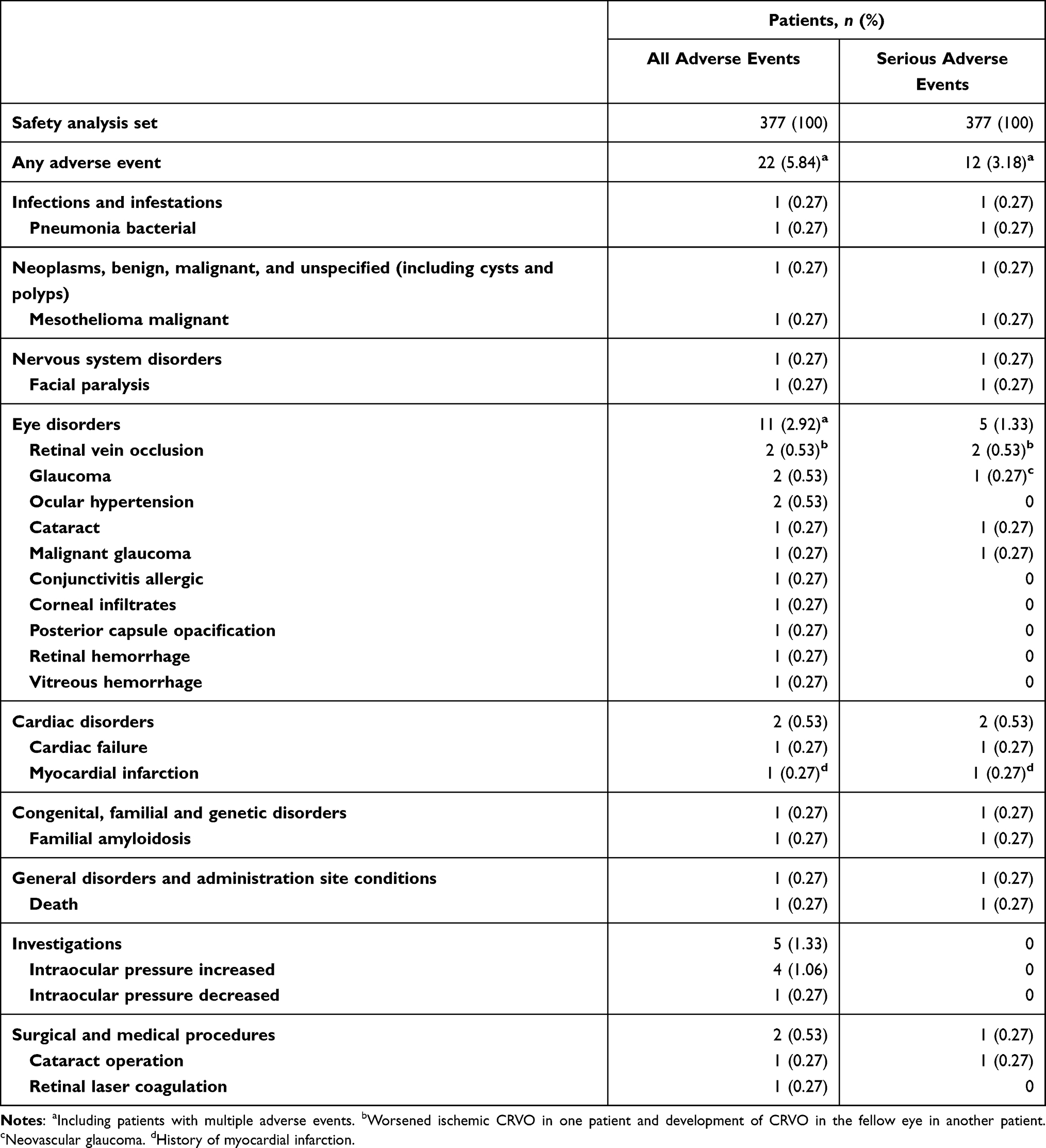 |
Table 2 Incidence of Adverse Events |
ADRs occurred in 5 patients (1.33%) in the SAS: 3 patients with increased intraocular pressure (all not serious) and 1 patient each with RVO and malignant glaucoma (both serious). Of the 3 patients with increased intraocular pressure, 1 patient had glaucoma, which was suspected to be a factor in this ADR in addition to IVT-AFL. No non-ocular ADRs were reported.
Among the 299 patients whose change in intraocular pressure was calculated, 59 had comorbidities or a history of glaucoma or ocular hypertension, with 13 patients (22.0%) having a change of 10 mmHg or more from baseline. Of the remaining 240 patients, 8 patients (3.3%) had a change of more than 10 mmHg.
Safety specifications defined by the risk management plan and observed as AEs were increased intraocular pressure (n = 6) and myocardial infarction (n = 1) (Table 3). No endophthalmitis or sterile intraocular inflammation was observed in this study.
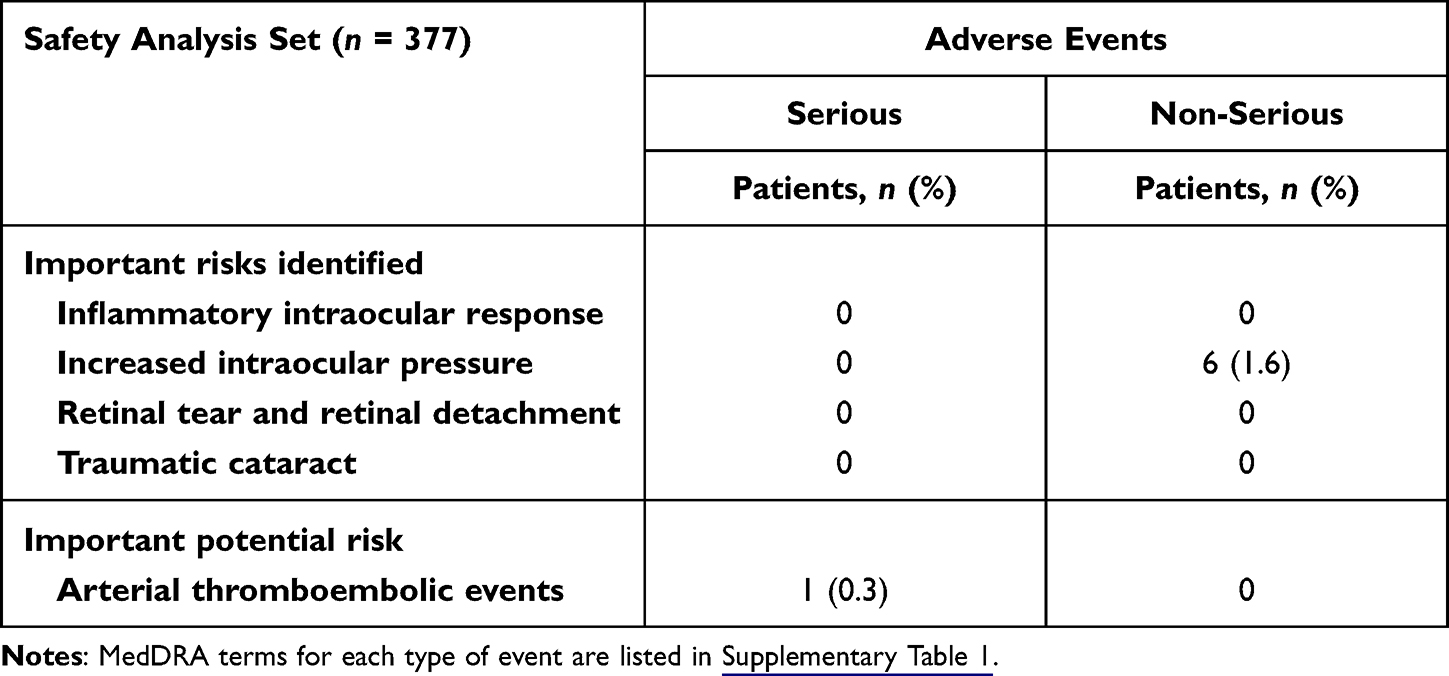 |
Table 3 Safety Specifications: Incidence of Serious and Non-Serious Adverse Events |
When stratified by patient characteristics, the 95% CIs for the incidence proportion of ADRs overlapped for all stratification factors, suggesting that no patient factors affected the occurrence of ADRs.
Effectiveness Outcomes
Treatment Status
The number of injections in the complete EAS (n = 360) was 2.1 ± 1.0 at 6 months, 2.7 ± 1.6 at 12 months, and 3.4 ± 2.4 (median 3, range 1–14) at 24 months. The duration of observation was 613.0 ± 279.5 days (median 728.0, range 1–1,204). The treatment continuation rate was 86.9% at 6 months, 76.7% at 12 months, and 61.4% at 24 months. The main reasons for discontinuation were referral to another hospital (n = 41, 29.5%), treatment goal achieved (n = 40, 28.8%), insufficient effectiveness (n = 10, 7.2%), and AEs (n = 2, 1.4%).
Visual Acuity
LogMAR BCVA was 0.709 ± 0.535 (median 0.523, range −0.08 to 2.00) (n = 357) at baseline and 0.543 ± 0.559 (median 0.398, range −0.18 to 2.00) (n = 97) after 24 months of treatment with IVT-AFL (Figure 2A). The change in logMAR BCVA between baseline and 24 months was −0.161 ± 0.446 (median −0.109, range −1.52 to 1.00, 95% CI −0.251 to −0.071) (n = 97) and the number of injections was 4.6 ± 2.8 (median 4, range 1–14). At 24 months, 32.0% of patients were evaluated as improved and 89.7% as improved or maintained (Supplementary Figure S1).
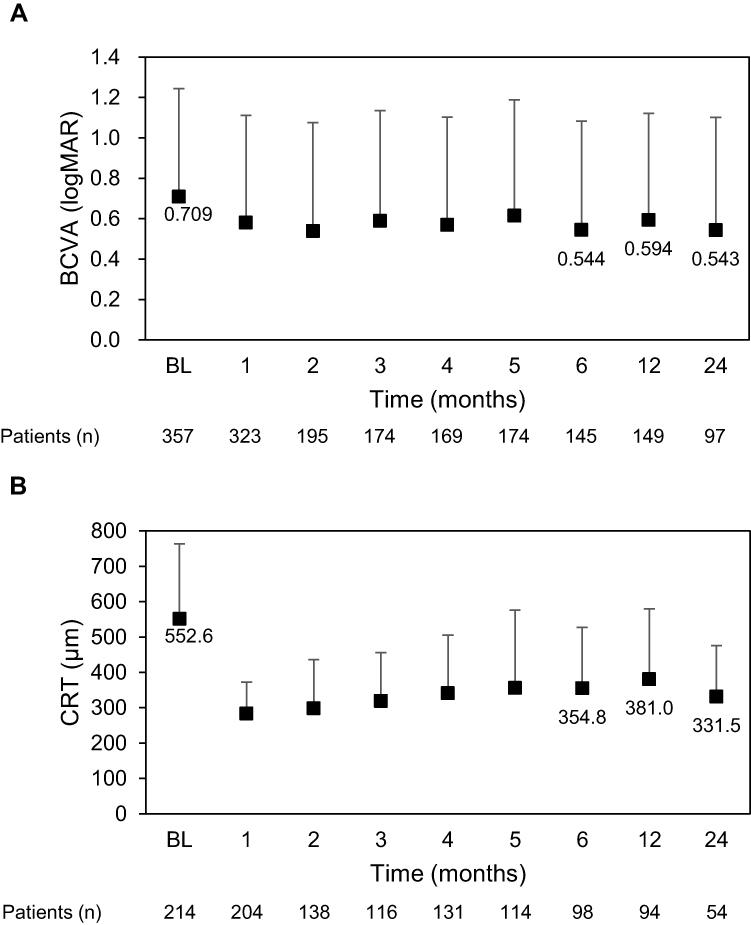 |
Figure 2 BCVA and CRT across 24 months. (A) LogMAR BCVA and number of patients across 24 months. (B) CRT (μm) and number of patients across 24 months. Markers and whiskers show the mean and standard deviation of BCVA and CRT, respectively. Abbreviations: BCVA, best corrected visual acuity; BL, baseline; CRT, central retinal thickness; logMAR, logarithm of the minimum angle of resolution. |
Post hoc analysis showed the proportion of patients with decimal BCVA >0.5 at the final visit to be 37.5% (134/357). Of the patients with a baseline decimal BCVA of >0.1 to ≤0.5, 38.1% had a final decimal BCVA >0.5.
Central Retinal Thickness
CRT was 552.6 ± 211.3 μm (median 535.5, range 72.0–1258) (n = 214) at baseline and 331.5 ± 144.0 (median 291.5, range 95.0–764.0) (n = 54) after 24 months of treatment with IVT-AFL (Figure 2B). The change in CRT between baseline and 24 months was −181.4 ± 258.3 μm (median −155.0, range −905 to 323, 95% CI −259.0 to −103.8) (n = 45).
Subgroup Analysis Based on Prior Treatment Status
LogMAR BCVA in the subgroups of patients with and without prior treatment was 0.826 ± 0.570 (n = 131) and 0.646 ± 0.503 (n = 219), respectively, at baseline and 0.792 ± 0.659 (n = 40) and 0.376 ± 0.396 (n = 56) at 24 months (Figure 3A). The change in logMAR BCVA between baseline and 24 months in the patients with and without prior treatment was −0.088 ± 0.487 (n = 40, 95% CI −0.244 to 0.068, 3.7 ± 2.5 injections) and −0.212 ± 0.415 (n = 56, 95% CI −0.323 to −0.101, 5.3 ± 3.0 injections), respectively.
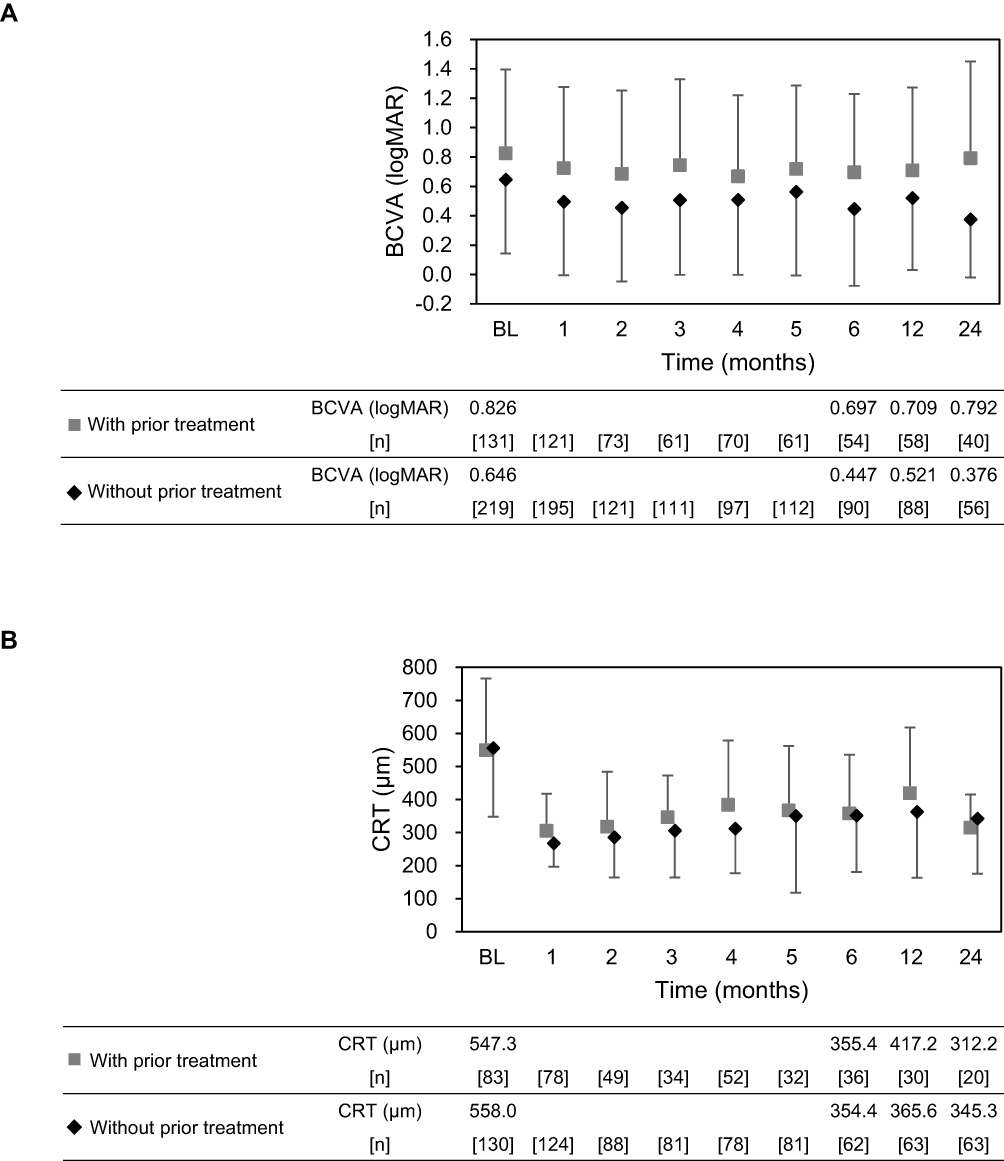 |
Figure 3 Subgroup analysis based on presence or absence of prior treatment. (A) LogMAR BCVA and number of patients across 24 months. (B) CRT (μm) and number of patients across 24 months. Markers and whiskers show the mean and standard deviation of BCVA and CRT, respectively. Abbreviations: BCVA, best corrected visual acuity; BL, baseline; CRT, central retinal thickness; logMAR, logarithm of the minimum angle of resolution. |
CRT in the patients with and without prior treatment was 547.3 ± 217.1 μm (n = 83) and 558.0 ± 207.9 μm (n = 130), respectively, at baseline and 312.2 ± 100.8 μm (n = 20) and 345.3 ± 166.6 μm (n = 33) at 24 months (Figure 3B). The change in CRT between baseline and 24 months in the patients with and without prior treatment was −225.0 ± 263.4 μm (n = 17, 95% CI −360.4 to −89.6) and −159.3 ± 260.2 μm (n = 27, 95% CI −262.2 to −56.4), respectively.
Subgroup Analysis Based on Decimal BCVA at Baseline
LogMAR BCVA in the subgroup of patients with a baseline decimal BCVA of ≤0.1, >0.1 to ≤0.5, or >0.5 was 1.326 ± 0.330 (n = 126), 0.519 ± 0.177 (n = 147), and 0.114 ± 0.097 (n = 84), respectively, at baseline and 0.948 ± 0.615 (n = 31), 0.506 ± 0.440 (n = 42), and 0.083 ± 0.148 (n = 24) at 24 months (Figure 4A). The change in logMAR BCVA between baseline and 24 months in the patients with a baseline decimal BCVA of ≤0.1, >0.1 to ≤0.5, or >0.5 was −0.434 ± 0.537 (n = 31, 95% CI −0.631 to −0.237, 4.1 ± 3.1 injections), −0.026 ± 0.397 (n = 42, 95% CI −0.149 to 0.098, 4.6 ± 2.9 injections), and −0.044 ± 0.161 (n = 24, 95% CI −0.133 to 0.024, 5.1 ± 2.4 injections), respectively.
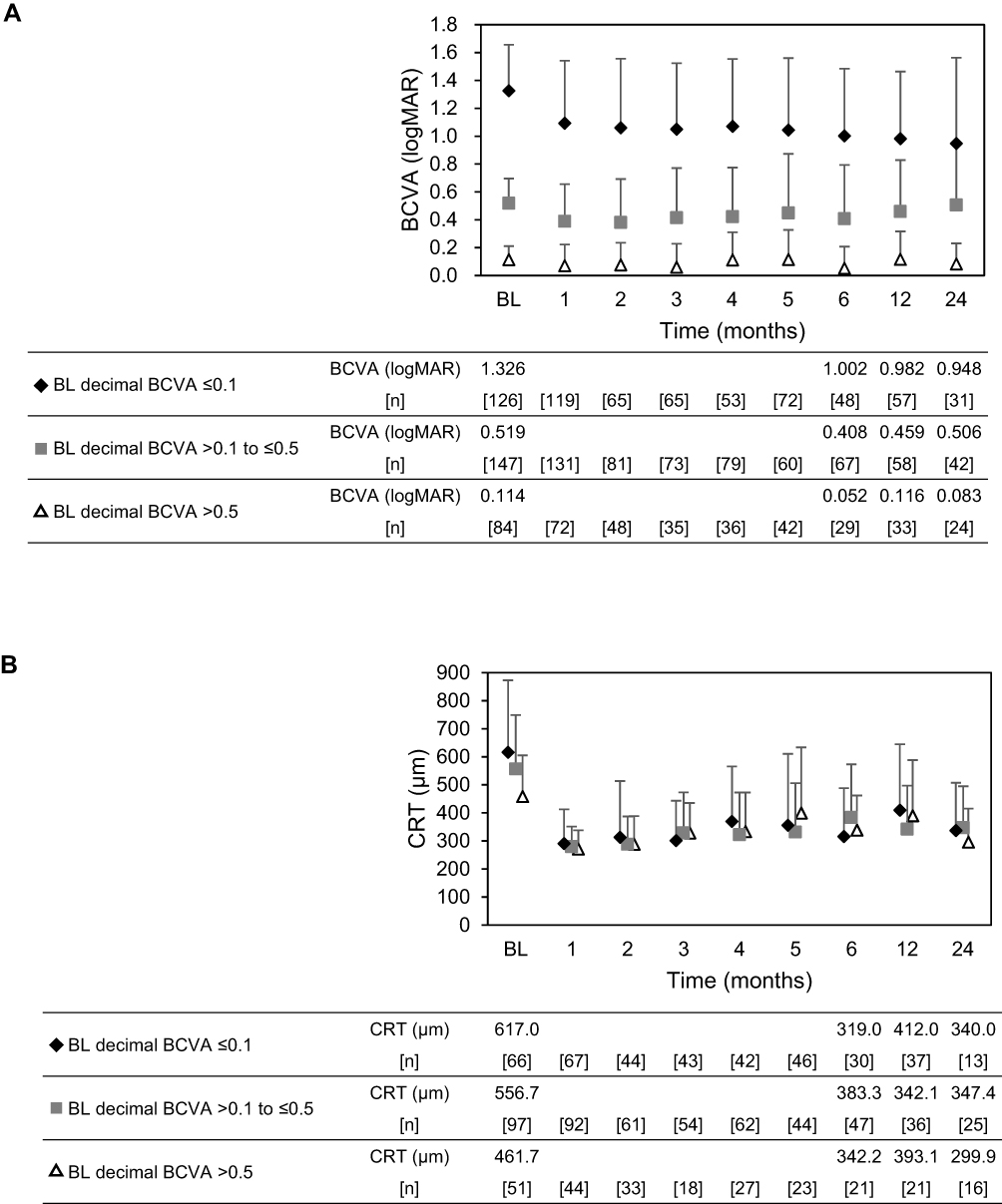 |
Figure 4 Subgroup analysis based on baseline decimal BCVA. (A) LogMAR BCVA and number of patients across 24 months. (B) CRT (μm) and number of patients across 24 months. Markers and whiskers show the mean and standard deviation of BCVA and CRT, respectively. Abbreviations: BCVA, best corrected visual acuity; BL, baseline; CRT, central retinal thickness; logMAR, logarithm of the minimum angle of resolution. |
CRT in the subgroups of patients with a baseline decimal BCVA of ≤0.1, >0.1 to ≤0.5, or >0.5 was 617.0 ± 254.6 μm (n = 66), 556.7 ± 191.8 μm (n = 97), and 461.7 ± 146.1 μm (n = 51), respectively, at baseline and 340.0 ± 169.1 μm (n = 13), 347.4 ± 147.6 μm (n = 25), and 299.9 ± 118.5 μm (n = 16) at 24 months (Figure 4B). The change in CRT between baseline and 24 months in the patients with a baseline decimal BCVA of ≤0.1, >0.1 to ≤0.5, or >0.5 was −294.4 ± 375.2 μm (n = 9, 95% CI −582.8 to −6.1), −173.0 ± 219.7 μm (n = 22, 95% CI −270.4 to −75.6), and −122.1 ± 220.1 μm (n = 14, 95% CI −249.1 to 5.0), respectively.
Given that the RCTs of IVT-AFL included patients with a baseline BCVA of 20/40 to 20/320,7,11 a subgroup analysis with boundaries for baseline decimal BCVA set at 0.0625 and 0.5 was performed as a post hoc analysis.
LogMAR BCVA in the subgroup of patients with baseline decimal BCVA of <0.0625 and ≥0.0625 to ≤0.5 was 1.547 ± 0.288 (n = 70) and 0.666 ± 0.283 (n = 203), respectively, at baseline and 1.051 ± 0.685 (n = 18) and 0.577 ± 0.467 (n = 55) at 24 months. The change in logMAR BCVA between baseline and 24 months in the patients with a baseline decimal BCVA of <0.0625 and ≥0.0625 to ≤0.5 was −0.547 ± 0.518 (n = 18, 95% CI −0.832 to −0.317, 3.1 ± 2.6 injections) and −0.076 ± 0.434 (n = 55, 95% CI −0.194 to 0.041, 4.8 ± 3.1 injections), respectively.
Discussion
In this study, the safety profile of IVT-AFL was assessed in patients with macular edema secondary to CRVO in a real-world setting, and no new safety concerns were observed beyond those reported in the RCTs.7,11 Although approximately 70% of the patients with AEs experienced their first AEs within the time period of the first three injections, there were some patients in whom the first AE happened after the seventh injection, indicating that careful administration and observation is needed for the entire duration of treatment.
Although no intraocular inflammation events were reported in the present study, an integrated analysis of RCTs found 1.42 patients with intraocular inflammation per 100 patient-years in the IVT-AFL group with a risk ratio of 0.66 relative to the sham-controlled group.20
In the present study, 3 patients had increased intraocular pressure as an ADR. However, among the patients with comorbidities or history of glaucoma or ocular hypertension, a relatively high proportion of patients experienced an increase in intraocular pressure of 10 mmHg or more, suggesting that these patients need to be carefully monitored.
Unlike the RCTs,7,11 this study did not exclude patients with a history of arterial thromboembolic events (Supplementary Table 3). Therefore, our findings are a better reflection of the real-world clinical use of IVT-AFL. In this study, an SAE of cardiac failure occurred in 1 patient, who had a medical history of myocardial infarction; however, a causal relationship between this event and treatment was ruled out. Doses of anti-VEGF agents are higher when administered systemically than when delivered by intravitreal injection, and it has been reported that anti-VEGF therapy for cancer may decrease production of nitric oxide and prostacyclin and increase that of erythropoietin, thereby increasing the risk of arterial thromboembolic events.21 Moreover, there is a report showing that intravitreal anti-VEGF injections decrease the plasma VEGF level.22 The risk of arterial thromboembolic events has been recognized as a potential risk, whereas no effects on a sensitive indicator of systemic VEGF inhibition, namely, blood pressure, was revealed by systemic pharmacokinetic/pharmacodynamic analysis of IVT-AFL in patients with retinal diseases.23
In this 24-month study, IVT-AFL rapidly improved mean BCVA and CRT in patients with macular edema secondary to CRVO and these results were sustained throughout the study period. However, the degree of improvement in both BCVA and CRT was smaller in this study than in the RCTs. The number of injections tended to be higher in the first 6 months after initiation of IVT-AFL and to decrease thereafter, resulting in patients receiving fewer injections in this study (4.6 ± 2.8 injections in 97 patients with BCVA data at both baseline and 24 months) compared with the RCTs. Furthermore, there were differences in baseline characteristics and study design between the RCTs and our real-world non-interventional study. In the RCTs, the injection regimen consisted initially of 6 monthly doses followed by maintenance doses given pro re nata,24,25 whereas in the real world, a regimen consisting of fewer or only one introduction dose might be adopted and physicians would carefully assess the need for reinjection after close observation. Additionally, there were no reinjection criteria based on morphological signs in this study. These factors coupled with fewer treatments than in the RCTs likely contributed to the less robust improvements in BCVA and CRT in the present study. Given the differences between real-world use and RCTs, it is necessary to consider an appropriate anti-VEGF treatment strategy for each patient in order to resolve the issue of the tendency for fewer treatments in clinical practice.
In the subgroup analysis of treatment-naïve patients, there was a higher number of injections and higher gains in BCVA compared with previously treated patients. This finding suggests the possibility that appropriate administration of treatment starting in the early stage of macular edema secondary to CRVO improves BCVA, as shown in clinical trials and expected by physicians. In the group with good BCVA at baseline, BCVA was maintained during the study. In the group with poor BCVA at baseline, although there was a marked gain in BCVA between baseline and the final visit, the final BCVA remained low. Specifically, in patients with a baseline BCVA in the middle range, which was an inclusion criterion for the RCTs, the change in logMAR BCVA was only −0.076. This was approximately +3.8 when converted to Early Treatment Diabetic Retinopathy Study letters and was considerably smaller compared with the change observed in the RCTs (over +13 letters),24,25 suggesting the potential to improve the treatment regimen in this population by administering a sufficient number of injections.
Recovery and retention of useful visual acuity (decimal BCVA ≥0.5) is a primary treatment goal for macular disease.26 In the present study, BCVA was improved or maintained at 24 months from baseline in 89.7% of patients, whereas only 37.5% had a decimal BCVA >0.5 at the final visit. This suggests that the rate of achieving the treatment goal in current clinical practice might be insufficient and that there is a need for early intervention and an improved regimen (eg, a treat-and-extend regimen) in order to obtain better vision and achieve better patient satisfaction.
Limitations
Decisions regarding diagnosis and examination were made at the physicians’ discretion. The eligibility criteria did not include or exclude patients based on risk of AEs or ADRs, but there is the possibility of selection bias if physicians did so. Unlike in the previous RCTs, the intervals between follow-up visits were not tightly controlled; therefore, not all data were collected for each outcome at each evaluation point, and the cohort data should be interpreted with caution.
Conclusion
This study did not detect any new safety signals concerning IVT-AFL in patients with macular edema secondary to CRVO under real-world clinical conditions. Given that nearly 90% of patients maintained BCVA throughout the 24 months of this study, it appears that the benefit–risk profile of IVT-AFL remains positive. More treatment benefit is likely to be obtained by early diagnosis and intervention, and by monitoring and administering injections at appropriate times. However, considering the trend of fewer treatments observed in this study, there may be little expectation of substantial improvement in visual acuity in patients who have been previously treated, especially in those with low baseline vision, who may show gains but continue to have low vision. These factors should be taken into account when considering treatment involving anti-VEGF agent in patients with macular edema secondary to CRVO.
Data Sharing Statement
Availability of the data underlying this publication will be determined in accordance with Bayer’s commitment to the EFPIA/PhRMA “Principles for responsible clinical trial data sharing.” This pertains to the scope, time point, and process of data access.
As such, Bayer commits to sharing upon reasonable request from qualified scientific and medical researchers those patient-level clinical trial data, study-level clinical trial data, and protocols from clinical trials in patients for medicines and indications approved in the United States (US) and European Union (EU) as necessary for conducting legitimate research. This applies to data on new medicines and indications that have been approved by the EU and US regulatory agencies on or after January 01, 2014.
Interested researchers can use www.clinicalstudydatarequest.com to request access to anonymized patient-level data and supporting documents from clinical studies to conduct further research that can help advance medical science or improve patient care. Information on the Bayer criteria for listing studies and other relevant information is provided in the “Study sponsors” section of the portal.
Data access will be granted to anonymized patient-level data, protocols, and clinical study reports after approval by an independent scientific review panel. Bayer is not involved in the decisions made by the independent review panel. Bayer will take all necessary measures to ensure that patient privacy is safeguarded.
Statement of Ethics
This surveillance was conducted as the regulatory-mandated study in compliance with the Good Post-marketing Study Practice (GPSP) and Good Vigilance Practice of the Ministry of Health, Labour and Welfare in Japan, and was registered on ClinicalTrials.gov (NCT02040220). In accordance with the governing GxP regulation of Japan post-marketing surveillance (ie, the GPSP ordinance), the process of informed consent was not defined at the start of this study, and approval by the ethics committee of each institution was not mandatory. Therefore, this surveillance was performed without informed consent based on the endorsement of the relevant health authorities.
Acknowledgments
Medical writing and editing support were provided by LiteraMed K.K. and ThinkSCIENCE, Inc. and the costs were borne by Bayer Yakuhin, Ltd. The study concept and design were provided by Bayer Yakuhin, Ltd. Bayer Yakuhin, Ltd. funded, collected, analyzed, and interpreted the data, and CMIC Co., Ltd. conducted the data management. All participating investigators provided care for the study patients and collected data.
Disclosure
Masahiko Shimura has no financial interest regarding this study. Makoto Fukumatsu, Jun Tsujimura, Kazufumi Hirano, and Toshiyuki Sunaya are employees of Bayer Yakuhin, Ltd. The authors report no other conflicts of interest in this work.
References
1. Campochiaro PA, Hafiz G, Shah SM, et al. Ranibizumab for macular edema due to retinal vein occlusions: implication of VEGF as a critical stimulator. Mol Ther. 2008;16(4):791–799. doi:10.1038/mt.2008.10
2. Klein R, Klein BE, Moss SE, Meuer SM. The epidemiology of retinal vein occlusion: the Beaver Dam Eye Study. Trans Am Ophthalmol Soc. 2000;98:133–141.
3. Rogers S, McIntosh RL, Cheung N, et al. International Eye Disease Consortium. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology. 2010;117:313–319.
4. Song P, Xu Y, Zha M, Zhang Y, Rudan I. Global epidemiology of retinal vein occlusion: a systematic review and meta-analysis of prevalence, incidence, and risk factors. J Glob Health. 2019;9:010427.
5. Laouri M, Chen E, Looman M, Gallagher M. The burden of disease of retinal vein occlusion: review of the literature. Eye. 2011;25:981–988.
6. Adamis AP, Shima DT. The role of vascular endothelial growth factor in ocular health and disease. Retina. 2005;25:111–118.
7. Boyer D, Heier J, Brown DM, et al. Vascular endothelial growth factor Trap-Eye for macular edema secondary to central retinal vein occlusion: six-month results of the Phase 3 COPERNICUS study. Ophthalmology. 2012;119:1024–1032.
8. Brown DM, Campochiaro PA, Singh RP, et al. CRUISE Investigators. Ranibizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology. 2010;117:1124–1133.
9. Papadopoulos N, Martin J, Ruan Q, et al. Binding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumab. Angiogenesis. 2012;15:171–185.
10. Noma H, Mimura T, Yasuda K, Shimura M. Role of soluble vascular endothelial growth factor receptor signaling and other factors or cytokines in central retinal vein occlusion with macular edema. Invest Ophthalmol Vis Sci. 2015;56(2):1122–1128. doi:10.1167/iovs.14-15789
11. Holz FG, Roider J, Ogura Y, et al. VEGF Trap-Eye for macular oedema secondary to central retinal vein occlusion: 6-month results of the phase III GALILEO study. Br J Ophthalmol. 2013;97:278–284.
12. Hykin P, Prevost AT, Vasconcelos JC, et al. LEAVO Study Group. Clinical Effectiveness of Intravitreal Therapy With Ranibizumab vs Aflibercept vs Bevacizumab for Macular Edema Secondary to Central Retinal Vein Occlusion: a Randomized Clinical Trial. JAMA Ophthalmol. 2019;137(11):1256–1264.
13. Falavarjani KG, Nguyen QD. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: a review of literature. Eye. 2013;27:787–794.
14. Witkin AJ, Hahn P, Murray TG, et al. Occlusive Retinal Vasculitis Following Intravitreal Brolucizumab. J Vitreoretin Dis. 2020;4:269–279.
15. Campochiaro PA, Clark WL, Boyer DS, et al. Intravitreal aflibercept for macular edema following branch retinal vein occlusion: the 24-week results of the VIBRANT study. Ophthalmology. 2015;122:538–544.
16. Heier JS, Brown DM, Chong V, et al. VIEW 1 and VIEW 2 Study Groups. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119:2537–2548.
17. Ikuno Y, Ohno-Matsui K, Wong TY, et al. MYRROR Investigators. Intravitreal Aflibercept Injection in Patients with Myopic Choroidal Neovascularization: the MYRROR Study. Ophthalmology. 2015;122:1220–1227.
18. Korobelnik JF, Do DV, Schmidt-Erfurth U, et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology. 2014;121:2247–2254.
19. Terasaki H, Shiraki K, Ohji M, et al. Efficacy and Safety Outcomes of Intravitreal Aflibercept Focusing on Patients with Diabetic Macular Edema from Japan. Retina. 2019;39:938–947.
20. Kitchens JW, Do DV, Boyer DS, et al. Comprehensive review of ocular and systemic safety events with intravitreal aflibercept injection in randomized controlled trials. Ophthalmology. 2016;123:1511–1520.
21. Kamba T, McDonald DM. Mechanisms of adverse effects of anti-VEGF therapy for cancer. Br J Cancer. 2007;96:1788–1795.
22. Jampol LM, Glassman AR, Liu D, et al. Plasma vascular endothelial growth factor concentrations after intravitreous anti-vascular endothelial growth factor therapy for diabetic macular edema. Ophthalmology. 2018;125:1054–1063.
23. Kaiser PK, Kodjikian L, Korobelnik JF, et al. Systemic pharmacokinetic/pharmacodynamic analysis of intravitreal aflibercept injection in patients with retinal diseases. BMJ Open Ophthalmol. 2019;4(1):e000185.
24. Heier JS, Clark WL, Boyer DS, et al. Intravitreal aflibercept injection for macular edema due to central retinal vein occlusion: two-year results from the COPERNICUS study. Ophthalmology. 2014;121:1414–1420.
25. Ogura Y, Roider J, Korobelnik JF, et al. GALILEO Study Group. Intravitreal aflibercept for macular edema secondary to central retinal vein occlusion: 18-month results of the phase 3 GALILEO study. Am J Ophthalmol. 2014;158:1032–1038.
26. Shimura M, Kitano S, Muramatsu D, et al. Japan Clinical Retina Study (J-CREST) group. Real-world management of treatment-naive diabetic macular oedema: 2-year visual outcome focusing on the starting year of intervention from STREAT-DME study. Br J Ophthalmol. 2020;104:1755–1761.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.